Colon ischemia. Bible class 12 September Stefan Christen. ACG Clinical Guideline: Am J Gastroenterol 2015
|
|
|
- Vincent Townsend
- 5 years ago
- Views:
Transcription
1 Colon ischemia Bible class 12 September 2018 Stefan Christen ACG Clinical Guideline: Am J Gastroenterol 2015
2 Definition
3 Definition Imbalance between blood supply and metabolic demands of the colonocytes
4 Definition Imbalance between blood supply and metabolic demands of the colonocytes A complete stop of the blood flow is not necessarily, sometimes only significantly reduction
5 Definition Imbalance between blood supply and metabolic demands of the colonocytes A complete stop of the blood flow is not necessarily, sometimes only significantly reduction Injury depends on acuteness of the event, degree of preexisting vascular collateralization, length of time
6 Definition Imbalance between blood supply and metabolic demands of the colonocytes A complete stop of the blood flow is not necessarily, sometimes only significantly reduction Injury depends on acuteness of the event, degree of preexisting vascular collateralization, length of time Reperfusion injury may produce more damage than just reduction of blood flow without reperfusion
7 Definition Imbalance between blood supply and metabolic demands of the colonocytes A complete stop of the blood flow is not necessarily, sometimes only significantly reduction Injury depends on acuteness of the event, degree of preexisting vascular collateralization, length of time Reperfusion injury may produce more damage than just reduction of blood flow without reperfusion -> local hypoperfusion and reperfusion injury
8 Definition Imbalance between blood supply and metabolic demands of the colonocytes A complete stop of the blood flow is not necessarily, sometimes only significantly reduction Injury depends on acuteness of the event, degree of preexisting vascular collateralization, length of time Reperfusion injury may produce more damage than just reduction of blood flow without reperfusion -> local hypoperfusion and reperfusion injury In most cases, no specific cause for ischemia is identified
9 Manifestations (clinical)
10 Manifestations (clinical) Sudden (mild) abdominal pain
11 Manifestations (clinical) Sudden (mild) abdominal pain Urgent desire to defecate
12 Manifestations (clinical) Sudden (mild) abdominal pain Urgent desire to defecate Within 24 hours bright red marroon blood per rectum or bloody diarrhea
13 Manifestations (clinical) Sudden (mild) abdominal pain Urgent desire to defecate Within 24 hours bright red marroon blood per rectum or bloody diarrhea Hb often stable (<5% transfusion)
14 Manifestations (clinical) Sudden (mild) abdominal pain Urgent desire to defecate Within 24 hours bright red marroon blood per rectum or bloody diarrhea Hb often stable (<5% transfusion) Symptomes often resolve within 2 3 days
15 Manifestation II
16 Manifestation II Reversible: - Colopathy with subepithelial hemorrhage, edema and ulcerations -Resorption usually within 3 day (Ulcerations may persist for several months)
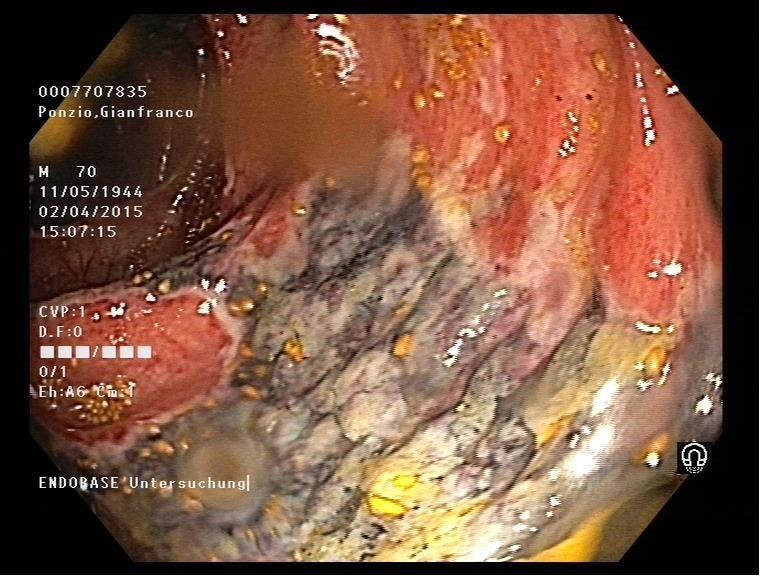
17 Manifestation II Reversible: - Colopathy with subepithelial hemorrhage, edema and ulcerations -Resorption usually within 3 day (Ulcerations may persist for several months) Irreversible: (up to 9%) - Gangrene, fulminant colitis - Chronic ischemic colitis (rare) - Stricture (rare)
18 Manifestation II Reversible: - Colopathy with subepithelial hemorrhage, edema and ulcerations -Resorption usually within 3 day (Ulcerations may persist for several months) Irreversible: (up to 9%) - Gangrene, fulminant colitis - Chronic ischemic colitis (rare) - Stricture (rare) Recurrent sepsis due to bacterial translocation
19 EPIDEMIOLOGY
20 EPIDEMIOLOGY % of all patients hospitalized for acute lower gastrointestinal Bleeding
21 EPIDEMIOLOGY % of all patients hospitalized for acute lower gastrointestinal Bleeding - Annual incidence rate of 17.7 cases/100,000 person-years
22 EPIDEMIOLOGY % of all patients hospitalized for acute lower gastrointestinal Bleeding - Annual incidence rate of 17.7 cases/100,000 person-years - Nearly four fold increase over 34 years
23 EPIDEMIOLOGY % of all patients hospitalized for acute lower gastrointestinal Bleeding - Annual incidence rate of 17.7 cases/100,000 person-years - Nearly four fold increase over 34 years - More common in women than in men (57 76%)
24 EPIDEMIOLOGY % of all patients hospitalized for acute lower gastrointestinal Bleeding - Annual incidence rate of 17.7 cases/100,000 person-years - Nearly four fold increase over 34 years - More common in women than in men (57 76%) - Mortality rate 4 to 12%
25 Classification
26 Classification Type I: Etiology not clear -> no specific therapy
27 Classification Type I: Etiology not clear -> no specific therapy Type II: Etiology identified - systemic hypotension - decreased cardiac output - aortic surgery -> treat the underlining disease
28 Risk Factors
29 Risk Factors Cardivascular RF - hypertension (57 72%), diabetes mellitus (17 28%), dyslipidemia (18 33%), renal disease (4 18%), coronary artery disease (18 37%), congestive heart failure (9 16%), peripheral vascular disease (8 21%)
30 Risk Factors Cardivascular RF - hypertension (57 72%), diabetes mellitus (17 28%), dyslipidemia (18 33%), renal disease (4 18%), coronary artery disease (18 37%), congestive heart failure (9 16%), peripheral vascular disease (8 21%) Diseases with risk of embolism/thrombosis - atrial fibrillation (9 14%), thrombophylia, hypercoagulable states (young patients!-> Further diagnostic tests)
31 Risk Factors Cardivascular RF - hypertension (57 72%), diabetes mellitus (17 28%), dyslipidemia (18 33%), renal disease (4 18%), coronary artery disease (18 37%), congestive heart failure (9 16%), peripheral vascular disease (8 21%) Diseases with risk of embolism/thrombosis - atrial fibrillation (9 14%), thrombophylia, hypercoagulable states (young patients!-> Further diagnostic tests) Chronic obstructive pulmonary disease (10 18%) (motality )
32 Risk Factors Cardivascular RF - hypertension (57 72%), diabetes mellitus (17 28%), dyslipidemia (18 33%), renal disease (4 18%), coronary artery disease (18 37%), congestive heart failure (9 16%), peripheral vascular disease (8 21%) Diseases with risk of embolism/thrombosis - atrial fibrillation (9 14%), thrombophylia, hypercoagulable states (young patients!-> Further diagnostic tests) Chronic obstructive pulmonary disease (10 18%) (motality ) Injury of the vessels: - type IIIb aortic dissection, surgery
33 Risk Factors Cardivascular RF - hypertension (57 72%), diabetes mellitus (17 28%), dyslipidemia (18 33%), renal disease (4 18%), coronary artery disease (18 37%), congestive heart failure (9 16%), peripheral vascular disease (8 21%) Diseases with risk of embolism/thrombosis - atrial fibrillation (9 14%), thrombophylia, hypercoagulable states (young patients!-> Further diagnostic tests) Chronic obstructive pulmonary disease (10 18%) (motality ) Injury of the vessels: - type IIIb aortic dissection, surgery Irritable bowel syndrome, cases of longdistance running in runners (26-42 years of age), Sickle cell crisis
34 RF Drugs
35 RF Drugs Moderate evidence:
36 RF Drugs Moderate evidence: constipation-inducing drugs, immunomodulator drugs, illicit drugs (amphetamines, cocaine)
37 RF Drugs Moderate evidence: constipation-inducing drugs, immunomodulator drugs, illicit drugs (amphetamines, cocaine) Low evidence:
38 RF Drugs Moderate evidence: constipation-inducing drugs, immunomodulator drugs, illicit drugs (amphetamines, cocaine) Low evidence: chemotherapeutic drugs, decongestants (pseudoephedrine), diuretics, ergot alcaloids, hormonal therapies, psychotropic drugs, serotoninergic drugs
39 Localisation
40 Localisation Usually segmental
41 Localisation Usually segmental Left colon most affected
42 Localisation Usually segmental Left colon most affected Rectum-uncommonly affected (dual blood supply)
43 Localisation Usually segmental Left colon most affected Rectum-uncommonly affected (dual blood supply) Isolated right colon ischemia:
44 Localisation Usually segmental Left colon most affected Rectum-uncommonly affected (dual blood supply) Isolated right colon ischemia: -more frequently atrial fibrillation (2x), coronary artery disease, chronic kidney disease on hemodyalisis - worse outcomes - only 25-46% have rectal bleeding
45
46 Watershed
47 Watershed
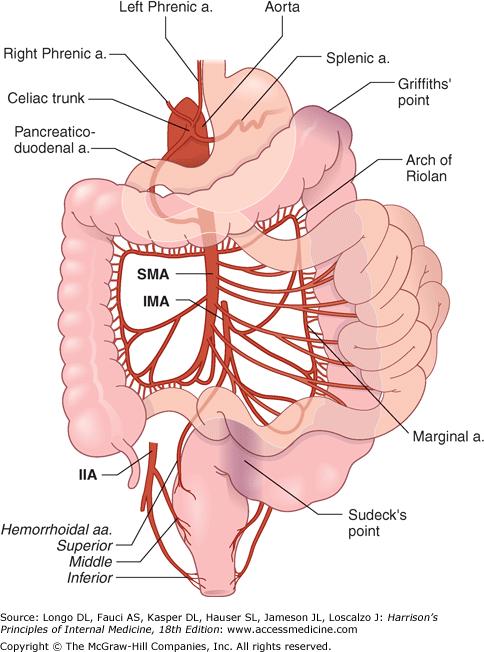
48 Watershed
49 Recomendet laboratory tests
50 Recomendet laboratory tests Complete blood count Electrolyt pannel Albumin Lactate LDH ph CK Amylase (assosiated with acute bowel ischemia) Exclude infectious colitis: Stool cultrue, Cl.difficile assay, ova and parasites
51 Risk factors of sever ischemia
52 Risk factors of sever ischemia Male gender Puls >100bpm Blood pressure <90 mm Hg Abdominal pain without rectal bleeding Ulcerations at endoscopy Peritoneal signs Ischemia of the right colon Free fluid on CT BUN >20mg/dl Hb <12g/dl LDH >350U/l Na<136 COPD, NI, Hepatitis C, Warfarin use WBC>15.000
53 Risk factors of sever ischemia Male gender Puls >100bpm Blood pressure <90 mm Hg Abdominal pain without rectal bleeding Ulcerations at endoscopy Peritoneal signs Ischemia of the right colon Free fluid on CT BUN >20mg/dl Hb <12g/dl LDH >350U/l Na<136 COPD, NI, Hepatitis C, Warfarin use WBC>15.000
54 Classification of disease severity
55 Classification of disease severity Mild: no risk factors
56 Classification of disease severity Mild: no risk factors Moderate: up to three risk factors
57 Classification of disease severity Mild: no risk factors Moderate: up to three risk factors Severe: more than three risk factors or -peritoneal signs - pneumatosis or portal gas at imaging - gangrene on colonoscopy - pancolonic distribution/irci
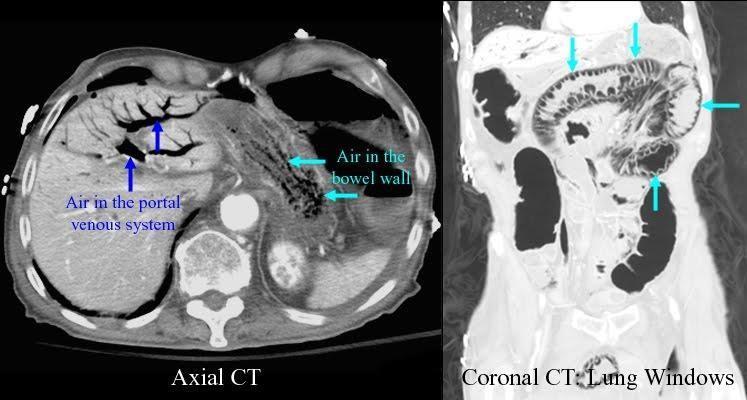
58 Imaging
59 Imaging CT with i.v. and oral contrast (first imaging modality of choice)
60 Imaging CT with i.v. and oral contrast (first imaging modality of choice) Multiphasic CT angiography, MR angiography, Splanchnic angiography

61 Imaging Plain radiography (thumbprinting sign)
62 Imaging
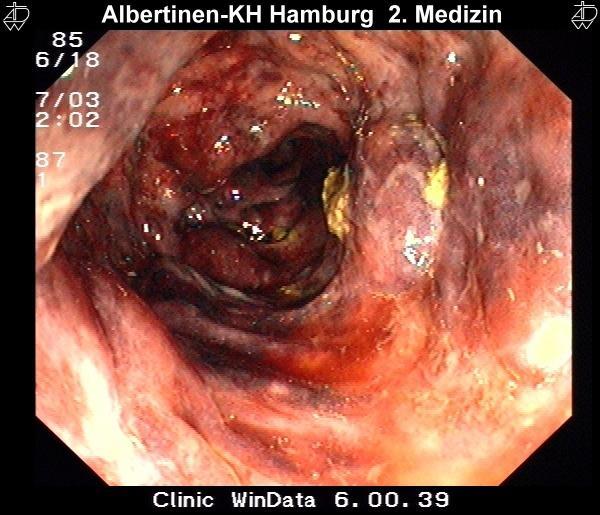
63 Colonoscopy
64 Colonoscopy - Early colonoscopy within 48h of presentation
65 Colonoscopy - Early colonoscopy within 48h of presentation -Typical signs disappear (47% vs 10% >5 d)
66 Colonoscopy - Early colonoscopy within 48h of presentation -Typical signs disappear (47% vs 10% >5 d) - Not too much insufflation, CO2
67 Colonoscopy - Early colonoscopy within 48h of presentation -Typical signs disappear (47% vs 10% >5 d) - Not too much insufflation, CO2 - The endoscopic procedure should be stopped at the distal-most extent of the disease (distribution of desease wit CT)
68 Colonoscopy - Early colonoscopy within 48h of presentation -Typical signs disappear (47% vs 10% >5 d) - Not too much insufflation, CO2 - The endoscopic procedure should be stopped at the distal-most extent of the disease (distribution of desease wit CT) - Contraindication acute peritonitis, gangrene, pneumatosis
69 Colonoscopy - Early colonoscopy within 48h of presentation -Typical signs disappear (47% vs 10% >5 d) - Not too much insufflation, CO2 - The endoscopic procedure should be stopped at the distal-most extent of the disease (distribution of desease wit CT) - Contraindication acute peritonitis, gangrene, pneumatosis - No biopsy in gangrene
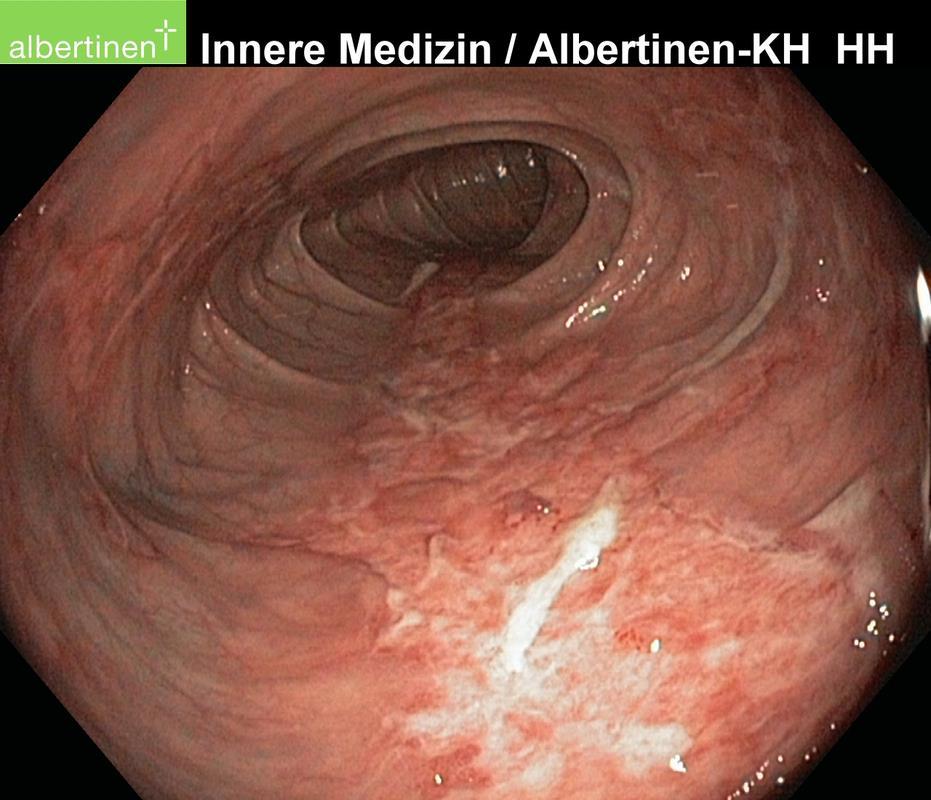
70 single-stripe sign

71
72
73
74 Histopathology
75 Histopathology Infarction and ghost cells (pathognomonic) (8%)
76 Histopathology Infarction and ghost cells (pathognomonic) (8%) Other histologic signs: mucosal and submucosal hemorrhage, edema, capillary fibrin thrombi
77 Treatment
78 Treatment Mostly no specific therapy i.v. fluid, maybe parenteral nutrition
79 Treatment Mostly no specific therapy i.v. fluid, maybe parenteral nutrition Surgery
80 Treatment Mostly no specific therapy i.v. fluid, maybe parenteral nutrition Surgery Antibiotic therapy in moderate or severe disease Broad antimicrobial regimens for 7 days
81 Treatment Mostly no specific therapy i.v. fluid, maybe parenteral nutrition Surgery Antibiotic therapy in moderate or severe disease Broad antimicrobial regimens for 7 days Cardial work-up if a cardiac source of embolism is suspected
82 Indication for surgery Acute: Subacute: Chronic:
83 Indication for surgery Acute: peritoneal signs, massive bleeding, fulminant colitis, toxic megacolon, portal venous gas or pneumatosis intestinalis, Subacute: Chronic:
84 Indication for surgery Acute: peritoneal signs, massive bleeding, fulminant colitis, toxic megacolon, portal venous gas or pneumatosis intestinalis, Consider if hypotension, tachycardia, pain without bleeding, fluid on CT, gangrene, right sided or pancolonic Subacute: Chronic:
85 Indication for surgery Acute: peritoneal signs, massive bleeding, fulminant colitis, toxic megacolon, portal venous gas or pneumatosis intestinalis, Consider if hypotension, tachycardia, pain without bleeding, fluid on CT, gangrene, right sided or pancolonic Subacute: failure to respond to treatment within 2-3 weeks with continued symptoms or a proteinlosing colopathy Chronic:
86 Indication for surgery Acute: peritoneal signs, massive bleeding, fulminant colitis, toxic megacolon, portal venous gas or pneumatosis intestinalis, Consider if hypotension, tachycardia, pain without bleeding, fluid on CT, gangrene, right sided or pancolonic Subacute: failure to respond to treatment within 2-3 weeks with continued symptoms or a proteinlosing colopathy Chronic: symptomatic colon stricture, symptomatic segmental ischemic colitis
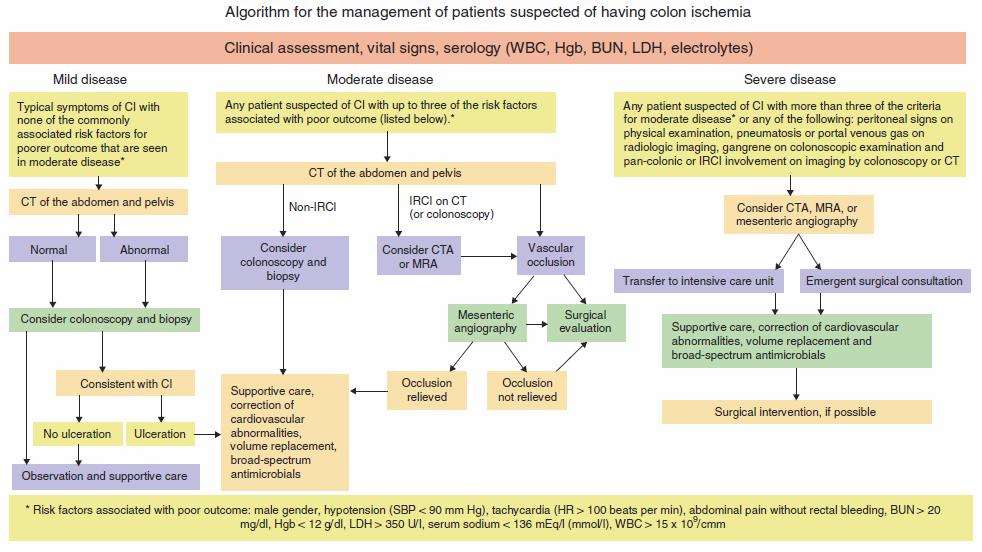
87 Management
88 Questions?
Colon ischemia. ACG Clinical Guideline; Am J Gastroenterol 2015
 Colon ischemia ACG Clinical Guideline; Am J Gastroenterol 2015 Manifestations Acute, reversible Irreversible : gangrene, fulminant colitis/stricture formation, chronic ischemic colitis Recurrent sepsis
Colon ischemia ACG Clinical Guideline; Am J Gastroenterol 2015 Manifestations Acute, reversible Irreversible : gangrene, fulminant colitis/stricture formation, chronic ischemic colitis Recurrent sepsis
Colon Ischemia (CI): New Developments and Guidelines for Management. Spectrum of CI
: New Developments and Guidelines for Management. Spectrum of CI") Colon Ischemia (CI): New Developments and Guidelines for Management Lawrence J. Brandt, MD, MACG Professor of Medicine and Surgery Albert Einstein College of Medicine Emeritus Chief of Gastroenterology
Colon Ischemia (CI): New Developments and Guidelines for Management Lawrence J. Brandt, MD, MACG Professor of Medicine and Surgery Albert Einstein College of Medicine Emeritus Chief of Gastroenterology
3/20/2009. Julio Garcia-Aguilar Chair, Department of Surgery City of Hope, Duarte, California
 Ischemic Colitis Ischemic Colitis Julio Garcia-Aguilar Chair, Department of Surgery City of Hope, Duarte, California Ischemic colitis (IC) represents greater than 50% of all intestinal ischemia IC most
Ischemic Colitis Ischemic Colitis Julio Garcia-Aguilar Chair, Department of Surgery City of Hope, Duarte, California Ischemic colitis (IC) represents greater than 50% of all intestinal ischemia IC most
ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois
 ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois SCBT/MR 2010 San Diego, California March 8, 2010 13:40-14:00
ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois SCBT/MR 2010 San Diego, California March 8, 2010 13:40-14:00
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY MESENTERIC ISCHAEMIA P Zwanepoel INTRODUCTION Mesenteric ischaemia results from hypoperfusion of the gut, most commonly due to occlusion, thrombosis or vasospasm.
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY MESENTERIC ISCHAEMIA P Zwanepoel INTRODUCTION Mesenteric ischaemia results from hypoperfusion of the gut, most commonly due to occlusion, thrombosis or vasospasm.
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
MESENTERIC ISCHEMIA THE FORGOTTEN DIAGNOSIS. Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, Illinois
 MESENTERIC ISCHEMIA THE FORGOTTEN DIAGNOSIS Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, Illinois SCBT/MR 2010 San Diego, California March 8, 2010 16:00-16:10
MESENTERIC ISCHEMIA THE FORGOTTEN DIAGNOSIS Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, Illinois SCBT/MR 2010 San Diego, California March 8, 2010 16:00-16:10
Chapter 8 Ischemic Colitis
 Chapter 8 Ischemic Colitis Peter Van Eyken, Daniela Fanni, and Clara Gerosa Abstract The large bowel accounts for roughly half of all episodes of gastrointestinal ischemia. Three major manifestations of
Chapter 8 Ischemic Colitis Peter Van Eyken, Daniela Fanni, and Clara Gerosa Abstract The large bowel accounts for roughly half of all episodes of gastrointestinal ischemia. Three major manifestations of
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Role of radiology in colo-rectal bleedings. Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE
 Role of radiology in colo-rectal bleedings Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE Epidemiology Lower GI bleeding accounts for 20-25% of all GI bleeding Annual incidence in USA :21-27/100000 Longstreth
Role of radiology in colo-rectal bleedings Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE Epidemiology Lower GI bleeding accounts for 20-25% of all GI bleeding Annual incidence in USA :21-27/100000 Longstreth
ICD-10 Physician Education. Palliative Care SIP
 ICD-10 Physician Education Palliative Care SIP 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
ICD-10 Physician Education Palliative Care SIP 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
Shock, Hemorrhage and Thrombosis
 Shock, Hemorrhage and Thrombosis 1 Shock Systemic hypoperfusion due to: Reduction in cardiac output Reduction in effective circulating blood volume Hypotension Impaired tissue perfusion Cellular hypoxia
Shock, Hemorrhage and Thrombosis 1 Shock Systemic hypoperfusion due to: Reduction in cardiac output Reduction in effective circulating blood volume Hypotension Impaired tissue perfusion Cellular hypoxia
Ischemic colitis. Incidence, Risk Factors, Clinical Manifestation and Outcome. Yrsa Yngvadóttir
 Ischemic colitis Incidence, Risk Factors, Clinical Manifestation and Outcome Yrsa Yngvadóttir Thesis for the degree of Bachelor of Science University of Iceland Faculty of Medicine School of Health Science
Ischemic colitis Incidence, Risk Factors, Clinical Manifestation and Outcome Yrsa Yngvadóttir Thesis for the degree of Bachelor of Science University of Iceland Faculty of Medicine School of Health Science
Instruct patient and caregivers: Need for constant monitoring Potential complications of drug therapy
 Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
Yes No Unknown. Major Infection Information
 Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Understanding the Benefits and Risks
 LOTRONEX and its authorized generic alosetron hydrochloride: Understanding the Benefits and Risks The LOTRONEX REMS Program Prescriber Education Slide Deck LOTRONEX is a registered trademark of Prometheus
LOTRONEX and its authorized generic alosetron hydrochloride: Understanding the Benefits and Risks The LOTRONEX REMS Program Prescriber Education Slide Deck LOTRONEX is a registered trademark of Prometheus
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Circulatory Disturbances 5: Thrombosis, Embolism, Infarction, Shock
 Circulatory Disturbances 5: Thrombosis, Embolism, Infarction, Shock Shannon Martinson, Feb 2016 http://people.upei.ca/smartinson/ VPM 152 General Pathology Thrombosis, Embolism, Infarction, Shock Learning
Circulatory Disturbances 5: Thrombosis, Embolism, Infarction, Shock Shannon Martinson, Feb 2016 http://people.upei.ca/smartinson/ VPM 152 General Pathology Thrombosis, Embolism, Infarction, Shock Learning
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Asthma J45.20 Mild, uncomplicated J45.21 Mild, with (acute) exacerbation J45.22 Mild, with status asthmaticus
 exacerbation J45.22 Mild, with status asthmaticus") A Fib & Flutter I48.0 Paroxysmal atrial fibrillation I48.1 Persistent atrial fibrillation I48.2 Chronic atrial fibrillation I48.3 Typical atrial flutter Asthma J45.20 Mild, uncomplicated J45.21 Mild, with
A Fib & Flutter I48.0 Paroxysmal atrial fibrillation I48.1 Persistent atrial fibrillation I48.2 Chronic atrial fibrillation I48.3 Typical atrial flutter Asthma J45.20 Mild, uncomplicated J45.21 Mild, with
Alliance A Symptomatic brain radionecrosis after receiving radiosurgery for
 RANDOMIZED PHASE II STUDY: CORTICOSTEROIDS + BEVACIZUMAB VS. CORTICOSTEROIDS + PLACEBO (BEST) FOR RADIONECROSIS AFTER RADIOSURGERY FOR BRAIN METASTASES Pre-registration Eligibility Criteria Required Initial
RANDOMIZED PHASE II STUDY: CORTICOSTEROIDS + BEVACIZUMAB VS. CORTICOSTEROIDS + PLACEBO (BEST) FOR RADIONECROSIS AFTER RADIOSURGERY FOR BRAIN METASTASES Pre-registration Eligibility Criteria Required Initial
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
LOTRONEX and its authorized generic alosetron hydrochloride:
 LOTRONEX and its authorized generic alosetron hydrochloride: Understanding the Benefits and Risks The Prescribing Program for LOTRONEX TM Prescriber Education Slide Deck PROMETHEUS and the Link Design
LOTRONEX and its authorized generic alosetron hydrochloride: Understanding the Benefits and Risks The Prescribing Program for LOTRONEX TM Prescriber Education Slide Deck PROMETHEUS and the Link Design
Online Supplementary Data. Country Number of centers Number of patients randomized
 A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
A Case of Pneumatosis Cystoides Intestinalis Mimicking Intestinal Perforation
 Showa Univ J Med Sci 26 2, 169 173, June 2014 Case Report A Case of Pneumatosis Cystoides Intestinalis Mimicking Intestinal Perforation Takahiro UMEMOTO 1, Yoshikuni HARADA 1, Makiko SAKATA 1, Gaku KIGAWA
Showa Univ J Med Sci 26 2, 169 173, June 2014 Case Report A Case of Pneumatosis Cystoides Intestinalis Mimicking Intestinal Perforation Takahiro UMEMOTO 1, Yoshikuni HARADA 1, Makiko SAKATA 1, Gaku KIGAWA
Diseases of the Colon. Jack Bragg, D.O., F.A.C.O.I.
 Diseases of the Colon Jack Bragg, D.O., F.A.C.O.I. I have no disclosures I work for the Curators of the University of Missouri Inflammatory Bowel Disease ULCERATIVE COLITIS CROHN S DISEASE Transmural Inflammation
Diseases of the Colon Jack Bragg, D.O., F.A.C.O.I. I have no disclosures I work for the Curators of the University of Missouri Inflammatory Bowel Disease ULCERATIVE COLITIS CROHN S DISEASE Transmural Inflammation
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
STROKE - IMAGING. Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli.
 STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Vascular Imaging in the Pediatric Abdomen. Jonathan Swanson, MD
 Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Cardiac Pathology & Rehabilitation
 Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Pharmacotherapy Handbook
 Pharmacotherapy Handbook Eighth Edition Barbara G. Wells, PharmD, HP, FCCP, BCPP Dean and Professor Executive Director, Research Institute of Pharmaceutical Sciences School of Pharmacy, The University
Pharmacotherapy Handbook Eighth Edition Barbara G. Wells, PharmD, HP, FCCP, BCPP Dean and Professor Executive Director, Research Institute of Pharmaceutical Sciences School of Pharmacy, The University
Index. Crit Care Clin 19 (2003)
") Crit Care Clin 19 (2003) 331 335 Index A ACVECC. See American College of Veterinary Emergency and Critical Care (ACVECC). Aging. See also Elderly; Geriatric critical care. respiratory function effects
Crit Care Clin 19 (2003) 331 335 Index A ACVECC. See American College of Veterinary Emergency and Critical Care (ACVECC). Aging. See also Elderly; Geriatric critical care. respiratory function effects
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
INTRODUCTION TO DIAGNOSTIC ENDOSCOPY
 INTRODUCTION TO DIAGNOSTIC ENDOSCOPY EGD & Colonoscopy Procedure Kolegium Ilmu Bedah Indonesia B. Parish Budiono Sub Bagian Bedah Digestif FK UNDIP/RSUP Dr. Kariadi Semarang GI Endoscopy GI Endoscopy is
INTRODUCTION TO DIAGNOSTIC ENDOSCOPY EGD & Colonoscopy Procedure Kolegium Ilmu Bedah Indonesia B. Parish Budiono Sub Bagian Bedah Digestif FK UNDIP/RSUP Dr. Kariadi Semarang GI Endoscopy GI Endoscopy is
Cytomegalovirus Colitis in an Immunocompetent Patient: A Case Report
 ISPUB.COM The Internet Journal of Surgery Volume 17 Number 2 Cytomegalovirus Colitis in an Immunocompetent Patient: A Case Report M Ud Citation M Ud. Cytomegalovirus Colitis in an Immunocompetent Patient:
ISPUB.COM The Internet Journal of Surgery Volume 17 Number 2 Cytomegalovirus Colitis in an Immunocompetent Patient: A Case Report M Ud Citation M Ud. Cytomegalovirus Colitis in an Immunocompetent Patient:
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Medical APMLE. Podiatry and Medical.
 Medical APMLE Podiatry and Medical http://killexams.com/exam-detail/apmle Question: 290 Signs and symptoms of hemolytic transfusion reactions include: A. Hypothermia B. Hypertension C. Polyuria D. Abnormal
Medical APMLE Podiatry and Medical http://killexams.com/exam-detail/apmle Question: 290 Signs and symptoms of hemolytic transfusion reactions include: A. Hypothermia B. Hypertension C. Polyuria D. Abnormal
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Javier Marquez Graciani, MD Attending Dr F. Joglar
 Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Inflammatory Bowel Disease Ischemic bowel disease
 Inflammatory Bowel Disease Ischemic bowel disease Inflammatory Bowel Disease The two disorders that comprise IBD are: ulcerative colitis Crohn disease The distinction between ulcerative colitis and Crohn
Inflammatory Bowel Disease Ischemic bowel disease Inflammatory Bowel Disease The two disorders that comprise IBD are: ulcerative colitis Crohn disease The distinction between ulcerative colitis and Crohn
TROPONIN POSITIVE 2/20/2015 WHAT DOES IT MEAN? When should a troponin level be obtained?
 TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
Episodes of Care Risk Adjustment
 Episodes of Care Risk Adjustment Episode Types Wave 1 Asthma Acute Exacerbation Perinatal Total Joint Replacement Wave 2 Acute Percutaneous Coronary Intervention COPD Acute Exacerbation Non-acute Percutaneous
Episodes of Care Risk Adjustment Episode Types Wave 1 Asthma Acute Exacerbation Perinatal Total Joint Replacement Wave 2 Acute Percutaneous Coronary Intervention COPD Acute Exacerbation Non-acute Percutaneous
CT imaging findings of acute mesenteric ischemia and ischemic colitis. A brief pictorial essay.
 CT imaging findings of acute mesenteric ischemia and ischemic colitis. A brief pictorial essay. Poster No.: C-0750 Congress: ECR 2011 Type: Educational Exhibit Authors: Y. Arias Morales, J. P. Giraldo
CT imaging findings of acute mesenteric ischemia and ischemic colitis. A brief pictorial essay. Poster No.: C-0750 Congress: ECR 2011 Type: Educational Exhibit Authors: Y. Arias Morales, J. P. Giraldo
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Research Article Predisposing Factors of Ischemic Colitis: Data from 14 Years of Experience in a Single Center
 Hindawi Gastroenterology Research and Practice Volume 2017, Article ID 1049810, 5 pages https://doi.org/10.1155/2017/1049810 Research Article Predisposing Factors of Ischemic Colitis: Data from 14 Years
Hindawi Gastroenterology Research and Practice Volume 2017, Article ID 1049810, 5 pages https://doi.org/10.1155/2017/1049810 Research Article Predisposing Factors of Ischemic Colitis: Data from 14 Years
Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is
 R. Siebert Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is a progressive decline in blood pressure
R. Siebert Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is a progressive decline in blood pressure
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Diarrhoea on the AMU. Dr Chris Roseveare
 Diarrhoea on the AMU Dr Chris Roseveare The Society for Acute Medicine, Spring Meeting, Radisson Blu Hotel, Dublin 3-4 May 2012 Acute diarrhoea in developed countries adult populations Mainly a primary
Diarrhoea on the AMU Dr Chris Roseveare The Society for Acute Medicine, Spring Meeting, Radisson Blu Hotel, Dublin 3-4 May 2012 Acute diarrhoea in developed countries adult populations Mainly a primary
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis?
 Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
Bachelor of Chinese Medicine Shock
 BCM Year 2 Dr. Irene Ng Jan 28, 2003 9:30 am 1:00 pm Rm 004 UPB Bachelor of Chinese Medicine 2002 2003 Shock Learning objectives Be able to: know the definition of shock know the classification and causes
BCM Year 2 Dr. Irene Ng Jan 28, 2003 9:30 am 1:00 pm Rm 004 UPB Bachelor of Chinese Medicine 2002 2003 Shock Learning objectives Be able to: know the definition of shock know the classification and causes
Hemodynamic Disorders, Thrombosis, and Shock. Richard A. McPherson, M.D.
 Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Ischemic Heart Diseases. Dr. Nabila Hamdi MD, PhD
 Ischemic Heart Diseases Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast the different types of angina regarding their pathogenesis, clinical manifestations and evolution. Discuss myocardial infarct,
Ischemic Heart Diseases Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast the different types of angina regarding their pathogenesis, clinical manifestations and evolution. Discuss myocardial infarct,
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Pneumatosis intestinalis, not always a surgical emergency
 Pneumatosis intestinalis, not always a surgical emergency Poster No.: C-2233 Congress: ECR 2012 Type: Educational Exhibit Authors: E. Vanhoutte, M. Lefere, R. Vanslembrouck, D. Bielen, G. De 1 1 2 1 1
Pneumatosis intestinalis, not always a surgical emergency Poster No.: C-2233 Congress: ECR 2012 Type: Educational Exhibit Authors: E. Vanhoutte, M. Lefere, R. Vanslembrouck, D. Bielen, G. De 1 1 2 1 1
Treatment of the Medically Compromised Patient
 Treatment of the Medically Compromised Patient Nashville Area Continuing Dental Education Series November 3, 2010 Harry J. Brown, MD Chief Medical Officer, Nashville Area Outline General Principles Specific
Treatment of the Medically Compromised Patient Nashville Area Continuing Dental Education Series November 3, 2010 Harry J. Brown, MD Chief Medical Officer, Nashville Area Outline General Principles Specific
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE
 ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease
 BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease David A Owen University of British Columbia CAUSES OF DIARRHEA DIARRHEA COLITIS PRESENT COLITIS ABSENT INFECTIOUS NON-INFECTIOUS
BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease David A Owen University of British Columbia CAUSES OF DIARRHEA DIARRHEA COLITIS PRESENT COLITIS ABSENT INFECTIOUS NON-INFECTIOUS
ENROLLMENT : Line of Business Summary
 ENROLLMENT : Line of Business Summary Date Range : JAN 2017 through DEC 2017 COMPREHENSIVE MAJOR MEDICAL Print Date : 1/19/2018 9:43:49AM Page 1 of 1 Month Year Single 2 Person : Emp/Spouse 2 Person :
ENROLLMENT : Line of Business Summary Date Range : JAN 2017 through DEC 2017 COMPREHENSIVE MAJOR MEDICAL Print Date : 1/19/2018 9:43:49AM Page 1 of 1 Month Year Single 2 Person : Emp/Spouse 2 Person :
Algorithm for managing severe ulcerative colitis
 Tropical Gastroenterology 2014;Suppl:S40 44 Algorithm for managing severe ulcerative colitis Vineet Ahuja 1, Ajay Kumar 2, Rakesh Kochhar 3 ABSTRACT Dept of Gastroenterology, 1 All India Institute of Medical
Tropical Gastroenterology 2014;Suppl:S40 44 Algorithm for managing severe ulcerative colitis Vineet Ahuja 1, Ajay Kumar 2, Rakesh Kochhar 3 ABSTRACT Dept of Gastroenterology, 1 All India Institute of Medical
HYPEREMIA AND CONGESTION
 HYPEREMIA AND CONGESTION Learning Objectives Define congestion and hyperemia Differentiate between the two with regard to: Mechanisms / underlying causes Appearance (gross and histologic) Effects Differentiate
HYPEREMIA AND CONGESTION Learning Objectives Define congestion and hyperemia Differentiate between the two with regard to: Mechanisms / underlying causes Appearance (gross and histologic) Effects Differentiate
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Listing Form: Heart or Cardiovascular Impairments. Medical Provider:
 Listing Form: Heart or Cardiovascular Impairments Medical Provider: Printed Name Signature Patient Name: Patient DOB: Patient SS#: Date: Dear Provider: Please indicate whether your patient s condition
Listing Form: Heart or Cardiovascular Impairments Medical Provider: Printed Name Signature Patient Name: Patient DOB: Patient SS#: Date: Dear Provider: Please indicate whether your patient s condition
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Common Gastrointestinal Problems in the Elderly
 Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery
 Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery Rahul Narang, MD Colon and Rectal Surgery Assistant Professor of Surgery No Disclosure Clostridium Difficile Colitis: Treatments,
Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery Rahul Narang, MD Colon and Rectal Surgery Assistant Professor of Surgery No Disclosure Clostridium Difficile Colitis: Treatments,
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most