CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock
|
|
|
- Mercy Price
- 5 years ago
- Views:
Transcription
1 CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Yoshiya Toyoda, MD, PhD William Maul Measey Professor of Surgery Chief, Cardiovascular Surgery Surgical Director, Mechanical Circulatory Support Surgical Director, Thoracic Transplantation Temple University School of Medicine Philadelphia, PA
2 Coronary Artery Disease (CAD) Cardiovascular disease (CVD) accounts for 34 % of all U.S. deaths each year, countless resources, and healthcare expenditures that approach $300 billion annually. Coronary artery disease (CAD) is the most common type of heart disease. It is the leading cause of death in the United States in both men and women. CAD resulting in myocardial infarction (MI) claims over one million lives each year in the U.S. and leads to countless more permanent disabilities including heart failure. Approximately five million Americans currently live with heart failure, and an additional 400,000 patients are newly diagnosed each year. CHF is the most common admitting diagnosis for patients over the age of 65 years, and is associated not only with a decreased quality of life, but also significant mortality. CHF carries a mortality rate of at least 40 % within 2 years of diagnosis. For those patients with the most advanced stages of CHF (New York Heart Association class IV), the 1-year mortality rate exceeds 50 %. In addition, the treatment of CHF is associated with very high and continuingly escalating costs. Not only is CHF the most expensive DRG covered by Medicare and Medicaid, remarkably it is estimated that total medical costs (inpatient and outpatient) associated with the treatment of CHF exceed $29 billion per year.
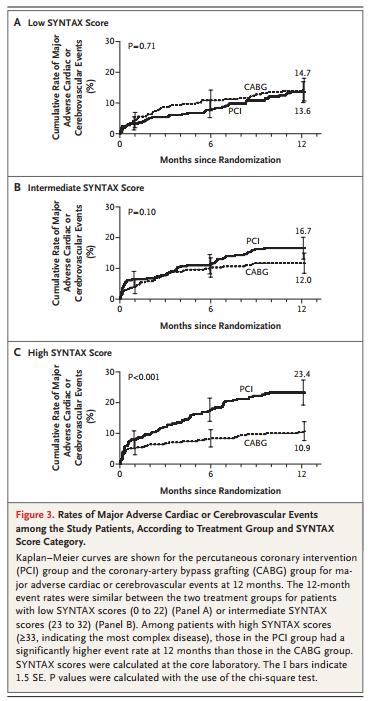
3 Coronary Artery Disease (CAD) CABG vs. PCI for Left Main or Three Vessel Disease Syntax (The SYNergy between percutaneous coronary intervention with TAXus and cardiac surgery study) 1-year Data. NEJM 2009;360: Randomly assigned 1800 patients with three-vessel or left main coronary artery disease to undergo CABG or PCI (in a 1:1 ratio). A noninferiority comparison of the two groups was performed for the primary end point a major adverse cardiac or cerebrovascular event (i.e., death from any cause, stroke, myocardial infarction, or repeat revascularization) during the 12-month period after randomization. Results Most of the preoperative characteristics were similar in the two groups. Rates of major adverse cardiac or cerebrovascular events at 12 months were significantly higher in the PCI group (17.8%, vs. 12.4% for CABG; P=0.002), in large part because of an increased rate of repeat revascularization (13.5% vs. 5.9%, PP<0.001) as a result, the criterion for noninferiority was not met. At 12 months, the rates of death and myocardial infarction were similar between the two groups; stroke was significantly more likely to occur with CABG (2.2%, vs. 0.6% with PCI; P=0.003). Conclusions CABG remains the standard of care for patients with three-vessel or left main coronary artery disease, since the use of CABG, as compared with PCI, resulted in lower rates of the combined end point of major adverse cardiac or cerebrovascular events at 1 year.

4 Syntax 1-year Data. NEJM 2009;360:

5 Syntax 1-year Data. NEJM 2009;360:
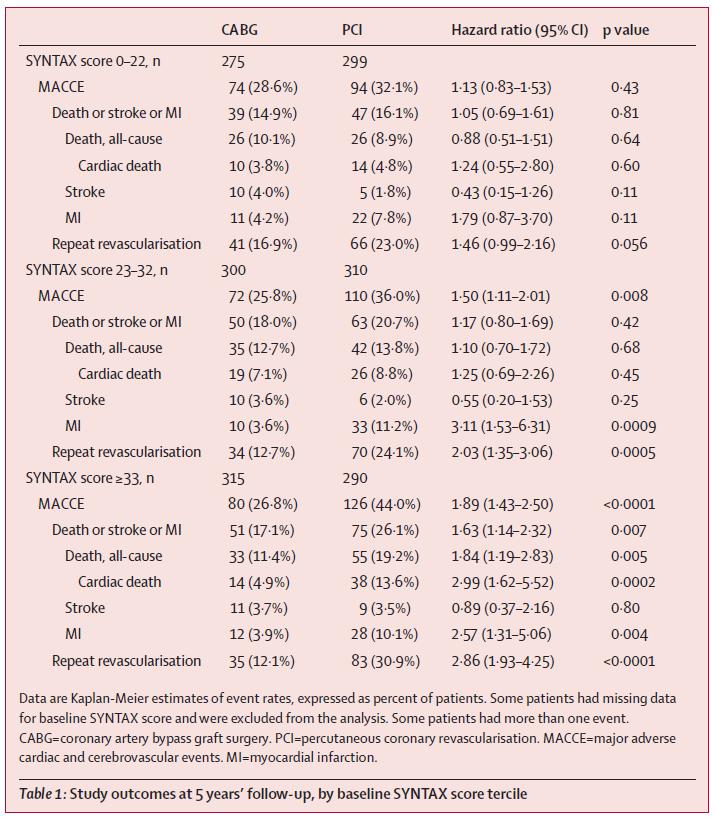
6 Syntax 5-year Data. Lancet, 381 (2013), pp patients were randomly assigned to CABG (n=897) or PCI (n=903). After 5 years follow-up, Kaplan-Meier estimates of MACCE were 26 9% in the CABG group and 37 3% in the PCI group (p<0 0001). Estimates of myocardial infarction (3 8% in the CABG group vs 9 7% in the PCI group; p<0 0001) and repeat revascularisation (13 7% vs 25 9%; p<0 0001) were significantly increased with PCI versus CABG. All-cause death (11 4% in the CABG group vs 13 9% in the PCI group; p=0 10) and stroke (3 7% vs 2 4%; p=0 09) were not significantly different between groups. 28 6% of patients in the CABG group with low SYNTAX scores had MACCE versus 32 1% of patients in the PCI group (p=0 43) and 31 0% in the CABG group with left main coronary disease had MACCE versus 36 9% in the PCI group (p=0 12); however, in patients with intermediate or high SYNTAX scores, MACCE was significantly increased with PCI (intermediate score, 25 8% of the CABG group vs 36 0% of the PCI group; p=0 008; high score, 26 8% vs 44 0%; p<0 0001). 3-year/5-year SYNTAX trial data in 2012 comparing PCI and CABG provides compelling insights into the statistically significant and overwhelming survival and event-free survival benefit conferred on patients who receive CABG surgery. At 5-year follow-up, clinical results from SYNTAX showed that CABG was superior to DES- PCI with respect to the composite endpoint of death, myocardial infarction, stroke, or repeat revascularization, with the benefit driven predominantly by decreased rates of repeat revascularization and myocardial infarction with no significant differences in rates of death or stroke.
7
8
9 CABG vs. Medical Therapy in Ischemic Cardiomyopathy The Coronary Artery Surgery Study (CASS) trial in 1985, showed that coronary artery bypass graft (CABG) improved survival in comparing 420 medically treated and 231 CABG patients with left ventricular ejection fraction (LVEF) 35% in the nonrandomized Registry cohort. The benefit was most apparent for patients with angina and LVEF 25%; medically treated patients in this cohort had a 43 % 5-year survival while CABG recipients benefited from a 63 % 5-year survival. Operative mortality in the CASS series was 6.9 %.
10 CABG in Ischemic Cardiomyopathy STITCH trial. NEJM 2016;374: CABG in ICMP (LVEF<35%) From July 2002 to May 2007, a total of 1212 patients with an ejection fraction of 35% or less and coronary artery disease amenable to CABG were randomly assigned to undergo CABG plus medical therapy (CABG group, 610 patients) or medical therapy alone (medical-therapy group, 602 patients). The primary outcome was death from any cause. Major secondary outcomes included death from cardiovascular causes and death from any cause or hospitalization for cardiovascular causes. The median duration of follow-up, including the current extended-follow-up study, was 9.8 years. RESULTS A primary outcome event occurred in 359 patients (58.9%) in the CABG group and in 398 patients (66.1%) in the medical-therapy group (hazard ratio with CABG vs. medical therapy, 0.84; 95% confidence interval [CI], 0.73 to 0.97; P=0.02 by log-rank test). A total of 247 patients (40.5%) in the CABG group and 297 patients (49.3%) in the medical-therapy group died from cardiovascular causes (hazard ratio, 0.79; 95% CI, 0.66 to 0.93; P=0.006 by log-rank test). Death from any cause or hospitalization for cardiovascular causes occurred in 467 patients (76.6%) in the CABG group and in 524 patients (87.0%) in the medical-therapy group (hazard ratio, 0.72; 95% CI, 0.64 to 0.82; P<0.001 by log-rank test). CONCLUSIONS In a cohort of patients with ischemic cardiomyopathy, the rates of death from any cause, death from cardiovascular causes, and death from any cause or hospitalization for cardiovascular causes were significantly lower over 10 years among patients who underwent CABG in addition to receiving medical therapy than among those who received medical therapy alone.

11 CABG in Ischemic Cardiomyopathy STITCH trial. NEJM 2016;374: CABG in ICMP (LVEF<35%)

12 STITCH trial. NEJM 2016;374: CABG in ICMP

13 Myocardial viability by MRI and survival. JACC 2012;59: Many believe that the selection of patients with ischemic cardiomyopathy for CABG should be based on the presence of viable myocardium. DE-CMR may be useful to predict, not only functional improvement of patients with CAD and LV dysfunction, but also survival. Indeed, the study showed that revascularization of dysfunctional viable myocardium provides a significant improvement in patient outcomes versus medical treatment. It thus suggests that patients with viable myocardium should be revascularized to improve survival.
14 Patients with viable myocardium and low LVEF (24+/- 7%): Complete Revascularization is better than incomplete revascularization or medical therapy.
15 Case. Cardiogenic Shock Complicating MI W.S., 55-year-old Male, 69 in, 222 lbs, BMI 32 Active Smoker (43 pack years) DM, HLD, PVD (SFA stent), COPD, OSA Shortness of Breath for 2 weeks NSTEMI (TnI 4.4), NYHA Class IV WBC 9.1, Hct 45, Plt 285 ABG: 7.46/21/81 BUN: 13, Cr 0.82, T-Bil 1.1, Alb 3.2, INR 1.0

16 Case. Cardiogenic Shock Complicating MI W.S., 55M, NSTEMI, Shortness of Breath for 2 weeks LVEF: 10-15% LVID ed: 68mm LVID es: 63mm MV: mild MR RV: TV: Dilated Decreased function no TR

17

18
19

20
21
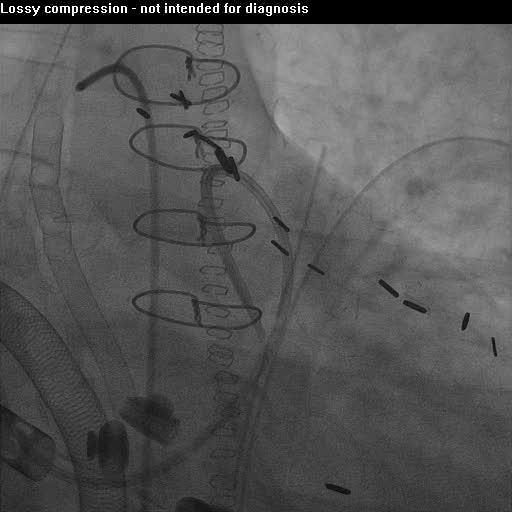
22 Case. Cardiogenic Shock Complicating MI W.S., 55M, LM+3VD, NSTEMI, NYHA Class IV HR: 114 AoP: 92/75 (83) LVP: 98/36 RAP: 17/12(14) RVP: 50/18 PAP: 51/34(41) PCWP: 39/37(34) SaO2: 94 SvO2: 57 CO (Fick): 4.05 CI (Fick): 1.85 LVSWI: RVSWI: 6.08 PVR: 1.73
 LM+3VD, Non STEMI, NYHA IV VFib Cardioversion x 2")
23 Case. Cardiac Arrest Complicating MI W.S., 55-year-old Male Ischemic Cardiomyopathy (LVEF 10-15%) LM+3VD, Non STEMI, NYHA IV VFib Cardioversion x 2 IABP Insertion VFib Cardioversion x 8 Intubation, CPR Next Step??
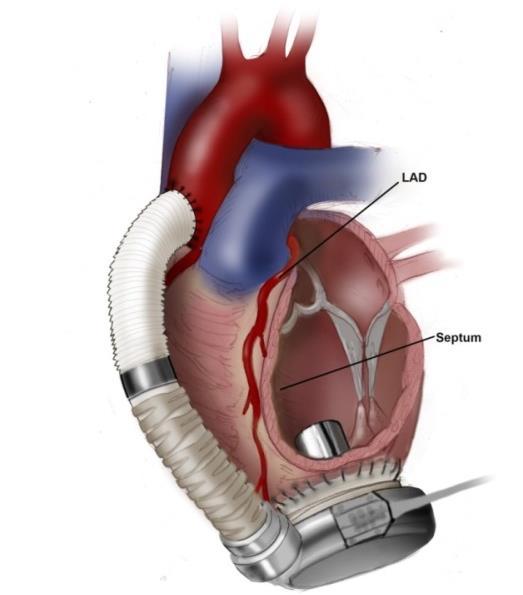
24 Case. Cardiogenic Shock Complicating MI W.S., 55-year-old Male Ischemic Cardiomyopathy (LVEF 10-15%) LM+3VD, Non STEMI, NYHA IV, Cardiac Arrest Emergency Off-Pump CABG x 6 LIMA-LAD SVG-Diag1-Diag2 SVG-RI-OM-PDA
 LM+3VD, Non STEMI,")

25 Case. Cardiac Arrest Complicating MI W.S., 55-year-old Male Ischemic Cardiomyopathy (LVEF 10-15%) LM+3VD, Non STEMI, NYHA IV, Cardiac Arrest S/P OPCAB x 6 POD#0: Hemodynamically Stable POD#1: VFib Cardioversion x 3 Centrimag LVAD, Off Pump 31Fr. venous cannula in left atrium 20Fr. arterial cannula in aorta

26


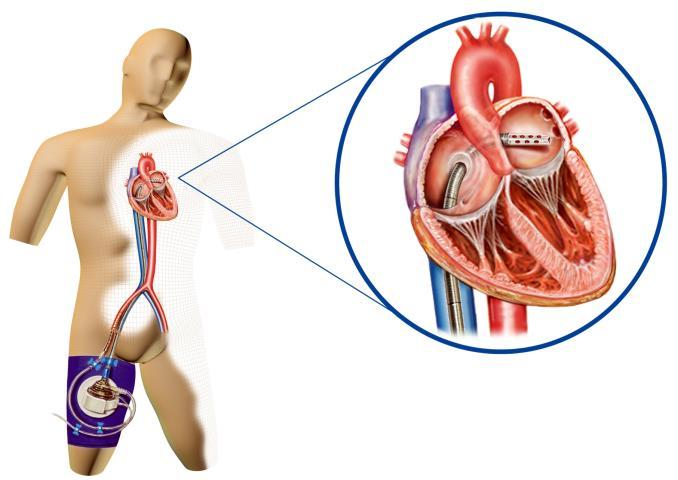


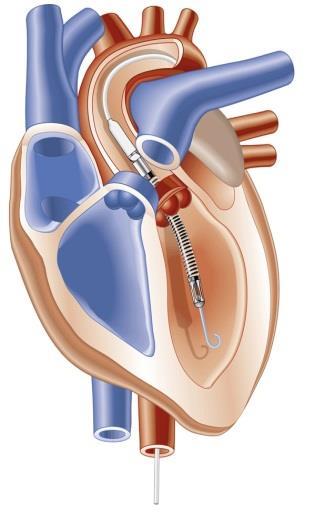

27 Short-Term Mechanical Circulatory Support CentriMag Rotaflow Impella Biomedicus TandemHeart







28 Long-Term Mechanical Circulatory Support HeartMate II HeartMate 3 HeartWare HVAD Syncardia TAH


29 Case. 55 M, acute on chronic heart failure, ischemic cardiomyopathy, NSTEMI VFib x 2 IABP Insertion VFib x 8, Intubation, CPR Emergency CABG with VAD back up OPCAB x 6 POD#0 Hemodynamically stable POD#1 Vfib x 3 Centrimag LVAD POD#2: VFib x 2 POD#3: VFib x 26
30

31

32
33

34
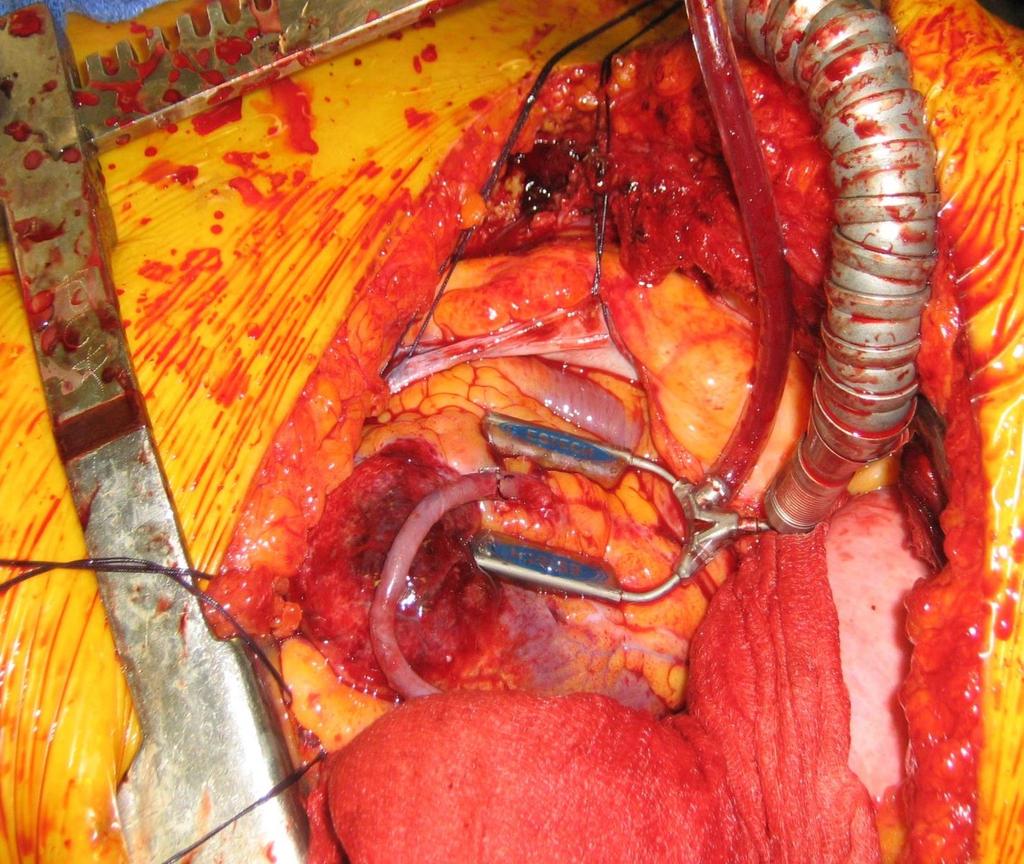
35 Case. Cardiac Arrest Complicating MI W.S., 55-year-old Male Ischemic Cardiomyopathy (LVEF 10-15%) LM+3VD, Non STEMI, NYHA IV, Cardiac Arrest S/P OPCAB x 6 POD#1: VFib Cardioversion x 3 Centrimag LVAD POD#2-3: VFib Cardioversion x 28 All grafts patent Centrimag RVAD, Off Pump 40Fr. venous in right atrium 20Fr. arterial in pulmonary artery
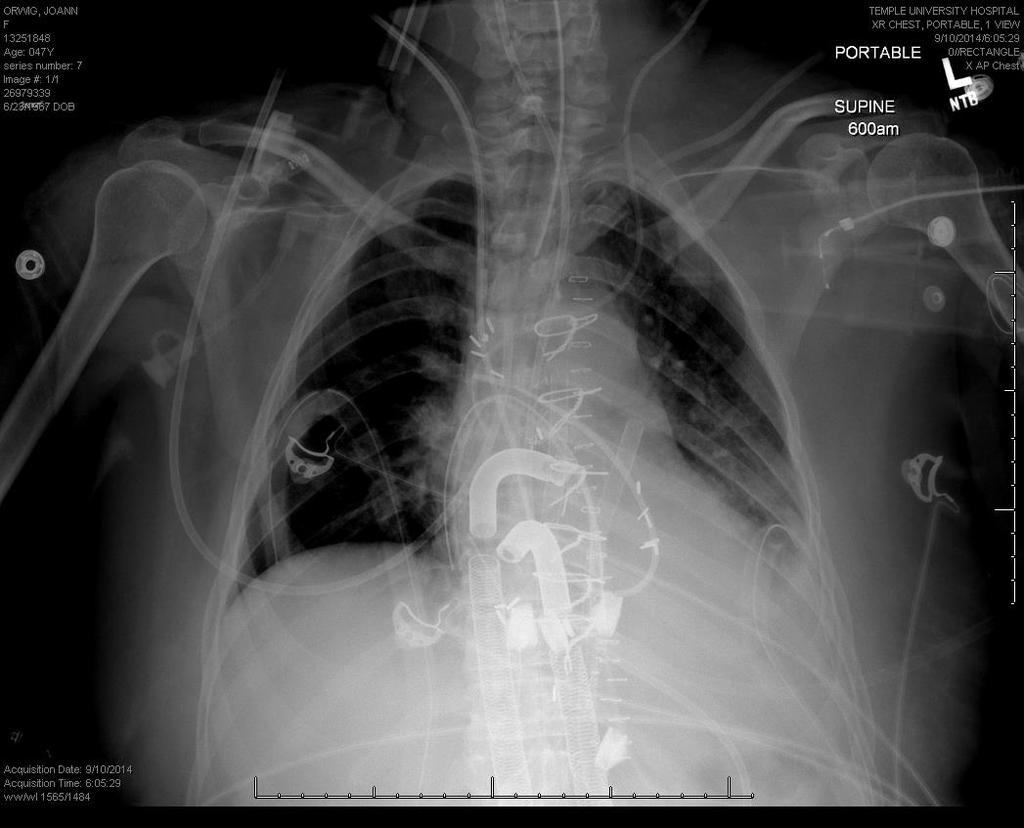
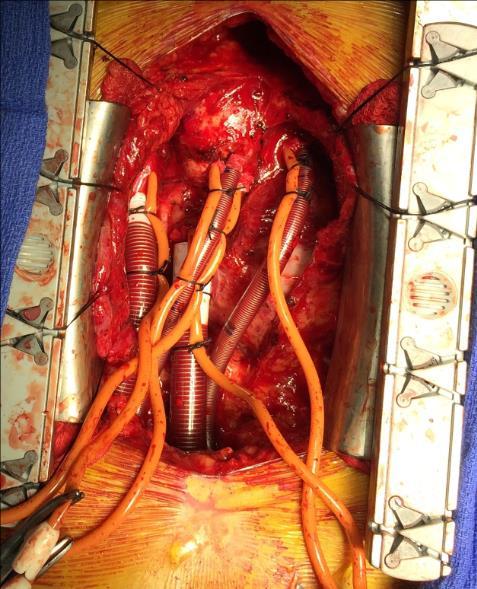
36 Bi-Ventricular Assist Device with Central Cannulation


37 Securing the cannula for ambulation

38 Ambulation on CentriMag BiVAD POD#1: Centrimag LVAD: 6.5 L/min POD#3: Centrimag RVAD: 5.5 L/min POD#4~11: Vfib Cardioversion x 29
39 W.S., 55M, Ischemic Cardiomyopathy Preop.: VFib Cardioversion x 10 OPCAB x 6 POD#1: VFib Cardioversion x 3 Centrimag LVAD POD#2-3:VFib Cardioversion x 28 Centrimag RVAD POD#4-11: VFib Cardioversion x 29 POD#12 POD#28 Centrimag LVAD: 6.5L/min 2.4L/min Centrimag RVAD: 5.5L/min 1.5L/min
40 W.S., 55M, s/p OPCAB x 6, Centrimag BiVAD POD#38: BiVAD Explantation HR 93 BP 95/57(71) RAP 13 PAP 38/21(25) PCWP 16 CO/CI 9.5/4.3 SvO2 87 POD#58: Discharged Home

41 CentriMag BiVAD, Bridge-to-Recovery for Ischemic Cardiomyopathy, Cardiogenic Shock/Cardiac Arrest, s/p OPCAB x 6, Doing well 5 years postop
42 Acute on chronic heart failure, ischemic cardiomyopathy, NSTEMI Cardiogenic Shock, Vfib, IABP Complete Revascularization, OPCAB x 6 Postcardiotomy Vfib VAD as Bridge-to-Recovery Recovery, Centrimag Explant


, cardiogenic")


43 Case. 72 M, acute on chronic heart failure, ischemic cardiomyopathy, NSTEMI Diffuse CAD (3VD), cardiogenic shock placed on Impella LVAD LVEF 10-15%, LVDd 66mm LVDs 58mm despite on Impella CP

 Explant of")

44 Case. 72 M, ischemic cardiomyopathy, cardiogenic shock on Impella s/p Off Pump CABG x 6 (LIMA-Diag-LAD, SVG-RI-OM, SVG-PDA-PLA) Explant of Impella. Discharged home on POD#16. SVG-RI-OM All grafts patent LIMA-Diag-LAD SVG-PDA-PLA


45 Case. 61F, Cardiogenic shock following STEMI, Severe PAD, Smoker Diffuse CAD (Left main + 3VD), STEMI, cardiogenic shock placed on IABP LVEF 15-20%, Emergency OPCAB x 3 (LIMA-LAD, SVG-RCA-OM)

 Persistent low")

46 Case. 61F, Cardiogenic shock following STEMI S/P Emergency CABG x 3 (LIMA-LAD, SVG-RCA-OM) Persistent low cardiac output, Ventricular tachcardia/fibrillation POD# 6: All grafts patent
 POD# 6: HeartMate II LVAD Implantation POD# 43:")
47 Case. 61F, Cardiogenic shock following STEMI S/P Emergency CABG x 3 (LIMA-LAD, SVG-RCA-OM) POD# 6: HeartMate II LVAD Implantation POD# 43: Discharge home
 POD#6 from OPCAB: s/p")

48 Case. 61F, Cardiogenic shock following STEMI S/P Emergency CABG x 3 (LIMA-LAD, SVG-RCA-OM) POD#6 from OPCAB: s/p HeartMate II LVAD POD#85 from HeartMate II LVAD: HeartMate II LVAD Explant 5 Years postop. NYHA Class I, LVEF 45%, improved from 15-20%


49 At least one in three heart surgeons has refused to treat critically ill patients because they are worried it will affect their mortality ratings if things go wrong. 84 percent said they were aware of other surgeons doing the same. Clinical decision-making had been adversely affected by the culture of transparency.
 Through Median")
50 Off Pump Double Lung Tx OPCAB x 1 (LIMA-LAD) Through Median Sternotomy


51 Single Left Lung Tx + OPCAB x 2 (SVG-Ramus-LAD) for IPF + CAD + Radiation Chest



52 Recipient: 63M, 71in, 207lbs, IPF, CAD Donor: 44M, 71in, 181lbs Single Left Lung Tx, Off-Pump OPCAB x 1 (LIMA-LAD) Ischemic Time: 172 minutes Hospital Stay: 11 days
53 Lung Transplantation at Temple N=240, Concomitant CABG + Lung Transplant (N=17, 7%) CABG: bypass grafts 1-3 Survival rate: 100% during the first year
54 Isolated CABG (YT: n=466) at Temple from to Complete Revascularization CABG x 4 8 (n=310, 67%) x 1 x 2 x 3 x 4 x 5 x 6 x 7 x 8
55 Isolated CABG (YT: n=466) at Temple from to Off Pump vs. On Pump 50, 11% 416, 89% Off Pump On Pump
56 Isolated CABG (n=382) at Temple from to Demographics CABG (Off- Pump) (n=180) CABG (On- Pump) (n=202) P-value Age 63 ± 9 62 ± Gender (male) 66% 70% Height (inches) 66 ± 7 67 ± Weight (lbs) 192 ± ± BMI (kg/m 2 ) 31 ± 7 30 ± Smokers 65% 23% Hypertension 80% 86% Diabetes 54% 51% 0.331
57 Isolated CABG (n=382) at Temple from to CABG (Off- Pump) (n=180) CABG (On- Pump) (n=202) P-value Race 34%- AA 27%- W 49%- O 24%- AA 27%- W 40%- O Previous MI 21% 33% Previous CVA 13% 12% Pre-EF (%) 44 ± 18 (5-70%) 48 ± 16 (10-70%) 0.982
58 Isolated CABG (n=382) at Temple from to CABG (Off- Pump) (n=180) CABG (On- Pump) (n=202) P-value Emergency/ Urgent Grafts (average) Bypass grafts# (ranges) Observed/Expect ed Mortality Index Cerebrovascular Events (stroke) 56% 35% ± ± to 8 1 to
59 CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Off Pump vs. On Pump Avoid global ischemia to already damaged myocardium Use shunt to minimize regional ischemia On pump, beating heart without global ischemia: when hemodynamically unstable, severe cardiomegaly Proximal anastomosis first to measure the exact length of free grafts Proximal anastomoses with HeartString to avoid side biting clamp for hostile aorta Sequential anastomoses with respect to the target anatomy More targets possible
60 CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Cardiogenic Shock Mechanical circulatory support to achieve optimum hemodynamics: Bridge-to-Decision Peripheral: IABP, Impella (LVAD, RVAD), TandemHeart (LVAD, RVAD), Veno- Arterial ECMO Central: Veno-Arterial ECMO, LVAD, RVAD, BiVAD Bridge-to-PCI, Support for high risk PCI Bridge-to-CABG Bridge-to-Long Term VAD: no viability, poor targets, poor run off, good social support
61 CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Complete revascularization Use of mechanical circulatory support Off Pump vs. On Pump
Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease
 Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Management of High-Risk CAD : Surgeons Perspective
 Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome
 Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Mechanical Cardiac Support in Acute Heart Failure. Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research
 Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Heart-lung transplantation: adult indications and outcomes
 Brief Report Heart-lung transplantation: adult indications and outcomes Yoshiya Toyoda, Yasuhiro Toyoda 2 Temple University, USA; 2 University of Pittsburgh, USA Correspondence to: Yoshiya Toyoda, MD,
Brief Report Heart-lung transplantation: adult indications and outcomes Yoshiya Toyoda, Yasuhiro Toyoda 2 Temple University, USA; 2 University of Pittsburgh, USA Correspondence to: Yoshiya Toyoda, MD,
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
EACTS Adult Cardiac Database
 EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium
 FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
Declaration of conflict of interest NONE
 Declaration of conflict of interest NONE Claudio Muneretto MD, PhD Director of Division of Cardiac Surgery University of Brescia Medical School Italy Hybrid Chymera Different features and potential advantages
Declaration of conflict of interest NONE Claudio Muneretto MD, PhD Director of Division of Cardiac Surgery University of Brescia Medical School Italy Hybrid Chymera Different features and potential advantages
Revascularization Strategies in Patients with Severe LV Dysfunction
 Revascularization Strategies in Patients with Severe LV Dysfunction Richard Lee, M.D., M.B.A. Saint Louis University The Center for Comprehensive Cardiovascular Care C4 Severe LV Dysfunction Defined as
Revascularization Strategies in Patients with Severe LV Dysfunction Richard Lee, M.D., M.B.A. Saint Louis University The Center for Comprehensive Cardiovascular Care C4 Severe LV Dysfunction Defined as
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Right Ventricular Failure: Prediction, Prevention and Treatment
 Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability
 Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Who is the high risk patient?
 Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention
 Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Update on Mechanical Circulatory Support. AATS May 5, 2010 Toronto, ON Canada
 Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011
 Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR
 PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
เอกราช อร ยะช ยพาณ ชย
 30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
Acute Mechanical Circulatory Support Right Ventricular Support Devices
 Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Case - Advanced HF and Shock (INTERMACS 1)
") Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA. IMP v4
 1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
3/1/2017. Heart Failure is a major driver of morbidity and mortality in the US 1-7
 Approaches to Cardiogenic Shock Margarita Camacho MD, FACS Surgical Director Cardiac Transplant and Mechanical Assist Device Program RWJ/Barnabas Health Heart Centers at Newark Beth Israel Medical Center
Approaches to Cardiogenic Shock Margarita Camacho MD, FACS Surgical Director Cardiac Transplant and Mechanical Assist Device Program RWJ/Barnabas Health Heart Centers at Newark Beth Israel Medical Center
Case Presentation #1
 Case Presentation #1 SCAI Fellows Course December 7, 2013 Barry F Uretsky, MD University of Arkansas for Medical Sciences Central Arkansas Veterans Health System Little Rock, AR Case Presentation #1 65
Case Presentation #1 SCAI Fellows Course December 7, 2013 Barry F Uretsky, MD University of Arkansas for Medical Sciences Central Arkansas Veterans Health System Little Rock, AR Case Presentation #1 65
Ted Feldman, M.D., MSCAI FACC FESC
 Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
PCI vs. CABG From BARI to Syntax, Is The Game Over?
 PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
The SYNTAX-LE MANS Study
 The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
Surgical Options for Advanced Heart Failure
 Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
Left Ventricular Assist Devices (LVADs): Overview and Future Directions
: Overview and Future Directions") Left Ventricular Assist Devices (LVADs): Overview and Future Directions FATIMA KARAKI, M.D. PGY-3, DEPARTMENT OF MEDICINE WASHINGTON UNIVERSITY IN ST. LOUIS ST. LOUIS, MISSOURI, USA St. Louis, Missouri,
Left Ventricular Assist Devices (LVADs): Overview and Future Directions FATIMA KARAKI, M.D. PGY-3, DEPARTMENT OF MEDICINE WASHINGTON UNIVERSITY IN ST. LOUIS ST. LOUIS, MISSOURI, USA St. Louis, Missouri,
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management
 Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Importance of the third arterial graft in multiple arterial grafting strategies
 Research Highlight Importance of the third arterial graft in multiple arterial grafting strategies David Glineur Department of Cardiovascular Surgery, Cliniques St Luc, Bouge and the Department of Cardiovascular
Research Highlight Importance of the third arterial graft in multiple arterial grafting strategies David Glineur Department of Cardiovascular Surgery, Cliniques St Luc, Bouge and the Department of Cardiovascular
Echo assessment of patients with an ECMO device
 Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
HREVS: A Randomized Trial of PCI vs CABG vs Hybrid Revascularization in Patients With Coronary Artery Disease. Vladimir Ganyukov, MD, PhD
 HREVS: A Randomized Trial of PCI vs CABG vs Hybrid Revascularization in Patients With Coronary Artery Disease Vladimir Ganyukov, MD, PhD Nikita Kochergin MD, Aleksandr Shilov MD, PhD, Roman Tarasov, MD,
HREVS: A Randomized Trial of PCI vs CABG vs Hybrid Revascularization in Patients With Coronary Artery Disease Vladimir Ganyukov, MD, PhD Nikita Kochergin MD, Aleksandr Shilov MD, PhD, Roman Tarasov, MD,
Overview of MCS in Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation
 Overview of MCS in 2017 Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation Technology Embracing Progress Technology Adoption Internet Adoption of Technology Pioneer in the
Overview of MCS in 2017 Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation Technology Embracing Progress Technology Adoption Internet Adoption of Technology Pioneer in the
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium. Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute
 Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France
 Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France Background on LM stenosis 5% of patients undergoing angiography Of the myocardium 80% Bifurcation
Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France Background on LM stenosis 5% of patients undergoing angiography Of the myocardium 80% Bifurcation
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Recovering Hearts. Saving Lives.
 Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Supplementary Online Content
 Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical Hospital Center Zagreb University of Zagreb School of Medicine Zagreb, CROATIA
 3rd Dubrovnik Cardiology Highlights An ESC Update Programme in Cardiology 26.09.-29.09.2013, Hotel Excelsior, Dubrovnik, Croatia Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical
3rd Dubrovnik Cardiology Highlights An ESC Update Programme in Cardiology 26.09.-29.09.2013, Hotel Excelsior, Dubrovnik, Croatia Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical
Counterpulsation. John N. Nanas, MD, PhD. Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece
 John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
STEMI ST Elevation Myocardial Infarction
 STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
High Risk PCI for Heart Failure
 High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
The MAIN-COMPARE Study
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Coronary Interventions Indications, Treatment Options and Outcomes
 Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017
 EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
PROMUS Element Experience In AMC
 Promus Element Luncheon Symposium: PROMUS Element Experience In AMC Jung-Min Ahn, MD. University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea PROMUS Element Clinical
Promus Element Luncheon Symposium: PROMUS Element Experience In AMC Jung-Min Ahn, MD. University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea PROMUS Element Clinical
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA
 CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
Cardiac surgery - CAD
 Cardiac surgery - CAD University of Pecs, Medical Faculty Heart Institute http://aok.pte.hu/en/egyseg/dokumentumok/290 Treatment strategies for CAD medical nitrate, anti-tct, (lysis), beta-blocker... interventional
Cardiac surgery - CAD University of Pecs, Medical Faculty Heart Institute http://aok.pte.hu/en/egyseg/dokumentumok/290 Treatment strategies for CAD medical nitrate, anti-tct, (lysis), beta-blocker... interventional
Surgical Options for Temporary MCS
 Surgical Options for Temporary MCS Michael A. Acker, MD Julian Johnson Professor of Surgery Chief of Cardiovascular Surgery Director of Heart and Vascular Center University of Pennsylvania Health System
Surgical Options for Temporary MCS Michael A. Acker, MD Julian Johnson Professor of Surgery Chief of Cardiovascular Surgery Director of Heart and Vascular Center University of Pennsylvania Health System
Alex versus Xience Registry Preliminary report
 Interventional Cardiology Network Alex versus Xience Preliminary report Mariusz Gąsior 1,2, Marek Gierlotka 1, Lech Poloński 1,2 1 3rd Department of Cardiology, Medical University of Silesia Centre tor
Interventional Cardiology Network Alex versus Xience Preliminary report Mariusz Gąsior 1,2, Marek Gierlotka 1, Lech Poloński 1,2 1 3rd Department of Cardiology, Medical University of Silesia Centre tor
Implantable Ventricular Assist Devices and Total Artificial Hearts
 Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
The MAIN-COMPARE Registry
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Advances in Advanced Heart Failure Therapies. Disclosures. Management Algorithm for Patients in Cardiogenic Shock
 Advances in Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center May 20, 2013 Joseph G. Rogers, M.D. Associate Professor
Advances in Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center May 20, 2013 Joseph G. Rogers, M.D. Associate Professor
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
Management of High-Risk Coronary Artery Disease
 Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD
 A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support
 Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced
Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced
The Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery: The SYNTAX Study
 The Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery: The SYNTAX Study Five-Year Results in the French Subset René Koning, MD On behalf of the SYNTAX investigators Three-year
The Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery: The SYNTAX Study Five-Year Results in the French Subset René Koning, MD On behalf of the SYNTAX investigators Three-year
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial
 Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial Myeong-Ki Hong, MD. PhD on behalf of the IVUS-XPL trial investigators
Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial Myeong-Ki Hong, MD. PhD on behalf of the IVUS-XPL trial investigators
CORONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
ECMO as a bridge to durable LVAD therapy. Jonathan Haft, MD Department of Cardiac Surgery University of Michigan
 ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ
 Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
The Case for Multivessel Revascularization in Shock
 The Case for Multivessel Revascularization in Shock Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 9.37 9.49 am Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
The Case for Multivessel Revascularization in Shock Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 9.37 9.49 am Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
Andrew Civitello MD, FACC
 Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Name of Policy: Ventricular Assist Devices and Total Artificial Hearts
 Name of Policy: Ventricular Assist Devices and Total Artificial Hearts Policy #: 033 Latest Review Date: February 2014 Category: Surgery Policy Grade: A Background/Definitions: As a general rule, benefits
Name of Policy: Ventricular Assist Devices and Total Artificial Hearts Policy #: 033 Latest Review Date: February 2014 Category: Surgery Policy Grade: A Background/Definitions: As a general rule, benefits