PET MYOCARDIAL PERFUSION AND QUANTIFICATION OF FLOW
|
|
|
- Anabel Shelton
- 5 years ago
- Views:
Transcription
1 PET MYOCARDIAL PERFUSION AND QUANTIFICATION OF FLOW Robert Bober, MD, FACC Director of Nuclear Cardiology and Molecular Imaging John Ochsner Heart and Vascular Institute The Ochsner Clinical School University of Queensland Ochsner Medical Center, New Orleans, LA
2 Disclosures Bracco research support, consultant Off-label discussions - None
3 Learning Objectives 1. Discuss the basics of positron emission tomography (PET) imaging and how PET differs from standard single-photon emission computed tomography (SPECT) 2. Discuss evaluation of coronary flow reserve, myocardial perfusion, and absolute myocardial flow by PET imaging and their value in the assessment and management of coronary artery disease (CAD) 3. Introduce the concept of coronary flow capacity and its potential impact on patient care 4. Use cardiac PET imaging to help identify patients for whom revascularization procedures may reduce coronary events
4 Program Agenda PET Instrumentation and how it differs from SPECT Using PET and Flow to Guide Revascularization Measurements of Myocardial Flow Kinetic Models Cases Self Assessment Module
5 PET Instrumentation

6 Conventional SPECT Limited count sensitivity Limited energy resolution Limited spatial and contrast resolution Limited accuracy of measuring uptake without AC Garcia EV, et al. Cardiol Clin. 2009;27(2):
7 PET Instrumentation Line of Response P N N P P P N N B + P 0-5 mm Annihilation 511 KeV γ γ 511 KeV B + Coincidence Event Detected in Ring PET Scanner Cardiac PET. In: Heller GV, Hendel RC. Handbook of Nuclear Cardiology. 1st ed. London, UK: Springer; Turkington TG. J Nucl Med Technol. 2001;29(1):4-11.
8 2D vs 3D Acquisition 2D Turkington TG. J Nucl Med Technol. 2001;29(1):4-11. Multi-ring PET Acquisition Modes 3D
9 Camera Specifications PET 511 KeV photons LIST mode (most) >3 million counts/sec ~35 M counts/study Sensitivity (detection of emitted photons) 2%-15% Spatial resolution < 2-3 mm SPECT Photon energies <140KeV Binned mode (most) counts/sec 7-10 M counts/study Sensitivity 2-3x s less than PETàlonger acquisition Spatial resolution mm Wackers, JACC. 2010;55(18) GB Saha, Basics of Pet Imaging Gould, State of the Art PET 2013, supplement Salerno, Circ Imaging. 2009;2:
10 Attenuation Correction Photon attenuation results from emitted radiation interacting with tissue. For PET, the path length represents the LOR, along which the dually emitted photons travel. Therefore, attenuation is independent of the point of origin along the LOR. For SPECT, due to its single-photon emission nature, attenuation changes depending on the point of emission. LOR, line of response.
11

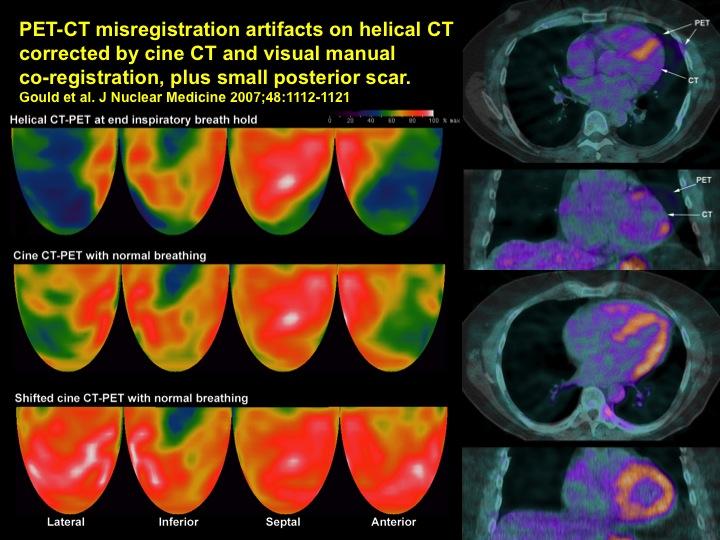
12 Courtesy K. Lance Gould, MD.

13 Courtesy K. Lance Gould, MD.
14 How PET Differs From SPECT
15 Higher Accuracy Current literature supports a high diagnostic accuracy for cardiac PET perfusion imaging, due to: Robust attenuation correction High count densities (improved image quality and interpretation) Tracers that follow MBF in a more linear fashion than current SPECT tracers MBF, myocardial blood flow
16 SROC Curves for Diagnostic Accuracy of Rb-82 PET and Tc-99m SPECT With ECG-Gating and Attenuation Correction Sensi*vity 85% Specificity 85% Sensi*vity 90% Specificity 88% N = 1755 N = 1344 AUC, area under the curve; Q, Cochran Q statistic; SROC, summary receiver-operating characteristic. Mc Ardle BA, et al. J Am Coll Cardiol. 2012;60(18):
17 Summary ROC Curves for SPECT and PET MPI N = 11,862 patients MPI, myocardial perfusion imaging; ROC, receiver operating characteristic Parker MW, et al. Circ Cardiovasc Imaging. 2012;5(6):
18 Overall Diagnostic Accuracy for PET and SPECT: 70% Stenosis Threshold P = 0.02 P = 0.03 Sensi1vity Specificity Accuracy SPECT PET Bateman TM, et al. J Nucl Cardiol. 2006;13(1):24-33.
19 Diagnostic Accuracy for Localizing Disease to Individual Coronary Arteries: 70% Threshold P = P = P = Sensi1vity Specificity Accuracy SPECT PET Bateman TM, et al. J Nucl Cardiol.2006;13:24-33.
20 Body Habitus and Gender Results from studies by Bateman and colleagues demonstrate superior accuracy of PET, independent of both body habitus and gender Bateman TM, et al. J Nucl Cardiol. 2006;13(1):24-33.
21 Diagnostic Accuracy Men 69% 84% *P=0.05 Women 67% 88% *P=0.01 BMI<30 70% 87% *P=0.05 BMI>30 67% 85% *P=0.02 MVD Sensi1vity 48% 71% *P= MVD, multivessel disease. Based on data from Bateman TM, et al. J Nucl Cardiol. 2006;13(1): SPECT PET
22 Risk Stratification SPECT has a wealth of data on risk stratification. More data are emerging for cardiac PET risk stratification. For PET, risk stratification is based on: Size and severity of perfusion abnormalities Decreased ejection fraction at stress Overall ventricular function Coronary flow reserve (CFR)
23 Unadjusted Hazard of Events by % Myocardium Abnormal on Vasodilator Stress Rb-82 PET All-cause Death Cardiac Death Dorbala S, et al. J Am Coll Cardiol. 2013;61(2):
24 Downstream Testing Because of improved image quality, reader confidence is increased. The downstream effect is referral to catheterization for consideration for potential revascularization, NOT to confirm diagnosis. Studies have demonstrated fewer catheterizations following PET compared with SPECT studies.

:1069-1076.")
25 CAD Intervention Utilization Rates vs CAD Management Costs CAD Management Costs in Pts Studied with SPECT vs PET MPI Utilization Rates of Diagnostic Coronary Arteriography, PTCI, and CABG in Pts Studied with SPECT vs PET MPI 50% CABG, coronary artery bypass graft; CAD, coronary artery disease; PTCI, percutaneous transluminal coronary intervention Merhige ME, et al. J Nucl Med. 2007;48(7): % 50%
26 Radiation Exposure Radiation exposure reduction has become an import consideration when selecting a test. ASNC recommended target dose <9 msv for a routine study (recommended to be implemented by 2014). PET flow tracers have been examined, and it has been demonstrated that patient exposure is below that recommended by ASNC. ASNC, American Society of Nuclear Cardiology Cerqueira MD, et al. J Nucl Cardiol. 2010; 17(4):

27 Typical Effective Doses From Cardiac Imaging Procedures Einstein AJ. J Am Coll Cardiol. 2012;59(6):
28 Protocol Patient Convenience Rest/stress Rb-82 protocols can be accomplished in minutes. Rb mci Pharmacologic stress* Rb mci CT transmission Gated rest Gated stress CT transmission sec sec Approx 1 min Approx 7 min Approx 6 min Approx 7 min Approx 1 min *Dipyridamole, adenosine, or dobutamine
29 USING PET AND FLOW TO GUIDE REVASCULARIZATION
30 Current Revascularization Practice LHC (angiogram) gold standard See and fix approach based on % stenosis Current guidelines: 50% LM and 70% for revascularization FFR/stress intermediate lesions 1 FFR used in 6% of patients 2 LHC, left heart catheterization; LM, left main; FFR, fractional flow reserve 1. Levine GN, et al. J Am Coll Cardiol. 2011;58(24):e44-e Dattilo PB, et al. J Am Coll Cardiol. 2012;60(22):
31 Revascularization guided by % stenosis will lead to better outcomes DATA???
32 COURAGE and STICH Revascularization based on % stenosis Stress testing NOT mandatory Decisions to guide revascularization based on judgment of angiographer FFR not utilized Boden WE, et al. N Engl J Med. 2007;356(15): Velazquez EJ, et al. N Engl J Med. 2011;364(17): COURAGE, Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation; STICH, Surgical Treatment for Ischemic Heart Failure.
33 Rates of Survival and Freedom From Major Cardiovascular Events The BARI 2D Study Group. N Engl J Med. 2009;360(24):

34 Revascularization Guided by % Stenosis Will Lead to Better Outcomes DATA Revasculariza1on guided by % stenosis will lead to beter outcomes
35 Repe11on of Error Does Not Cons1tute Experience Edmund Tramont, MD 1999ish
:991-1001.")
36 FAME I and II FFR-guided revascularization I - FFR vs angiography II - FFR vs optimal medical therapy Pijls N, et al. J Am Coll Cardiol. 2010;56(3): De Bruyne B, et al. N Engl J Med. 2012;367(11): FAME, Fractional Flow Reserve versus Angiography for Multivessel Evaluation; MACE, major adverse cardiac events; PCI, percutaneous coronary intervention
:2215-2224. MFR, myocardial flow reserve; SSS, summed stress score.")
37 Herzog BA, et al. J Am Coll Cardiol. 2009;54(2): Ziadi MC, et al. J Am Coll Cardiol. 2011;58(7): Murthy VL, et al. Circulation. 2011;124(20): MFR, myocardial flow reserve; SSS, summed stress score.
38 Introduction to Coronary Blood Flow Ischemia myocardial O 2 supply vs demand Adequate supply is maintained with ability to increase CBF 2 major resistances to flow Epicardial arteries (>350 µm) Arterioles and capillaries (microvasculature) Resting microvascular (R 2 ) >>> epicardial (R 1 ) Normally regulation occurs at level of microvasculature CBF increases automatically to increase O 2 demands Exercise Pharmacologic stress Neurohormonal CBF, coronary blood flow

39 Epicardial Vessels and the Microvasculature
40 Pathologic Conditions R 1 > R 2 Coronary stenosis and diffuse disease à Flow impaired at level of epicardial artery R 2 > R 1 Autoregulation impaired à Flow impaired within microvasculature
41 Coronary Flow Reserve = 2.9 Baseline flow remains stable up to ~83% stenosis. Hyperemic flow starts diminishing ~40% stenosis. Gould KL, et al. Am J Cardiol. 1974;33(1):87-94.

42 A Brief Word on FFR FFR = fractional flow reserve Pressure-derived flow surrogate Stress test of an artery in the cath lab Distal coronary pressure FFR = Proximal coronary pressure During Maximal Hyperemia
:1464-1475. Johnson NP, et al. JACC Cardiovasc Imaging.")
43 Relationships of CFR, FFR, and Absolute Flow Danad I, et al. J Am Coll Cardiol. 2014;64(14): Johnson NP, et al. JACC Cardiovasc Imaging. 2012;5(2):
:193-202.")
44 Relationships of CFR, FFR, and Absolute Flow Johnson NP, et al. JACC Cardiovasc Imaging. 2012;5(2):
45 Invasive CFR vs % Stenosis CFR, coronary flow reserve; LAD, left anterior descending artery White CW, et al. N Engl J Med. 1984;310(13):

46 % Stenosis vs FFR Tonino PA, et al. J Am Coll Cardiol. 2010;55(25):
47 Why is there a huge disparity between flow and anatomy?
48 Flow Dynamics Dependent on lesion length Dependent on lesion diameter to the 4th power A small decrease in diameter or increase in length has a profound effect on flow Gould KL. Circ Res. 1985;57(3):
49 Limitations of Anatomic Measures of Stenosis Severity by Angiogram or IVUS Blood Flow No stenosis CFR = % stenosis CFR = % stenosis CFR = 3.4 Diffuse no stenosis IVUS 38% CFR = 1.4 Diffuse + 60% Artgm IVUS 75% CFR = 1.0 Diffuse + 62% Artgm IVUS 75% & adaptive remodeling CFR = 3.5 IVUS, intravascular ultrasound; Artgm, arteriogram Gould KL. JACC Cardiovasc Imaging. 2009;2(8):
50 Flow vs Stenosis Paradox Flow is determined by a combination of Stenosis Diffuse disease Arterial remodeling Microvascular function Impossible to visually determine the physiologic impact of aggregate disease
51 Measurements of Myocardial Flow Kinetic Models
52 Analogy of Kinetic Modeling Problem: measure height of a tree Solutions Chop it down Sun + shadow + trigonometry Photograph tree and yard stick; scaling All methods are valid and should yield similar results
53 How Is Flow Calculated? Kinetic modeling (various models) Basic principles Flow = (myocardial activity) (time activity of arterial blood pool) (extraction coefficient) PET is capable of measuring myocardial activity (M) and activity blood pool (A). Extraction coefficient of Rb-82 and N-13 calculated experimentally. F = M/(1 e -( F/F) )(A) for Rb-82. Different kinetic models have different assumptions for extraction coefficient and measurements of A. Yoshida K, et al. J Nucl Med. 1996;37(10):
54 Relative Imaging Activity Myocardial Activity Time (s)


55 Time-Activity Curves, Rb-82 Blood Pool Activity Activity Myocardial Activity Time (s)
 Vasquez AF, et al. JACC Cardiovasc Imaging.")
56 For Each Site Percent with Optimal Arterial Input (highest arterial input without spillover) Vasquez AF, et al. JACC Cardiovasc Imaging. 2013;6(5):
57 Arterial Input Function (Ao) Most SP automated selection typically at basal plane of LV and LA Some SP allows manual choice Best Ao could differ between stress and rest LA, left atrium; LV, left ventricle; SP, software package
58 2D vs 3D 3D >10Mcps (~30 mci, 1100 MBq), decline in accuracy and increased image noise from high randoms and dead-time factors At higher activities, the random rate becomes prohibitive in 3D Reduced dose of isotope required to obtain accurate input function Reduced dose reduces myocardial count density
59 Technical Requirements of Flow? Register attenuation/emission images 2D - Linear count recovery up to 3M cps 3D - Linear count recovery up to 12M cps and avoid scanner saturation from 1 st pass bolus (need for internal QC on all images) Selection and QC of input function Confirm not in or on LV LV, left ventricle; QC, quality control Gould KL, et al. J Am Coll Cardiol. 2013;62(18):
:402-412. Courtesy of K.")
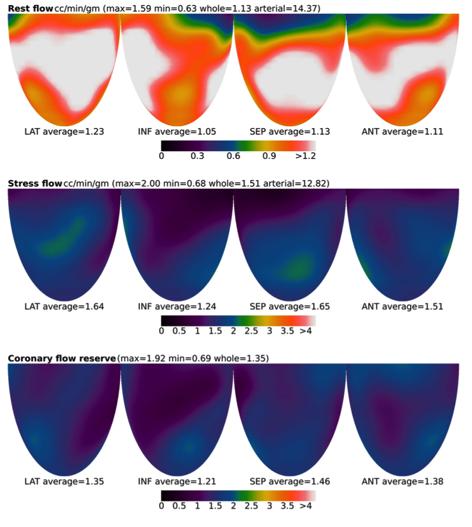
60 CFR in 1674 Rest Dipyridamole Quantitative PET Perfusion Images Based on data from Sdringola S, et al. JACC Cardiovasc Imaging. 2011;4(4): Courtesy of K. Lance Gould, MD.
61 Is My Software Correct? (assuming technical requirements are met) Sample 20 NORMAL patients. Young, no risk factors, no tobacco, screen for caffeine Resting flows should all be <1 cc/min/gm AND Stress flows should all be ~3.5 cc/min/gm CFR ~>4.3 Something is wrong if you do not get these values!
62 Is My Software Correct? (assuming technical requirements are met) Sample 20 ABNORMAL patients with definite ischemia (classic angina, perfusion abnormality, and cath-correlated disease) Low stress in ischemic zone should be <0.9 cc/min/gm with low CFR <1.74 Occluded vessels CFR <1.0 Something is wrong if you do not get these values!
 Tahari AK, et al. Eur J Nucl Med Mol Imaging.")
63 25 patients with low-to-intermediate probability of CAD 26 patients with known CAD 3 different software applications GE Discovery VCT PET/CT (2D mode, FBP) Tahari AK, et al. Eur J Nucl Med Mol Imaging. 2014;(1):

64 Tahari AK, et al. Eur J Nucl Med Mol Imaging. 2014;(1):
65 Tahari AK, et al. Eur J Nucl Med Mol Imaging. 2014;(1):
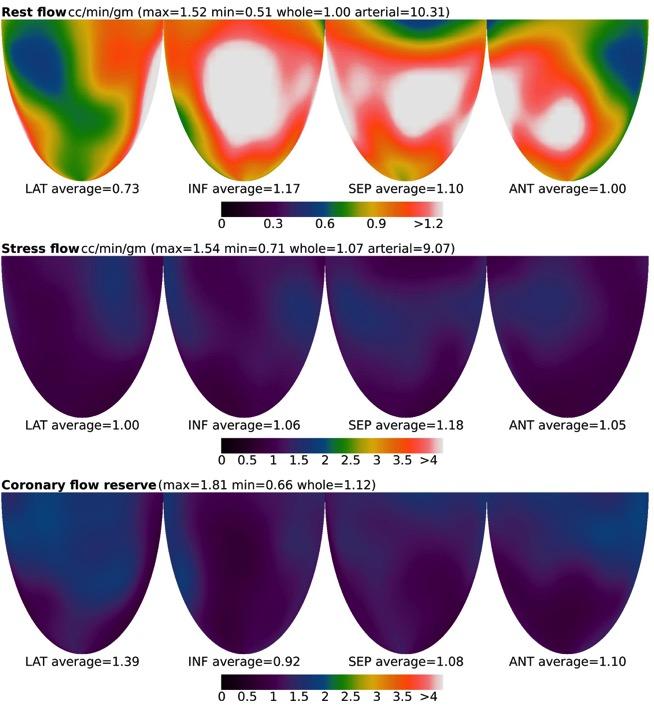
66 Measurement of Absolute Flow Requires blood pool and myocardial activity Extraction coefficient and kinetic modeling software Results typically in cc/min/g of myocardium Absolute flow measured at rest and stress (rmbf and smbf)
67 We Can Measure Flow Now What? What is normal? Is there a point where flow drops below metabolic demand? Is there a flow threshold that is associated with angina or ST depression? Is CFR or stress flow more important? CFR, coronary flow reserve
68 Conceptual Thresholds of Flow Causing Ischemia Percent or Number of Cases Flow Value(s)?? FLOW Stents/CABG Medical Therapy Courtesy of K. Lance Gould, MD.
69 Ischemic Thresholds for Flow CFR < CFR < CFR, coronary flow reserve Johnson NP, et al. JACC Cardiovasc Imaging. 2011;4(9):


70 Conceptual Thresholds of Flow Causing Ischemia Percent or Number of Cases Stress flow 0.9 cc/min/g and CFR of 1.7 FLOW Stents/CABG Medical Therapy Courtesy of K. Lance Gould, MD.
:430-440.")
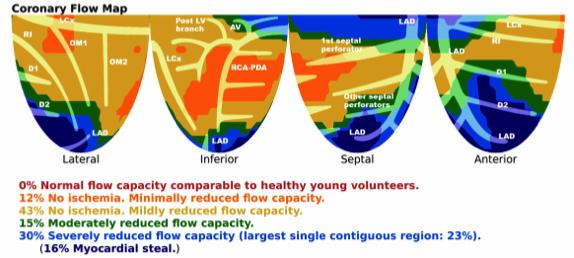
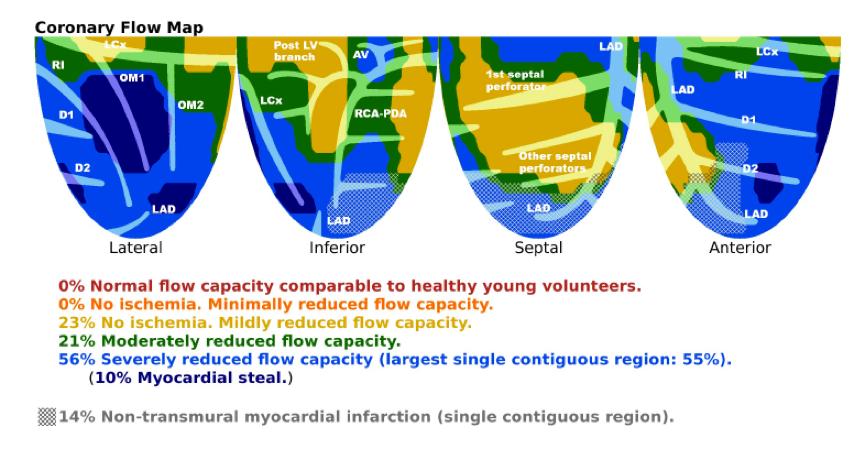
71 Coronary Flow Capacity Johnson NP, et al. JACC Cardiovasc Imaging. 2012;5(4):
:1670-1680.")
72 Invasive Coronary Flow Capacity Map van de Hoef TP, et al. JACC Cardiovasc Interv. 2015;8(13):
73 Scatter Plot of Invasive Flow Data Across the Coronary Flow Capacity Concept van de Hoef TP, et al. JACC Cardiovasc Interv. 2015;8(13):

74 Scatter Plots of Fractional Flow Reserve Across Map of Coronary Flow Capacity van de Hoef TP, et al. JACC Cardiovasc Interv. 2015;8(13):
75 Risk of Major Adverse Cardiac Events According to Coronary Flow Capacity Strata van de Hoef TP, et al. JACC Cardiovasc Interv. 2015;8(13):

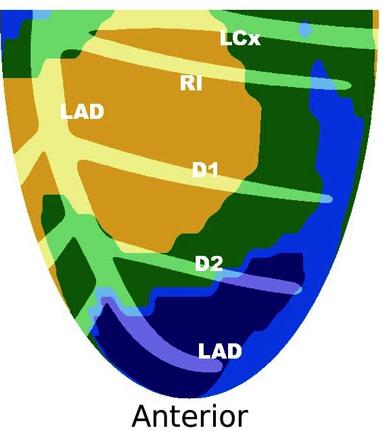
76 Left Ventricular Quadrants in Cardiac PET Johnson NP, et al. JACC Cardiovasc Imaging. 2011;5(4):
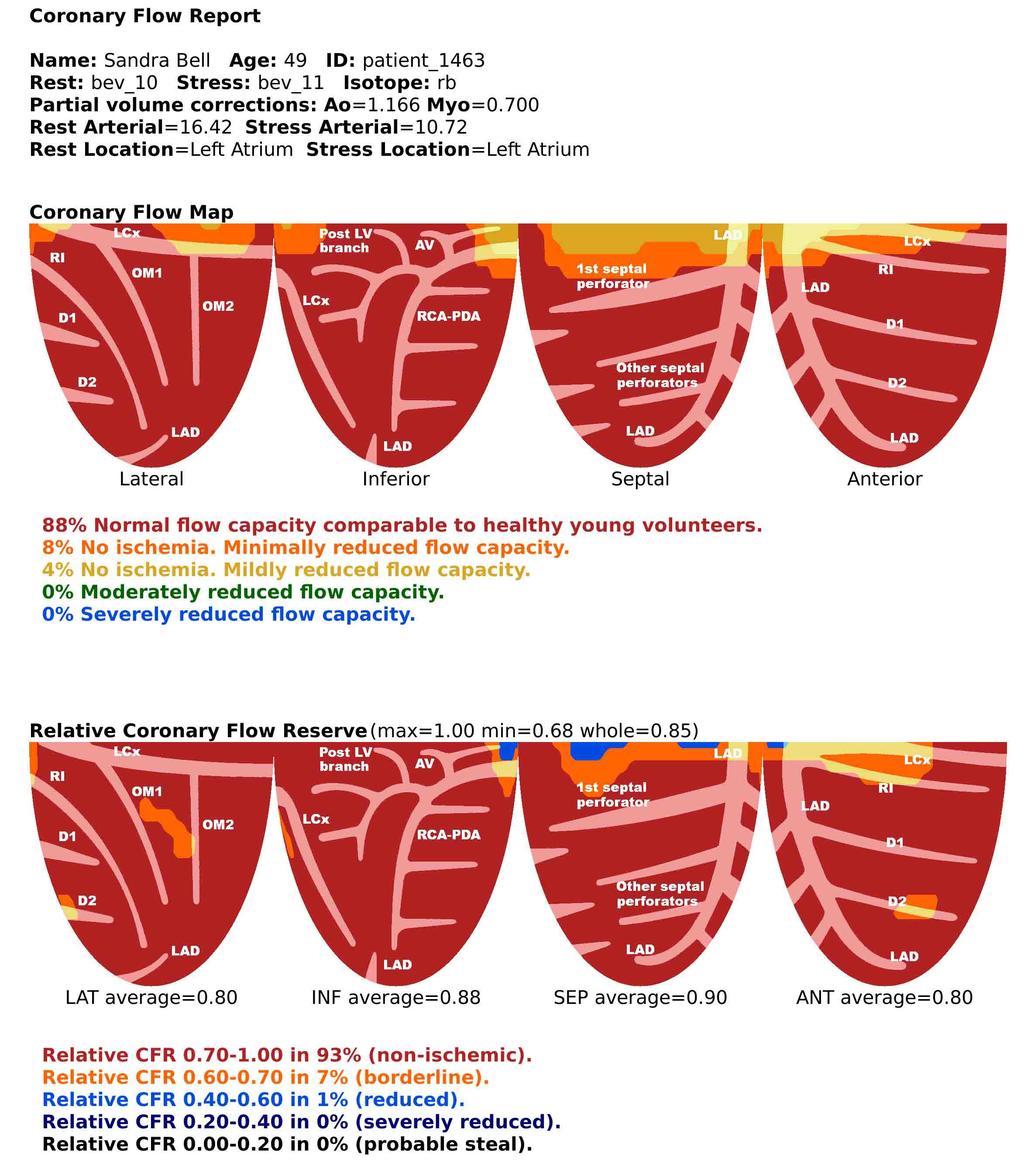
77 Case 1 49-year-old female admitted for chest pain Diabetes mellitus, hypertension, and tobacco use BP 173/109 mm Hg Troponin negative ECG sinus rhythm, no acute ST changes

78 Case 1 AV, atrioventricular; D1, first diagonal branch; D2, second diagonal branch; LAD, left anterior descending artery; LCx, left circumflex artery; LV, left ventricular; OM1, first obtuse marginal branch; OM2, second obtuse marginal branch; PDA, posterior descending artery; RI, ramus intermedius

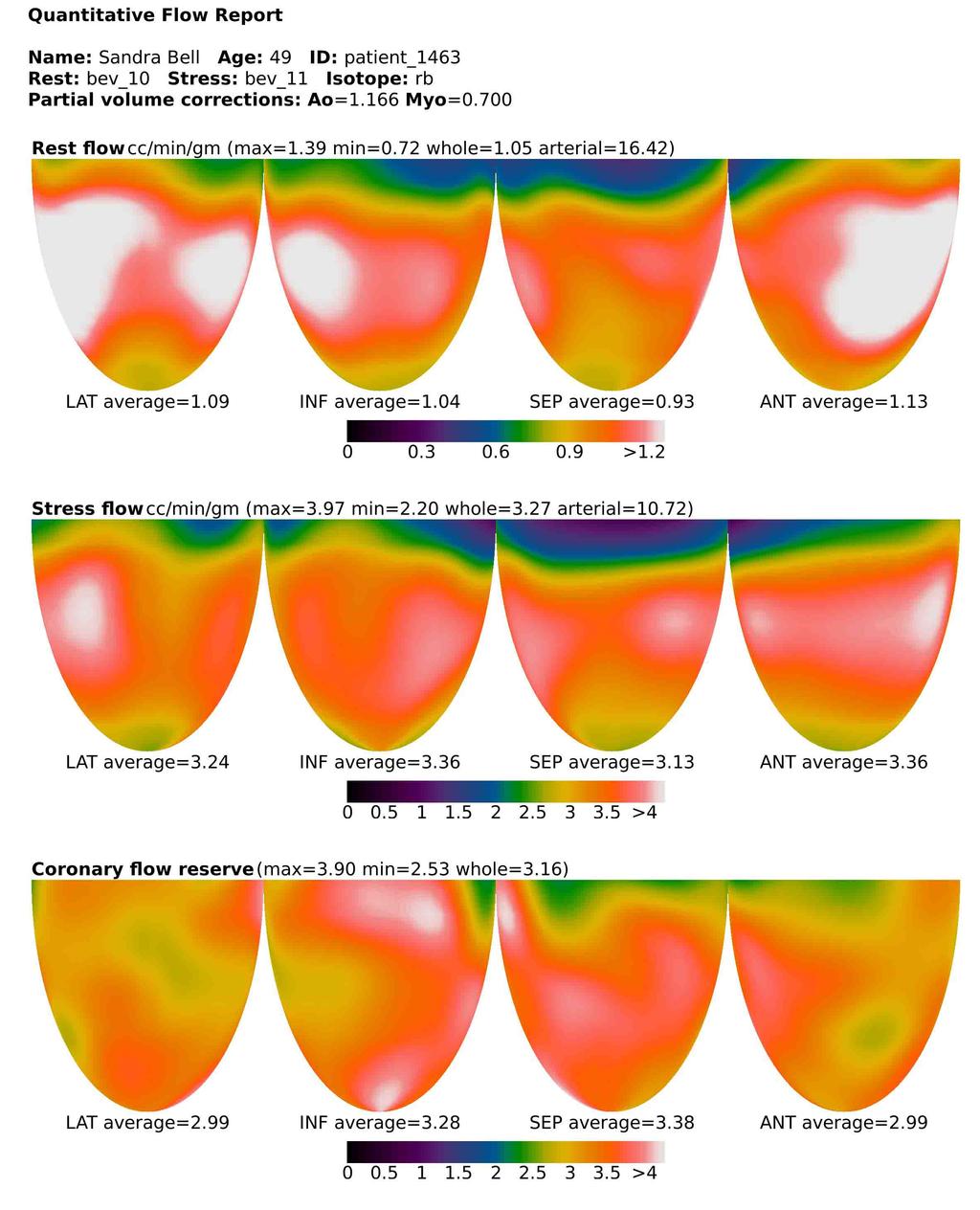
79 Case 1
80 Case 1
81 Case 5 65-year-old woman with chest pain in ED BP 170/110 mm Hg Tobacco use, hypertension, unknown lipids, denies diabetes mellitus ECG left ventricular hypertrophy with strain Troponin borderline ED, emergency department.
82 Case 5
83 Case 5
84 Case 5
85 Case 6 44-year-old woman transferred for TMR for lifestyle-limiting angina h/o: >5 PCIs, 5-vessel CABG, 4/5 grafts occluded Known RCA and LCX occlusion Patent SVG jump to OM1-OM2 Patient arrived and PCI of LAD was performed Angina walking to bathroom later that PM CABG, coronary artery bypass graft; TMR, transmyocardial revascularization; LAD, left anterior descending artery; SVG, saphenous vein graft.
86 Case 6
87 Case 6
88 Case 6
89 Case 7 87-year-old man with chest pain and SOB Found to be in atrial fibrillation with RVR Hypertension, hyperlipidemia, diabetes mellitus Troponin 3.5 Beta-blockers à converted to sinus LHC occluded RCA and 3VD referred for CABG PET requested for 2nd opinion by patient RVR, rapid ventricular response; 3VD, three-vessel disease.
90 Case 7
91 Case 7

92 Case 7
 smbf no change (2.0±0.6 vs 1.9±0.7 cc/min/g, p=0.7). Bober, R, The Effect of Coronary Revascularization on Regional Myocardial Blood Flow.")
93 Defect, Interven1on No Defect, Interven1on No Defect, No Interven1on Increased 0.6±0.7 cc/min/g (1.2±0.4 vs 1.7±0.8, p<0.001). smbf no change (1.7±0.3 vs 1.5±0.4 cc/min/g, p=0.16) smbf no change (2.0±0.6 vs 1.9±0.7 cc/min/g, p=0.7). Bober, R, The Effect of Coronary Revascularization on Regional Myocardial Blood Flow. J Nucl Cardiol. 2016
94 Cardiac PET With Flow Reserve Measuring the Effects of Revascularization 65-year-old man History of HTN, DM, CAD s/p CABG LIMA to LAD, SVG to PLB, and SVG to OM2 PET to assess symptoms of exertional dyspnea Angiogram with 2-vessel PCI performed No change in symptoms Repeat PET PET, positron emission tomography; HTN, hypertension; DM, diabetes mellitus; CAD, coronary artery disease; s/p, status post; CABG, coronary artery bypass graft; LIMA, left internal mammary artery; LAD, left anterior descending artery; SVG, saphenous vein graft; PLB, posterolateral branch; OM2, second obtuse marginal branch; PCI, percutaneous coronary intervention.



95 PET Prior to PCI PET 4 weeks after PCI SUCCESS?? Bober R, et al. Progress in Cardiovascular Diseases, 2015;57(6):

96 PET Prior to PCI PET 4 weeks after PCI NO BENEFIT (at best)
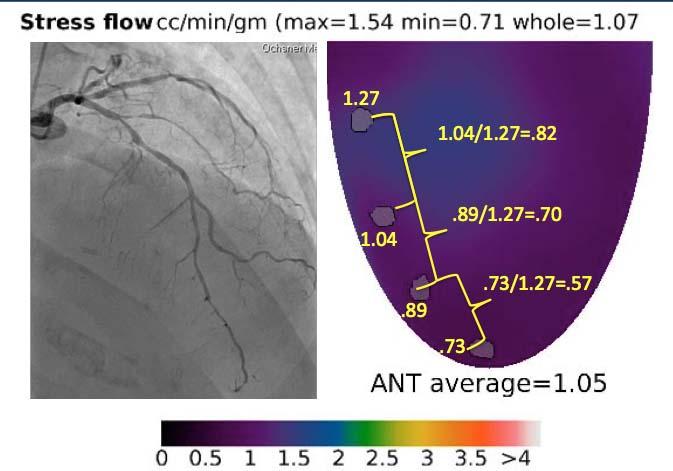
97 Case # 65 y/o female presented with NSTEMI Occluded high OM (culprit) PCI, high grade disease in PDA and proximal LAD medically managed CP recurred in ~ 1 week Returned and underwent LHC Prox LAD FFR =.82 Therefore PCI of PDA Continued with angina

98 Case #
99 Case
100
101



102 /1.27= /1.27= /1.27=.57

103
104 LE y/o man with HTN, HPL, DM, tobacco use, Hep C, CKD Initial SPECT 5-12 for DOE and CP fixed defect base to mid inferior wall Normal wall motion on gated SPECT and ECHO Interpreted as likely diaphragm attenuation Medically managed Second SPECT 8-14 for DOE and fatigue Fixed defect base to distal inferior wall Abnormal inferior wall motion (low normal LVEF) Interpreted as infarct with peri-infarct ischemia Medically optimized. No LHC as patients sxs improved and no angina

105 LE SPECT
106 LE SPECT
107 LE Was CP free for ~ 3 years however started to develop exertional CP and worsening DOE Opted for repeat stress for risk stratification over LHC. SPECT interpreted as no change since 2014 however, in this patient with angina and a known fixed perfusion abnormality, SPECT scanning with Tc-99 based isotopes can misclassify ischemic tissue as infarction (based on the flow properties of Tc-99 and tissue attenuation) Consider PET stress testing with absolute flow. PET stress flow obtained

108 LE SPECT
109 LE Review of 2014 and 2015 SPECTS

110 Preview of 2014 and 2015 SPECTS

111 LE PET
112 LE PET
113 LE PET Flows

114 LE PET Flow Capacity
115 LE Summary SPECTS All with FIXED (rest and stress) inferior wall defects 2012 thought to be attenuation thought to be secondary to CAD (infarct) PET No resting defect à no infarction Ischemic flows in RCA and LCX territory LAD flows not normal however, not ischemic Presence of disease expected Not flow limiting LHC- High grade disease in OM1 and RCA Mild/moderate distal LAD disease
116 Polling Question When comparing the difference between photons of SPECT and PET tracers, the true statement regarding SPECT photons: a) Are emitted at ~ 511KeV b) Are emitted as single photons c) Attenuation is independent of the point of origin along the Line of Response d) Are higher energy than PET photons GB Saha, Basics of Pet Imaging
117 Polling Question Coronary Flow Reserve (CFR) is: a) Absolute hyperemic flow minus absolute resting flow b) Absolute resting flow minus absolute hyperemic flow c) The ratio of absolute hyperemic flow to absolute resting flow d) The ratio of absolute resting flow to hyperemic flow Gould KL, et al. Am J Cardiol. 1974;33(1):87-94.
118 Polling Question The estimated effective dose of radiation for cardiac PET rest/stress study with Rb-82 is: a) 10 msv b) <5 msv c) msv d) 6-9 msv Einstein AJ. J Am Coll Cardiol. 2012;59(6):
119 Polling Question Under normal conditions, what is the major resistance to coronary flow? a) Myocardial microvasculature b) Sympathetic nervous system c) Epicardial vessel d) Diastolic filling time Gould KL. Circ Res. 1985;57(3):
120 Polling Question Identify the true statement regarding Coronary Flow Capacity a) Is the integration of both CFR and absolute myocardial stress flow due to a combination of discrete, diffuse and microvascular disease. b) Is the ratio of stress to resting myocardial blood flow. c) Is dependent on patient BMI (body mass index). d) Doesn t not fluctuate within an individual. Johnson NP, et al. JACC Cardiovasc Imaging. 2012;5(4):
Advantages of PET Myocardial Imaging
 Advantages of PET Myocardial Imaging Legal Disclaimers These materials were prepared in good faith by MITA as a service to the profession and are believed to be reliable based on current scientific literature.
Advantages of PET Myocardial Imaging Legal Disclaimers These materials were prepared in good faith by MITA as a service to the profession and are believed to be reliable based on current scientific literature.
Conflict of Interest Disclosure
 Comparative Advantages of PET Over SPECT: Is PET Really Better? Timothy M. Bateman M.D. Co-Director, Cardiovascular Radiologic Imaging Mid America Heart Institute Professor of Medicine University of Missouri-Kansas
Comparative Advantages of PET Over SPECT: Is PET Really Better? Timothy M. Bateman M.D. Co-Director, Cardiovascular Radiologic Imaging Mid America Heart Institute Professor of Medicine University of Missouri-Kansas
Nuclear Cardiology Cardiac Myocardial Perfusion with 82 Rb. Dominique Delbeke, MD, PhD Vanderbilt University Medical Center Nashville, TN
 Nuclear Cardiology Cardiac Myocardial Perfusion with 82 Rb Dominique Delbeke, MD, PhD Vanderbilt University Medical Center Nashville, TN VUMC PET/CT conference 2009 82 Rb Cardiac Perfusion PET 82 Rb is
Nuclear Cardiology Cardiac Myocardial Perfusion with 82 Rb Dominique Delbeke, MD, PhD Vanderbilt University Medical Center Nashville, TN VUMC PET/CT conference 2009 82 Rb Cardiac Perfusion PET 82 Rb is
Pearls & Pitfalls in nuclear cardiology
 Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
FFR Incorporating & Expanding it s use in Clinical Practice
 FFR Incorporating & Expanding it s use in Clinical Practice Suleiman Kharabsheh, MD Consultant Invasive Cardiology Assistant professor, Alfaisal Univ. KFHI - KFSHRC Concept of FFR Maximum flow down a vessel
FFR Incorporating & Expanding it s use in Clinical Practice Suleiman Kharabsheh, MD Consultant Invasive Cardiology Assistant professor, Alfaisal Univ. KFHI - KFSHRC Concept of FFR Maximum flow down a vessel
Fractional Flow Reserve: Basics, FAME 1, FAME 2. William F. Fearon, MD Associate Professor Stanford University Medical Center
 Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
SPECT or PET for Cardiovascular Screening in High-Risk Patients
 SPECT or PET for Cardiovascular Screening in High-Risk Patients Paeng, Jin Chul MD PhD Department of Nuclear Medicine Seoul National University Hospital Contents Recent Development in SPECT and PET Technology
SPECT or PET for Cardiovascular Screening in High-Risk Patients Paeng, Jin Chul MD PhD Department of Nuclear Medicine Seoul National University Hospital Contents Recent Development in SPECT and PET Technology
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Debate Should we use FFR? I will say NO.
 Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
Debate Should we use FFR? I will say NO. Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol Gwon Research fund from Abbott Korea
FFR in Multivessel Disease
 FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
Conflict of Interest Disclosure
 Challenges and Opportunities for SPECT & PET in 2013: Implementing Latest Acquisition and Processing Protocols Timothy M. Bateman M.D. Co-Director, Cardiovascular Radiologic Imaging Mid America Heart Institute
Challenges and Opportunities for SPECT & PET in 2013: Implementing Latest Acquisition and Processing Protocols Timothy M. Bateman M.D. Co-Director, Cardiovascular Radiologic Imaging Mid America Heart Institute
Myocardial Perfusion: Positron Emission Tomography
 Myocardial Perfusion: Positron Emission Tomography TH. Schindler, MD University Hospitals of Geneva, Cardiovascular Center, Geneva, Switzerland ESC 2010 Stockholm Personal Disclosure Research Grant support
Myocardial Perfusion: Positron Emission Tomography TH. Schindler, MD University Hospitals of Geneva, Cardiovascular Center, Geneva, Switzerland ESC 2010 Stockholm Personal Disclosure Research Grant support
PET for the Evaluation of Myocardial Viability
 PET for the Evaluation of Myocardial Viability Myocardial viability assessment is an important part of cardiac PET to assist physicians to decide upon the best surgical or medical procedures. F-18 FDG
PET for the Evaluation of Myocardial Viability Myocardial viability assessment is an important part of cardiac PET to assist physicians to decide upon the best surgical or medical procedures. F-18 FDG
Abnormal, Autoquant Adenosine Myocardial Perfusion Heart Imaging. ID: GOLD Date: Age: 46 Sex: M John Doe Phone (310)
") Background: Reason: preoperative assessment of CAD, Shortness of Breath Symptom: atypical chest pain Risk factors: hypertension Under influence: a beta blocker Medications: digoxin Height: 66 in. Weight:
Background: Reason: preoperative assessment of CAD, Shortness of Breath Symptom: atypical chest pain Risk factors: hypertension Under influence: a beta blocker Medications: digoxin Height: 66 in. Weight:
PCIs on Intermediate Lesions NCDR Cath-PCI Registry
 Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Hybrid cardiac imaging Advantages, limitations, clinical scenarios and perspectives for the future
 Hybrid cardiac imaging Advantages, limitations, clinical scenarios and perspectives for the future Prof. Juhani Knuuti, MD, FESC Turku, Finland Disclosure: Juhani Knuuti, M.D. Juhani Knuuti, M.D. has financial
Hybrid cardiac imaging Advantages, limitations, clinical scenarios and perspectives for the future Prof. Juhani Knuuti, MD, FESC Turku, Finland Disclosure: Juhani Knuuti, M.D. Juhani Knuuti, M.D. has financial
FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!!
 FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!! Juan Antonio Pastor-Cervantes,M.D FSCAI, FACC Cardiovascular Institute Memorial Regional Hospital Hollywood Florida
FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!! Juan Antonio Pastor-Cervantes,M.D FSCAI, FACC Cardiovascular Institute Memorial Regional Hospital Hollywood Florida
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
Fractional Flow Reserve and instantaneous wave -free Ratio. Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου
 Fractional Flow Reserve and instantaneous wave -free Ratio Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου DISCLOSURES There are no financial conflicts of interest relevant to this presentation
Fractional Flow Reserve and instantaneous wave -free Ratio Λάμπρος Κ. Μόσιαλος Επεμβατικός Καρδιολόγος ΓΝ Παπαγεωργίου DISCLOSURES There are no financial conflicts of interest relevant to this presentation
New Insight about FFR and IVUS MLA
 New Insight about FFR and IVUS MLA Can IVUS MLA Predict FFR
New Insight about FFR and IVUS MLA Can IVUS MLA Predict FFR
Fractional Flow Reserve from Coronary CT Angiography (and some neat CT images)
") Fractional Flow Reserve from Coronary CT Angiography (and some neat CT images) Victor Cheng, M.D. Director, Cardiovascular CT Oklahoma Heart Institute 1 Disclosures Tornadoes scare me 2 Treating CAD Fixing
Fractional Flow Reserve from Coronary CT Angiography (and some neat CT images) Victor Cheng, M.D. Director, Cardiovascular CT Oklahoma Heart Institute 1 Disclosures Tornadoes scare me 2 Treating CAD Fixing
Multisclice CT in combination with functional imaging for CAD. Temporal Resolution. Spatial Resolution. Temporal resolution = ½ of the rotation time
 Multisclice CT in combination with functional imaging for CAD Prof. Juhani Knuuti, MD, FESC Turku University Hospital and University of Turku Turku, Finland MSCT and functional imaging for CAD Practical
Multisclice CT in combination with functional imaging for CAD Prof. Juhani Knuuti, MD, FESC Turku University Hospital and University of Turku Turku, Finland MSCT and functional imaging for CAD Practical
Instantaneous Wave-Free Ratio
 Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Management of stable CAD FFR guided therapy: the new gold standard
 Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Fractional Flow Reserve. A physiological approach to guide complex interventions
 Fractional Flow Reserve A physiological approach to guide complex interventions What is FFR? Fractional Flow Reserve (FFR) is a lesion specific, physiological index determining the hemodynamic severity
Fractional Flow Reserve A physiological approach to guide complex interventions What is FFR? Fractional Flow Reserve (FFR) is a lesion specific, physiological index determining the hemodynamic severity
Hospital, 6 Lukon Road, Lukong Town, Changhua Shien, Taiwan 505, Taiwan.
 Volume 1, Issue 1 Image Article Resolution of Inferior Wall Ischemia after Successful Revascularization of LAD Lesion: The Value of Myocardial Perfusion Imaging in Guiding Management of Multi-vessel CAD
Volume 1, Issue 1 Image Article Resolution of Inferior Wall Ischemia after Successful Revascularization of LAD Lesion: The Value of Myocardial Perfusion Imaging in Guiding Management of Multi-vessel CAD
CLINICAL CONSEQUENCES OF THE
 CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
FRACTIONAL FLOW RESERVE: STANDARD OF CARE
 FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
New Challenges in Nuclear Cardiology Practice
 New Challenges in Nuclear Cardiology Practice Brian G. Abbott, MD, FACC, FASNC, FAHA President, ASNC 2016 Associate Professor of Medicine Warren Alpert Medical School of Brown University Director, Cardiovascular
New Challenges in Nuclear Cardiology Practice Brian G. Abbott, MD, FACC, FASNC, FAHA President, ASNC 2016 Associate Professor of Medicine Warren Alpert Medical School of Brown University Director, Cardiovascular
CASE from South Korea
 CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
CT or PET/CT for coronary artery disease
 CT or PET/CT for coronary artery disease Rotterdam 2012 Juhani Knuuti, MD, PhD, FESC Turku PET Centre University of Turku Turku, Finland Juhani.knuuti@utu.fi Turku PET Centre University of Turku Åbo Akademi
CT or PET/CT for coronary artery disease Rotterdam 2012 Juhani Knuuti, MD, PhD, FESC Turku PET Centre University of Turku Turku, Finland Juhani.knuuti@utu.fi Turku PET Centre University of Turku Åbo Akademi
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines
 Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
How to Evaluate Microvascular Function and Angina. Myeong-Ho Yoon Ajou University Hospital
 How to Evaluate Microvascular Function and Angina Myeong-Ho Yoon Ajou University Hospital Angina without Coronary Artery Disease (CAD) Prevalence: 20-30% going c-angiography, with a higher prevalence (almost
How to Evaluate Microvascular Function and Angina Myeong-Ho Yoon Ajou University Hospital Angina without Coronary Artery Disease (CAD) Prevalence: 20-30% going c-angiography, with a higher prevalence (almost
Form 4: Coronary Evaluation
 Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one. Angio NOT DONE: n invasive test performed Followup
Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one. Angio NOT DONE: n invasive test performed Followup
Fractional Flow Reserve and the Results of the FAME Study
 Imaging and Physiology Summit Seoul, Korea November 21 st, 2009 Fractional Flow Reserve and the Results of the FAME Study William F. Fearon, M.D. Assistant Professor Division of Cardiovascular Medicine
Imaging and Physiology Summit Seoul, Korea November 21 st, 2009 Fractional Flow Reserve and the Results of the FAME Study William F. Fearon, M.D. Assistant Professor Division of Cardiovascular Medicine
SPECT-CT: Τι πρέπει να γνωρίζει ο Καρδιολόγος
 SPECT-CT: Τι πρέπει να γνωρίζει ο Καρδιολόγος Δρ Αναστασία Κίτσιου Διευθύντρια, Καρδιολογική Κλινική, Σισμανόγλειο ΓΝΑ Chair, Education Committee, Section on Nuclear Cardiology & Cardiac CT, EACVI, ESC
SPECT-CT: Τι πρέπει να γνωρίζει ο Καρδιολόγος Δρ Αναστασία Κίτσιου Διευθύντρια, Καρδιολογική Κλινική, Σισμανόγλειο ΓΝΑ Chair, Education Committee, Section on Nuclear Cardiology & Cardiac CT, EACVI, ESC
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Form 4: Coronary Evaluation
 Patient Details Hidden Show Show/Hide Annotations Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one.
Patient Details Hidden Show Show/Hide Annotations Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one.
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Does Coronary Flow Trump Coronary Anatomy?
 JACC: CARDIOVASCULAR IMAGING VOL. 2, NO. 8, 29 29 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-878X/9/$36. PUBLISHED BY ELSEVIER INC. DOI:1.116/j.jcmg.29.6.4 STATE-OF-THE-ART PAPER Does Coronary
JACC: CARDIOVASCULAR IMAGING VOL. 2, NO. 8, 29 29 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-878X/9/$36. PUBLISHED BY ELSEVIER INC. DOI:1.116/j.jcmg.29.6.4 STATE-OF-THE-ART PAPER Does Coronary
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
Je bénéficie régulièrement de fonds privés, dans le cadre de projets de recherche ou d activités de formation.
 Je bénéficie régulièrement de fonds privés, dans le cadre de projets de recherche ou d activités de formation. Ces fonds proviennent essentiellement d industriels travaillant dans les domaines de l imagerie
Je bénéficie régulièrement de fonds privés, dans le cadre de projets de recherche ou d activités de formation. Ces fonds proviennent essentiellement d industriels travaillant dans les domaines de l imagerie
FFR-CT Not Ready for Primetime
 FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
Welcome! To submit questions during the presentation: or Text:
 Welcome! To participate in the interactive Q & A please do the following: 1. Download the Socrative Student App 2. Enter Teacher s Room Code: ZD0F3X5Q 3. Select Quiz: Intermountain Cardiac Stress Testing
Welcome! To participate in the interactive Q & A please do the following: 1. Download the Socrative Student App 2. Enter Teacher s Room Code: ZD0F3X5Q 3. Select Quiz: Intermountain Cardiac Stress Testing
REVIEW. A precise, three-dimensional atlas of myocardial perfusion correlated with coronary arteriographic anatomy
 REVIEW A precise, three-dimensional atlas of myocardial perfusion correlated with coronary arteriographic anatomy Yuko Nakagawa, MD, a Keiichi Nakagawa, MD, b Stefano Sdringola, MD, c,d Nizar Mullani,
REVIEW A precise, three-dimensional atlas of myocardial perfusion correlated with coronary arteriographic anatomy Yuko Nakagawa, MD, a Keiichi Nakagawa, MD, b Stefano Sdringola, MD, c,d Nizar Mullani,
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Which Test When? Avoid the Stress of Stress Testing. Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute
 Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Case report. Resistance in the cath lab : the utility of hyperemic stenosis resistance in the functional assessment of coronary artery disease
 Resistance in the cath lab : the utility of hyperemic stenosis resistance in the functional assessment of coronary artery disease Kalpa De Silva, Divaka Perera Cardiovascular Division, The Rayne Institute,
Resistance in the cath lab : the utility of hyperemic stenosis resistance in the functional assessment of coronary artery disease Kalpa De Silva, Divaka Perera Cardiovascular Division, The Rayne Institute,
Controversies in Coronary Revascularization. Atlanta CCU April 15, 2016
 Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium. Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute
 Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
CARDIAC PET PERFUSION IMAGING with RUBIDIUM-82
 CARDIAC PET PERFUSION IMAGING with RUBIDIUM-82 Pr Denis AGOSTINI Président du Groupe de Cardiologie Nucléaire et IRM CHU Caen Bordeaux 2006 Cardiac Perfusion-Metabolism Mismatch with PET Cumulative Survival
CARDIAC PET PERFUSION IMAGING with RUBIDIUM-82 Pr Denis AGOSTINI Président du Groupe de Cardiologie Nucléaire et IRM CHU Caen Bordeaux 2006 Cardiac Perfusion-Metabolism Mismatch with PET Cumulative Survival
ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE
 ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE Angioplasty Summit TCT ASIA Seoul, Korea, april 24th, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands A rather common
ROLE OF CORONARY PRESSURE & FFR IN MULTIVESSEL DISEASE Angioplasty Summit TCT ASIA Seoul, Korea, april 24th, 2008 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands A rather common
Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures?
 Keenan Research Centre Li Ka Shing Knowledge Institute Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures? Howard Leong-Poi, MD, FRCPC Associate Professor of Medicine St.
Keenan Research Centre Li Ka Shing Knowledge Institute Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures? Howard Leong-Poi, MD, FRCPC Associate Professor of Medicine St.
Coronary Artery Imaging. Suvipaporn Siripornpitak, MD Inter-hospital Conference : Rajavithi Hospital
 Coronary Artery Imaging Suvipaporn Siripornpitak, MD Inter-hospital Conference : Rajavithi Hospital Larger array : cover scan area Detector size : spatial resolution Rotation speed : scan time Retrospective
Coronary Artery Imaging Suvipaporn Siripornpitak, MD Inter-hospital Conference : Rajavithi Hospital Larger array : cover scan area Detector size : spatial resolution Rotation speed : scan time Retrospective
Fractional Flow Reserve: Review of the latest data
 Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Case Presentation #1
 Case Presentation #1 SCAI Fellows Course December 7, 2013 Barry F Uretsky, MD University of Arkansas for Medical Sciences Central Arkansas Veterans Health System Little Rock, AR Case Presentation #1 65
Case Presentation #1 SCAI Fellows Course December 7, 2013 Barry F Uretsky, MD University of Arkansas for Medical Sciences Central Arkansas Veterans Health System Little Rock, AR Case Presentation #1 65
Qualitative and Quantitative Assessment of Perfusion
 APCDE 2011 Qualitative and Quantitative Assessment of Perfusion Hyun Ju Yoon Chonnam National University Hospital Gwangju, Korea ISCHEMIC CASCADE Blood flow mismatch Perfusion defects on nuclear imaging,
APCDE 2011 Qualitative and Quantitative Assessment of Perfusion Hyun Ju Yoon Chonnam National University Hospital Gwangju, Korea ISCHEMIC CASCADE Blood flow mismatch Perfusion defects on nuclear imaging,
1. LV function and remodeling. 2. Contribution of myocardial ischemia due to CAD, and
 1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
Technical Aspects and Clinical Indications of FFR
 Technical Aspects and Clinical Indications of FFR Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst - OLV Clinic Aalst, Belgium Potential conflicts of interest Consulting fees and honoraria on
Technical Aspects and Clinical Indications of FFR Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst - OLV Clinic Aalst, Belgium Potential conflicts of interest Consulting fees and honoraria on
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Gated blood pool ventriculography: Is there still a role in myocardial viability?
 Gated blood pool ventriculography: Is there still a role in myocardial viability? Oliver C. Alix, MD Adult Clinical and Nuclear Cardiology St. Luke s Medical Centre - Global City Case Presentation A 62-year-old
Gated blood pool ventriculography: Is there still a role in myocardial viability? Oliver C. Alix, MD Adult Clinical and Nuclear Cardiology St. Luke s Medical Centre - Global City Case Presentation A 62-year-old
FFR= Qs/Qn. Ohm s law R= P/Q Q=P/R
 32 ο Πανελλήνιο Καρδιολογικό Συνζδριο, Θεσσαλονίκη 20/10/2011 Gould KL et al, JACC CARDIOVASC IMAG 2009 Gould KL et al AM J CARDIOL 1974 & JACC CARDIOVASC IMAG 2009 Under maximal hyperemia: Rs=Rn FFR=
32 ο Πανελλήνιο Καρδιολογικό Συνζδριο, Θεσσαλονίκη 20/10/2011 Gould KL et al, JACC CARDIOVASC IMAG 2009 Gould KL et al AM J CARDIOL 1974 & JACC CARDIOVASC IMAG 2009 Under maximal hyperemia: Rs=Rn FFR=
Radiologic Assessment of Myocardial Viability
 November 2001 Radiologic Assessment of Myocardial Viability Joshua Moss, Harvard Medical School Year III Patient EF 66yo female with a 3-year history of intermittent chest pain previously relieved by sublingual
November 2001 Radiologic Assessment of Myocardial Viability Joshua Moss, Harvard Medical School Year III Patient EF 66yo female with a 3-year history of intermittent chest pain previously relieved by sublingual
Σεμινάριο Ομάδων Εργασίας Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική
 Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική") ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome
 Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Imaging congestive heart failure: role of coronary computed tomography angiography (CCTA)
") Imaging congestive heart failure: role of coronary computed tomography angiography (CCTA) Gianluca Pontone, MD, PhD, FESC, FSCCT Director of MR Unit Deputy Director of Cardiovascul CT Unit Clinical Cardiology
Imaging congestive heart failure: role of coronary computed tomography angiography (CCTA) Gianluca Pontone, MD, PhD, FESC, FSCCT Director of MR Unit Deputy Director of Cardiovascul CT Unit Clinical Cardiology
Validation of CT Perfusion Imaging Against Invasive Angiography and FFR on a 320-MDCT Scanner
 Validation of CT Perfusion Imaging Against Invasive Angiography and FFR on a 320-MDCT Scanner Zhen Qian, Gustavo Vasquez, Sarah Rinehart, Parag Joshi, Eric Krivitsky, Anna Kalynych, Dimitri Karmpaliotis,
Validation of CT Perfusion Imaging Against Invasive Angiography and FFR on a 320-MDCT Scanner Zhen Qian, Gustavo Vasquez, Sarah Rinehart, Parag Joshi, Eric Krivitsky, Anna Kalynych, Dimitri Karmpaliotis,
Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center
 CMR Perfusion and Viability A STICH Out of Time? Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center Can Imaging Improve
CMR Perfusion and Viability A STICH Out of Time? Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center Can Imaging Improve
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
FFR-Guided PCI. 4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea. Stanford
 4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea FFR-Guided PCI William F. Fearon, M.D. Associate Professor Division of Cardiovascular Medicine University Medical Center Disclosure Statement
4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea FFR-Guided PCI William F. Fearon, M.D. Associate Professor Division of Cardiovascular Medicine University Medical Center Disclosure Statement
Typical chest pain with normal ECG
 Typical chest pain with normal ECG F. Mut, C. Bentancourt, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history Male 41 y.o. Overweight, hypertension, high cholesterol,
Typical chest pain with normal ECG F. Mut, C. Bentancourt, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history Male 41 y.o. Overweight, hypertension, high cholesterol,
Photon Attenuation Correction in Misregistered Cardiac PET/CT
 Photon Attenuation Correction in Misregistered Cardiac PET/CT A. Martinez-Möller 1,2, N. Navab 2, M. Schwaiger 1, S. G. Nekolla 1 1 Nuklearmedizinische Klinik der TU München 2 Computer Assisted Medical
Photon Attenuation Correction in Misregistered Cardiac PET/CT A. Martinez-Möller 1,2, N. Navab 2, M. Schwaiger 1, S. G. Nekolla 1 1 Nuklearmedizinische Klinik der TU München 2 Computer Assisted Medical
Myocardial Perfusion SPECT How to do it E. Moralidis
 Myocardial Perfusion SPECT How to do it E. Moralidis Aristotelian University AHEPA Hospital Thessaloniki Myocardial perfusion SPECT procedure Stress Imaging Data analysis and reporting Myocardial perfusion
Myocardial Perfusion SPECT How to do it E. Moralidis Aristotelian University AHEPA Hospital Thessaloniki Myocardial perfusion SPECT procedure Stress Imaging Data analysis and reporting Myocardial perfusion
Update in Nuclear Cardiology: Patient-Centered Imaging Radiation Dose Reduction
 Update in Nuclear Cardiology: Patient-Centered Imaging Radiation Dose Reduction E. Gordon DePuey, M.D. Icahn School of Medicine ant Mt. Sinai New York, NY Disclosures: Grant Support: Michael J. Fox Foundation
Update in Nuclear Cardiology: Patient-Centered Imaging Radiation Dose Reduction E. Gordon DePuey, M.D. Icahn School of Medicine ant Mt. Sinai New York, NY Disclosures: Grant Support: Michael J. Fox Foundation
Clinical Appropriateness Guidelines: Percutaneous Coronary Intervention
 Clinical Appropriateness Guidelines: Percutaneous Coronary Intervention Appropriate Use Criteria Effective Date: January 2, 2018 Proprietary Date of Origin: 08/27/2015 Last revised: 08/01/2017 Last reviewed:
Clinical Appropriateness Guidelines: Percutaneous Coronary Intervention Appropriate Use Criteria Effective Date: January 2, 2018 Proprietary Date of Origin: 08/27/2015 Last revised: 08/01/2017 Last reviewed:
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Myocardial perfusion scintigraphy using rubidium-82 positron emission tomography
 Published Online August 21, 2013 Myocardial perfusion scintigraphy using rubidium-82 positron emission tomography Parthiban Arumugam *, Deborah Tout, and Christine Tonge Nuclear Medicine Centre, Central
Published Online August 21, 2013 Myocardial perfusion scintigraphy using rubidium-82 positron emission tomography Parthiban Arumugam *, Deborah Tout, and Christine Tonge Nuclear Medicine Centre, Central
Myocardial blood flow PET evaluation and quantification. Dr. Erick Alexánderson. Rosas
 Myocardial blood flow PET evaluation and quantification Dr. Erick Alexánderson Rosas Clinical case 62 year old female patient with a history of DM2 and chronic systemic hypertension She complains of progressive
Myocardial blood flow PET evaluation and quantification Dr. Erick Alexánderson Rosas Clinical case 62 year old female patient with a history of DM2 and chronic systemic hypertension She complains of progressive
MD F A F C A C MAS A N S C
 Myocardial Perfusion Imaging and Coronary Calcium Scoring: Complimentary or Competitive David Wolinsky MD FACC MASNC Section Head Nuclear Cardiology, Cleveland Clinic Florida Immediate Past President,
Myocardial Perfusion Imaging and Coronary Calcium Scoring: Complimentary or Competitive David Wolinsky MD FACC MASNC Section Head Nuclear Cardiology, Cleveland Clinic Florida Immediate Past President,
Flexibility of the COMBO Dual Therapy Stent
 TM CaseSpotlight Flexibility of the COMBO Dual Therapy Stent Doctor Peter den Heijer is an of the Catheterization Laboratory at the Department of Cardiology of the Amphia Ziekenhuis, Breda, The Netherlands.
TM CaseSpotlight Flexibility of the COMBO Dual Therapy Stent Doctor Peter den Heijer is an of the Catheterization Laboratory at the Department of Cardiology of the Amphia Ziekenhuis, Breda, The Netherlands.
Evaluating Clinical Risk and Guiding management with SPECT Imaging
 Evaluating Clinical Risk and Guiding management with SPECT Imaging Raffaele Giubbini Chair and Nuclear Medicine Unit University & Spedali Civili Brescia- Italy U.S. Congressional Budget Office. Technological
Evaluating Clinical Risk and Guiding management with SPECT Imaging Raffaele Giubbini Chair and Nuclear Medicine Unit University & Spedali Civili Brescia- Italy U.S. Congressional Budget Office. Technological
2017 Cardiology Survival Guide
 2017 Cardiology Survival Guide Chapter 4: Cardiac Catheterization/Percutaneous Coronary Intervention A cardiac catheterization involves a physician inserting a thin plastic tube (catheter) into an artery
2017 Cardiology Survival Guide Chapter 4: Cardiac Catheterization/Percutaneous Coronary Intervention A cardiac catheterization involves a physician inserting a thin plastic tube (catheter) into an artery
Coronary stenting: the appropriate use of FFR
 Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease?
 CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease? Madan Mohan MD MRCP FACC CQO, Division of Cardiovascular Medicine University Hospitals Case Medical Center Assistant
CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease? Madan Mohan MD MRCP FACC CQO, Division of Cardiovascular Medicine University Hospitals Case Medical Center Assistant
FRACTIONAL FLOW RESERVE Step-by-step measurement, Practical tips & Pitfalls
 FRACTIONAL FLOW RESERVE Step-by-step measurement, Practical tips & Pitfalls Ahmed M ElGuindy, MSc, MRCP(UK) Division of Cardiology Aswan Heart Centre 2013 Fractional Flow Reserve Essential diagnostic tool
FRACTIONAL FLOW RESERVE Step-by-step measurement, Practical tips & Pitfalls Ahmed M ElGuindy, MSc, MRCP(UK) Division of Cardiology Aswan Heart Centre 2013 Fractional Flow Reserve Essential diagnostic tool
Form 4: Coronary Evaluation
 Page of 7 Patient Details Hidden Show Show/Hide Annotations Stickies: Toggle All Toggle Open Toggle Resolved Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation
Page of 7 Patient Details Hidden Show Show/Hide Annotations Stickies: Toggle All Toggle Open Toggle Resolved Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation
Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement --
 --Practical Set Up Pressure Measurement --") Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement -- JoonHyung Doh, MD, PhD Assistant Professor, Vision21 Cardiac and Vascular Center Inje University Ilsan Paik Hospital Goyang, Korea
Fractional Flow Reserve (FFR) --Practical Set Up Pressure Measurement -- JoonHyung Doh, MD, PhD Assistant Professor, Vision21 Cardiac and Vascular Center Inje University Ilsan Paik Hospital Goyang, Korea
FFR in Left Main Disease
 FFR in Left Main Disease William F. Fearon, MD Associate Professor of Medicine Director, Interventional Cardiology Stanford University Medical Center Why FFR instead of IVUS? Physiologic versus anatomic
FFR in Left Main Disease William F. Fearon, MD Associate Professor of Medicine Director, Interventional Cardiology Stanford University Medical Center Why FFR instead of IVUS? Physiologic versus anatomic
The Latest on CT Fractional Flow Reserve. Dimitris Mitsouras, Ph.D.
 The Latest on CT Fractional Flow Reserve Dimitris Mitsouras, Ph.D. Assistant Professor of Radiology Harvard Medical School Director, Applied Imaging Science Lab Brigham and Women s Hospital Disclosures
The Latest on CT Fractional Flow Reserve Dimitris Mitsouras, Ph.D. Assistant Professor of Radiology Harvard Medical School Director, Applied Imaging Science Lab Brigham and Women s Hospital Disclosures
Evaluation of Intermediate Coronary lesions: Can You Handle the Pressure? Jeffrey A Southard, MD May 4, 2013
 Evaluation of Intermediate Coronary lesions: Can You Handle the Pressure? Jeffrey A Southard, MD May 4, 2013 Disclosures Consultant- St Jude Medical Boston Scientific Speaker- Volcano Corporation Heart
Evaluation of Intermediate Coronary lesions: Can You Handle the Pressure? Jeffrey A Southard, MD May 4, 2013 Disclosures Consultant- St Jude Medical Boston Scientific Speaker- Volcano Corporation Heart
Nuclear Perfusion Imaging of Angina
 January 2002 Nuclear Perfusion Imaging of Angina Davin Quinn HMS III Beth Israel Deaconess Medical Center Radiology Department Goals of Presentation Understand what a perfusion scan is Understand what
January 2002 Nuclear Perfusion Imaging of Angina Davin Quinn HMS III Beth Israel Deaconess Medical Center Radiology Department Goals of Presentation Understand what a perfusion scan is Understand what
EDITORIAL. Guiding coronary revascularization using PET stress myocardial perfusion imaging: The proof is in the pudding
 EDITORIAL Guiding coronary revascularization using PET stress myocardial perfusion imaging: The proof is in the pudding Ajay V. Srivastava, MD, FACC, a and Karthik Ananthasubramaniam, MD FRCP(Glas)FACC
EDITORIAL Guiding coronary revascularization using PET stress myocardial perfusion imaging: The proof is in the pudding Ajay V. Srivastava, MD, FACC, a and Karthik Ananthasubramaniam, MD FRCP(Glas)FACC
Atypical pain and normal exercise test
 Atypical pain and normal exercise test F. Mut, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history 67-year old male with several coronary risk factors. Atypical
Atypical pain and normal exercise test F. Mut, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history 67-year old male with several coronary risk factors. Atypical
Dave Kettles, St Dominics Hospital East London.
 Dave Kettles, St Dominics Hospital East London. 110 x 150 Angina for a couple of months Trop T negative T wave inversion across the chest leads Not wanting to risk radial Huge struggle with femoral
Dave Kettles, St Dominics Hospital East London. 110 x 150 Angina for a couple of months Trop T negative T wave inversion across the chest leads Not wanting to risk radial Huge struggle with femoral
FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT
 FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT01724957 Dobrin Vassilev MD, PhD Assoc. Prof. in Cardiology Head Cardiology Clinic, Alexandrovska University Hospital Medical
FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT01724957 Dobrin Vassilev MD, PhD Assoc. Prof. in Cardiology Head Cardiology Clinic, Alexandrovska University Hospital Medical