Cardiopulmonary Failure: Management of the End Stage Patient "Transplant in Waiting
|
|
|
- Bruno Owens
- 5 years ago
- Views:
Transcription
1 Cardiopulmonary Failure: Management of the End Stage Patient "Transplant in Waiting David A. Hormuth, MD, MBA, FACS Chairman of Cardiothoracic Surgery Section St. Vincent Medial Group Evansville / Indianapolis Indiana
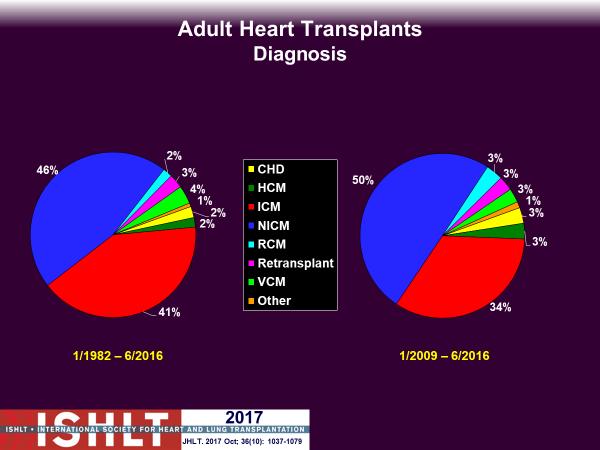
2 Thoracic Organ Transplantation has evolved to become the standard of care for patients with end stage cardiopulmonary failure The major issue affecting these patients include: Donor availability Distance from the transplanting center Deterioration while waiting
3 Transplant Candidate: Hormuth Clinically and physiologically severe disease Medical therapy ineffective or unavailable Substantial limitations in activities of daily living Limited life expectancy Adequate cardiac function without significant coronary disease Ambulatory, with rehabilitation potential Acceptable nutritional status Satisfactory psychosocial profile and emotional support system
4 Heart Transplant: Hormuth Common indications include: New York Heart Association (NYHA) class III or IV heart failure refractory to maximal medical therapy Debilitating ischemia not amenable to interventional or surgical revascularization Recurrent, symptomatic ventricular arrhythmias refractory to medical therapy, implantable cardioverter defibrillator (ICD) therapy, and surgical treatment
5
6 Defin
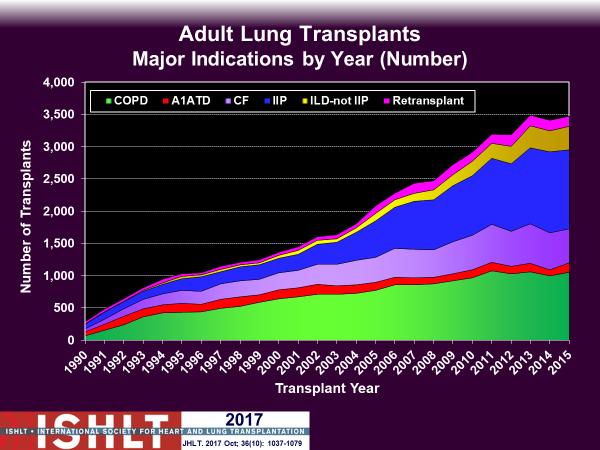
7 Lung Transplant: Hormuth Chronic Obstructive Pulmonary Disease Patients with a BODE index *of 7 to 10 or at least one of the following * BODE index includes body mass index, degree of airflow obstruction (assessed by percent predicted FEV 1 ), degree of dyspnea (assessed by the modified Medical Research Council [MMRC] dyspnea scale), and exercise capacity (assessed by the 6-minute walk distance). The index increases as body mass index, FEV 1, and distance walked decrease and as the MMRC scale increases History of hospitalization for exacerbation associated with acute hypercapnia (P co 2 >50 mm Hg) Pulmonary hypertension or cor pulmonale, or both, despite oxygen therapy FEV 1 < 20% predicted and either DLCO < 20% predicted or homogeneous distribution of emphysema
8 Lung Transplant: Hormuth Cystic Fibrosis and other Causes of Bronchiectasis Oxygen-dependent respiratory failure Hypercapnia Pulmonary hypertension
9 Lung Transplant: Hormuth Idiopathic Pulmonary Fibrosis and NSIP Histologic or radiographic evidence of usual interstitial pneumonia and any of the following: DLCO < 39% predicted 10% or greater decrement in FVC during 6 months of follow-up A decrease in pulse oximetry below 88% during a 6-MWT Honeycombing on high-resolution computed tomography (fibrosis score > 2) Histologic evidence of NSIP and any of the following: DLCO < 35% predicted 10% or greater decrement in FVC or 15% decrease in DLCO during 6 months of follow-up
10 Lung Transplant: Hormuth Pulmonary Arterial Hypertension Persistent New York Heart Association class III or IV on maximal medical therapy Low (< 350 m) or declining 6-MWT Failing therapy with intravenous epoprostenol or equivalent Cardiac index <2 L/min/m 2 Right atrial pressure >15 mm Hg
11 Acute Cardiac Failure
12

13 Defin Contemporary Medical Therapy for Heart Failure Patients with Reduced Ejection Fraction Robert J. Mentz, Douglas L. Mann and G. Michael Felker Heart Failure: A Companion to Braunwald's Heart Disease, 34,
14 Defin
15 Management of Acute Decompensated Heart Failure Lynne Warner Stevenson Heart Failure: A Companion to Braunwald's Heart Disease, 33,
16

17 Anatomic and Physiologic Aspects of the Pulmonary Vasculature Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 12,
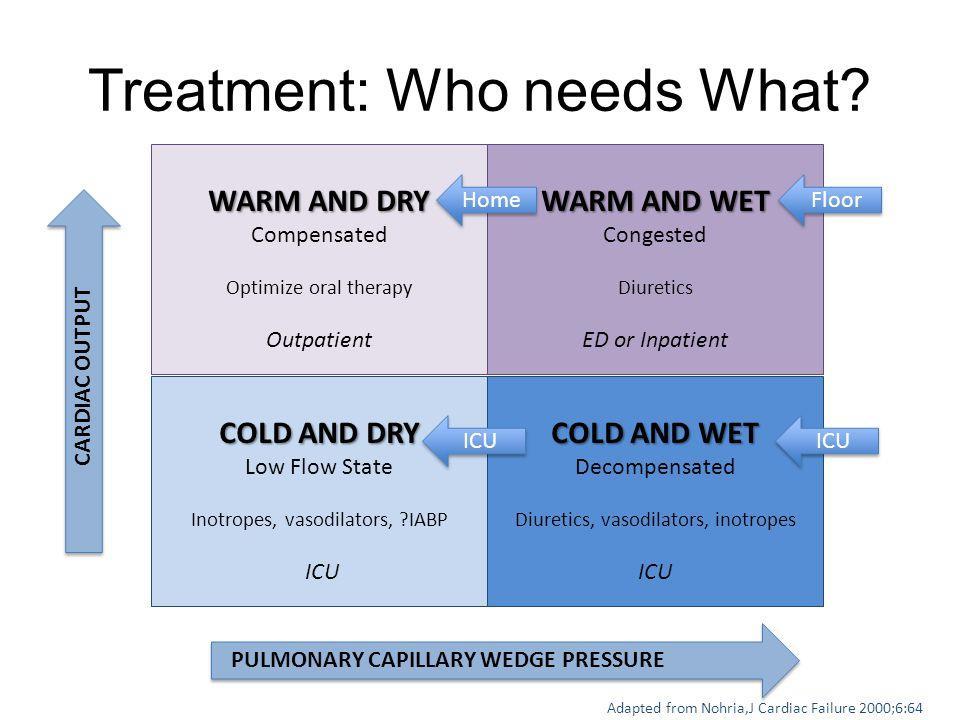
18 Indications for Invasive Hemodynamic Monitoring with Pulmonary Artery Catheter Acute Circulatory Compromise Diagnostic Uncertainty or Need for Escalating Therapies a. Whose fluid status, perfusion, or systemic or pulmonary vascular resistances are uncertain * b. Whose systolic pressure remains low or is associated with symptoms, despite initial therapy c. Whose renal function is worsening with therapy d. Who require parenteral vasoactive agents e. Who may need consideration for mechanical circulatory support or transplantation
19 Diuretics, intravenous vasodilators, and intravenous inotropic agents are the major medications used during acute management of decompensated heart failure Management of Acute Decompensated Heart Failure Lynne Warner Stevenson Heart Failure: A Companion to Braunwald's Heart Disease, 33, In the acutely ischemic ventricle, compliance is decreased with little change in volume, and the curve is shifted to the right. In the chronically dilated ventricle, the Starling curve is actually reversed in that reduction of markedly elevated filling pressures leads to higher stroke volume
20 Intravenous Vasodilators AGENT INITIAL DOSE EFFECTIVE DOSE RANGE Nitroglycerine 20 µg/min µg/min Nitroprusside 10 µg/min µg/min * Usually <4 µg/kg/min Nesiritide With or without 1- to 2-µg/kg bolus µg/kg/min
21 Intravenous Inotropic Agents AGENT INITIAL DOSE EFFECTIVE DOSE RANGE Dobutamine 1-2 µg/kg/min 2-10 µg/kg/min for inotropy and vasodilation Dopamine (augment Diuresis) 2µg/kg/min 2-4 µg/kg/min for inotropy and vasodilation Dopamine (treat hypotension) 4-5 µg/kg/min 5-15µg/kg/min for inotropy and vasoconstriction Milrinone 50 to 75 µg/kg bolus over 10 minutes µg/kg/min for inotropy and vasodilation
22
23 Acute Pulmonary Failure
24 (COPD) refers to chronic disorders that disturb airflow, whether the most prominent process is within the airways or within the lung parenchyma Emphysema is a diagnosis made on the basis of destruction of lung parenchyma and enlargement of air spaces distal to the terminal bronchiole Chronic bronchitis is a diagnosis made on the basis of chronic cough and sputum production Chronic Obstructive Pulmonary Disease Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 6,
25 Schematic diagram of the effect of smoking on airway inflammation and structural components of alveolar walls the latter by altering the relationship between elastase and α 1 -antitrypsin (also called α 1 -protease inhibitor ) Chronic Obstructive Pulmonary Disease Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 6,
26 Fletcher C, Peto R: The natural history of chronic air flow obstruction. Brit Med J 1977, 1:
27 COPD: Hormuth An acute exacerbation of chronic obstructive pulmonary disease (AECOPD) A clinical diagnosis made when a patient with COPD experiences a sustained (e.g., h) increase in cough, sputum production, and/or dyspnea The average experiences two episodes per year, and 10% of these episodes require hospitalization Data from the National Emphysema Treatment Trial show that patients with severe emphysema and who are eligible for lung volume reduction surgery have 6.1 days/year of hospitalization if they remain on medical therapy but only 3.2 days/year if given lung volume reduction surgery (P = 0.005)
28 COPD: Hormuth ETIOLOGY AND CONFOUNDING FACTORS Bacterial infections are implicated in the majority of AECOPD episodes Rhinovirus and respiratory syncytial virus have been implicated as causes for AECOPD in several studies Air pollution Acute left heart dysfunction was present in 25 30% of patients with AECOPD Pulmonary embolism About 30% of cases of AECOPD, no specific etiology could be identified
29 COPD: Hormuth Clinical manifestations of AECOPD using the THE WINNIPEG CRITERIA Type of Exacerbations Type 1 All three of the following symptoms: increase in sputum volume, increase in sputum purulence, increase in shortness of breath Type 2 Any two of the following symptoms: increase in sputum volume, increase in sputum purulence, increase in shortness of breath Type 3 Any one of the following symptoms: increase in sputum volume, increase in sputum purulence, increase in shortness of breath, plus at least one of the following: upper respiratory tract infection lasting 5 d, fever; increase in wheezes, increase in cough, increase in heart rate 20%riable
30 COPD: Hormuth Older age Severe underlying chronic obstructive pulmonary disease/already receiving long-term oxygen therapy Marked increase in breathlessness Poor or deteriorating general condition with little activity Cyanosis or worsening peripheral edema Impaired level of consciousness or confusion Difficulty in coping at home Significant comorbidities (particularly arrhythmias, heart failure, and insulin-dependent diabetes) Failure to respond to initial medical treatment Oxygen saturation < 90%

31 COPD/Heart Failure: Hormuth
: 56 61 Jelena Čelutkienė, Mindaugas Balčiūnas, Denis Kablučko, Liucija Vaitkevičiūtė, Jelena Blaščiuk,and Edvardas")
32 Challenges of Treating Acute Heart Failure in Patients with Chronic Obstructive Pulmonary Disease Card Fail Rev Apr; 3(1): Jelena Čelutkienė, Mindaugas Balčiūnas, Denis Kablučko, Liucija Vaitkevičiūtė, Jelena Blaščiuk,and Edvardas Danilacorresponding author COPD: Hormuth
33 Modalities available for treatment of COPD are: 1. Bronchodilators 2. Antibiotics 3. Corticosteroids 4. Phosphodiesterase-4 inhibitors 5. Supplemental oxygen 6. Exercise rehabilitation 7. Chest physiotherapy 8. Surgery (selected cases)
34 Pulmonary Fibrosis: Hormuth Idiopathic pulmonary fibrosis (IPF) is a progressive, life-threatening, interstitial lung disease of unknown etiology. IPF is the most common of the idiopathic interstitial pneumonias and carries the worst prognosis, with median survival ranging from 2.5 to 3.5 years Rate of decline and progression to death in patients with IPF may take several clinical forms: slow physiologic deterioration with worsening severity of dyspnea rapid deterioration and progression to death periods of relative stability interposed with periods of acute respiratory decline sometimes manifested by hospitalizations for respiratory failure
35 Acute Exacerbations of IPF (Acute exacerbation of IPF is defined by the onset of rapid deterioration (within days to a few weeks) in symptoms, lung function, and radiographic appearance (bilateral groundglass opacities and consolidation superimposed on a reticular pattern on HRCT) in the absence of infection, heart failure, pulmonary embolism, or other identifiable cause
36 Acute IPF exacerbations (within 4 wk., all of the following): Decline of 5% in resting room air SpO2 from last recorded level OR decline of 8 mm Hg in resting room air PaO2 from last recorded level Clinically significant worsening of dyspnea or cough within 30 d, triggering unscheduled medical care (e.g. clinic, study visit, hospitalization) New, superimposed ground-glass opacities or consolidation on CT scan or new alveolar opacities on chest radiograph No clinical (i.e., absence of grossly purulent sputum, fever > 39 C orally) or microbiologic evidence for infection Other causes excluded (e.g., pneumothorax, cardiac events, infections, and thromboembolism)
37 Progression of IPF 10% decrease in % predicted FVC or 15% decrease in % predicted DlCO/TlCO Confirmation of worsening must be documented with repeat assessments at least 4 wk apart American Journal of Respiratory and Critical Care Medicine Volume 183, Issue 4 February Clinical Course and Prediction of Survival in Idiopathic Pulmonary Fibrosis
38 Pathogenesis of AE-IPF It is not clear whether AE-IPF is secondary to acceleration of the primary disease process or represents a clinically silent trigger such as a viral infection or silent aspiration Presently AE-IPF lacks an effective treatment Bhatti H, Girdhar A, Usman F, Cury J, Bajwa A. Approach to acute exacerbation of idiopathic pulmonary fibrosis. Ann Thorac Med 2013;8:71-7
39
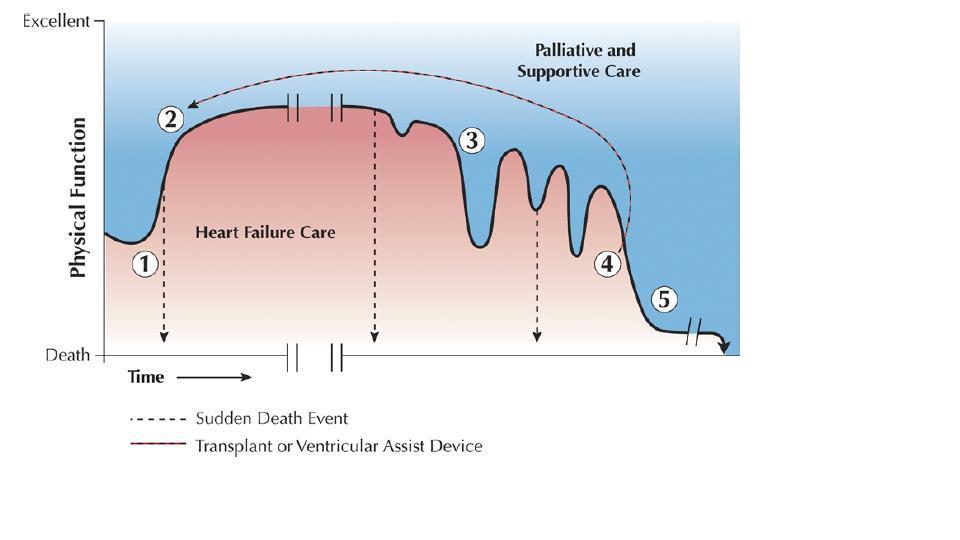
40 The Clinical Time Frame
41 Cystic Fibrosis: Hormuth Complex genetic disease affecting many organs, although 85% of the mortality is a result of lung disease Begins early in life with inflammation and impaired mucociliary clearance and consequent chronic infection of the airways There is progressive decline of lung function with episodes of acute worsening of respiratory Symptoms, often referred to as pulmonary exacerbations.
42 Cystic Fibrosis: Hormuth Clinical features of an exacerbation may include: increased cough Increased sputum production shortness of breath chest pain loss of appetite loss of weight lung function decline
43 Cystic Fibrosis: Hormuth Pulmonary exacerbations have an adverse impact on patients quality of life and a major impact on the overall cost of care Identifying optimal treatment methods for these events could produce significant improvements in quality and length of life for patients with CF
44 American Journal of Respiratory and Critical Care Medicine Volume 168, Issue 8 October Pathophysiology and Management of Pulmonary Infections in Cystic Fibrosis Cystic Fibrosis: Hormuth
45 Acute Pulmonary Failure

46 Defin Classification and Pathophysiologic Aspects of Respiratory Failure Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 27,
47 Definition of Respiratory Failure Inability of the respiratory system to maintain adequate gas exchange For patients with normal baseline arterial blood gas measurements, criteria for respiratory failure are P o 2 < 60 mm Hg or P co 2 > 50 mm Hg Categories of acute respiratory failure are: 1. Hypoxemic (with normal or low P co 2 ) 2. Hypercapnic/hypoxemic Classification and Pathophysiologic Aspects of Respiratory Failure Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 27,
48 Pulmonary Vascular Response to Hypoxia Alveoli in an area of lung contain gas with a low P o 2, generally less than 60 to 70 mm Hg, the vessels supplying that region of lung undergo vasoconstriction Protective mechanism for decreasing perfusion to poorly ventilated alveoli. Hypoxia may alter the release of vasoactive mediators, either increasing the release of vasoconstrictors or decreasing the release of vasodilators Nitric oxide, is produced by vascular endothelial cells, acts via increasing cyclic guanosine monophosphate to produce vascular smooth muscle relaxation
49 Clinical and Therapeutic Aspects of Hypercapnia/Hypoxemic Respiratory Failure Frequent precipitants of acute-on-chronic respiratory failure are: 1. Respiratory infection 2. Drugs (e.g., sedatives, narcotics) 3. Heart failure 4. Less common: pulmonary emboli, exposure to environmental pollutant Classification and Pathophysiologic Aspects of Respiratory Failure Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 27,
50 Therapeutic approach to these patients has three main components: (1) support of gas exchange (2) treatment of the acute precipitating event (3) treatment of the underlying pulmonary disease Classification and Pathophysiologic Aspects of Respiratory Failure Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 27,

51 Ventilation and hypercapnic respiratory failure Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 2, 11-21
52 Management strategies for patients with ARDS Identify and treat underlying/predisposing cause of ARDS Ventilatory support Lung protective ventilatory support strategy Application of PEEP (per ARDSnet protocol) Restore and maintain hemodynamic function Conservative fluid replacement strategy using goaloriented approach Vasopressor and inotropic support as needed to meet goal Acute Respiratory Failure David P. Gurka and Robert A. Balk Critical Care Medicine: Principles of Diagnosis and Management in the Adult, 37, e6
53 Management strategies for patients with ARDS Prevent complications of critical illness Stress ulcer (stress-related mucosal disease) prophylaxis Strategies for PE and DVT Prevent ventilator-associated pneumonia (VAP) Control glucose and metabolic function Prevent development of multiple organ dysfunction/failure Adequate nutrition Avoid over sedation and medication errors Use of weaning protocol with spontaneous breathing trials when ready to wean Cautious use of steroids for fibroproliferative phase (avoid if patient has received neuromuscular blocking drugs Acute Respiratory Failure David P. Gurka and Robert A. Balk Critical Care Medicine: Principles of Diagnosis and Management in the Adult, 37, e6

54 Acute hypoxemic respiratory failure An acute drop in Pa o 2 < 60 mm Hg Approach to oxygenation, hypoxemia, and hypoxemic respiratory failure Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 1, 1-10
55 Mechanical Ventilation: Hormuth The Goal of Invasive Mechanical Ventilation Provide adequate respiratory support Avoid causing ventilator-associated lung injury Lung-protective ventilation strategy low lung volumes (6 8 mg/kg) Prioritizes low lung volumes over normal ph and pco 2 [increasing the minute ventilation is done by increasing the rate, not the TV] Invasive mechanical ventilation Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 19,
56 Treatment Gridlines: Hormuth Mild chronic hypoxemic respiratory failure where PaO 2 falls gradually over time (typical PaO 2 values in the range) Caused by heterogeneous lung destruction, most commonly seen in chronic obstructive pulmonary disease (COPD) Hypoxemia occurs from VQ mismatch (pink puffers) or hypoventilation (blue bloaters) Causes mild symptoms of cognitive impairment (not exercise limitation), and increases the risk of heart failure In COPD Exercise is limited by ventilation Treat to prevent heart failure, arrhythmia, and risk of sudden death (not to improve exercise tolerance) Approach to oxygenation, hypoxemia, and hypoxemic respiratory failure Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 1, 1-10
57 Treatment Guidelines: Hormuth Chronic severe hypoxemic respiratory failure, Pa o 2 < 55 mm Hg Commonly seen in pulmonary fibrosis Fibrotic thickening of the pulmonary interstitium leads to diffusion limitation Less commonly caused by small vessel pulmonary vascular disease (eg, idiopathic pulmonary arterial hypertension [IPAH]) Loss of vascular cross-sectional area from obliteration of small to medium pulmonary arteriole Management of Acute Decompensated Heart Failure Lynne Warner Stevenson Heart Failure: A Companion to Braunwald's Heart Disease, 33,
58 Acute on Chronic Hypercapnic Respiratory Failure and Mixed Acute Hypercapnic Failure Acute on chronic hypercapnic respiratory failure Patients with chronic hypercapnic respiratory failure are extremely vulnerable to superimposed acute hypercapnic respiratory failure because they have no reserve (already have a baseline increase in their WOB or P co 2 ) An individual with COPD who develops a renal tubular acidosis (RTA), may experience respiratory failure from the increased MV demand An individual without lung disease, renal failure may only complain of fatigue and a decreased exercise tolerance when faced with a RTA Mixed acute hypercapnic failure Any combination of impaired pulmonary mechanics, metabolic acidosis, and blunted respiratory drive may (and commonly do) occur Ventilation and hypercapnic respiratory failure Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 2, 11-21

59 Invasive mechanical ventilation Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 19, Mechanical Ventilation: Hormuth

60 Invasive mechanical ventilation Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 19, Mechanical Ventilation: Hormuth

61 Invasive mechanical ventilation Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 19, Mechanical Ventilation: Hormuth

62 Invasive mechanical ventilation Judd W. Landsberg MD Clinical Practice Manual for Pulmonary and Critical Care Medicine, Chapter 19, Mechanical Ventilation: Hormuth
63 Cardiopulmonary Failure: Management of the End Stage Patient "Transplant in Waiting SUMMARY
64 Acute Heart Failure: Hormuth Optimize volume status (decongest, reduce pulmonary capillary wedge pressure) Optimize hemodynamics (improve low output state, increase cardiac index) Identify etiology Cause of heart failure (HF) Cause of acute decompensated heart failure (ADHF) Optimize long-term oral therapy Minimize therapeutic side effects and adverse treatment effects Identify indications for revascularization
65 Acute Heart Failure: Hormuth Identify indications for cardiac resynchronization therapy or implantable cardioverter-defibrillator or both Identify thromboembolism risk and need for anticoagulation Educate patient, family members, and caregivers about self-management Consider using disease management programs Consider referral for hospice
66 Management of Acute Decompensated Heart Failure Lynne Warner Stevenson Heart Failure: A Companion to Braunwald's Heart Disease, 33,
67 Diuretics, intravenous vasodilators, and intravenous inotropic agents are the major medications used during acute management of decompensated heart failure Management of Acute Decompensated Heart Failure Lynne Warner Stevenson Heart Failure: A Companion to Braunwald's Heart Disease, 33,
68 An exacerbation -acute event characterized by worsening of symptoms that requires a change in medication. The precipitating factor is often a respiratory tract infection of either viral or bacterial origin. A variety of bacteria are often chronically present in the tracheobronchial tree of patients with COPD, and an acute exacerbation can sometimes be due to the acquisition of a new strain of the colonizing bacteria. Other factors that cause acute deterioration in patients include exposure to air pollutants, bronchospasm (particularly if patients have a superimposed asthmatic component to their disease), and heart failure. However, in up to one-third of cases, the cause of an exacerbation cannot be identified. When exacerbations are severe, patients may go into frank respiratory failure Chronic Obstructive Pulmonary Disease Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 6,

69 The Clinical Time Frame
70 Overview of Diffuse Parenchymal Lung Diseases Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 9, Schematic diagram illustrates interrelationships between various pathologic and physiologic features of diffuse parenchymal lung disease
71
72
73 Thank You Questions??
74 Defin Chronic Obstructive Pulmonary Disease Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 6, The mounted section of the whole lung shows diffuse involvement seen with panacinar emphysema. (From Thurlbeck WM. Chronic Airflow Obstruction in Lung Disease. Philadelphia, PA: WB Saunders; 1976.)
75 A large group of disorders affects the alveolar wall in a fashion that ultimately may lead to diffuse scarring or fibrosis more than 150 diffuse parenchymal lung disease the diffuse parenchymal lung diseases, regardless of cause, have two major pathologic components: an inflammatory process in the alveolar wall and alveolar spaces (sometimes called an alveolitis ) and a scarring or fibrotic process Overview of Diffuse Parenchymal Lung Diseases Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 9,

76 Photomicrograph of diffuse parenchymal lung disease shows markedly thickened alveolar walls. Cellular inflammatory process and fibrosis are present Overview of Diffuse Parenchymal Lung Diseases Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 9,

77 Defin Overview of Diffuse Parenchymal Lung Diseases Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 9, Low-power photomicrograph of usual interstitial pneumonia shows prominent fibrosis accompanied by honeycombing
78 End-Stage Diffuse Parenchymal Lung Disease result of the inflammation and fibrosis affecting the alveolar walls (1) decreased compliance (increased stiffness) of the lung, (2) generalized decrease in lung volumes, (3) loss of alveolarcapillary surface area resulting in impaired diffusing capacity, (4) abnormalities in small airway function without generalized airflow obstruction, (5) disturbances in gas exchange, usually consisting of hypoxemia without CO 2 retention, and (6) in some cases, pulmonary hypertension. Overview of Diffuse Parenchymal Lung Diseases Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 9,
79 Overview of Diffuse Parenchymal Lung Diseases Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 9, Schematic diagram illustrates interrelationships between various pathologic and physiologic features of diffuse parenchymal lung disease
80

81 Management of Acute Decompensated Heart Failure Lynne Warner Stevenson Heart Failure: A Companion to Braunwald's Heart Disease, 33,
82 Acute Pulmonary Failure
83 Diuretics, intravenous vasodilators, and intravenous inotropic agents are the major medications used during acute management of decompensated heart failure Management of Acute Decompensated Heart Failure Lynne Warner Stevenson Heart Failure: A Companion to Braunwald's Heart Disease, 33,

84
85 Dietary and medication issues Progression of underlying heart disease Cardiac arrhythmias New ventricular dyssynergy Poorly controlled or uncontrolled hypertension Myocardial ischemia or infarction Progression of valvular heart disease Pulmonary disease Anemia Systemic infection Thyroid disorders Adverse effects of medications Steroids Nonsteroidal anti-inflammatory drugs Cyclooxygenase-2 inhibitors Thiazolidinediones Pregabalin Anthracyclines Targeted chemotherapy agents
86 Defin Chronic Obstructive Pulmonary Disease Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 6, The mounted section of the whole lung shows diffuse involvement seen with panacinar emphysema. (From Thurlbeck WM. Chronic Airflow Obstruction in Lung Disease. Philadelphia, PA: WB Saunders; 1976.)
87 Subcategory Clinical Diagnosis Pathologic Pattern Common Radiographic Description Chronic fibrosing interstitial pneumonias Idiopathic pulmonary fibrosis (IPF) Usual interstitial pneumonia (UIP) Reticular (fibrosis), honeycombing Idiopathic nonspecific interstitial pneumonia Nonspecific interstitial pneumonia (NSIP Ground glass Smoking-related interstitial pneumonias Respiratory bronchiolitis interstitial lung disease (RB-ILD Respiratory bronchiolitis Bronchial wall thickening, centrilobular nodules, ground glass Desquamative interstitial pneumonia (DIP) Desquamative interstitial pneumonia (DIP) Ground glass Acute/subacute interstitial pneumonias Cryptogenic organizing pneumonia (COP Organizing pneumonia (formerly bronchiolitis obliterans with organizing pneumonia, BOOP Patchy consolidation, often peripheral (subpleural) Acute interstitial pneumonia (AIP) Diffuse alveolar damage (DAD) Diffuse alveolar filling Overview of Diffuse Parenchymal Lung Diseases Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 9,

88 Defin Overview of Diffuse Parenchymal Lung Diseases Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 9,


89 Defin Chronic Obstructive Pulmonary Disease Steven E. Weinberger MD, MACP, FRCP, Barbara A. Cockrill MD and Jess Mandel MD, FACP Principles of Pulmonary Medicine, 6, The mounted section of the whole lung shows diffuse involvement seen with panacinar emphysema. (From Thurlbeck WM. Chronic Airflow Obstruction in Lung Disease. Philadelphia, PA: WB Saunders; 1976.)
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than
 TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Ontario s Referral and Listing Criteria for Adult Lung Transplantation
 Ontario s Referral and Listing Criteria for Adult Lung Transplantation Version 3.0 Trillium Gift of Life Network Adult Lung Transplantation Referral & Listing Criteria PATIENT REFERRAL CRITERIA: The patient
Ontario s Referral and Listing Criteria for Adult Lung Transplantation Version 3.0 Trillium Gift of Life Network Adult Lung Transplantation Referral & Listing Criteria PATIENT REFERRAL CRITERIA: The patient
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines
 Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease
 Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
HYPERSENSITIVITY PNEUMONITIS
 HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Respiratory diseases in Ostrołęka County
 Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Liebow and Carrington's original classification of IIP
 Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Policy Specific Section: May 16, 1984 April 9, 2014
 Medical Policy Heart Transplant Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Transplant Original Policy Date: Effective Date: May 16, 1984 April 9, 2014 Definitions
Medical Policy Heart Transplant Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Transplant Original Policy Date: Effective Date: May 16, 1984 April 9, 2014 Definitions
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600
 Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
Pulmonary Test Brenda Shinar
 Pulmonary Test 2016 Brenda Shinar 1. What is a Renal Tubular Acidosis? What is the difference between the types of RTAs in terms of who gets them and how to diagnose them? Type 1, 2, and 4? Metabolic acidosis
Pulmonary Test 2016 Brenda Shinar 1. What is a Renal Tubular Acidosis? What is the difference between the types of RTAs in terms of who gets them and how to diagnose them? Type 1, 2, and 4? Metabolic acidosis
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
Lung Allograft Dysfunction
 Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Endobronchial valve insertion to reduce lung volume in emphysema
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Endobronchial valve insertion to reduce lung volume in emphysema Emphysema is a chronic lung disease that
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Endobronchial valve insertion to reduce lung volume in emphysema Emphysema is a chronic lung disease that
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012
 Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Lung diseases of Vascular Origin. By: Shefaa Qa qqa
 Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Session Guidelines. This is a 15 minute webinar session for CNC physicians and staff
 Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
PATHOPHYSIOLOGICAL PROCESS TEMPLATE
 1 PATHOPHYSIOLOGICAL PROCESS TEMPLATE DISEASE: Chronic obstructive pulmonary disease (COPD) DEFINITION: COPD can be defined as a disease in which there is a significant damage to the lungs thus reducing
1 PATHOPHYSIOLOGICAL PROCESS TEMPLATE DISEASE: Chronic obstructive pulmonary disease (COPD) DEFINITION: COPD can be defined as a disease in which there is a significant damage to the lungs thus reducing
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Respiratory Pathophysiology Cases Linda Costanzo Ph.D.
 Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
9/15/11. Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September Scleroderma. Hard skin
 Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
 OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index ACE inhibitors, see Angiotensin-converting enzyme inhibitors Aging
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index ACE inhibitors, see Angiotensin-converting enzyme inhibitors Aging
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Pathophysiology of COPD 건국대학교의학전문대학원
 Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
Referring for specialist respiratory input. Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL
 Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Myocardial Infarction: Left Ventricular Failure
 CARDIOVASCULAR PHYSIOLOGY 93 Case 17 Myocardial Infarction: Left Ventricular Failure Marvin Zimmerman is a 52-year-old construction manager who is significantly overweight. Despite his physician's repeated
CARDIOVASCULAR PHYSIOLOGY 93 Case 17 Myocardial Infarction: Left Ventricular Failure Marvin Zimmerman is a 52-year-old construction manager who is significantly overweight. Despite his physician's repeated
STUDY OF PULMONARY ARTERIAL HYPERTENSION IN RESPIRATORY DISORDERS
 STUDY OF PULMONARY ARTERIAL HYPERTENSION IN RESPIRATORY DISORDERS *Hegde R.R., Bharambe R.S., Phadtare J.M. and Ramraje N.N. Department of Pulmonary Medicine, Grant Government Medical College, Mumbai-8
STUDY OF PULMONARY ARTERIAL HYPERTENSION IN RESPIRATORY DISORDERS *Hegde R.R., Bharambe R.S., Phadtare J.M. and Ramraje N.N. Department of Pulmonary Medicine, Grant Government Medical College, Mumbai-8
PULMONARY HYPERTENSION
 PULMONARY HYPERTENSION REVIEW & UPDATE Olga M. Fortenko, M.D. Pulmonary & Critical Care Medicine Pulmonary Vascular Diseases Sequoia Hospital 650-216-9000 Olga.Fortenko@dignityhealth.org Disclosures None
PULMONARY HYPERTENSION REVIEW & UPDATE Olga M. Fortenko, M.D. Pulmonary & Critical Care Medicine Pulmonary Vascular Diseases Sequoia Hospital 650-216-9000 Olga.Fortenko@dignityhealth.org Disclosures None
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Pulmonary Hypertension: Another Use for Viagra
 Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Evolution of Surgical Therapies for End-Stage Cardiopulmonary Failure. Heart Failure at the Shoe XI October 5, 2012
 Evolution of Surgical Therapies for End-Stage Cardiopulmonary Failure Heart Failure at the Shoe XI October 5, 2012 Robert S.D. Higgins, MD, MSHA Executive Director, Comprehensive Transplant Center Evolution
Evolution of Surgical Therapies for End-Stage Cardiopulmonary Failure Heart Failure at the Shoe XI October 5, 2012 Robert S.D. Higgins, MD, MSHA Executive Director, Comprehensive Transplant Center Evolution
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW
 SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
Pulmonary veno-occlusive disease
 Disclosure Objectives Pulmonary veno-occlusive disease Tilman Humpl The Hospital for Sick Children University of Toronto, Canada Advisor/Research Grants Actelion Pfizer Historical aspects Epidemiology/Genetics
Disclosure Objectives Pulmonary veno-occlusive disease Tilman Humpl The Hospital for Sick Children University of Toronto, Canada Advisor/Research Grants Actelion Pfizer Historical aspects Epidemiology/Genetics
Home Pulse Oximetry for Infants and Children
 Last Review Date: April 21, 2017 Number: MG.MM.DM.12aC2v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: April 21, 2017 Number: MG.MM.DM.12aC2v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth