Ασυμπτωματικός ασθενής με διαταραχές αγωγής. Πρόγνωση θεραπεία
|
|
|
- Elaine Kelley
- 5 years ago
- Views:
Transcription

1 Ασυμπτωματικός ασθενής με διαταραχές αγωγής. Πρόγνωση θεραπεία Dr Ηλίας Θ. Ζάρβαλης Καρδιολόγος Επιμελητής Α Καρδιολογική Κλινική Γ. Ν. Παπαγεωργίου Θεσσαλονίκη


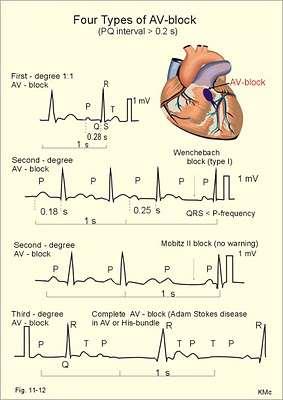
2 1899 he provided a description of irregular pulses due to partial blockage of AV conduction which created a progressive lengthening of conduction time 1924 Mobitz classified second-degree AV block into type I and type II using the electrocardio-gram
3

4 HV challenge: atrial pacing procainamide
5 AV block remains one of the most common reasons for pacemaker implantation there are still open questions about the indications for pacing lack of large, comparative, randomized studies, The situation may become even more complex when the conduction disturbance is intermittent The decision to implant a pacemaker is based, to a large extent, on the presence of symptoms that are directly related to the bradycardia caused by the AV block

6 complete AV block a number of nonrandomized studies showing that permanent cardiac pacing improves survival especially in patients who experience episodes of syncope
7 Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block Class I indication at any anatomic level in awake, symptom-free patients in sinus rhythm, with documented periods of asystole greater than or equal to 3.0 seconds or any escape rate less than 40 bpm, or with an escape rhythm that is below the AV node. (Level of Evidence: C) asymptomatic persistent third-degree AV block at any anatomic site with average awake ventricular rates of 40 bpm or faster if cardiomegaly or LV dysfunction is present or if the site of block is below the AV node. (Level of Evidence: B) at any anatomic level in awake, symptom-free patients with AF and bradycardia with 1 or more pauses of at least 5 seconds or longer. (Level of Evidence: C) ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. Circ 2008
8 Permanent pacemaker implantation is indicated for Class I indication Permanent pacemaker implantation is indicated for second- or third-degree AV block during exercise in the absence of myocardial ischemia. (Level of Evidence: C) at any anatomic level after catheter ablation of the AV junction. (Level of Evidence: C) at any anatomic level associated with postoperative AV block that is not expected to resolve after cardiac surgery. (Level of Evidence: C) at any anatomic level associated with neuromuscular diseases with AV block (Level of Evidence: B) ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. Circ 2008
9 Permanent pacemaker implantation is indicated for Class IIa indication Permanent pacemaker implantation is reasonable for persistent third-degree AV block with an escape rate greater than 40 bpm in asymptomatic adult patients without cardiomegaly. (Level of Evidence: C) ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. Circ 2008


10 Second-degree block type II Mobitz II
11 Second-degree block type II Mobitz II D. Zipes. Circ 1979 is usually infranodal (either intra- or infra- His) especially when the QRS is wide
12 Type II second-degree AV block symptoms are frequent prognosis is compromised and progression to third-degree AV block is common and sudden. Thus, type II second-degree AV block with a wide QRS typically indicates diffuse conduction system disease and constitutes an indication for pacing even in the absence of symptoms
13 second-degree AV block Class IIa indication for P/M Permanent pacemaker implantation is reasonable for asymptomatic second-degree AV block at intra- or infra-his levels found at electrophysiological study. (Level of Evidence: B) asymptomatic type II second-degree AV block with a narrow QRS. (Level of Evidence: B) When type II second-degree AV block occurs with a wide QRS, including isolated right bundle-branch block, pacing becomes a Class I recommendation. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. Circ 2008
14 second-degree AV block type I Mobitz I or Wenckenbach usually due to delay in the AV node irrespective of QRS width
15 Natural History of Chronic Second-degree Atrioventricular Nodal Block ECGs in all patients demonstrated episodes of type I second degree block electrophysiologic diagnosis of second-degree AV nodal block. 34% had no evidence of organic heart disease, and second-degree AV nodal block was considered to be idiopathic None of the patients (with or without syncope) were treated with pacemakers FU:1395 ± 636 days, 1/19 P/M 66% had clinically diagnosable organic heart disease FU:1347 ± 825 days, P/M:10/15 Among our 56 patients with chronic AV nodal block, 18 had an associated intraventricular conduction defect. All these patients had organic heart disease and most presented with either congestive heart failure or syncope. BORIS STRASBERG et al Circ 1981
16 second-degree AV block type I Mobitz I or Wenckenbach The natural history is related to the presence or absence of organic disease it is usually benign in the former and more malignant in the latter progression to advanced AV block in this situation is uncommon pacing is usually not indicated unless the patient is symptomatic.
17 asymptomatic type I second-degree AV block Class III indication for P/M Permanent pacemaker implantation is not indicated for asymptomatic type I second-degree AV block at the supra-his (AV node) level or that which is not known to be intra- or infra-hisian. (Level of Evidence: C) ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. Circ 2008
18 Survival in second degree atrioventricular block group 1: Mobitz type I block group 2: Mobitz type II block group 3: 2:1 or 3:1 block The presence or absence of bundle branch block did not appear to influence prognosis Even patients without major symptoms fared badly if left unpaced. DAVID B SHAW et al. Br Heart J 1985
19 Is Mobitz type I atrioventricular block benign in adults? Syncopal reason for referral was defined as a disturbance of consciousness (syncope or presyncope) Cardiac reason was palpitation, breathlessness, chest pain, or suspected cardiac failure Coincidental reason was discovery of Mobitz I on the preoperative ECG, during the health check, or during an intercurrent infection or other disease D B Shaw et al. Heart. 2004
20 Life table survival curves for patients with Mobitz I atrioventricular block who did not receive a pacemaker and for matched normal populations D B Shaw et al. Heart. 2004
21 Survival to the first outcome (death, deterioration in conduction, or symptomatic bradycardia) in patients with Mobitz I and to death in a matched normal population D B Shaw et al. Heart. 2004
22 Mobitz I was not benign in most of those studied who were aged > 45 years In class 3 47% of pts with organic heart disease D B Shaw et al. Heart. 2004
 and increased risk of ventricular")
23 Bifascicular blocks LBBB, RBBB+LAH, RBBB+LPH Prevalence: 1% to 1.5% in the adult population often a manifestation of serious underlying heart disease higher probability of progression to advanced atrioventricular block (AVB) and increased risk of ventricular arrhythmias, which results in an increase in mortality when compared to the general population. bundle-branch block is highly agedependent, uncommon (1.2%) at age 50 to becoming common (17%) at age 80 in the same population. Eriksson P et al. Circulation 1998;98:
24 Long-term mortality predictors in patients with chronic bifascicular block. Between 1998 and 2006, 259 consecutive patients with chronic bifascicular block FU: 4.5 years. mean age: 73 years, 47% structural heart disease, LVEF 35% in 12% of patients, 42% impaired renal function. prior syncope/pre-syncope (82% of the whole population). Marti-Almor J et al. Europace 2009;11:
25 Long-term mortality predictors in patients with chronic bifascicular block. death occurred in 20% of patients, cardiac death accounting for only about one-third (7%) of all deaths. Marti-Almor J et al. Europace 2009;11:
26 Hazard ratio for total and cardiac mortality during the follow-up using bivariate Cox models Marti-Almor J et al. Europace 2009;11:

27 Hazard ratio for total and cardiac mortality during the follow-up using multivariate Cox models Marti-Almor J et al. Europace 2009;11:
28 Long-term prognosis in patients with bifascicular block the predictive value of noninvasive and invasive assessment An annual all-cause mortality and sudden death of 4.7% and 2%, respectively F. TABRIZI et al. Journal of Internal Medicine July 2006
29 Long-term prognosis in patients with bifascicular block the predictive value of noninvasive and invasive assessment F. TABRIZI et al. Journal of Internal Medicine July 2006
30 total mortality rate in patients with bifascicular block Marti-Almor J et al. Europace 2009: (20.1% in a median follow-up of 4.5 years) Tabrizi F et al. J Intern Med 2006: a mortality rate of 33%, half of them due to SCD McAnulty JH et al. N Engl J Med 1982: mortality rate among BFB patients of 29%, 42% of which due to SCD Dhingra RC et al. Circulation 1981:total mortality of 38% was determined after a 7 year follow-up period, with SCD being mainly responsible for this mortality rate.
31 total mortality rate in patients with bifascicular block higher percentage of patients with structural heart disease and lower LVEF in these previous studies Moreover, drugs such as ACE-inhibitors, angiotensin receptor blockers, beta-blockers, or statins, with proven survival benefits, were less frequently administered when these studies were published than currently
32 Progression of atrioventricular block annual incidence of AVB ranging between 5% and 11% according to different series In asymptomatic patients, this is lower, ranging from 0.6% to 0.8%
33 independent predictors of advanced AVB? the presence of syncope and documentation of prolonged HV intervals in electrophysiological studies (EPS) The progression rate to AV block at 4 years was 4, 12, and 24%, respectively, for patients with an HV interval,55 ms (normal), 70 ms and 100 ms The sensitivity and specificity of the EPS has been questioned consensus on the limit value of the HV interval necessary to indicate the implementation of a pacemaker? currently accepted value is 70 ms in symptomatic patients and 100 ms in asymptomatic patients
34 Martí-Almor J et al. Rev Esp Cardiol Novel Predictors of Progression of Atrioventricular Block in Patients With Chronic Bifascicular Block 249 patients with BFB Mean age, 73.4 years median FU: 4.5 years 47% had structural heart disease
35 results no difference in the HV interval between different types of BFB HV interval was higher in patients with structural heart disease (68), compared to patients without heart disease (64) and Patients with CF II had a significantly higher HV interval (71), than patients in FC I (64) Martí-Almor J et al. Rev Esp Cardiol. 2010

36 Martí-Almor J et al. Rev Esp Cardiol. 2010
37 annual probability of requiring a pacemaker in symptomatic and asymptomatic patients the most important predictor was the HV interval, although this is only able to predict the need for PM in symptomatic patients in 33%. However, if you associate a QRS width > 140 ms, and renal failure, the probability increases to 95% in symptomatic patients and 59% of asymptomatic patients Martí-Almor J et al. Rev Esp Cardiol. 2010
38 Sensitivity and Specificity of the HV Interval the cut-off of 70 ms (guidelines of the ESC 2009) sensitivity of 74% and a specificity of 78% a cut-off of HV>64 ms sensitivity increase to 83% and specificity decreased to 70% with a positive predictive value (PPV) of 54% and negative predictive value (NPV) of 91%, with an area under the ROC curve of (95% CI, ) Martí-Almor J et al. Rev Esp Cardiol. 2010
39 Mechanism of Syncope in Patients With Bundle Branch Block and Negative Electrophysiological Test a negative EPS cannot rule out a paroxysmal AV block as the cause of syncope 33% of the patients with a negative study had a documented episode of AV block Brignole M et al. Circulation 2001;104:
40 Significance of chronic bifascicular block without apparent organic heart disease RC Dhingra et al. Circ 1979
41 spontaneous progression of conduction disease strong association of prolonged HV interval and severity of organic heart disease in patients with chronic bifascicular block the risk of developing spontaneous AV block in patients with primary conduction disease was significantly lower than in those with organic heart disease (1% vs 5%) In asymptomatic subjects with chronic bifascicular block, the risk of AV block is low and the sensitivity and specificity of a prolonged HV interval in predicting AV block would presumably be low His bundle recording would not be indicated as a routine diagnostic procedure. RC Dhingra et al. Circ 1979
42 Recommendations for Permanent Pacing in Class I: Chronic Bifascicular Block Permanent pacemaker implantation is indicated for advanced second-degree AV block or intermittent third-degree AV block. (Level of Evidence: B) Permanent pacemaker implantation is indicated for type II second-degree AV block. (Level of Evidence: B) Permanent pacemaker implantation is indicated for alternating bundle-branch block. (Level of Evidence: C) ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. Circ 2008
43 Recommendations for Permanent Pacing in Chronic Bifascicular Block Class IIa: Permanent pacemaker implantation is reasonable for an incidental finding at electrophysiological study of a markedly prolonged HV interval (greater than or equal to 100 milliseconds) in asymptomatic patients. (Level of Evidence: B) Permanent pacemaker implantation is reasonable for an incidental finding at electrophysiological study of pacing-induced infra-his block that is not physiological. (Level of Evidence: B) ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. Circ 2008
44 Diagnostic value of programmed ventricular stimulation in patients with bifascicular block: a prospective study of patients with and without syncope The inducibility of ventricular arrhythmias is high in patients with bifascicular block Clinical events during follow-up were not predicted by programmed ventricular stimulation in either of the two groups. The finding of inducible ventricular arrhythmia in patients with bifascicular block should therefore be interpreted with caution. A Englund et al. J Am Coll Cardiol, 1995
45 Συμπεράσματα Οι ασθενείς με διαταραχές της αγωγής έχουν αυξημένο ποσοστό επίπτωσης καρδιακής νόσου Η πρόγνωση τους ως αναφορά την θνητότητα και την επιδείνωση σε πλήρη κκα είναι χειρότερη από τον γενικό πληθυσμό και φαίνεται ότι συσχετίζεται με την υποκείμενη καρδιοπάθεια Οι ασυμπτωματικοί χωρίς καρδιακή νόσο ασθενείς έχουν καλύτερη πρόγνωση Η ΗΦΜ, ιδιαίτερα σε ασυμπτωματικούς ασθενείς έχει χαμηλή ευαισθησία και ειδικότητα ως προγνωστικό εργαλείο επιδείνωσης της αγωγής αλλά και αιφνίδιου θανάτου από κοιλιακή ταχυκαρδία
46 Θεραπεύουμε τους ασθενείς και όχι ΗΚΦηματα
The ECG Course. Boone County Fire Protection District EMS Education
 The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
Indications for Permanent Pacing Joe Gallinghouse, M.D. Texas Cardiac Arrhythmia Austin, Texas
 Indications for Permanent Pacing Joe Gallinghouse, M.D. Texas Cardiac Arrhythmia Austin, Texas Remember the Suture! Impulse Formation and Conduction Disturbances Cardiac Electrical Anatomy Sinoatrial Node
Indications for Permanent Pacing Joe Gallinghouse, M.D. Texas Cardiac Arrhythmia Austin, Texas Remember the Suture! Impulse Formation and Conduction Disturbances Cardiac Electrical Anatomy Sinoatrial Node
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013
 Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Is there a prognostic relevance of electrophysiological studies in bundle branch block patients?
 Received: 17 November 2016 Revised: 3 February 2017 Accepted: 9 February 2017 DOI: 10.1002/clc.22700 CLINICAL INVESTIGATIONS Is there a prognostic relevance of electrophysiological studies in bundle branch
Received: 17 November 2016 Revised: 3 February 2017 Accepted: 9 February 2017 DOI: 10.1002/clc.22700 CLINICAL INVESTIGATIONS Is there a prognostic relevance of electrophysiological studies in bundle branch
La strategia diagnostica: il monitoraggio ecg prolungato. Michele Brignole
 La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες
 Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou
Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/AV Blocks Connie J. Mattera, M.S., R.N., EMT-P
 Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
ESC/EHRA. Guidelines on Cardiac Pacing. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece
 ESC/EHRA Guidelines on Cardiac Pacing Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Reasons for European Guidelines? Scientific reasons Cultural and political reasons
ESC/EHRA Guidelines on Cardiac Pacing Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Reasons for European Guidelines? Scientific reasons Cultural and political reasons
13/09/2018. The ISSUE Studies. International (Italy & Spain) Study of Syncope of Uncertain Etiology. ISSUE study Pre-defined inclusion cathegories
 Study of Syncope of Uncertain Etiology. ISSUE study Pre-defined inclusion cathegories") The Studies Jean-Claude Deharo Aix-Marseille Université, France In Cardiac Electrophysiology Methods and Models Editors: Daniel C. Sigg, Paul A. Iaizzo, Yong-Fu Xiao, Bin He Springer 2010 study Pre-defined
The Studies Jean-Claude Deharo Aix-Marseille Université, France In Cardiac Electrophysiology Methods and Models Editors: Daniel C. Sigg, Paul A. Iaizzo, Yong-Fu Xiao, Bin He Springer 2010 study Pre-defined
Dipartimento di Scienze Cardiovascolari Università Campus Bio-Medico di Roma Dott. Vito Calabrese
 Dipartimento di Scienze Cardiovascolari Università Campus Bio-Medico di Roma Dott. Vito Calabrese Because the primary objective was cure symptomatic bradicardya due to syncope Because this is the common
Dipartimento di Scienze Cardiovascolari Università Campus Bio-Medico di Roma Dott. Vito Calabrese Because the primary objective was cure symptomatic bradicardya due to syncope Because this is the common
«Aσθενής με ασυμπτωματικό WPW και παροξυσμική κολπική μαρμαρυγή» Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ.
 «Aσθενής με ασυμπτωματικό WPW και παροξυσμική κολπική μαρμαρυγή» Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ» the primary mechanism of SCD in patients with WPW is the rapid conduction
«Aσθενής με ασυμπτωματικό WPW και παροξυσμική κολπική μαρμαρυγή» Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ» the primary mechanism of SCD in patients with WPW is the rapid conduction
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation
 The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
National Coverage Determination (NCD) for Cardiac Pacemakers (20.8)
 for Cardiac Pacemakers (20.8)") Page 1 of 12 Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Cardiac Pacemakers (20.8) Tracking Information Publication Number 100-3 Manual Section Number 20.8 Manual
Page 1 of 12 Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Cardiac Pacemakers (20.8) Tracking Information Publication Number 100-3 Manual Section Number 20.8 Manual
Asymptomatic patient with WPW
 Asymptomatic patient with WPW Dimosthenis Avramidis, MD. Arrythmiologist Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece Preexcitation
Asymptomatic patient with WPW Dimosthenis Avramidis, MD. Arrythmiologist Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece Preexcitation
Improving Patient Outcomes with a Syncope Center. Suneet Mittal, MD
 Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
MANAGEMENT OF ASYMPTOMATIC BRADYCARDIA. Pr. HABIB HAOUALA Service de Cardiologie Hôpital militaire de Tunis
 MANAGEMENT OF ASYMPTOMATIC BRADYCARDIA Pr. HABIB HAOUALA Service de Cardiologie Hôpital militaire de Tunis DISCLOSURE STATEMENT OF FINANCIAL INTEREST Grant/research: Medtronic;Sanofi; Novartis Consulting
MANAGEMENT OF ASYMPTOMATIC BRADYCARDIA Pr. HABIB HAOUALA Service de Cardiologie Hôpital militaire de Tunis DISCLOSURE STATEMENT OF FINANCIAL INTEREST Grant/research: Medtronic;Sanofi; Novartis Consulting
2018 ESC SYNCOPE GUIDELINES SUMMARY
 208 ESC SYNCOPE GUIDELINES SUMMARY NEW GUIDELINES OVERVIEW OF UPDATED RECOMMENDATIONS SINCE 2009 208 EUROPEAN SOCIETY OF CARDIOLOGY SYNCOPE GUIDELINES Goals of 208 Task Force Reducing Cost & Admissions:
208 ESC SYNCOPE GUIDELINES SUMMARY NEW GUIDELINES OVERVIEW OF UPDATED RECOMMENDATIONS SINCE 2009 208 EUROPEAN SOCIETY OF CARDIOLOGY SYNCOPE GUIDELINES Goals of 208 Task Force Reducing Cost & Admissions:
2:1 Block with Wenckebach Mechanism in Children Due to Different Etiologies F Laloğlu 1, N Ceviz 1, H Keskin 2, H Olgun 1 ABSTRACT
 2:1 Block with Wenckebach Mechanism in Children Due to Different Etiologies F Laloğlu 1, N Ceviz 1, H Keskin 2, H Olgun 1 ABSTRACT Objective: In children 2:1 Atrioventricular Block (AVB) with Wenckebach
2:1 Block with Wenckebach Mechanism in Children Due to Different Etiologies F Laloğlu 1, N Ceviz 1, H Keskin 2, H Olgun 1 ABSTRACT Objective: In children 2:1 Atrioventricular Block (AVB) with Wenckebach
Remote Monitoring & the Smart Home of the 21 Century
 Cardiostim EHRA Europace 2016, Nice - June 8-11, 2016 Remote Monitoring & the Smart Home of the 21 Century Antonio Raviele, MD, FESC, FHRS President ALFA -Alliance to Fight Atrial fibrillation- Venezia
Cardiostim EHRA Europace 2016, Nice - June 8-11, 2016 Remote Monitoring & the Smart Home of the 21 Century Antonio Raviele, MD, FESC, FHRS President ALFA -Alliance to Fight Atrial fibrillation- Venezia
Supplementary Online Content
 Supplementary Online Content Wahbi K, Meune C, Porcher R, et al. Electrophysiological study with prophylactic pacing and survival in adults with myotonic dystrophy and conduction system disease. JAMA.
Supplementary Online Content Wahbi K, Meune C, Porcher R, et al. Electrophysiological study with prophylactic pacing and survival in adults with myotonic dystrophy and conduction system disease. JAMA.
Σε όλους τους ασθενείς με σύνδρομο ευερέθιστου καρωτιδικού κόλπου και συγκοπή πρέπει να εμφυτεύεται μόνιμος βηματοδότης Κατά
 Σε όλους τους ασθενείς με σύνδρομο ευερέθιστου καρωτιδικού κόλπου και συγκοπή πρέπει να εμφυτεύεται μόνιμος βηματοδότης Κατά Δρ. H.Θ. Ζάρβαλης Καρδιολογική Κλινική Γ.Ν. Παπαγεωργίου Θεσσαλονίκη Classification
Σε όλους τους ασθενείς με σύνδρομο ευερέθιστου καρωτιδικού κόλπου και συγκοπή πρέπει να εμφυτεύεται μόνιμος βηματοδότης Κατά Δρ. H.Θ. Ζάρβαλης Καρδιολογική Κλινική Γ.Ν. Παπαγεωργίου Θεσσαλονίκη Classification
AHA/ACC Scientific Statement
 AHA/ACC Scientific Statement Eligibility and Disqualification for Competitive Athletes With Cardiovascular Abnormalities: Task Force 9: Arrhythmias and Conduction Defects A Scientific Statement From the
AHA/ACC Scientific Statement Eligibility and Disqualification for Competitive Athletes With Cardiovascular Abnormalities: Task Force 9: Arrhythmias and Conduction Defects A Scientific Statement From the
His Bundle Pacing: Where is it going? Kenneth A. Ellenbogen, M.D. Kontos Professor, VCU School of Medicine November 17, 2017
 His Bundle Pacing: Where is it going? Kenneth A. Ellenbogen, M.D. Kontos Professor, VCU School of Medicine November 17, 2017 Conflicts Medtronic: Research, Honoraria, Consulting Boston Scientific: Research,
His Bundle Pacing: Where is it going? Kenneth A. Ellenbogen, M.D. Kontos Professor, VCU School of Medicine November 17, 2017 Conflicts Medtronic: Research, Honoraria, Consulting Boston Scientific: Research,
Bradydysrhythmias and Atrioventricular Conduction Blocks
 Emerg Med Clin N Am 24 (2006) 1 9 Bradydysrhythmias and Atrioventricular Conduction Blocks Jacob W. Ufberg, MD*, Jennifer S. Clark, MD Department of Emergency Medicine, Temple University School of Medicine,
Emerg Med Clin N Am 24 (2006) 1 9 Bradydysrhythmias and Atrioventricular Conduction Blocks Jacob W. Ufberg, MD*, Jennifer S. Clark, MD Department of Emergency Medicine, Temple University School of Medicine,
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions
 InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc.
 Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc. The Miracle of Living February 21, 2018 Matthew Ostrom MD,FACC,FHRS Division of
Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc. The Miracle of Living February 21, 2018 Matthew Ostrom MD,FACC,FHRS Division of
Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm
 Discharges ICD Storm") Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm Guy Amit, MD, MPH Soroka University Medical Center Ben-Gurion University of the Negev Beer-Sheva, Israel Disclosures Consultant:
Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm Guy Amit, MD, MPH Soroka University Medical Center Ben-Gurion University of the Negev Beer-Sheva, Israel Disclosures Consultant:
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Second Degree Atrioventricular Block
 Marquette University e-publications@marquette Physician Assistant Studies Faculty Research and Publications Physician Assistant Studies, Department 2-18-2011 Second Degree Atrioventricular Block James
Marquette University e-publications@marquette Physician Assistant Studies Faculty Research and Publications Physician Assistant Studies, Department 2-18-2011 Second Degree Atrioventricular Block James
WPW in Athletes Should we treat all? age? RAMI FOGELMAN SCHNEIDER CHILDREN MEDICAL CENTER OF ISRAEL
 WPW in Athletes Should we treat all? age? RAMI FOGELMAN SCHNEIDER CHILDREN MEDICAL CENTER OF ISRAEL W.P.W Clues in sinus rhythm No Q in Lt chest leads (WPW 88%, control 5%) PR < 100msec (WPW 80%, control
WPW in Athletes Should we treat all? age? RAMI FOGELMAN SCHNEIDER CHILDREN MEDICAL CENTER OF ISRAEL W.P.W Clues in sinus rhythm No Q in Lt chest leads (WPW 88%, control 5%) PR < 100msec (WPW 80%, control
A Case of Alternating Bundle Branch Block in Combination With Intra-Hisian Block
 A Case of Alternating Bundle Branch Block in Combination With IntraHisian Block Yukie OGURA, 1 MD, Junichi KATO, 1 MD, Yuji OGAWA, 1 MD, Takahiro SHIOKOSHI, 1 MD, Toru KITAOKA, 1 MD, Takahide SUZUKI, 1
A Case of Alternating Bundle Branch Block in Combination With IntraHisian Block Yukie OGURA, 1 MD, Junichi KATO, 1 MD, Yuji OGAWA, 1 MD, Takahiro SHIOKOSHI, 1 MD, Toru KITAOKA, 1 MD, Takahide SUZUKI, 1
PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D.
 PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D. Cardiologist and Electrophysiologist No conflict of interest related to this presentation Objectives 1. PVCs are benign. What is the Evidence?
PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D. Cardiologist and Electrophysiologist No conflict of interest related to this presentation Objectives 1. PVCs are benign. What is the Evidence?
The relevance of a junctional rhythm during neurocardiogenic reaction provoked by tilt testing
 The relevance of a junctional rhythm during neurocardiogenic reaction provoked by tilt testing Dorota Zyśko, Jacek Gajek Wroclaw Medical University, Wroclaw, Poland ESC STOCKHOLM 2010 Junctional rhythm
The relevance of a junctional rhythm during neurocardiogenic reaction provoked by tilt testing Dorota Zyśko, Jacek Gajek Wroclaw Medical University, Wroclaw, Poland ESC STOCKHOLM 2010 Junctional rhythm
Sincope e bradicardia sinusale: quale è la terapia appropriata?
 Sincope e bradicardia sinusale: quale è la terapia appropriata? Paolo Alboni, Key points: 1 Fisiopatologia della sincope nei pz con BS 2 Diagnosi del tipo of sincope nei pz con BS 3 Trattamento della syncope
Sincope e bradicardia sinusale: quale è la terapia appropriata? Paolo Alboni, Key points: 1 Fisiopatologia della sincope nei pz con BS 2 Diagnosi del tipo of sincope nei pz con BS 3 Trattamento della syncope
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
ΜΥΟΚΑΡΔΙΟΠΑΘΕΙΕΣ. Ανεξήγητη βραδυκαρδία µε ή χωρίς διαταραχές κολποκοιλιακής αγωγής: τι µπορεί να κρύβει? ΕΦΗ Ι. ΠΡΑΠΠΑ Καρδιολόγος
 ΜΥΟΚΑΡΔΙΟΠΑΘΕΙΕΣ Ανεξήγητη βραδυκαρδία µε ή χωρίς διαταραχές κολποκοιλιακής αγωγής: τι µπορεί να κρύβει? ΕΦΗ Ι. ΠΡΑΠΠΑ Καρδιολόγος Β Καρδιολογική Κλινική, ΠΓΝΑ «Ο ΕΥΑΓΓΕΛΙΣΜΟΣ» CONFLICT of INTEREST : none
ΜΥΟΚΑΡΔΙΟΠΑΘΕΙΕΣ Ανεξήγητη βραδυκαρδία µε ή χωρίς διαταραχές κολποκοιλιακής αγωγής: τι µπορεί να κρύβει? ΕΦΗ Ι. ΠΡΑΠΠΑ Καρδιολόγος Β Καρδιολογική Κλινική, ΠΓΝΑ «Ο ΕΥΑΓΓΕΛΙΣΜΟΣ» CONFLICT of INTEREST : none
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Dos and Don t in Cardiac Arrhythmia. Case 1 -ECG. Case 1. Management. Emergency Admissions. Reduction of TE risk -CHADS 2 score. Hospital Admissions
 Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Long-term mortality predictors in patients with chronic bifascicular block
 Europace (2009) 11, 1201 1207 doi:10.1093/europace/eup181 CLINICAL RESEARCH Electrophysiology and Ablation Long-term mortality predictors in patients with chronic bifascicular block Julio Marti-Almor*,
Europace (2009) 11, 1201 1207 doi:10.1093/europace/eup181 CLINICAL RESEARCH Electrophysiology and Ablation Long-term mortality predictors in patients with chronic bifascicular block Julio Marti-Almor*,
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC
 Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
ECG interpretation basics
 ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Pediatrics. Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment. Overview
 Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect
 Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC
, FACC") Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC Consultant Interventional Cardiology & Structural Heart Disease Department of Medicine Sultan Qaboos University Hospital hatim.al.lawati@gmail.com April 2017
Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC Consultant Interventional Cardiology & Structural Heart Disease Department of Medicine Sultan Qaboos University Hospital hatim.al.lawati@gmail.com April 2017
Asymptomatic WPW Syndrome; Observation or Ablation? 전남대학교병원순환기내과 박형욱
 Asymptomatic WPW Syndrome; Observation or Ablation? 전남대학교병원순환기내과 박형욱 Let It Be? Vs. Just Do It? Natural history of asymptomatic WPW Incidence of sudden cardiac death in natural history studies involving
Asymptomatic WPW Syndrome; Observation or Ablation? 전남대학교병원순환기내과 박형욱 Let It Be? Vs. Just Do It? Natural history of asymptomatic WPW Incidence of sudden cardiac death in natural history studies involving
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation?
 How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
Cardiac Resynchronisation Therapy for all Patients Requiring Ventricular Pacing
 Cardiac Resynchronisation Therapy for all Patients Requiring Ventricular Pacing Philippe Mabo University Hospital, Rennes, France ESC Congress 2010, Stockholm 29 Aug 2010 Which Patients? Candidate for
Cardiac Resynchronisation Therapy for all Patients Requiring Ventricular Pacing Philippe Mabo University Hospital, Rennes, France ESC Congress 2010, Stockholm 29 Aug 2010 Which Patients? Candidate for
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ
 Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Implantable loop recorders Michele Brignole Arrhythmologic Center, Lavagna, Italy
 Implantable loop recorders Michele Brignole Arrhythmologic Center, Lavagna, Italy DECLARATION OF CONFLICT OF INTEREST Medtronic, minimal ILR: available devices Reveal DX/XT, Medtronic Confirm, St Jude
Implantable loop recorders Michele Brignole Arrhythmologic Center, Lavagna, Italy DECLARATION OF CONFLICT OF INTEREST Medtronic, minimal ILR: available devices Reveal DX/XT, Medtronic Confirm, St Jude
Conduction disorders
 Conduction disorders L.V. Bogun, N.I. Yabluchansky, F.M. Abdueva, O.Y. Bichkova, A.N. Fomich, P.A. Garkavyi, A.L. Kulik, N.V. Lysenko, N.V. Makienko, L.A. Martimyanova, I.V. Soldatenko, E.E. Tomina Department
Conduction disorders L.V. Bogun, N.I. Yabluchansky, F.M. Abdueva, O.Y. Bichkova, A.N. Fomich, P.A. Garkavyi, A.L. Kulik, N.V. Lysenko, N.V. Makienko, L.A. Martimyanova, I.V. Soldatenko, E.E. Tomina Department
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Antony French Consultant Cardiologist & Electrophysiologist
 Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
Göran Kennebäck 1 *, Fariborz Tabrizi 1,2, Peter Lindell 1, and Rolf Nordlander 2. Introduction. Methods. Patient population
 Europace (2007) 9, 186 191 doi:10.1093/europace/eul185 High-degree atrioventricular block during anti-arrhythmic drug treatment: use of a pacemaker with a bradycardia-detection algorithm to study the time
Europace (2007) 9, 186 191 doi:10.1093/europace/eul185 High-degree atrioventricular block during anti-arrhythmic drug treatment: use of a pacemaker with a bradycardia-detection algorithm to study the time
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
When to ablate patients with premature ventricular complexes?
 When to ablate patients with premature ventricular complexes? Nikolaos Fragakis Assistant Professor, FESC 3rd University Cardiology Department Hippokration Hospital, Thessaloniki 58 year-old female Case
When to ablate patients with premature ventricular complexes? Nikolaos Fragakis Assistant Professor, FESC 3rd University Cardiology Department Hippokration Hospital, Thessaloniki 58 year-old female Case
Cardiac rhythm detailed monitoring by an implanted pacemaker: The iecg solution
 Cardiac rhythm detailed monitoring by an implanted pacemaker: The iecg solution Francesco Zanon, MD, FESC, FHRS Arrhythmia and Electrophysiology Unit, Cardiology Dept. Santa Maria della Misericordia General
Cardiac rhythm detailed monitoring by an implanted pacemaker: The iecg solution Francesco Zanon, MD, FESC, FHRS Arrhythmia and Electrophysiology Unit, Cardiology Dept. Santa Maria della Misericordia General
Tachycardia-induced heart failure - Does it exist?
 Tachycardia-induced heart failure - Does it exist? PD Dr Etienne Delacrétaz Clinique Cecil et Hôpital de Fribourg SSC Cardiology meeting 2015 Zürich Rapid atrial fibrillation is a common cause of heart
Tachycardia-induced heart failure - Does it exist? PD Dr Etienne Delacrétaz Clinique Cecil et Hôpital de Fribourg SSC Cardiology meeting 2015 Zürich Rapid atrial fibrillation is a common cause of heart
Revisions to the BC Guide for Physicians in Determining Fitness to Drive a Motor Vehicle
 Revisions to the BC Guide for Physicians in Determining Fitness to Drive a Motor Vehicle Thank you for taking the time to review the draft Cardiovascular Diseases and Disorders chapter. Please provide
Revisions to the BC Guide for Physicians in Determining Fitness to Drive a Motor Vehicle Thank you for taking the time to review the draft Cardiovascular Diseases and Disorders chapter. Please provide
Value of the implantable loop recorder for the management of patients with unexplained syncope
 Europace (2004) 6, 70e76 Value of the implantable loop recorder for the management of patients with unexplained syncope Lucas Boersma a, ), Lluís Mont b, Alessandro Sionis b, Emilio García b, Josep Brugada
Europace (2004) 6, 70e76 Value of the implantable loop recorder for the management of patients with unexplained syncope Lucas Boersma a, ), Lluís Mont b, Alessandro Sionis b, Emilio García b, Josep Brugada
Atrial Fibrillation: Rate vs. Rhythm. Michael Curley, MD Cardiac Electrophysiology
 Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
EP WIRE on Management Preexcitation syndromes
 EP WIRE on Management Preexcitation syndromes 1. Is your Institution: A University Hospital 70.7% 41 A Private Hospital 13.8% 8 Other Type of Hospital 15.5% 9 Institution name: 50 answered question 58
EP WIRE on Management Preexcitation syndromes 1. Is your Institution: A University Hospital 70.7% 41 A Private Hospital 13.8% 8 Other Type of Hospital 15.5% 9 Institution name: 50 answered question 58
Tachycardias II. Štěpán Havránek
 Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ
 ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ ΣΤΕΛΙΟΣ ΠΑΡΑΣΚΕΥΑÏΔΗΣ ΔΙΕΥΘΥΝΤΗΣ ΕΣΥ Α Καρδιολογική Κλινική ΑΠΘ, Νοσοκομείο ΑΧΕΠΑ, Θεσσαλονίκη NO CONFLICT OF INTEREST Sudden Cardiac Death
ΤΙ ΠΡΕΠΕΙ ΝΑ ΓΝΩΡΙΖΕΙ ΟΓΕΝΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ ΓΙΑ ΤΙΣ ΔΙΑΥΛΟΠΑΘΕΙΕΣ ΣΤΕΛΙΟΣ ΠΑΡΑΣΚΕΥΑÏΔΗΣ ΔΙΕΥΘΥΝΤΗΣ ΕΣΥ Α Καρδιολογική Κλινική ΑΠΘ, Νοσοκομείο ΑΧΕΠΑ, Θεσσαλονίκη NO CONFLICT OF INTEREST Sudden Cardiac Death
Supplementary Online Content
 Supplementary Online Content Tseng ZH, Hayward RM, Clark NM, et al. Sudden death in patients with cardiac implantable electronic devices. JAMA Intern Med. Published online June 22, 2015. doi:10.1001/jamainternmed.2015.2641.
Supplementary Online Content Tseng ZH, Hayward RM, Clark NM, et al. Sudden death in patients with cardiac implantable electronic devices. JAMA Intern Med. Published online June 22, 2015. doi:10.1001/jamainternmed.2015.2641.
Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada
 Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας και Βηματοδότησης BrS: Diagnosis 5:10000 First described
Διαχείρηση Ασυμπτωματικού ασθενούς με ΗΚΓ τύπου Brugada Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας και Βηματοδότησης BrS: Diagnosis 5:10000 First described
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Tehran Arrhythmia Center
 Tehran Arrhythmia Center The Worst Scenario A 4 year old kid High heart rates first noted by parents at 20 months of age. Family physician detected rates as high as 220 bpm at that age. He was visited,
Tehran Arrhythmia Center The Worst Scenario A 4 year old kid High heart rates first noted by parents at 20 months of age. Family physician detected rates as high as 220 bpm at that age. He was visited,
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Η χρήση των νέων καθετήρων με αισθητήρα πίεσης Κλινικά δεδομένα και παραδείγματα
 Η χρήση των νέων καθετήρων με αισθητήρα πίεσης Κλινικά δεδομένα και παραδείγματα Νικόλαος Φραγκάκης Επίκουρος Καθηγητής Καρδιολογίας ΑΠΘ Γ Κ/Δ Κλινική Ιπποκράτειο Νοσοκομείο Θεσσαλονίκης Why Contact Force?
Η χρήση των νέων καθετήρων με αισθητήρα πίεσης Κλινικά δεδομένα και παραδείγματα Νικόλαος Φραγκάκης Επίκουρος Καθηγητής Καρδιολογίας ΑΠΘ Γ Κ/Δ Κλινική Ιπποκράτειο Νοσοκομείο Θεσσαλονίκης Why Contact Force?
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Case Report Mahaim Fiber Accelerated Automaticity and Clues to a Mahaim Fiber Being Morphologically an Ectopic or a Split AV Node
 www.ipej.org 62 Case Report Mahaim Fiber Accelerated Automaticity and Clues to a Mahaim Fiber Being Morphologically an Ectopic or a Split AV Node Shomu Bohora, Narayanan Namboodiri, Santosh Dora, VK Ajit
www.ipej.org 62 Case Report Mahaim Fiber Accelerated Automaticity and Clues to a Mahaim Fiber Being Morphologically an Ectopic or a Split AV Node Shomu Bohora, Narayanan Namboodiri, Santosh Dora, VK Ajit
Ενδείξεις αμφικοιλιακής βηματοδότησης. Ποιοι ασθενείς με καρδιακή ανεπάρκεια πρέπει να λάβουν αμφικοιλιακό απινιδωτή;
 Ενδείξεις αμφικοιλιακής βηματοδότησης. Ποιοι ασθενείς με καρδιακή ανεπάρκεια πρέπει να λάβουν αμφικοιλιακό απινιδωτή; Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας
Ενδείξεις αμφικοιλιακής βηματοδότησης. Ποιοι ασθενείς με καρδιακή ανεπάρκεια πρέπει να λάβουν αμφικοιλιακό απινιδωτή; Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Management of Syncope in Heart Failure. University of Iowa
 Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
Clinical Cardiac Electrophysiology
 Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
as the cause of recurrent syncope 3 allows appropriate management aimed
 Case Report Hellenic J Cardiol 2009; 50: 155-159 The Role of the Implantable Loop Recorder in the Investigation of Recurrent Syncope SKEVOS K. SIDERIS 1, TERESA A. MOUSIAMA 1, PAVLOS N. STOUGIANNOS 1,
Case Report Hellenic J Cardiol 2009; 50: 155-159 The Role of the Implantable Loop Recorder in the Investigation of Recurrent Syncope SKEVOS K. SIDERIS 1, TERESA A. MOUSIAMA 1, PAVLOS N. STOUGIANNOS 1,
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
 Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Summary, conclusions and future perspectives
 Summary, conclusions and future perspectives Summary The general introduction (Chapter 1) of this thesis describes aspects of sudden cardiac death (SCD), ventricular arrhythmias, substrates for ventricular
Summary, conclusions and future perspectives Summary The general introduction (Chapter 1) of this thesis describes aspects of sudden cardiac death (SCD), ventricular arrhythmias, substrates for ventricular
Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας. Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.
 Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.Γεννηματάς Clinical Trials on Fibrinolysis N = 61.41 AMI pts, ( GUSTO I, GUSTOIIb,
Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.Γεννηματάς Clinical Trials on Fibrinolysis N = 61.41 AMI pts, ( GUSTO I, GUSTOIIb,
Debate: Asymptomatic Patients with Ventricular Preexcitation Require EP Testing for Risk Stratification. Carlo Pappone, MD, PhD, FACC
 Debate: Asymptomatic Patients with Ventricular Preexcitation Require EP Testing for Risk Stratification Carlo Pappone, MD, PhD, FACC The Wolff-Parkinson-White Syndrome Demographics Δ waves detectable on
Debate: Asymptomatic Patients with Ventricular Preexcitation Require EP Testing for Risk Stratification Carlo Pappone, MD, PhD, FACC The Wolff-Parkinson-White Syndrome Demographics Δ waves detectable on