March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
|
|
|
- Marvin Cooper
- 6 years ago
- Views:
Transcription
1 Case 1
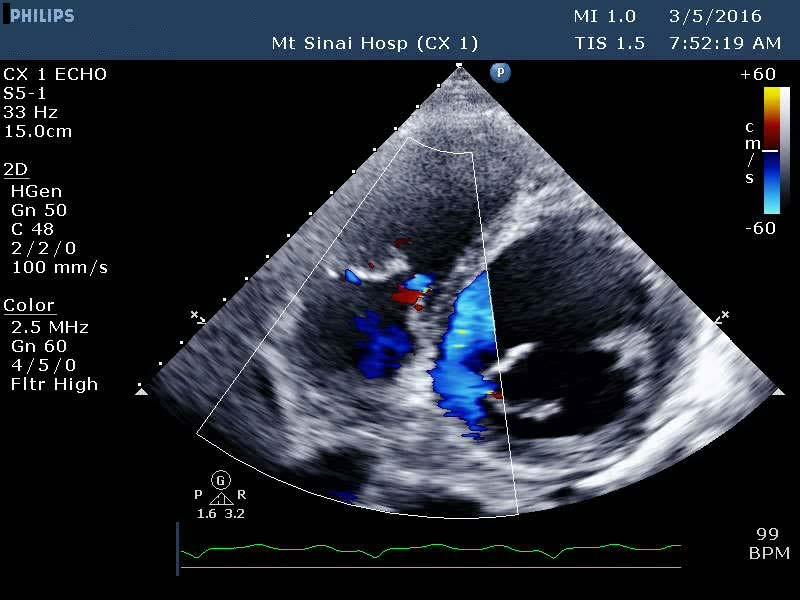
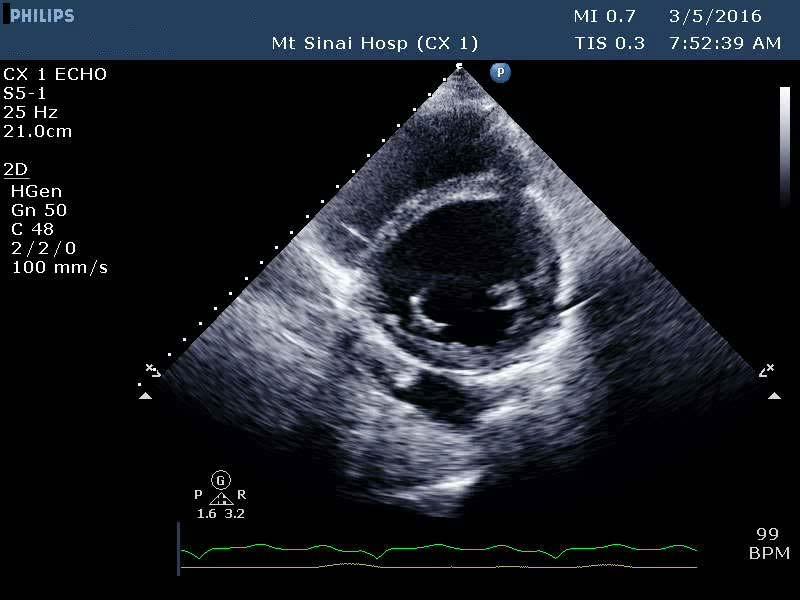
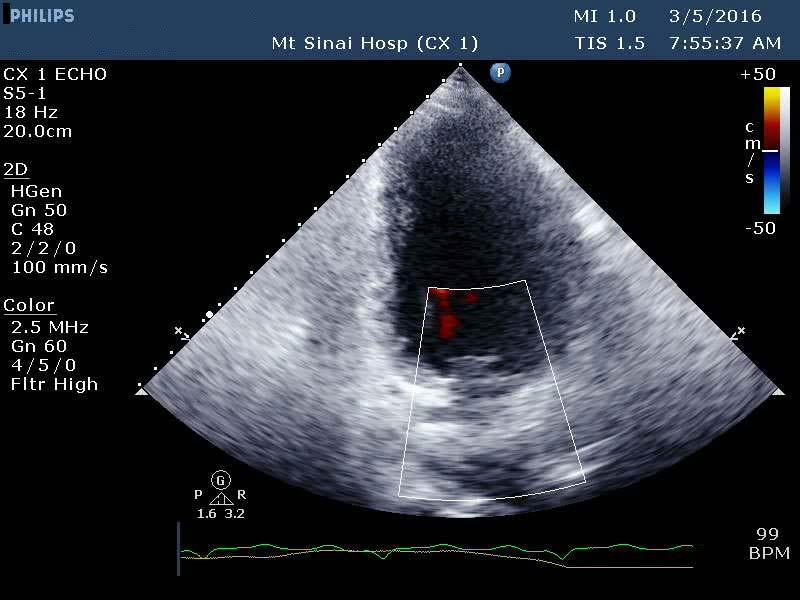
2 March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10 days ED admission: found hyperkalemic (6mEq/L); worsening SOB, anxiety PEA arrest 5 min after Lorazepam administration Resuscitated; admitted to CCU

3 Transthoracic Echocardiogram Mar 2016 BP 130/40 mmhg Height 5 11 Weight 167 lb


4 BP 130/40 mmhg Height 5 11 Weight 167 lb
5
6
7



8 Cardiac Catheterization Coronaries: 100% mid LAD, 100% OM1, 80% RCA Hemodynamics: LV 120/16; PCW 20mmHg, PA 62/24 mmhg, RA15mmHg, CI 1.7L/min/m²
9 Myocardial Perfusion Scan Abnormal, consistent with moderate anteroapical, mild apical and septal, and mild to moderate inferolateral viability. Mild to moderate anteroseptal and mild inferoposterior scarring LVEF 22%
10 Summary 59-year-old male with progressive dyspnea and orthopnea presents to ER with acute CHF symptoms and PEA arrest Imaging: Moderate-severe AI, mild MR, mild TR (RVSP 44mmHg) LVEDD 7.5 cm, LVESD 6.2 cm, LA 4.5cm, LVEF 21% Sub-total LV hypokinesia (basal segments hypokinetic) Moderate RV dilatation, moderate-severe RV dysfunction. 3 Vessel CAD
11 Management Hypothermic protocol, extubated Commenced aggressive diuresis Medical therapy for CAD HF therapy: carvedilol, Lisinopril, Digoxin, Spironolactone Endocrine + Nutritional optimization (noted T2DM, protein deficit) CT Surgery consult
12 M 59y: 1 st presentation of ischemic/valvular cardiomyopathy; severe AI What would you recommend? 1. Continue medical therapy + follow-up in 4 weeks 2. CABG + AVR 3. Refer for LVAD 4. PCI then follow-up in 4 weeks
13 Plan of Care Presented with operative risk, patient opted to defer surgery and try medical therapy first Continue diuresis, neurohormonal inhibitors (entresto) Nutritional, metabolic, and endocrine optimization Follow up with HF, Cardiology and CVS as outpatient

14 March to October 2016 Doing well Asymptomatic. Walks 5 miles daily Writing weekly articles for NY Times On GDMT for HF

15 6 Month Follow-Up Cardiology Visit. October 2016 Continues to do well NYHA class I Wishes to continue current plan of medical therapy Declined AICD Follow up in 4 months with exercise stress-test
 Terminated for dyspnea ST")

16 Stress Echocardiogram Feb min 01sec; 4 METS (70-84% pred peak HR) Terminated for dyspnea ST elevation anterior/septal segments; transient ischemic LV dilatation Severe PHTN at peak (RVSP 86mmHg Vs 40mmHg at rest)
17 February 2017 Admitted post-stress test Cardiac catheterization: Coronaries unchanged. Hemodynamics LV 120/16 mmhg, Ao 120/50 mmhg, PCW 12 mmhg, PA 35/15 mmhg, RA 6 mmhg, CI 2.5 l/min/m 2 Echocardiogram Severe AI, LVEF 25%, LVEDD 7.5 cm, Moderate RV dysfunction
18 Summary 60 y male with asymptomatic ischemic cardiomyopathy, severe aortic regurgitation and severe LV systolic dysfunction re-presents with positive stress test.
19 What would you recommend? 1. Continue medical therapy 2. CABG + AVR 3. PCI + TAVR 4. Refer for transplantation 5. Further testing
20 Patient opts for surgery which valve? 1. Biological 2. Mechanical

21 March 2016 AVR: 25mm St Jude Trifecta Bovine Pericardial Valve CABG x 4: LIMA to LAD; LIMA to D1; Radial Artery to OM1; SVG to PDA Uneventful recovery, discharged home on POD 7


22 Discharge Transthoracic Echocardiogram BP 119/69 mmhg Height 72in Weight 173 lb


23 Absent AR, trace MR, mild TR (RVSP 30mmHg) LVEDD 5.5cm, LVESD 4.7cm, EF 33%

24 4-month F/U Transthoracic Echocardiogram BP 119/69 mmhg Height 72in Weight 173 lb


25 Mar 2016:Baseline EF 21% Jul 2017: Postop EF 38%

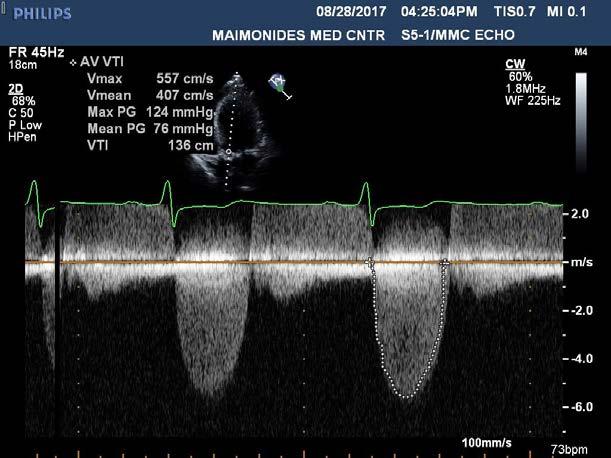
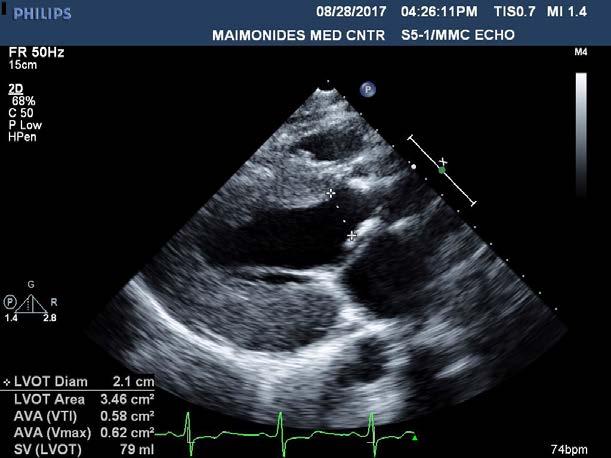
26 Case 2 26 year old male with remote history of heart murmur Progressive dyspnea on mild exertion past few months Referred for cardiology consult by PCP


27 Transthoracic Echocardiogram Aug 2017 BP 130/40 mmhg Height 5 11 Weight 167 lb



28


29
, severe AR, complex AV calcification involving the AMVL, mild MR, mild TR concentric LVH (LVPWd 1.7cm, IVSd 1.6cm) LVEDD 5.9cm, LVESD 3.")
30 Summary Previously asymptomatic 26-year-old male with known heart murmur develops dyspnea on mild exertion Initial TTE report: Severe AS (AVA 0.7cm², mean PG 75 mmhg), severe AR, complex AV calcification involving the AMVL, mild MR, mild TR concentric LVH (LVPWd 1.7cm, IVSd 1.6cm) LVEDD 5.9cm, LVESD 3.6cm, LA 4.5cm, EF 55-60%

31 What would you recommend? 1. Active surveillance, repeat TTE in 3 months 2. Aortic valve replacement - mechanical 3. Aortic valve replacement - biological 4. TAVR 5. Ross

32 Management All AVR options were discussed in detail Patient felt strongly against anticoagulation Opted for Ross procedure Underwent Ross operation. Doing well 3 weeks post-op
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
CASE STUDIES IN ADVANCED HEART FAILURE
 CASE STUDIES IN ADVANCED HEART FAILURE Navin Rajagopalan, MD Director, Congestive Heart Failure Medical Director, Cardiac Transplantation Gill Heart Institute, Cardiovascular Medicine DISCLOSURES NOTHING
CASE STUDIES IN ADVANCED HEART FAILURE Navin Rajagopalan, MD Director, Congestive Heart Failure Medical Director, Cardiac Transplantation Gill Heart Institute, Cardiovascular Medicine DISCLOSURES NOTHING
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
APOLLO TMVR Trial Update: Case Presentation
 APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Susan P. D Anna MSN, APRN BC February 14, 2019
 Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Is there Equal Opportunity in Heart Failure?? Susan P. D Anna MSN, APRN BC February 14, 2019 Disclosures: I have no financial disclosures. I am not an expert on this topic, but see a lot of women with
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Percutaneous coronary intervention of RIMA. The real challenge!
 Percutaneous coronary intervention of RIMA The real challenge! Speaker's name: I do not have any potential conflict of interest Clinical Case 76-year old woman Previous History Actual Disease Diabetes
Percutaneous coronary intervention of RIMA The real challenge! Speaker's name: I do not have any potential conflict of interest Clinical Case 76-year old woman Previous History Actual Disease Diabetes
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Conflict Disclosures. Vermont Cardiac Network. Outline. Series Learning Objectives 4/27/2016. Scott E. Friedman April 28, 2016
 Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Abnormal, Autoquant Adenosine Myocardial Perfusion Heart Imaging. ID: GOLD Date: Age: 46 Sex: M John Doe Phone (310)
") Background: Reason: preoperative assessment of CAD, Shortness of Breath Symptom: atypical chest pain Risk factors: hypertension Under influence: a beta blocker Medications: digoxin Height: 66 in. Weight:
Background: Reason: preoperative assessment of CAD, Shortness of Breath Symptom: atypical chest pain Risk factors: hypertension Under influence: a beta blocker Medications: digoxin Height: 66 in. Weight:
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis
 TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
Revascularization Strategies in Patients with Severe LV Dysfunction
 Revascularization Strategies in Patients with Severe LV Dysfunction Richard Lee, M.D., M.B.A. Saint Louis University The Center for Comprehensive Cardiovascular Care C4 Severe LV Dysfunction Defined as
Revascularization Strategies in Patients with Severe LV Dysfunction Richard Lee, M.D., M.B.A. Saint Louis University The Center for Comprehensive Cardiovascular Care C4 Severe LV Dysfunction Defined as
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Ve V rmont rmon Card Car iac d Netw Ne ork tw Scott E. Friedman April 28, 2016
 Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability
 Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Culprit vs Multivalve Transcatheter Intervention
 Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
Clinical Summary. Live Cases I - IX
 Clinical Summary Live Cases I - IX Case #1 2017/09/16 Age: 66 Target Vessel: RCA proximal Relevant Diagnosis: Single vessel CAD with normal LVEF Coronary Risk Factors: Hypertension, smoke (90py) ECG abnormality:
Clinical Summary Live Cases I - IX Case #1 2017/09/16 Age: 66 Target Vessel: RCA proximal Relevant Diagnosis: Single vessel CAD with normal LVEF Coronary Risk Factors: Hypertension, smoke (90py) ECG abnormality:
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Acute Circulatory Support Should We or Shouldn t We?
 Acute Circulatory Support Should We or Shouldn t We? Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional Research
Acute Circulatory Support Should We or Shouldn t We? Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional Research
@02-126_Coronary_calcification.ppt. Professor Molecular and Medical Pharmacology
 Assessment of Myocardial Viability Jamshid Maddahi, M.D., FACC, FASNC Professor Molecular and Medical Pharmacology (Nuclear Medicine) and Medicine (Cardiology) David Geffen School of Medicine at UCLA Director,
Assessment of Myocardial Viability Jamshid Maddahi, M.D., FACC, FASNC Professor Molecular and Medical Pharmacology (Nuclear Medicine) and Medicine (Cardiology) David Geffen School of Medicine at UCLA Director,
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
Welcome 17 Michigan TAVR Participating Hospitals!
 Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Imaging and heart failure
 Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
5 Important Things to Know About Heart Failure. Kia Afshar, MD
 5 Important Things to Know About Heart Failure Kia Afshar, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1) Understand
5 Important Things to Know About Heart Failure Kia Afshar, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1) Understand
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Blank DISCLOSURES 1/17/2017 COMPLEX VALVE CASES CHALLENGES IN EVALUATING AND MANAGING MULTIVALVULAR HEART DISEASE ECHO HAWAII 1/23/17 NONE
 Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
2/14/2018 CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION. Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1
 CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1 1 PRESENTATION 57 yo male with a past medical history of hypertension
CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1 1 PRESENTATION 57 yo male with a past medical history of hypertension
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: FORM NAME: H F A DATE: 10/01/2015 VERSION: D CONTACT YEAR NUMBER: FORM SEQUENCE NUMBER: General Instructions: The Heart Failure Hospital Record
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: FORM NAME: H F A DATE: 10/01/2015 VERSION: D CONTACT YEAR NUMBER: FORM SEQUENCE NUMBER: General Instructions: The Heart Failure Hospital Record
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream
 Going Mainstream") The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
Approach to the patient with Shortness of Breath
 Approach to the patient with Shortness of Breath Colin Edwards AUG 2015 Dyspnoea Basic concepts Definition: Dyspnoea is defined as abnormal or uncomfortable breathing in the context of what is normal for
Approach to the patient with Shortness of Breath Colin Edwards AUG 2015 Dyspnoea Basic concepts Definition: Dyspnoea is defined as abnormal or uncomfortable breathing in the context of what is normal for
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Cardiac Care Network of Ontario
 Cardiac Care Network of Ontario Cardiac Wait Times Patient Triage Business Rules December 2016 TABLE OF CONTENTS 1. Introduction... 3 1.1. Document Purpose... 3 1.2. Document Structure... 3 2. Algorithms...
Cardiac Care Network of Ontario Cardiac Wait Times Patient Triage Business Rules December 2016 TABLE OF CONTENTS 1. Introduction... 3 1.1. Document Purpose... 3 1.2. Document Structure... 3 2. Algorithms...
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle
 Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr..
 Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
QCVC Committees Scientific Activities Central Hall General Information FAC. SPECT tomography has the advantage of quantifying biventricular volumes.
 QCVC Committees Scientific Activities Central Hall General Information FAC Thematic Units Arrhythmias and Electrophysiology Basic Research Bioengineering and Medical Informatics Cardiac Surgical Intensive
QCVC Committees Scientific Activities Central Hall General Information FAC Thematic Units Arrhythmias and Electrophysiology Basic Research Bioengineering and Medical Informatics Cardiac Surgical Intensive
Valvular Heart Disease: Recognition and Management in the Outpatient Setting
 Valvular Heart Disease: Recognition and Management in the Outpatient Setting Ian S. Harris UCSF Division of Cardiology Case 1: 80 year old man with a history of hypertension, complaining of exertional
Valvular Heart Disease: Recognition and Management in the Outpatient Setting Ian S. Harris UCSF Division of Cardiology Case 1: 80 year old man with a history of hypertension, complaining of exertional
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Cardiology Cath Conference
 Cardiology Cath Conference David Stultz, MD Cardiology Fellow, PGY-6 February 14, 2006 Case #1 84 yo WM brought by squad this am for? syncope Pt reports Chest pain stuttering over several days. This am
Cardiology Cath Conference David Stultz, MD Cardiology Fellow, PGY-6 February 14, 2006 Case #1 84 yo WM brought by squad this am for? syncope Pt reports Chest pain stuttering over several days. This am
Clinical Summary. Live Cases I - IX
 Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Looking Outside the Box: Incidental Extracardiac Finding in Echo
 Looking Outside the Box: Incidental Extracardiac Finding in Echo Dr. Aijaz Shah Head of Division, Adult Echocardiography Laboratory Prince Sultan Cardiac Centre Riyadh Case 1 17 year old boy presented
Looking Outside the Box: Incidental Extracardiac Finding in Echo Dr. Aijaz Shah Head of Division, Adult Echocardiography Laboratory Prince Sultan Cardiac Centre Riyadh Case 1 17 year old boy presented
CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE
 CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE SSC Journée d Automne 25 novembre 2010 Dr. Charles Seydoux, spéc. FMH en médecine interne et en cardiologie, Lausanne Dr. Claudia Bösch, Oberärztin Herzinsuffizienz
CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE SSC Journée d Automne 25 novembre 2010 Dr. Charles Seydoux, spéc. FMH en médecine interne et en cardiologie, Lausanne Dr. Claudia Bösch, Oberärztin Herzinsuffizienz
Severe Aortic Stenosis in Elderly Patients: Surgical Versus Transcatheter Aortic Valve Replacement (TAVR)
") Severe Aortic Stenosis in Elderly Patients: Surgical Versus Transcatheter Aortic Valve Replacement (TAVR) James Dralle, MD Chief, Cardiothoracic Surgery AtlantiCare Regional Medical Center Transcatheter
Severe Aortic Stenosis in Elderly Patients: Surgical Versus Transcatheter Aortic Valve Replacement (TAVR) James Dralle, MD Chief, Cardiothoracic Surgery AtlantiCare Regional Medical Center Transcatheter
Beating outside the Box a case presentation on pericarditis. Kathryn R. Brim, DO, PGY1 Internal Medicine Resident
 Beating outside the Box a case presentation on pericarditis Kathryn R. Brim, DO, PGY1 Internal Medicine Resident Presentation Mr. P.A. is a 47 year old male who presented to the emergency department with
Beating outside the Box a case presentation on pericarditis Kathryn R. Brim, DO, PGY1 Internal Medicine Resident Presentation Mr. P.A. is a 47 year old male who presented to the emergency department with
1. LV function and remodeling. 2. Contribution of myocardial ischemia due to CAD, and
 1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Why guess when you could know? Gold Standard. Cardiac catheterization (Angiogram) Invasive Risks: Infection, hematoma, death
 Invasive Risks: Infection, hematoma, death") Why guess when you could know? Gold Standard Cardiac catheterization (Angiogram) Invasive Risks: Infection, hematoma, death PCI decisions Number of vessels involved Surgeon experience level The anatomic
Why guess when you could know? Gold Standard Cardiac catheterization (Angiogram) Invasive Risks: Infection, hematoma, death PCI decisions Number of vessels involved Surgeon experience level The anatomic
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Pearls & Pitfalls in nuclear cardiology
 Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Risk of Subsequent Pregnancy in Women with a History of Peripartum Cardiomyopathy Uri Elkayam, MD
 Risk of Subsequent Pregnancy in Women with a History of Peripartum Cardiomyopathy Uri Elkayam, MD Professor of Medicine / Cardiology Professor of Obstetrics and Gynecology University of Southern California
Risk of Subsequent Pregnancy in Women with a History of Peripartum Cardiomyopathy Uri Elkayam, MD Professor of Medicine / Cardiology Professor of Obstetrics and Gynecology University of Southern California
Highlights from EuroEcho 2009 Echo in cardiomyopathies
 Highlights from EuroEcho 2009 Echo in cardiomyopathies Bogdan A. Popescu University of Medicine and Pharmacy, Bucharest, Romania ESC Congress 2010 Hypertrophic cardiomyopathy To determine the differences
Highlights from EuroEcho 2009 Echo in cardiomyopathies Bogdan A. Popescu University of Medicine and Pharmacy, Bucharest, Romania ESC Congress 2010 Hypertrophic cardiomyopathy To determine the differences
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Case Summary. Workshop Overview. Mr. M
 9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
RADIATION HEART DISEASE: MANAGEMENT STRATEGIES
 RADIATION HEART DISEASE: MANAGEMENT STRATEGIES AMMAR CHAUDHARY MBChB, ABIM, FRCPC ASSOCIATE CONSULTANT CARDIOLOGIST KING FAISAL SPECIALIST HOSPITAL & RESEARCH CENTER - JEDDAH Scope of the Problem ~ 50
RADIATION HEART DISEASE: MANAGEMENT STRATEGIES AMMAR CHAUDHARY MBChB, ABIM, FRCPC ASSOCIATE CONSULTANT CARDIOLOGIST KING FAISAL SPECIALIST HOSPITAL & RESEARCH CENTER - JEDDAH Scope of the Problem ~ 50
What the Cardiologist needs to know from Medical Images
 What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia
 Transcatheter Transapical Aortic Valve Implantation Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia Ahmed Elwatidy, MD,PhD, FRCS S Kassab, MD,S Ahmari, MD, H Amri, MD, H Ismail, MD, A Calafiori,
Transcatheter Transapical Aortic Valve Implantation Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia Ahmed Elwatidy, MD,PhD, FRCS S Kassab, MD,S Ahmari, MD, H Amri, MD, H Ismail, MD, A Calafiori,
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
CARDIOLOGY GRAND ROUNDS
 CARDIOLOGY GRAND ROUNDS Presentation: Speakers: Percutaneous Repair of Paravalvular Prosthetic Regurgitation Paul Sorajja, MD Director of the Center for Valve and Structural Heart Disease Minneapolis Heart
CARDIOLOGY GRAND ROUNDS Presentation: Speakers: Percutaneous Repair of Paravalvular Prosthetic Regurgitation Paul Sorajja, MD Director of the Center for Valve and Structural Heart Disease Minneapolis Heart
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
TAVI complication. Possible aetiology and how to manage
 TAVI complication. Possible aetiology and how to manage Dr Sanjeevan Pasupati Waikato Hospital, Hamilton, New Zealand Operators: Dr Sanjeevan Pasupati, Mr Nand Kejriwal, Mr Adam Elgamel Valve Positioning
TAVI complication. Possible aetiology and how to manage Dr Sanjeevan Pasupati Waikato Hospital, Hamilton, New Zealand Operators: Dr Sanjeevan Pasupati, Mr Nand Kejriwal, Mr Adam Elgamel Valve Positioning
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Presenter Disclosure. Patrick O. Myers, M.D. No Relationships to Disclose
 Presenter Disclosure Patrick O. Myers, M.D. No Relationships to Disclose Aortic Valve Repair by Cusp Extension for Rheumatic Aortic Insufficiency in Children Long term Results and Impact of Extension Material
Presenter Disclosure Patrick O. Myers, M.D. No Relationships to Disclose Aortic Valve Repair by Cusp Extension for Rheumatic Aortic Insufficiency in Children Long term Results and Impact of Extension Material
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이
 Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
TAVR : Caring for your patients before and after TAVR
 TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional