Colorectal Surgery SSI Prevention Bundle and ERAS. NYSPFP Webinar
|
|
|
- Sylvia Carpenter
- 6 years ago
- Views:
Transcription
1 Colorectal Surgery SSI Prevention Bundle and ERAS NYSPFP Webinar Christopher Mantyh, MD Duke University Medical Center Professor of Surgery Chief of Colorectal Surgery Chief of Quality
2 Who Cares About Quality in Surgery? The Government CMS ties reported outcomes to payment or penalties medicare.gov/hospitalcompare, Health Grades Current reported surgical outcomes Lower extremity bypass outcomes Colon surgery outcomes Outcomes in operations in patients > 65 years Insurance companies Using follow CMS on reimbursements New bundle payments for a disease state Complications will negatively effect this
3 Who Cares About Quality in Surgery? Hospitals Directly compare hospitals in an location: patient shoppers, referral shoppers Reimbursement: currently a bonus, soon penalties Change from Volume=Quantity/Cost based purchasing to Value=Quality/Cost based purchasing Surgeons Self-realization that surgical complications can be prevented Save money, morbidity, mortality American College of Surgeons established NSQIP to accurately compare outcomes It is the right thing to do Patients



4 Increasing Financial Penalty for HAIs 100% 80% 60% 40% 20% 0% VBP Domain Weights Clinical Process Patient Experiences Outcome Efficiency 6% AMI = acute myocardial infarction; HAC = hospital-acquired condition; HF = heart failure; RRP = Readmission Reduction Program; VBP = Value-Based Purchasing Program. 1. CMS. Hospital-Acquired Conditions. Available at: Accessed July 21, CMS. Hospital Value-Based Purchasing Program Fact Sheet. Available at: Network-MLN/MLNProducts/downloads/Hospital_VBPurchasing_Fact_Sheet_ICN pdf. Accessed August 4, CMS. Readmissions Reduction Program. Available at: Accessed August 4, Arkansas Foundation for Medical Care, Quality Improvements Organization. Available at: Accessed August 20, CareFusion Corporation or one of its subsidiaries. All rights reserved. 4
5 Improvement Initiative for NSQIP: Colorectal SSI Peri-operative bundle Increase laparoscopy ERAS Wound VAC over open cases Wound classification: critically important in risk stratification Use as a model system for general surgery Identify high risk SSI operations Liver, pancreas, gastric, groin node dissections, HIPEC
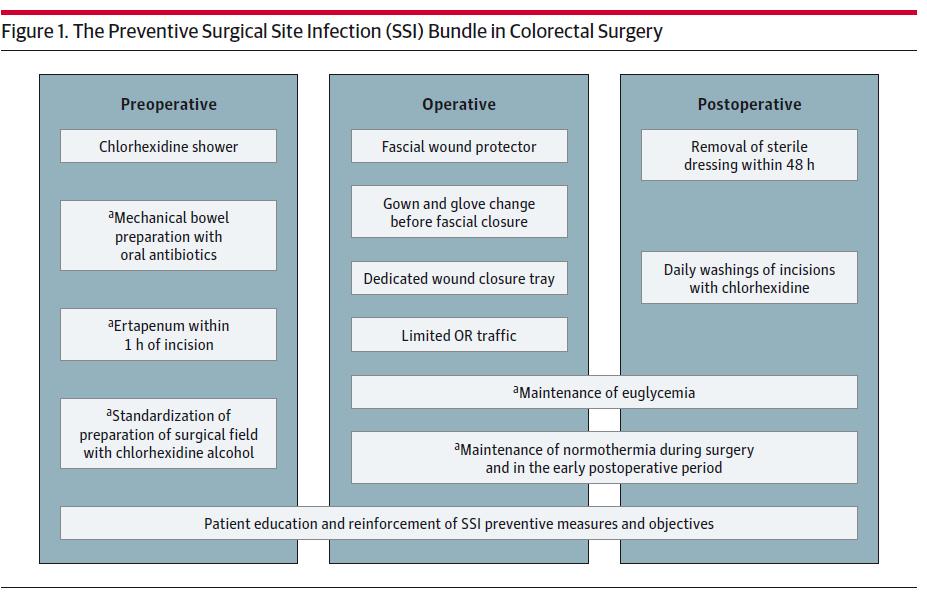
6 Colorectal Peri-operative Bundle Pre-operative Chlorhexidine (CHG) shower * Chart review- 61% of patients documented to have received pre-op scrub and 91% of those patients completed pre-operative scrub Mechanical bowel prep + oral antibiotics + pre-operative IV antibiotics CHG 70% alcohol prep Intra-operative Antibiotic: Ertapenem (no re-dosing) or Cipro + Flagyl Normothermia Alexis wound protectors (open cases) Change gown and gloves follow anastomosis or at fascial closure Wound closure tray Limit OR traffic *RN CIRCULATORS APPLYING SURGICAL SCRUB AND FOLEY PLACEMENT AS OF SEPTEMBER 2012
7 Peri-operative Bundle (cont.) Post-operative No re-dosing of antibiotics unless clearly documented reason Leave sterile dressings on for 48 hrs CHG wipes daily after dressing removal Strip VACs (trial)

8



9 Bundle Reduced SSI Post-op sepsis LOS Variable direct costs
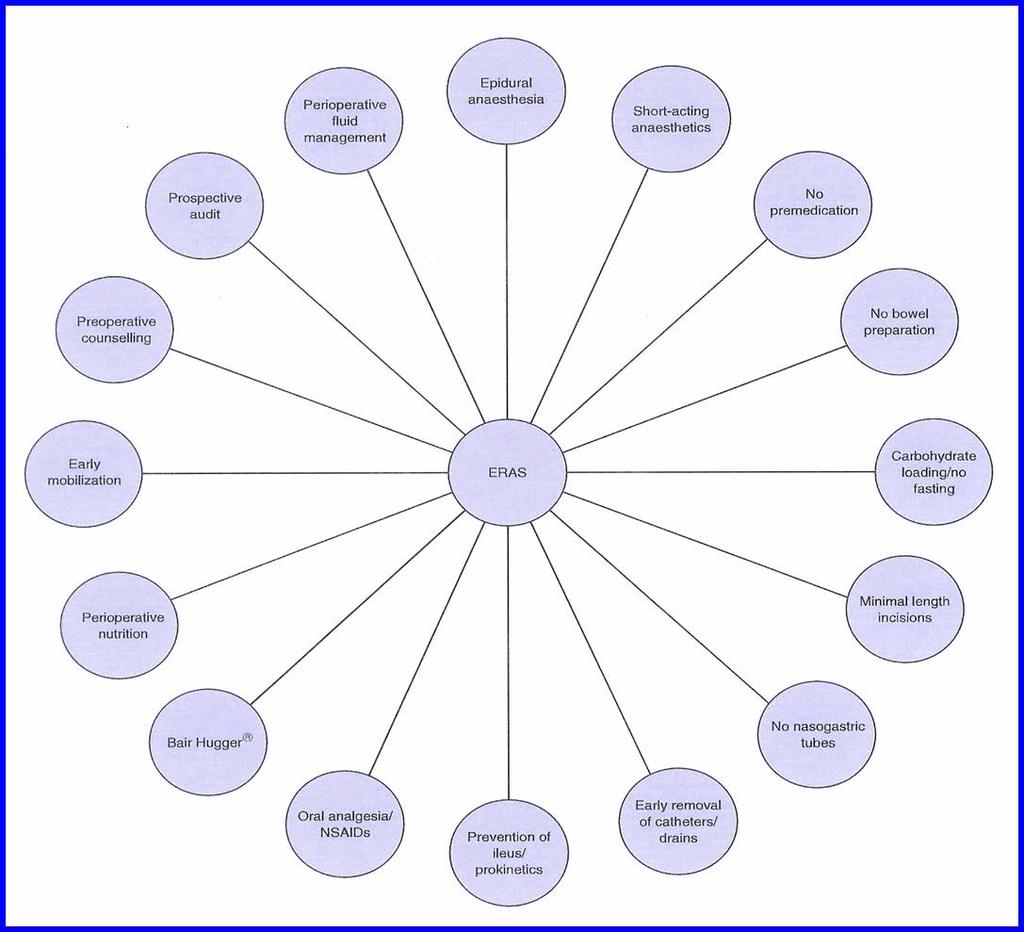
10 Enhance Recovery After Surgery (ERAS)
11
12 Surgical Stress
13

14 Duke CRS ERAS Protocol
15 Duke CRS ERAS PREOP HOLDING, day of operation -IDENTIFY fast track patients and initiate protocol -THROMBOPROPHYLAXIS timed with epidural -EPIDURAL anesthesia placement INTRAOP -ANTIBIOTICS PROPHYLAXIS before skin incision -SCD s on before induction -GOAL-DIRECTED IVF THERAPY with ESOPHAGEAL MONITORING -TEMPERATURE regulation -NG/OG discontinued before leaving OR POSTOP -IDENTIFY ERAS patients for protocol participation -DIET begins night of surgery -AMBULATION begins night of surgery -HOB at 30 degrees at all times -IVF </= 1L/24hrs (70kg) -EPIDURAL and SCD continuation -post-op THROMBOPROPHYLAXIS begins POD 1
16 Goal Directed Fluid Management Reduce bowel edema Decreases POI Reduces pulmonary complications Especially useful in long procedures with expected extubation Is NOT fluid restrictive
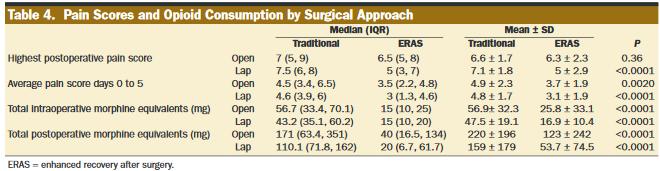
17 Multi-modality Pain Management Previously opioids more opioids additional opioids American Society of Anesthesia 2004 Task Force: Opioid dose-sparing effects (reduced opioid-related adverse events) can be achieved via the use of non-opioid agents and regional blocks. Recommended all patients receive around the clock regimen of a non-opioid agent NSAIDs COXIBs Acetaminophen Consider supplemental regional anesthesia techniques Anesthesiology 2004, 100:
18 Duke Peri-operative Pain Management: Low Thoracic Epidurals T10 region Give test dose once sited as normal 5000U SC heparin can be given immediately after placement Hydromorphone 0.4mg-0.6mg before induction of anesthesia Lidocaine bolus at least 10 minutes pre-incision (40-100mg) 1 g IV acetaminophen prior to incision Run infusion of 0.25% bupivacaine throughout case (3-6 ml/hr) No intraoperative iv opioids after induction without discussion with Attending Anesthesiologist Switch to bupivacaine 0.125%/hydromorphone 10mcg/ml in epidural pump before leaving for PACU at end of case. Settings: Infusion 4-6 ml/hour; 2ml bolus every 30 minutes Max dose set for infusion over 4 hours + 6 boluses (12ml) (example - infusion 5ml/hr; max 32ml over 4 hours)
19 Peri-operative Pain Management Post-operative Continue epidural for 2-3 days (bowel function) IV acetaminophen until tolerating orals Oral opioids with d/c epidural If tolerating liquids, solids move to oral acetaminophen Ibuprofen PRN Ketorolac used sparingly Dry, or elderly patients can push into kidney failure Gastric bleeding Surgical bleeding
 on colorectal surgery (CRS) outcomes at a single institution. Kennan et al, J Am Coll Surg.")
20 OBJECTIVE The purpose of this study was to examine the impact of the implementation of the enhanced recovery pathway (ERP) and preventative surgical site infection bundle (SSIB) on colorectal surgery (CRS) outcomes at a single institution. Kennan et al, J Am Coll Surg. 221: , 2015

21 THE PREVENTIVE SSI BUNDLE Kennan et al, J Am Coll Surg. 221: , 2015

22 THE ENHANCED RECOVERY PATHWAY Kennan et al, J Am Coll Surg. 221: , 2015

23 COMPLIANCE Kennan et al, J Am Coll Surg. 221: , 2015
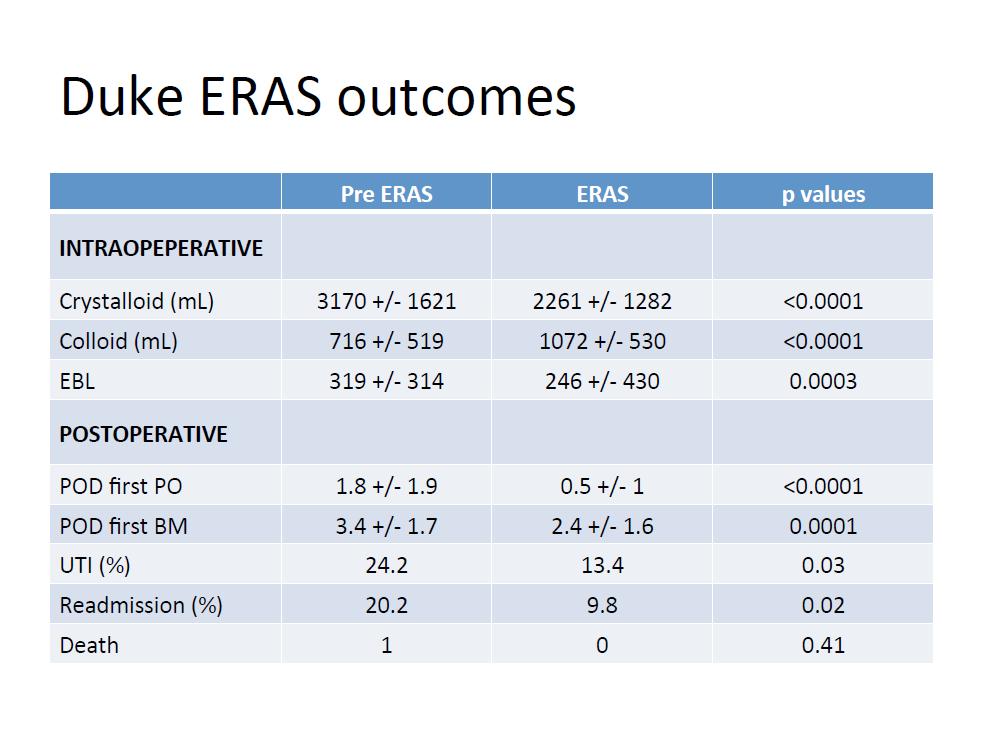
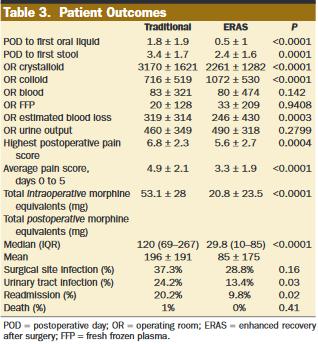
24 Duke ERAS Results Oral intake on the day of surgery 65.5% of ERAS patients vs. 18.8% (p <0.0001). Eating solids on POD1 49% of ERAS patients vs. 12.5% (p< 0.001). Ambulating on POD1 70% of ERAS patients were ambulating. Bowel movement 2.4 days in the ERAS group vs. 3.4 days (p=0.008).
25
26 30-day Post-Operative Outcomes of ACS-NSQIP Sampled Patients Who Underwent Major, Elective Colorectal Surgery, Stratified by the Presence of the Enhanced Recovery Pathway and/or Preventative Surgical Site Infection Bundle 30-day Post-Operative Outcomes Total Cohort 9/2006-3/2013 (n = 787) Pre-ERP/Bundle 9/2006-1/2010 (n = 337) Post-ERP/Pre-Bundle 2/2010-6/2011 (n = 165) Post-ERP/Bundle 7/2011-3/2013 (n = 285) p-value Length of stay (median, Q1, Q3) 5 (4, 8) 6 (4, 8) 5 (4, 8) 5 (3, 7) < Mortality 7 (0.9%) 2 (0.6%) 1 (0.6%) 4 (1.4%) Unplanned reoperation 37 (4.7%) 24 (7.1%) 4 (2.4%) 9 (3.2%) Wound complication 150 (19.1%) 96 (28.5%) 32 (19.4%) 22 (7.7%) < Superficial SSI 132 (16.8%) 83 (24.6%) 31 (18.8%) 18 (6.3%) < Deep SSI 6 (0.8%) 5 (1.5%) 1 (0.6%) 0 (0%) Organ space SSI 46 (5.8%) 28 (8.3%) 10 (6.1%) 8 (2.8%) Deep venous thrombosis 10 (1.3%) 3 (0.9%) 7 (4.2%) 0 (0%) < Pulmonary embolism 5 (0.6%) 1 (0.3%) 2 (1.2%) 2 (0.7%) Stroke/CVA 6 (0.8%) 0 (0%) 3 (1.8%) 3 (1.1%) Unplanned reintubation 17 (2.2%) 9 (2.7%) 4 (2.4%) 4 (1.4%) Pneumonia 18 (2.3%) 10 (3%) 5 (3%) 3 (1.1%) Myocardial infarction 9 (1.1%) 2 (0.6%) 3 (1.8%) 4 (1.4%) Cardiac arrest 1 (0.1%) 0 (0%) 0 (0%) 1 (0.4%) Sepsis 55 (7%) 30 (8.9%) 20 (12.1%) 5 (1.8%) < Septic shock 11 (1.4%) 8 (2.4%) 2 (1.2%) 1 (0.4%) Urinary tract infection 42 (5.3%) 25 (7.4%) 9 (5.5%) 8 (2.8%) 0.039
27

28 J Am Coll Surg. 221: , 2015
29 Kennan et al, J Am Coll Surg. 221: , 2015
30 DISCUSSION This study is the first examine the combined effect of the ERP and SSIB Our experience exemplifies how the process of quality improvement in surgery must be an ongoing effort, and that sequential adoption of separately studied care protocols can provide incremental improvements in patient care. Not only did patient outcomes improve with the introduction of the ERP and SSIB, but these measures also provided cost-savings in the care of CRS patients. Continual assessments and updates of existing evidence based care protocols such as the ERP and SSIB will lead to continual improvement in post-operative outcomes and increased value of care delivered.
31 DUH Variable Direct Cost/Case by Cost Group Inpatient Colectomy Primary Procedure Discharges COST_GROUP FY11 FY12 FY13 THRU FP9 % CHG F.SURGERY SVC % A.INTERMEDIATE SVC % C.PHARMACY SVC % B.INTENSIVE NRS SVC % J.LABS % O.BLOOD % I.RAD SVCS % G.RESP CARE % H.PT OT SPEECH SVCS % E.OTHER DIAG AND THERA % K.ER TRANSP % D.CARDIO SVC % M.MED SURG SUPPL % N.OP CLINIC % TOTAL VAR DIR COST/CASE % ALOS % DISCHARGES % 50% 40% 30% 20% 10% 0% % of FY13 Total VDC/Case 48% 22% 10% 6% 5% 2% 2% 1% 1% 1% 9/3/ Data source = DSR/EPSI
32 ALOS and Variable Direct Cost by Primary Surgeon, FY12-FY13 YTD thru FP9, Colectomy Discharges MD DISCHARGES ALOS MEDIAN LOS AVG VAR DIR COST MEDIAN VAR DIR COST MD $13,018 $10,019 MD ,982 7,686 MD ,577 9,343 MD ,524 13,653 MD ,541 15,946 MD ,206 12,757 ALL OTHERS Colorectal surgeons Non colorectal surgeons OVERALL /3/
33 30-day Post-Operative Outcomes of ACS-NSQIP Sampled Patients Who Underwent Major, Elective Colorectal Surgery in Pre-ERP/Bundle Vs. Post-ERP/Bundle Period After Inverse Proportional Weighting Characteristic Pre-ERP/Bundle 9/2006-1/20120 Post-ERP/Bundle 7/2011-3/2013 p-value Length of stay 7.9+/ /-5.5 <0.001 Mortality (30 d) 0.7% 1.9% Unplanned reoperation 6.9% 2.8% Wound complication 26.3% 8.3% <0.001 Superficial SSI 22.5% 7.1% <0.001 Deep SSI 1.5% 0.0% Organ space SSI 7.6% 2.5% Deep venous thrombosis 1.0% 0.0% Pulmonary embolism 0.3% 0.7% Stroke/CVA 0.0% 1.3% Unplanned reintubation 2.7% 0.8% Pneumonia 2.9% 1.0% Myocardial infarction 0.5% 1.4% Cardiac arrest 0.0% 0.5% Sepsis 8.9% 1.7% <0.001 Septic shock 2.4% 0.5% Urinary tract infection 7.6% 2.8% 0.008


34 HCAHPS: Duke Colorectal Surgery Trend in Pain Management 38% improvement since 2011
35

36
37 Do ERAS/Bundles Matter? National data Published studies NSQIP, STS Institutional data LOS Costs Readmissions Bundles/ERAS will succeed Incremental changes are unlikely to succeed
38 Pearls from ERAS/Bundles ERAS works Reduces LOS Reduces narcotics if use multimodality therapy Reduces wound infections Reduces overall complications May improve patient satisfaction It is coming to a hospital near you It usually involves tweaking the system, not reinventing the wheel
39 Pearls from ERAS/Bundles Each hospital/surgeon/group different Use what you have and what will work Need buy in from everyone ERAS is plastic: mold it Review every 6 months Talk to your administration, be pro-active Present your data Show the bad data and how to fix it
40 Getting Buy-In: Team Approach Anesthesia Pain management Epidurals, axial blocks Multi-modal treatment Peri-op IV fluids Normothermia, normoglycemia Surgical partners: Need to do collectively to avoid confusion with rest of support OR nurses OR time out (check list), wound classification Prep patient, Foley placement Floor Nurses Wound management Foley removal Ambulation, VTE prophylaxis Discharge education (prevent re-admissions)
41 The Hurdle: Why and How? Am I or we (division/institution) practicing best medicine? Avoid the buts my patients are sicker my partners are set in their ways too complicated, never work here I don t have time Establish a core group Surgeon, anesthesiologist, nurse (s) Database to track (NSQIP, institutional) Engage administration Set modest goals Present data as it comes in Be malleable and be patient! Celebrate success
42 The Hurdle: Why and How? The data Share it early and often What is working, what is not Administration Hospital Compare etc. Joint Commission Bundled cost to insurance Are your competitors doing this? Be diligent What is your compliance with bundles/eras? Tract LOS, complications, costs
43 ERAS/Bundles Conclusions Biggest advance in surgery over the last 20 years Cost (yes) Length of stay (yes) Return to work/daily activities (yes) Pain (yes) Reduction in complications (yes) SSI UTI VTE Patient satisfaction (probably) Poorly measured Survival (probably) Stay tuned studies coming
44 Thank You, Acknowledgements, Questions Surgery Julie Thacker, MD John Migaly, MD Jeff Sun, MD Jeff Keenan, MD Anesthesia Tim Miller, MD Nursing Regina Woody, RN Jill Haslam, RN
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES
 EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
Click to edit Master subtitle style
 Does Enhanced Recovery Improve Outcomes? Click to edit Master subtitle style Kaare Weber, MD Director of Surgery Associate Medical Director, Surgery A MEMBER OF THE MONTEFIORE HEALTH SYSTEM mes? Click
Does Enhanced Recovery Improve Outcomes? Click to edit Master subtitle style Kaare Weber, MD Director of Surgery Associate Medical Director, Surgery A MEMBER OF THE MONTEFIORE HEALTH SYSTEM mes? Click
Presentation at ACS NSQIP National Conference in July Surgical Site Infection Reduction Strategies
 Presentation at ACS NSQIP National Conference in July 2015 Surgical Site Infection Reduction Strategies PeaceHealth Sacred Heart Medical Center at RiverBend Level II Trauma Center 379 Beds 15,060 cases
Presentation at ACS NSQIP National Conference in July 2015 Surgical Site Infection Reduction Strategies PeaceHealth Sacred Heart Medical Center at RiverBend Level II Trauma Center 379 Beds 15,060 cases
Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination
 Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination Jason D. Sciarretta, MD, FACS Grand Strand Medical Center, Myrtle Beach, SC University of South Carolina
Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination Jason D. Sciarretta, MD, FACS Grand Strand Medical Center, Myrtle Beach, SC University of South Carolina
Enhanced Recovery After Colorectal Surgery at Royal Inland Hospital Kamloops, BC. Our Data Experience
 Enhanced Recovery After Colorectal Surgery at Royal Inland Hospital Kamloops, BC Our Data Experience No Disclosures 1/26/2015 2 Purpose To tell our story of how we collect and share our ERACS data 1/26/2015
Enhanced Recovery After Colorectal Surgery at Royal Inland Hospital Kamloops, BC Our Data Experience No Disclosures 1/26/2015 2 Purpose To tell our story of how we collect and share our ERACS data 1/26/2015
ERAS. Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic
 ERAS Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic Outline Definition Justification Ileus Pain Outline Specifics Data BMC Data Worldwide Data Implementation What is ERAS? AKA Fast-track
ERAS Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic Outline Definition Justification Ileus Pain Outline Specifics Data BMC Data Worldwide Data Implementation What is ERAS? AKA Fast-track
Enhanced Recovery After Surgery Getting it Right
 Enhanced Recovery After Surgery Getting it Right Aalok Agarwala, M.D., M.B.A. Division Chief, General Surgery Anesthesia Associate Director, Quality and Safety, MGH DACCPM Assistant Professor, Harvard
Enhanced Recovery After Surgery Getting it Right Aalok Agarwala, M.D., M.B.A. Division Chief, General Surgery Anesthesia Associate Director, Quality and Safety, MGH DACCPM Assistant Professor, Harvard
Enhanced Recovery after Surgery
 Enhanced Recovery after Surgery AKA ERAS What is Enhanced Recovery (ER)? Paradigm shift in surgery and surgical care of the patient Philosophy of care Perioperative continuum Multidisciplinary Patient
Enhanced Recovery after Surgery AKA ERAS What is Enhanced Recovery (ER)? Paradigm shift in surgery and surgical care of the patient Philosophy of care Perioperative continuum Multidisciplinary Patient
SCORES FOR 4 TH QUARTER, RD QUARTER, 2014
 SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
A Comprehensive Multi-disciplinary Approach to Improve Surgical Outcomes Following Elective Colon and Rectal Surgery
 A Comprehensive Multi-disciplinary Approach to Improve Surgical Outcomes Following Elective Colon and Rectal Surgery Tripurari Mishra MD, Deepa Bhat MD, Mina Saeed MD, Jan Kaminski MD, Mihaela Banulescu
A Comprehensive Multi-disciplinary Approach to Improve Surgical Outcomes Following Elective Colon and Rectal Surgery Tripurari Mishra MD, Deepa Bhat MD, Mina Saeed MD, Jan Kaminski MD, Mihaela Banulescu
Early Recovery after Surgery (ERAS):
:") Early Recovery after Surgery (ERAS): Applying Consistently What We ve Known for 20 Years Dr. Kurt Heiss, MD Objectives Laying Foundation: Who, Why Explore Components: What Start a Program: How and When
Early Recovery after Surgery (ERAS): Applying Consistently What We ve Known for 20 Years Dr. Kurt Heiss, MD Objectives Laying Foundation: Who, Why Explore Components: What Start a Program: How and When
Preventing Surgical Site Infections: The SSI Bundle
 Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
ERAS: Enhanced Recovery After Surgery. Christopher L. Wu, M.D. Professor of Anesthesiology The Johns Hopkins University; Baltimore, Maryland
 ERAS: Enhanced Recovery After Surgery Christopher L. Wu, M.D. Professor of Anesthesiology The Johns Hopkins University; Baltimore, Maryland Overview History and basic principles of ERAS Review published
ERAS: Enhanced Recovery After Surgery Christopher L. Wu, M.D. Professor of Anesthesiology The Johns Hopkins University; Baltimore, Maryland Overview History and basic principles of ERAS Review published
Quality Improvement Updates Foley Discontinuation Protocol Surgical Care Improvement Project
 Quality Improvement Updates Foley Discontinuation Protocol Surgical Care Improvement Project Barbara J Martin, RN, MBA Quality Consultant, Center for Clinical Improvement Indwelling Urinary Catheters Insertion,
Quality Improvement Updates Foley Discontinuation Protocol Surgical Care Improvement Project Barbara J Martin, RN, MBA Quality Consultant, Center for Clinical Improvement Indwelling Urinary Catheters Insertion,
Measure Applications Partnership. Hospital Workgroup In-Person Meeting Follow- Up Call
 Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #358: Patient-Centered Surgical Risk Assessment and Communication National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #358: Patient-Centered Surgical Risk Assessment and Communication National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL MEASURES:
If you reduce variability in volume administration, HOW. you can reduce post-surgical complications, LOS and associated costs 1-4
 A large body of clinical evidence* demonstrates If you reduce variability in volume administration, you can reduce post-surgical complications, LOS and associated costs 1-4 Complications Too Dry Too Wet
A large body of clinical evidence* demonstrates If you reduce variability in volume administration, you can reduce post-surgical complications, LOS and associated costs 1-4 Complications Too Dry Too Wet
Improving Colectomy Outcomes in the Enhanced Recovery In NSQIP (ERIN) Pilot
 Pilot") Improving Colectomy Outcomes in the Enhanced Recovery In NSQIP (ERIN) Pilot Julia R. BerianMD; Kristen A. Ban MD; Sanjay MohantyMD,MS; Jennifer L. ParuchMD,MS; Clifford Y. KoMD,MS,MSHS; Julie K. Thacker
Improving Colectomy Outcomes in the Enhanced Recovery In NSQIP (ERIN) Pilot Julia R. BerianMD; Kristen A. Ban MD; Sanjay MohantyMD,MS; Jennifer L. ParuchMD,MS; Clifford Y. KoMD,MS,MSHS; Julie K. Thacker
ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY
 PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY") Department of Surgery Divison of General Surgery ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY December 2016 Disclosure Paresh
Department of Surgery Divison of General Surgery ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY December 2016 Disclosure Paresh
Assessment. Consults & Referrals
 University of Virginia Health System Clinical Pathway: Whipple Enhanced Recovery After () LOS: 4-5 days Date of Origin/Revision: June 29, 2016/September 6, 2017/January 31, 2018 : SAS : : : D1 D2 D 3/
University of Virginia Health System Clinical Pathway: Whipple Enhanced Recovery After () LOS: 4-5 days Date of Origin/Revision: June 29, 2016/September 6, 2017/January 31, 2018 : SAS : : : D1 D2 D 3/
SSI. Ren yu Zhang MD
 Ren yu Zhang MD 3 27 2014 1 SSI 16 million operative procedures in 2010. Overall SSI rate 1.9% for 2006 8. Accounts 31% of healthcare associated infection. Leads to further morbidity and mortality. Economic
Ren yu Zhang MD 3 27 2014 1 SSI 16 million operative procedures in 2010. Overall SSI rate 1.9% for 2006 8. Accounts 31% of healthcare associated infection. Leads to further morbidity and mortality. Economic
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons. Karol A Gutowski, MD, FACS
 Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Appendix G Explanation/Clarification Summary
 Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion
 How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
Hemodynamic Optimization HOW TO IMPLEMENT?
 Hemodynamic Optimization HOW TO IMPLEMENT? Why Hemodynamic Optimization? Are post-surgical complications exceptions? Patients undergoing surgery may develop post-surgical complications. The morbidity rate,
Hemodynamic Optimization HOW TO IMPLEMENT? Why Hemodynamic Optimization? Are post-surgical complications exceptions? Patients undergoing surgery may develop post-surgical complications. The morbidity rate,
The Centers for Medicare & Medicaid Services (CMS) Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures
 Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures") ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
Simone Targa. Impact of an ERAS Colorectal Program on clinical outcomes and costs
 Impact of an ERAS Colorectal Program on clinical outcomes and costs Simone Targa U.O. di Clinica Chirurgica Azienda Ospedaliero-Universitaria di Ferrara Arcispedale S. Anna ERAS Protocol ENHANCED RECOVERY
Impact of an ERAS Colorectal Program on clinical outcomes and costs Simone Targa U.O. di Clinica Chirurgica Azienda Ospedaliero-Universitaria di Ferrara Arcispedale S. Anna ERAS Protocol ENHANCED RECOVERY
Mandatory Elements of Healthcare Reform Walter Coleman. healthcare consulting
 Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Baptist Health Lexington. ERAS Protocols
 Baptist Health Lexington ERAS Protocols Enhanced Recovery After Surgery BHLex Colorectal ERAS Protocol Preoperative Patient/Family Education: PAT and office, ERAS brochure & educational flyer/checklist
Baptist Health Lexington ERAS Protocols Enhanced Recovery After Surgery BHLex Colorectal ERAS Protocol Preoperative Patient/Family Education: PAT and office, ERAS brochure & educational flyer/checklist
Surgical Site Infection (SSI) Surveillance Update (with special reference to Colorectal Surgeries)
 Surveillance Update (with special reference to Colorectal Surgeries)") Surgical Site Infection (SSI) Surveillance Update (with special reference to Colorectal Surgeries) Where we started and where we re going Anjum Khan MBBS MSc CIC Infection Control Professional Department
Surgical Site Infection (SSI) Surveillance Update (with special reference to Colorectal Surgeries) Where we started and where we re going Anjum Khan MBBS MSc CIC Infection Control Professional Department
Quality Committee Core Measures Report AMI. Acute Myocardial Infarction
 AMI 2011 Acute Myocardial Infarction ASPIRIN AT ARRIVAL: A higher number is better. This measure shows the percentage of heart attack patients who receive aspirin within 24 hrs of arrival at hospital.
AMI 2011 Acute Myocardial Infarction ASPIRIN AT ARRIVAL: A higher number is better. This measure shows the percentage of heart attack patients who receive aspirin within 24 hrs of arrival at hospital.
Operational Efficiency in Colon Surgery Enhanced Recovery Pathways: 23 hour laparoscopic colectomy
 Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
SCIP and NSQIP the Alphabet Soup of Surgical Quality
 SCIP and NSQIP the Alphabet Soup of Surgical Quality NSQIP National Conference Christopher C Johnson M.D. Caryn Foster RN, SCR Nicholas Hellenthal M.D., F.A.C.S. 7/26/15 Disclosure None Introduction The
SCIP and NSQIP the Alphabet Soup of Surgical Quality NSQIP National Conference Christopher C Johnson M.D. Caryn Foster RN, SCR Nicholas Hellenthal M.D., F.A.C.S. 7/26/15 Disclosure None Introduction The
Anesthesia for OutPatient Spine Surgery. Michael A. Kellams, D.O.
 Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Disclosures. Personalized Approaches to Gastrointestinal Cancers. Objectives. What is personalized cancer care. Go through some genomic studies
 Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Compliance with SCIP core measures and the Impact on Surgical Site Infections
 Compliance with SCIP core measures and the Impact on Surgical Site Infections Using NSQIP to Evaluate Patient Outcomes and Reimbursement Guidelines Rickesha L. Wilson, MD July 28, 2014 2014 ACS NSQIP National
Compliance with SCIP core measures and the Impact on Surgical Site Infections Using NSQIP to Evaluate Patient Outcomes and Reimbursement Guidelines Rickesha L. Wilson, MD July 28, 2014 2014 ACS NSQIP National
Form 1: Demographics
 Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Enhanced Recovery Thoracic Surgery. Esophagus Pathway
 Enhanced Recovery Thoracic Surgery Esophagus Pathway Preoperative Patient Education/Expectations for Hospital and Home Medical Risk Consultation: Cardiac Clearance and PFTs for All Patients Surgery Wellness
Enhanced Recovery Thoracic Surgery Esophagus Pathway Preoperative Patient Education/Expectations for Hospital and Home Medical Risk Consultation: Cardiac Clearance and PFTs for All Patients Surgery Wellness
CMS Hospital IQR Program Measure Comparison Tables FY 2018 (CY 2016) Measures Required to Meet Hospital IQR APU Requirements NHSN Submission
 Measures Required to Meet Hospital IQR APU Requirements NHSN Submission") CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
A comparison of peri-operative outcomes between elective and non-elective total hip arthroplasties
 Original Article Page 1 of 8 A comparison of peri-operative outcomes between elective and non-elective total hip arthroplasties Hiba K. Anis 1, Nipun Sodhi 2, Marine Coste 2, Joseph O. Ehiorobo 2, Jared
Original Article Page 1 of 8 A comparison of peri-operative outcomes between elective and non-elective total hip arthroplasties Hiba K. Anis 1, Nipun Sodhi 2, Marine Coste 2, Joseph O. Ehiorobo 2, Jared
Welcome Charles Kennedy
 Welcome Charles Kennedy Comoderators Girish P. Joshi, MBBS, MD, FFARCI Professor of Anesthesiology and Pain Management University of Texas Southwestern Medical Center Dallas, Texas David E. Beck, MD, FACS
Welcome Charles Kennedy Comoderators Girish P. Joshi, MBBS, MD, FFARCI Professor of Anesthesiology and Pain Management University of Texas Southwestern Medical Center Dallas, Texas David E. Beck, MD, FACS
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
To staple or to sew. Zeng Xuan Hu
 To staple or to sew Zeng Xuan Hu Fast Track Surgery Multimodal Rehabilitation Accelerated recovery Accelerated rehabilitation Enhanced recovery Optimize perioperative care by reducing the expected stress
To staple or to sew Zeng Xuan Hu Fast Track Surgery Multimodal Rehabilitation Accelerated recovery Accelerated rehabilitation Enhanced recovery Optimize perioperative care by reducing the expected stress
Rapid Response Teams. January 17, Safe Table Webinar
 Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Performance Measure. Inpatient Clinical Process of Care Measures
 Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS
 NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS Bruce L. Hall, MD, PhD, MBA, FACS Clinical Support Physician Lead Paula Farrell, RN, BSN ACS NSQIP Clinical Support Specialist Case Studies &
NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS Bruce L. Hall, MD, PhD, MBA, FACS Clinical Support Physician Lead Paula Farrell, RN, BSN ACS NSQIP Clinical Support Specialist Case Studies &
R Sim, D Cheong, KS Wong, B Lee, QY Liew Tan Tock Seng Hospital Singapore
 Prospective randomized, double-blind, placebo-controlled study of pre- and postoperative administration of a COX-2- specific inhibitor as opioid-sparing analgesia in major colorectal resections R Sim,
Prospective randomized, double-blind, placebo-controlled study of pre- and postoperative administration of a COX-2- specific inhibitor as opioid-sparing analgesia in major colorectal resections R Sim,
AMI Talking Points. Provide appropriate treatment to Acute MI patients with these core measures:
 AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
Best Practices for Fast Track in Bariatric Surgery: Enhanced Recovery After Bariatric Surgery
 Best Practices for Fast Track in Bariatric Surgery: Enhanced Recovery After Bariatric Surgery Abdelrahman Nimeri, MBBCh, FACS, FASMBS ACS NSQIP Surgeon Champion Chief of General, Thoracic & Vascular Surgery
Best Practices for Fast Track in Bariatric Surgery: Enhanced Recovery After Bariatric Surgery Abdelrahman Nimeri, MBBCh, FACS, FASMBS ACS NSQIP Surgeon Champion Chief of General, Thoracic & Vascular Surgery
How to Address an Inappropriately high Readmission Rate?
 How to Address an Inappropriately high Readmission Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Medical Officer CDC/DHPQ Disclosure Slide No COI and no disclosures. OBJECTIVES
How to Address an Inappropriately high Readmission Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Medical Officer CDC/DHPQ Disclosure Slide No COI and no disclosures. OBJECTIVES
Balanced Analgesia With NSAIDS and Coxibs. Raymond S. Sinatra MD, Ph.D
 Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting.
 The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting. { Thalia Petropoulou, Clinical Fellow Paul Hainsworth,Colorectal
The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting. { Thalia Petropoulou, Clinical Fellow Paul Hainsworth,Colorectal
Demographics. MBSAQIP Case Number: *ACS NSQIP Case Number: *LMRN: *DOB: / / *Gender: Male Female
 Demographics MBSAQIP Case Number: *IDN: *ACS NSQIP Case Number: Name: *LMRN: *DOB: / / *Gender: Male Female *Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other
Demographics MBSAQIP Case Number: *IDN: *ACS NSQIP Case Number: Name: *LMRN: *DOB: / / *Gender: Male Female *Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other
Malnutrition: An independent Risk Factor for Postoperative Complications
 Malnutrition: An independent Risk Factor for Postoperative Complications Bryan P. Hooks, D.O. University of Pittsburgh-Horizon June 24, 2017 Orthopedic Surgeon-Adult Reconstruction Disclosures: None Objectives:
Malnutrition: An independent Risk Factor for Postoperative Complications Bryan P. Hooks, D.O. University of Pittsburgh-Horizon June 24, 2017 Orthopedic Surgeon-Adult Reconstruction Disclosures: None Objectives:
ENHANCED RECOVERY PROTOCOLS FOR KNEE REPLACEMENT
 ENHANCED RECOVERY PROTOCOLS FOR KNEE REPLACEMENT Jeff Gadsden, MD, FRCPC, FANZCA Associate Professor Duke University Department of Anesthesiology Regional Anesthesia and Acute Pain Medicine DISCLOSURES
ENHANCED RECOVERY PROTOCOLS FOR KNEE REPLACEMENT Jeff Gadsden, MD, FRCPC, FANZCA Associate Professor Duke University Department of Anesthesiology Regional Anesthesia and Acute Pain Medicine DISCLOSURES
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital
 Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
-DVT and PE Reduction Strategy in AWR- Can We Win? Luciano Tastaldi, MD
 -DVT and PE Reduction Strategy in AWR- Can We Win? Luciano Tastaldi, MD Summary of the Project Objectives Present Numbers Evolution Challenges of Implementation Discuss Future Directions -Problem at CCF-
-DVT and PE Reduction Strategy in AWR- Can We Win? Luciano Tastaldi, MD Summary of the Project Objectives Present Numbers Evolution Challenges of Implementation Discuss Future Directions -Problem at CCF-
Outpatient Total Knee Arthroplasty: Anesthetic Implications
 Outpatient Total Knee Arthroplasty: Anesthetic Implications Anthony Edelman, MD, MBA Clinical Assistant Professor Director, Division of Orthopedic Anesthesia Disclosures None Objectives Examine current
Outpatient Total Knee Arthroplasty: Anesthetic Implications Anthony Edelman, MD, MBA Clinical Assistant Professor Director, Division of Orthopedic Anesthesia Disclosures None Objectives Examine current
Enhanced Recovery After Surgery (ERAS)
") Enhanced Recovery After Surgery (ERAS) Brad White, D.O. Anesthesiology Residency Program Director Oklahoma State University Medical Center Assistant Clinical Professor of Anesthesiology Oklahoma State
Enhanced Recovery After Surgery (ERAS) Brad White, D.O. Anesthesiology Residency Program Director Oklahoma State University Medical Center Assistant Clinical Professor of Anesthesiology Oklahoma State
Wind, Water, Wound, Walk Do the Data Deliver the Dictum?
 Wind, Water, Wound, Walk Do the Data Deliver the Dictum? Elizabeth M. Sonnenberg, MD, Caroline E. Reinke, MD MSHP, Edmund K. Bartlett, MD, Karole T. Collier, Giorgos C. Karakousis, MD, Daniel N. Holena,
Wind, Water, Wound, Walk Do the Data Deliver the Dictum? Elizabeth M. Sonnenberg, MD, Caroline E. Reinke, MD MSHP, Edmund K. Bartlett, MD, Karole T. Collier, Giorgos C. Karakousis, MD, Daniel N. Holena,
Quality & Hospital Acquired Conditions
 Quality & Hospital Acquired Conditions Rebecca Armbruster, DO, MS, FACOI Medical Director Resource Management Patricia Heys, BS Director of Infection Prevention & Control Sally Hinkle, DNP, MPA, RN Director
Quality & Hospital Acquired Conditions Rebecca Armbruster, DO, MS, FACOI Medical Director Resource Management Patricia Heys, BS Director of Infection Prevention & Control Sally Hinkle, DNP, MPA, RN Director
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2019 Payment Update
 Program Measures for the FY 2019 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
Enhanced Recovery After Surgery in Combination with the Advanced Colon Bundle
 Enhanced Recovery After Surgery in Combination with the Advanced Colon Bundle September 2017 1 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
Enhanced Recovery After Surgery in Combination with the Advanced Colon Bundle September 2017 1 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
Enhanced Recovery After Surgery: Where Do Pharmacists Come In?
 Enhanced Recovery After Surgery: Where Do Pharmacists Come In? Melinda C. Joyce, Pharm.D., FAPhA, FACHE Vice President, Corporate Support Services Med Center Health Bowling Green, Kentucky Annual Meeting
Enhanced Recovery After Surgery: Where Do Pharmacists Come In? Melinda C. Joyce, Pharm.D., FAPhA, FACHE Vice President, Corporate Support Services Med Center Health Bowling Green, Kentucky Annual Meeting
Nursing Management Plan Small or large bowel
 Nursing Management Plan Small or large bowel Highlight the procedure/s and add other details: Open / Laparoscopic Assisted Hemicolectomy / Right / Left / Extended Sigmoid Colectomy / Transverse Colectomy
Nursing Management Plan Small or large bowel Highlight the procedure/s and add other details: Open / Laparoscopic Assisted Hemicolectomy / Right / Left / Extended Sigmoid Colectomy / Transverse Colectomy
Surgical Site Infections: the international guidelines for best practices and effective actions
 Surgical Site Infections: the international guidelines for best practices and effective actions SSIs are the second most common type of adverse event occurring in hospitalised patients. SSIs have been
Surgical Site Infections: the international guidelines for best practices and effective actions SSIs are the second most common type of adverse event occurring in hospitalised patients. SSIs have been
FTS Oesophagectomy: minimal research to date 3,4
 Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
7/31/2015. Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice. Objectives. Enhanced Recovery Society
 Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice Margaret Odhner MS, ANP-BC, COCN Kim Meacham, MSN FNP-C, CWON Objectives 1. Describe the Enhanced Recover After Surgery (ERAS) pathway.
Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice Margaret Odhner MS, ANP-BC, COCN Kim Meacham, MSN FNP-C, CWON Objectives 1. Describe the Enhanced Recover After Surgery (ERAS) pathway.
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2020 Payment Update
 Program Measures for the FY 2020 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
Advances in Joint Replacement
 Advances in Joint Replacement Seth Greenky, MD Chairman, Musculoskeletal Services, St. Joseph s Hospital Partner, Syracuse Orthopedic Specialists Associate Clinical Professor, Upstate Medical Center CoMedical
Advances in Joint Replacement Seth Greenky, MD Chairman, Musculoskeletal Services, St. Joseph s Hospital Partner, Syracuse Orthopedic Specialists Associate Clinical Professor, Upstate Medical Center CoMedical
Opioid reduction strategies in an academic tertiary medical center
 Opioid reduction strategies in an academic tertiary medical center Terry Bosen, PharmD Medication Safety Program Director Vanderbilt University Medical Center Tennessee MME data per capita MME = Morphine
Opioid reduction strategies in an academic tertiary medical center Terry Bosen, PharmD Medication Safety Program Director Vanderbilt University Medical Center Tennessee MME data per capita MME = Morphine
Preoperative Optimization and Surgical Site Infection Reduction
 Preoperative Optimization and Surgical Site Infection Reduction David Evans, MD Medical Director of Trauma Services Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn
Preoperative Optimization and Surgical Site Infection Reduction David Evans, MD Medical Director of Trauma Services Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn
Preoperative Optimization and Surgical Site Infection Reduction
 Preoperative Optimization and Surgical Site Infection Reduction David Evans, MD Medical Director of Trauma Services Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn
Preoperative Optimization and Surgical Site Infection Reduction David Evans, MD Medical Director of Trauma Services Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn
Anesthetic Techniques for Rapid Recovery in Total Knee Arthroplasty
 Anesthetic Techniques for Rapid Recovery in Total Knee Arthroplasty Scott T. Ball, MD Chief, Adult Joint Reconstruction Department of Orthopaedic Surgery University of California, San Diego Disclosures
Anesthetic Techniques for Rapid Recovery in Total Knee Arthroplasty Scott T. Ball, MD Chief, Adult Joint Reconstruction Department of Orthopaedic Surgery University of California, San Diego Disclosures
ADE and Harm Collaborative: Reducing ADEs and harm associated with opioids - Safer post-operative pain management. March 21, 2013
 ADE and Harm Collaborative: Reducing ADEs and harm associated with opioids - Safer post-operative pain management March 21, 2013 Agenda, March 21, 2013 Welcome Collaborative education overview Post-operative
ADE and Harm Collaborative: Reducing ADEs and harm associated with opioids - Safer post-operative pain management March 21, 2013 Agenda, March 21, 2013 Welcome Collaborative education overview Post-operative
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Every Day Counts: Interventions to Improve VTE and Length of Stay in Patients Undergoing Radical Cystectomy
 Every Day Counts: Interventions to Improve VTE and Length of Stay in Patients Undergoing Radical Cystectomy John A. Brockman, Steven B. Brandes, Arnold D. Bullock, Robert L. Grubb III, Gurdarshan Sandhu,
Every Day Counts: Interventions to Improve VTE and Length of Stay in Patients Undergoing Radical Cystectomy John A. Brockman, Steven B. Brandes, Arnold D. Bullock, Robert L. Grubb III, Gurdarshan Sandhu,
Preventing CLABSI & CAUTI Preventive Measures for Central Line Associated Bloodstream Infection & Catheter Associated UTI
 Preventing CLABSI & CAUTI Preventive Measures for Central Line Associated Bloodstream Infection & Catheter Associated UTI Kaiser Permanente For Internal use only Objectives By the end of this lesson, you
Preventing CLABSI & CAUTI Preventive Measures for Central Line Associated Bloodstream Infection & Catheter Associated UTI Kaiser Permanente For Internal use only Objectives By the end of this lesson, you
2016 Hospital Measures
 2016 Hospital Measures Vicki Tang Olson, Stratis Health Statewide Quality Reporting and Measurement System (SQRMS) Annual Forum June 22, 2015 Objectives Share the process used for 2016 hospital measures
2016 Hospital Measures Vicki Tang Olson, Stratis Health Statewide Quality Reporting and Measurement System (SQRMS) Annual Forum June 22, 2015 Objectives Share the process used for 2016 hospital measures
WHS POSTOPERATIVE POWERPLAN CHANGES
 Medications simplified and standardized to improve safety and effectiveness in the management of pain, itching, nausea/vomiting. Management: o The Anesthesiologist will continue to manage pain in the PACU.
Medications simplified and standardized to improve safety and effectiveness in the management of pain, itching, nausea/vomiting. Management: o The Anesthesiologist will continue to manage pain in the PACU.
Proof 2. CLINICAL PATHWAY PLAN CLINIQUE GENERAL SURGERY CHIRURGIE GÉNÉRAL Enhanced Recovery After Surgery (ERAS) Bowel Surgery /
 Bowel Surgery /") CLINICAL PATHWAY PLAN CLINIQUE GENERAL SURGERY CHIRURGIE GÉNÉRAL Enhanced Recovery After Surgery (ERAS) Bowel Surgery / Proof 2 Addressograph/Plaque Cancer Assessment Clinic (CAC) Date: yyaa mm dj Day
CLINICAL PATHWAY PLAN CLINIQUE GENERAL SURGERY CHIRURGIE GÉNÉRAL Enhanced Recovery After Surgery (ERAS) Bowel Surgery / Proof 2 Addressograph/Plaque Cancer Assessment Clinic (CAC) Date: yyaa mm dj Day
Enhanced Recovery After Discharge: does it happen?
 Enhanced Recovery After Discharge: does it happen? Nader K Francis ERAS-UK Southampton 14 th November 2014 BJS 2014 Functional / symptoms Length of hospital stay 37 Readmission 29 Pain 16 Fatigue 9 BJS
Enhanced Recovery After Discharge: does it happen? Nader K Francis ERAS-UK Southampton 14 th November 2014 BJS 2014 Functional / symptoms Length of hospital stay 37 Readmission 29 Pain 16 Fatigue 9 BJS
Educational Learning Objectives. Evidence into Practice. Audience. Case Presentation. Outline. Multimodal Approach to Colorectal Surgery
 Educational Learning Objectives Multimodal Approach to Colorectal Surgery Value and Impact of Nutrition Interventions May 5, 2011 Dr. Corilee A. Watters, MSc, RD, PhD, CNSC Asst. Prof, Nutrition, University
Educational Learning Objectives Multimodal Approach to Colorectal Surgery Value and Impact of Nutrition Interventions May 5, 2011 Dr. Corilee A. Watters, MSc, RD, PhD, CNSC Asst. Prof, Nutrition, University
Michael Minarich, MD General Surgery Resident, PGY4 Cooper University Hospital
 BMI as Major Preoperative Risk Factor for Intraabdominal Infection After Distal Pancreatectomy: an Analysis of National Surgical Quality Improvement Program Database Michael Minarich, MD General Surgery
BMI as Major Preoperative Risk Factor for Intraabdominal Infection After Distal Pancreatectomy: an Analysis of National Surgical Quality Improvement Program Database Michael Minarich, MD General Surgery
Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals
 Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals Mila H. Ju, MD, MS Ryan P. Merkow, MD, MS Jeanette W. Chung,
Is Readmission a Good Quality Measure for Surgical Care? Examining the Underlying Reasons for Readmissions after Surgery at ACS NSQIP Hospitals Mila H. Ju, MD, MS Ryan P. Merkow, MD, MS Jeanette W. Chung,
Predicting Short Term Morbidity following Revision Hip and Knee Arthroplasty
 Predicting Short Term Morbidity following Revision Hip and Knee Arthroplasty A Review of ACS-NSQIP 2006-2012 Arjun Sebastian, M.D., Stephanie Polites, M.D., Kristine Thomsen, B.S., Elizabeth Habermann,
Predicting Short Term Morbidity following Revision Hip and Knee Arthroplasty A Review of ACS-NSQIP 2006-2012 Arjun Sebastian, M.D., Stephanie Polites, M.D., Kristine Thomsen, B.S., Elizabeth Habermann,
Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications
 Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications Abstract Authors: Karen Martin, RHIT, CPHQ - Surgical Clinical Reviewer - Quality Management Analyst,
Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications Abstract Authors: Karen Martin, RHIT, CPHQ - Surgical Clinical Reviewer - Quality Management Analyst,
Thirty-Day Outcomes of Laparoscopic vs. Open Total Proctocolectomy with Ileoanal Anastomosis in Children
 Thirty-Day Outcomes of Laparoscopic vs. Open Total Proctocolectomy with Ileoanal Anastomosis in Children Jeremy D. Kauffman MD, Paul D. Danielson MD, Nicole M. Chandler MD Johns Hopkins All Children s
Thirty-Day Outcomes of Laparoscopic vs. Open Total Proctocolectomy with Ileoanal Anastomosis in Children Jeremy D. Kauffman MD, Paul D. Danielson MD, Nicole M. Chandler MD Johns Hopkins All Children s
SCOAP Report: Q Hospital XX
 SCOAP Report: Q1 2009 Hospital XX SCOAP is an approved Coordinated Quality Improvement Program protected under Washington State Law, RCW 43.70.510. Unauthorized use or reproduction is strictly prohibited
SCOAP Report: Q1 2009 Hospital XX SCOAP is an approved Coordinated Quality Improvement Program protected under Washington State Law, RCW 43.70.510. Unauthorized use or reproduction is strictly prohibited
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations
 50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
Upstate New York Surgical Quality Initiative
 Upstate New York Surgical Quality Initiative 30-Day Readmissions: A Snapshot of Regional Practice Experience in Colorectal Surgery ACS NSQIP National Conference 10 th Annual Meeting, July 27 th, 2015 Bradley
Upstate New York Surgical Quality Initiative 30-Day Readmissions: A Snapshot of Regional Practice Experience in Colorectal Surgery ACS NSQIP National Conference 10 th Annual Meeting, July 27 th, 2015 Bradley
DIVISION OF QUALITY & PATIENT SAFETY. The National Comparative Effectiveness Summit, Washington D.C. 11/6/2012
 Cost Effectiveness of MRSA Screening & Decolonization Joseph A. Bosco, MD, Vice Chair of Clinical Affairs James Slover, MD, MS, Associate Professor, Orthopaedic Surgeon Lorraine Hutzler, Quality Project
Cost Effectiveness of MRSA Screening & Decolonization Joseph A. Bosco, MD, Vice Chair of Clinical Affairs James Slover, MD, MS, Associate Professor, Orthopaedic Surgeon Lorraine Hutzler, Quality Project
GENERAL SURGICAL ADULT POST-OPERATIVE ORDERS 1 of 4
 down ADULT POST-OPERATIVE 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Admit to: Post Anesthesia Care Unit (PACU),
down ADULT POST-OPERATIVE 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Admit to: Post Anesthesia Care Unit (PACU),
Breakout Session 2: Bariatric Quality Improvement
 Breakout Session 2: Bariatric Quality Improvement Updated Agenda: 1. Drilling down on the data: Matt Hutter Online Reports and Bariatric SAR 2. Collaboratives to Accelerate QI Robin Blackstone 3. MGH and
Breakout Session 2: Bariatric Quality Improvement Updated Agenda: 1. Drilling down on the data: Matt Hutter Online Reports and Bariatric SAR 2. Collaboratives to Accelerate QI Robin Blackstone 3. MGH and
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery
 Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery Zhobin Moghadamyeghaneh MD 1, Michael J. Stamos MD 1 1 Department of Surgery, University of California, Irvine Nothing to
Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery Zhobin Moghadamyeghaneh MD 1, Michael J. Stamos MD 1 1 Department of Surgery, University of California, Irvine Nothing to
Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures
 Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures Audrey Paulman, MD, MMM Principal Clinical Coordinator & Jackie Trojan, RN, BSN Quality Improvement Advisor This material
Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures Audrey Paulman, MD, MMM Principal Clinical Coordinator & Jackie Trojan, RN, BSN Quality Improvement Advisor This material
Day of Surgery Discharge after Unicompartmental Knee Arthroplasty (UKA): An Effective Perioperative Pathway. Jay Patel, MD Hoag Orthopedic Institute
: An Effective Perioperative Pathway. Jay Patel, MD Hoag Orthopedic Institute") Day of Surgery Discharge after Unicompartmental Knee Arthroplasty (UKA): An Effective Perioperative Pathway Jay Patel, MD Hoag Orthopedic Institute UKA Rapid Recovery Protocol Purpose of Study Describe
Day of Surgery Discharge after Unicompartmental Knee Arthroplasty (UKA): An Effective Perioperative Pathway Jay Patel, MD Hoag Orthopedic Institute UKA Rapid Recovery Protocol Purpose of Study Describe
COOK COUNTY HEALTH Meaningful Metrics
 COOK COUNTY HEALTH Meaningful Metrics 2018-2019 Ronald Wyatt MD MHA January 18, 2019 2 Meaningful Measures 3 Meaningful Measures Framework Meaningful Measure Areas Achieve: High quality healthcare Meaningful
COOK COUNTY HEALTH Meaningful Metrics 2018-2019 Ronald Wyatt MD MHA January 18, 2019 2 Meaningful Measures 3 Meaningful Measures Framework Meaningful Measure Areas Achieve: High quality healthcare Meaningful