How to manage patient with Non ST elevation Acute coronary syndrome
|
|
|
- Trevor Baker
- 5 years ago
- Views:
Transcription

1 How to manage patient with Non ST elevation Acute coronary syndrome Dr.M.Gholipour Assistant proffessor in interventional cardiology Faculty member of guilan university of medical sciences
2 Definitions schemic heart disease may be manifested clinically as either chronic stable angina or an acute coronary syndrome (ACS). Features that help differentiate ACS from stable angina are (1) onset of symptoms at rest (or with minimal exertion) and lasting longer than 10 minutes unless treated promptly (2) severe, oppressive pressure or chest discomfort (2) an accelerating pattern of symptoms that develop more frequently, occur with greater severity, or awaken the patient from sleep
3 Epidemiology n the United States, three recent trends have changed the frequency distribution of the types of ACS: (1) wider use of primary preventive therapies (aspirin, statins, smoking cessation) appears to have resulted in fewer cases of STEM (2) aging of the U.S. population, with higher rates of diabetes and chronic kidney disease (CKD), have increased the incidence of NSTE-ACS (3) the use of more sensitive assays for myocardial necrosis (i.e., cardiacspecific troponin [ctn]) has shifted the classification of NSTE- ACS away from UA toward NSTEM
4 PATHOPHYSOLOGY rupture of unstable atheromatous plaque imbalance between the supply and demand NSTE-ACS coronary arterial vasoconstriction gradual intraluminal narrowing of an epicardial coronary artery

5 Platlet adhesion,activation,aggergation

6 Platelet activation mechanisms and sites of blockade of antiplatelet therapies
7 CLNCAL ASSESSMENT History and Physical Examination NSTE-ACS resulting from atherosclerosis is relatively uncommon in 1) men younger than 40 years and 2) women younger than 50 years, but the incidence rises steadily thereafter The initial symptom is typically described as pressure, heaviness, or frank pain beneath the sternum is usually more intense and lasts longer (>20 minutes). Associated radiation to the ulnar aspect of the proximal part of the left arm, either shoulder, the neck, or the jaw may occur, but symptoms may be present anywhere between the ear and epigastrum
8 Laboratory
9 NSTE-ACS Definite or likely Short term risk management TM SCORE or GRASE SCORE
10 Short-Term Risk of Death or Nonfatal Myocardial schemia in Patients with Unstable Angina HGH RSK 1)Accelerating tempo of ischemic symptoms in preceding 48 hours 2)Prolonged ongoing (>20 min) pain at rest 3) Pulmonary edema, most likely caused by ischemia/new or worsening MR murmur/s 3 or new or worsening rales/hypotension, bradycardia, tachycardia/age >75 yr 4) Angina at rest with transient ST-segment changes > 0.05 mv/undle branch block, new or presumed new/sustained ventricular tachycardia 5) Elevated cardiac Tn, TnT, or CK-M NTERMEDATE RSK 1)Prior M, peripheral or cerebrovascular disease, or CAG; prior ASA use 2) Prolonged (>20 min) rest angina, now resolved, with intermediate or high likelihood of CAD/Rest angina (>20 min) or relieved with rest or sublingual nitroglycerin/nocturnal angina/new-onset or progressive CCS class or V angina in past 2 wk without prolonged (20 min) rest pain, but with intermediate or high likelihood of CAD 3) Age > 70 yr 4)T wave changes/pathologic Q waves or resting STsegment depression < 0.1 mv in multiple lead groups (anterior, inferior, lateral) 5) Slightly elevated cardiac Tn, TnT, or CK-M
11 TM Risk Score for NSTE-ACS The TM risk score is determined by the sum of the presence of 7 variables at admission; 1 point is given for each of the following variables: 65 y of age; 3 risk factors for CAD; prior coronary stenosis 50%; ST deviation on ECG; 2 anginal events in prior 24 h; use of aspirin in prior 7 d; and elevated cardiac biomarkers. TM Score All cause mortality,new or recurrent M,or severe recurrent ischemia,requiring urgent revascularization throgh 14d after randomization
12 GRACE (Global Registry of Acute Coronary Events) risk score was developed to predict death, and death/m, in a cohort of patients with NSTEM enrolled into a multinational observational registry. Nine factors based on the presenting clinical and biomarker characteristics of the patients were identified as independent predictors of death or a combined outcome of death and M both in-hospital and at 6 months: (1) age, (2) heart failure, (3) peripheral vascular disease, (4) admission systolic blood pressure, (5) Killip class, (6) initial serum creatinine concentration, (7) elevated cardiac markers, (8) cardiac arrest on admission, and (9) ST segment deviation.
13
14 NSTE-ACS Definite or likely schemia-guided strategy Early invasive strategy Medical treatment
15 schemia-guided Strategy Versus Early nvasive Strategies The early invasive strategy recommendations are stratified by timing: mmediate (within 2 hours): Refractory angina Sign or symptom of HF or new or worsening mitral regurgitation Hemodynamic instability Recurrent angina or ischemia at rest or with low level activities despite intensive medical therapy Sustain VT ot VF
16 Early (within 24 hours): None of the immediate characteristics but new ST-segment depression, a GRACE risk score > 140, or temporal change in troponin Delayed invasive: (25-72hours) None of the above but diabetes mellitus Renal insufficiency (GFR <60 ml/min/1.73 m²) Reduced LV systolic function (EF <0.40) Early postinfarction angina PC within 6 mo Prior CAG GRACE risk score ; TM score 2
17 schemia-guided strategy Ø Low-risk score (e.g., TM [0 or 1], GRACE [<109]) Ø Ø Low-risk Tn-negative female patients Patient or clinician preference in the absence of high-risk features
18 2014 AHA/ACC NSTE-ACS Clinical Practice Guidelines Standard Medical Therapies Oxygen Class 1. Supplemental oxygen should be administered to patients with NSTE-ACS with arterial oxygen saturation less than 90%, respiratory distress, or other high-risk features of hypoxemia. (Level of Evidence: C)
19 Contraindications to nitrate use are hypotension or the use of phosphodiesterase type 5 (PDE-5) inhibitors (e.g., sildenafil, tadalafil, vardenafil) within the previous 24 to 48 hours. PDE-5 inhibitors reduce the breakdown of cyclic guanosine monophosphate (cgmp) and thereby cause an exaggeration and prolongation of the vasodilator effects of nitrates, which can result in severe hypotension, myocardial ischemia, or even death. Nitrates should be used with caution in patients with severe aortic valve stenosis, hypertrophic cardiomyopathy with left ventricular outflow obstruction at rest, right ventricular infarction, or hemodynamically significant pulmonary embolism.
20 2014 AHA/ACC NSTE-ACS Clinical Practice Guidelines Nitrates Administer sublingual NTG every 5 min 3 for continuing ischemic pain and then assess need for V NTG Administer V NTG for persistent ischemia, HF, or hypertension Nitrates are contraindicated with recent use of a phosphodiesterase inhibitors C
21 blockers nitiate oral beta blockers within the first 24 h in the absence of HF, lowoutput state, risk for cardiogenic shock, or other contraindications to beta blockade Use of sustained-release metoprolol succinate, carvedilol, or bisoprolol is recommended for beta-blocker therapy with concomitant NSTE-ACS, stabilized HF, and reduced systolic function Re-evaluate to determine subsequent eligibility in patients with initial contraindications to beta blockers t is reasonable to continue beta-blocker therapy in patients with normal LV function with NSTE-ACS a A C C C
22 eta blockers can be administered to patients with heart failure once their condition has stabilized. f ischemia and/or chest pain persists despite intravenous nitrate therapy, intravenous beta blockers may be used cautiously, followed by oral administration. ntravenous beta blockers should be avoided in patients with acute M and heart failure at initial evaluation. The choice of beta blockers can be individualized by taking into account the drug s pharmacokinetics, physician familiarity, and cost, but beta blockers with intrinsic sympathomimetic activity, such as pindolol, should generally be avoided.
23 CCs(calcium chanel blockers) Administer initial therapy with nondihydropyridine CCs with recurrent ischemia and contraindications to beta blockers in the absence of LV dysfunction, increased risk for cardiogenic shock, PR interval >0.24 s, or second- or third-degree atrioventricular block without a cardiac pacemaker Administer oral nondihydropyridine calcium antagonists with recurrent ischemia after use of beta blocker and nitrates in the absence of contraindications CCs are recommended for ischemic symptoms when beta blockers are notsuccessful, are contraindicated, or cause unacceptable side effects Long-acting CCs and nitrates are recommended for patients with coronary artery spasm mmediate-release nifedipine is contraindicated in the absence of a beta blocker C C C
24 Ranolazine This novel antianginal agent exerts its effects without altering the heart rate or blood pressure. ts predominant mechanism of action is inhibition of the late sodium current in myocardial cells, thereby reducing some of the deleterious effects attributed to the overload of intracellular sodium and calcium during ischemia Ranolazine reduces ischemic episodes and the need for nitroglycerin in patients with chronic stable angina, both as monotherapy and in combination with calcium channel blockers or beta blockers. Ranolazine underwent evaluation in a placebocontrolled trial of 6560 patients with NSTE-ACS who were monitored for an average of almost 1 year. n the overall trial population, ranolazine did not reduce the primary composite outcome of cardiovascular death, M, or recurrent ischemia but did decrease the incidence of recurrent ischemia. The primary outcome, however, was reduced significantly in the subgroups of patients with elevated natriuretic peptides (by 21%) and in those with previous stable angina (by 14%).
25 Angiotensin-converting enzyme (ACE) inhibitors: A slight change in level of recommendation was made. ACE inhibitor is a class recommendation for patients with stable chronic kidney disease (CKD) LVEF < 40%, hypertension (HTN), heart failure, or Diabetes mellitus (DM). n all other patients with cardiac or vascular disease was downgraded from a class a recommendation in prior ACS guidelines to a b recommendation
26 Cholesterol Management Class 1. High-intensity statin therapy should be initiated or continued in all patients with NSTE-ACS and no contraindications to its use (Level of Evidence: A) Class a 1. t is reasonable to obtain a fasting lipid profile in patients with NSTE-ACS, preferably within 24 hours of presentation. (Level of Evidence: C)
27 For early initial oral antiplatelet therapy Clopidogrel loading dose followed by daily maintenance dose in patients unable to take aspirin P2Y12 inhibitor, in addition to aspirin, for up to 12 mo for patients treated initially with either an early invasive or initial ischemia-guided strategy P2Y12 inhibitor therapy (clopidogrel, prasugrel, or ticagrelor) continued for at least 12 mo in post PC patients treated with coronary stents Clopidogrel:300-mg or 600-mg loading dose, then 75 mg/d Ticagrelor:180-mg loading dose, then 90 mg D Ticagrelor in preference to clopidogrel for patients treated with an early invasive or ischemia-guided strategy
28 P2Y12 (Adenosine Diphosphate) nhibitors Management of ACS now routinely includes dual antiplatelet therapy (DAPT), which consists of ASA and a P2Y12 inhibitor.the latter falls into two groups: thienopyridines (ticlopidine, clopidogrel, and prasugrel) and a cyclopentyltriazolopyrimidine (ticagrelor). Thienopyridines act by irreversibly blocking binding of ADP to the platelet surface P2Y12 receptor, thereby interfering with both platelet activation and aggregation by ADP. They are prodrugs that require oxidation by the hepatic cytochrome P-450 (CYP) system to form active metabolites. Thienopyridines also reduce fibrinogen, blood viscosity, and erythrocyte deformability and aggregability through mechanisms that appear to be independent of ADP. n contrast, ticagrelor acts directly as a reversible blocker of the P2Y12 receptor. Drugs that inhibit the CYP system do not affect ticagrelor
29 Glycoprotein b/a nhibitors These drugs block the final common pathway of platelet aggregation, fibrinogen-mediated crosslinkage of plate-lets, caused by a variety of stimuli (e.g., thrombin, ADP, collagen, serotonin. Three agents in this class are available: abciximab, a monoclonal antibody approved only in patients undergoing PC; eptifibatide; and tirofiban (the latter two are reversible small-molecule inhibitors). Each of these agents is adminis-tered as an intravenous bolus followed by continuous infusion. The activity of the small-molecule receptor blockers and the accompanying bleeding risk subside promptly after discontinuation of the infusion. Tirofiban and eptifibatide have short half-lives ( 2 hours), with restoration of platelet function in about 4 hours; thus they should be discontinued 2 to 4 hours before major surgery. Abciximab has prolonged action ( 12 hours) and cannot be reversed rapidly, so major surgery should be deferred until at least 24 hours after administration
30 Parenteral anticoagulant therapy SC enoxaparin for duration of hospitalization or until PC is performed ivalirudin until diagnostic angiography or PC is performed in patients with early invasive strategy only SC fondaparinux for the duration of hospitalization or until PC is performed Administer additional anticoagulant with anti-a activity if PC is performed while patient is on fondaparinux V UFH for 48 h or until PC is performed
31 Direct Thrombin nhibitors These drugs have a potential advantage over indirect thrombin inhibitors such as UFH or LMWH in that they do not require antithrombin and can inhibit clot-bound thrombin. They do not interact with plasma proteins, they provide a very stable level of anticoagulation, and they do not cause thrombocytopenia thus making them an excellent choice for anticoagulation in patients with a history of HT. ivalirudin, the most widely used direct thrombin inhibitor in patients with ACS or undergoing PC, binds reversibly to thrombin and has a half-life of approximately 25 minutes.
32 n patients with NSTE-ACS before angiography, the recommended dose of bivalirudin is a 0.1-mg/kg intravenous bolus followed by an infusion at 0.25 mg/kg/hr. f started during the procedure, a 0.75-mg/ kg bolus dose of bivalirudin should be administered, followed by an infusion at 1.75 mg/kg/hr during PC. t may be discontinued shortly after PC to permit removal of arterial access sheaths. n patients with renal dysfunction, the infusion should be modified as follows: (1) if the creatinine clearance is lower than 30 ml/min and the patient is not being managed with hemodialysis, the infusion rate should be reduced to 1 mg/kg/hr, and (2) in patients undergoing hemodialysis, the infusion rate should be reduced to 0.25 mg/kg/hr.
33 Factor Xa nhibitors Fondaparinux This synthetic pentasaccharide is an indirect Xa inhibitor and requires the presence of antithrombin for its action. n patients undergoing PC, however, fondaparinux was associated with more than a threefold increased risk for catheter-related thrombi. Supplemental UFH at the time of catheterization (85 units/kg if no GP b/ a inhibitor was used; 60 units/kg with a concomitant GP b/a inhibitor) appeared to minimize the risk for this problem with fondaparinux. Thus fondaparinux is an alternative for patients with NSTE-ACS managed noninvasively and, in particular, for patients at higher risk for bleeding. Otamixaban At infusions of and mg/kg/hr, the investigational direct factor Xa inhibitor otamixaban is associated with fewer ischemic complications and similar safety as UFH plus eptifibatide in patients with ACS A large phase trial of otamixaban is under way.

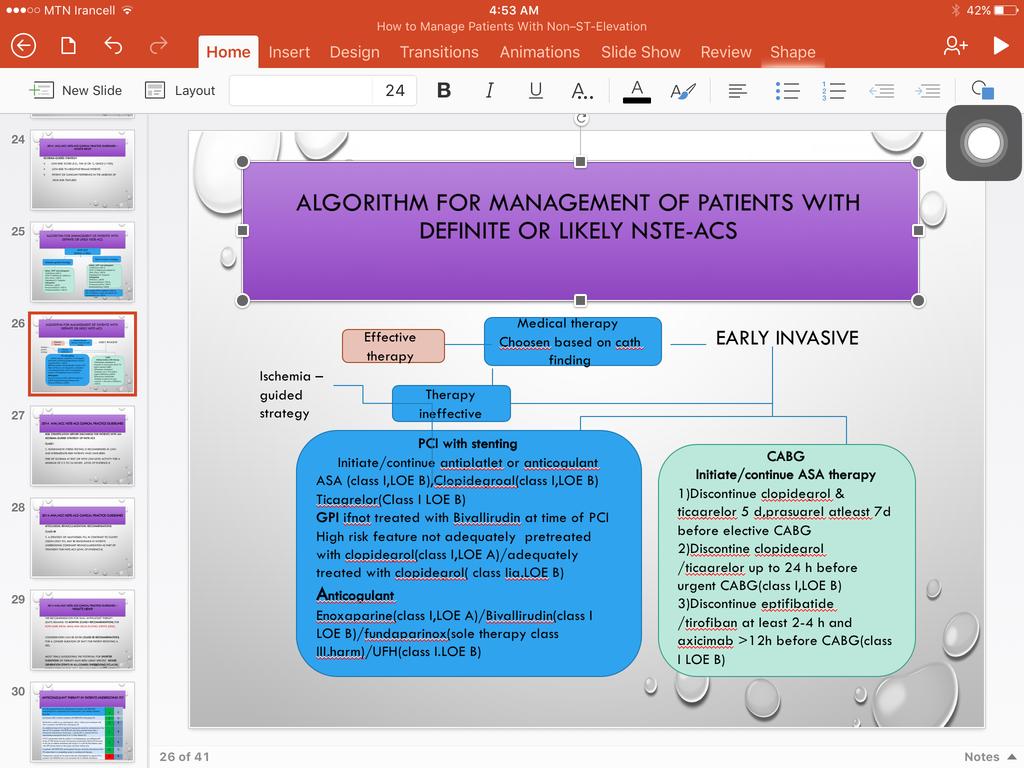
34 Algorithm for Management of Patients With Definite or Likely NSTE-ACS
35
36 Risk Stratification efore Discharge for Patients With an schemia- Guided Strategy of NSTE-ACS Class 1. Noninvasive stress testing is recommended in low- and intermediaterisk patients who have been free of ischemia at rest or with low-level activity for a minimum of )12 to 24 hours (Level of Evidence:
37 Myocardial Revascularization: Recommendations Class b 1. A strategy of multivessel PC, in contrast to culprit lesion-only PC, may be reasonable in patients undergoing coronary revascularization as part of treatment for NSTE-ACS (level of evidence )
38 The recommendation for dual antiplatelet therapy (DAPT) remains 12 months (Class recommendation) for both bare metal (MS) and drug-eluting stents (DESs). Consideration can be given (Class b recommendation) for a longer duration of DAPT for patient receiving a DES. Most trials suggesting the potential for shorter durations of therapy have been using specific newer generation stents in all-comers undergoing PC.More information in this area, primarily from observational studies
39 Anticoagulant Therapy in Patients Undergoing PC An anticoagulant should be administered to patients with NSTE-ACS undergoing PC to reduce the risk of intracoronary and catheter thrombus formation. ntravenous UFH is useful in patients with NSTE-ACS undergoing PC ivalirudin is useful as an anticoagulant with or without prior treatment with UFH in patients with NSTE-ACS undergoing PC An additional dose of 0.3 mg/kg V enoxaparin should be administered at the time of PC to patients with NSTE-ACS who have received fewer than 2 therapeutic subcutaneous doses (e.g., 1 mg/kg SC) or received the last subcutaneous enoxaparin dose 8 to 12 hours before PC f PC is performed while the patient is on fondaparinux, an additional 85 U/kg of UFH should be given intravenously immediately before PC because of the risk of catheter thrombosis (60 U/kg V if a GP b/a inhibitor used with UFH dosing based on the targetactivated clotting time n patients with NSTE-ACS, anticoagulant therapy should be discontinued after PC unless there is a compelling reason to continue such therapy. Fondaparinux should not be used as the sole anticoagulant to support PC in patients with NSTEACS due to an increased risk of catheter thrombosis C C C
40 Clarified that in the setting of ACS, aspirin should be continued/administered prior to CAG (and clopidogrel, ticagrelor be discontinued). class n patients referred for urgent CAG, clopidogrel and ticagrelor should be discontinued for at least 24 hours to reduce major bleeding (Level of Evidence: ) n patients referred for CAG, short-acting intravenous GP b/a inhibitors (eptifibatide or tirofiban) should be discontinued for at least 2 to 4 hours before surgery and abciximab for at least 12 hours before to limit blood loss and transfusion (Level of Evidence: )
41 Late Hospital and Posthospital Oral Antiplatelet Therapy Class 1. Aspirin should be continued indefinitely. The maintenance dose should be 81 mg daily in patients treated with ticagrelor and 81 mg to 325 mg daily in all other patients (Level of Evidence: A) 2. n addition to aspirin, a P2Y12 inhibitor (either clopidogrel or ticagrelor) should be continued for up to 12 months in all patients with NSTE-ACS without contraindications who are treated with an ischemia-guided strategy. Options include: Clopidogrel: 75 mg daily (Level of Evidence: ) or Ticagrelor: 90 mg twice daily (Level of Evidence: ) 3. n patients receiving a stent (bare-metal stent or DES) during PC for NSTE-ACS, P2Y12 inhibitor therapy should be given for at least 12 months. Options include: Clopidogrel: 75 mg daily (Level of Evidence: ) or. Prasugrel: 10 mg daily (Level of Evidence: ) or Ticagrelor: 90 mg twice daily (Level of Evidence: ) Class b 1. Continuation of DAPT beyond 12 months may be considered in patients undergoing stent implantation. (Level of Evidence: C)
42 Combined Oral Anticoagulant Therapy and Antiplatelet Therapy in Patients With NSTEACS Class 1. The duration of triple antithrombotic therapy with a vitamin K antagonist, aspirin, and a P2Y12 receptor inhibitor in patients with NSTE-ACS should be minimized to the extent possible to limit the risk of bleeding. (Level of Evidence: C) 2. Proton pump inhibitors should be prescribed in patients with NSTE-ACS with a history of gastrointestinal bleeding who require triple antithrombotic therapy with a vitamin K antagonist,aspirin, and a P2Y12 receptor inhibitor (Level of Evidence: C) Class a 1. Proton pump inhibitor use is reasonable in patients with NSTE-ACS without a known history of gastrointestinal bleeding who require triple antithrombotic therapy with a vitamin K antagonist, aspirin, and a P2Y12 receptor inhibitor (Level of Evidence: C) Class b,targeting oral anticoagulant therapy to a lower international normalized ratio (e.g., 2.0 to 2.5) may be reasonable in patients with NSTE-ACS managed with aspirin and a P2Y12 inhibitor.( Level of Evidence: C)
43 Special Patient Groups: Recommendations Older patient Treat older patients ( 75 y of age) with GDMT, early invasive strategy, and revascularization as appropriate ndividualize pharmacotherapy in older patients, with dose adjusted by weight and/or CrCl to reduce adverse events caused by age-related changes in pharmacokinetics/dynamics, volume of distribution, comorbidity, drug interactions, and increased drug sensitivity Undertake patient-centered management for older patients, considering patient preferences/goals, comorbidities, functional and cognitive status, and life expectancy ivalirudin rather than GP b/a inhibitor plus UFH is reasonable for older patients ( 75 y of age), given similar efficacy but less bleeding risk t is reasonable to choose CAG over PC in older patients, particularly those with DM or multivessel disease, because of the potential for improved survival and reduced CVD events a a A A
44 Special Patient Groups: Recommendations HF and cardiogenic shock Treat patients with a history of HF according to the same risk stratification guidelines and recommendations for patients without HF Select a revascularization strategy based on the extent of CAD, associated cardiac lesions, LV dysfunction, and prior revascularization Recommend early revascularization for cardiogenic shock due to cardiac pump failure DM Recommend medical treatment and decisions for testing and revascularization similar to those for patients without DM A
45 Chronic Kidney Disease Class 1. 1.CrCl should be estimated in patients with NSTE-ACS, and doses of renally cleared medications should be adjusted according to the pharmacokinetic data for specific medications. (Level of Evidence: ) 2. Patients undergoing coronary and LV angiography should receive adequate hydration. (Level of Evidence: C) 3.Calculation of the contrast volume to creatinine clearance ratio is useful to predict the maximum volume of contrast media that can be given without significantly increasing the risk for contrastinduced nephropathy. (Level of evidence:.)(guideline 2012) Class a 1. An invasive strategy is reasonable in patients with mild (stage 2) and moderate (stage 3) CKD (Level of Evidence: )
46 Special Patient Groups: Recommendations Women Women with NSTE-ACS should be managed with the same pharmacological therapy as that for men for acute care and for secondary prevention, with attention to weight and/or renally calculated doses of antiplatelet and anticoagulant agents to reduce bleeding risk Women with NSTE-ACS and high-risk features (e.g., troponin positive) should undergo an early invasive strategy Myocardial revascularization is reasonable in pregnant women with NSTE-ACS if an ischemiaguided strategy is ineffective for management of life-threatening complications Women with NSTE-ACS and low-risk features should not undergo early invasive treatment because of the lack of benefit and the possibility of harm a A C
47 Class 1. All patients with NSTE-ACS should be evaluated for the risk of bleeding. (Level of Evidence: C) 2. Anticoagulant and antiplatelet therapy should be weight-based where appropriate and should be adjusted when necessary for CKD to decrease the risk of bleeding in patients with NSTE-ACS (Level of Evidence: ) Class : No enefit Special Patient Groups: Recommendations Anemia, leeding and transfusion 1. A strategy of routine blood transfusion in hemodynamically stable patients with NSTE-ACS and hemoglobin levels greater than 8 g/dl is not recommended (Level of Evidence: )
48 Special Patient Groups: Recommendations Vasospastic (Prinzmetal) Angina CCs alone or in combination with long-acting nitrates are useful to treat and reduce the frequency of vasospastic angina Treatment with HMG-CoA reductase inhibitor, cessation of tobacco use and additional atherosclerosis risk factor modification are useful in patients with vasospastic angina. Coronary angiography (invasive or noninvasive) is recommended in patients with episodic chest pain accompanied by transient ST elevation to rule out severe obstructive CAD Provocative testing during invasive coronary angiography may be considered in patients with suspected vasospastic angina when clinical criteria and noninvasive testing fail to establish the diagnosis b C
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
European Heart Journal 2015 doi: /eurheartj/ehv320
 European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 1 2 Clinical implications of high-sensivity troponin assays European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 Conditions other than Type
European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 1 2 Clinical implications of high-sensivity troponin assays European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 Conditions other than Type
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
2015 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation
 2015 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation Thierry Gillebert European Society of Cardiology, Slides kindly provided
2015 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation Thierry Gillebert European Society of Cardiology, Slides kindly provided
MI MANAGEMENT: ACS Guideline Review. Ben Ochoa BS, RCIS, RCS
 MI MANAGEMENT: ACS Guideline Review en Ochoa S, RCIS, RCS Objectives Discuss management of patients with Non-ST-Elevation Acute Coronary Syndromes. Discuss management of patients with ST-Elevation Acute
MI MANAGEMENT: ACS Guideline Review en Ochoa S, RCIS, RCS Objectives Discuss management of patients with Non-ST-Elevation Acute Coronary Syndromes. Discuss management of patients with ST-Elevation Acute
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Acute Coronary Syndromes: Different Continents, Different Guidelines?
 Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
 A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
AIMS: CHEST PAIN. Causes of chest pain. Causes of chest pain: Cardiac causes: Acute coronary syndromes pericarditis thoracic aortic dissection
 CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Pharmacology. Drugs affecting the Cardiovascular system (Antianginal Drugs)
") Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
2014 AHA/ACC Guideline for the Management of Patients With Non ST-Elevation Acute Coronary Syndromes
 2014 AHA/ACC Guideline for the Management of Patients With Non ST-Elevation Acute Coronary Syndromes Developed in Collaboration with the Society of Thoracic Surgeons and Society for Cardiovascular Angiography
2014 AHA/ACC Guideline for the Management of Patients With Non ST-Elevation Acute Coronary Syndromes Developed in Collaboration with the Society of Thoracic Surgeons and Society for Cardiovascular Angiography
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France
 Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France Disclosures Research grants: Astra-Zeneca, Merck, Novartis, Pfizer, sanofi-aventis, Servier, The MedCo Fees
Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France Disclosures Research grants: Astra-Zeneca, Merck, Novartis, Pfizer, sanofi-aventis, Servier, The MedCo Fees
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndrome (ACS) Initial Evaluation and Management
 Initial Evaluation and Management") Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Ischaemic heart disease. IInd Chair and Clinic of Cardiology
 Ischaemic heart disease IInd Chair and Clinic of Cardiology Definition Syndrome due to chronic insufficient oxygen supply to myocardial cells Nomenclature: ischaemic heart disease (IHD), coronary artery
Ischaemic heart disease IInd Chair and Clinic of Cardiology Definition Syndrome due to chronic insufficient oxygen supply to myocardial cells Nomenclature: ischaemic heart disease (IHD), coronary artery
Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017
 Clinician Guide SEPTEMBER 2017") Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
Acute Coronary Syndromes: Review and Update
 Acute Coronary Syndromes: Review and Update Core Curriculum for the Cardiovascular Clinician September 14-17, 2016 R. David Anderson, MD, MS, FACC Professor of Medicine Director of Interventional Cardiology
Acute Coronary Syndromes: Review and Update Core Curriculum for the Cardiovascular Clinician September 14-17, 2016 R. David Anderson, MD, MS, FACC Professor of Medicine Director of Interventional Cardiology
Anticoagulation Update David J. Moliterno, MD
 David J., MD Anticoagulant Agents n Cardiovascular Medicine: An Update David J., MD Professor and Chairman Division of Cardiovascular Medicine The University of Kentucky Linda and Jack Gill Heart nstitute
David J., MD Anticoagulant Agents n Cardiovascular Medicine: An Update David J., MD Professor and Chairman Division of Cardiovascular Medicine The University of Kentucky Linda and Jack Gill Heart nstitute
Otamixaban for non-st-segment elevation acute coronary syndrome
 Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Disclosure. Acute Coronary Syndromes (ACS) Objectives. Pathophysiology. Risk Factors. Update on Treatment of Acute Coronary Syndromes 3/5/2015
 Objectives. Pathophysiology. Risk Factors. Update on Treatment of Acute Coronary Syndromes 3/5/2015") Disclosure Update on Treatment of Acute Coronary Syndromes Duchess Domingo, Pharm.D. PGY-1 Pharmacy Practice Resident Broward Health Medical Center I do not have a vested interest in or affiliation with
Disclosure Update on Treatment of Acute Coronary Syndromes Duchess Domingo, Pharm.D. PGY-1 Pharmacy Practice Resident Broward Health Medical Center I do not have a vested interest in or affiliation with
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Coronary Heart Disease. Raja Nursing Instructor RN, DCHN, Post RN. BSc.N
 Coronary Heart Disease Raja Nursing Instructor RN, DCHN, Post RN. BSc.N 31/03/2016 Objectives Define coronary heart disease (CHD). Identify the causes and risk factors of CHD Discuss the pathophysiological
Coronary Heart Disease Raja Nursing Instructor RN, DCHN, Post RN. BSc.N 31/03/2016 Objectives Define coronary heart disease (CHD). Identify the causes and risk factors of CHD Discuss the pathophysiological
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
Appropriate Timing for Coronary Revascularization Post - MI. Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center
 Appropriate Timing for Coronary Revascularization Post - M Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center Disclosures nterventional cardiologist Clinical Cardiovascular
Appropriate Timing for Coronary Revascularization Post - M Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center Disclosures nterventional cardiologist Clinical Cardiovascular
6/1/18 LEARNING OBJECTIVES PATIENT POPULATION PRESENTATIONS
 PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
Acute Coronary Syndromes: Challenges to Management. Claire Williams November 2017
 Acute Coronary Syndromes: Challenges to Management Claire Williams November 2017 Challenge 1: Diagnosis Chest pain >20 minutes ECG Challenge 1: Diagnosis Treat as STEMI Chest pain >20 minutes ECG STEMI
Acute Coronary Syndromes: Challenges to Management Claire Williams November 2017 Challenge 1: Diagnosis Chest pain >20 minutes ECG Challenge 1: Diagnosis Treat as STEMI Chest pain >20 minutes ECG STEMI
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Acute myocardial infarction. Cardiovascular disorders. main/0202_new 02/03/06. Search date August 2004 Nicholas Danchin and Eric Durand
 main/0202_new 02/03/06 Acute myocardial infarction Search date August 2004 Nicholas Danchin and Eric Durand QUESTIONS Which treatments improve outcomes in acute myocardial infarction?...4 Which treatments
main/0202_new 02/03/06 Acute myocardial infarction Search date August 2004 Nicholas Danchin and Eric Durand QUESTIONS Which treatments improve outcomes in acute myocardial infarction?...4 Which treatments
Prehospital and Hospital Care of Acute Coronary Syndrome
 Ischemic Heart Diseases Prehospital and Hospital Care of Acute Coronary Syndrome JMAJ 46(8): 339 346, 2003 Katsuo KANMATSUSE* and Ikuyoshi WATANABE** * Professor, Second Internal Medicine, Nihon University,
Ischemic Heart Diseases Prehospital and Hospital Care of Acute Coronary Syndrome JMAJ 46(8): 339 346, 2003 Katsuo KANMATSUSE* and Ikuyoshi WATANABE** * Professor, Second Internal Medicine, Nihon University,
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Acute Coronary Syndrome: Management of the patients with Unstable Angina and Non-ST Segment Elevation Myocardial Infarction Rahman S, Rahman KA
 Acute Coronary Syndrome: Management of the patients with Unstable Angina and Non-ST Segment Elevation Myocardial Infarction Rahman S, Rahman KA Introduction Acute Coronary Syndrome (ACS) kills and disables
Acute Coronary Syndrome: Management of the patients with Unstable Angina and Non-ST Segment Elevation Myocardial Infarction Rahman S, Rahman KA Introduction Acute Coronary Syndrome (ACS) kills and disables
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Vorapaxar for the secondary prevention of atherothrombotic events after myocardial infarction Draft scope (pre-referral)
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Vorapaxar for the secondary prevention of atherothrombotic events after myocardial infarction Draft scope (pre-referral)
Ischemic heart disease
 Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Nanik Hatsakorzian Pharm.D/MPH
 Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Quinn Capers, IV, MD
 Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Pre Hospital and Initial Management of Acute Coronary Syndrome
 Pre Hospital and Initial Management of Acute Coronary Syndrome Dr. Muhammad Fadil, SpJP 3rd SymCARD 2013 Classification of ACS ESC Guidelines for the management of Acute Coronary Syndrome in patients without
Pre Hospital and Initial Management of Acute Coronary Syndrome Dr. Muhammad Fadil, SpJP 3rd SymCARD 2013 Classification of ACS ESC Guidelines for the management of Acute Coronary Syndrome in patients without
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Management of Myocardial Infarction & Congestive Heart Failure. Dr. Dionne Dames-Rahming
 Management of Myocardial Infarction & Congestive Heart Failure Dr. Dionne Dames-Rahming Myocardial Infarction Objectives of Medical Management Decrease morbidity Reduce further myocardial damage or injury
Management of Myocardial Infarction & Congestive Heart Failure Dr. Dionne Dames-Rahming Myocardial Infarction Objectives of Medical Management Decrease morbidity Reduce further myocardial damage or injury
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy
 Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Clopidogrel and ASA after CABG for NSTEMI
 Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
Pharmacologic Therapy of Coronary Disease
 Pharmacologic Therapy of Coronary Disease M. MOHSEN IBRAHIM, MD Prof. of Cardiology- Cairo University President of the Egyptian Hypertension Society Introduction Coronary artery disease (CAD) is possibly
Pharmacologic Therapy of Coronary Disease M. MOHSEN IBRAHIM, MD Prof. of Cardiology- Cairo University President of the Egyptian Hypertension Society Introduction Coronary artery disease (CAD) is possibly
10 Steps to Managing Non-ST Elevation ACS
 Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Ischemic Heart Disease
 Ischemic Heart Disease Definition: Ischemic heart disease (IHD) is a condition in which there is an inadequate supply of blood and oxygen to a portion of the myocardium; it typically occurs when there
Ischemic Heart Disease Definition: Ischemic heart disease (IHD) is a condition in which there is an inadequate supply of blood and oxygen to a portion of the myocardium; it typically occurs when there
Platelet-fibrin clot. 50Kd STEMI. Abciximab. Video of a IIb/IIIa inhibitor in action. Unstable Angina and non-stsegment
 Objectives IIb/IIIa, Vitamin K, and Direct Thrombin Inhibition in Cardiology Michael Gulseth, Pharm. D., BCPS Assistant Professor, Duluth Pharmacy 6122 February 14, 2005 Describe the pharmacology, kinetics,
Objectives IIb/IIIa, Vitamin K, and Direct Thrombin Inhibition in Cardiology Michael Gulseth, Pharm. D., BCPS Assistant Professor, Duluth Pharmacy 6122 February 14, 2005 Describe the pharmacology, kinetics,
Treatment of Acute Coronary Syndromes
 Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
NSTEACS Case Presentation
 NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
NCDR CathPCI Registry v4.4 Diagnostic Catheterization and Percutaneous Coronary Intervention Registry
 A. DEMOGRAPHICS Last Name 2000 : First Name 2010 : Middle Name 2020 : SSN 2030 : - - - SSN N/A 2031 Patient ID 2040 : (auto) Other ID 2045 : Birth Date 2050 : *** @ Sex 2060 : *** @ O Male O Female Race:
A. DEMOGRAPHICS Last Name 2000 : First Name 2010 : Middle Name 2020 : SSN 2030 : - - - SSN N/A 2031 Patient ID 2040 : (auto) Other ID 2045 : Birth Date 2050 : *** @ Sex 2060 : *** @ O Male O Female Race:
Coronary Artery Disease Clinical Practice Guidelines
 Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on