Advanced Pediatric Emergency Medicine Assembly
|
|
|
- Alban McKenzie
- 6 years ago
- Views:
Transcription
1 (+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine Assembly March New York, NY Fever and Neutropenia Children with malignancy who are undergoing chemotherapy frequently develop neutropenia during therapy. When that child (or any child with neutropenia) develops fever in the face of neutropenia, there is concern that the child may have a life-threatening infection. Protocolized care in this population has been shown to streamline care and improve outcomes. This speaker will discuss multidisciplinary protocol development and outcomes from institutions where clinical care protocols are in place. OBJECTIVES Describe risk faced by a child with fever and neutropenia Recognize a child with fever and neutropenia including the warning signs of severe disease Discuss development and implementation of a protocol to mange this population of patients Outline outcome measures that can be monitored to ascertain if care is improving as a result of the guideline 3/24/2015 2:15 PM-2:45 PM Grand Ballroom TU-6 DISCLOSURES: (+) No significant financial relationships to disclose

2 Management of pediatric fever and neutropenia Joan E. Shook M.D., M.B.A. FACEP FAAP Professor of Pediatrics Baylor College of Medicine Chief Safety Officer Chief Clinical Information Officer Texas Children s Hospital I have no conflicts of interest to disclose
3 Plan for the session By the end of the session the participant should 1. Have an updated understanding of fever and neutropenia in children 2. Understand the utility an evidence based (EB) guideline in the management of a child with fever and neutropenia 3. Feel comfortable assessing his/her practice in light of a EB guideline Page 2 Page 2
4 Neutropenia in children Children with depressed immune function, including neutropenia, are at increased risk for serious bacterial, viral and fungal infections Children at risk for developing neutropenia include patients using chemotherapeutic agents or other medications that alter immune function Page 3 Phillips et al J Clin Oncol 2012 Page 3
5 Neutropenia in children Fever and neutropenia (FN) are common complications in children who receive chemotherapy for cancer Risk is enhanced by the presence of in-dwelling catheters Children with HIV, Crohn s, rheumatoid arthritis, lupus, and underlying immunodeficiency states either congenital or acquired may also have neutropenia Page 4 Phillips et al J Clin Oncol 2012 Page 4
6 Definitions: Fever and Neutropenia (FN) Fever Temperature > 38 o C for more than an hour or Single temperature >38.3 o C Neutropenia defined by absolute neutrophil count (ANC) Classic: ANC<1500/mm 3 Moderate neutropenia: ANC between /mm 3 Severe neutropenia: ANC<500/mm 3 Risk of infection increases as ANC decreases Page 5 Page 5
7 Unsuspected neutropenia in children Review of 1888 children 0-21y who presented with ANC<1000 with no known risk factors for SBI (central venous line or immunodeficiency) Evaluated for SBI using blood, urine and CSF 15/453 (3.3%) infants < 3mos had SBI 7 bacteremia 4 meningitis 8 UTI 18/1435 (0.01%) >3mos had SBI 1 bacteremia 14 UTI Page 6 Melendez E and M Harper AEM 2010 Page 6
8 Unsuspected neutropenia in children Review of 1888 children 0-21y who presented with ANC<1000 with no known risk factors for SBI (central venous line or immunodeficiency) Conclusion: children with incidental neutropenia are not at increased risk of SBI Page 7 Melendez E and M Harper AEM 2010 Page 7
9 Pediatric cancer patients in the ED Review of cohort of pediatric (<19y) patients with cancer presenting between Data source: Nationwide Emergency Department Sample database 294,289 visits identified Fever and fever neutropenia accounted for 20% of visits 44% of patients were admitted overall 88% FN patients were admitted Page 8 Page 8 Mueller, E et al Ped Blood Cancer2015
10 Pediatric cancer patients in the ED 294,289 PED visits Diagnosis % visits Adm% Transfer% Home% 1 Fever FN Bloodstream infection 4 URI Pneumonia Neutropenia Headache Seizure UTI Dehydration Page 9 Page 9 Mueller, E et al Ped Blood Cancer2015
11 Pediatric cancer patients in the ED Variations in practice noted Patients presenting to metropolitan teaching hospital had higher odds of admission and patients presenting to nonmetropolitan hospital had lower odds of admission than patients presenting to metropolitan non-teaching hospital Socioeconomic factors had significant impact on admission Lower odds of admission with self pay patients Higher odds of admission with zip codes with high SES Page 10 Page 10 Mueller, E et al Ped Blood Cancer2015
12 Etiology and clinical course of FN Review of 337 episodes of FN in children with cancer at St. Jude s Children s Research Hospital Infection proven (isolation of an organism from a sterile body site in a clinical setting consistent with an infection) in 86 (25%) 54 (63%) had bacterial infections 29(34%) had viral infections Infection probable (clinical or radiographic findings of infection where patient shows prompt response to antimicrobials) in 75 (22%) Fever of unknown origin in 177 (53%) Infection related mortality: 0.6% Page 11 Hakim, H et al J Ped Hemat Oncol 2009 Page 11
13 Etiology and clinical course of FN Bacteremia accounted for most of proven episodes (n=41) Most common organisms: Strep viridans (13), Pseudomonas (6), E. coli (6) Median time to positive BC 12 hours: 93% positive within 24 hours Viral etiologies more frequent than found in prior studies Better availability of viral diagnostics Fever of unknown origin in 177 (53%) characterized by Shorter median duration of fever Longer duration since last chemotherapy Less likely to have AML Page 12 Hakim, H et al J Ped Hemat Oncol 2009 Page 12
14 Guideline for Management of FN in Children with Cancer International Pediatric Fever and Neutropenia Guideline panel was convened to develop an evidence based (EB) algorithm for pediatric oncology patients Treatment algorithms for adults with cancer exist Consensus statements exist on risk stratification for adults on when to assess for risk of adverse events These algorithms cannot be applied to children Page 13 Lehrnbecher, T et al J Clin Onc 2012 Page 13
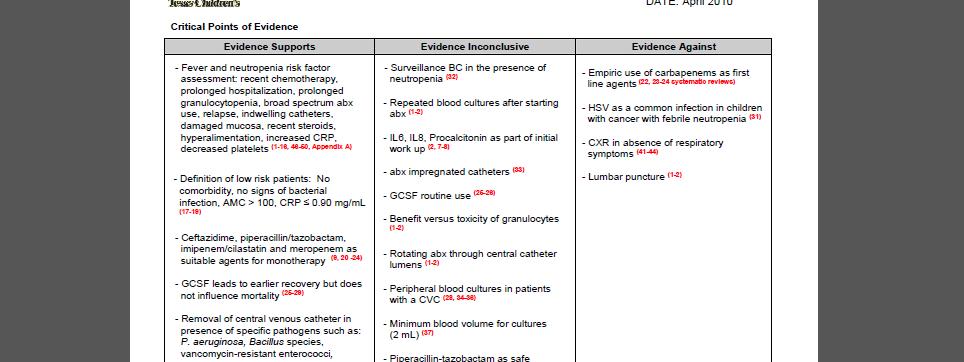
15 EB Guideline: clinical features History and physical examination Patient specific markers Age, Malignancy type Disease status Treatment specific factors Type and timing of chemotherapy Episode specific factors Height of the fever Blood counts, CRP Mucositis, hypotension Page 14 Page 14
16 EB Guideline: risk stratification Six low risk stratification schemas have been validated in different populations No single low risk prediction rule exists Choice of strategy is institution dependent Need to take into consideration the ability of the institution to implement complex rules, lab turnaround for required tests etc. Children with severe myelosuppression and those undergoing stem cell transplantation are always high risk Page 15 Page 15
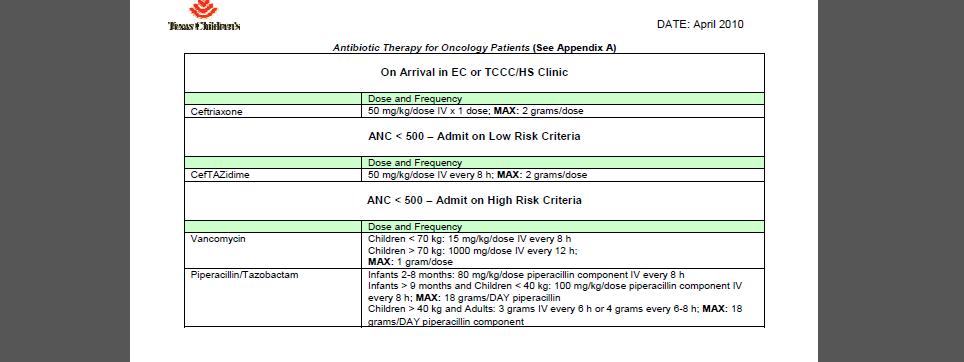
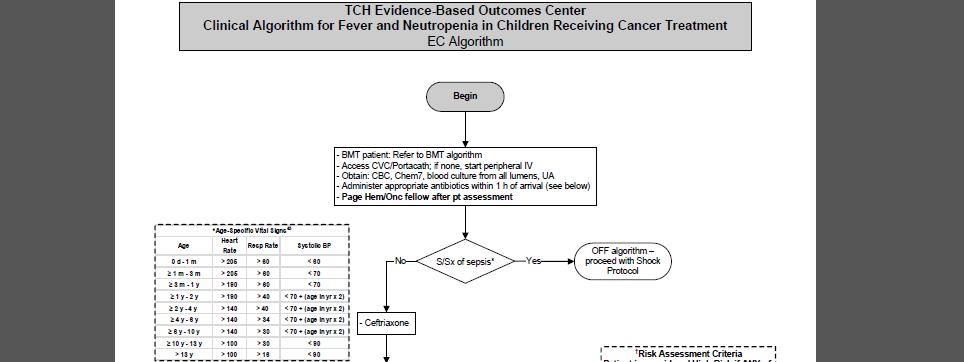
17 EB Guideline: lab & imaging studies Obtain blood cultures (BC) at the onset of FN from all lumens of central venous catheters Consider obtaining peripheral BC at the same time Consider urinalysis and urine culture in patients for whom a clean catch specimen can be obtained readily Obtain CXR only in symptomatic patients Page 16 Page 16
18 A word about blood cultures Several studies have evaluated the utility of peripheral blood cultures 13% of bacteremias are detected on the peripheral culture only Not known whether this is an artifact of culture volumes Peripheral blood cultures can be useful in identifying a CLABSI Not all centers encourage peripheral blood cultures Henry, M and L Sung Pedi Clin NA 2015 Page 17 Page 17
19 How about newer diagnostics? Comparisons have been done of polymerase chain reaction (PCR) targeting bacterial and fungal DNA and RNA with conventional blood cultures as well as supplementing conventional blood cultures with PCR-based and conventional viral diagnostics Proportion of fever and neutropenia episodes with microbiologically defined infection increases dramatically when advanced diagnostics are used Techniques lack standardization Need to understand the association of clinical findings to molecular detection results before recommending the use of these studies routinely Page 18 Page 18 Ammann, RA et al Curr Opin Infect Dis 2012
20 EB Guideline: antibiotic choice Monotherapy with antipseudomonal beta-lactam or carbapenem as empiric therapy in high risk FN Add a second gram-negative agent or glycopeptide for patients who are clinically unstable or resistant organisms are suspected Considerable site- and region-specific differences in the incidence resistant organisms exist Influence the initial choice of empiric antibiotics Page 19 Page 19
21 Inpatient vs Outpatient therapy Study of 37 children with FN who had no signs of septic shock (hypotension, tachycardia, delayed capillary refill or rigors) and no significant comorbidities requiring monitoring or treatment (focus of infection, pain, mucositis, vomiting, diarrhea or dehydration) All given cefipime 50mg/kg IV in ED ANC < 500 Half were discharged on IV cefipime while the other half were admitted Page 20 Orme, L et al Ped Blood Cancer 2014 Page 20
22 Role of outpatient management Outpatient management can be considered for low risk patients Has been shown to be feasible Intravenous and oral regimens have been studied Several advantages to outpatient management Enhanced quality of life Reduction in costs Reduced risk of nosocomial infection Page 21 Henry and Sung 2015 Page 21
23 Outpatient management low risk patients In order to implement this approach 1. Must be able to identify low risk population 2. Must have program in place to monitor the patient and expedite admission to the hospital if deterioration occurs 3. Social circumstances and travel considerations determine the feasibility of this approach in some patients 4. Optimal frequency of follow up has not been determined 5. Oral and intravenous antibiotic regimens have been used with equal efficacy 6. Consultation with oncology is essential Page 22 Henry and Sung 2015 Page 22
24 Risk stratification No adverse outcomes due to outpatient management Parent questionnaires showed higher QOL for outpatient care group More able to keep up with household tasks More able to spend time with other family members Page 23 Orme 2014 Page 23
25 EB Guideline: on-going therapy Patients who respond to initial empiric antibiotic therapy Discontinue double coverage in hours if there is no microbiologic indication to continue it Patients with persistent fever or who become clinically unstable, escalate the therapy Initiate empiric antifungal treatment if febrile > 96 hours after initiation of antimicrobial therapy Page 24 Page 24
26 ED Approach Standardization of processes improves care and allows you to evaluate outcomes Multidisciplinary evidence based algorithms provide shared baseline Electronic medical record facilitates the utilization of evidence based algorithms Page 25 Page 25
27 Page 26 Page 26
28 Page 27 Page 27
29 Page 28 Page 28
30 Page 29 Page 29
31 Page 30 Page 30
32 Page 31 Page 31
33 Page 32 Page 32

34 Page 33 Page 33
35 Page 34 Page 34
36 Measuring quality of care Time to antibiotic administration is a widely used measure of quality of care for children with cancer and FN Retrospective study of 1628 admissions that were reviewed for the presence of an adverse event (inhospital mortality, PICU admission, >40cc/kg within 24 hour) and length of stay Page 35 Fletcher et al Ped Blood Cancer 2013 Page 35
37 Measuring quality of care in FN 11.1% of admissions had an adverse event (AE) 0.7% mortality 4.7% PICU admission 10.1% fluid resuscitation in first 24 hours of hospitalization TTA administration minutes associated with AE when compared to <60 minutes Admission from the ED (as opposed to from clinic) associated with AE Page 36 Fletcher et al 2009 Page 36
38 Time to Antibiotics (TTA) TTA<60 minutes shown to decrease need for ICU care in FN cancer patients 45% hospitals in Children s Oncology Group track TTA Goal is <60 minutes Quality improvement methods are effective in improving TTA Page 37 Salstrom, JL et al Ped Blood Cancer 2015 Page 37
39 TTA Retrospective analysis of outcomes after achieving TTA<60 min Reduced need for PICU Reduced admissions Reduced total cost of care Page 38 Salstrom et al 2015 Page 38
40 Improving TTA Standardized process and order set were created for use on pediatric patients with fever and neutropenia 130 episodes of FN were analyzed After implementation of new process, time to ordering antibiotics was reduced by over half (72 minutes to 27 minutes) and time to administration also was reduced (154 minutes to 95 minutes) Page 39 Cash, T et al PEC 2014 Page 39

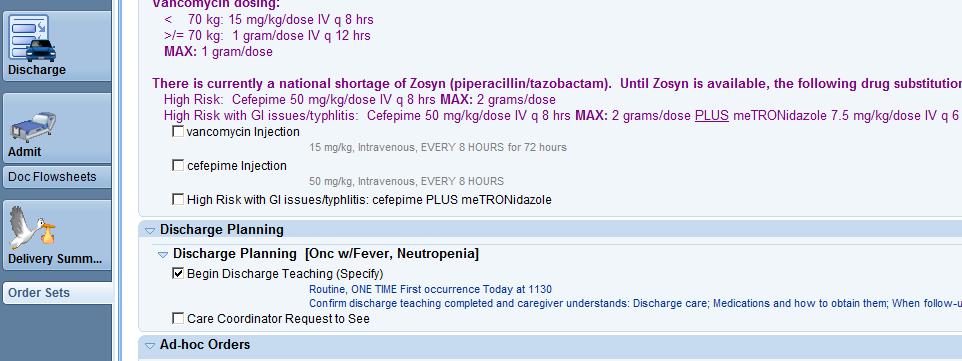
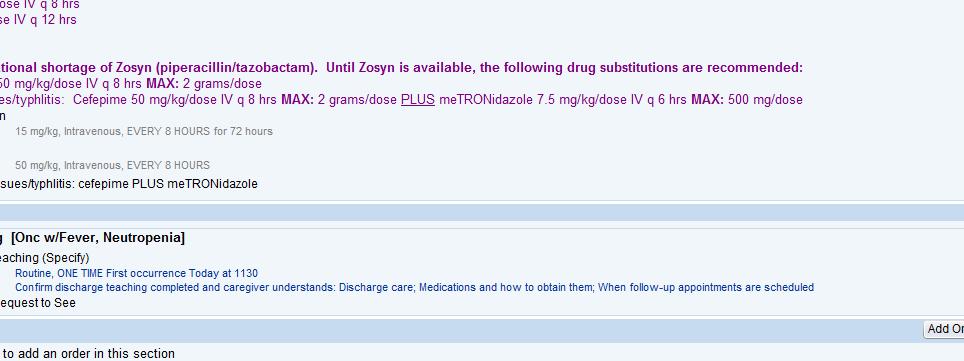
41 Best Practice Alert Page 40 Page 40
42 Fever in nonneutropenic pediatric oncology patients Retrospective review of 392 episodes of fever in 138 children who were nonneutropenic but had CVC Mean ANC 3100/mm 3 24 (6%) episodes of bacteremia were documented: No deaths due to bacteremia 10 patients admitted directly from the ED due to chills, signs of localized infection or break in the CVC Page 41 Bartholomew, F et al J Peds 2015 Page 41
43 Fever in nonneutropenic pediatric oncology patients Retrospective review of 392 episodes of fever in 138 children who were nonneutropenic but had CVC Fever found to be only predictor of bacteremia (39.4 C vs 38.7 C) Primary language spoken, race, income, sex, CVC type, ANC were not predictive Page 42 Bartholomew, F et al J Peds 2015 Page 42
44 Bottom line: letter from a father My daughter, Elizabeth, is a liver-small bowel transplant recipient on chemotherapy for PTLD and on Saturday evening, (her) axillary temperature was When we arrived, we were placed on the SHOCK treatment protocol to make a long story short, within 30 minutes of arrival, an IV was started, blood cultures were drawn, IV fluids initiated and antibiotics ordered This was the most amazing ER experience we have ever had...it is comforting to know that my child will be treated so rapidly and effectively and be spared a more complicated course I want to thank you for the treatment that she received Page 43 Page 43
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
FEBRILE NEUTROPENIA CURRENT GUIDELINES FOR CHILDREN Alia Zaidi, MD. St. Jude International Outreach Program
 SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p25oti35nt7
SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p25oti35nt7
Guideline for the Management of Fever and Neutropenia in Children with Cancer and/or Undergoing Hematopoietic Stem-Cell Transplantation
 Guideline for the Management of Fever Neutropenia in Children with Cancer /or Undergoing Hematopoietic Stem-Cell Transplantation COG Supportive Care Endorsed Guidelines Click here to see all the COG Supportive
Guideline for the Management of Fever Neutropenia in Children with Cancer /or Undergoing Hematopoietic Stem-Cell Transplantation COG Supportive Care Endorsed Guidelines Click here to see all the COG Supportive
Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008
 Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008 Study Title: Observational Study to Determine the Effect of an Emergency Department Adult Oncology Stat Antibiotic Protocol on Clinical Outcomes
Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008 Study Title: Observational Study to Determine the Effect of an Emergency Department Adult Oncology Stat Antibiotic Protocol on Clinical Outcomes
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
A Care Pathway exists for the management of neutropenic fever. Copies of the care pathway document are available in EAU, A&E, Deanesly and CHU.
 Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Febrile Neutropenia. These podcasts are designed to give medical students an overview of key topics in pediatrics. The
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Febrile Neutropenia. These podcasts are designed to give medical students an overview of key topics in pediatrics. The
Neutropenic Sepsis Acute General Management and Support. Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology
 Neutropenic Sepsis Acute General Management and Support Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology Who Am I? I am A Medical Oncologist (MCCN) Site specialist
Neutropenic Sepsis Acute General Management and Support Ernie Marshall Macmillan Consultant in Medical Oncology Clatterbridge Centre for Oncology Who Am I? I am A Medical Oncologist (MCCN) Site specialist
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
 MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Neutropenic Fever 1 InpatientPediatric Treatment
 Neutropenic Fever InpatientPediatric Treatment (Hematologic Cancers and Stem Cell Patients) te: This algorithm should not be used for patients receiving CAR cell therapy. Page of 8 Patient presents with
Neutropenic Fever InpatientPediatric Treatment (Hematologic Cancers and Stem Cell Patients) te: This algorithm should not be used for patients receiving CAR cell therapy. Page of 8 Patient presents with
Neutropenic Fever 1 InpatientPediatric Treatment
 Neutropenic Fever 1 InpatientPediatric Treatment (Solid Tumors) Note: This algorithm should not be used for patients receiving CAR cell therapy. Page 1 of 7 Patient presents with fever or develops fever
Neutropenic Fever 1 InpatientPediatric Treatment (Solid Tumors) Note: This algorithm should not be used for patients receiving CAR cell therapy. Page 1 of 7 Patient presents with fever or develops fever
J Clin Oncol 35: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 35 NUMBER 18 JUNE 20, 2017 JOURNAL OF CLINICAL ONCOLOGY S P E C I A L A R T I C L E Guideline for the Management of Fever and Neutropenia in Children With Cancer and Hematopoietic Stem-Cell Transplantation
VOLUME 35 NUMBER 18 JUNE 20, 2017 JOURNAL OF CLINICAL ONCOLOGY S P E C I A L A R T I C L E Guideline for the Management of Fever and Neutropenia in Children With Cancer and Hematopoietic Stem-Cell Transplantation
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Ailyn T. Isais-Agdeppa, MD*, Lulu Bravo, MD*
 A FIVE-YEAR RETROSPECTIVE STUDY ON THE COMMON MICROBIAL ISOLATES AND SENSITIVITY PATTERN ON BLOOD CULTURE OF PEDIATRIC CANCER PATIENTS ADMITTED AT THE PHILIPPINE GENERAL HOSPITAL FOR FEBRILE NEUTROPENIA
A FIVE-YEAR RETROSPECTIVE STUDY ON THE COMMON MICROBIAL ISOLATES AND SENSITIVITY PATTERN ON BLOOD CULTURE OF PEDIATRIC CANCER PATIENTS ADMITTED AT THE PHILIPPINE GENERAL HOSPITAL FOR FEBRILE NEUTROPENIA
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS
 CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
2018 CNISP HAI Surveillance Case definitions
 2018 CNISP HAI Surveillance Case definitions The following case definitions for the surveillance of healthcare-associated infections (HAIs) are used by all acute-care hospitals that participate in the
2018 CNISP HAI Surveillance Case definitions The following case definitions for the surveillance of healthcare-associated infections (HAIs) are used by all acute-care hospitals that participate in the
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
Guidelines in the Management of Febrile Neutropenia for Clinical Practice
 REFERENCES 1. Tangka FK, Trogdon JG, Richardson LC, Howard D, Sabatino SA, Finkelstein EA. Cancer treatment cost in the United States: has the burden shifted over time? Cancer. 2010;116(14):3477-3484.
REFERENCES 1. Tangka FK, Trogdon JG, Richardson LC, Howard D, Sabatino SA, Finkelstein EA. Cancer treatment cost in the United States: has the burden shifted over time? Cancer. 2010;116(14):3477-3484.
Supplemental Online Case Discussion: Febrile Neutropenia
 Supplemental Online Case Discussion: Febrile Neutropenia Alison C. Young, Fiona J. Collinson St James s Institute of Oncology, St James s University Hospital, Leeds, West Yorkshire, United Kingdom Case
Supplemental Online Case Discussion: Febrile Neutropenia Alison C. Young, Fiona J. Collinson St James s Institute of Oncology, St James s University Hospital, Leeds, West Yorkshire, United Kingdom Case
Effect of Outpatient Treatment of Febrile Neutropenia on the Risk Threshold for the Use of CSF in Patients with Cancer Treated with Chemotherapy
 Blackwell Science, LtdOxford, UKVHEValue in Health1098-30152005 ISPOR814752Original ArticleOutpatient Treatment of Febrile NeutropeniaCosler et al. Volume 8 Number 1 2005 VALUE IN HEALTH Effect of Outpatient
Blackwell Science, LtdOxford, UKVHEValue in Health1098-30152005 ISPOR814752Original ArticleOutpatient Treatment of Febrile NeutropeniaCosler et al. Volume 8 Number 1 2005 VALUE IN HEALTH Effect of Outpatient
Top 5 papers in clinical mycology
 Top 5 papers in clinical mycology Dirk Vogelaers Department of General Internal Medicine University Hospital Ghent Joint symposium BVIKM/BSIMC and SBMHA/BVMDM Influenza-associated aspergillosis in critically
Top 5 papers in clinical mycology Dirk Vogelaers Department of General Internal Medicine University Hospital Ghent Joint symposium BVIKM/BSIMC and SBMHA/BVMDM Influenza-associated aspergillosis in critically
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Ready to answer the questions?
 파워포인트문서의제목 Reference 1. IDSA GUIDELINES. Clinical Practice Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Disease Society of America.
파워포인트문서의제목 Reference 1. IDSA GUIDELINES. Clinical Practice Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Disease Society of America.
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Clostridium difficile Infection (CDI) Management Guideline
 Management Guideline") Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in Infants: Pediatric Dilemmas in Antibiotherapy
 Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
CASE SCENARIO EXERCISE
 påçííáëü=pìêîéáää~ååé=çñ=eé~äíüå~êé ^ëëçåá~íéç=fåñéåíáçå=mêçöê~ããé CASE SCENARIO EXERCISE CATHETER-ASSOCIATED URINARY TRACT INFECTION SURVEILLANCE SCOTTISH SURVEILLANCE OF HEALTHCARE ASSOCIATED INFECTION
påçííáëü=pìêîéáää~ååé=çñ=eé~äíüå~êé ^ëëçåá~íéç=fåñéåíáçå=mêçöê~ããé CASE SCENARIO EXERCISE CATHETER-ASSOCIATED URINARY TRACT INFECTION SURVEILLANCE SCOTTISH SURVEILLANCE OF HEALTHCARE ASSOCIATED INFECTION
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Blood cultures in ED. Dr Sebastian Chang MBBS FACEM
 Blood cultures in ED Dr Sebastian Chang MBBS FACEM Why do we care about blood cultures? blood cultures are the most direct method for detecting bacteraemia in patients a positive blood culture: 1. can
Blood cultures in ED Dr Sebastian Chang MBBS FACEM Why do we care about blood cultures? blood cultures are the most direct method for detecting bacteraemia in patients a positive blood culture: 1. can
Prompt Administration of Antibiotics Is Associated With Improved Outcomes in Febrile Neutropenia in Children With Cancer
 Pediatr Blood Cancer 2013;60:1299 1306 Prompt Administration of Antibiotics Is Associated With Improved Outcomes in Febrile Neutropenia in Children With Cancer Matthew Fletcher, MD, 1 Hailey Hodgkiss,
Pediatr Blood Cancer 2013;60:1299 1306 Prompt Administration of Antibiotics Is Associated With Improved Outcomes in Febrile Neutropenia in Children With Cancer Matthew Fletcher, MD, 1 Hailey Hodgkiss,
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Performance of a modified MASCC index score for identifying low-risk febrile neutropenic cancer patients
 DOI 10.1007/s00520-007-0347-3 ORIGINAL ARTICLE Performance of a modified MASCC index score for identifying low- febrile neutropenic cancer patients Luciano de Souza Viana & José Carlos Serufo & Manoel
DOI 10.1007/s00520-007-0347-3 ORIGINAL ARTICLE Performance of a modified MASCC index score for identifying low- febrile neutropenic cancer patients Luciano de Souza Viana & José Carlos Serufo & Manoel
Children who are neutropenic and unwell, even if normothermic, should be assumed to have infection and be treated appropriately.
 PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Comparison of Meropenem with Ceftazidime as Monotherapy of Cancer Patients with Chemotherapy induced Febrile Neutropenia
 Comparison of Meropenem with Ceftazidime as Monotherapy of Cancer Patients with Chemotherapy induced Febrile Neutropenia I. Malik ( National Cancer lnsititute, Karachi ) Shaharyar (, Department of Radiotherapy
Comparison of Meropenem with Ceftazidime as Monotherapy of Cancer Patients with Chemotherapy induced Febrile Neutropenia I. Malik ( National Cancer lnsititute, Karachi ) Shaharyar (, Department of Radiotherapy
5/1/2015 SEPSIS SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 INFECTION CAN BE CONFIRMED BY:
 SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
Osteomyelitis Samir S. Shah, MD, MSCE
 Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
TOPICS. Wheezing/Asthma THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE
 THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE Ghazala Q. Sharieff MD, MBA Wheezing/asthma Croup Immunizations and fever Appendicitis Complex febrile seizures Procedures Head Injury Zofran
THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE Ghazala Q. Sharieff MD, MBA Wheezing/asthma Croup Immunizations and fever Appendicitis Complex febrile seizures Procedures Head Injury Zofran
The Child with HIV and a Fever 1
 The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS
 PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS RATIONALE: It is increasingly being recognised that not all neutropenic patients have the same risk of complications during episodes
PILOT STUDY PROPOSAL FOR EARLY DISCHARGE OF LOW-RISK NEUTROPENIC PATIENTS RATIONALE: It is increasingly being recognised that not all neutropenic patients have the same risk of complications during episodes
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY
 PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
The Role of Observation Care in the Evaluation and Management of Cancer Emergencies
 The Role of Observation Care in the Evaluation and Management of Cancer Emergencies Adam Klotz, MD Associate Attending Physician Memorial Sloan Kettering Cancer Center FACULTY DISCLOSURE Nothing to disclose
The Role of Observation Care in the Evaluation and Management of Cancer Emergencies Adam Klotz, MD Associate Attending Physician Memorial Sloan Kettering Cancer Center FACULTY DISCLOSURE Nothing to disclose
Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians
 MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael
MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Data Descriptor: Pediatric patients at risk for fever in chemotherapyinduced neutropenia in Bern, Switzerland,
 www.nature.com/scientificdata OPEN Received: 3 October 2017 Accepted: 9 January 2018 Published: 13 March 2018 Data Descriptor: Pediatric patients at risk for fever in chemotherapyinduced neutropenia in
www.nature.com/scientificdata OPEN Received: 3 October 2017 Accepted: 9 January 2018 Published: 13 March 2018 Data Descriptor: Pediatric patients at risk for fever in chemotherapyinduced neutropenia in
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
CANCER RELATED INFECTION AND USE OF COLONY STIMULATING FACTORS
 CANCER RELATED INFECTION AND USE OF COLONY STIMULATING FACTORS Suphat Subongkot, Pharm.D, BCPS, BCOP Clinical Pharmacy, Khon Kaen University, Thailand Learning Objectives Summarize national guidelines
CANCER RELATED INFECTION AND USE OF COLONY STIMULATING FACTORS Suphat Subongkot, Pharm.D, BCPS, BCOP Clinical Pharmacy, Khon Kaen University, Thailand Learning Objectives Summarize national guidelines
Oncologist. The. Symptom Management and Supportive Care
 The Oncologist Symptom Management and Supportive Care Cancer-Associated Neutropenic Fever: Clinical Outcome and Economic Costs of Emergency Department Care D. MARK COURTNEY, a AMER Z. ALDEEN, a STEPHEN
The Oncologist Symptom Management and Supportive Care Cancer-Associated Neutropenic Fever: Clinical Outcome and Economic Costs of Emergency Department Care D. MARK COURTNEY, a AMER Z. ALDEEN, a STEPHEN
A Practical Approach to Leukopenia/Neutropenia in Children. Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014
 A Practical Approach to Leukopenia/Neutropenia in Children Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014 Disclosures EPIC trial MAST Therapeutics SUSTAIN trial Selexys Pharmaceuticals
A Practical Approach to Leukopenia/Neutropenia in Children Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014 Disclosures EPIC trial MAST Therapeutics SUSTAIN trial Selexys Pharmaceuticals
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE (MEDICAID) Colony Stimulating Factors (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Pharmacy Prior Authorization MERC CARE (MEDICAID) Colony Stimulating Factors (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Choc septique. Frédéric Pène
 Choc septique Frédéric Pène Réanimation Médicale, Hôpital Cochin, AP-HP Université Paris Descartes Institut Cochin, Inserm U1016, CNRS UMR-8104, Département 3i No conflict of interest A 54 y.o. male patient
Choc septique Frédéric Pène Réanimation Médicale, Hôpital Cochin, AP-HP Université Paris Descartes Institut Cochin, Inserm U1016, CNRS UMR-8104, Département 3i No conflict of interest A 54 y.o. male patient
Granulozytensupport in der Therapie der akuten Leukämie, eine Chance?
 Granulozytensupport in der Therapie der akuten Leukämie, eine Chance? Volker Witt in cooperation with TFM MUW Vienna Anti-infective prophylaxis in pediatric patients with acute myeloid leukemia. Lehrnbecher
Granulozytensupport in der Therapie der akuten Leukämie, eine Chance? Volker Witt in cooperation with TFM MUW Vienna Anti-infective prophylaxis in pediatric patients with acute myeloid leukemia. Lehrnbecher
Antifungals and current treatment guidelines in pediatrics and neonatology
 Dragana Janic Antifungals and current treatment guidelines in pediatrics and neonatology Dragana Janic. University Children`s Hospital, Belgrade, Serbia 10/10/17 Hotel Crowne Plaza, Belgrade, Serbia; www.dtfd.org
Dragana Janic Antifungals and current treatment guidelines in pediatrics and neonatology Dragana Janic. University Children`s Hospital, Belgrade, Serbia 10/10/17 Hotel Crowne Plaza, Belgrade, Serbia; www.dtfd.org
Neutropenic Sepsis Guideline
 Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days
 RESEARCH ARTICLE Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days AUTHORS Rianna C. Evans, MD, Bryan R. Fine, MD, MPH Division of Pediatric Hospital Medicine, Department of Pediatrics,
RESEARCH ARTICLE Time to Detection of Bacterial Cultures in Infants Aged 0 to 90 Days AUTHORS Rianna C. Evans, MD, Bryan R. Fine, MD, MPH Division of Pediatric Hospital Medicine, Department of Pediatrics,
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
A Clinical Pathway to Reduce Time to Antibiotic Administration in Pediatric Cancer Patients With Fever and Potential Neutropenia
 research report A Clinical Pathway to Reduce Time to Antibiotic Administration in Pediatric Cancer Patients With Fever and Potential Neutropenia Adam Lamble, MD 1 ; Thuan Nguyen MD, PhD 2 ; Susan Lindemulder,
research report A Clinical Pathway to Reduce Time to Antibiotic Administration in Pediatric Cancer Patients With Fever and Potential Neutropenia Adam Lamble, MD 1 ; Thuan Nguyen MD, PhD 2 ; Susan Lindemulder,
AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF)
") AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF) Colony Stimulating Factor (CSF) Neupogen (filgrastim; G-CSF), Neulasta (peg-filgrastim; G-CSF); Neulasa
AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF) Colony Stimulating Factor (CSF) Neupogen (filgrastim; G-CSF), Neulasta (peg-filgrastim; G-CSF); Neulasa
Clinical characteristics and therapeutic outcome of patients with febrile neutropenia: Our clinical experience
 International Journal of Clinical Medicine Research 2014; 1(1): 26-30 Published online April 30, 2014 (http://www.aascit.org/journal/ijcmr) Clinical characteristics and therapeutic outcome of patients
International Journal of Clinical Medicine Research 2014; 1(1): 26-30 Published online April 30, 2014 (http://www.aascit.org/journal/ijcmr) Clinical characteristics and therapeutic outcome of patients
Title: Author: Speciality / Division: Directorate:
 Antifungal guidelines for CANDIDIASIS INFECTIONS (Adults) Proven infection: Targeted antifungal therapy should be prescribed for: o Positive cultures from a sterile site with clinical or radiological abnormality
Antifungal guidelines for CANDIDIASIS INFECTIONS (Adults) Proven infection: Targeted antifungal therapy should be prescribed for: o Positive cultures from a sterile site with clinical or radiological abnormality
Cedars Sinai Medical Center Pediatric Electives
 PE 235.03 MEDICAL GENETICS COURSE CHAIR: John M. Graham, M.D., ScD.. By arrangement - Please contact the Student Coordinator 1. Counseling techniques and the approach to the patient and family with hereditary
PE 235.03 MEDICAL GENETICS COURSE CHAIR: John M. Graham, M.D., ScD.. By arrangement - Please contact the Student Coordinator 1. Counseling techniques and the approach to the patient and family with hereditary
AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF)
") AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF) Colony Stimulating Factor (CSF) Neupogen (filgrastim; G-CSF), Neulasta (peg-filgrastim; G-CSF); Neulasa
AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF) Colony Stimulating Factor (CSF) Neupogen (filgrastim; G-CSF), Neulasta (peg-filgrastim; G-CSF); Neulasa
Supportive Care For Hematological Malignancies
 Supportive Care For Hematological Malignancies Nawaf Alkhayat, MD Pediatric Hematology, Oncology & BMT Prince Sultan Military Medical City Riyadh, KSA Supportive care Definition Why we need supportive
Supportive Care For Hematological Malignancies Nawaf Alkhayat, MD Pediatric Hematology, Oncology & BMT Prince Sultan Military Medical City Riyadh, KSA Supportive care Definition Why we need supportive
2. Is therapy prescribed by, or in consultation with, a hematologist and/or oncologist?
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Colony Stimulating Factors (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Colony Stimulating Factors (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection
 Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Fever in Children. Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital
 Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
New Antimicrobials and Rapid Diagnostics: Implications for Antibiotic Stewardship
 New Antimicrobials and Rapid Diagnostics: Implications for Antibiotic Stewardship Mia A. Taormina, DO, FACOI Chair, Department of Infectious Disease, DuPage Medical Group Disclosures While product trade
New Antimicrobials and Rapid Diagnostics: Implications for Antibiotic Stewardship Mia A. Taormina, DO, FACOI Chair, Department of Infectious Disease, DuPage Medical Group Disclosures While product trade
The Role of POCT in Management of Infectious Disease in the Critical Care Setting
 The Role of POCT in Management of Infectious Disease in the Critical Care Setting Nathan A Ledeboer Associate Professor of Pathology Medical College of Wisconsin Medical Director, Microbiology and Molecular
The Role of POCT in Management of Infectious Disease in the Critical Care Setting Nathan A Ledeboer Associate Professor of Pathology Medical College of Wisconsin Medical Director, Microbiology and Molecular
Urinary tract infection. Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine
 Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Circle Yes or No Y N. (Note: requests without this information will not be accepted.) [If no, then no further questions.]
![Circle Yes or No Y N. (Note: requests without this information will not be accepted.) [If no, then no further questions.]](/thumbs/82/85863866.jpg "Circle Yes or No Y N. (Note: requests without this information will not be accepted.) [If no, then no further questions.]") 04/25/2016 Prior Authorization AETA BETTER HEALTH OF LA MEDICAID Colony Stimulating Factors (LA88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
04/25/2016 Prior Authorization AETA BETTER HEALTH OF LA MEDICAID Colony Stimulating Factors (LA88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Febrile Neutropenia Jean A Klastersky
 Febrile Neutropenia Febrile Neutropenia Jean A Klastersky Consultant, Medical Oncology Institut Jules Bordet Centre des Tumeurs de l Universite Libre de Bruxelles Brussels Belgium Published by Springer
Febrile Neutropenia Febrile Neutropenia Jean A Klastersky Consultant, Medical Oncology Institut Jules Bordet Centre des Tumeurs de l Universite Libre de Bruxelles Brussels Belgium Published by Springer
Panel Discussion: What s New with DRGs and ICD?
 Panel Discussion: What s New with DRGs and ICD? Moderator: Angie Comfort, RHIA, CDIP, CCS, CCS-P Thilo Koepfer, MD Wilbur Lo, MD, CDIP, CCA Objectives Get updated on the current status of ICD- 11 IR-DRG
Panel Discussion: What s New with DRGs and ICD? Moderator: Angie Comfort, RHIA, CDIP, CCS, CCS-P Thilo Koepfer, MD Wilbur Lo, MD, CDIP, CCA Objectives Get updated on the current status of ICD- 11 IR-DRG
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Continuing malaria education modules. Module 1 Severe malaria triage, diagnosis, and treatment
 The MalariaCare Toolkit Tools for maintaining high-quality malaria case management services Continuing malaria education modules Module 1 Severe malaria triage, diagnosis, and treatment Download all the
The MalariaCare Toolkit Tools for maintaining high-quality malaria case management services Continuing malaria education modules Module 1 Severe malaria triage, diagnosis, and treatment Download all the
IMPACT #: Local Inventory #: form 04. Age at admission: d. mo yr. Postal code:
 - Date of birth: birth: Date of admission: year month day year month day Age at admission: d mo yr Postal code: Ethnic code: Hospital: Gender: 1 = male 2 = female 1 = Impact 2 = Other local, specify: Code
- Date of birth: birth: Date of admission: year month day year month day Age at admission: d mo yr Postal code: Ethnic code: Hospital: Gender: 1 = male 2 = female 1 = Impact 2 = Other local, specify: Code
Febrile neutropenia. Febrile neutropenia. Febrile neutropenia. Febrile neutropenia 1/30/2019. Infection in patients with cancer
 Manit Sae-teaw B.Pharm, BCP, BCOP Glad dip in pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University Fever Oral temperature measurement of 38.3 C (101.0 F) single 38.0 C (100.4
Manit Sae-teaw B.Pharm, BCP, BCOP Glad dip in pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University Fever Oral temperature measurement of 38.3 C (101.0 F) single 38.0 C (100.4
Supplementary Online Content
 Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September