Infectious Diseases Emergencies. Tirdad T. Zangeneh, DO, FACP, FIDSA Division of Infectious Diseases University of Arizona
|
|
|
- Bridget Tate
- 6 years ago
- Views:
Transcription



1 Infectious Diseases Emergencies Tirdad T. Zangeneh, DO, FACP, FIDSA Division of Infectious Diseases University of Arizona

2 Disclosures I have a grant from Astellas Pharmaceuticals I will not discuss off-label use and/or investigational use in my presentation
3 Learning Objectives Review principles of recognition and management of a selection of commonly encountered infectious disease emergencies in the primary care setting Identify strategies to diagnose, treat, and prevent life threatening infectious diseases commonly encountered by primary care providers Discuss effective management strategies when working with infectious disease consultants/specialists
4 I have a bad headache A 55 year old healthy woman c/o severe headache for 3 days, associated with fever, nausea, and vomiting Self-diagnosed sinus infection but did not take any antibiotics Her family called EMS when she became disoriented



5 Meningoencephalitis
6 A Continuum of Syndromes Meningitis Acute: Fever, headache, +/- altered mental status Chronic: More gradual, less severe Encephalitis Mental status change may occur early and may progress to obtundation or coma Behavioral and speech disturbances
7 Analyzing the CSF The CSF formula Opening pressure Cell count and differential Protein Glucose Gram stain and culture Normal Values Pressure 9 18 cm H 2 O WBC/mm Protein mg/dl Glucose mg/dl Appearance - Clear Do not waste CSF on unnecessary tests; it is difficult to get more!
8 Differential Diagnosis WBC 90% mononuclear Normal glucose Mildly elevated protein Viral or Aseptic Neurosyphilis Enteroviral PCR West Nile IgM HSV PCR VDRL WBC 90% neutrophils Glucose < 10 Elevated protein Bacterial Await Gram stain and culture Blood cultures WBC 90% mononuclear Glucose < 40 Very elevated protein Fungal TB Fungal culture Cryptococcal Ag Coccidioides Ab AFB culture
9 Management
10 Treatment of S. pneumoniae Penicillin resistance is increasing Antibiotic levels in CSF reach only 2-10% of serum levels PCN CSF breakpoints: <0.1 ug/ml ug/ml 2.0 ug/ml

11 Treatment
12 My father is just not himself An 82 year old man presented to the clinic with fever, fatigue, urinary incontinence, confusion, and was reported to have been walking naked in the house Urinalysis showed significant bacteriuria and pyuria and was diagnosed with a UTI and was prescribed Levofloxacin The following day he continued to have fever and worsening confusion He was transferred to the ED that evening with reports of having developed aphasia, ataxia, and an episode of seizure

13 Herpes Simplex Virus (HSV) Encephalitis Reactivation in cranial nerve ganglia and retrograde spread along axons Involvement of temporal lobe with personality changes, seizures, focal neurologic findings Diagnosis: HSV 1/2 CSF PCR Intravenous Acyclovir is recommended
14 Herpes Simplex Virus (HSV) Encephalitis Meningitis HSV 2 >> 1 Associated with primary infection Normal mental status Can be recurrent (Mollaret) Benign Encephalitis HSV 1 >> 2 Usually not primary in adults Abnormal mental status Usually no oral lesions Acyclovir decreases mortality Whitley et al JAMA 1982:247:317
15 My Foot is Swollen A 50-y/o woman presented to the ED because of severe pain and swelling of her left foot She had been well until 2 days earlier, when she noticed a lesion on her foot, thought to be an insect bite The next day, her foot became swollen and painful, she felt ill and febrile, and on the way to the ED she became confused and hypotensive The skin appeared cyanotic and cool. The foot was mottled with a black eschar; the swelling extended up the thigh
16 Necrotizing Fasciitis Necrotizing soft tissue infections include necrotizing forms of cellulitis, myositis, and fasciitis Type I necrotizing fasciitis, at least one anaerobic species is isolated in combination with one or more facultative anaerobic species such as streptococci (other than group A) and members of the Enterobacteriaceae Type II, group A streptococci are isolated alone or in combination with other species, most commonly S. aureus



17 Clinical Presentation Necrotizing fasciitis can affect any part of the body but is most common on the extremities Other sites of predilection are the abdominal wall, perianal and groin areas, and postoperative wounds The portal of entry is usually a site of trauma, postsurgical procedure, perirectal abscess, decubitus ulcer, or intestinal perforation
18 Clinical Presentation Clinical features suggestive of necrotizing fasciitis: Severe, constant pain Bullae (occlusion of deep blood vessels that traverse the fascia) Skin necrosis or ecchymosis that precedes skin necrosis Gas in the soft tissues, detected by palpation or imaging Edema that extends beyond the margin of erythema Cutaneous anesthesia Systemic toxicity (fever, leukocytosis, delirium, and renal failure) Rapid spread, especially during antibiotic therapy


19 Diagnosis Prompt diagnosis is crucial because of the rapidity with which the process can progress and a mortality rate of 24% to 34% The most expeditious route to diagnosis is through surgical exploration without delay for imaging studies; CT scanning and magnetic resonance imaging (MRI) can demonstrate subcutaneous and fascial edema, and tissue gas Frozen section examination of biopsy specimens is helpful for early diagnosis

20 Stevens DL, Bryant AE. N Engl J Med ;377:

21 Treatment

22 Treatment IDSA Guidelines 2014
23 Clindamycin is highly recommended for the treatment of Necrotizing fasciitis caused by which bacteria? A. MRSA B. MSSA C. Vibrio Vulnificus D. Streptococcal pyogenes E. Anaerobic infection with Bacteroides species F. Streptococcal agalactiae
24 Group A streptococci Clindamycin has greater efficacy against Group A streptococci because of greater activity against large bacterial populations in stationary phase of growth Suppression of toxins and virulence factors by inhibiting bacterial protein synthesis For group A streptococcal and b-hemolytic streptococci, treatment may be narrowed to the combination of penicillin and clindamycin

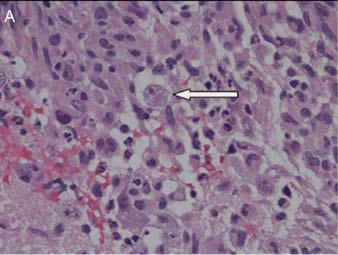
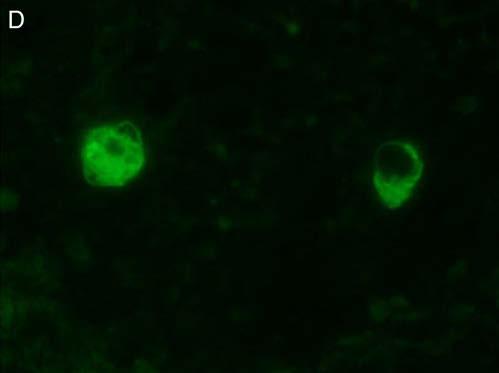
25 Please examine me! 45 y/o woman with Diabetes is in the ICU with respiratory failure on broad spectrum antibiotics On day 3 of ICU admission the nurse notifies you that the patient has developed periorbital and facial swelling, and has dark material present on the palate

26 Invasive Orbitorhinocerebral Mucormycosis


27 Pathogenesis Role in Diabetic Ketoacidosis: Diminished capacity of transferrin to bind to and sequester free iron at a ph of <7.4
28 Risk Factors
29 Management Histopathology with culture is recommended for identification Broad, non-septate hyphae with right-angle branching using calcofluor white and methenamine silver stains
30 My back is killing me A 24 y/o Woman presents to the ED with c/o fever, severe back pain described as "shooting and stabbing in nature, lower extremity weakness with decreased sensation, difficulty walking, and bladder dysfunction
31 Imaging Epidural abscess extending from the L4-S1 levels causing severe thecal sac stenosis with cauda equina impingement
32 Microbiology S. aureus (Over 60% of cases) Gram-negative bacilli Streptococci Coagulase-negative staphylococci Anaerobes Others (fungi, tuberculosis, parasites)

33 Abscesses are more likely to develop in larger epidural spaces that contain infection-prone fat
34 Management of Spinal Epidural Abscess
35 I feel like I am going to die A 23 year old man is admitted with c/o of fever, chills, headaches, malaise, myalgias, nausea and vomiting He reported visiting family in White River three days prior to his presentation Labs: Sodium 121, Hemoglobin 10, Platelets 94,000, AST 210, ALT 250

36 Rocky Mountain Spotted Fever in Arizona From 2002-present, over 266 cases of RMSF have been reported in Arizona There have been 21 deaths Case fatality 7%, ~ 15 X higher than the U.S. rate 2013: Confirmed-9 Probable-54 death-1 Cases occur in clusters due to common household exposures


37 The Primary Arizona Tick Vector of RMSF Rhipicephalus sanguineus Brown dog tick
38 RMSF: Clinical Manifestations Early (first 4 days): Fever, headache, myalgia, abdominal pain + N/V/D; light rash may be present Thrombocytopenia, hyponatremia, elevated liver enzymes (AST, ALT) may occur Late (day 5 or later): Definitive petechial rash, altered mental status, seizures, cough, dyspnea, arrhythmias, hypotension, and severe abdominal pain
39 RMSF: The Rash Generally not apparent until day 2-5 of symptoms (only seen in 68% of AZ patients) Begins as 1 to 5 mm macules progressing to maculopapular May begin on ankles, wrists, and forearms, spreads to trunk Petechial rash is a late finding, occurs on or after day 6 Rash may be asymmetric, localized, or absent


40



41 Severe Sequelae
42 Antimicrobial Therapy of RMSF Pregnant adult or tetracycline allergic Non-pregnant adult or child >45 kg Child <45 kg Chloramphenicol 500 mg qid, less likely to prevent death Doxycycline 100 mg bid p.o. or i.v. Doxycycline 4.4 mg/kg/day in 2 divided doses p.o. or i.v. Therapy should be continued at least 72 h after defervescence AND until evidence of clinical improvement
43 Confirmation of R. rickettsii Serology (RMSF titer) Indirect immunofluorescence assay (IFA) Requires paired sera (acute and convalescent) Look for a change (4-fold) in antibody titers for confirmed infections Positive single titers or titers that do not rise are considered probable cases PCR Available at CDC. Can give a rapid result (48 hours) Skin biopsy (2-4mm) Whole blood of severely ill/fatal cases NOTE: Negative PCR does not rule-out RMSF

44 Brain Abscess

45 Brain Abscess: Clinical Presentation



46



47


48



49 Fatal Aspergillus fumisynneamatus Sinusitis with CNS invasion in a healthy 36 year old man
50 Red Herring A 75 year old man was seen in the clinic for having had fever, fatigue, and weight loss. He was admitted for further workup Urinalysis indicated hematuria and pyuria and cultures grew >100,000 CFU/mL of E. Coli One out of 4 blood cultures grew Viridans streptococci which was regarded as a contaminant
51 Red Herring He was discharged with a seven day course of Ciprofloxacin, but his symptoms persisted for another two months and he was prescribed several courses of antibiotics for reoccurring UTIs He presented to the ED three months after the initial hospitalization with altered mental status and heart failure He complained of back pain described as stabbing in nature, lower extremity weakness with decreased sensation, difficulty walking, and bladder dysfunction


52 Actual Diagnosis: Subacute Bacterial Endocarditis due to Viridans streptococci resulting in spinal epidural and brain abscesses
53 Infective Endocarditis (IE) Infection of the endocardium that involves the cardiac valves and adjacent structures Bacterial (most common), fungal, rickettsia Acute and subacute course



54 Microbiology S. aureus 31 percent Viridans group streptococci 17 percent Enterococci 11 percent Coagulase-negative staphylococci 11 percent Streptococcus bovis 7 percent Non-HACEK gram-negative bacteria 2 percent Fungi 2 percent HACEK 2 percent *Haemophilus spp Aggregatibacter [formerly Actinobacillus spp.] Cardiobacterium hominis Eikenella corrodens Kingella kingae


55 Consequences of Septic Emboli Mitral or aortic valve Left ventricle Aorta Large vessel Small vessel (Janeway lesions)
56 CNS Involvement Patients with left-sided IE were prospectively evaluated with cerebral MRI regardless of neurologic symptoms The total cerebrovascular complication rate was 65%, including 35% (symptomatic) and 30% (clinically silent) Middle cerebral artery and its branches are involved commonly Hemorrhagic transformation of septic emboli commonly results in fatal intracerebral hemorrhage Martin et al. Clin Infect Dis. 2008; 47:23
57 Which of the following would be the mostly likely pathogen in this rapidly expanding skin lesion in a febrile neutropenic patient with acute leukemia? A) Fusarium solani B) Streptococcus pyogenes C) Borrelia burgdoferi D) Pseudomonas aeruginosa

58 Which of the following would be the mostly likely pathogen in this rapidly expanding skin lesion in a febrile neutropenic patient with acute leukemia? A) Fusarium solani B) Streptococcus pyogenes C) Borrelia burgdoferi D) Pseudomonas aeruginosa
59 Neutropenic Fever Hospitalization for febrile neutropenia (FN) is associated with considerable morbidity, mortality, and cost By the early 1960s Gram-negative bacteremia in neutropenic patients carried a mortality rate of 90% In-hospital mortality associated with FN was 9.5% between 1995 and 2000 across 115 US medical centers (total of 41,779 patients) Hospital mortality of 50% has been reported in neutropenic patients with severe sepsis Kuderer NM, Cancer. 2006, Legrand M, Crit Care Med Klastersky J, Journal of Antimicrobial Chemotherapy. 2009



60 Sequence of events during neutropenia Mandell GL, Principals and Practice of Infectious Diseases, 8 th edition, 2016
61 Definitions Fever: A single oral temperature of 38.3 C (101 F) or a temperature of 38.0 C (100.4 F) sustained over 1 hour Neutropenia: ANC <500 cells/mm 3 or ANC that is expected to decrease to <500 cells/mm 3 during the next 48 hours The term profound is used to describe neutropenia in which the ANC is <100 cells/mm 3 and prolonged >7 days Functional neutropenia refers to qualitative defects of circulating neutrophils Freifeld AG, CID. 2011
62 Etiology Most patients will have no infectious etiology documented and clinically documented infections occur in 20% 30% of episodes Common sites of tissue-based infection include the intestinal tract, lungs, and skin Bacteremia occurs in 10% 25% of patients, with most occurring in the setting of prolonged or profound neutropenia (ANC <100 neutrophils/mm 3 ) Klastersky J. CID 2004; 39:S32 7 Ramphal R. CID 2004; 39:S25 31


63 Etiology of Bacteremia Mandell GL, Principals and Practice of Infectious Diseases, 8 th edition, 2016


64 Fever occurs frequently during chemotherapy-induced neutropenia: 10% 50% of patients with solid tumors Clinically documented infections occur in 20% 30% of febrile episodes Greater than 80% of those with hematologic malignancies will develop fever during 1 chemotherapy cycle associated with neutropenia Freifeld AG, CID. 2011
65 Initial in-hospital Treatment (A-II) Anticipated prolonged (>7 days duration) and profound neutropenia (ANC <100 cells/mm 3 ) Co-morbid conditions, hypotension, pneumonia, new-onset abdominal pain, or neurologic changes High-risk patients require intravenous empirical antibiotics with an antipseudomonal b-lactam agent (A-I) Low-risk patients with anticipated brief (<7 days duration) neutropenic period or few co-morbidities, are candidates for oral empirical therapy Freifeld AG, CID. 2011
66 Initial Empiric Therapy In high-risk patients requiring hospitalization for empirical antibiotic therapy, monotherapy with an anti-pseudomonal b-lactam agent is recommended Cefepime Carbapenem (meropenem or imipenem-cilastatin) Piperacillin-tazobactam Other antimicrobials may be added to the initial regimen for management of complications or if antimicrobial resistance is suspected or proven Aminoglycosides Fluoroquinolones Vancomycin Freifeld AG, CID. 2011
67 Indications for Use of Empiric Antibiotics Active Against Gram-Positive Organisms Hemodynamic instability, severe sepsis, or Pneumonia Positive blood culture for gram-positive bacteria, before final identification and susceptibility testing is available Clinically suspected serious catheter-related infection, skin or soft-tissue infection at any site Colonization with MRSA, vancomycin-resistant enterococcus, or penicillinresistant Streptococcus pneumoniae Severe mucositis, with fluoroquinolone prophylaxis Freifeld AG, CID. 2011
68 How Long Should Empirical Antibiotic Therapy be Given? In patients with unexplained fever, initial regimen is continued until there are clear signs of marrow recovery Increasing ANC that exceeds 500 cells/mm3 If appropriate treatment course has been completed and signs and symptoms of a documented infection have resolved, patients who remain neutropenic may resume oral fluoroquinolone prophylaxis until marrow recovery Freifeld AG, CID. 2011


69 Empirical or Preemptive Antifungal Therapy Empirical antifungal therapy and investigation is considered for patients with persistent or recurrent fever after 4 7 days of antibiotics and duration of neutropenia of >7 days Invasive mold infections, occur almost exclusively in high-risk patients with profound neutropenia lasting longer than days With preemptive treatment, antifungals are given when evidence is suggested, using a combination of clinical, serologic, and imaging findings Freifeld AG, CID. 2011

70 Cutaneous Presentations
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Michael Stander, Pharm.D.
 Michael Stander, Pharm.D. Endocarditis: Goals Epidemiology Presentation of acute and subacute. Diagnosis: What is Dukes Criteria and how do we approach the diagnosis of endocarditis? Treatment: Understand
Michael Stander, Pharm.D. Endocarditis: Goals Epidemiology Presentation of acute and subacute. Diagnosis: What is Dukes Criteria and how do we approach the diagnosis of endocarditis? Treatment: Understand
SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA. Lin Li, MD August, 2012
 SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA Lin Li, MD August, 2012 Case 1 32 year old male working in Arizona; on leave back in Singapore Presented to hospital A for fever x (7-10)
SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA Lin Li, MD August, 2012 Case 1 32 year old male working in Arizona; on leave back in Singapore Presented to hospital A for fever x (7-10)
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Sepsis and Infective Endocarditis
 Sepsis and Infective Endocarditis Michal Holub Department of Infectious Diseases First Faculty of Medicine Charles University in Prague and University Military Hospital Bacteremia and Sepsis bacteremia
Sepsis and Infective Endocarditis Michal Holub Department of Infectious Diseases First Faculty of Medicine Charles University in Prague and University Military Hospital Bacteremia and Sepsis bacteremia
Infective endocarditis (IE) By Assis. Prof. Nader Alaridah MD, PhD
 By Assis. Prof. Nader Alaridah MD, PhD") Infective endocarditis (IE) By Assis. Prof. Nader Alaridah MD, PhD Infective endocarditis (IE) is an inflammation of the endocardium.. inner of the heart muscle & the epithelial lining of heart valves.
Infective endocarditis (IE) By Assis. Prof. Nader Alaridah MD, PhD Infective endocarditis (IE) is an inflammation of the endocardium.. inner of the heart muscle & the epithelial lining of heart valves.
ACCME/Disclosures 4/13/2016 IDPB
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
Morbidity & Mortality Conference Downstate Medical Center. Daniel Kaufman, MD
 Morbidity & Mortality Conference Downstate Medical Center University Case Presentation Hospital of Brooklyn Daniel Kaufman, MD Necrotizing Fasciitis and Soft- Tissue Infections Necrotizing Fasciitis Deep
Morbidity & Mortality Conference Downstate Medical Center University Case Presentation Hospital of Brooklyn Daniel Kaufman, MD Necrotizing Fasciitis and Soft- Tissue Infections Necrotizing Fasciitis Deep
Microbiological diagnosis of infective endocarditis; what is new?
 Microbiological diagnosis of infective endocarditis; what is new? Dr Amani El Kholy, MD Professor of Clinical Pathology (Microbiology), Faculty of Medicine, Cairo University ESC 2017 1 Objectives Lab Diagnostic
Microbiological diagnosis of infective endocarditis; what is new? Dr Amani El Kholy, MD Professor of Clinical Pathology (Microbiology), Faculty of Medicine, Cairo University ESC 2017 1 Objectives Lab Diagnostic
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
General surgery department of SGMU Lecturer ass. Khilgiyaev R.H. Anaerobic infection. Gas gangrene
 Anaerobic infection Gas gangrene Anaerobic bacteria Anaerobic bacteria are the most numerous inhabitants of the normal gastrointestinal tract, including the mouth Bacteroides fragilis and Clostridium The
Anaerobic infection Gas gangrene Anaerobic bacteria Anaerobic bacteria are the most numerous inhabitants of the normal gastrointestinal tract, including the mouth Bacteroides fragilis and Clostridium The
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
MICHIGAN MEDICINE GUIDELINES FOR TREATMENT OF URINARY TRACT INFECTIONS IN ADULTS
 When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
- Mycoplasma and Ureaplasma. - Rickettsia
 - Mycoplasma and Ureaplasma - Rickettsia Mycoplasma and Ureaplasma Family: Mycoplasmataceae Genus: Mycoplasma Species: M. pneumoniae Species: M. hominis Species: M. genitalium Genus: Ureaplasma Species:
- Mycoplasma and Ureaplasma - Rickettsia Mycoplasma and Ureaplasma Family: Mycoplasmataceae Genus: Mycoplasma Species: M. pneumoniae Species: M. hominis Species: M. genitalium Genus: Ureaplasma Species:
Bacteriemia and sepsis
 Bacteriemia and sepsis Case 1 An 80-year-old man is brought to the emergency room by his son, who noted that his father had become lethargic and has decreased urination over the past 4 days. The patient
Bacteriemia and sepsis Case 1 An 80-year-old man is brought to the emergency room by his son, who noted that his father had become lethargic and has decreased urination over the past 4 days. The patient
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Febrile neutropenia. Febrile neutropenia. Febrile neutropenia. Febrile neutropenia 1/30/2019. Infection in patients with cancer
 Manit Sae-teaw B.Pharm, BCP, BCOP Glad dip in pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University Fever Oral temperature measurement of 38.3 C (101.0 F) single 38.0 C (100.4
Manit Sae-teaw B.Pharm, BCP, BCOP Glad dip in pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University Fever Oral temperature measurement of 38.3 C (101.0 F) single 38.0 C (100.4
Ready to answer the questions?
 파워포인트문서의제목 Reference 1. IDSA GUIDELINES. Clinical Practice Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Disease Society of America.
파워포인트문서의제목 Reference 1. IDSA GUIDELINES. Clinical Practice Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Disease Society of America.
Overview. Clinical Scenario. Endocarditis: Treatment & Prevention. Prophylaxis The Concept. Jeremy D. Young, MD, MPH. Division of Infectious Diseases
 Endocarditis: Treatment & Prevention Jeremy D. Young, MD, MPH Division of Infectious Diseases Clinical Scenario Patient with MVP scheduled to have wisdom teeth extracted. Has systolic murmur with mid-systolic
Endocarditis: Treatment & Prevention Jeremy D. Young, MD, MPH Division of Infectious Diseases Clinical Scenario Patient with MVP scheduled to have wisdom teeth extracted. Has systolic murmur with mid-systolic
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
Ailyn T. Isais-Agdeppa, MD*, Lulu Bravo, MD*
 A FIVE-YEAR RETROSPECTIVE STUDY ON THE COMMON MICROBIAL ISOLATES AND SENSITIVITY PATTERN ON BLOOD CULTURE OF PEDIATRIC CANCER PATIENTS ADMITTED AT THE PHILIPPINE GENERAL HOSPITAL FOR FEBRILE NEUTROPENIA
A FIVE-YEAR RETROSPECTIVE STUDY ON THE COMMON MICROBIAL ISOLATES AND SENSITIVITY PATTERN ON BLOOD CULTURE OF PEDIATRIC CANCER PATIENTS ADMITTED AT THE PHILIPPINE GENERAL HOSPITAL FOR FEBRILE NEUTROPENIA
Dr Babak Tamizi far MD. Assistant Professor Of Internal Medicine Al-Zahra Hospital Isfahan University Of Medical Sciences
 Dr Babak Tamizi far MD. Assistant Professor Of Internal Medicine Al-Zahra Hospital Isfahan University Of Medical Sciences ١ ٢ ٣ A 57-year-old man presents with new-onset fever, shortness of breath, lower
Dr Babak Tamizi far MD. Assistant Professor Of Internal Medicine Al-Zahra Hospital Isfahan University Of Medical Sciences ١ ٢ ٣ A 57-year-old man presents with new-onset fever, shortness of breath, lower
Alberta Health Public Health Notifiable Disease Management Guidelines January 2013
 January 2013 Rickettsial Infections Revision Dates Case Definition Reporting Requirements Remainder of the Guideline (i.e., Etiology to References sections inclusive) January 2013 January 2013 December
January 2013 Rickettsial Infections Revision Dates Case Definition Reporting Requirements Remainder of the Guideline (i.e., Etiology to References sections inclusive) January 2013 January 2013 December
UPDATE ON FEBRILE NEUTROPENIA
 UPDATE ON FEBRILE NEUTROPENIA Clinical approach and management Dr.Shafiq A. Alimad Head of medical department at university of science and technology hospital YICID 15-December-2014 INTRODUCTION Cancer
UPDATE ON FEBRILE NEUTROPENIA Clinical approach and management Dr.Shafiq A. Alimad Head of medical department at university of science and technology hospital YICID 15-December-2014 INTRODUCTION Cancer
Urinary Tract Infections in Hospitalized Patients
 Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Endocarditis, including Prophylaxis
 Endocarditis, including Prophylaxis ACOI Board Review 2018 gerald.blackburn@beaumont.org (No Disclosures) Infective Endocarditis Persistant bacteremia (blood cultures drawn >12 hrs apart) w/ organisms
Endocarditis, including Prophylaxis ACOI Board Review 2018 gerald.blackburn@beaumont.org (No Disclosures) Infective Endocarditis Persistant bacteremia (blood cultures drawn >12 hrs apart) w/ organisms
In the absence of underlying edema or other skin abnormalities, erysipelas
 ERYSIPELAS Erysipelas is a distinct type of superficial cutaneous cellulitis with marked dermal lymphatic vessel involvement caused by group A β-hemolytic streptococcus (very uncommonly group C or G streptococcus)
ERYSIPELAS Erysipelas is a distinct type of superficial cutaneous cellulitis with marked dermal lymphatic vessel involvement caused by group A β-hemolytic streptococcus (very uncommonly group C or G streptococcus)
OSTEOMYELITIS. If it occurs in adults, then the axial skeleton is the usual site.
 OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
-> Education -> Excellence
 Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Osteomieliti STEOMIE
 OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
IDSA GUIDELINES EXECUTIVE SUMMARY
 IDSA GUIDELINES Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America Alison G. Freifeld, 1 Eric
IDSA GUIDELINES Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America Alison G. Freifeld, 1 Eric
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
UTI IN ELDERLY. Zeinab Naderpour
 UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Clinical Information on West Nile Virus (WNV) Infection
 Infection") Clinical Information on West Nile Virus (WNV) Infection Introduction In 1999, West Nile Virus (WNV), an Old World flavivirus, producing a spectrum of disease including severe meningoencephalitis, appeared
Clinical Information on West Nile Virus (WNV) Infection Introduction In 1999, West Nile Virus (WNV), an Old World flavivirus, producing a spectrum of disease including severe meningoencephalitis, appeared
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Bacterial Infections of the Urinary System *
 OpenStax-CNX module: m64804 1 Bacterial Infections of the Urinary System * Douglas Risser This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 1 Learning
OpenStax-CNX module: m64804 1 Bacterial Infections of the Urinary System * Douglas Risser This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 1 Learning
Vancomycin: Class: Antibiotic.
 Vancomycin: Class: Antibiotic. Indications: Treatment of patients with infections caused by staphylococcal species and streptococcal Species. Available dosage form in the hospital: 1G VIAL, 500MG VIAL.
Vancomycin: Class: Antibiotic. Indications: Treatment of patients with infections caused by staphylococcal species and streptococcal Species. Available dosage form in the hospital: 1G VIAL, 500MG VIAL.
Life-threatening infections. Frank Bowden October 5, 2018
 Life-threatening infections Frank Bowden October 5, 2018 David Sackett Evidence Based Medicine is the integration of best research evidence with clinical expertise and patient values. The Golden Rules
Life-threatening infections Frank Bowden October 5, 2018 David Sackett Evidence Based Medicine is the integration of best research evidence with clinical expertise and patient values. The Golden Rules
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH)
") Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
The EM Educator Series
 The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
Infective Endocarditis for Primary Care Physicians
 Infective Endocarditis for Primary Care Physicians David N Gilbert, MD Disclosures Consultant to: Merck Pfizer Medicine Company Cempra 1 Introduction There are roughly 30,000 new cases of IE in the US
Infective Endocarditis for Primary Care Physicians David N Gilbert, MD Disclosures Consultant to: Merck Pfizer Medicine Company Cempra 1 Introduction There are roughly 30,000 new cases of IE in the US
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile in urinary bladder.. It contains fluids,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile in urinary bladder.. It contains fluids,
Infective Endocarditis
 Frank Lowy Infective Endocarditis 1. Introduction Infective endocarditis (IE) is an infection of the heart valves. A large number of different bacteria are capable of causing this disease. Depending on
Frank Lowy Infective Endocarditis 1. Introduction Infective endocarditis (IE) is an infection of the heart valves. A large number of different bacteria are capable of causing this disease. Depending on
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Moath Darweesh. Zaid Emad. Anas Abu -Humaidan
 3 Moath Darweesh Zaid Emad Anas Abu -Humaidan Introduction: First two lectures we talked about acute and chronic meningitis, which is considered an emergency situation. If you remember, CSF examination
3 Moath Darweesh Zaid Emad Anas Abu -Humaidan Introduction: First two lectures we talked about acute and chronic meningitis, which is considered an emergency situation. If you remember, CSF examination
Advanced Pediatric Emergency Medicine Assembly
 (+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
(+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
Daniel C. DeSimone, MD Assistant Professor of Medicine
 Daniel C. DeSimone, MD Assistant Professor of Medicine Faculty photo will be placed here Desimone.Daniel@mayo.edu 2015 MFMER 3543652-1 Infective Endocarditis Mayo School of Continuous Professional Development
Daniel C. DeSimone, MD Assistant Professor of Medicine Faculty photo will be placed here Desimone.Daniel@mayo.edu 2015 MFMER 3543652-1 Infective Endocarditis Mayo School of Continuous Professional Development
Appropriate Use of Antibiotics for the Treatment of Acute Upper Respiratory Tract Infections in Adults
 Appropriate Use of Antibiotics for the Treatment of Acute Upper Respiratory Tract Infections in Adults Kyong Ran Peck, M.D. Division of Infectious Diseases Sungkyunkwan University School of Medicine, Samsung
Appropriate Use of Antibiotics for the Treatment of Acute Upper Respiratory Tract Infections in Adults Kyong Ran Peck, M.D. Division of Infectious Diseases Sungkyunkwan University School of Medicine, Samsung
The Streptococci. Diverse collection of cocci. Gram-positive Chains or pairs significant pathogens
 The Streptococci Diverse collection of cocci. Gram-positive Chains or pairs significant pathogens Strong fermenters Facultative anaerobes Non-motile Catalase Negative 1 Classification 1 2 Classification
The Streptococci Diverse collection of cocci. Gram-positive Chains or pairs significant pathogens Strong fermenters Facultative anaerobes Non-motile Catalase Negative 1 Classification 1 2 Classification
CNS Infections in the Pediatric Age Group
 CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
Abscess. A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body.
 Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
GROUP A STREPTOCOCCUS (GAS) INVASIVE
 INVASIVE") GROUP A STREPTOCOCCUS (GAS) INVASIVE Case definition CONFIRMED CASE Laboratory confirmation of infection with or without clinical evidence of invasive disease: isolation of group A streptococcus (Streptococcus
GROUP A STREPTOCOCCUS (GAS) INVASIVE Case definition CONFIRMED CASE Laboratory confirmation of infection with or without clinical evidence of invasive disease: isolation of group A streptococcus (Streptococcus
Acute Cholangitis. Kelsey Knotts PharmD Candidate Class of 2016
 Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,.
 Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,. 12-10-2017 Group B streptococci are uniformly sensitive to penicillin
Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,. 12-10-2017 Group B streptococci are uniformly sensitive to penicillin
8/11/2015. Febrile neutropenia Bone marrow transplant Immunosuppressant medications
 Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
EMPIRICAL TREATMENT OF SELECT INFECTIONS ADULT GUIDELINES. Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection
 URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
Central Nervous System Infection
 Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report
 Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Infective endocarditis
 Infective endocarditis Today's lecture is about infective endocarditis, the Dr started the lecture by asking what are the most common causative agents of infective endocarditis? 1-Group A streptococci
Infective endocarditis Today's lecture is about infective endocarditis, the Dr started the lecture by asking what are the most common causative agents of infective endocarditis? 1-Group A streptococci
Infective Endocarditis عبد المهيمن أحمد
 Infective Endocarditis إعداد : عبد المهيمن أحمد أحمد علي Infective endocarditis Inflammation of the heart valve or endocardium of the heart. The agents are usually bacterial, but other organisms can also
Infective Endocarditis إعداد : عبد المهيمن أحمد أحمد علي Infective endocarditis Inflammation of the heart valve or endocardium of the heart. The agents are usually bacterial, but other organisms can also
DEFINITION Cellulitis is an acute, spreading inflammation of the dermis and subcutaneous tissue, often complicating a wound or other skin condition.
 DEFINITION Cellulitis is an acute, spreading inflammation of the dermis and subcutaneous tissue, often complicating a wound or other skin condition. Cellulitis may be further classified by the unique area
DEFINITION Cellulitis is an acute, spreading inflammation of the dermis and subcutaneous tissue, often complicating a wound or other skin condition. Cellulitis may be further classified by the unique area
Aurora Health Care South Region EMS st Quarter CE Packet
 Name: Dept: Date: Aurora Health Care South Region EMS 2010 1 st Quarter CE Packet Meningitis Meningitis is an inflammatory disease of the leptomeninges. Leptomeninges refer to the pia matter and the arachnoid
Name: Dept: Date: Aurora Health Care South Region EMS 2010 1 st Quarter CE Packet Meningitis Meningitis is an inflammatory disease of the leptomeninges. Leptomeninges refer to the pia matter and the arachnoid
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Choc septique. Frédéric Pène
 Choc septique Frédéric Pène Réanimation Médicale, Hôpital Cochin, AP-HP Université Paris Descartes Institut Cochin, Inserm U1016, CNRS UMR-8104, Département 3i No conflict of interest A 54 y.o. male patient
Choc septique Frédéric Pène Réanimation Médicale, Hôpital Cochin, AP-HP Université Paris Descartes Institut Cochin, Inserm U1016, CNRS UMR-8104, Département 3i No conflict of interest A 54 y.o. male patient
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
Fungal Meningitis. Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse Bern
 Fungal Meningitis Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse 51 3010 Bern Death due to infectious diseases in sub-saharan Africa Park BJ. Et al AIDS 2009;23:525
Fungal Meningitis Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse 51 3010 Bern Death due to infectious diseases in sub-saharan Africa Park BJ. Et al AIDS 2009;23:525
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
Dr. Arghya Samanta PG-3 Department of Pediatrics
 Dr. Arghya Samanta PG-3 Department of Pediatrics A 3 year old male K/C/O B-cell Acute lymphoblastic leukemia Undergoing induction phase of chemotherapy On day 23 of induction Presented with - high grade
Dr. Arghya Samanta PG-3 Department of Pediatrics A 3 year old male K/C/O B-cell Acute lymphoblastic leukemia Undergoing induction phase of chemotherapy On day 23 of induction Presented with - high grade
Skin & Soft Tissue Infections: Classic Case Presentations
 Skin & Soft Tissue Infections: Classic Case Presentations Mark Beilke, M.D. Professor of Medicine Chief of Infectious Diseases Clement J. Zablocki VA Medical Center Objectives Diagnose and treat water
Skin & Soft Tissue Infections: Classic Case Presentations Mark Beilke, M.D. Professor of Medicine Chief of Infectious Diseases Clement J. Zablocki VA Medical Center Objectives Diagnose and treat water
URINARY TRACT INFECTIONS
 URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
 MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Health Protection Scotland (HPS) SSI Surveillance Protocol 7th Edition
 Health Protection Scotland (HPS) SSI Surveillance Protocol 7th Edition") 1 Contents Female reproductive system operations (Abdominal hysterectomy and Caesarean section)... 3 Intra-abdominal infections... 3 Endometritis... 4 Other infections of the female reproductive tract...
1 Contents Female reproductive system operations (Abdominal hysterectomy and Caesarean section)... 3 Intra-abdominal infections... 3 Endometritis... 4 Other infections of the female reproductive tract...
Infections in Non-HIV Immunocompromised Hosts
 Infections in Non-HIV Immunocompromised Hosts Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Infections in Non-HIV Immunocompromised Hosts Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal catastrophes in ICU, 1017 1044. See also specific types, e.g., Abdominal compartment syndrome treatment of, 1032 1037 antimicrobial,
Index Note: Page numbers of article titles are in boldface type. A Abdominal catastrophes in ICU, 1017 1044. See also specific types, e.g., Abdominal compartment syndrome treatment of, 1032 1037 antimicrobial,
Aciphin Ceftriaxone Sodium
 Aciphin Ceftriaxone Sodium Only for the use of Medical Professionals Description Aciphin is a bactericidal, long-acting, broad spectrum, parenteral cephalosporin preparation, active against a wide range
Aciphin Ceftriaxone Sodium Only for the use of Medical Professionals Description Aciphin is a bactericidal, long-acting, broad spectrum, parenteral cephalosporin preparation, active against a wide range
Blood culture 壢新醫院 病理檢驗科 陳啟清技術主任
 Blood culture 壢新醫院 病理檢驗科 陳啟清技術主任 A Positive Blood Culture Clinically Important Organism Failure of host defenses to contain an infection at its primary focus Failure of the physician to effectively eradicate,
Blood culture 壢新醫院 病理檢驗科 陳啟清技術主任 A Positive Blood Culture Clinically Important Organism Failure of host defenses to contain an infection at its primary focus Failure of the physician to effectively eradicate,
West Nile Virus. Syndrome. (Family: Flaviviridae) Severe Manifestations (Typically >50 years of age) NEUROLOGICAL (Meningoencephalitis >Meningitis)
 Severe Manifestations (Typically >50 years of age) NEUROLOGICAL (Meningoencephalitis >Meningitis)") Severe Manifestations (Typically >50 years of age) Syndrome NEUROLOGICAL (Meningoencephalitis >Meningitis) CSF WBC Protein Glucose-WNL Confusion Change in Sensorium Stupor Seizures Ataxia Cranial Nerve
Severe Manifestations (Typically >50 years of age) Syndrome NEUROLOGICAL (Meningoencephalitis >Meningitis) CSF WBC Protein Glucose-WNL Confusion Change in Sensorium Stupor Seizures Ataxia Cranial Nerve
Urinary Tract Infections: From Simple to Complex. Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014
 Urinary Tract Infections: From Simple to Complex Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014 Learning Objectives Develop empiric antimicrobial treatment
Urinary Tract Infections: From Simple to Complex Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014 Learning Objectives Develop empiric antimicrobial treatment
Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center
 CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
Annex 4. Case definitions of infections
 Protocol for validation of PPS of HAIs and antimicrobial use in European LTCF TECHNICAL DOCUMENT Annex 4. Case definitions of infections Healthcare-associated infections and antimicrobial use in European
Protocol for validation of PPS of HAIs and antimicrobial use in European LTCF TECHNICAL DOCUMENT Annex 4. Case definitions of infections Healthcare-associated infections and antimicrobial use in European
CNS INFECTIONS 1 Acute meningitis
 Definition CNS INFECTIONS 1 Acute meningitis DR. BADRI PAUDEL Bacterial meningitis is a medical emergency. Meningitis is an acute infection within the subarachnoid space. usually secondary bacteremia or
Definition CNS INFECTIONS 1 Acute meningitis DR. BADRI PAUDEL Bacterial meningitis is a medical emergency. Meningitis is an acute infection within the subarachnoid space. usually secondary bacteremia or
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection
 Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Human Herpes Virus-6 Limbic Encephalitis
 Case Studies [1] March 19, 2013 Case history: A 32-year-old Caucasian female with newly diagnosed acute myeloid leukemia (AML) was treated with induction chemotherapy and attained complete remission. She
Case Studies [1] March 19, 2013 Case history: A 32-year-old Caucasian female with newly diagnosed acute myeloid leukemia (AML) was treated with induction chemotherapy and attained complete remission. She
Heart on Fire: Infective Endocarditis. Objectives. Disclosure 8/27/2018. Mary McGreal DNP, RN, ANP-c, CCRN
 Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN
 MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
Objectives. Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection
 that drive empiric antimicrobial selection") Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
GOALS AND OBJECTIVES INFECTIOUS DISEASE
 GOALS AND OBJECTIVES INFECTIOUS DISEASE Infectious Disease and HIV Overview: The Infectious Diseases Program at the University of Southern California prepares trainees for the management of problems in
GOALS AND OBJECTIVES INFECTIOUS DISEASE Infectious Disease and HIV Overview: The Infectious Diseases Program at the University of Southern California prepares trainees for the management of problems in
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys.
 UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections.
 In the name of God Principles of post Tx infections 1: Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections. Infection processes can progress
In the name of God Principles of post Tx infections 1: Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections. Infection processes can progress
Diagnosis and Management of UTI s in Care Home Settings. To Dip or Not to Dip?
 Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does