3/1/2017. Heart Failure is a major driver of morbidity and mortality in the US 1-7
|
|
|
- Amice Robbins
- 5 years ago
- Views:
Transcription
1 Approaches to Cardiogenic Shock Margarita Camacho MD, FACS Surgical Director Cardiac Transplant and Mechanical Assist Device Program RWJ/Barnabas Health Heart Centers at Newark Beth Israel Medical Center Newark, NJ Disclosures Sunshine Heart, Inc. Consultant Heart Failure is a major driver of morbidity and mortality in the US 1-7 Heart failure is a growing issue in the US ~6.0 million adults (2.8%) in the US have heart failure 670,000 new cases each year #1 reason for hospitalization in people >65 After 4 hospitalizations, median survival is <6 months 1. JACC HF. 2013;1: Rose EA, et al. Long-term mechanical left ventricular assistance for end-stage heart failure. N Engl J Med. Nov. 2001;5;345(20): Rogers, Butler, Lansman, et al. J Am Coll Cardiol. 2007;50: Hershberger, Nauman, Walker, et al. J Card Fail. 2003;22: Gorodeski, Chu, Reese, et al. Circ Heart Fail. 2009;2: Data on file. Pleasanton, Calif: Thoratec Corp. More costly than all forms of cancer combined 1
 in the United States, with projected left ventricular assist device (LVAD) candidates. U.S. population estimate is derived from U.")
2 Transplants are considered the gold standard, but the supply of donor hearts is limited 1 Proposing heart transplantation to cure heart failure is analogous to proposing the lottery to cure poverty. LW Stevenson Current estimates of adult patients with advanced heart failure (HF) in the United States, with projected left ventricular assist device (LVAD) candidates. U.S. population estimate is derived from U.S. Census data. Estimate of HF prevalence is derived from latest American Heart Association (AHA) statistics. 2. UNOS Website: 3. O Connell. Advanced Heart Failure Therapies Forum, Atlanta Indications for Acute Support Bridge to Recovery/Decision (mostly salvage cases) Cardiogenic shock due to refractory heart failure Bridge to Transplant (BTT) Bridge to Durable Device ECMO Veno-venous (VV) pre-/post lung transplant, ARDS Veno-arterial (VA) prolonged shock, post-cardiotomy Post-cardiotomy failure Bridge to Recovery/Decision Bridge to Recovery Bridge to Another Device Bridge to Transplant Withdrawal of Support 2
3 Timing earlier referral is best Identify candidates who will benefit from MCS Avoid end-organ damage Improve quality of life More rapid post-operative recovery if referred before co-morbidities begin to appear, i.e. renal dysfunction If referred earlier, they can be kept on the radar and receive timely intervention, rather than no intervention due to too late referral Avoid patients who are too sick to benefit Types of Assist Devices Short term support Percutaneous (Impella, Tandem Heart) Surgical (CentriMag, Impella LD and 5.0) ECMO (V-V / V-A) Why not implant long term VAD support in cardiogenic shock? Unclear neurologic status Respiratory failure Acute renal and liver dysfunction Antithrombotic burden (antiplatelets, IIb/IIIa inhibitors) Uncertain potential for cardiac recovery Unknown psycho-social status 3

4 Reasonable Evidence to Justify Short Term MCS Patients in refractory cardiogenic shock with relative contraindications for permanent VAD can be: 1. Supported safely with temporary MCS devices. 2. Be bridged to a permanent VAD once contraindications for permanent VAD no longer exist. 3. Suitability for bridge to transplant ascertained while on initial temporary support. Short term devices provide an opportunity to act first and ask later Cardiogenic shock MCS network Spoke Hospital Hospitals in area contacted to establish open channel of communication Spoke Hospital Hub Spoke Hospital Consider early transfer to hub facility (transplant/vad) Potential for spoke centers Spoke Less than 250 miles to gain experience with Hospital implant Implant and transfer model 4



5 ABIOMED AB5000 System Bi-ventricular support (Both sides of heart) Off-pump, easy cannula all Heart Centers No Coring of the heart, lower bleeding vs. BTT VADs CENTRIMAG MAGLEV PUMP Elimination of seals and bearings Elimination of friction and heat generation in the blood path reducing the risk for thrombus formation and hemolysis Uniform washing of the rotor surface minimizes areas of blood stagnation and turbulence in the pump 5





6 CentriMag System Components Pump Motor Console CENTRIMAG PUMP CENTRIMAG PUMP & MOTOR 6





7 Bearingless Pump & Motor No bearing and seals Disposable pump head 31 cc priming volume Max. pump speed: 5500 RPM Max. flow: 9.9 LM Rotor has magnetic core ECMO CIRCUIT Venous cannula Oxygenator CentriMag pump Arterial cannula Flow probe Percutaneous Cannulation (for ECMO) Generally Femoral vein to Femoral artery In adults Fr venous drainage cannula and Fr arterial return cannula 7


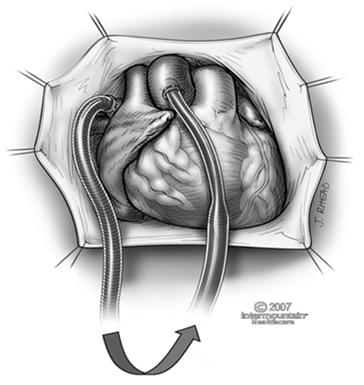
8 Left Heart Cannulation LA Ao IHC




9 Bilateral Support LA Ao PA RA IHC 2005 SURGICAL CANNULATION 9

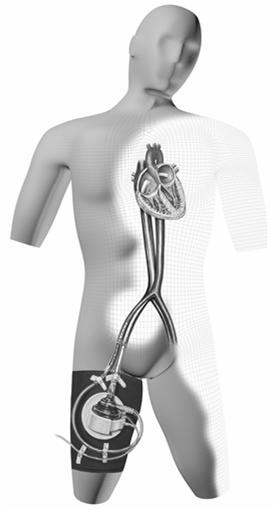

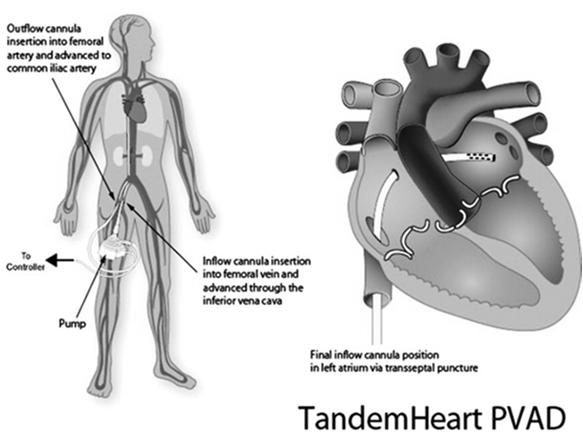
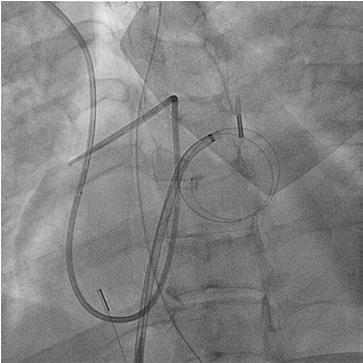
10 Tandem Heart 10


11 Tandem Extremity Protection 11

12 Tandem Heart Texas Heart Experience 117 patients with severe refractory cardiogenic shock 58 patients (48%) were undergoing active CPR at time of insertion 80 patients with ischemic and 37 patients with nonischemic cardiomyopathy 60% 30-day survival and 55% 6-month survival Tandem Heart Texas Heart Experience Cardiac index increased from 0.5 to 3.0 SBP increased from 75 to 100 Mixed venous O2 saturation increased from 49% to 69% Urine output increased from 70 cc/day to 1,200 cc/day Kar B, Gregoric I, Basra SS, et. Al. Percutaneous Ventricuar Assist Device In Severe Refractory Cardiogenic Shock;JACC 57(6):688-96, 2011 Abiomed Impella


13 Impella is the only percutaneous heart pump proven safe and effective for hemodynamic stabilization to enable Heart Recovery. Indications now include Protected PCI and Cardiogenic Shock in the setting of AMI and Postcardiotomy. Heart Recovery is an improvement in heart muscle function that enables a patient to sustain quality of life at home with their native heart 13



14 HCS-PMA-PP rc 3/1/2017 FDA Indication The Impella 2.5, Impella CP, Impella 5.0 and Impella LD catheters, in conjunction with the Automated Impella Controller console, are intended for short-term use (<4 days for the Impella 2.5 and Impella CP and <6 days for the Impella 5.0 and Impella LD) and indicated for the treatment of ongoing cardiogenic shock that occurs immediately (<48 hours) following acute myocardial infarction (AMI) or open heart surgery as a result of isolated left ventricular failure that is not responsive to optimal medical management and conventional treatment measures with or without an intraaortic balloon pump. The intent of the Impella system therapy is to reduce ventricular work and to provide the circulatory support necessary to allow heart recovery and early assessment of residual myocardial function. * Optimal medical management and conventional treatment measures include volume loading and use of pressors and inotropes, with or without IABP Data Supporting FDA Indications Scientific Evidence Total # of Patients # of Impella Patients Cardiogenic Shock Protected PCI Recover I FDA Study ISAR Shock RCT U.S. Impella Registry Literature review 2, Total 2,981 1,123 Protect I FDA Study Protect II FDA Study U.S. Impella Registry 1, Literature review 2, Total 4,331 1,638 24,000 Patients from FDA medical device reporting (MDR) database Hemodynamic Stabilization with Impella Unloads Left Ventricle & Coronary Perfusion End Organ Perfusion Right Side Support Escalation & Ambulation Right Side Impella RP Left Side Impella 2.5/CP/5.0 Seyfarth et al., JACC, 2008 Remmelink M et al., Cath Card Interv Lam K. et al,. Clin Res Cardiol, 2009 Casassus et a., JOIC, 2015 Anderson MB. et al., J Ht Lg Transplant Lima B. et al., Am J Cardiol


15 Incidence of Cardiogenic Shock Growing Cardiogenic Shock in STEMI Increasing 1 STEMI Cardiogenic Shock in Medicare Age Increasing 2 56,508 36,969 53% Dhaval Kolte et al. J Am Heart Assoc 2014 NATIONWIDE INPATIENT SAMPLE 2. Centers for Medicare and Medicaid database, MEDPAR FY14 Age >65 only, excludes non-medicare population Cardiogenic Shock Remains Leading Cause of Mortality in Acute Myocardial Infarction Death Rate, % High In-Hospital Mortality During AMI Cardiogenic Shock N = 23,696 and Ongoing Hazard Post Discharge % after AMI Cardiogenic Shock 2 Mortality % Post Discharge N = 112, Jeger, et al. Ann Intern Med Shah, et al. JACC 2016 NCDR Registry Mortality in PCI with Cardiogenic Shock Remains a Clinical Challenge In-Hospital Mortality AMI Cardiogenic Shock with PCI 1 28% N = 32,598 11% 31% p< AMI Cardiogenic Shock with PCI only; Overall mortality >50% Wayangankar, et al. JACC Int 2016 CATH-PCI Registry 15
 Medical Therapy (n=21) IABP (n=301) Medical Therapy (n=299) 41.3% 39.")
, Level of Evidence A, ESC STEMI Guidelines 2014 1-")

")
16 IABP in AMI Cardiogenic Shock: No Hemodynamic or Survival Benefit IABP SHOCK I Randomized Controlled Trial 1 N = 40 IABP-SHOCK II Randomized Controlled Trial 2 N = 600 IABP (n=19) Medical Therapy (n=21) IABP (n=301) Medical Therapy (n=299) 41.3% 39.7% CPO = MAP x Cardiac Output x log-rank, p=0.92 IABP Increased hazard risk of stroke, downgraded to Class III (harm), Level of Evidence A, ESC STEMI Guidelines Prondzinsky R. et al. Jn Critical Care Medicine IABP SHOCK I 2010 Clinicaltrial.gov # NCT Thiele H et al. NEJM Clinicaltrial.gov #NCT Impella Heart Pump: How It Works Placement in Left Ventricle Impeller and blood outflow Animation Click here Hemodynamic Stability & LV Unloading with Impella Improvement in Cardiac Index ISAR SHOCK Randomized Controlled Trial (L/min/m 2 ) Impella ±0.64 P= ±0.45 Augmented CI N=26 IABP 1.84± ±0.59 N.S. Native Heart Impella 2.5 Ventricular Unloading Native CI Pre- Support On Impella Pre-Support On IABP Seyfarth et al., JACC,

17 Improved Myocardial Perfusion with Impella Coronary Flow Velocity (cm/s) n=11 72 Impella OFF 61 18% p< Bedside planar images with gamma camera Impella ON Occluded RCA/LCX Territory Pre- Support On Support 1. Remmelink, et. al. CCI, Aqel et. al. J Nuclear Cardiology, 2009 CTO of LCX and RCA untreated 2 Improved End Organ Perfusion With Impella Reduction of Blood Lactate Concentration P<.0001 Blood Lactate (mmol/l) Numbers of days from Impella Implant Casassus, et. al, J Interven Cardiol, 2015 Which patient for an acute device? Cardiac arrest with ongoing CPR Cardiogenic shock, IABP-dependent on inotropes and pressors Intra-operative failure to wean from cardiopulmonary bypass Bridge to a decision: indeterminate neurologic status or other significant co-morbidity (i.e., possible incurable malignancy) with critical clinical deterioration 17
18 Device Choices for Cardiac arrest with ongoing CPR CentriMag AB5000 Alternate: Impella 5.0 or Tandem Heart Device Choices for Cardiogenic shock, IABP-dependent on inotropes and pressors CentriMag Impella 5.0 Tandem Heart Device Choices for Bridge to a decision: indeterminate neurologic status or other significant co-morbidity (i.e., possible incurable malignancy) with critical clinical deterioration CentriMag Impella 5.0 Tandem Heart AB
19 Device Choices for Biventricular Bridge to Transplant (BTT) CentriMag or AB5000 (in-patient only) Tandem Heart or Impella (consider axillary approach, in-patient only) 2008: 38 year old mother of three children with sudden, unexplained cardiogenic shock Was at a southern NJ hospital more than an hour away; EF 15% IABP placed for initial stabilization, allowed transfer to NBI Upon arrival, was on maximum pressors and inotropes with MAP 40-50, mixed venous O2 saturation 40%, extremities blue/grey, cold and clammy Intubated, following commands What to do next?? Sternotomy and place short-term LVAD offpump Insertion of femoral V-A ECMO 19
20 She was brought to the operating room.. CentriMag LVAD implanted off-pump Left IABP in overnight to augment BP IABP removed the next day; OOB on POD #2 LVAD explanted 5 days later Discharged home after uneventful hospital recovery 2013: 41 y.o male s/p HeartMate II LVAD followed by heart transplant Seven months post-transplant, becomes noncompliant with immunosuppression meds Suffers 3B rejection with subsequent hemodynamic instability. IABP placed, results in improved mixed venous O2 sats and hemodynamic improvement Few days later, likely due to ongoing myocardial necrosis due to rejection, suffers recurrent VT storms that become more frequent, EF 20% What to do next?? Re-do sternotomy and insertion of CentriMag short-term LVAD Concern: he is only 6-8 months s/p two sternotomies for HM II LVAD followed by heart transplant Insertion of femoral V-A ECMO 20
21 He was brought to the operating room.. Peripheral V-A ECMO established using cannulas surgically placed (open technique) in right femoral artery and right femoral vein Smaller re-perfusion catheter was placed in distal right femoral artery IABP left in place for BP augmentation ECMO removed 2 weeks later, EF 35% Case Presentations 33 y.o. female, acute closure LAD, Impella placed at outside hospital but not functioning well, transferred in cardiogenic shock on high-dose pressors and inotropes Case Presentations 54 y.o. male admitted with recurrent VT, stable during work-up, suffered Vfib arrest, refractory Vfib, with ongoing CPR to OR 21
22 Case Presentations 56 y.o. male awaiting heart transplant, Status 1A inpatient, EF 8%, decompensated CHF refractory to IABP and high-dose inotropes and pressors Case Presentations: Failure to Wean from cardiopulmonary bypass 55 y.o. acute aortic dissection involving rca, underwent Bentall, had RV failure despite additional SVG to RCA Case Presentations: Failure to Wean from Cardiopulmonary Bypass 62 y.o. male suffered massive MI at outside hospital, had IABP, intubated, two episodes cardiac arrest, transferred in cardiogenic shock, underwent emergency CABG 22
MCS for Acute Heart Failure Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant
 MCS for Acute Heart Failure 2016 Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant Why do we decompensate? Which Heart Failure Patients Should Get Palliative Care and Who
MCS for Acute Heart Failure 2016 Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant Why do we decompensate? Which Heart Failure Patients Should Get Palliative Care and Who
Cardiogenic Shock and Initiatives to Reduce Mortality
 Cardiogenic Shock and Initiatives to Reduce Mortality Tanveer Rab, MD, FACC William O Neill, MD, FACC Perwaiz Meraj, MD, FACC Alex Truesdell, MD, FACC The Golden Hours? 50% dead within 10 hours Overall
Cardiogenic Shock and Initiatives to Reduce Mortality Tanveer Rab, MD, FACC William O Neill, MD, FACC Perwaiz Meraj, MD, FACC Alex Truesdell, MD, FACC The Golden Hours? 50% dead within 10 hours Overall
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
Echo assessment of patients with an ECMO device
 Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
CARDIOGENIC SHOCK 2017 Eric Adler MD Associate Clinical Professor, UCSD
 CARDIOGENIC SHOCK 2017 Eric Adler MD Associate Clinical Professor, UCSD CARDIOGENIC SHOCK Definition INADEQUATE TISSUE PERFUSION RESULTING FROM CARDIAC DYSFUNCITON IN SETTING OF EUVOLEMIA HEMODYAMIC
CARDIOGENIC SHOCK 2017 Eric Adler MD Associate Clinical Professor, UCSD CARDIOGENIC SHOCK Definition INADEQUATE TISSUE PERFUSION RESULTING FROM CARDIAC DYSFUNCITON IN SETTING OF EUVOLEMIA HEMODYAMIC
Mechanical Cardiac Support in Acute Heart Failure. Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research
 Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
ECMO as a bridge to durable LVAD therapy. Jonathan Haft, MD Department of Cardiac Surgery University of Michigan
 ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
เอกราช อร ยะช ยพาณ ชย
 30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Andrew Civitello MD, FACC
 Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Case - Advanced HF and Shock (INTERMACS 1)
") Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know!
: What Every Pharmacist Needs to Know!") Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
A National Cardiogenic Shock Initiative (CSI):
:") A National Cardiogenic Shock Initiative (CSI): Insights from the Impella Quality (IQ) Program, cvad Registry and the Detroit CSI Experience William O Neill, MD, FACC Medical Director Structural Heart Disease
A National Cardiogenic Shock Initiative (CSI): Insights from the Impella Quality (IQ) Program, cvad Registry and the Detroit CSI Experience William O Neill, MD, FACC Medical Director Structural Heart Disease
Update on Mechanical Circulatory Support. AATS May 5, 2010 Toronto, ON Canada
 Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Cardiogenic Shock Protocol
 Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Surgical Options for Temporary MCS
 Surgical Options for Temporary MCS Michael A. Acker, MD Julian Johnson Professor of Surgery Chief of Cardiovascular Surgery Director of Heart and Vascular Center University of Pennsylvania Health System
Surgical Options for Temporary MCS Michael A. Acker, MD Julian Johnson Professor of Surgery Chief of Cardiovascular Surgery Director of Heart and Vascular Center University of Pennsylvania Health System
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock
 CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Yoshiya Toyoda, MD, PhD William Maul Measey Professor of Surgery Chief, Cardiovascular Surgery Surgical Director, Mechanical
CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Yoshiya Toyoda, MD, PhD William Maul Measey Professor of Surgery Chief, Cardiovascular Surgery Surgical Director, Mechanical
Ventricular Assisting Devices in the Cathlab. Unrestricted
 Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
The Role of Mechanical Circulatory Support in Cardiogenic Shock: When to Utilize
 The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
ECMO AND SHORT-TERM SUPPORT:
 ECMO AND SHORT-TERM SUPPORT: UTILIZATION GUIDELINES AND IMPACT OF THE NEW HEART ALLOCATION SYSTEM Jeffrey Teuteberg Section Chief of Heart Failure, Cardiac Transplant and Mechanical Circulatory Support
ECMO AND SHORT-TERM SUPPORT: UTILIZATION GUIDELINES AND IMPACT OF THE NEW HEART ALLOCATION SYSTEM Jeffrey Teuteberg Section Chief of Heart Failure, Cardiac Transplant and Mechanical Circulatory Support
Implantable Ventricular Assist Devices and Total Artificial Hearts. Policy Specific Section: June 13, 1997 March 29, 2013
 Medical Policy Implantable Ventricular Assist Devices and Total Artificial Hearts Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective
Medical Policy Implantable Ventricular Assist Devices and Total Artificial Hearts Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective
Counterpulsation. John N. Nanas, MD, PhD. Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece
 John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
Ted Feldman, M.D., MSCAI FACC FESC
 Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Understanding the Pediatric Ventricular Assist Device
 Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
ECMO as a Bridge to Heart Transplant in the Era of LVAD s.
 Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania ECMO as a Bridge to Heart Transplant in the Era of
Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania ECMO as a Bridge to Heart Transplant in the Era of
ST-Elevation Myocardial Infarction & Cardiogenic Shock. - What Should We Do?
 ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA. IMP v4
 1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
Impella Ins & Outs. CarVasz November :45 12:15
 Impella Ins & Outs CarVasz November 21 2014 10:45 12:15 Nicolas M. Van Mieghem, MD, PhD, FESC Clinical Director of Interventional Cardiology Thoraxcenter, Erasmus MC Rotterdam Background IABP is widely
Impella Ins & Outs CarVasz November 21 2014 10:45 12:15 Nicolas M. Van Mieghem, MD, PhD, FESC Clinical Director of Interventional Cardiology Thoraxcenter, Erasmus MC Rotterdam Background IABP is widely
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ
 Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support
 Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced
Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced
To ECMO Or Not To ECMO Challenges of venous arterial ECMO. Dr Emily Granger St Vincent s Hospital Darlinghurst NSW
 To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
Total Artificial Hearts and Implantable Ventricular Assist Devices
 Total Artificial Hearts and Implantable Ventricular Assist Devices Policy Number: 7.03.11 Last Review: 12/2013 Origination: 12/2001 Next Review: 12/2014 Policy Blue Cross and Blue Shield of Kansas City
Total Artificial Hearts and Implantable Ventricular Assist Devices Policy Number: 7.03.11 Last Review: 12/2013 Origination: 12/2001 Next Review: 12/2014 Policy Blue Cross and Blue Shield of Kansas City
Recovering Hearts. Saving Lives.
 Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Ventricular Assist Devices (VADs) and Percutaneous Cardiac Support Systems
 and Percutaneous Cardiac Support Systems") Medical Coverage Policy Effective Date... 2/15/2018 Next Review Date... 2/15/2019 Coverage Policy Number... 0054 Ventricular Assist Devices (VADs) and Percutaneous Cardiac Support Systems Table of Contents
Medical Coverage Policy Effective Date... 2/15/2018 Next Review Date... 2/15/2019 Coverage Policy Number... 0054 Ventricular Assist Devices (VADs) and Percutaneous Cardiac Support Systems Table of Contents
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention
 Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities
 The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
3/1/2017. Chronic Mechanical Support for Heart Failure. Heart Failure is a major driver of morbidity and mortality in the US 1-7
 Chronic Mechanical Support for Heart Failure Margarita Camacho MD, FACS Surgical Director Cardiac Transplant and Mechanical Assist Device Program RWJ/Barnabas Health Heart Centers at Newark Beth Israel
Chronic Mechanical Support for Heart Failure Margarita Camacho MD, FACS Surgical Director Cardiac Transplant and Mechanical Assist Device Program RWJ/Barnabas Health Heart Centers at Newark Beth Israel
Name of Policy: Ventricular Assist Devices and Total Artificial Hearts
 Name of Policy: Ventricular Assist Devices and Total Artificial Hearts Policy #: 033 Latest Review Date: February 2014 Category: Surgery Policy Grade: A Background/Definitions: As a general rule, benefits
Name of Policy: Ventricular Assist Devices and Total Artificial Hearts Policy #: 033 Latest Review Date: February 2014 Category: Surgery Policy Grade: A Background/Definitions: As a general rule, benefits
The Optimal Team for 24/7 CCU shock management
 The Optimal Team for 24/7 CCU shock management Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 3.10 3.25 pm Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
The Optimal Team for 24/7 CCU shock management Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 3.10 3.25 pm Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
Ramani GV et al. Mayo Clin Proc 2010;85:180-95
 THERAPIES FOR ADVANCED HEART FAILURE: WHEN TO REFER Navin Rajagopalan, MD Assistant Professor of Medicine University of Kentucky Director, Congestive Heart Failure Medical Director of Cardiac Transplantation
THERAPIES FOR ADVANCED HEART FAILURE: WHEN TO REFER Navin Rajagopalan, MD Assistant Professor of Medicine University of Kentucky Director, Congestive Heart Failure Medical Director of Cardiac Transplantation
Overview of MCS in Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation
 Overview of MCS in 2017 Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation Technology Embracing Progress Technology Adoption Internet Adoption of Technology Pioneer in the
Overview of MCS in 2017 Bruce B Reid, MD Surgical Director Artificial Heart Program/Heart Transplantation Technology Embracing Progress Technology Adoption Internet Adoption of Technology Pioneer in the
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Strengthening Your VAD Program
 Disclosure: I have no financial conflicts of interest. Strengthening Your VAD Program Octavio E. Pajaro MD, PhD Chair, Cardiothoracic Surgery Mayo Clinic Arizona Surgical Director, Heart Transplantation
Disclosure: I have no financial conflicts of interest. Strengthening Your VAD Program Octavio E. Pajaro MD, PhD Chair, Cardiothoracic Surgery Mayo Clinic Arizona Surgical Director, Heart Transplantation
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA
 CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
Cardiogenic Shock. Dr. JPS Henriques. Academic Medical Center University of Amsterdam The Netherlands
 Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Pediatric Mechanical Circulatory Support (MCS)
") Pediatric Mechanical Circulatory Support (MCS) Ivan Wilmot, MD Heart Failure, Transplant, MCS Assistant Professor The Heart Institute Cincinnati Children s Hospital Medical Center The University of Cincinnati
Pediatric Mechanical Circulatory Support (MCS) Ivan Wilmot, MD Heart Failure, Transplant, MCS Assistant Professor The Heart Institute Cincinnati Children s Hospital Medical Center The University of Cincinnati
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management
 Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Who is the high risk patient?
 Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Which mechanical assistance for cardiogenic shock?
 Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Implantable Ventricular Assist Devices and Total Artificial Hearts
 Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
High Risk PCI for Heart Failure
 High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
Adult Extracorporeal Life Support (ECLS)
") Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
New Horizons in Cardiogenic Shock. Timothy D. Henry, MD Director of Cardiology Cedars-Sinai Heart Institute
 New Horizons in Cardiogenic Shock Timothy D. Henry, MD Director of Cardiology Cedars-Sinai Heart Institute AMI Shock Mortality Unchanged in > 20 years 74355 US AMI/CGS cases per year 1,2 78954 78500 79823
New Horizons in Cardiogenic Shock Timothy D. Henry, MD Director of Cardiology Cedars-Sinai Heart Institute AMI Shock Mortality Unchanged in > 20 years 74355 US AMI/CGS cases per year 1,2 78954 78500 79823
Antonio Colombo. Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy. Miracor Symposium. Speaker: 15. Parigi: May 16-19, 2017
 Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Parigi: May 16-19, 2017 Miracor Symposium Speaker: 15 Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific Institute, Milan, Italy Nothing to disclose PiCSO Impulse System Elective high risk
Acute Mechanical Circulatory Support Right Ventricular Support Devices
 Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
MANAGEMENT OF CARDIOGENIC SHOCK
 MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio
 Biventricular Heart Failure Advanced Treatment Options at The Cleveland Clinic Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio I have no disclosures. Examine respiratory and
Biventricular Heart Failure Advanced Treatment Options at The Cleveland Clinic Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio I have no disclosures. Examine respiratory and
VADS; How far have we come?
 VADS; How far have we come? 1 Most Recent Period Estimates of Relative Survival Rates for Prostate and Breast Cancer Relative Survival Rate, % (SE)* 5 Years 10 Years 15 Years 20 Years Breast cancer 86.4
VADS; How far have we come? 1 Most Recent Period Estimates of Relative Survival Rates for Prostate and Breast Cancer Relative Survival Rate, % (SE)* 5 Years 10 Years 15 Years 20 Years Breast cancer 86.4
Left Ventricular Assist Devices (LVADs): Overview and Future Directions
: Overview and Future Directions") Left Ventricular Assist Devices (LVADs): Overview and Future Directions FATIMA KARAKI, M.D. PGY-3, DEPARTMENT OF MEDICINE WASHINGTON UNIVERSITY IN ST. LOUIS ST. LOUIS, MISSOURI, USA St. Louis, Missouri,
Left Ventricular Assist Devices (LVADs): Overview and Future Directions FATIMA KARAKI, M.D. PGY-3, DEPARTMENT OF MEDICINE WASHINGTON UNIVERSITY IN ST. LOUIS ST. LOUIS, MISSOURI, USA St. Louis, Missouri,
MEDICAL POLICY SUBJECT: VENTRICULAR ASSIST DEVICES
 MEDICAL POLICY PAGE: 1 OF: 7 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 7 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Description. Section: Surgery Effective Date: April 15, Subsection: Transplant Original Policy Date: September 13, 2012 Subject:
 Last Review Status/Date: March 2016 Page: 1 of 30 Description Mechanical devices to assist or replace a failing heart have been developed over many decades of research. A ventricular assist device (VAD)
Last Review Status/Date: March 2016 Page: 1 of 30 Description Mechanical devices to assist or replace a failing heart have been developed over many decades of research. A ventricular assist device (VAD)
Implantable Ventricular Assist Devices and Total Artificial Hearts
 Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Outcomes for 15,259 US Patients With Acute MI Cardiogenic Shock (AMICS) Supported With Impella
 Supported With Impella") Outcomes for 15,259 US Patients With Acute MI Cardiogenic Shock (AMICS) Supported With Impella William O Neill, MD, FACC Medical Director Structural Heart Disease at Henry Ford Hospital, MI AMI Shock Mortality
Outcomes for 15,259 US Patients With Acute MI Cardiogenic Shock (AMICS) Supported With Impella William O Neill, MD, FACC Medical Director Structural Heart Disease at Henry Ford Hospital, MI AMI Shock Mortality
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Guideline compliance, utilization trends
 Guideline compliance, utilization trends and device selection Tilmann Schwab Cardiology / Intensive care Cardiac support IABP LVAD Transluminal l LVAD Cardiac support Emergency cardiac life support (ECLS)
Guideline compliance, utilization trends and device selection Tilmann Schwab Cardiology / Intensive care Cardiac support IABP LVAD Transluminal l LVAD Cardiac support Emergency cardiac life support (ECLS)
Ventricular Assist Devices for Permanent Therapy: Current Status and Future
 Ventricular Assist Devices for Permanent Therapy: Current Status and Future Prospects Francis D. Pagani MD PhD Professor of Cardiac Surgery University of Michigan April 28 th, 2012 Disclosures NHLBI and
Ventricular Assist Devices for Permanent Therapy: Current Status and Future Prospects Francis D. Pagani MD PhD Professor of Cardiac Surgery University of Michigan April 28 th, 2012 Disclosures NHLBI and
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support
 Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Surgical Options for Advanced Heart Failure
 Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR
 PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
Acute Circulatory Support Should We or Shouldn t We?
 Acute Circulatory Support Should We or Shouldn t We? Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional Research
Acute Circulatory Support Should We or Shouldn t We? Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional Research
MEDICAL POLICY SUBJECT: VENTRICULAR ASSIST DEVICES. POLICY NUMBER: CATEGORY: Technology Assessment
 MEDICAL POLICY SUBJECT: VENTRICULAR ASSIST DEVICES PAGE: 1 OF: 8 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including
MEDICAL POLICY SUBJECT: VENTRICULAR ASSIST DEVICES PAGE: 1 OF: 8 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including
Why Children Are Not Small Adults? Treatment of Pediatric Patients Needing Mechanical Circulatory Support
 Why Children Are Not Small Adults? Treatment of Pediatric Patients Needing Mechanical Circulatory Support Utpal S Bhalala, MD, FAAP Assistant Professor and Director of Research Pediatric Critical Care
Why Children Are Not Small Adults? Treatment of Pediatric Patients Needing Mechanical Circulatory Support Utpal S Bhalala, MD, FAAP Assistant Professor and Director of Research Pediatric Critical Care
Accepted Manuscript. Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD S (18)
") Accepted Manuscript Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD PII: S0002-9343(18)30496-0 DOI: 10.1016/j.amjmed.2018.04.045 Reference: AJM 14684
Accepted Manuscript Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD PII: S0002-9343(18)30496-0 DOI: 10.1016/j.amjmed.2018.04.045 Reference: AJM 14684
Innovative ECMO Configurations in Adults
 Innovative ECMO Configurations in Adults Practice at a Single Center with Platinum Level ELSO Award for Excellence in Life Support Monika Tukacs, BSN, RN, CCRN Columbia University Irving Medical Center,
Innovative ECMO Configurations in Adults Practice at a Single Center with Platinum Level ELSO Award for Excellence in Life Support Monika Tukacs, BSN, RN, CCRN Columbia University Irving Medical Center,
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS
 ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
Implantable Ventricular Assist Devices and Total Artificial Hearts
 Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Disclosures. No disclosures to report
 Disclosures No disclosures to report Update on MOMENTUM 3 Trial: The Final Word? Francis D. Pagani MD PhD Otto Gago MD Professor of Cardiac Surgery University of Michigan Ann Arbor, Michigan, USA LVAD
Disclosures No disclosures to report Update on MOMENTUM 3 Trial: The Final Word? Francis D. Pagani MD PhD Otto Gago MD Professor of Cardiac Surgery University of Michigan Ann Arbor, Michigan, USA LVAD