Managing IHD and acute Myocardial Infarction
|
|
|
- Benedict Andrews
- 6 years ago
- Views:
Transcription

1 Managing IHD and acute Myocardial Infarction
2 In Ireland- 1 out of every 10 deaths ( 22% of all premature deaths) in 2006 were due to CVD 30,000 15, Source Central statistical office
3 RATIONAL FOR THERAPY ASYMPTOMATIC PHASE PRIMARYPREVENTION VASCULOPROTECTIVE THERAPY ANGINA ANTIANGINAL THERAPY PLAQUE INITIATION PROGRESSION PLAQUE RUPTURE Myocardial Infarction; Death MANAGING ACUTE MI
4 Learning Objectives Managing Angina Managing Acute MI Acute coronary syndromes Focus on the therapeutics/ rationale.
5 Treating angina Anti-anginal agents Vasculo-protective agents Nitrates β blockers Calcium channel blockers Aspirin, Clopidogrel, Statin, ACE-I β blockers Improve exercise tolerance No role in prevention of MI Lower rate of progression to complicated plaque Prevention of MI
6 Anti- anginal agents Nitrate ; beta blockers; calcium channel blockers; K + channel blockers Antianginals typically increase effort tolerance on treadmill testing by seconds Very similar in efficacy Anticipate the need for treatment with two or three agents in many patients
7 Therapeutic targets: antianginals Contractile state Heart rate Wall tension L.V.WORKLOAD O2 DEMAND O2 SUPPLY BLOOD FLOW ARTERIAL O 2 L.V. filling L.V. PRESSURE
8 NITRATES C-gmp mediated relaxation of vascular smooth muscle in veins more than arteries Mimics actions of endothelium derived nitrous oxide INCREASED CORONARY FLOW DECREASED FILLING DECREASED RETURN
9 NITRATES Contractile state Heart rate Wall tension L.V.WORKLOAD O2 DEMAND O2 SUPPLY BLOOD FLOW ARTERIAL O 2 L.V. filling L.V. PRESSURE
10 Pharmacological properties Tolerance (tachyphylaxis) - reduced therapeutic effects Monday morning sickness? due to depletion of free tissue SH Long-acting preparations /infusions/transdermal patches Nitrate free period
11 Indications Relief of acute angina attack Prophylaxis of stable angina (prior to exercise GTN or long-acting) Left ventricular failure
12 Cautions/Contraindications Hypotension Aortic stenosis HOCM Constrictive pericarditis Co-administration with phospho-diesterase inhibitors can lead to life threatening hypotension
13 Side effects Headache Flushing Dizziness Postural hypotension Tachycardia Overdose rarely precipitates methaemoglobinaemia
14 Reduced heart rate Reduced contractility Arterial smooth muscle relaxation
15 BETABLOCKERS Contractile state Heart rate Wall tension L.V.WORKLOAD O2 DEMAND O2 SUPPLY BLOOD FLOW ARTERIAL O 2 L.V. filling L.V. PRESSURE
16 Pharmacological properties Cardioselective eg atenolol metoprolol Non selective eg propranolol Intrinsic sympathomimetic (partial agonist) activity eg celiprolol pindolol Alpha-blocking activity eg carvedilol Lipid soluble (eg propranolol) versus water soluble (eg atenolol) Up-regulation of receptors withdrawal syndrome
17 Indications Symptomatic angina Hypertension Acute coronary syndromes Post myocardial infarction Stable heart failure Arrhythmias Thyrotoxicosis/Benign essential tremor
18 Dose Rational choice - long-acting cardioselective beta blocker od or bd Anti-anginal effects are dose related Titrate to resting heart rate bpm
19 Side effects Beta-1 effects Bradycardia, heart block, heart failure Beta-2 effects bronchospasm, worsening PVD, Raynaud s phenomenon Fatigue, depression, nightmares, impotence May mask hypoglycaemia and worsen glycaemic control in IDDM
20 Cautions/Contraindications C/I in asthma Uncontrolled heart failure Bradycardia Heart block Phaeochromocytoma without prior alpha blockade Caution coronary spasm/copd/pvd Avoid abrupt withdrawal
21 Important Interaction Verapamil and beta blockers precipitate heart block +- asystole Must NOT give IV verapamil to beta blocked patients Extreme caution combined orally
22 Calcium antagonists
23 CALCIUM CHANNEL BLOCKERS Contractile state Heart rate Wall tension L.V.WORKLOAD O2 DEMAND O2 SUPPLY BLOOD FLOW ARTERIAL O 2 L.V. filling L.V. PRESSURE
24 Pharmacological properties 3 classes Phenylalkylamines eg verapamil - relatively cardioselective - -ve chronotropic and inotropic Dihydropyridines eg nifedipine amlodipine - relatively smooth muscle selective - potent vasodilator Benzothiazepines eg diltiazem - intermediate
25 Indications Symptomatic control of angina Coronary spasm Hypertension Arrhythmias Subarachnoid haemorrhage (nimodipine)
26 Side effects Peripheral vasodilation - flushing, headache, ankle oedema Cardiac effects - AV block, heart failure Constipation Short-acting dihydropyridines may mortality in MI
27 Potassium channel activators
28 Potassium channel activators - nicorandil Activates K ATP channel NO donor effects Arterial and venodilator S/E Flushing, dizziness, headache Usually 3 rd or 4 th line agent
29 POT. CHANNEL BLOCKERS Contractile state Heart rate Wall tension L.V.WORKLOAD O2 DEMAND O2 SUPPLY BLOOD FLOW ARTERIAL O 2 L.V. filling L.V. PRESSURE
30 Vasculoprotective agents (25-30%) (20-25%) Aspirin statins
31 Vasculoprotective agents LDL cholesterol reduction to mmol/l ACE-Inhibitors in patients with hypertension, particularly those with Diabetes Hypertension LV hypertrophy and dysfunction history of myocardial infarction, impaired renal function
32 Revascularisation therapy Re-establish vascular patency Percutaneous (i.e., balloon angioplasty & stenting) coronary-artery bypass surgery (CABG) No benefits in patients with chronic stable angina Indications 1. Angina not controlled with optimal/ maximal therapy 2. Patients with high risk of future myocardial infarction

33 Bare-metal stents may be narrowed or obstructed by ingrowth of tissue. With drug-eluting stents, this process is inhibited, but since the struts remain uncovered, they may be prone to thrombosis after antiplatelet therapy is discontinued.
34 In chronic stable angina Class II due to single vessel disease patients early recanalisation does not offer benefit over vasculo-protective therapy.
35 PUTTING IT TOGETHER ASPIRIN / CLOPIDOGREL in low doses A CARDIOSELECTIVE BETABLOCKER ( UNLESS ASTHMA / PVD / OTHER C.I) OR CALCIUM CHANNEL BLOCKER ACE-I, STATIN AGGRESSIVE LIFESTYLE CHANGES TREAT LIPID /BP/ DIABETES CONSIDER INVASIVE PROCEDURES

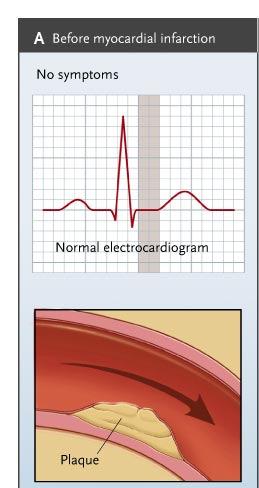
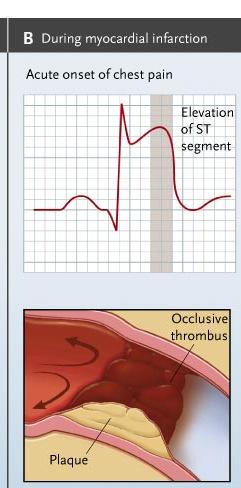
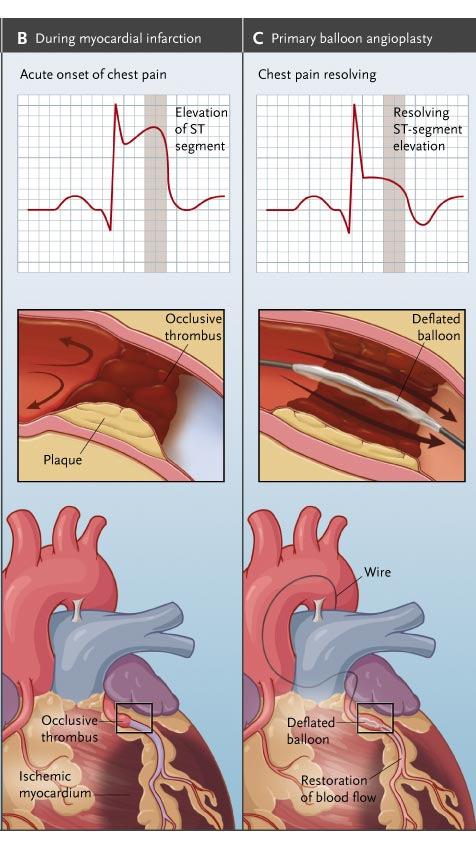
36 TOTAL OCCLUSION (M.I.)
37
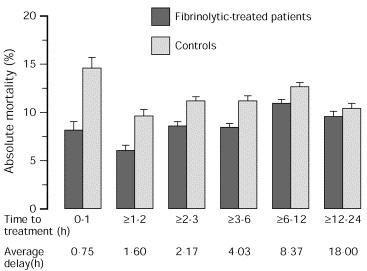
38 Mortality post MI: the importance of evidence based intervention! undiagnosed diagnosed undiagnosed diagnosed
39
40 Immediate treatment Oxygen Intravenous morphine mg+ antiemetic cyclizine 50mg Aspirin mg chewed/dispersible Clopidogrel mg Nitrates GTN 0.4mg sublingual +/- IV Beta blockers Transfer to Coronary care Unit ACE-I within 36 hours
41


42 Restoring patency Maintaining patency Baloon angioplasty with stenting Anti platelet therapy tissue plasminogen activator Others
43 The most appropriate reperfusion therapy 90% recanalisation 1% fall in benefit over fibrinolysis with ever 10 minutes passed 0% fall in benefit over fibrinolysis 30min 60min 90min Presence complicated MI and cardiogenic shock are exceptions to this rule Patients with high risk for bleeding complications have better outcomes with angioplasty
44 The most appropriate reperfusion therapy Lab and personnel Cardiogenic shock Pulmonary oedema High risk for haemorrhagic complications Time <90 min Delay to invasive strategy (upto 24 hrs)
45 Maintaining patency Abciximab as early as possible before primary PCI. Low molecular weight heparin Un-fractionated heparin if renal failure is present
46 Maintain normal glucose, K+ Mg levels
47 Fibrinolysis Primary PCI not available Thrombolysis 50-60% recanalisation Door to needle time <30mins Effective up to 12 hours
48 Fibrinolysis Mode of action Activate plasminogen to form plasmin which degrades fibrin breaking up thrombi Streptokinase, alteplase, reteplase, tenecteplase Streptokinase antibodies within 4 days Alteplase, reteplase followed by heparin for 48 hours
49 Indications Acute ST elevation myocardial infarction Acute pulmonary embolism Acute ischaemic stroke
50 Contraindications Recent haemorrhage trauma or surgery Recent dental extraction Coagulation defects;bleeding disorders Aortic dissection History of cerebrovascular disease Active peptic ulceration Severe menorrhagia Severe hypertension Active cavitating lung disease Acute pancreatitis Severe liver disease Oesophageal varices Previous reaction to streptokinase (Streptokinase)
51 Relative contraindications Venepuncture Recent invasive procedure External chest compressions Pregnancy Abdominal aortic aneurysm Diabetic retinopathy Anticoagulant therapy
52 Side effects Nausea and vomiting Bleeding Reperfusion arrhythmias Hypotension Back pain Allergic reactions (esp streptokinase)
53 Unstable angina/nstemi Oxygen Nitrates GTN 0.4mg sublingual +- IV Intravenous morphine2.5-10mg + antiemetic Aspirin mg chewed/dispersible Heparin eg enoxaparin 1mg/kg 12 hourly Beta-blocker atenolol 5mg over 5 mins repeated after mins Clopidogrel if undergoing PCI Glycoprotein IIb/IIIa inhibitors (abciximab) if undergoing PCI ACE inhibitor if indicated Tight glycaemic control Optimise potassium and magnesium
54 Reading/Website list British national formulary BNF American heart association guidelines
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Angina Pectoris. Edward JN Ishac, Ph.D. Smith Building, Room
 Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth University
Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth University
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Pharmacology. Drugs affecting the Cardiovascular system (Antianginal Drugs)
") Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Acute myocardial infarction. Cardiovascular disorders. main/0202_new 02/03/06. Search date August 2004 Nicholas Danchin and Eric Durand
 main/0202_new 02/03/06 Acute myocardial infarction Search date August 2004 Nicholas Danchin and Eric Durand QUESTIONS Which treatments improve outcomes in acute myocardial infarction?...4 Which treatments
main/0202_new 02/03/06 Acute myocardial infarction Search date August 2004 Nicholas Danchin and Eric Durand QUESTIONS Which treatments improve outcomes in acute myocardial infarction?...4 Which treatments
Diagnosis and Management of Acute Myocardial Infarction
 Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Treatment of T Angina reatment of By Ali Alalawi
 Treatment of Angina By Ali Alalawi Determinants of Oxygen Demand Need to improve ratio of: Coronary blood flow / cardiac work Or Cardiac O2 Supply / Cardiac Requirement Coronary Circulation vs Other Circulation
Treatment of Angina By Ali Alalawi Determinants of Oxygen Demand Need to improve ratio of: Coronary blood flow / cardiac work Or Cardiac O2 Supply / Cardiac Requirement Coronary Circulation vs Other Circulation
CARDIAC REHABILITATION PROGRAMME:- MEDICATION
 CARDIAC REHABILITATION PROGRAMME:- MEDICATION AIM OF THIS SESSION Understand the reasons for taking your medications, Discuss the common side effects associated with these medications - knowing when to
CARDIAC REHABILITATION PROGRAMME:- MEDICATION AIM OF THIS SESSION Understand the reasons for taking your medications, Discuss the common side effects associated with these medications - knowing when to
ANGINA PECTORIS. angina pectoris is a symptom of myocardial ischemia in the absence of infarction
 Pharmacology Ezra Levy, Pharm.D. ANGINA PECTORIS A. Definition angina pectoris is a symptom of myocardial ischemia in the absence of infarction angina usually implies severe chest pain or discomfort during
Pharmacology Ezra Levy, Pharm.D. ANGINA PECTORIS A. Definition angina pectoris is a symptom of myocardial ischemia in the absence of infarction angina usually implies severe chest pain or discomfort during
AIMS: CHEST PAIN. Causes of chest pain. Causes of chest pain: Cardiac causes: Acute coronary syndromes pericarditis thoracic aortic dissection
 CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
Core Safety Profile. Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg. Date of FAR:
/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg. Date of FAR:") Core Safety Profile Active substance: Bisoprolol Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg P - RMS: FI/H/PSUR/0002/002 Date of FAR: 13.12.2011
Core Safety Profile Active substance: Bisoprolol Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg P - RMS: FI/H/PSUR/0002/002 Date of FAR: 13.12.2011
When the learner has completed this module, she/he will be able to:
 Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Cardiology. Self Learning Package. Module 5: Pharmacology: Treatment of Acute Coronary. Prevention
 Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Anticoagulants. Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT
 Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Angina Pectoris Dr. Shariq Syed
 Angina Pectoris Dr. Syed 1 What is Angina Pectoris (AP)? Commonly known as angina is chest pain often due to ischemia of the heart muscle, Because of obstruction or spasm of the coronary arteries 2 What
Angina Pectoris Dr. Syed 1 What is Angina Pectoris (AP)? Commonly known as angina is chest pain often due to ischemia of the heart muscle, Because of obstruction or spasm of the coronary arteries 2 What
Ischemic Heart Disease
 Ischemic Heart Disease Definition: Ischemic heart disease (IHD) is a condition in which there is an inadequate supply of blood and oxygen to a portion of the myocardium; it typically occurs when there
Ischemic Heart Disease Definition: Ischemic heart disease (IHD) is a condition in which there is an inadequate supply of blood and oxygen to a portion of the myocardium; it typically occurs when there
CHAPTER-I MYOCARDIAL INFARCTION
 CHAPTER-I MYOCARDIAL INFARCTION Definition A myocardial infarction, more commonly known as MI or acute myocardial infarction (AMI) or heart attack is a condition where there is interruption of blood supply
CHAPTER-I MYOCARDIAL INFARCTION Definition A myocardial infarction, more commonly known as MI or acute myocardial infarction (AMI) or heart attack is a condition where there is interruption of blood supply
Quinn Capers, IV, MD
 Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Objectives. Treatment of ACS. Early Invasive Strategy. UA/NSTEMI General Concepts. UA/NSTEMI Initial Therapy/Antithrombotic
 Objectives Treatment of ACS Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Define early invasive strategy and what patients typically receive this approach Compare/contrast the medications
Objectives Treatment of ACS Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Define early invasive strategy and what patients typically receive this approach Compare/contrast the medications
Cardiovascular Concerns in Intermediate Care
 Cardiovascular Concerns in Intermediate Care GINA ST. JEAN RN, MSN, CCRN-CSC CLINICAL NURSE EDUCATOR HEART AND & CRITICAL AND INTERMEDIATE CARE Objectives: Identify how to do a thorough assessment of the
Cardiovascular Concerns in Intermediate Care GINA ST. JEAN RN, MSN, CCRN-CSC CLINICAL NURSE EDUCATOR HEART AND & CRITICAL AND INTERMEDIATE CARE Objectives: Identify how to do a thorough assessment of the
Adrenergic Receptor as part of ANS
 Adrenergic Receptor as part of ANS Actions of Adrenoceptors Beta-1 adrenergic receptor Located on the myocytes of the heart Specific actions of the β1 receptor include: 0 Increase cardiac output, by 0
Adrenergic Receptor as part of ANS Actions of Adrenoceptors Beta-1 adrenergic receptor Located on the myocytes of the heart Specific actions of the β1 receptor include: 0 Increase cardiac output, by 0
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
ISCHEMIC HEART DISEASE (IHD)
") ISCHEMIC HEART DISEASE (IHD) 1 Dr. Ahmed A. Elberry, MBBCH, MSc, MD Assistant Professor of Clinical Pharmacy Faculty of pharmacy, KAU DEFINITIONS IHD: O2 or blood supply to myocardium resulting from coronary
ISCHEMIC HEART DISEASE (IHD) 1 Dr. Ahmed A. Elberry, MBBCH, MSc, MD Assistant Professor of Clinical Pharmacy Faculty of pharmacy, KAU DEFINITIONS IHD: O2 or blood supply to myocardium resulting from coronary
Angina pectoris due to coronary atherosclerosis : Atenolol is indicated for the long term management of patients with angina pectoris.
 Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Pharmacotherapy of Angina Pectoris
 Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Pharmacotherapy of Angina Pectoris
 Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Drug Treatment of Ischemic Heart Disease
 Drug Treatment of Ischemic Heart Disease Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan November, 2017 Categories of Ischemic Heart Disease Fixed "Stable, Effort Angina Variant
Drug Treatment of Ischemic Heart Disease Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan November, 2017 Categories of Ischemic Heart Disease Fixed "Stable, Effort Angina Variant
Platelet aggregation inhibitor. Cardiac chest pain or suspected Myocardial Infarction.
 s Aspirin Platelet aggregation inhibitor. Anti-inflammatory agent and an inhibitor of platelet function. Useful agent in the treatment of various thromboembolic diseases such as acute myocardial infarction.
s Aspirin Platelet aggregation inhibitor. Anti-inflammatory agent and an inhibitor of platelet function. Useful agent in the treatment of various thromboembolic diseases such as acute myocardial infarction.
Drug Profiles Professional Responder
 Entonox Classification Medical Gas Entonox (50% oxygen 50% nitrous oxide) Effects Potent analgesic, weak anesthetic Onset Rapid Peak Immediate Indications Relief of moderate to severe pain Cardiac-related
Entonox Classification Medical Gas Entonox (50% oxygen 50% nitrous oxide) Effects Potent analgesic, weak anesthetic Onset Rapid Peak Immediate Indications Relief of moderate to severe pain Cardiac-related
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
Cardiac Drugs: Chapter 9 Worksheet Cardiac Agents. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate.
 Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
REBEL. Platinum Chromium Coronary Stent System. Patient Information Guide
 REBEL Patient Information Guide REBEL PATIENT INFORMATION GUIDE You have recently had a REBEL bare metal stent implanted in the coronary arteries of your heart. The following information is important for
REBEL Patient Information Guide REBEL PATIENT INFORMATION GUIDE You have recently had a REBEL bare metal stent implanted in the coronary arteries of your heart. The following information is important for
Antianginal Drugs 18 I. OVERVIEW II. TYPES OF ANGINA
 Antianginal Drugs 18 I. OVERVIEW Atherosclerotic disease of the coronary arteries, also known as coronary artery disease or ischemic heart disease, is the most common cause of mortality around the world.
Antianginal Drugs 18 I. OVERVIEW Atherosclerotic disease of the coronary arteries, also known as coronary artery disease or ischemic heart disease, is the most common cause of mortality around the world.
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Cardiovascular risk reduction in diabetes Lipids (NICE CG181)
") Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
The number of patients being treated for angina in the
 Vol 4 January 2012 Clinical Pharmacist 13 Management of stable angina involves symptomatic relief of chest pain, longer-acting control of symptoms and prevention of cardiovascular complications. This article
Vol 4 January 2012 Clinical Pharmacist 13 Management of stable angina involves symptomatic relief of chest pain, longer-acting control of symptoms and prevention of cardiovascular complications. This article
How to give thrombolysis in acute myocardial infarction
 Page 1 of 6 How to give thrombolysis in acute myocardial infarction Original article: Michael Tam In the major urban hospitals, there will be little place for thrombolysis in acute STEMI (STelevation myocardial
Page 1 of 6 How to give thrombolysis in acute myocardial infarction Original article: Michael Tam In the major urban hospitals, there will be little place for thrombolysis in acute STEMI (STelevation myocardial
Ischaemic heart disease. IInd Chair and Clinic of Cardiology
 Ischaemic heart disease IInd Chair and Clinic of Cardiology Definition Syndrome due to chronic insufficient oxygen supply to myocardial cells Nomenclature: ischaemic heart disease (IHD), coronary artery
Ischaemic heart disease IInd Chair and Clinic of Cardiology Definition Syndrome due to chronic insufficient oxygen supply to myocardial cells Nomenclature: ischaemic heart disease (IHD), coronary artery
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Ischaemic Heart Disease
 Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Current Treatment Of Ischemic Heart Disease In the United States: An Overview. By Dr Gary Mo
 Current Treatment Of Ischemic Heart Disease In the United States: An Overview By Dr Gary Mo 1 Ischemic Heart Disease in the US 1. Cardiovascular disease remains the most common cause of death and is responsible
Current Treatment Of Ischemic Heart Disease In the United States: An Overview By Dr Gary Mo 1 Ischemic Heart Disease in the US 1. Cardiovascular disease remains the most common cause of death and is responsible
TRANSPARENCY COMMITTEE OPINION. 4 November 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 4 November 2009 RANEXA 375 mg extended release tablet Pack of 60 (CIP: 394 370-7) RANEXA 500 mg extended release tablet
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 4 November 2009 RANEXA 375 mg extended release tablet Pack of 60 (CIP: 394 370-7) RANEXA 500 mg extended release tablet
Beta blockers in primary hypertension. Dr. Md. Billal Alam Associate Professor of Medicine DMC
 Beta blockers in primary hypertension Dr. Md. Billal Alam Associate Professor of Medicine DMC Development of antihypertensive drugs Beta blockers 1958 - The first beta-blocker, dichloroisoproterenol, was
Beta blockers in primary hypertension Dr. Md. Billal Alam Associate Professor of Medicine DMC Development of antihypertensive drugs Beta blockers 1958 - The first beta-blocker, dichloroisoproterenol, was
Course: Exercise and Aging for Special Populations
 Copyright EFS Inc. All Rights Reserved. Course: Exercise and Aging for Special Populations Session 2: Cardiovascular and Metabolic Disease Considerations for Exercise Program Design Presentation Created
Copyright EFS Inc. All Rights Reserved. Course: Exercise and Aging for Special Populations Session 2: Cardiovascular and Metabolic Disease Considerations for Exercise Program Design Presentation Created
DRUGS USED IN ANGINA PECTORIS
 DRUGS USED IN ANGINA PECTORIS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 16, 2010 Materials on: Exam #7 Required reading: Katzung, Chapter 12 1 TYPES OF ISCHEMIC HEART DISEASE
DRUGS USED IN ANGINA PECTORIS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 16, 2010 Materials on: Exam #7 Required reading: Katzung, Chapter 12 1 TYPES OF ISCHEMIC HEART DISEASE
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126
 Stable angina: management Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Stable angina: management Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Drug Treatment of Ischemic Heart Disease
 Drug Treatment of Ischemic Heart Disease Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Categories of Ischemic Heart Disease Fixed "Stable, Effort Angina Variant
Drug Treatment of Ischemic Heart Disease Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Categories of Ischemic Heart Disease Fixed "Stable, Effort Angina Variant
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
 A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
Post Operative Troponin Leak: David Smyth Christchurch New Zealand
 Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Coronary artery disease and as anticoagulant (inhibiting the clotting of the blood) in patients undergoing surgery to treat blockages
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Coronary artery disease and as anticoagulant (inhibiting the clotting of the blood) in patients undergoing surgery to treat blockages
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets
 METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
Nitroglycerin and Heparin Drip Interfacility Protocols
 Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 26 Caring for Clients with Coronary Heart Disease and Dysrhythmias Coronary Heart Disease (CHD) Leading
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 26 Caring for Clients with Coronary Heart Disease and Dysrhythmias Coronary Heart Disease (CHD) Leading
Treatment of Stable Coronary Artery Disease Pharmacotherapy
 Treatment of Stable Coronary Artery Disease Pharmacotherapy José López-Sendón Hospital Universitario La Paz. Madrid. Spain Conflict of interest: I will discuss off label use and/or investigational use
Treatment of Stable Coronary Artery Disease Pharmacotherapy José López-Sendón Hospital Universitario La Paz. Madrid. Spain Conflict of interest: I will discuss off label use and/or investigational use
Supplementary Table S1: Proportion of missing values presents in the original dataset
 Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Stable angina: current guidelines and advances in management
 DRUG REVIEW n Stable angina: current guidelines and advances in management Anoop Shah MRCP and Keith Fox FRCP Our Drug Review discusses the current recommended management of stable angina, focussing on
DRUG REVIEW n Stable angina: current guidelines and advances in management Anoop Shah MRCP and Keith Fox FRCP Our Drug Review discusses the current recommended management of stable angina, focussing on
Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017
 Clinician Guide SEPTEMBER 2017") Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Effects of felodipine on haemodynamics and exercise capacity in patients with angina pectoris
 Br. J. clin. Pharmac. (1987), 23, 391-396 Effects of felodipine on haemodynamics and exercise capacity in patients with angina pectoris J. V. SHERIDAN, P. THOMAS, P. A. ROUTLEDGE & D. J. SHERIDAN Departments
Br. J. clin. Pharmac. (1987), 23, 391-396 Effects of felodipine on haemodynamics and exercise capacity in patients with angina pectoris J. V. SHERIDAN, P. THOMAS, P. A. ROUTLEDGE & D. J. SHERIDAN Departments
Ischemic heart disease
 Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Chapter / Section / Drug
 2 Cardiovascular System 2.1 Positive inotropic drugs Digoxin Digoxin specific antibody ( DigiFab ) 2.2 Diuretics 2.2.1 Thiazides and related diuretics Indapamide (1 st Line) Bendroflumethiazide Metolazone
2 Cardiovascular System 2.1 Positive inotropic drugs Digoxin Digoxin specific antibody ( DigiFab ) 2.2 Diuretics 2.2.1 Thiazides and related diuretics Indapamide (1 st Line) Bendroflumethiazide Metolazone
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
The dose for paediatric patients may never exceed the adult dose.
 The medication formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to support Emergency First Responders to be competent in the use of medications permitted under Clinical Practice
The medication formulary is published by the Pre-Hospital Emergency Care Council (PHECC) to support Emergency First Responders to be competent in the use of medications permitted under Clinical Practice
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
Chest Pain. Dr Robert Huggett Consultant Cardiologist
 Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet