Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
|
|
|
- Jonathan West
- 5 years ago
- Views:
Transcription


 < 36 C (96.")


")







 Gram stain Culture")

 work-up indicated Start")



 1 HSV DNA PCR of")
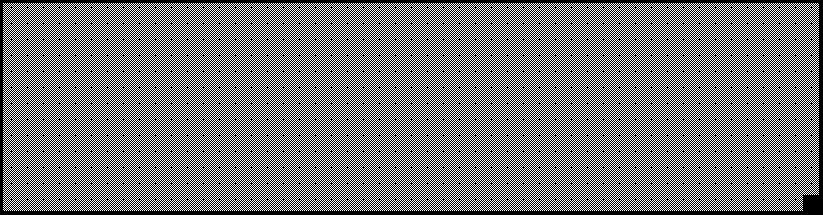
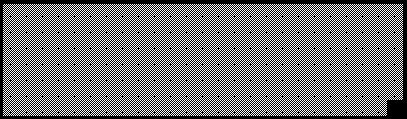
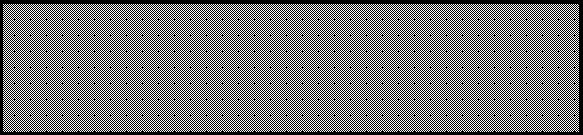
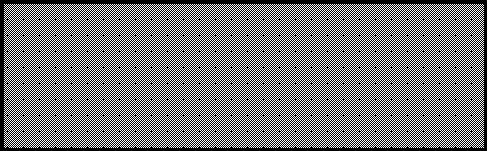
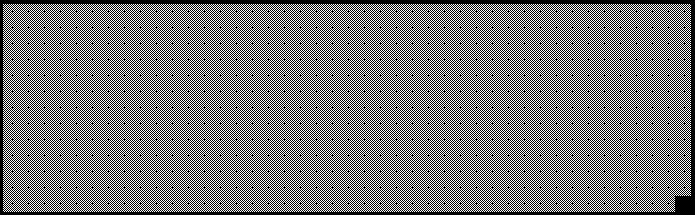
1 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured in Emergency Department reported measurement at home.! ALERT Patient Toxic/Septic Appearance Full Sepsis Workup & treat as appropriate. (LINK TO SEPSIS PATHWAY/GUIDELINE) Consider HSV work up and empiric ED treatment for patients with any of the following conditions: Historical and Clinical Features Severe illness / Hypothermia / Lethargy Seizures Hepatosplenomegaly Postnatal HSV contact Vesicular rash Conjunctivitis Interstitial pneumonitis Laboratory Findings Thrombocytopenia CSF pleocytosis without clear bacterial infection Transaminitis Focal infection Complete Blood Count with differential Blood Culture Complete Metabolic Panel Urinalysis with Micro Urine Culture: Catheter or Suprapubic Cerebrospinal Fluid (Hold Tube # 4) Gram stain Culture Cell count with differential Glucose Protein Stool culture & Stool WBC(If patient has diarrhea) Herpes Simplex Virus (HSV) work-up indicated Start empiric antibiotic treatment: Ampicillin x1 + Gentamicin x1 Manage OFF-PATHWAY Contraindications for Ceftriaxone in patients < 28 days of age: Patient expected to or receiving calcium containing IV products. Total Bilirubin > 10 (See risk factors for hyperbilirubinemia) 1 HSV DNA PCR of Blood Meningitis/Encephalitis PCR Panel of CSF Swab/scraping of skin or mucous membrane lesions for HSV DFA AND HSV culture Surface HSV cultures in viral transport media tube Conjunctiva Throat Nasopharynx Rectum Skin vesicle (if present) ADD antiviral treatment: Acyclovir Normal CSF Values 0-20 WBC/mm 3 Protein 0-30 days: < 100 mg/dl Normal Gram Stain ADMIT to Inpatient Management Pathway Patient Age: 0-7 Days 1 Confirm meningitic dose of Ampicillin (Redose if needed) 2 Add Cefotaxime (Use Cefepime if supply unavailable) 3 Consider HSV testing and Acyclovir therapy Patient Age: 8-28 Days 1 Confirm meningitic dose of Ampicillin (Redose if needed) 2 Add Ceftriaxone Confirm meningitic dosing (Use Cefepime if contraindicated ❶) 3 Consider HSV workup and Acyclovir therapy









 < 36 C (96.")




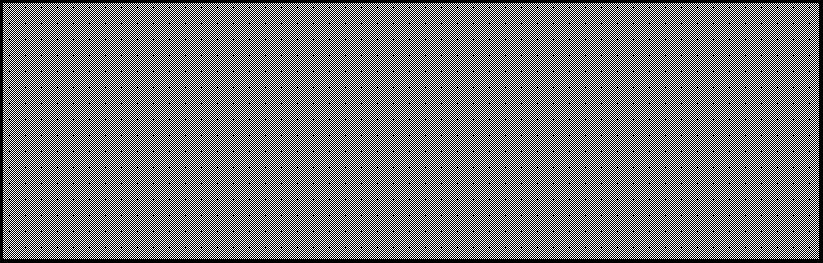
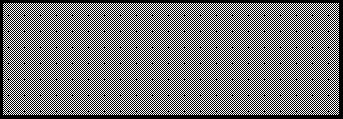
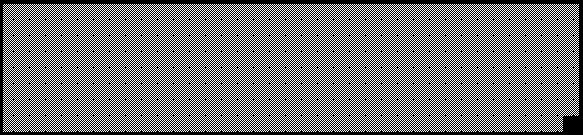
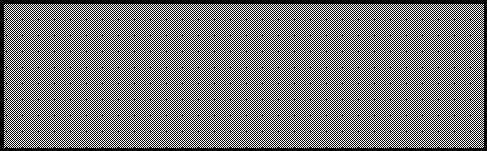
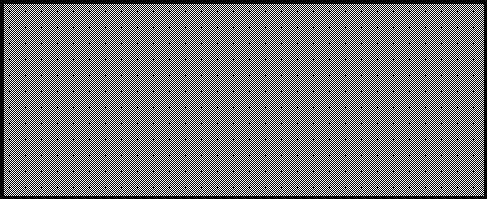
2 Age: Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age Low Risk Criteria for Serious Bacterial Infection Historical and Clinical Features days Full-term ( 37 weeks gestation) No prolonged NICU stay No chronic medical problems No systemic antibiotics within 72 hours Well-appearing and easily consolable No focal infections on exam Fecal Leucocytes Stool WBC 5 hpf Blood WBC 5,000 AND 15,000 Immature WBC/neutrophil Ratio < 0.2 Absolute Band Count < 1500/mm 3 Standard UA: WBC < 5/HPF Negative LE, Nitrite, Bacteria Chest X-ray (if obtained) No infiltrate Normal CSF Values 0-20 WBC/mm 3 Protein 0-30 days: < 100 mg/dl Normal Gram Stain DISCHARGE Home Follow-up in 24 hours No Antibiotics OPTION 1 ADMIT for Observation Manage OFF-PATHWAY Focal bacterial infection Complete Blood Count with differential Blood Culture Basic metabolic panel Urinalysis with Micro Urine Culture: Catheter or Suprapubic Stool culture & Stool WBC(If patient has diarrhea) INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured in Emergency Department reported measurement at home. OPTION 2 OPTION 3 Meets Low Risk Criteria CSF Collected Empiric antibiotic treatment: Ceftriaxone DISCHARGE Home Follow-up in 24 hours Patient family & PCP must be in agreement! ALERT Patient Toxic/Septic Appearance Full Sepsis Workup & treat as appropriate. (LINK TO SEPSIS PATHWAY/GUIDELINE) Order Lumbar Puncture: Cerebrospinal Fluid (Hold Tube # 4) Gram stain Culture Cell count with differential Glucose Protein Empiric antibiotic treatment: Ceftriaxone + Vancomycin ADMIT to Inpatient Manage OFF-PATHWAY






 measured in")













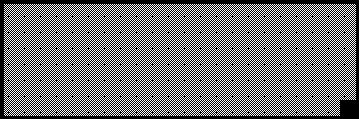

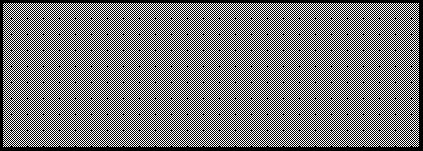
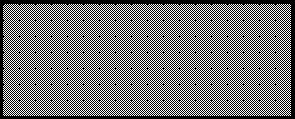
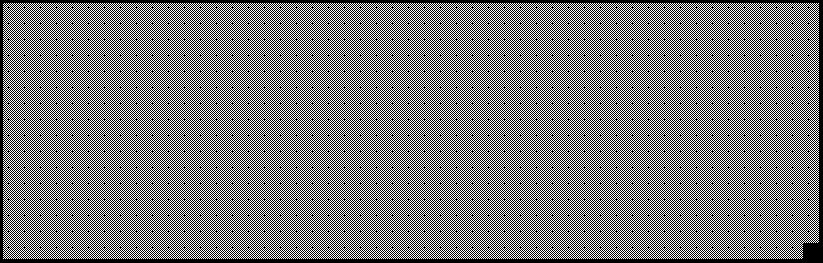
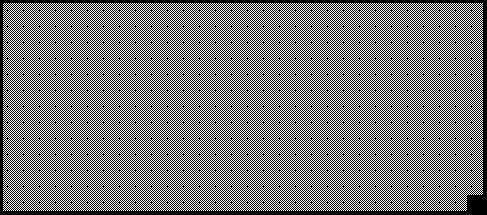
3 Age: 2-6 Months Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 39 C (102.2 F) < 36 C (96.5 F) measured in Emergency Department reported measurement at home.! ALERT Patient Toxic/Septic Appearance Full Sepsis Workup & treat as appropriate. (LINK TO SEPSIS PATHWAY/GUIDELINE) Treat with Supportive Care Defined Focal Bacterial Infection: Cellulitis, abscess, pneumonia, osteomyelitis, bacterial arthritis, omphalitis, meningitis Defined Viral Syndrome Croup Bronchiolitis Stomatitis Influenza Varicella Manage OFF-Pathway Consider Alternate Management Pathway Community Acquired Pneumonia Urinary Tract Infection Acute Osteomyelitis Prolonged fever >5 days: Consider Kawasaki Disease Patient received 2 or more doses of Pneumococcal Conjugate Vaccine (PCV) Continue UTI Assessment Complete Blood Count with differential WBC > 15,000/mm 3 < 5,000/mm 3 Influenza/ Bronchiolitis Meets Low Risk UTI Criteria? Order Blood Culture Urinalysis with Micro Urine Culture: Catheter or Suprapubic After UTI Assessment is Complete Empiric antibiotic treatment: Ceftriaxone UTI Management Guideline Urinalysis positive ED Discharge Criteria Tolerating liquids Reliable PCP or ED follow-up PCP and Caregiver comfortable with discharge Good social support Education complete ADMIT to Inpatient Management Pathway DISCHARGE Home Follow-up in 24 hours


 < 36 C measured in Emergency")



 ADD antiviral treatment:")



 ADD antiviral")


 Monitor")





 1 Inpatient")
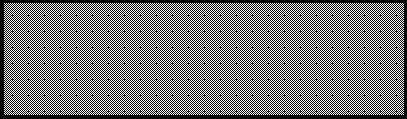
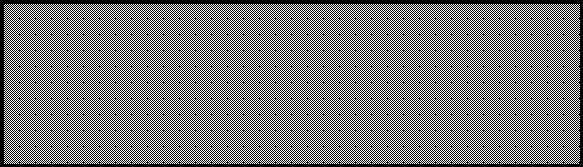
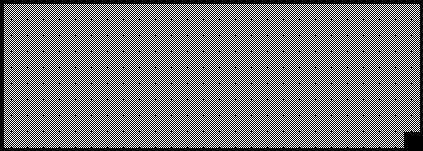
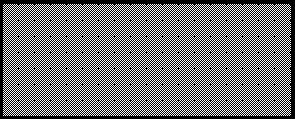
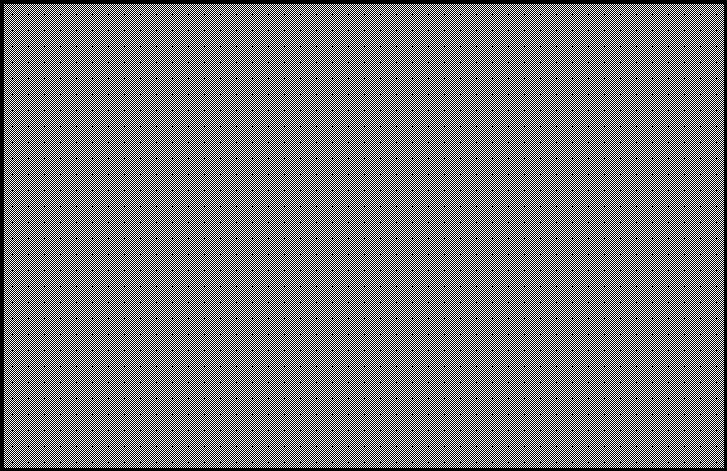
4 EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age Fever Without Source 0-89 Days of Age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C measured in Emergency Department reported measurement at home. Normal CSF Values 0-20 WBC/mm 3 Protein 0-30 days: < 100 mg/dl Normal Gram Stain 0 7 Days of Age 8 28 Days of Age Days of Age High Risk for Serious Bacterial Infection 1 Meningitic dose of Ampicillin 2 Cefotaxime (Use Cefepime if unavailable) ADD antiviral treatment: Acyclovir (If clinical suspicion of HSV) Continue antibiotic treatment: Ampicillin + Gentamicin Contraindication for Ceftriaxone? ❶ 1 Meningitic dose of Ampicillin 2 Add Ceftriaxone 1 Meningitic dose of Ampicillin 2 Cefotaxime (Use Cefepime if supply unavailable) ADD antiviral treatment: Acyclovir (If clinical suspicion of HSV) Continue antibiotic treatment: Ceftriaxone Observation 36 hours (Longer if ill-appearing) ADD antiviral treatment: Acyclovir (If clinical suspicion of HSV) Monitor Cultures: Blood Urine CSF GPC on CSF gram stain 1 Add Vancomycin 2 Continue Ceftriaxone/Cefotaxime 3 Continue Ampicillin Observation: hours (Longer if ill-appearing) Monitor Cultures: Blood Urine CSF 1 Add Vancomycin 2 Continue Ceftriaxone Risk factors for hyperbilirubinemia ABO incompatibility HDN Lethargy Temperature instability Sepsis Acidosis Albumin < 3g/dL Dehydration Weight loss Poor feeding Irritability Jaundice Contraindications for Ceftriaxone in patients < 28 days of age: Patient expected to or receiving calcium containing IV products. Total Bilirubin > 10 (See risk factors for hyperbilirubinemia) 1 Inpatient Discharge Criteria Blood, urine, CSF, & HSV evaluation negative Clinically stable based on provider assessment Reliable PCP Follow-up Education complete Manage OFF-PATHWAY DISCHARGE Home Follow-up in 24 hours







 Recommend screening for any")
5 Risk Factors for UTI and Screening Recommendations Probability of UTI > 1%: 2 or more risk factors Female Risk Factors* Non-black T 39 C Fever 2 days No apparent source of fever Age < 12 months *Recommend screening if prior history of UTI, fever 2 days > 2 months Not Toilet Trained Probability of UTI > 1%: Uncircumcised Circumcised with 3 or more Risk Factors Male Risk Factors* Non-black T 39 C Fever 2 days No apparent source of fever Age < 6 months Toilet Trained 18 years All Patients Symptoms referable to urinary tract Prior history of UTI, fever 2 days Prolonged fever ( 5 days) Recommend screening for any of the above factors
 No prolonged NICU stay No chronic medical problems No systemic antibiotics within 72 hours Well-appearing and")

6 Serious Bacterial Infection Low Risk Criteria for Serious Bacterial Infection Historical and Clinical Features days Full-term ( 37 weeks gestation) No prolonged NICU stay No chronic medical problems No systemic antibiotics within 72 hours Well-appearing and easily consolable No focal infections on exam Fecal Leucocytes Stool WBC 5 hpf Blood WBC 5,000 AND 15,000 Immature WBC/neutrophil Ratio < 0.2 Absolute Band Count < 1500/mm 3 Standard UA: WBC < 5/HPF Negative LE, Nitrite, Bacteria Chest X-ray (if obtained) No infiltrate



7 Herpes Simplex Virus Patiens with any of the following conditions should be considered for a Herpes Simplex Virus work up and empiric treatment: Historical and Clinical Features Severe illness / Hypothermia / Lethargy Seizures Hepatosplenomegaly Postnatal HSV contact Vesicular rash Conjunctivitis Interstitial pneumonitis Laboratory Findings Thrombocytopenia CSF pleocytosis without clear bacterial infection Transaminitis Herpes Simplex Virus Workup Consists of the following labs: HSV DNA PCR of Blood Meningitis/Encephalitis PCR Panel of CSF Swab/scraping of skin or mucous membrane lesions for HSV DFA AND HSV culture Surface HSV cultures in viral transport media tube Conjunctiva Throat Nasopharynx Rectum Skin vesicle (if present)

8 UTI Definition and Urinalysis DCMC Positive Urinalysis (UA) Definition: The presence of Leukocyte Esterase Nitrites microscopic analysis results positive for leukocytes or bacteria is suggestive of an active UTI. When more than one of these findings is present at the same time, the sensitivity and specificity increase significantly. Dell Children s and Seton Family of Hospitals does not currently perform an enhanced urinalysis on urine specimens routinely. The following criteria are guide in diagnosing a UTI in young children using the standard method of collection and processing. Diagnostic Interpretation Nitrites Poor sensitivity: Conversion of nitrates to nitrites by bacteria takes approximately 4 hours and not all bacteria reduce nitrate levels combined with frequency of infants voiding. Helpful when positive. Few false positives and high specificity. Leukocyte Esterase Positive leukocyte esterase is suggestive of a UTI. However, children may have WBC present in their urine in conditions other than a UTI (e.g. Kawasaki Disease) White Blood Cells Positive if: (WBC) - Pyuria 5 WBC per HBF via standard method Pyuria is absent in approximately 10% of children with a UTI Bacteriuria Presence of bacteriuria alone in the absence of other findings does not define a UTI. Culture Method Definite* Indeterminant Contaminant Suprapubic Any growth Growth of non-pathogens, Mixed culture Catheter 50,000 CFU/ML 10,000 CFU/ML Growth of non-pathogens, Mixed culture, < 10,000 CFU/ml * If also with presence of pyuria or bacteriuria Consider obtaining repeat specimen Mixed Culture = uropathogen + non-pathogen or two uropathogens Bag UA specimens should never be sent for urine culture. Only catheter or suprapubic methods are appropriate for culture collection in this age. Uropathogens Gram Negative Escherichia coli (~80%) Klebsiella Proteus Enterobacter Citrobacter Gram Positive Staphylococcus saprophyticus Enterococcus Staphylococcus aureus Non-pathogens Lactobacillus Coagulase-negative Staph Corynebacterium



9 Antimicrobial and Antiviral Dose Recommendations Drug a,b,c,d Dose Duration e N-MENINGITIC 7 days of age: 50 mg/kg/dose IV q8h 5 doses Ampicillin N-MENINGITIC > 7days of age: 50 mg/kg/dose IV q6h 6 doses MENINGITIC 7 days of age: 100 mg/kg/dose IV q8h 5 doses MENINGITIC > 7days of age: 100 mg/kg/dose IV q6h 6 doses Cefepime 50 mg/kg/dose IV q8h 5 doses Cefotaxime 7 days of age: 50 mg/kg/dose q8h 5 doses > 7days of age: 50 mg/kg/dose q6h 6 doses Ceftriaxone d If to be admitted: 50 mg/kg/dose IV q12h 3 doses If to be discharged: mg/kg/dose IV (ED ONLY) 1 dose Gentamicin b 4 mg/kg/dose IV q24h 2 doses Vancomycin c 7 days of age: 20 mg/kg/dose IV q8h > 7days of age: 20 mg/kg/dose IV q6h Recommended Dose for UTI a Dosing in this table is for patients with normal renal function. Please contact pharmacy for assistance with dosing in renal insufficiency. b For gentamicin, serum drug levels are not necessary unless treatment is anticipated or continued for more than 2 doses, SCr is increased more than 0.3 mg/dl from normal value for age, or UOP less than 1 ml/kg/hr. c For vancomycin, serum drug levels are not necessary unless treatment is anticipated or continued for more than 2 doses, SCr is increased more than 0.3 mg/dl from normal value for age, or UOP less than 1 ml/kg/hr. d Ceftriaxone is contraindicated with calcium containing IV products or hyperbilirubinemia. Meningitic dosing of ceftriaxone is mg/kg/day divided every hours but CSF concentrations are optimal when dosed at 50mg/kg/dose IV q12h; once daily dosing should be reserved for patients to be discharged from the ED. e If cultures become positive at any time, treat specific condition, narrow agent and lengthen antibiotic duration as appropriate. 5 doses 6 doses Drug Dose Duration Cefazolin 17 mg/kg/dose q8h 7 Days Recommended Dose for Antiviral Drug Dose Duration Acyclovir 20 mg/kg/dose IV q8h 5 doses until HSV surface cultures AND PCR Blood & CSF negative Exceptions: Seizures, Lethargy, or ongoing Fever
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys.
 UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
Urinary tract infection. Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine
 Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Nicolette Janzen, MD Texas Children's Hospital
 Which UTIs Need a VCUG? Applying AAP Guidelines Nicolette Janzen, MD Texas Children's Hospital Goals 1 2 3 4 5 Review the guidelines Present clinical scenarios Discuss VCUG and nuclear cystogram Discuss
Which UTIs Need a VCUG? Applying AAP Guidelines Nicolette Janzen, MD Texas Children's Hospital Goals 1 2 3 4 5 Review the guidelines Present clinical scenarios Discuss VCUG and nuclear cystogram Discuss
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
 1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Fever in Young Infants 7 90 days of age
 Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
4/11/2017 COMMUNITY ACQUIRED PNEUMONIA. Disclaimer. A Review of How to Treat Common Infections in a Pediatric Patient. Objectives for Technicians
 Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Paediatrica Indonesiana. Urine dipstick test for diagnosing urinary tract infection
 Paediatrica Indonesiana VOLUME 53 November NUMBER 6 Original Article Urine dipstick test for diagnosing urinary tract infection Syarifah Julinawati, Oke Rina, Rosmayanti, Rafita Ramayati, Rusdidjas Abstract
Paediatrica Indonesiana VOLUME 53 November NUMBER 6 Original Article Urine dipstick test for diagnosing urinary tract infection Syarifah Julinawati, Oke Rina, Rosmayanti, Rafita Ramayati, Rusdidjas Abstract
Fever in Infants: Pediatric Dilemmas in Antibiotherapy
 Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Pediatric urinary tract infection. Dr. Nariman Fahmi Pediatrics/2013
 Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
The Child with HIV and a Fever 1
 The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase
 By Dr. Lindokuhle Mahlase") UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase Epidemiology By age 7 years, 8 % of girls and 2 % of boys will have had a UTI. Most infections occur in the first 2 years of life ; boys
UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase Epidemiology By age 7 years, 8 % of girls and 2 % of boys will have had a UTI. Most infections occur in the first 2 years of life ; boys
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018
 When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018 UTIs in Patients >/ 65 yo - Most common infectious illness [1]. - Urinary tract
When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018 UTIs in Patients >/ 65 yo - Most common infectious illness [1]. - Urinary tract
4/11/2017. A Review of How to Treat Common Infections in a Pediatric Patient. Disclaimer. Objectives for Pharmacists
 A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
URINARY TRACT INFECTIONS
 URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
Evaluating Fever in Infants. Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist
 Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
NEONATAL SEPSIS. Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI-RSCM
 NEONATAL SEPSIS Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI- Background Neonatal sepsis : Early-onset Late-onset Early-onset : mostly premature neonates Within 24 hours 85% 24-48 hours
NEONATAL SEPSIS Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI- Background Neonatal sepsis : Early-onset Late-onset Early-onset : mostly premature neonates Within 24 hours 85% 24-48 hours
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra
 UTI Dr jayaprakash.k.p,asst prof,ich,govt.medical college,kottayam What is UTI? It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra What is prevalence of UTI?
UTI Dr jayaprakash.k.p,asst prof,ich,govt.medical college,kottayam What is UTI? It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra What is prevalence of UTI?
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
Dr. Bob Wilson Golden BC
 Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
EMPIRICAL TREATMENT OF SELECT INFECTIONS ADULT GUIDELINES. Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection
 URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
Bacterial Infections of the Urinary System *
 OpenStax-CNX module: m64804 1 Bacterial Infections of the Urinary System * Douglas Risser This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 1 Learning
OpenStax-CNX module: m64804 1 Bacterial Infections of the Urinary System * Douglas Risser This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 1 Learning
CHAPTER 167 Pediatric Fever
 CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
UTI Update: Have We Been Led Astray? Disclosure. Objectives
 UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Neonatal Sepsis. Neonatal sepsis ehandbook
 Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Key Definitions. Downloaded from
 Key Definitions In order to make sure that every member of the team is clear about the definitions that will be used, we have provided a list of key terms in the next few pages along with commonly used
Key Definitions In order to make sure that every member of the team is clear about the definitions that will be used, we have provided a list of key terms in the next few pages along with commonly used
Urinary Tract Infections
 Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Urinary Tract Infections in Hospitalized Patients
 Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
UTI IN ELDERLY. Zeinab Naderpour
 UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: Urinary tract infections (UTIs) are tied with pneumonia as the second most common type of healthcare-associated infection, second only
Catheter-Associated Urinary Tract Infection () Event Introduction: Urinary tract infections (UTIs) are tied with pneumonia as the second most common type of healthcare-associated infection, second only
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Surveillance report Published: 7 July 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Urinary tract infection in under 16s: diagnosis and management (2007) NICE guideline CG54 Surveillance report Published: 7 July 2016 nice.org.uk NICE 2016. All rights reserved.
Surveillance report 2016 Urinary tract infection in under 16s: diagnosis and management (2007) NICE guideline CG54 Surveillance report Published: 7 July 2016 nice.org.uk NICE 2016. All rights reserved.
Urine bench. John Ferguson Sept 2013
 Urine bench John Ferguson Sept 2013 Overview Specimen collection- separate presentation Urinalysis: protein, blood, white cells, nitrite Microscopy- crystals and casts- separate presentations quantitative
Urine bench John Ferguson Sept 2013 Overview Specimen collection- separate presentation Urinalysis: protein, blood, white cells, nitrite Microscopy- crystals and casts- separate presentations quantitative
Neonatal sepsis INCIDENCE RISK FACTORS RISK FACTORS 5/18/2015
 Angelica Floren MD.FAAP. Caring for Little Miracles 6 Th Annual Care Of the Sick Newborn Conference Neonatal sepsis Neonatal sepsis is a disease that may start with minimal or nonspecific symptoms and
Angelica Floren MD.FAAP. Caring for Little Miracles 6 Th Annual Care Of the Sick Newborn Conference Neonatal sepsis Neonatal sepsis is a disease that may start with minimal or nonspecific symptoms and
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Diagnosis and Management of UTI s in Care Home Settings. To Dip or Not to Dip?
 Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
Rational Evaluation of the Febrile Infant
 Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Your first patient of the day
 Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
How to interpret your urine sample results
 How to interpret your urine sample results Chronic UTI Info Factsheet Series Once you have submitted your urine sample for analysis, it will be sent off to the local laboratory or hospital laboratory if
How to interpret your urine sample results Chronic UTI Info Factsheet Series Once you have submitted your urine sample for analysis, it will be sent off to the local laboratory or hospital laboratory if
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile in urinary bladder.. It contains fluids,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile in urinary bladder.. It contains fluids,
How to interpret your urine sample results
 How to interpret your urine sample results Chronic UTI Info Factsheet Series Once you have submitted your urine sample for analysis, it will be sent off to the local laboratory or hospital laboratory if
How to interpret your urine sample results Chronic UTI Info Factsheet Series Once you have submitted your urine sample for analysis, it will be sent off to the local laboratory or hospital laboratory if
Children s Services Medical Guideline
 See also: NICE Guidelines These local guidelines are in conjunction with NICE UTI Algorithms Renal scarring and subsequent nephropathy are important causes of later hypertension and renal failure. Early
See also: NICE Guidelines These local guidelines are in conjunction with NICE UTI Algorithms Renal scarring and subsequent nephropathy are important causes of later hypertension and renal failure. Early
ENCEPHALITIS. Diana Montoya Melo
 ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
URINARY TRACT INFECTIONS IN LONG TERM CARE. Tuesday, 8 November, 11
 URINARY TRACT INFECTIONS IN LONG TERM CARE OBJECTIVES UNDERSTAND THE SCALE OF DISEASE IN LTC SETTINGS DEVELOP AN UNDERSTANDING OF THE DIFFERENT PRESENTATIONS OF UTIs IN THIS SETTING AND WORKUP BECOME AWARE
URINARY TRACT INFECTIONS IN LONG TERM CARE OBJECTIVES UNDERSTAND THE SCALE OF DISEASE IN LTC SETTINGS DEVELOP AN UNDERSTANDING OF THE DIFFERENT PRESENTATIONS OF UTIs IN THIS SETTING AND WORKUP BECOME AWARE
Guidelines for the management of urinary tract infections in children 0-17 years
 Guidelines for the management of urinary tract infections in children 0-17 years Guideline to be used where appropriate in conjunction with the Ashford and St Peter s sepsis guideline (Dr Ruth Mew 2016)
Guidelines for the management of urinary tract infections in children 0-17 years Guideline to be used where appropriate in conjunction with the Ashford and St Peter s sepsis guideline (Dr Ruth Mew 2016)
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
PEACEHEALTH LABORATORIES
 360-414-2306 www.peacehealthlabs.org Critical Values Call List - Longview Critical values are reported per the criteria published below. Laboratory results meeting these criteria indicate potential life-threatening
360-414-2306 www.peacehealthlabs.org Critical Values Call List - Longview Critical values are reported per the criteria published below. Laboratory results meeting these criteria indicate potential life-threatening
CATHETER-ASSOCIATED URINARY TRACT INFECTIONS
 CATHETER-ASSOCIATED URINARY TRACT INFECTIONS Hamid Emadi M.D Associate professor of Infectious diseases Department Tehran university of medical science The most common nosocomial infection The urinary
CATHETER-ASSOCIATED URINARY TRACT INFECTIONS Hamid Emadi M.D Associate professor of Infectious diseases Department Tehran university of medical science The most common nosocomial infection The urinary
Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days
 RESEARCH ARTICLE Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days AUTHORS Rianna C. Evans, MD, Bryan R. Fine, MD, MPH Division of Pediatric Hospital Medicine, Department of Pediatrics,
RESEARCH ARTICLE Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days AUTHORS Rianna C. Evans, MD, Bryan R. Fine, MD, MPH Division of Pediatric Hospital Medicine, Department of Pediatrics,
Lecture 1: Genito-urinary system. ISK
 Urinary Tract Infections Lecture 1: Genito-urinary system. ISK 07 08 2009. Getting Clear on the Terminology UTI Cystitis Urosepsis Asymptomatic Bacteriuria Asymptomatic UTI Pyuria Symptomatic UTI Pylonephritis
Urinary Tract Infections Lecture 1: Genito-urinary system. ISK 07 08 2009. Getting Clear on the Terminology UTI Cystitis Urosepsis Asymptomatic Bacteriuria Asymptomatic UTI Pyuria Symptomatic UTI Pylonephritis
FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N M A T E R. I E
 FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N L @ M A T E R. I E Level 4 teaching hospital based in Dublin s north inner city Over 600 in-patient
FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N L @ M A T E R. I E Level 4 teaching hospital based in Dublin s north inner city Over 600 in-patient
Emergency Neurological Life Support Meningitis and Encephalitis
 Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured
 9 million visits/year! Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured Interpretation of the culture result has been controversial-
9 million visits/year! Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured Interpretation of the culture result has been controversial-
Urinary tract infections, renal malformations and scarring
 Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE
 Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
35.0. ug/ml Trough. 8.0 Carbamazepine 15.0 ug/ml Digoxin 2.5 ng/ml Gentamicin Peak Random Trough
 The following are a list by department of Critical (Panic) Values: CHEMISTRY TEST LESS THAN GREATER THAN UNITS Glucose 0-7days 40 200 mg/dl Glucose > 7 days 50 400 mg/dl Glucose, CSF 25 mg/dl Sodium 121
The following are a list by department of Critical (Panic) Values: CHEMISTRY TEST LESS THAN GREATER THAN UNITS Glucose 0-7days 40 200 mg/dl Glucose > 7 days 50 400 mg/dl Glucose, CSF 25 mg/dl Sodium 121
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Urinary tract infection and hyperbilirubinemia
 The Turkish Journal of Pediatrics 2006; 48: 51-55 Original Urinary tract infection and hyperbilirubinemia Hülya Bilgen 1, Eren Özek 1, Tamer Ünver 1, Neşe Bıyıklı 2 Harika Alpay 2, Dilşat Cebeci 3 Divisions
The Turkish Journal of Pediatrics 2006; 48: 51-55 Original Urinary tract infection and hyperbilirubinemia Hülya Bilgen 1, Eren Özek 1, Tamer Ünver 1, Neşe Bıyıklı 2 Harika Alpay 2, Dilşat Cebeci 3 Divisions
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela
 Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
Mesporin TM. Ceftriaxone sodium. Rapid onset, sustained action, for a broad spectrum of infections
 Ceftriaxone sodium Rapid onset, sustained action, for a broad spectrum of infections 1, 2, 3 Antibiotic with a broad spectrum of activity Broad spectrum of activity against gram-positive* and gram-negative
Ceftriaxone sodium Rapid onset, sustained action, for a broad spectrum of infections 1, 2, 3 Antibiotic with a broad spectrum of activity Broad spectrum of activity against gram-positive* and gram-negative
Advanced Pediatric Emergency Medicine Assembly
 (+)Kathy Shaw, MD, FACEP Associate Chair and PSO, Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania; Nicolas Crognale Endowed Chair and Chief, Division of Enmergency Medicine,
(+)Kathy Shaw, MD, FACEP Associate Chair and PSO, Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania; Nicolas Crognale Endowed Chair and Chief, Division of Enmergency Medicine,
Urinary Tract Infections in Children
 Urinary Tract Infections in Children Eric Balighian, MD,* Michael Burke, MD* *St Agnes Hospital, Baltimore, MD Educational Gaps Consideration of risk factors for urinary tract infections (UTIs) in young
Urinary Tract Infections in Children Eric Balighian, MD,* Michael Burke, MD* *St Agnes Hospital, Baltimore, MD Educational Gaps Consideration of risk factors for urinary tract infections (UTIs) in young
11/15/2010. Asymptomatic Bacteriuria UTI. Symptomatic UTI. Asymptomatic UTI. Cystitis. Pylonephritis. Pyuria. Urosepsis
 Urinary Tract Infections Renal vein Inferior vena cava Urinary bladder Urethra Renal artery Kidney Aorta Ureter Lecture 1: Genito-urinary system. 06 08 2010. (a) Sherwood Fig. 12-6a, p.530 An introduction
Urinary Tract Infections Renal vein Inferior vena cava Urinary bladder Urethra Renal artery Kidney Aorta Ureter Lecture 1: Genito-urinary system. 06 08 2010. (a) Sherwood Fig. 12-6a, p.530 An introduction
Urinary tract infections Dr. Hala Al Daghistani
 Urinary tract infections Dr. Hala Al Daghistani UTIs are considered to be one of the most common bacterial infections. Diagnosis depends on the symptoms, urinalysis, and urine culture. UTIs occur more
Urinary tract infections Dr. Hala Al Daghistani UTIs are considered to be one of the most common bacterial infections. Diagnosis depends on the symptoms, urinalysis, and urine culture. UTIs occur more
Guillain-Barré Syndrome
 Guillain-Barré Syndrome A Laboratory Perspective Laura Dunn Biomedical Scientist (Trainee Healthcare Scientist) Diagnosis of GBS GBS is generally diagnosed on clinical grounds Basic laboratory studies
Guillain-Barré Syndrome A Laboratory Perspective Laura Dunn Biomedical Scientist (Trainee Healthcare Scientist) Diagnosis of GBS GBS is generally diagnosed on clinical grounds Basic laboratory studies
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 4/ Issue 66/ Aug 17, 2015 Page 11432
 BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
CNS INFECTIONS 1 Acute meningitis
 Definition CNS INFECTIONS 1 Acute meningitis DR. BADRI PAUDEL Bacterial meningitis is a medical emergency. Meningitis is an acute infection within the subarachnoid space. usually secondary bacteremia or
Definition CNS INFECTIONS 1 Acute meningitis DR. BADRI PAUDEL Bacterial meningitis is a medical emergency. Meningitis is an acute infection within the subarachnoid space. usually secondary bacteremia or
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
MICHIGAN MEDICINE GUIDELINES FOR TREATMENT OF URINARY TRACT INFECTIONS IN ADULTS
 When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age
 Proceeding S.Z.P.G.M.I. Vol: 25(2): pp. 61-65, 2011. Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age Lubna Riaz, Muhammad Aslam, Waqar Hussain, Anita
Proceeding S.Z.P.G.M.I. Vol: 25(2): pp. 61-65, 2011. Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age Lubna Riaz, Muhammad Aslam, Waqar Hussain, Anita
Pediatric Urinary Tract Infections
 Pediatric Urinary Tract Infections Sarmistha B. Hauger M.D. Pediatric Infectious Diseases Specially For Children Dell Children s Medical Center of Central Texas CME Conference 5/08 Pediatric UTI Epidemiology
Pediatric Urinary Tract Infections Sarmistha B. Hauger M.D. Pediatric Infectious Diseases Specially For Children Dell Children s Medical Center of Central Texas CME Conference 5/08 Pediatric UTI Epidemiology
UTI: A practical approach. Justin Seroy, DO Infectious Disease Attending BUMC-P
 UTI: A practical approach Justin Seroy, DO Infectious Disease Attending BUMC-P UTI Pathophysiology Uropathogens colonize urethra, vagina or perineal area -> Enter lower urinary tract ->bladder ->kidney
UTI: A practical approach Justin Seroy, DO Infectious Disease Attending BUMC-P UTI Pathophysiology Uropathogens colonize urethra, vagina or perineal area -> Enter lower urinary tract ->bladder ->kidney