Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management
|
|
|
- Elfreda Lawrence
- 6 years ago
- Views:
Transcription

1 Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY
2 Disclosure Abbott/St. Jude Med./Thoratec Consultant
3 Case presentation 58 yom with ischemic cardiomyopathy; LVEF 10-15%; s/p multiple PCIs at outside hospital; s/p AICD Able to walk ½ block; sleeps on a recliner Pre-op RHC: RA 18, PA 72/22/48, PCWP 28, Fick CO 3.73 and Fick CI 1.51; PVR 5.4 After nipride: PA 60/23/38, PCWP 21, CO 5.6, CI 2.3; PVR 3.03 To OR for continuous flow LVAD

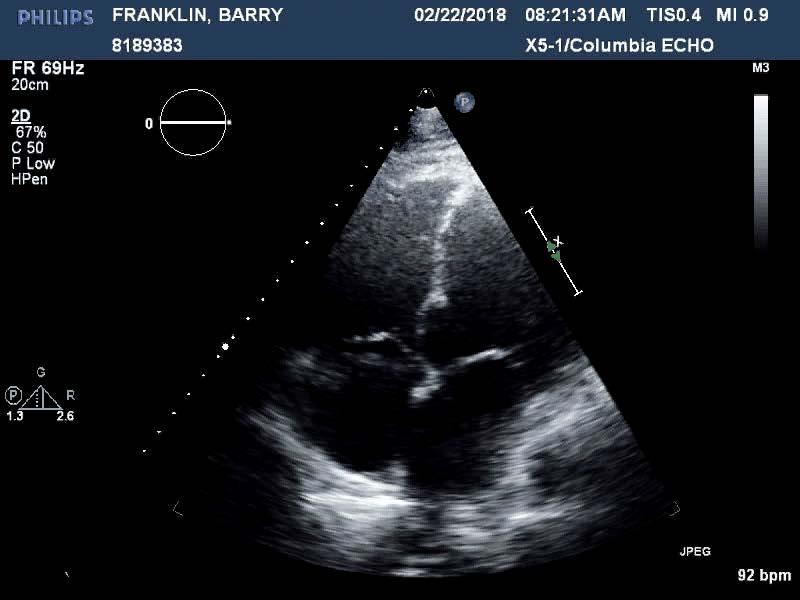
4 Pre-operative echo shows severe biventricular dysfunction
5 What should be done?
6 Discussion points Prediction of RV failure after continuous flow LVAD placement Timing of RVAD insertion Simultaneous vs. early post-op vs. delayed post-op Device options Management considerations Amount of support Duration of support Weaning parameters Other considerations (anticoagulation, ambulation)
, and worse survival after cardiac transplant Why does RV failure occur, and how do we predict it?")
7 RV failure is bad Severe right heart failure after LVAD surgery is a serious complication Up to 35% of patients receiving a continuous flow LVAD developed post-operative RV failure Post-operative RV failure is associated with high rates of mortality (19-43%), and worse survival after cardiac transplant Why does RV failure occur, and how do we predict it? Post-LVAD RV failure is also associated with delayed or failed restoration of end-organ function, prolonged ICU course, and prolonged hospital stay
8 Why does this happen? Complex and dynamic forces at play: Mechanical insult from actual surgery RV geometry Cardiopulmonary bypass Bleeding; blood and product transfusion Insertion LVAD of LVAD placed and turned on RV afterload RV size RV function
9 Many studies have found a variety of risk factors that increase odds of developing postoperative RV failure Pre-operative temporary mechanical circulatory support as bridge Impella, TandemHeart, VA-ECMO, CentriMag High BUN, creatinine, AST, total bilirubin Suggests pre-operative volume overload, inadequate optimization Suggests impaired end-organs caused by end-stage heart failure Pre-operative cardiac arrest Particularly AMI in LAD distribution; septal dysfunction Pre-operative IV vasopressor medications Suggests vasoplegia Suggests how ill
10 And there are various formulas and methods to predict RV failure after LVAD Right ventricular risk factor score EUROMACS-RHF risk score Pulmonary artery pulsatility index High central venous pressure : pulmonary capillary wedge pressure ratio Low right ventricular stroke work index (RVSWI) Echocardiographic parameters: severe RV dysfunction

11 For instance: the Michigan right ventricular failure risk factor score But this score is limited: Based on preoperative values only Does not incorporate intraoperative data for real-time decisionmaking

12 What about the EUROMACS Right-Sided Heart Failure Risk Score? Only looks at five variables: INTERMACS class Use of multiple inotropes Severe RV dysfunction on echo RA/PCWP Hemoglobin But what about patient demographics? And endorgan function?

13 A final example from Columbia Large body size is an important risk factor for mortality on biventricular support and should be incorporated into selection decisions. No other study has duplicated this finding regarding BSA
14 Do we still lack a perfect predictor? Derived from single-center cohorts using variable definitions of RHF They have modest predictive value when validated in independent cohorts Prediction is difficult because of the complex pathophysiology of RV failure: RV myocardial dysfunction Ventricular interdependence Elevated RV afterload
 Diego Bellavia et.al.")
15 We are currently unable to accurately predict RV failure Even the best meta-analysis identified several predictors but they have low sensitivity (~30%) Diego Bellavia et.al. Eur J Heart Fail 2017 Variables that stood out on some studies as predictive were meaningless in others RV Failure

16 How (and when) to treat RV failure? Pre-operative optimization: Diuresis and volume management Pulmonary vasodilators Inotropy for adequate systemic BP Intra-operative options: Careful management of blood loss Inhaled nitric Minimizing transfusions, using coagulation factor replacement Planned placement of temporary RVAD Post-operative management:

17 We know that unplanned RVAD placement after LVAD leads to poor outcomes Only half of patients were able to wean from RVAD support Unplanned RVAD resulted in ongoing end-organ dysfunction Hospital mortality was significantly higher in unplanned RVAD patients
18 Placement of prophylactic RVAD in highrisk LVAD patients: the Columbia approach Patient who presented with INTERMACS 1 or 2 status Severe intra-operative vasoplegia (high-dose pressor requirement, normal estimated cardiac output) Renal dysfunction; minimal response to post-cpb diuresis; high CVP Severe RV dysfunction on pre-operative or intra-operative echo Those that do not tolerate chest closure; allows for chest closure

19 In equivocal cases, is it better to wait and implant if severe RV failure develops? Unequivocally, do not wait SIMULTANEOUS Technical complications of RVAD placement Another device to monitor Manageable drawbacks WAITING Higher risk of post-operative renal failure Prolonged mechanical ventilation Prolonged ICU course and hospital stay Higher mortality- irrecoverable
20 What are our device options? CentriMag Protek Duo Impella RP Second rotary pump VA-ECMO

21 Surgical RVAD versus percutaneous RVAD: our experience Percutaneous alternatives to surgical RVAD include the Impella RP and the Protek Duo Impella RP is a microaxial intra-corporal device Protek Duo is a centrifugal flow extracorporal device Figure 1. Chest radiographs illustrating placement of A) Impella RP, with femoral cannulation and B) Protek Duo, with internal jugular cannulation
22 Surgical RVAD versus percutaneous RVAD: our experience Surgical RVAD had significantly higher flows compared to percutaneous RVAD 5.4 LPM versus 3.8 LPM Additionally, LVAD flows were higher in the surgical RVAD group versus the percutaneous RVAD group 5.8 LPM versus 5.0 LPM Patients with percutaneous RVAD had shorter device time than surgical RVAD (11.0 +/- 8.2 versus / days, p = 0.04) prvad had lower transfusion requirements than surgical RVAD 3.1 +/- 3.5 versus /- 9.2 units, p = 0.007) Surgical RVAD allows higher flows on both RVAD and LVAD than the percutaneous RVAD However, there was a non-significant trend towards higher mortality with surgical RVAD Courtesy of Dr. Reshad Garan, Columbia University Medical Center
23 Changes in hemodynamic parameters with prvad and srvad support
24 Changes in vasopressor and inotrope doses over time with prvad (indicated by solid line) and srvad (indicated by dotted line) vasoprssor inotrope

25 Surgical RVAD (for example, CentriMag) Versatile inflow site: internal jugular vein, femoral vein, RA/RV via graft Outflow into the main PA via 8 mm ringed PTFE graft; Fr EOPA cannula into the graft; tunneled through the chest wall Allows for RVAD decannulation without opening the chest; can flow higher than percutaneous RVAD Able to add in an oxygenator

26 TandemHeart Protek Duo 29 Fr or 31 Fr dual lumen cannula Percutaneously introduced via the right IJ and directed through the RVOT and distal to the pulmonary valve Drainage holes in the RA; return in the main PA Option to add-in oxygenator as needed Can be done in the hybrid OR or under TEE guidance


27 TandemHeart Protek Duo
28 Other device considerations Impella RP: Easy insertion via the femoral vein However, patient cannot ambulate Requires bolus heparin at insertion and subsequent continuous heparin purge, possibly resulting in higher levels of anticoagulation VA ECMO: Difficult to differentiate LVAD flow from VA-ECMO flow Competition between VA ECMO and LVAD can result in possible LV thrombus

29 RVAD Management Flow as much as you can in the early postoperative period Allow for recovery of end-organ function and resolution of post-operative vasoplegia Ventricular shape on TTE does not matter: do not consider septal shifting before achieve maximal MCS support Do not need pulsatility on a-line or PA line

30 Adjuncts for RV recovery Early institution of CVVH if adequate volume removal cannot be obtained via medication-directed diuresis Continuous inhaled nitric oxide and transition to other pulmonary vasodilators Maintaining hemoglobin of 8 g/dl or greater

31 Timing of weaning: slow is best When pressors are off or very low Inotropy is at lower levels Vasodilatory shock has resolved Cardiogenic shock is improving Creatinine and LFTs are normalizing Use echo to optimize LV on short-axis view End-organ function has recovered Need to maintain LV geometry to allow for septal function Patients can be ambulated Slowly wean RVAD flows to 2 LPM
32 RVAD removal: in OR or procedure room Bring RVAD flows temporarily to 1 LPM Monitor hemodynamics Look at CVP, MAP, PA pressure and pulsatility Can check mixed venous and lactic acid Echo evaluation But remember: RV contractility is not sole indicator for RVAD removal

33 RVAD weaning parameters- on echo Short axis view is key No RV bulging into the LV During echo weaning test, evaluate both ventricles Adjust both RVAD and LVAD speeds Septum should not be flat: this suggests that patient is volume overloaded or that LVAD speed is not optimized
34 Other management considerations: Ambulation: avoid using femoral cannulation such as ProTek Duo and even surgical RVADs which allow for increased mobility. We aim for early mobility Extubation: Early extubation should always be facilitated Anticoagulation: We do not provide higher levels of anticoagulation for BiVAD patients Small right-sided embolism undetectable
35 Case presentation 58 yom with ischemic cardiomyopathy; LVEF 10-15%; s/p multiple PCIs at outside hospital; s/p AICD Able to walk ½ block; sleeps on a recliner Pre-op RHC: RA 18, PA 72/22/48, PCWP 28, Fick CO 3.73 and Fick CI 1.51; PVR 5.4 After nipride: PA 60/23/38, PCWP 21, CO 5.6, CI 2.3; PVR 3.03 To OR for continuous flow LVAD
36 Pre-operative echo shows severe biventricular dysfunction
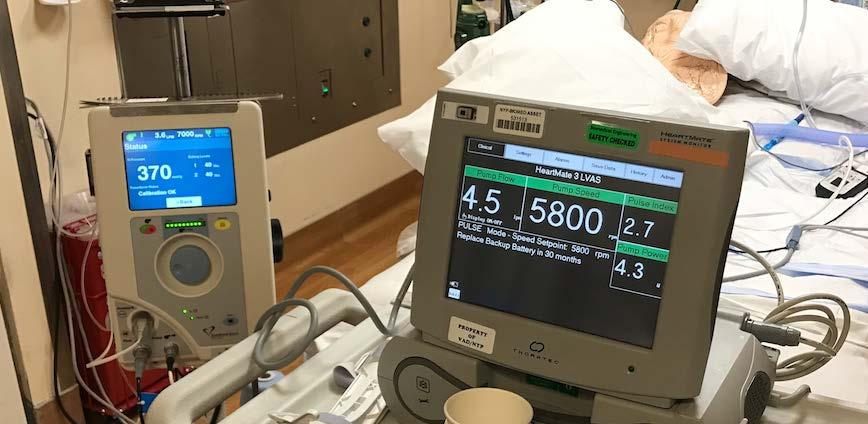
37 Intra-operative course: Uneventful placement of HM3 LVAD Off bypass with significant pressor requirement; did not improve despite addition of epinephrine CVP high (18-20); poor response to diuresis, mixed venous marginal (low 50s) RV severely dysfunctional both on inspection and on TEE Attempted adjusting LVAD speeds, but no clinical improvement Decision made to place TEE-guided ProtekDuo New left IJ central line; swan moved to left neck Placed 29 Fr ProtekDuo via R IJ, through RVOT and beyond pulmonary valve Closed chest after RVAD on and maximum flow; tolerated chest closure well To the ICU : HM3 5.3/6000 RPM; RVAD 4.5 LPM; milrinone 0.25; dobutamine 5; pressors low at 4/2; CVP 14; brisk response to diuresis


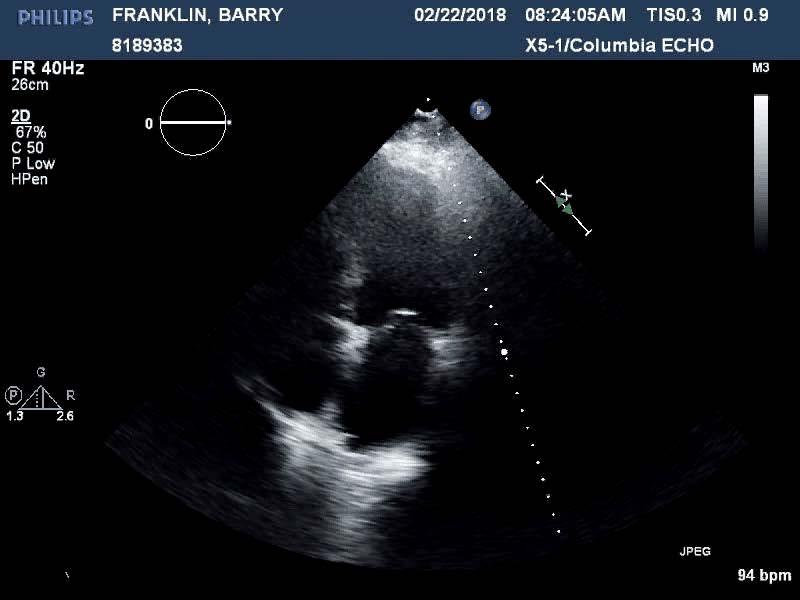
38 Post-operative echo after RVAD placement Echo during RVAD weaning trial
39 Post-operative course uneventful Extubated POD #2 Pressors off by POD #3, dobutamine weaned off POD #4 excellent urine output RVAD removed POD# 7 To step-down unit POD #10 To skilled nursing facility POD #20


40
41 3 steps to avoid post ope RV failure Patient selection Prevention of RV failure Treatment of RV failure
Right Heart Failure in LVAD patients: Prevention and Management.
 Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania Right Heart Failure in LVAD patients: Prevention and
Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania Right Heart Failure in LVAD patients: Prevention and
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD
 A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
Right Ventricular Failure: Prediction, Prevention and Treatment
 Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Acute Mechanical Circulatory Support Right Ventricular Support Devices
 Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
ECMO as a bridge to durable LVAD therapy. Jonathan Haft, MD Department of Cardiac Surgery University of Michigan
 ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Mechanical Cardiac Support in Acute Heart Failure. Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research
 Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Andrew Civitello MD, FACC
 Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
เอกราช อร ยะช ยพาณ ชย
 30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support
 Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Complications of VAD therapy - RV failure
 Complications of VAD therapy - RV failure Nana Afari-Armah, MD Advanced heart failure and transplant cardiology Temple University Hospital 3/24/18 Goals Understand the role of the right ventricle in LVAD
Complications of VAD therapy - RV failure Nana Afari-Armah, MD Advanced heart failure and transplant cardiology Temple University Hospital 3/24/18 Goals Understand the role of the right ventricle in LVAD
Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio
 Biventricular Heart Failure Advanced Treatment Options at The Cleveland Clinic Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio I have no disclosures. Examine respiratory and
Biventricular Heart Failure Advanced Treatment Options at The Cleveland Clinic Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio I have no disclosures. Examine respiratory and
Please cite this article as: Ellie J Coromilas MD, Koji Takeda MD, PhD, Masahiko Ando MD,
 Accepted Manuscript Comparison of Percutaneous and Surgical Right Ventricular Assist Device Support Following Durable Left Ventricular Assist Device Insertion Ellie J Coromilas MD, Koji Takeda MD, PhD,
Accepted Manuscript Comparison of Percutaneous and Surgical Right Ventricular Assist Device Support Following Durable Left Ventricular Assist Device Insertion Ellie J Coromilas MD, Koji Takeda MD, PhD,
Case - Advanced HF and Shock (INTERMACS 1)
") Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Echo assessment of patients with an ECMO device
 Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Innovative ECMO Configurations in Adults
 Innovative ECMO Configurations in Adults Practice at a Single Center with Platinum Level ELSO Award for Excellence in Life Support Monika Tukacs, BSN, RN, CCRN Columbia University Irving Medical Center,
Innovative ECMO Configurations in Adults Practice at a Single Center with Platinum Level ELSO Award for Excellence in Life Support Monika Tukacs, BSN, RN, CCRN Columbia University Irving Medical Center,
Update on Mechanical Circulatory Support. AATS May 5, 2010 Toronto, ON Canada
 Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
 Derivation and Validation of a Novel Right-Sided Heart Failure Model After Implantation of Continuous Flow Left Ventricular Assist Devices: the EUROMACS-RHF Risk Score Osama I.I. Soliman, MD, PhD, FACC,
Derivation and Validation of a Novel Right-Sided Heart Failure Model After Implantation of Continuous Flow Left Ventricular Assist Devices: the EUROMACS-RHF Risk Score Osama I.I. Soliman, MD, PhD, FACC,
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA
 CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
LV Distension and ECLS Lungs
 LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
Mechanical Cardiac Support and Cardiac Transplant: The Role for Echocardiography
 Mechanical Cardiac Support and Cardiac Transplant: The Role for Echocardiography David Langholz, M.D., F.A.C.C. Co-Director Cardiovascular Imaging Fredrick Meijer Heart and Vascular Institute Spectrum
Mechanical Cardiac Support and Cardiac Transplant: The Role for Echocardiography David Langholz, M.D., F.A.C.C. Co-Director Cardiovascular Imaging Fredrick Meijer Heart and Vascular Institute Spectrum
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
What are the indications for Tricuspid valve repair during LVAD Implant RANJIT JOHN, MD UNIVERSITY OF MINNESOTA
 What are the indications for Tricuspid valve repair during LVAD Implant RANJIT JOHN, MD UNIVERSITY OF MINNESOTA Contraindications for LVAD Lack of social support system Nonreversible end organ failure
What are the indications for Tricuspid valve repair during LVAD Implant RANJIT JOHN, MD UNIVERSITY OF MINNESOTA Contraindications for LVAD Lack of social support system Nonreversible end organ failure
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Initial experience with Imacor htee-guided management of patients following transplant and mechanical circulatory support.
 Thomas Jefferson University Jefferson Digital Commons Department of Cancer Biology Faculty Papers Department of Cancer Biology Fall 11-1-2012 Initial experience with Imacor htee-guided management of patients
Thomas Jefferson University Jefferson Digital Commons Department of Cancer Biology Faculty Papers Department of Cancer Biology Fall 11-1-2012 Initial experience with Imacor htee-guided management of patients
Understanding the Pediatric Ventricular Assist Device
 Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
The Role of Mechanical Circulatory Support in Cardiogenic Shock: When to Utilize
 The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities
 The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Echocardiographic Structural Assessment Pre- LVAD
 None Disclosures Echocardiographic Structural Assessment Pre- LVAD LVEF ( 25% for DT LVAD) Right ventricle Valvular disease Intra- cardiac shunts Intra- cardiac thrombi Ascending aorta Case 1 50 yo M
None Disclosures Echocardiographic Structural Assessment Pre- LVAD LVEF ( 25% for DT LVAD) Right ventricle Valvular disease Intra- cardiac shunts Intra- cardiac thrombi Ascending aorta Case 1 50 yo M
Artificial Heart Program
 Artificial Heart Program Provider Review: General VAD Overview Indications for VAD Bridge to transplant (BTT) historically most common (~80%) allow rehab from severe CHF while awaiting donor Bridge to
Artificial Heart Program Provider Review: General VAD Overview Indications for VAD Bridge to transplant (BTT) historically most common (~80%) allow rehab from severe CHF while awaiting donor Bridge to
ORIGINAL ARTICLE. Alexander M. Bernhardt a, *, Theo M.M.H. De By b, Hermann Reichenspurner a and Tobias Deuse a. Abstract INTRODUCTION
 European Journal of Cardio-Thoracic Surgery 48 (2015) 158 162 doi:10.1093/ejcts/ezu406 Advance Access publication 29 October 2014 ORIGINAL ARTICLE Cite this article as: Bernhardt AM, De By TMMH, Reichenspurner
European Journal of Cardio-Thoracic Surgery 48 (2015) 158 162 doi:10.1093/ejcts/ezu406 Advance Access publication 29 October 2014 ORIGINAL ARTICLE Cite this article as: Bernhardt AM, De By TMMH, Reichenspurner
Cardiogenic Shock Protocol
 Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
DEMYSTIFYING VADs. Nicolle Choquette RN MN Athabasca University
 DEMYSTIFYING VADs Nicolle Choquette RN MN Athabasca University Objectives odefine o Heart Failure o VAD o o o o Post Operative Complications Acute Long Term Nursing Interventions What is Heart Failure?
DEMYSTIFYING VADs Nicolle Choquette RN MN Athabasca University Objectives odefine o Heart Failure o VAD o o o o Post Operative Complications Acute Long Term Nursing Interventions What is Heart Failure?
Surgical Options for Temporary MCS
 Surgical Options for Temporary MCS Michael A. Acker, MD Julian Johnson Professor of Surgery Chief of Cardiovascular Surgery Director of Heart and Vascular Center University of Pennsylvania Health System
Surgical Options for Temporary MCS Michael A. Acker, MD Julian Johnson Professor of Surgery Chief of Cardiovascular Surgery Director of Heart and Vascular Center University of Pennsylvania Health System
ORIGINAL ARTICLE. Abstract INTRODUCTION
 European Journal of Cardio-Thoracic Surgery 52 (2017) 1055 1061 doi:10.1093/ejcts/ezx189 Advance Access publication 22 June 2017 ORIGINAL ARTICLE Cite this article as: Takeda K, Garan AR, Ando M, Han J,
European Journal of Cardio-Thoracic Surgery 52 (2017) 1055 1061 doi:10.1093/ejcts/ezx189 Advance Access publication 22 June 2017 ORIGINAL ARTICLE Cite this article as: Takeda K, Garan AR, Ando M, Han J,
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation.
 Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
ECMO and VAD implantation
 1 Udine ECMO Workshop ECMO and VAD implantation Prof. Tomaso Bottio Division of Cardiac Surgery (Director Prof. Gino gerosa) ECMO Extracorporeal membrane oxygena1on (ECMO) is a rescue therapy to support
1 Udine ECMO Workshop ECMO and VAD implantation Prof. Tomaso Bottio Division of Cardiac Surgery (Director Prof. Gino gerosa) ECMO Extracorporeal membrane oxygena1on (ECMO) is a rescue therapy to support
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Intra-operative Echocardiography: When to Go Back on Pump
 Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Short and long term mechanical circulatory support: Management in intensive care. Dr Ana Hurtado Consultant Intensivist Harefield Hospital, UK
 Short and long term mechanical circulatory support: Management in intensive care Dr Ana Hurtado Consultant Intensivist Harefield Hospital, UK Right device for the right patient why are you doing this?
Short and long term mechanical circulatory support: Management in intensive care Dr Ana Hurtado Consultant Intensivist Harefield Hospital, UK Right device for the right patient why are you doing this?
Hardware in the Chest - From VADs to Valves
 Hardware in the Chest - From VADs to Valves Cristina Fuss, MD Purpose Recognize the device Indication and function Cristina Fuss, MD Department of Diagnostic Radiology FROM VADS TO VALVES Implanting technique
Hardware in the Chest - From VADs to Valves Cristina Fuss, MD Purpose Recognize the device Indication and function Cristina Fuss, MD Department of Diagnostic Radiology FROM VADS TO VALVES Implanting technique
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR
 PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock
 CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Yoshiya Toyoda, MD, PhD William Maul Measey Professor of Surgery Chief, Cardiovascular Surgery Surgical Director, Mechanical
CABG for ischemic cardiomyopathy, post myocardial infarction and cardiogenic shock Yoshiya Toyoda, MD, PhD William Maul Measey Professor of Surgery Chief, Cardiovascular Surgery Surgical Director, Mechanical
AATS/Cardiothoracic Critical Care Symposium
 AATS/Cardiothoracic Critical Care Symposium Balancing Pharmacologic and Mechanical Support Robert L Kormos MD, FACS, FRCS(C), FAHA I have no disclosures and will not discuss off label use of drugs or devices
AATS/Cardiothoracic Critical Care Symposium Balancing Pharmacologic and Mechanical Support Robert L Kormos MD, FACS, FRCS(C), FAHA I have no disclosures and will not discuss off label use of drugs or devices
From Recovery to Transplant: One Patient's Journey
 From Recovery to Transplant: One Patient's Journey Tonya Elliott, RN, MSN Assist Device and Thoracic Transplant Coordinator Inova Transplant Center at Inova Fairfax Hospital Falls Church, VA Introduction
From Recovery to Transplant: One Patient's Journey Tonya Elliott, RN, MSN Assist Device and Thoracic Transplant Coordinator Inova Transplant Center at Inova Fairfax Hospital Falls Church, VA Introduction
Adult Extracorporeal Life Support (ECLS)
") Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD?
 Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD? Mechanical Circulatory Support Symposium 2018 (Houston, TX) Charles Hoopes, MD Professor of Surgery University of Alabama (Birmingham)
Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD? Mechanical Circulatory Support Symposium 2018 (Houston, TX) Charles Hoopes, MD Professor of Surgery University of Alabama (Birmingham)
Implantable Ventricular Assist Devices and Total Artificial Hearts. Policy Specific Section: June 13, 1997 March 29, 2013
 Medical Policy Implantable Ventricular Assist Devices and Total Artificial Hearts Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective
Medical Policy Implantable Ventricular Assist Devices and Total Artificial Hearts Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
How to mend a broken heart: transplantation or LVAD?
 SCDU DI CARDIOCHIRURGIA Università degli Studi di Torino Ospedale S. Giovanni Battista Direttore: Prof. Mauro Rinaldi How to mend a broken heart: transplantation or LVAD? Massimo Boffini Mauro Rinaldi
SCDU DI CARDIOCHIRURGIA Università degli Studi di Torino Ospedale S. Giovanni Battista Direttore: Prof. Mauro Rinaldi How to mend a broken heart: transplantation or LVAD? Massimo Boffini Mauro Rinaldi
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
Which mechanical assistance for cardiogenic shock?
 Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
The Optimal Team for 24/7 CCU shock management
 The Optimal Team for 24/7 CCU shock management Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 3.10 3.25 pm Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
The Optimal Team for 24/7 CCU shock management Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 3.10 3.25 pm Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
To ECMO Or Not To ECMO Challenges of venous arterial ECMO. Dr Emily Granger St Vincent s Hospital Darlinghurst NSW
 To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
Right Ventricular Failure Following LVAD Insertion: What s New in RV Support? Theresa Anne Gelzinis, M.D. University of Pittsburgh, Pittsburgh, PA
 Session: L241 Session: L412 Right Ventricular Failure Following LVAD Insertion: What s New in RV Support? Theresa Anne Gelzinis, M.D. University of Pittsburgh, Pittsburgh, PA Disclosures: This presenter
Session: L241 Session: L412 Right Ventricular Failure Following LVAD Insertion: What s New in RV Support? Theresa Anne Gelzinis, M.D. University of Pittsburgh, Pittsburgh, PA Disclosures: This presenter
Ramani GV et al. Mayo Clin Proc 2010;85:180-95
 THERAPIES FOR ADVANCED HEART FAILURE: WHEN TO REFER Navin Rajagopalan, MD Assistant Professor of Medicine University of Kentucky Director, Congestive Heart Failure Medical Director of Cardiac Transplantation
THERAPIES FOR ADVANCED HEART FAILURE: WHEN TO REFER Navin Rajagopalan, MD Assistant Professor of Medicine University of Kentucky Director, Congestive Heart Failure Medical Director of Cardiac Transplantation
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
ECMO as a Bridge to Heart Transplant in the Era of LVAD s.
 Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania ECMO as a Bridge to Heart Transplant in the Era of
Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania ECMO as a Bridge to Heart Transplant in the Era of
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know!
: What Every Pharmacist Needs to Know!") Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
ECMO AND SHORT-TERM SUPPORT:
 ECMO AND SHORT-TERM SUPPORT: UTILIZATION GUIDELINES AND IMPACT OF THE NEW HEART ALLOCATION SYSTEM Jeffrey Teuteberg Section Chief of Heart Failure, Cardiac Transplant and Mechanical Circulatory Support
ECMO AND SHORT-TERM SUPPORT: UTILIZATION GUIDELINES AND IMPACT OF THE NEW HEART ALLOCATION SYSTEM Jeffrey Teuteberg Section Chief of Heart Failure, Cardiac Transplant and Mechanical Circulatory Support
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Surgical Options for Advanced Heart Failure
 Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
Heart-lung transplantation: adult indications and outcomes
 Brief Report Heart-lung transplantation: adult indications and outcomes Yoshiya Toyoda, Yasuhiro Toyoda 2 Temple University, USA; 2 University of Pittsburgh, USA Correspondence to: Yoshiya Toyoda, MD,
Brief Report Heart-lung transplantation: adult indications and outcomes Yoshiya Toyoda, Yasuhiro Toyoda 2 Temple University, USA; 2 University of Pittsburgh, USA Correspondence to: Yoshiya Toyoda, MD,
Predictors and impact of right heart failure severity following left ventricular assist device implantation
 Original Article Predictors and impact of right heart failure severity following left ventricular assist device implantation Ronald D. Baxter 1, Kristen M. Tecson 2, Sasha Still 1, Justin D. G. Collier
Original Article Predictors and impact of right heart failure severity following left ventricular assist device implantation Ronald D. Baxter 1, Kristen M. Tecson 2, Sasha Still 1, Justin D. G. Collier
Rhondalyn C. McLean. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume VII, A. Study Purpose and Rationale
 A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Bridge to Heart Transplantation
 Bridge to Heart Transplantation Ulf Kjellman MD, PhD Senior Consultant Surgeon Heart Centre KFSH&RC 1 Disclosure Appointed for Proctorship by Thoratec/St.Jude/Abbott 2 To run a full overall covering transplant
Bridge to Heart Transplantation Ulf Kjellman MD, PhD Senior Consultant Surgeon Heart Centre KFSH&RC 1 Disclosure Appointed for Proctorship by Thoratec/St.Jude/Abbott 2 To run a full overall covering transplant
 CASE PRESENTATION Ravi Dhanisetty, M.D. SUNY Downstate 23 July 2009 CASE PRESENTATION xx yr old female with chest pain for 3 days. Initially taken to outside hospital 3 days history of chest pain, shortness
CASE PRESENTATION Ravi Dhanisetty, M.D. SUNY Downstate 23 July 2009 CASE PRESENTATION xx yr old female with chest pain for 3 days. Initially taken to outside hospital 3 days history of chest pain, shortness
ECLS as Bridge to Transplant
 ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
The Role of ECMO in Thoracic Surgery. Matthew Hartwig, MD
 The Role of ECMO in Thoracic Surgery Matthew Hartwig, MD Disclosure Slide Consultant for Mallincrodkt and Quark Pharmaceuticals Case #1 28 y.o. female with tracheal mass No previous medical or surgical
The Role of ECMO in Thoracic Surgery Matthew Hartwig, MD Disclosure Slide Consultant for Mallincrodkt and Quark Pharmaceuticals Case #1 28 y.o. female with tracheal mass No previous medical or surgical
ST-Elevation Myocardial Infarction & Cardiogenic Shock. - What Should We Do?
 ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
VADS; How far have we come?
 VADS; How far have we come? 1 Most Recent Period Estimates of Relative Survival Rates for Prostate and Breast Cancer Relative Survival Rate, % (SE)* 5 Years 10 Years 15 Years 20 Years Breast cancer 86.4
VADS; How far have we come? 1 Most Recent Period Estimates of Relative Survival Rates for Prostate and Breast Cancer Relative Survival Rate, % (SE)* 5 Years 10 Years 15 Years 20 Years Breast cancer 86.4
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Ted Feldman, M.D., MSCAI FACC FESC
 Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Impella Ins & Outs. CarVasz November :45 12:15
 Impella Ins & Outs CarVasz November 21 2014 10:45 12:15 Nicolas M. Van Mieghem, MD, PhD, FESC Clinical Director of Interventional Cardiology Thoraxcenter, Erasmus MC Rotterdam Background IABP is widely
Impella Ins & Outs CarVasz November 21 2014 10:45 12:15 Nicolas M. Van Mieghem, MD, PhD, FESC Clinical Director of Interventional Cardiology Thoraxcenter, Erasmus MC Rotterdam Background IABP is widely
Ventricular Assisting Devices in the Cathlab. Unrestricted
 Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
LVAD Complications, Recovery
 LVAD Complications, Recovery Abbas Ardehali, M.D., F.A.C.S. Professor of Surgery and Medicine, Division of Cardiac Surgery William E. Connor Chair in Cardiothoracic Transplantation Director, UCLA Heart,
LVAD Complications, Recovery Abbas Ardehali, M.D., F.A.C.S. Professor of Surgery and Medicine, Division of Cardiac Surgery William E. Connor Chair in Cardiothoracic Transplantation Director, UCLA Heart,
The recommended steps for treating postcardiotomy
 Feasibility Study of a Temporary Percutaneous Left Ventricular Assist Device in Cardiac Surgery Antonis A. Pitsis, MD, FETCS, Aikaterini N. Visouli, MD, Daniel Burkhoff, MD, PhD, Petros Dardas, MD, FESC,
Feasibility Study of a Temporary Percutaneous Left Ventricular Assist Device in Cardiac Surgery Antonis A. Pitsis, MD, FETCS, Aikaterini N. Visouli, MD, Daniel Burkhoff, MD, PhD, Petros Dardas, MD, FESC,
UNIVERSITY OF UTAH HEALTH CARE HOSPITALS AND CLINICS
 UNIVERSITY OF UTAH HEALTH CARE HOSPITALS AND CLINICS CARDIAC MECHANICAL SUPPORT PROGRAM GUIDELINES CARDIAC MECHANICAL SUPPORT: LVAD BASICS FREQUENT SCENARIOS AND TROUBLESHOOTING Review Date: July 2011
UNIVERSITY OF UTAH HEALTH CARE HOSPITALS AND CLINICS CARDIAC MECHANICAL SUPPORT PROGRAM GUIDELINES CARDIAC MECHANICAL SUPPORT: LVAD BASICS FREQUENT SCENARIOS AND TROUBLESHOOTING Review Date: July 2011
Intraoperative application of Cytosorb in cardiac surgery
 Intraoperative application of Cytosorb in cardiac surgery Dr. Carolyn Weber Heart Center of the University of Cologne Dept. of Cardiothoracic Surgery Cologne, Germany SIRS & Cardiopulmonary Bypass (CPB)
Intraoperative application of Cytosorb in cardiac surgery Dr. Carolyn Weber Heart Center of the University of Cologne Dept. of Cardiothoracic Surgery Cologne, Germany SIRS & Cardiopulmonary Bypass (CPB)
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS
 ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
Cite this article as:
 doi: 10.21037/acs.2018.08.06 Cite this article as: Loforte A, Baiocchi M, Gliozzi G, Coppola G, Di Bartolomeo R, Lorusso R. Percutaneous pulmonary artery venting via jugular vein while on peripheral extracorporeal
doi: 10.21037/acs.2018.08.06 Cite this article as: Loforte A, Baiocchi M, Gliozzi G, Coppola G, Di Bartolomeo R, Lorusso R. Percutaneous pulmonary artery venting via jugular vein while on peripheral extracorporeal
Implantable Ventricular Assist Devices and Total Artificial Hearts
 Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Implantable Ventricular Assist Devices and Total Artificial Hearts Policy Number: Original Effective Date: MM.06.017 05/21/1999 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
CentriMag Ventricular Assist System (VAS): Patient & Device Management Guidelines
: Patient & Device Management Guidelines") CentriMag Ventricular Assist System (VAS): Patient & Device Management Guidelines Levitronix Clinical & Technical Support Phone number(s) United States +1 (800) 372-4698 U.S. Clinical Support (Pager) +1
CentriMag Ventricular Assist System (VAS): Patient & Device Management Guidelines Levitronix Clinical & Technical Support Phone number(s) United States +1 (800) 372-4698 U.S. Clinical Support (Pager) +1
MANAGEMENT OF CARDIOGENIC SHOCK
 MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal