Anti coagulation Treatment Effects of Age Impact of NOAC. June 2014 Dov Gavish MD FESC Tel Aviv University ISRAEL
|
|
|
- Lesley Sherman
- 5 years ago
- Views:
Transcription








1 Anti coagulation Treatment Effects of Age Impact of NOAC June 2014 Dov Gavish MD FESC Tel Aviv University ISRAEL PE

2 VTE: deep vein thrombosis and pulmonary embolism are common in elderly Thrombosis is the formation or presence of a thrombus that may obstruct blood flow through a vein or artery 1 VTE occurs when thrombosis obstructs blood flow through a vein The term VTE encompasses: DVT PE VTE is a serious health issue 2 PE As the venous clot grows, it extends along the vein PE occurs when parts of the clot detach and travel in the blood to block vessels in the lungs Migration Embolus Thrombus DVT, deep vein thrombosis; PE, pulmonary embolism 1. Anderson FA, et al. Center for Outcomes Research, University of Massachusetts Medical Center; Goldhaber SZ. J Am Coll Cardiol 1992;19:

3 VTE rate increase with Age
4 DVT is Common in the elderly The aged have an elevated risk of developing deep vein thrombosis. The annual incidence rate of first DVT in individuals aged years is estimated to be per 1,000, and this doubles in those aged over Older patients also have higher in-hospital mortality associated with pulmonary embolism and DVT, at 21% and 3%, 4 Mar 2013
5 Potential complications and goal of treatment DVT complications: 1,2 PE Damage to valves in the deep veins Venous reflux Post-thrombotic syndrome (PTS) Goal of treatment Prevent embolization to the lungs Prevent extension into larger veins Prevent recurrence Avoid the chronic complications 1. Kearon C. Circulation 2003;107:I22 I30; 2. Ginsberg JS, et al. Arch Intern Med 2000;160:

6 AF is a problem of the older people 6 Mar 2013

7 Risk of stroke in AF. Patterns of recurrent AF may be classified as paroxysmal, persistent, or permanent. Lubitz S A et al. Eur Heart J 2010;31: Published on behalf of the European Society of Cardiology. All rights reserved. The Author For permissions please journals.permissions@oxfordjournals.org
8 Cumulative hazard Stroke risk is evident in sub clinical AF Sub clinical AF* is associated with a 2.5-times greater risk of ischemic stroke or systemic embolism 4.2% vs. 1.7% with no arrhythmia (P=0.007) 0.08 Risk of ischemic stroke or systemic embolism 0.06 Subclinical atrial tachyarrhythmias present Years of follow-up *Sub clinical atrial tachyarrhythmia's detected by implanted devices (n=2580) Healey JS et al. N Engl J Med 2012;366:120 9 Subclinical atrial tachyarrhythmias absent 8 Mar 2013
9 Virchow s triad for thrombogenesis (possibly age related) Atrial fibrillation Left ventricular dysfunction Immobility Venous insufficiency/ varicose veins Atrial fibrillation Trauma/surgery Atherosclerosis Venepuncture Heart valve disease/ replacement Indwelling catheters HYPERCOAGULABLE STATE Atrial fibrillation Malignancy Pregnancy Oestrogen therapy Trauma/surgery Sepsis Thrombophilia Inflammatory bowel disease Nephrotic syndrome Adapted from Watson T et al. Lancet 2009;373: April 2012
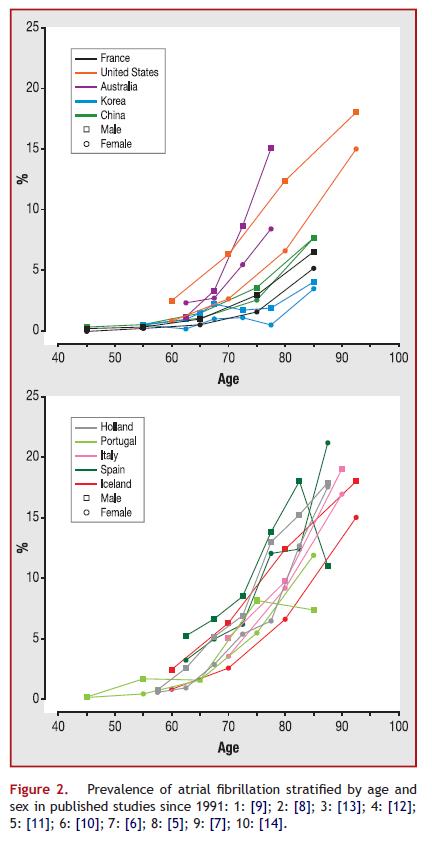
10 Prevalence of AF by age group Source: American Journal of Cardiology 2013; 112: (DOI: /j.amjcard ) Copyright 2013 Elsevier Inc. Terms and Conditions

11
. Go A et al.")
12 Prevalence of stroke by age and sex (National Health and Nutrition Examination Survey: ). Go A et al. Circulation 2013;127:e6-e245 Copyright American Heart Association
13 Two-year age-adjusted incidence of stroke/1000 AF is a significant risk factor for ischemic stroke No cardiovascular condition Cardiovascular condition * * * * 10 0 High blood pressure Coronary heart disease Congestive heart failure Atrial fibrillation Risk ratio *p<0.001 versus no cardiovascular condition Wolf et al, Stroke 1991
14 Stroke risk in patients with AF (%) Proportion of strokes attributable to AF increases with age Men Women Age (years) Marini et al, Stroke 2005
 Andersen KK et al. Stroke 2009;40:2068 72 15 Mar 2013")
15 Most strokes associated with AF are ischemic Types of stroke in patients with AF Haemorrhagic (8%) Ischaemic stroke (n=5810) Haemorrhagic stroke (n=484) Ischaemic (92%) Based on data collected in the Danish National Indicator Project for patients hospitalized for stroke (including 6294 patients with AF) Andersen KK et al. Stroke 2009;40: Mar 2013
16 AF annual costs to the EU economy Estimated 6.2 billion* Equates to per patient each year Greece Italy Poland Spain Netherlands Mean annual cost ( /patient) Total country costs ( million) *EuroHeart Study, data Ringborg A et al. Europace 2008;10: Mar 2013
17 Relative risk of stroke Risk of stroke varies widely between patients with AF Depends on a range of factors 1 Annual stroke rates can vary 20-fold with no vs multiple risk factors Prior stroke or TIA History of diabetes History of hypertension History of heart failure Increasing age* Risk factor *Relative risks are based on decades of age TIA = transient ischemic attack 1. Atrial Fibrillation Investigators. Arch Intern Med 1994;154: ; 2. Gage BF et al. JAMA 2001;285: Mar 2013
18 Severe disability (% of stroke patients) The increased disability that results from AF-related stroke persists over time Framingham Heart Study (US) * % 58% AF No AF % 36% 30% % 16% 11% 0 Acute phase 3 months 6 months 12 months Time after stroke event *Severe disability was defined as a score of 40 in the modified Barthel Index for activities of daily living Lin et al, Stroke 1996
19 New slide Risk factors for ischemic stroke Age (years) < Multivariate hazard ratios (95% CI) 1.0 (reference) 2.97 ( ) 5.28 ( ) Female sex 1.17 ( ) Previous ischemic stroke 2.81 ( ) Intracranial bleeding 1.49 ( ) Vascular disease (any) Myocardial infarction Previous CABG Peripheral artery disease 1.14 ( ) 1.09 ( ) 1.19 ( ) 1.22 ( ) Hypertension 1.17 ( ) Heart failure (history) 0.98 ( ) Diabetes mellitus 1.19 ( ) Thyroid disease Thyrotoxicosis 1.00 ( ) 1.03 ( ) CABG = coronary artery bypass graft Camm AJ et al. Eur Heart J doi: /eurheartj/ehs April Mar
20 Estimation of stroke risk in AF Classification scheme Patient population Risk factors identified Atrial Fibrillation Investigators 1 Five randomized studies N=1593, 106 strokes over a mean follow-up 1.4 yrs Age Hypertension Prior cerebral ischemia Diabetes Stroke Prevention and Atrial Fibrillation (SPAF) 2 Two randomized studies N=854, 68 strokes over a mean follow-up 2.3 yrs Blood pressure >160 mmhg Prior cerebral ischemia Recent heart failure Combination of age 75 yrs and female gender Framingham Heart Study 3 Recently identified AF N=705, 83 strokes and 382 strokes or death over a mean follow-up of 4.0 years Age Female gender Diabetes 1. Atrial Fibrillation Investigators. Arch Intern Med 1994;154: ; 2. SPAF Investigators. J Stroke Cerebrovasc Dis 1995;5:147 57; 3. Wang TJ et al. JAMA 2003;290: Mar 2013
21 CHADS 2 score Stroke risk assessment with CHADS CHADS 2 criteria Score Congestive heart failure 1 Hypertension 1 Age 75 yrs 1 Diabetes mellitus 1 Stroke/transient ischaemic attack Annual stroke rate (%)* 30 Gage BF et al. JAMA 2001;285: April Mar

22 Older than 75 =2 points!
23 Updated slide Assessing stroke risk: CHA 2 DS 2 -VASc CHA 2 DS 2 -VASc criteria Score CHF/LV dysfunction 1 Hypertension 1 Age 75 yrs 2 Diabetes mellitus 1 Stroke/TIA/TE 2 Vascular disease 1 Age yrs 1 Total score Patients (n=7329) Adjusted stroke rate (%/year)* Sex category (i.e. female gender) 1 *Theoretical rates without therapy; assuming that warfarin provides a 64% reduction in stroke risk, based on Hart RG et al CHF = congestive heart failure; LV = left ventricular; TE = thromboembolism; TIA = transient ischaemic attack Lip G et al. Chest 2010;137:263 72; Lip G et al. Stroke 2010; 41:2731 8; Camm J et al. Eur Heart J 2010;31: ; Hart RG et al. Ann Intern Med 2007;146: April Mar
24 Updated slide Assessing bleeding risk: HAS-BLED HAS-BLED risk criteria Score Hypertension (SBP >160 mmhg) 1 Abnormal renal or liver function (1 point each) 1 or 2 Stroke 1 Bleeding (history or predisposition) 1 Labile INRs (e.g. <60% TTR) 1 Elderly (e.g. age >65 yrs) 1 Drugs or alcohol (1 point each; includes antiplatelets and NSAIDs) 1 or 2 INR = International normalized ratio; NSAID = non-steroidal anti-inflammatory drug; SBP = systolic blood pressure; TTR = time in therapeutic range ESC guidelines: Camm J et al. Eur Heart J 2010;31: April Mar

25 Risk stratification: Stroke and bleeding

26 26 Mar 2013
27 Treatment options for AF ISCHAEMIC STROKE PREVENTION CONTROL OF HEART RATE MAINTENANCE OF SINUS RHYTHM PHARMACOLOGICAL Dabigatran etexilate Rivaroxaban Vitamin K antagonists (e.g. warfarin) ASA Clopidogrel NON-PHARMACOLOGICAL PHARMACOLOGICAL -blockers Calcium channel blockers (non-dhp) Digoxin NON-PHARMACOLOGICAL PHARMACOLOGICAL Anti-arrhythmic drugs Class IA Class IC Class III NON-PHARMACOLOGICAL Removal/isolation of left atrial appendage Ablation/permanent pacing Ablation Surgery (MAZE procedure) ASA = acetyl salicylic acid; DHP = dihydropyridine Adapted from Prystowsky EN. Am J Cardiol 2000;85:3D 11D Disclaimer: Dabigatran etexilate and rivaroxaban are now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details 27 April Mar

28 Tests to be performed in elderly with AF 28 Mar 2013

29 Geriatric assessment in elderly with AF 29 Mar 2013
30 New slide Challenges and limitations of ASA Limited efficacy for stroke prevention vs VKAs Limited effect on thromboembolic No evidence of reduced mortality with ASA in AF ASA limitations Increased bleeding risk Significant adverse events Unfavourable net clinical benefit ASA = acetylsalicylic acid; VKA = vitamin K antagonist 30 April Mar
31 Limited efficacy of ASA in reducing the risk of stroke in patients with AF Updated slide AFASAK SPAF EAFT ESPS II LASAF 125 mg/d 125 mg QOD UK-TIA 300 mg/d 1200 mg/d JAST All trials ASA better Placebo better Only the SPAF trial showed a benefit of ASA over placebo for reducing stroke risk RRR: 19%* (95% CI: 1 to 35%) RRR (%) 100 *Random effects model; error bars = 95% CI; *P>0.2 for homogeneity; Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic); for ischaemic stroke only, RRR was 21% (95% CI: 1 to 38%) ASA = acetylsalicylic acid; QOD = every other day Hart RG et al. Ann Intern Med 2007;146: April Mar
32 Warfarin reduces the risk of stroke in patients with AF Updated slide Favours warfarin Favours placebo AFASAK SPAF BAATAF CAFA SPINAF EAFT All trials RRR 64%* (95% CI: 49 74%) RRR (%) 100 When only ischaemic stroke was considered, dose-adjusted warfarin was associated with a 67% RRR (95% CI: 54 77%) Random effects model; Error bars = 95% CI; *P>0.2 for homogeneity; Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic), for ischaemic stroke only, the RRR was 67% (95% CI: 54 77%) VKA = vitamin K antagonist Hart RG et al. Ann Intern Med 2007;146: April Mar

33 33 Mar 2013
34 Updated slide ASA inferior to warfarin for stroke prevention in AF Warfarin better ASA better AFASAK I AFASAK II Chinese ATAFS EAFT PATAF SPAF II Age 75 yrs Age >75 yrs All trials RRR: 38%* (95% CI: 18 52%) RRR (%) Random effects model; error bars = 95% CI; *P>0.2 for homogeneity; Relative risk reduction (RRR) for all strokes (ischaemic and haemorrhagic); ASA = acetylsalicylic acid Hart RG et al. Ann Intern Med 2007;146: April Mar
35 Warfarin safer than aspirin at any age 35 Mar 2013
36 New slide Real-world data highlights ASA limitations Registry data highlights increased risk of thromboembolism with ASA vs VKA (n= ) * Compared with VKA, no additional benefit observed with VKA + ASA HR (95% CI) vs VKA for thromboembolism in highthromboembolic-risk patients ASA VKA + ASA No treatment Favours comparator Favours VKA Risk of bleeding increased with VKA, ASA, and VKA + ASA vs no treatment ASA alone was not associated with a positive net clinical benefit *Registry data for all patients with nonvalvular AF in Denmark ASA = acetylsalicylic acid; HR = hazard ratio; VKA = vitamin K antagonist Olesen JB et al. Thromb Haemost 2011;106: April Mar
37 Bleeds/year Bleeds/year Risk of major and intracranial bleeding not significantly different between ASA and OAC New slide Intracranial bleeding Major bleeding OAC (n=48599) ASA (n=61396) HAS-BLED total score* HAS-BLED total score* *Modified HAS-BLED score used in this study: 1 point each for systolic blood pressure <160 mmhg, renal dysfunction, liver dysfunction, stroke, bleeding, age >65 years, drugs affecting bleeding or alcohol abuse (maximum score = 7); score 0 2 indicates low bleeding risk, 3 indicates high bleeding risk; ASA = acetylsalicylic acid; OAC = oral anticoagulant Friberg L et al. Eur Hear J 2012:33: ; Pisters R et al. Chest 2010;138: April Mar
38 Cumulative event rate (% per year) SPAF III: adjusted-dose warfarin compared with low-intensity warfarin plus ASA 15 Ischaemic stroke or systemic embolism 10 Combination therapy Fixed-dose warfarin (INR )* & ASA (325 mg/d) 5 RRR 74% (95% CI: 50 87%) P< Adjusted-dose warfarin Warfarin (INR ) Years n= n= *Warfarin dose adjusted between 0.5 and 3.0 mg/day to achieve international normalized ratio (INR) when initiating therapy and then fixed for rest of study; ASA = acetyl salicylic acid; RRR = relative risk reduction SPAF Investigators. Lancet 1996;348: April Mar
39 Cumulative hazard rates ACTIVE W: dual antiplatelet therapy inferior to oral anticoagulation for stroke prevention in AF 0.05 All stroke RR 1.72 (95% CI: ) P=0.001 Dual antiplatelet therapy Clopidogrel (75 mg/d) & ASA ( mg/d) Oral anticoagulation VKA (target INR = ) Years n= n= For ischaemic stroke: RR 2.17 (95% CI: ) ASA = acetyl salicylic acid; INR = international normalized ratio; RR = relative risk; VKA = vitamin K antagonist ACTIVE Investigators. Lancet 2006;367: April Mar

40 How to start Warfarin in elderly 40 Mar 2013
41 New slide Challenges and limitations of VKAs Slow onset and offset of action Variability in dose response between individuals Subject to multiple food and drug interactions VKAs have many welldocumented limitations Anticoagulation reversal may not improve outcomes Narrow therapeutic window, requiring frequent monitoring ICH = intracranial haemorrhage; VKA = vitamin K antagonist Adapted from Connolly SJ et al. Circulation 2007;116: Risk of haemorrhage (particularly ICH) is high, and outcomes are poor 41 April Mar
42 The risks of ischemic stroke or intracranial bleed are high outside a narrow INR range Odds Ratio Adjusted odds-ratio for ischemic stroke and intracranial bleeding in relation to intensity of anticoagulation Ischaemic stroke risk Intracranial bleeding risk Ischaemic stroke risk Intracranial bleeding risk INR Fuster et al. Circulation 2011;123:e269-e367.Adapted from: Hylek and Singer. Ann Intern Med 1994;120: Oden et al. Thromb Res 2006;117:493-9.
43 Patients (%) Patients stop taking warfarin over time ~30% of AF patients treated with warfarin discontinued within 1 year (from a total population of 41,910 AF patients in the UK General Practice Research Database Patient age Age Age Age Age Age Age Time (years after starting treatment) Adapted from Gallagher et al. J Thromb Haemost 2008;6:1500-6
44 Patients (%) VKA therapy is underused Euro Heart Survey ( ): No VKA therapy in ~40% of AF patients who should be treated None Heparin only Antiplatelet Antiplatelet+VKA VKA (n=332) (n=697) (n=722) (n=371) (n=172) (n=72) (n=15) CHADS 2 score Adapted from Nieuwlaat et al. Eur Heart J 2006;27:
45 Patients unsuitable for VKAs (%) Many patients with AF unsuitable for treatment with VKAs Contraindications most frequent in elderly patients Often at greatest risk of stroke % 30 38% 37% % 0 >65 yrs 1 >65 yrs 2 >75 yrs 3 All ages 4 VKAs = vitamin K antagonists 1. Sudlow M et al. Lancet 1998;352: ; 2. Brass LM et al. Stroke 1997;28:2382 9; 3. Kalra L et al. Stroke 1999;30: ; 4. Go AS et al. Ann Intern Med 1999;131: April Mar
 29% 29% 15% 39% 29% 10% 2% 25% 3% 18% Sub therapeutic warfarin (INR <2.")
 Single antiplatelet therapy Data from a prospective stroke registry of 597 patients with AF INR = international normalized ratio; TIA =")
46 Most ischaemic strokes occur in patients who are under-anticoagulated >70% of ischaemic stroke patients with AF had an INR <2.0 Only 10% were within the therapeutic range (INR 2.0) 29% 29% 15% 39% 29% 10% 2% 25% 3% 18% Sub therapeutic warfarin (INR <2.0) Dual antiplatelet therapy No antithrombotics Therapeutic warfarin (INR 2.0) Single antiplatelet therapy Data from a prospective stroke registry of 597 patients with AF INR = international normalized ratio; TIA = transient ischaemic attack Gladstone DJ et al. Stroke 2009;40: April Mar
47 OAC use, CHADS 2 2 (% patients) Global AF registry: use of oral anticoagulants was low and varied between regions 100 Patients with a prior history of AF *P vs North America * 40 * * * * * 20 * 0 North America South America Western Europe Eastern Europe Middle East Africa India China Asia CHADS 2 = Congestive heart failure, Hypertension, Age 75 years, Diabetes mellitus, prior Stroke, or TIA (2); OAC = oral anticoagulation; TIA = transient ischaemic attack Healey J et al. ESC 2011; e-slides available at (accessed September 2011) 47 April 2012

48
49 INR Most strokes in patients on VKAs occur if patients are outside recommended INR ranges Updated slide Target INR range for study ACC/AHA/ESC recommended INR ( ) Stroke event 1.0 AFASAK CAFA SPAF BAATAF SPINAF ACC = American College of Cardiology; AHA = American Heart Association; ESC = European Society of Cardiology; INR = international normalized ratio; VKA = vitamin K antagonist Levi M et al. Semin Thromb Haemost 2009;35: April Mar
50 Strokes can still occur if patients are within recommended INR ranges INR Updated slide Target INR range for study ACC/AHA/ESC recommended INR ( ) Stroke event 1.0 AFASAK CAFA SPAF BAATAF SPINAF ACC = American College of Cardiology; AHA = American Heart Association; ESC = European Society of Cardiology; INR = international normalized ratio Levi M et al. Semin Thromb Haemost 2009;35: April Mar

")
51 Probability of event by 1 year plus point-wise 95% CI Probability of stroke/non-cns embolism according to cttr Piccini et al., J Am Heart Assoc, 2014 Center TTR (%) calculated from center INR values

52 So what shall we recommend?
53 Summary of the global unmet needs 100 persons with AF ~ One half receive a VKA 1 ~ One half are adequately treated 2 Few are still on treatment at six years 3 Effective, safer and more convenient therapies are urgently needed 1. Nieuwlaat et al. Eur Heart J 2006;27: Healey et al. Presented at the ESC meeting (Sunday August 28, 2011) Gallagher et al. J Thromb Haemost 2008;6: EU API234 Subject to local prior approval by BMS/Pfizer, as per relevant SOP and local rules, slide may be used with external audiences in local BMS/Pfizer arranged meetings
54 Mar
55 Direct thrombin inhibitors (DTIs) block both circulating and clot-bound thrombin Thrombin generation Heparin Antithrombin DTIs: dabigatran etexilate ximelagatran* AZD0837 Conversion of fibrinogen to fibrin Amplification DTIs: dabigatran etexilate ximelagatran* AZD0837 Clot-bound thrombin *Withdrawn from the market in 2006 DTI = direct thrombin inhibitor Adapted from Eikelboom J et al. J Am Coll Cardiol 2003;41:70S 8S Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details 55 April Mar
56 Direct and indirect FXa inhibition INDIRECT Binds to AT and potentiates the activity of AT against FXa (e.g. idraparinux, SSR ) DIRECT Binds directly to the active site of FXa, blocking substrate interactions (e.g. apixaban, rivaroxaban, edoxaban, betrixaban) Direct FXa inhibitor AT AT AT FXa FXa Indirect FXa inhibitor II Thrombin AT = antithrombin; FXa = Factor Xa Adapted from Turpie AG et al. N Engl J Med 2001;344: Fibrinogen Fibrin clot Disclaimer: Edoxaban and betrixaban are not approved for clinical use in stroke prevention in atrial fibrillation. Rivaroxaban and Apixaban are approved in this indication in certain countries. Please check local prescribing information for further details 56 April Mar
57 The promise of new oral anticoagulants Simplified dosing regimen No dietary restrictions Predictable anticoagulation and no need for routine coagulation monitoring Can be given at fixed doses Reduced potential for food and drug interactions Less labour-intensive Less impact on patients daily life Improved compliance Reduced administrative costs Improved quality of life Improved efficacy and safety 1. Raghaven N et al. Drugs Metab Dispos 2009;37:74 81; 2. Shantsila E, Lip GY. Curr Opin Investig Drugs 2008;9: ; 3. Mueck W et al. Clin Pharmacokinet 2008;47: ; 4. Mueck W et al. Thromb Haemost 2008;100: ; 5. Mueck W et al. Int J Clin Pharmacol Ther 2007;45:


58 Study design and inclusion ROCKET AF 1 RE-LY 2 ARISTOTLE 3,6 AVERROES 4 ENGAGE AF- TIMI 48 5 No. of patients Statistical objective No. study arms 14,264 18,113 18,201 5,599 20,500 Non-inferiority Noninferiority Noninferiority Superiority Non-inferiority Study drug Control AF type of pts included Double-blind rivaroxaban Double-blind warfarin (INR 2 3) Non-valvular Two doses of double-blind dabigatran Open-label warfarin (INR 2 3) Non-valvular Double-blind Apixaban Double-blind warfarin (INR 2 3) All except mechanical valves Double-blind apixaban Double-blind ASA Non-valvular 1. Patel MR et al, 2011; 2. Connolly SJ et al, 2009; 3. Lopes RD et al, 2010; 4. Connolly SJ et al, 2011; 5. Ruff CT et al, 2010; 6.Granger CB et al, Two doses of double-blind edoxaban Double-blind warfarin (INR 2 3) Non-valvular 58
59 Comparison of the pharmacological characteristics of newer OACs Parameter Dabigatran Rivaroxaban Apixaban Edoxaban Target Thrombin Factor Xa Factor Xa Factor Xa Oral bioavailability 6.5% %* ~66% 50% Plasma protein binding 34 35% 92 95% 87% 40 59% Dosing (for SPAF indication) *After oral ingestion Routine coagulation monitoring Fixed, twice daily Fixed, once daily Fixed, twice daily Fixed, once daily Prodrug Yes No No No Half-life (h) (young healthy) (elderly) T max (h) ~ No No No No Eriksson BI et al, 2011; Frost et al, 2007; Kubitza D et al, 2005; Kubitza D et al, 2005; Ogata K et al, 2010; Stangier et al, 2005; Raghavan N et al, 2009; Xarelto SmPC 2011; Xarelto PI 2011; Pradaxa SmPC 2011; Eliquis SmPC 2011; Dabigatran PI; ROCKET AF Investigators 2010; Lopes et al, 2010; Ruff et al,
60 Comparison of the pharmacological characteristics of new OACs Parameter Dabigatran Rivaroxaban Apixaban Edoxaban Renal clearance 80% 33%; additional 33% cleared after metabolic degradation to inactive drug Potential drug interactions Rifampicin, quinidine, amiodarone, potent P-gp inhibitors Potent inhibitors of both CYP3A4 and P-gp*, strong inducers of CYP3A4 ~25% 35% Potent CYP3A4 inhibitors* Potent inhibitors of both CYP3A4 and P-gp *CYP, cytochrome P-450 isoenzymes; P-gp, P-glycoprotein. Strong inhibitors of both CYP3A4 and Pgp include azole antifungals (e.g., ketoconazole, itraconazole, voriconazole, posaconazole) and protease inhibitors, such as ritonavir. Eriksson BI et al, 2011; Xarelto Summary of Product Characteristics
61 OAC therapy in patients with renal impairment Newer anticoagulants are partially cleared via the renal route 1 However, not all new anticoagulants rely on this route to the same extent 1 Excreted unchanged Rivaroxaban 2 Apixaban 3 Edoxaban 4 Dabigatran etexilate 5 Via kidney ~33%* ~25% # 35% ~80% Potentially managed via dose adjustment *Additional 33% cleared renally after metabolic degradation to inactive drug 6 # Estimated percentage of the orally administered dose Mean percentage after intravenous administration within the first 24 hours of dosing Contraindicated in patients with severe renal impairment 1. Eriksson BI et al, 2011; 2. Weinz C et al, 2009; 3. Raghavan N et al, 2008; 4. Ogata K et al, 2010; 5. Blech S et al, 2008; 6. Xarelto Summary of Product Characteristics
62 Dosing and dose evaluation for special populations ROCKET AF 1 RE-LY 2 ARISTOTLE 3 & AVERROES 4 ENGAGE AF-TIMI 48 5 Rivaroxaban Dabigatran Apixaban Edoxaban 20 mg od (15 mg od) 110 mg bid or 150 mg bid (randomized to two separate arms) 5 mg bid (2.5 mg bid) 30 mg od (15 mg od) or 60 mg od (30 mg od) (randomized to two separate arms) Dose adjustment for patients with: Moderate renal impairment CrCl ml/min No dose adjustment Dose adjustment for patients fulfilling 2 of the following criteria at baseline: Age 80 years Body weight 60 kg Serum creatinine 1.5mg/dl (133 µmol/l) Dose adjustment for patients fulfilling 1 of the following criteria at baseline: Concomitant verapamil or quinidine Body weight 60 kg CrCl ml/min 1. Patel MR et al, 2011; 2. Connolly SJ et al, 2009; 3. Lopes RD et al, 2010; 4. Connolly SJ et al, 2011; 5. Ruff CT et al,
63 Dosing for prevention of stroke in NVAF The recommended dose of apixaban is 5 mg taken orally twice daily (BD), swallowed with water, with or without food. Age 80 years Body weight 60 kg Serum creatinine 1.5 mg/dl (133 µmol/l) Dose Adjustment to 2.5mg BD At least 2 characteristics Severe renal impairment alone (CrCl: ml/min) Apixaban 2.5mg BD Prior to initiating apixaban, liver function testing should be performed If a dose is missed, the patient should take apixaban immediately and then continue with twice daily intake as before Apixaban SmPC EU API234 Subject to local prior approval by BMS/Pfizer, as per relevant SOP and local rules, slide may be used with external audiences in local BMS/Pfizer arranged meetings
64 NOAC Efficacy vs. Warfarin Not head to head comparison For illustrative purposes only ARISTOTLE RELY ROCKET-AF

65 Patient Characteristics Across Trials 30-40% elderly patients * # *CHF or LVEF 40%; #CHF or LVEF 35% Notably higher rates of diabetes, CHF, and prior stroke in ROCKET population Connolly N Engl J Med 2009;361:1139; Patel N Engl J Med :883;Granger N Engl J Med 2011;365:981; Ruff Am Heart J 2010;160:635

66 CHADS 2 Distribution Across Trials % CHADS 2 Score Dabigatran and apixaban: evaluated across a spectrum of stroke risk categories Rivaroxaban: evaluated in patients at high risk of stroke Connolly N Engl J Med 2009;361:1139; Patel N Engl J Med :883; Granger N Engl J Med 2011;365:981; Ruff Am Heart J 2010;160:635
67 Phase III trials vs. warfarin (aim INR ) RELY ROCKET ARISTOTLE Sample size 18,113 14,266 18,201 New treatment Design Dabigatran 110mg BID Dabigatran 150mg BID Non-inferiority PROBE Rivaroxaban 20mg QD Non-inferiority Double-blind TTR- Warfarin Apixaban 5mg BID Non-inferiority Double-blind Patients AF + CHADS2 1 AF + CHADS2 2 AF + CHADS2 1 Primary outcome Stroke (ischemic or hemorrhagic) or systemic embolism Stroke (ischemic or hemorrhagic) or systemic embolism Stroke (ischemic or hemorrhagic) or systemic embolism Safety outcome Primary: Major Bleeding Primary: Major Bleeding Primary: Major Bleeding Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011; ENGAGE- AF Study Investigators. AHJ 2010

68 Efficacy and safety in elderly

69

70

71
72 New antithrombotic therapies compared to warfarin Stroke or systemic embolism Dabigatran 150 mg b.i.d. Dabigatran 110 mg b.i.d. Rivaroxaban 20 mg o.d. Abixaban 5 mg b.i.d Favors NOAC Favors warfarin Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011
73 New antithrombotic therapies compared to warfarin Stroke of ischemic or unknown origin Dabigatran 150 mg b.i.d. Dabigatran 110 mg b.i.d. Rivaroxaban 20 mg o.d. Abixaban 5 mg b.i.d Favors NOAC Favors warfarin Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011
74 New antithrombotic therapies compared to warfarin All-cause mortality Dabigatran 150 mg b.i.d. Dabigatran 110 mg b.i.d. Rivaroxaban 20 mg o.d. Abixaban 5 mg b.i.d Favors NOAC Favors warfarin Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011
75 New antithrombotic therapies compared to warfarin Major bleeding Dabigatran 150 mg b.i.d. Dabigatran 110 mg b.i.d. Rivaroxaban 20 mg o.d. Abixaban 5 mg b.i.d Favors NOAC Favors warfarin Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011
76 New antithrombotic therapies compared to warfarin Gastrointestinal bleeding Dabigatran 150 mg b.i.d. Dabigatran 110 mg b.i.d. Rivaroxaban 20 mg o.d. Abixaban 5 mg b.i.d Favors NOAC Favors warfarin Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011
77 New antithrombotic therapies compared to warfarin Intracranial hemorrhage Dabigatran 150 mg b.i.d. Dabigatran 110 mg b.i.d. Rivaroxaban 20 mg o.d. Abixaban 5 mg b.i.d Favors NOAC Favors warfarin Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011
78 New antithrombotic therapies compared to warfarin Myocardial infarction Dabigatran 150 mg b.i.d. Dabigatran 110 mg b.i.d. Rivaroxaban 20 mg o.d. Abixaban 5 mg b.i.d Favors NOAC Favors warfarin Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011
79 ESC 2012 recommandations Choice of anticoagulant Non-valvular AF Valvular AF* Yes <65 years & lone AF (including female) No Assess risk of stroke (CHA 2 DS 2 -VASc score) VKA *Includes rheumatic valvular disease and prosthetic valves OAC therapy No antithrombotic therapy Assess bleeding risk (HAS-BLED score) Consider patient values and preferences NOAC** VKA **NOAC should be considered instead of VKA (INR 2 3) for most patients with AF. Adapted from Camm et al. Eur Heart J 2012;e-published August 2012, doi: /eurheartj/ehs253.
80 ESC 2012 recommendations Antithrombotic therapy Recommandations Class Level Antithrombotic therapy to prevent thromboembolism is recommended for all patients with AF, except in those patients (both male and female) who are at low risk (aged <65 years and lone AF), or with contraindications. I A The choice of antithrombotic therapy should be based upon the absolute risks of stroke / thromboembolism and bleeding and the net clinical benefit for a given patient. I A When patients refuse the use of any OAC (whether VKAs or NOACs), antiplatelet therapy should be considered, using combination therapy with ASA mg plus clopidogrel 75 mg daily (where there is a low risk of bleeding) or - less effectively - ASA mg daily. IIa B Camm et al. Eur Heart J 2012;e-published August 2012, doi: /eurheartj/ehs253. EU API234 Subject to local prior approval by BMS/Pfizer, as per relevant SOP and local rules, slide may be used with external audiences in local BMS/Pfizer arranged meetings

81 Recommended work chart for choosing anticoagulants 81 Mar 2013
82 Cumulative event rate (%) Primary efficacy outcome: time to first event Rivaroxaban N=2419 Enoxaparin/VKA N=2413 HR=1.12; p< (non-inferiority) Time to event (days) Number of patients at risk Rivaroxaban Enoxaparin/VKA ITT population
83 Cumulative event rate (%) Major bleeding Enoxaparin/VKA N= Time to event (days) Rivaroxaban N=2412 Number of patients at risk Rivaroxaban Enoxaparin/VKA Safety population
84 ESC 2012 guidelines: management of bleeding with new oral anticoagulants Patient on a new OAC presenting with bleeding Check haemodynamic status, basic coagulation tests to assess anticoagulation effect Minor Delay next dose or discontinue treatment Moderate Symptomatic/supportive treatment Mechanical compression Fluid replacement Blood transfusion Oral charcoal if recently ingested Very severe Consider rfviia or PCC Charcoal filtration Dabigatran only: haemodialysis Camm AJ et al. Eur Heart J 2012

85 So what have we learned?

86 conclusion 86 Mar 2013
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
Aims. AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies
 in non-valvular AF (NVAF) Practical Issues Patient Case Studies") Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies AF and Stroke AF prevalence approx doubles with each
Aims AF and Stroke risk Guidance re anticoagulation Novel oral anticoagulants (NOACs) in non-valvular AF (NVAF) Practical Issues Patient Case Studies AF and Stroke AF prevalence approx doubles with each
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS?
 IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS? J.Y. LE HEUZEY Georges Pompidou Hospital, René Descartes University, Paris H E G P Munich, August 27, 2012 Disclosure Consultant / Conferences / Advisory
IS THERE STILL A PLACE FOR VITAMINE K ANTAGONISTS? J.Y. LE HEUZEY Georges Pompidou Hospital, René Descartes University, Paris H E G P Munich, August 27, 2012 Disclosure Consultant / Conferences / Advisory
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients. Giancarlo Agnelli
 NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
Scoring Systems in AF 8/10/2016. Strategies in the Prevention of Atrial Fibrillation-Related Strokes. Overview
 Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Thrombosis and Thromboembolsim October Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy
 Thrombosis and Thromboembolsim October 2012 Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy Christian T. Ruff, MD, MPH TIMI Study Group Brigham and Women
Thrombosis and Thromboembolsim October 2012 Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy Christian T. Ruff, MD, MPH TIMI Study Group Brigham and Women
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Lessons from recent antithrombotic studies and trials in atrial fibrillation
 Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated?
 Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated? Renato D. Lopes, MD MHS PhD Professor of Medicine Division of Cardiology Duke Clinical
Identifying Patients for Anticoagulation: While Many Patients Remain Untreated, Who Should NOT be Anticoagulated? Renato D. Lopes, MD MHS PhD Professor of Medicine Division of Cardiology Duke Clinical
KCS Congress: Impact through collaboration
 Stroke Prevention in Atrial Fibrillation (SPAF) in Kenya Elijah N. Ogola FACC University of Nairobi Kenya Cardiac Society Annual Scientific Congress Mombasa 28 th June 1 st July 2017 KCS Congress: Impact
Stroke Prevention in Atrial Fibrillation (SPAF) in Kenya Elijah N. Ogola FACC University of Nairobi Kenya Cardiac Society Annual Scientific Congress Mombasa 28 th June 1 st July 2017 KCS Congress: Impact
New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy
 New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy Hans-Christoph Diener Department of Neurology and Stroke Center University Hospital Essen Germany Conflict of Interest
New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy Hans-Christoph Diener Department of Neurology and Stroke Center University Hospital Essen Germany Conflict of Interest
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Evaluate Risk of Stroke & Bleeding in AF Patients
 XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
Results from RE-LY and RELY-ABLE
 Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Antithrombotic Efficacy and Safety of Dabigatran Etexilate
 130419 Luncheon Symposium_2013 춘계심장학회 Antithrombotic Efficacy and Safety of Dabigatran Etexilate Hui-Nam Pak, MD, PhD. Division of Cardiology Yonsei University Health System Atrial Fibrillation Risk of
130419 Luncheon Symposium_2013 춘계심장학회 Antithrombotic Efficacy and Safety of Dabigatran Etexilate Hui-Nam Pak, MD, PhD. Division of Cardiology Yonsei University Health System Atrial Fibrillation Risk of
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016
 1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
A Patient Unsuitable for VKA Treatment
 Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Stepheny Sumrall, FNP, AGACNP Cardiovascular Clinic of Hattiesburg
 Novel Oral Anticoagulants Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for the Treatment of Atrial Fibrillation and Prevention of Stroke Stepheny Sumrall,
Novel Oral Anticoagulants Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for the Treatment of Atrial Fibrillation and Prevention of Stroke Stepheny Sumrall,
Old and New Anticoagulants For Stroke Prevention Benefits and Risks
 Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
controversies in anticoagulation: optimizing outcome for atrial fibrillation
 controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
Survey patients for Sx, signs of AF. Establish AF Dx. Evaluate & Tx underlying heart disease/other causes. Assess adequacy of rate or rhythm control
 Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Suggested General Approach to Managing Atrial Fibrillation Survey patients for Sx, signs of AF Establish AF Dx ECG Holter Event monitor Implanted device (pacer) Determine & Tx stroke risk (CHA 2 DS 2 VASc)
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
ADVANCES IN ANTICOAGULATION
 ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
Anticoagulant therapy, coumadines or direct antithrombins
 ATRIAL FIBRILLATION (AF) Anticoagulant therapy, coumadines or direct antithrombins Felicita Andreotti, MD PhD Aggregated Professor Dept of Cardiovascular Sciences, Catholic University, Rome, IT Consultant
ATRIAL FIBRILLATION (AF) Anticoagulant therapy, coumadines or direct antithrombins Felicita Andreotti, MD PhD Aggregated Professor Dept of Cardiovascular Sciences, Catholic University, Rome, IT Consultant
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
Novel Anticoagulants PHYSICIANS UPDATE 2014
 Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto
 Fibrillazione atriale: rischio tromboembolico, Venezia - 27/28 Novembre 2015 Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto Antonio Raviele, MD, FESC,
Fibrillazione atriale: rischio tromboembolico, Venezia - 27/28 Novembre 2015 Stratificazione del rischio, corretto bilancio tra ischemia e bleeding: il beneficio clinico netto Antonio Raviele, MD, FESC,
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Updates in Management of Venous Thromboembolic Disease
 Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention
 Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania
Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis
 Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Disclosures. Practical Considerations for Anticoagulation for Prevention of Venous Thromboembolism and Stroke Due to Atrial Fibrillation
 12:45 1:45 pm Practical Considerations for Anticoagulation for Prevention of Venous Thromboembolism and Stroke Due to Atrial Fibrillation SPEAKER Christian Ruff, MD, MPH Presenter Disclosure Information
12:45 1:45 pm Practical Considerations for Anticoagulation for Prevention of Venous Thromboembolism and Stroke Due to Atrial Fibrillation SPEAKER Christian Ruff, MD, MPH Presenter Disclosure Information
Atrial Fibrillation. Alan Bell, MD, CCFP. Staff Physician, Humber River Regional Hospital. University of Toronto
 Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012
 Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012 Professor Dan Atar Head, Dept. of Cardiology Councillor of the ESC,
Secondary Preven-on of Thromboembolic Stroke: Clinical Data and Recommenda-ons from the ESC Atrial Fibrilla-on Guideline Update 2012 Professor Dan Atar Head, Dept. of Cardiology Councillor of the ESC,
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Pharmacologic Agents to Prevent Stroke in Non-Valvular Atrial Fibrillation and PFO
 Pharmacologic Agents to Prevent Stroke in Non-Valvular Atrial Fibrillation and PFO Gregg W. Stone, MD Columbia University Medical Center The Cardiovascular Research Foundation Disclosures None Risk of
Pharmacologic Agents to Prevent Stroke in Non-Valvular Atrial Fibrillation and PFO Gregg W. Stone, MD Columbia University Medical Center The Cardiovascular Research Foundation Disclosures None Risk of
RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION
 FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION") RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION Craig I. Coleman, PharmD Professor, University of Connecticut School
RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION Craig I. Coleman, PharmD Professor, University of Connecticut School
Dr. Khalid Khan Consultant Cardiologist
 Dr. Khalid Khan Consultant Cardiologist BCUHB (Wrexham) WCS Spring Meeting 2012 When the pulse is irregular and tremulous and the beats occur at intervals, then the impulse of life fades; when the pulse
Dr. Khalid Khan Consultant Cardiologist BCUHB (Wrexham) WCS Spring Meeting 2012 When the pulse is irregular and tremulous and the beats occur at intervals, then the impulse of life fades; when the pulse
Modern Management in Primary Care (AF1)
") Modern Management in Primary Care (AF1) Dr Ravi Assomull Consultant Cardiologist London North West Healthcare NHS Trust Dr Yassir Javaid Primary Care Cardiovascular Lead East Midlands Strategic Clinical
Modern Management in Primary Care (AF1) Dr Ravi Assomull Consultant Cardiologist London North West Healthcare NHS Trust Dr Yassir Javaid Primary Care Cardiovascular Lead East Midlands Strategic Clinical
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
PRESENTATION TITLE. Case Studies
 PRESENTATION TITLE Case Studies 1) SH is a 67 year old male. He has a history of type 2 diabetes, controlled hypertension and peripheral artery disease. He takes naproxen 500mg bd for arthritis and admits
PRESENTATION TITLE Case Studies 1) SH is a 67 year old male. He has a history of type 2 diabetes, controlled hypertension and peripheral artery disease. He takes naproxen 500mg bd for arthritis and admits
Engage AF-TIMI 48. Edoxaban in AF: What can we expect? Cardiology Update John Camm. St. George s University of London United Kingdom
 Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS
: COMPARISON AND FREQUENTLY ASKED QUESTIONS") NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China
 AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China Case report 64-year-old Chinese man with history of hypertension,
AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China Case report 64-year-old Chinese man with history of hypertension,
Chapter 1 Introduction
 Chapter 1 Introduction There are several disorders which carry an increased risk of thrombosis, clots that interfere with normal circulation, including: venous thromboembolism (VTE), comprising both deep
Chapter 1 Introduction There are several disorders which carry an increased risk of thrombosis, clots that interfere with normal circulation, including: venous thromboembolism (VTE), comprising both deep
NOAC vs. Warfarin in AF Catheter Ablation
 KHRS 2013 2013-Jun-15 NOAC vs. Warfarin in AF Catheter Ablation Jin-Seok Kim, MD Department of Cardiology Sejong General Hospital Bucheon, Republic of Korea Clinical Burden of AF Rhythm Disturbance Thromboembolic
KHRS 2013 2013-Jun-15 NOAC vs. Warfarin in AF Catheter Ablation Jin-Seok Kim, MD Department of Cardiology Sejong General Hospital Bucheon, Republic of Korea Clinical Burden of AF Rhythm Disturbance Thromboembolic
Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali
 Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali Gianluca Botto, MD, FAAC, FESC Divisione di Cardiologia Ospedale Sant Anna, Como The Promise of NOAs Antithrombotic
Fibrillazione Atriale Non Valvolare: Come Orientare La Scelta Dei Nuovi Anticoagulanti Orali Gianluca Botto, MD, FAAC, FESC Divisione di Cardiologia Ospedale Sant Anna, Como The Promise of NOAs Antithrombotic
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS
 NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
TSHP 2014 Annual Seminar 1
 Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Anticoagulation: Novel Agents
 Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
Draft Agreed by Cardiovascular Working Party 25 Jan Adoption by CHMP for release for consultation 17 Feb 2011
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 London, 25 January 2011 EMA/CHMP/68875/2011 Committee for Medicinal Products for Human Use (CHMP) Concept paper on the need for a guideline on clinical investigation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 London, 25 January 2011 EMA/CHMP/68875/2011 Committee for Medicinal Products for Human Use (CHMP) Concept paper on the need for a guideline on clinical investigation
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care
 Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care 11 th and 25 th September 2014 3 KEY OBJECTIVES OF TALK 1.
Initial assessment of patient with AF in primary care DR BRUCE TAYLOR GPwSI Cardiology SCN Merseyside and Cheshire Clinical Lead Primary care 11 th and 25 th September 2014 3 KEY OBJECTIVES OF TALK 1.
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Dabigatran Evidence in Real Practice
 ADVANCES IN CARDIAC ARRHYTHMIAS and GREAT INNOVATIONS IN CARDIOLOGY XXVII GIORNATE CARDIOLOGICHE TORINESI Torino, Centro Congressi Unione Industriale 23-24 Ottobre 2015 Dabigatran Evidence in Real Practice
ADVANCES IN CARDIAC ARRHYTHMIAS and GREAT INNOVATIONS IN CARDIOLOGY XXVII GIORNATE CARDIOLOGICHE TORINESI Torino, Centro Congressi Unione Industriale 23-24 Ottobre 2015 Dabigatran Evidence in Real Practice
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
Apixaban for stroke prevention in atrial fibrillation. August 2010
 Apixaban for stroke prevention in atrial fibrillation August 2010 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Apixaban for stroke prevention in atrial fibrillation August 2010 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Modeling the Risk of Stroke and Bleeding in Atrial Fibrillation: What Are the Optimal Risk Scores? Roxana Mehran, MD
 Modeling the Risk of Stroke and Bleeding in Atrial Fibrillation: What Are the Optimal Risk Scores? Roxana Mehran, MD Mount Sinai School of Medicine New York, NY Session II. Weighing the Risks and Benefits
Modeling the Risk of Stroke and Bleeding in Atrial Fibrillation: What Are the Optimal Risk Scores? Roxana Mehran, MD Mount Sinai School of Medicine New York, NY Session II. Weighing the Risks and Benefits
Defining Sub-Clinical Atrial Fibrillation and its management
 Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution
 Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Prepared by Pfizer-BMS alliance in response to an unsolicited request Not for further distribution AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
AF review. Petr Polasek
 AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
AF review Petr Polasek Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging
 and advances in peri-procedural interruption of anticoagulation-- Bridging") Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
NOAC trials for AF: A review
 NOAC trials for AF: A review Chern-En Chiang, MD, PhD, FACC, FESC General Clinical Research Center Division of Cardiology Taipei Veterans General Hospital National Yang-Ming University Taipei, Taiwan Presenter
NOAC trials for AF: A review Chern-En Chiang, MD, PhD, FACC, FESC General Clinical Research Center Division of Cardiology Taipei Veterans General Hospital National Yang-Ming University Taipei, Taiwan Presenter
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
Subclinical AF: Implications of device based episodes
 Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio
 Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio Medical University Objectives 1. 2. 3. 4. Review and discuss
Tim Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Akron General Medical Center for Family Medicine Professor, Northeast Ohio Medical University Objectives 1. 2. 3. 4. Review and discuss
Atrial Fibrillation Key Messages
 Atrial Fibrillation Key Messages Dr Matthew Fay Westcliffe Medical Practice National Clinical Lead NHS Improvement www.escardio.org/guidelines European Heart Journal (2010) 31, 2369-2429 Clinical Events
Atrial Fibrillation Key Messages Dr Matthew Fay Westcliffe Medical Practice National Clinical Lead NHS Improvement www.escardio.org/guidelines European Heart Journal (2010) 31, 2369-2429 Clinical Events
Arrhythmias and Clinical EP Contemporary Management of Anticoagulant Therapies
 Arrhythmias and Clinical EP Contemporary Management of Anticoagulant Therapies Samuel Asirvatham, MD & Ivan Mendoza, MD Saturday, June 24, 2017 11:15 a.m. to 12 p.m. Disclosures Relevant financial relationship(s)
Arrhythmias and Clinical EP Contemporary Management of Anticoagulant Therapies Samuel Asirvatham, MD & Ivan Mendoza, MD Saturday, June 24, 2017 11:15 a.m. to 12 p.m. Disclosures Relevant financial relationship(s)
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Anticoagulation Beyond Coumadin
 Anticoagulation Beyond Coumadin Saturday, September 21, 2013 Crystal Mountain Resort and Spa Pratik Bhattacharya MD, MPH Stroke Neurologist, Michigan Stroke Network; Assistant Professor of Neurology; Wayne
Anticoagulation Beyond Coumadin Saturday, September 21, 2013 Crystal Mountain Resort and Spa Pratik Bhattacharya MD, MPH Stroke Neurologist, Michigan Stroke Network; Assistant Professor of Neurology; Wayne
Atrial Fibrillation in the Emergency Department
 Atrial Fibrillation in the Emergency Department Disclosures Edward Jauch, MD MS Research support National Institutes of Health funding (multiple trials) Novo Nordisk (drug in kind) STOP-IT Study Genentech
Atrial Fibrillation in the Emergency Department Disclosures Edward Jauch, MD MS Research support National Institutes of Health funding (multiple trials) Novo Nordisk (drug in kind) STOP-IT Study Genentech
Modern management of atrial fibrillation, from blood pressure control to anticoagulation
 Modern management of atrial fibrillation, from blood pressure control to anticoagulation Adel Khalifa S. Hamad, BMS, MD, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist
Modern management of atrial fibrillation, from blood pressure control to anticoagulation Adel Khalifa S. Hamad, BMS, MD, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist
Atrial Fibrillation. E. Kevin Heist, MD, PhD. Updates in General Internal Medicine for Specialists January 28, 2019
 Atrial Fibrillation E. Kevin Heist, MD, PhD Updates in General Internal Medicine for Specialists January 28, 2019 Disclosures Abbott Consultant, Research Grant Biotronik Consultant Boston Scientific Consultant
Atrial Fibrillation E. Kevin Heist, MD, PhD Updates in General Internal Medicine for Specialists January 28, 2019 Disclosures Abbott Consultant, Research Grant Biotronik Consultant Boston Scientific Consultant
Optimal antithrombotic therapy for atrial fibrillation in the elderly patients Rossella Marcucci 21 ottobre 2011
 Optimal antithrombotic therapy for atrial fibrillation in the elderly patients Rossella Marcucci 21 ottobre 2011 Advances in cardiovascular arrhytmies and great innovations in cardiology XXIV Giornate
Optimal antithrombotic therapy for atrial fibrillation in the elderly patients Rossella Marcucci 21 ottobre 2011 Advances in cardiovascular arrhytmies and great innovations in cardiology XXIV Giornate
Dr Calum Young Cardiologist Tauranga
 Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated) GPCME 2016: Anticoagulation
Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated) GPCME 2016: Anticoagulation