Direct Thrombin Inhibitors and Gp 2b/3a Receptor Blockers in the Cardiac Cath Lab. Eric J Dippel, MD FACC
|
|
|
- Vivien Goodman
- 5 years ago
- Views:
Transcription


1 Midwest Cardiovascular Research Foundation Direct Thrombin Inhibitors and Gp 2b/3a Receptor Blockers in the Cardiac Cath Lab Eric J Dippel, MD FACC
2 Plaque Rupture Stable Angina Unstable Angina Non Q-wave MI Q-wave MI Adapted from Cannon CP. J Thrombolysis. 1995;2:

3 Thrombus Formation

4



5 Events Leading to Thrombus Formation Adhesion Activation Aggregation
 Platelet-specific proteins (PF4, β -thromboglobulin proteins) Non platelet-specific proteins")
 Thromboxane Lysosomes (enzymes) galactosidases Resting proteases Platelet")
6 Platelet Activation α - Granules (secreted proteins) Plasma proteins (fibrinogen, fibronectin, vwf, Factor V, plasminogen) Platelet-specific proteins (PF4, β -thromboglobulin proteins) Non platelet-specific proteins (thrombospondin, PDGF, amyloid protein precursor) ther (vascular permeability factor, IL-1, PADGEM) Amine Storage Granules (Serotonin, ADP, ATP, Ca ++ ) Thromboxane Lysosomes (enzymes) galactosidases Resting proteases Platelet Activated Platelet

7 Coagulation Cascade

8 Coagulation Cascade

9 Coagulation Cascade

10 Coagulation Cascade
11

12 Ruptured Plaque

13 Coagulation Cascade

14 Coagulation Cascade

15 Coagulation Cascade
16 Coagulation Cascade
17 Targets for Anti-Thrombotics Tissue Factor Inhibitors Direct Xa Inhibitors Pentasaccharides AT LMWH Heparin AT Bivalirudin Hirudin Argatroban Tissue factor Plasma clotting cascade Factor Xa Prothrombin Thrombin Fibrinogen Fibrinolytics Aspirin Conformational activation of GPIIb/IIIa Platelet aggregation Fibrin Collagen Thromboxane A 2 ADP Thrombus Ticlopidine Clopidogrel GPIIb/IIIa inhibitors

18 Treatment of cclusive Coronary Thrombus Platelets Fibrin Antiplatelet therapy Aspirin Thienopyridines GP IIb/IIIa inhibitors Thrombin Antithrombin therapy Heparin LMWH Direct thrombin Plasminogen activators tpa rpa SK TNK-tPA Cannon CP. J Am Coll Cardiol 1999;34:
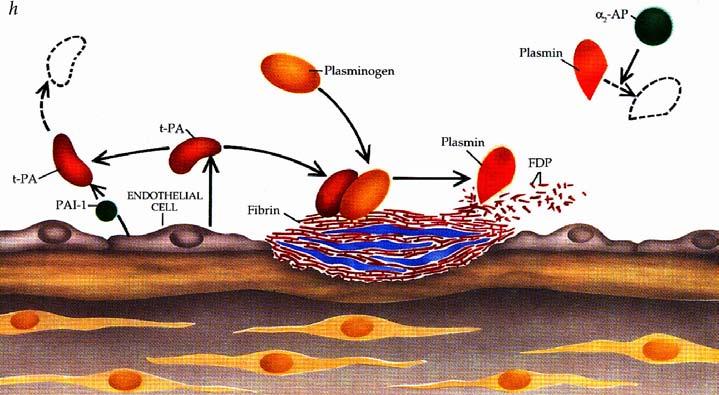
19 Plasmin cleaves fibrin Lyses clot FDPs (antiplatelet and anticoagulant) Fibrinogen Reperfusion Platelets Fibrin Thrombin Thrombus occluding coronary artery Thrombolytic therapy Exposes clot-bound thrombin Activates platelets PAI-1, thromboxane A 2, New thrombin fibrinogen generation Platelet activation Platelet activation Cleaves fibrinogen Thrombin production to fibrin Vasoconstriction Inhibits plasminogen activators Thrombus formation Vessel reocclusion Cannon CP. J Am Coll Cardiol 1999;34:


20 Heparin Recipe Kleiman. J Inv Card, Dec 2000.
21 Major Saccharide Components in Pharmaceutical Heparin C 2 - H S CH 2 S 3 H NHS 3 - Trisulfated Disaccharide CH 2 H - C 2 H H - - S 3 NHS 3 C 2 - H H CH 2 S 3 - H NHS 3 - Disulfated Disaccharide - CH 2 S 3 H NHAc - C 2 - CH 2 S C 2 H S 3 H - H NHS 3 S CH 2 S 3 H - NHS C CH 2 2 S 3 CH 2 S C 2 H S H 3 H - - NHS 3 H NHS 3 S CH 2 S 3 H - NHS 3 Antithrombin III Pentasaccharide Binding Sites
22 Heparin Non-specific binding to circulating proteins, acute phase reactants, and cellular binding sites Directly activates platelets Potentiates the platelet response to low levels of agonists such as ADP Unpredictable dose response
23 Antithrombotic Therapies and Platelet Aggregation in Normals 14 Saline UFH LMWH ARG 12 * p < 0.05, ** p < 0.01 vs. control Percent Maximum ** * * 2 0 ADP ( μ M) TRAP (0.625 μ M) Xiao Z, Theroux P. Circ 1998;97:
24 Platelet Activation by Unfractionated Heparin Fibrinogen Binding Index Unstimulated ADP 1.0 ( μ mol.1-1 ) UFH LMWH Heparin / fragmin (units.ml -1 ) (Normal Subjects) Knight CJ et al. Eur Heart J. 1998;19:1239
25 Prothrombin F 1.2 Va Ca ++ Xa Platelet F1.2 Thrombin Platelet Activation Fibrinogen AT III FPA Fibrin 1 TAT III
26 Thrombin Rebound After Cessation of Intravenous Heparin FPA Time 0 3 Hr 6 Hr 10 Hr 24 Hr 1 Miller, Granger, Califf. Circ. 1993;88:I FPA F (*p<0.03; **p<0.001) F1.2
27 Thrombin Generation Follows Heparin Discontinuation in Patients with Acute Coronary Syndromes 5 4 Baseline D/C Heparin IV Heparin Wean SC Heparin Wean F1.2 (nm) Baseline 1 Hour 4 Hours 24 Hours 1 Becker RC. JACC 1999;34:1020
28 Disadvantages of UFH Bleeding Thrombocytopenia Unfractionated Heparin Poor Bioavailability Stronger Drug Interactions Anticoagulant Response Variations
29 Heparin/LMWH: mechanism of action Heparin/AT complex inhibits thrombin and Factor Xa Must have adequate AT present for anticoagulant effect Thrombin inhibition requires bridging by heparin chain (at least 18 units) Antithrombin LMWH has greater activity against Xa than thrombin 2 Thrombin 1 Heparin Antithrombin Pentasaccharide sequence Heparin chains with pentasaccharide sequence (~30%) bind to AT causing a conformational change LMWH Antithrombin Pentasaccharide sequence Factor Xa X/E//109.a.1
30 Hirudin: : mechanism of action Binds directly to two sites on thrombin Binding is highly specific and almost irreversible very very long half-life life may account for the high bleed rates seen with hirudins in clinical trials 2 Hirudin Thrombin 1 Inactivates both circulating and clot-bound thrombin hirudin displaces thrombin from fibrin Fibrin X/E//110.a.1
31 Structure of Thrombin: Gly-Pro-Arg-Pro (active-site-binding portion) 2 Thrombin (Gly) 4 1 C-terminal dodecapeptide (Exosite 1-binding portion) Fibrin Active Site: : cleaves fibrinogen and coagulation factors Exosite Site 1: activates platelets, activates protein C, anchors fibrinogen A/E//20.b.1
32 Bivalirudin: mechanism of action Gly-Pro-Arg-Pro (active-site-binding portion) (Gly) 4 2 Thrombin 1 Inactivates both circulating and clot-bound thrombin bivalirudin competitively displaces thrombin from fibrin Thrombin slowly cleaves Arg 3 -Pro 4 bond, resulting in recovery of thrombin active site function C-terminal dodecapeptide (Exosite 1-binding portion) Fibrin A/E//20.b.1
33 Direct Thrombin Inhibitors Thrombin Refludan (lepirudin) Refludan Irreversible Indication: : HIT T1/2 = 1.3 hr Angiomax (bivalirudin) Novastan (argatroban) Angiomax Reversible PTCA 25 min Novastan Reversible HIT 45 min
34 Argatroban: : mechanism of action Argatroban only binds near the active site on thrombin Argatroban has a short half-life life 2 54% of argatroban binds to human serum proteins Argatroban Thrombin 1 X/E//111.a.1
35 Pharmacokinetic Profile Bolus 0.75 mg/kg [Bivalirudin] Mean ng/ml Infusion 2.5 mg/kg/h t ½ = 25 min. Clearance = 3.4 ml/min/kg Time from start of bivalirudin bolus (hours)
36 Hemorrhagic outcomes 10% 8% 6% 4% p < p < p < p < p = Heparin (N=2151) Bivalirudin (N=2161) 2% 0% Any major bleed 3g/dL [Hgb] Transfuse 2U 5g/dL [Hgb] RP or IC bleed
37 Bleeding by renal function B A T Incidence of major bleeding 25% 20% 15% 10% 5% 0% 3.1% 1.2% n=256 None ( 90 ml/min) heparin bivalirudin 8.5% 1.9% Mild (60 89 ml/min) 12.7% 6.0% Moderate (30 59 ml/min) 20.0% 0.0% n=275 n=461 n=454 n=250 n=301 n=7 n=12 Severe (<30 ml/min) Robson, J Invas Cardiol. 2000, 12SupplF: 33F-36F



38 Plaque Rupture Thrombus Mechanical Vasoconstrictive Distal Embolization Mechanical Plugging Serotonin Release Vasoconstriction


39 Microvascular Injury Activated IIb/IIIa stained red Platelet aggregate plugging a small vessel


40 Comparing the Physical Differences of the Glycoprotein 2b/3a Inhibitors Fibrinogen abciximab Small Molecules 2b/3a MAC-1 Platelet Surface 2b/3a av/β3
41 Response to Platelet Activation GP IIb/IIIa receptor antagonist Agonist Inhibition of platelet aggregation GP IIb/IIIa receptors occupied by antagonists ADP, thrombin, collagen and others Resting platelet GP IIb/IIIa receptors in unreceptive state Fibrinogen Aggregating platelets GP IIb/IIIa receptors occupied by fibrinogen which forms bridges between adjacent platelets
42 Major Differences Among GPIIb/IIIa Inhibitors Abciximab Eptifibatide Tirofiban Platelet-bound half-life Long Short Short (hours) (seconds) (seconds) Plasma half-life Short Long Long (minutes) (2.5 hr) (1.8 hr) Drug-to-receptor ratio ,500 1 >250 2 % of dose in bolus ~75% 3 <2 5% <2 5% Dosage adjustment in renal insufficiency None Yes Yes 1 IMPACT-II and PURSUIT doses. 2 RESTRE and PRISM- PLUS doses. 3 For any individual receiving a weight-adjusted, 12-hour infusion.
43 Major Differences Among GPIIb/IIIa Inhibitors Anticoagulant Properties Abciximab Eptifibatide Tirofiban Thrombin generation Activated clotting time +35 sec +25 sec N/A Reversibility* 12 hrs 4 6 hrs >4 hrs Reversibility with platelets Yes No No *50% Return of platelet function without platelet transfusion
44 During Drug Infusion Abciximab Small Molecule 80% 80% 80% 80% 80% 80% 80% 80% 80% Total dose of abciximab is an ~twofold molar excess over GPIIb/IIIa Total dose of small molecule antagonist is a >100-fold molar excess over GPIIb/IIIa Numbers represent GPIIb/IIIa receptor occupancy and are an approximation

45 Platelet Transfusion Rapidly Normalizes Bleeding Time Abciximab -
46 Immediately After Platelet Transfusion Abciximab Small Molecule 80% 80% 0% 80% 0% 80% 80% 20% 80% 80% 80% 80% 79% 80% 80% Very little free drug to block transfused platelets Large pool of free drug to block transfused platelets Numbers represent GPIIb/IIIa receptor occupancy and are an approximation
47 Absolute Differences over Time Effects of Small Molecule Therapy on Mortality % change vs placebo IMPACT II (n = 4,010) PURSUIT (n = 9,461) ESPRIT (n = 2,007) RESTRE (n = 2,141) PRISM+ (n = 1,570) PARAGN A (n = 7,232) Months after randomization IMPACT II: Lancet 1997; 349: , ACC 1999 ral presentation, PURSUIT: NEJM 1998; 339:436-43, ESC 1998; ral Presentation,PRISM-PLUS: NEJM 1998; 338: , RESTRE: Circ. 1997; 96: , JACC 1998; 32:28-34, PARAGN A: Circ 1998; 97: ESPRIT: SCAI 2000, ral Presentation.
48 Absolute Differences over Time Effects of Abciximab Therapy on Mortality EPIC (B&I) (n = 1404) EPILG (n = 2792) 0 EPISTENT (n = 1603) % change vs placebo * Abciximab p = * p = p = ERASER (n = 225) RAPPRT (n = 483) CAPTURE (n = 1265) Neumann(n = 401) ADMIRAL (n = 300) Months since randomization EPIC: NEJM 1994; 330:956-61, Lancet 1994; 343:881-86, JAMA 1997; 278:479-84, CAPTURE: Lancet 1997; 349: , ACC 2000 oral., EPILG: Internal Data, Centocor, EPISTENT: Lancet 1998; 352:87-92, NEJM 1999; 341:319-27, Lancet 1999; 354: , RAPPRT:. 1998; 98:734-41, ERASER: Circ. 1999; 100; , ADMIRAL: ETC 2000, oral pres., Neumann : JACC 2000; 35: pres Circ
")
49 Mortality at Maximum Duration of Follow-Up: All Patients Intention to Treat HR 0.83 ( )

50 Platelet Thrombi Cause Vessel cclusion at Site of Injury and Downstream Platelet Aggregation Platelet Attachment at Site of Endothelial Injury Transient Platelet Aggregation Mechanical bstruction Vasoconstriction Mechanical bstruction Vasocconstriction


51 Stenting the Tip of the Iceberg


52 Coronary Tree --Stenting the Tip of the Iceberg

53 SIRIUS - Clinical Events All Events (to 270 days) P<0.001 % 16.7% 4.7% TLR 3.2% 3.8% 7.4% 0.5% 7.2% ut-of-hosp death MI 3.7% 2.4% In-hosp MACE 1.0% Sirolimus (n=190) TVR (Non-TL) Control (n=210) In-hospital MACE ut-of-hosp death MI TVR (Non-TL) TLR
54 Meta-analysis analysis of Balloon vs. Stent Trials Balloon Stent p=0.106 p= % Patients * 3314 pts ** 4345 pts (17 trials) p=0.970 p= Day* 6 Month** 30 Day 6 Month DEATH DEATH / MI 1 Kong, Hasselblad, Topol, Califf (submitted)
55 Mortality Follow-up - Abciximab Latest Follow-up in All Randomized Trials % of Patients EPIC (3 years) 6.8 EPILG (1 year) EPISTENT (1 year) p = CAPTURE (4 years) ERASER (6 months) 0.0 RAPPRT (6 months) ADMIRAL (6 months) Neumann (1 year) EPIC: JAMA 1997; 278:479-84, CAPTURE: Simoons, oral presentation, ACC 2000, EPILG: Internal Data, Centocor, EPISTENT: Lancet 1999; 354: , RAPPRT: Circ. 1999; 98:734-41, ERASER Circ. 1999;100: , Neumann: JACC 2000; 35(4): , personal comm, JF Neumann; ADMIRAL: Montelescot, oral presentation, ACC Placebo Abciximab
56 Clinical Results of CACHET BC Trial Hemorrhage Death, MI, revasc Bivalirudin + ReoPro (24%) n = % 2.8% 75% reduction p-value <0.013 Heparin + ReoPro (100%) n = % 7.8% % of patients with events at 7 days
57 REPLACE-2: Design Multicenter international trial United States 78% of patients Europe 15% Canada 7% Double-blind, double dummy design 6002 Urgent or elective PCI patients Aspirin Clopidogrel Stent Bivalirudin Provisional GPIIb/IIIa Heparin Abciximab or Eptifibatide Endpoints 30-day Death MI Revasc Hemorrhage Economics, ischemia 6, 12m follow up Lincoff M et al. JAMA 2003

58 30-day endpoints All pre-specified endpoints of the trial were met p=0.329 p=0.328 p=0.197 p<0.001 p=0.178 p= % 9.2% Heparin + GPIIb/IIIa (N=3008) Bivalirudin (N=2994) 7.1% 7.6% 5.8% 6.6% 4.1% 2.4% 2.0% 1.6% 5.2% 3.5% Death, any MI, revasc, bleed Death, any MI, revasc CKMB >3xULN Major bleed Death, QMI, revasc Death, QMI, revasc, bleed Lincoff AM et al JAMA 2003; 289:
 Kong et al 2003 Am J Cardiol 2003; 92: 651-5 12 trials 20,186 patients (dds ratio) New Rx")
59 Mortality vs. heparin at 6 mo Karvourni et al 2003 J Am Coll Cardiol 2003; 41: trials 20,137 patients (Risk ratio) Kong et al 2003 Am J Cardiol 2003; 92: trials 20,186 patients (dds ratio) New Rx better Heparin better New Rx better Heparin better GPIIb/IIIa meta-analysis Bivalirudin REPLACE-2 N= Risk ratio ±95% CI for death at 6 months dds ratio ±95% CI for death at 6 months
60 Background: Current Management of ACS Early invasive strategy if moderate-high risk 1,2 Median time to cath 21 hours 3 Revascularization with PCI or CABG 1,2 55% PCI, 12% CABG, 33% medical mgt 3 Triple anti-platelet therapy 1,2 Aspirin Clopidogrel (initiated pre or post angiography) GP IIb/IIIa inhibitors - started upstream in all pts or in the CCL for PCI Unfractionated or LMW heparin 1,2,4 1 Braunwald et al JACC 2002; 2 Bertrand et al. EHJ 2002; SYNERGY. JAMA 2004;292:45-54
61 Bivalirudin in ACS: Hypotheses In moderate-high risk patients with ACS undergoing an invasive strategy, compared to UFH or LMWH + GP IIb/IIIa inhibitors: Bivalirudin + GP IIb/IIIa inhibitors will result in less adverse ischemic events and less bleeding Bivalirudin alone will result in similar rates of ischemic events and markedly reduced bleeding
62 ACUITY Design. Stone GW et al. AHJ 2004;148: Study Design First Randomization Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,800) Moderatehigh risk ACS Aspirin in all Clopidogrel dosing and timing per local practice R* UFH or Enoxaparin + GP IIb/IIIa Bivalirudin + GP IIb/IIIa Bivalirudin Alone Angiography within 72h Medical management PCI CABG *Stratified by pre-angiography thienopyridine use or administration
63 ACUITY Design. Stone GW et al. AHJ 2004;148: Study Design Second Randomization Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,800) Moderatehigh risk ACS Aspirin in all Clopidogrel dosing and timing per local practice UFH or Enoxaparin Routine upstream GPI in all pts R GPI started in CCL for PCI only R Bivalirudin Routine upstream GPI in all pts GPI started in CCL for PCI only Bivalirudin Alone Angiography within 72h Medical management PCI CABG
64 Primary Endpoint Measures (ITT) UFH/Enoxaparin + GPI vs. Bivalirudin + GPI Primary endpoint Risk ratio ±95% CI Bival UFH/Enox + IIb/IIIa + IIb/IIIa RR (95% CI) p value (non inferior) (superior) Net clinical outcome Ischemic composite Major bleeding Upper boundary non-inferiority 11.8% 11.7% 1.01 ( ) 7.7% 7.3% 1.07 ( ) 5.3% 5.7% 0.93 ( ) < < Bivalirudin + IIb/IIIa better UFH/Enox + IIb/IIIa better
65 Primary Endpoint Measures (ITT) UFH/Enoxaparin + GPI vs. Bivalirudin Alone Primary endpoint Risk ratio ±95% CI Bival alone UFH/Enox + IIb/IIIa RR (95% CI) p value (non inferior) (superior) Net clinical outcome Ischemic composite Major bleeding Upper boundary non-inferiority 10.1% 11.7% 0.86 ( ) 7.8% 7.3% 1.08 ( ) 3.0% 5.7% 0.53 ( ) < <0.001 <0.001 Bivalirudin alone better UFH/Enox + IIb/IIIa better
66 Components of the Ischemic Composite UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone UFH/Enox+GPI (N=4603) Bivalirudin+GPI (N=4604) Bivalirudin alone (N=4612) 30 day events (%) P Sup = 0.32 P Sup = 0.34 P Sup = 0.35 P Sup = % 7.7% 7.8% 4.9% 5.0% 5.4% 2.3% 2.7% 2.4% 1.3% 1.5% 1.6% Ischemic composite Death Myocardial infarction Unplanned revasc for ischemia
67 Major Bleeding Endpoints UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone Heparin+GPI (N=4603) Bivalirudin+GPI (N=4604) Bivalirudin alone (N=4612) P Sup =0.31 P Sup <.001 P Sup =0.38 P Sup < day events (%) 11.8% 11.1% 9.1% 5.7% 5.3% 3.0% All major bleeding Non CABG major bleeding (primary endpoint)
68 Net Clinical utcome Composite UFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone Risk ratio ±95% CI Bival Alone UFH/Enox + IIb/IIIa RR (95% CI) P P int Biomarkers (CK/Trop) Elevated (n=5368) Normal (n=3841) 12.2% 7.1% 13.3% 9.4% 0.92 ( ) 0.75 ( ) ST Deviation Yes (n=3197) No (n=6008) 13.0% 8.6% 13.7% 10.6% 0.96 ( ) 0.81 ( ) TIMI Risk Score Low (0-2) (n=1291) Intermed (3-4) (n=4407) High (5-7) (n=2449) Pre Thienopyridine Yes (n=5192) No (n=4023) 6.4% 10.2% 0.63 ( ) % 10.2% 0.92 ( ) % 15.2% 0.92 ( ) % 11.3% 12.2% 11.1% 0.76 ( ) 1.02 ( ) < Bivalirudin alone better UFH/Enox + IIb/IIIa better
69 Conclusions Heparin has significant limitations Requires a cofactor (ATIII) Non-specific protein binding Variable dose response Activates platelets Thrombocytopenia Thrombin rebound Would not gain FDA approval in 2007
70 Conclusions Low risk elective PCI Bivalirudin alone provides superior clinical outcomes compared to UFH alone, and no difference compared to UFH / Gp 2b3a Provided they have been adequately pre- treated with ASA and Plavix Bivalirudin alone has less bleeding than UFH / Gp 2b3a
71 Conclusions Moderate to high risk PCI No difference in ischemic complications comparing bivalirudin alone vs UFH / Gp 2b3a vs bivalirudin / Gp 2b3a Provided patients are adequately pre-loaded with ASA and Plavix Less bleeding with bivalirudin alone vs UFH / Gp 2b3a vs bivalirudin / Gp 2b3a
72 Death is a very good way to cut down on expenses. Woody Allen Love and Death
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC
 Mitchell W. Krucoff, MD, FACC") Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Pathophysiology of ACS
 Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Columbia University Medical Center Cardiovascular Research Foundation
 STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
Novel Anticoagulation Therapy in Acute Coronary Syndrome
 Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI
 Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Is the role of bivalirudin established?
 Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Is there a real need for new agents to optimize efficacy/safety balance
 Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
NOVEL ANTI-THROMBOTIC THERAPIES FOR ACUTE CORONARY SYNDROME: DIRECT THROMBIN INHIBITORS
 Judd E. Hollander, MD Professor, Clinical Research Director, Department of Emergency Medicine University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania OBJECTIVES: 1. Discuss the concept
Judd E. Hollander, MD Professor, Clinical Research Director, Department of Emergency Medicine University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania OBJECTIVES: 1. Discuss the concept
CHAPTER 17 Antithrombotic Agents Heparins
 CHAPTER 17 Antithrombotic Agents Heparins Structure Mechanism of Action Pharmacokinetics Limitations of Unfractionated Heparin Heparin Induced Thrombocytopenia Heparin Rebound Low Molecular Weight Heparins
CHAPTER 17 Antithrombotic Agents Heparins Structure Mechanism of Action Pharmacokinetics Limitations of Unfractionated Heparin Heparin Induced Thrombocytopenia Heparin Rebound Low Molecular Weight Heparins
Adjunctive Pharmacological Therapies in PCI : Antiplatelets and Anticoagulants
 Adjunctive Pharmacological Therapies in PCI : Antiplatelets and Anticoagulants Young-Hak Kim, MD Asan Medical Center, Seoul, Korea Why Drug? PCI localized therapy Drug systemic effect Fate of Disrupted
Adjunctive Pharmacological Therapies in PCI : Antiplatelets and Anticoagulants Young-Hak Kim, MD Asan Medical Center, Seoul, Korea Why Drug? PCI localized therapy Drug systemic effect Fate of Disrupted
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
Antiplatelet Therapy: how, why, when? For Coronary Stenting
 Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Bivalirudin should be indicated for all patients with STEMI. Adnan Kastrati Deutsches Herzzentrum, Munich, Germany
 Bivalirudin should be indicated for all patients with STEMI Adnan Kastrati Deutsches Herzzentrum, Munich, Germany 1 Heparin+IIb/IIIa, heparin alone or bivalirudin in STEMI: Do we have the answer? 2 Heparin+IIb/IIIa,
Bivalirudin should be indicated for all patients with STEMI Adnan Kastrati Deutsches Herzzentrum, Munich, Germany 1 Heparin+IIb/IIIa, heparin alone or bivalirudin in STEMI: Do we have the answer? 2 Heparin+IIb/IIIa,
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 8, 2014
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Anticoagulation Update David J. Moliterno, MD
 David J., MD Anticoagulant Agents n Cardiovascular Medicine: An Update David J., MD Professor and Chairman Division of Cardiovascular Medicine The University of Kentucky Linda and Jack Gill Heart nstitute
David J., MD Anticoagulant Agents n Cardiovascular Medicine: An Update David J., MD Professor and Chairman Division of Cardiovascular Medicine The University of Kentucky Linda and Jack Gill Heart nstitute
Antiplatelet and Antithrombotic Therapies in PCI Defining the Optimal Strategy
 Antiplatelet and Antithrombotic Therapies in PCI Defining the Optimal Strategy Franz-Josef Neumann Herz-Zentrum Bad Krozingen Antiplatelet and Antithrombotic Therapies in PCI Defining the Optimal Strategy
Antiplatelet and Antithrombotic Therapies in PCI Defining the Optimal Strategy Franz-Josef Neumann Herz-Zentrum Bad Krozingen Antiplatelet and Antithrombotic Therapies in PCI Defining the Optimal Strategy
Scottish Medicines Consortium
 Scottish Medicines Consortium bivalirudin, 250mg powder for concentrate for solution for injection or infusion (Angiox ) No. (516/08) The Medicines Company UK Ltd 07 November 2008 The Scottish Medicines
Scottish Medicines Consortium bivalirudin, 250mg powder for concentrate for solution for injection or infusion (Angiox ) No. (516/08) The Medicines Company UK Ltd 07 November 2008 The Scottish Medicines
2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY
 2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY Charles V. Pollack, Jr., MA, MD, FACEP, FAAEM, FAHA Professor and Chairman, Department of Emergency
2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY Charles V. Pollack, Jr., MA, MD, FACEP, FAAEM, FAHA Professor and Chairman, Department of Emergency
Oral Antiplatelet Therapy in PCI/ACS. Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine
 Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Otamixaban for non-st-segment elevation acute coronary syndrome
 Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
P2Y 12 blockade. To load or not to load before the cath lab?
 UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
An Update on Oral Anti-platelet therapy in patients with non-st Myocardial Infarction. Disclosures
 An Update on Oral Anti-platelet therapy in patients with non-st Myocardial Infarction R. Scott Wright, MD, FACC, FESC, FAHA, Professor of Medicine Mayo Clinic Fall Managed Care Forum November 2013 3098590-1
An Update on Oral Anti-platelet therapy in patients with non-st Myocardial Infarction R. Scott Wright, MD, FACC, FESC, FAHA, Professor of Medicine Mayo Clinic Fall Managed Care Forum November 2013 3098590-1
Scottish Medicines Consortium
 Scottish Medicines Consortium bivalirudin 250mg for injection or infusion (Angiox ) (156/05) Nycomed UK Ltd No. 4 February, 2005 The Scottish Medicines Consortium has completed its assessment of the above
Scottish Medicines Consortium bivalirudin 250mg for injection or infusion (Angiox ) (156/05) Nycomed UK Ltd No. 4 February, 2005 The Scottish Medicines Consortium has completed its assessment of the above
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Platelet-fibrin clot. 50Kd STEMI. Abciximab. Video of a IIb/IIIa inhibitor in action. Unstable Angina and non-stsegment
 Objectives IIb/IIIa, Vitamin K, and Direct Thrombin Inhibition in Cardiology Michael Gulseth, Pharm. D., BCPS Assistant Professor, Duluth Pharmacy 6122 February 14, 2005 Describe the pharmacology, kinetics,
Objectives IIb/IIIa, Vitamin K, and Direct Thrombin Inhibition in Cardiology Michael Gulseth, Pharm. D., BCPS Assistant Professor, Duluth Pharmacy 6122 February 14, 2005 Describe the pharmacology, kinetics,
TRANSPARENCY COMMITTEE OPINION. 29 April 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 29 April 2009 ANGIOX 250 mg, powder for concentrate for solution for injection or infusion by the intravenous route
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 29 April 2009 ANGIOX 250 mg, powder for concentrate for solution for injection or infusion by the intravenous route
Acute coronary syndrome (ACS) is an
 is an") OVERVIEW OF MEDICAL MANAGEMENT OF ACUTE CORONARY SYNDROMES Robert B. Parker, PharmD * Acute coronary syndrome (ACS) is an umbrella term used to describe any group of symptoms of acute myocardial ischemia
OVERVIEW OF MEDICAL MANAGEMENT OF ACUTE CORONARY SYNDROMES Robert B. Parker, PharmD * Acute coronary syndrome (ACS) is an umbrella term used to describe any group of symptoms of acute myocardial ischemia
Optimal antithrombotic therapy:
 Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
Percutaneous coronary intervention (PCI), in
, in") ECONOMIC IMPLICATIONS OF THE USE OF DIRECT THROMBIN INHIBITORS IN PERCUTANEOUS CORONARY INTERVENTION David J. Cohen, MD, MSc * ABSTRACT More than 1.2 million percutaneous coronary intervention (PCI) procedures
ECONOMIC IMPLICATIONS OF THE USE OF DIRECT THROMBIN INHIBITORS IN PERCUTANEOUS CORONARY INTERVENTION David J. Cohen, MD, MSc * ABSTRACT More than 1.2 million percutaneous coronary intervention (PCI) procedures
Early Management of Acute Coronary Syndrome
 Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company
 SMC No. (638/10) The Medicines Company") bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company 06 August 2010 The Scottish Medicines Consortium (SMC) has completed its
bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company 06 August 2010 The Scottish Medicines Consortium (SMC) has completed its
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
COAGULATION, BLEEDING, AND TRANSFUSION IN URGENT AND EMERGENCY CORONARY SURGERY
 COAGULATION, BLEEDING, AND TRANSFUSION IN URGENT AND EMERGENCY CORONARY SURGERY VALTER CASATI, M.D. DIVISION OF CARDIOVASCULAR ANESTHESIA AND INTENSIVE CARE CLINICA S. GAUDENZIO NOVARA (ITALY) ANTIPLATELET
COAGULATION, BLEEDING, AND TRANSFUSION IN URGENT AND EMERGENCY CORONARY SURGERY VALTER CASATI, M.D. DIVISION OF CARDIOVASCULAR ANESTHESIA AND INTENSIVE CARE CLINICA S. GAUDENZIO NOVARA (ITALY) ANTIPLATELET
STEMI: Newer Aspects in Pharmacological Treatment
 CHAPTER 14 STEMI: Newer Aspects in Pharmacological Treatment P. C. Manoria, Pankaj Manoria Introduction ST elevation myocardial infarction (STEMI) commonly results from disruption of a vulnerable plaque
CHAPTER 14 STEMI: Newer Aspects in Pharmacological Treatment P. C. Manoria, Pankaj Manoria Introduction ST elevation myocardial infarction (STEMI) commonly results from disruption of a vulnerable plaque
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department
: Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department") ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Treatment Strategies for the Prevention of Ischemic Complications in Patients Undergoing Percutaneous Coronary Intervention with Stent Placement
 Treatment Strategies for the Prevention of Ischemic Complications in Patients Undergoing Percutaneous Coronary Intervention with Stent Placement Pharmaceutical Care Project Outcomes Literature Evaluation
Treatment Strategies for the Prevention of Ischemic Complications in Patients Undergoing Percutaneous Coronary Intervention with Stent Placement Pharmaceutical Care Project Outcomes Literature Evaluation
Quinn Capers, IV, MD
 Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
C.R.E.D.O. Multicenter Multinational (USA, Canada) Prospective Randomized Double Blind Placebo Controlled Trial
 Prospective Randomized Double Blind Placebo Controlled Trial") Clopidogrel for the Reduction of Events During Observation Multicenter Multinational (USA, Canada) Prospective Randomized Double Blind Placebo Controlled Trial From Steinhubl et al, JAMA 2002;228:2411-20
Clopidogrel for the Reduction of Events During Observation Multicenter Multinational (USA, Canada) Prospective Randomized Double Blind Placebo Controlled Trial From Steinhubl et al, JAMA 2002;228:2411-20
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Index. Hematol Oncol Clin N Am 19 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Hematol Oncol Clin N Am 19 (2005) 203 208 Index Note: Page numbers of article titles are in boldface type. A Abciximab, as an antiplatelet agent, 93 94 Acute coronary syndromes, use of antiplatelet drugs
Hematol Oncol Clin N Am 19 (2005) 203 208 Index Note: Page numbers of article titles are in boldface type. A Abciximab, as an antiplatelet agent, 93 94 Acute coronary syndromes, use of antiplatelet drugs
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Anticoagulation therapy in acute coronary syndromes according to current guidelines
 Acute management of ACS Anticoagulation therapy in acute coronary syndromes according to current guidelines Marcin Grabowski, Marcin Leszczyk, Andrzej Cacko, Krzysztof J. Filipiak, Grzegorz Opolski 1 st
Acute management of ACS Anticoagulation therapy in acute coronary syndromes according to current guidelines Marcin Grabowski, Marcin Leszczyk, Andrzej Cacko, Krzysztof J. Filipiak, Grzegorz Opolski 1 st
Primary PCI in patients with STEMI Abbott Vascular. All rights reserved.
 Primary PCI in patients with STEMI Primary PCI in patients with STEMI Agenda 2 Primary PCI in patients with STEMI Definition: angioplasty ± stenting without prior or concomitant fibrinolytic therapy Objectives
Primary PCI in patients with STEMI Primary PCI in patients with STEMI Agenda 2 Primary PCI in patients with STEMI Definition: angioplasty ± stenting without prior or concomitant fibrinolytic therapy Objectives
Oral Anticoagulant Drugs
 Oral Anticoagulant Drugs Spoiled sweet clover caused hemorrhage in cattle(1930s). Substance identified as bishydroxycoumarin. Initially used as rodenticides, still very effective, more than strychnine.
Oral Anticoagulant Drugs Spoiled sweet clover caused hemorrhage in cattle(1930s). Substance identified as bishydroxycoumarin. Initially used as rodenticides, still very effective, more than strychnine.
ST-Elevation MI: Update on Bivalirudin and DES
 ST-Elevation MI: Update on Bivalirudin and DES George D. Dangas, MD, FACC, FSCAI, FAHA Professor of Medicine Director, Cardiovascular Innovation Mount Sinai Medical Center, New York, NY Disclosure Research
ST-Elevation MI: Update on Bivalirudin and DES George D. Dangas, MD, FACC, FSCAI, FAHA Professor of Medicine Director, Cardiovascular Innovation Mount Sinai Medical Center, New York, NY Disclosure Research
Chapter 15 Glycoprotein IIb/IIIa Antagonists
 Chapter 15 Glycoprotein IIb/IIIa Antagonists Introduction - GP IIb/IIIa receptors - Pharmacologic approaches - Preparations and dosages Mechanism of Action Clinical Efficacy - UA / NSTEMI - STEMI - PCI
Chapter 15 Glycoprotein IIb/IIIa Antagonists Introduction - GP IIb/IIIa receptors - Pharmacologic approaches - Preparations and dosages Mechanism of Action Clinical Efficacy - UA / NSTEMI - STEMI - PCI
Mortality from ST-segment elevated acute
 Choosing Pharmacotherapy for Primary PCI in Acute Myocardial Infarction A review of the agents and strategies commonly used during percutaneous intervention for ST-segment elevated myocardial infarction.
Choosing Pharmacotherapy for Primary PCI in Acute Myocardial Infarction A review of the agents and strategies commonly used during percutaneous intervention for ST-segment elevated myocardial infarction.
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Bivalirudin Clinical Trials Update Evidence and Future Perspectives
 Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Is Cangrelor hype or hope in STEMI primary PCI?
 Is Cangrelor hype or hope in STEMI primary PCI? ARUN KALYANASUNDARAM MD, MPH, FSCAI HOPE Issues with platelet inhibition in STEMI Delayed onset In acute settings, achieving the expected antiplatelet effect
Is Cangrelor hype or hope in STEMI primary PCI? ARUN KALYANASUNDARAM MD, MPH, FSCAI HOPE Issues with platelet inhibition in STEMI Delayed onset In acute settings, achieving the expected antiplatelet effect
Management of Acute Coronary Syndromes
 Management of Acute Coronary Syndromes Objectives 1. To outline the approach in managing a patient who presents with an acute coronary syndrome focusing on anti- thrombotic agents. Jenny Chiu, BScPhm,
Management of Acute Coronary Syndromes Objectives 1. To outline the approach in managing a patient who presents with an acute coronary syndrome focusing on anti- thrombotic agents. Jenny Chiu, BScPhm,
From STEMIs to Stents: Updates in PCI practice
 From STEMIs to Stents: Updates in PCI practice Arnold Seto, MD, MPA Assistant Clinical Professor, UC-Irvine and Long Beach VA Director of Interventional Cardiology Research Hospitalizations in the U.S.
From STEMIs to Stents: Updates in PCI practice Arnold Seto, MD, MPA Assistant Clinical Professor, UC-Irvine and Long Beach VA Director of Interventional Cardiology Research Hospitalizations in the U.S.
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN
 What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI
 HORIZONS-AMI: A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg W. Stone
HORIZONS-AMI: A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg W. Stone
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI. ISAR-REACT 4 Trial
 Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI ISAR-REACT 4 Trial Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität, Munich, Germany On behalf of F.-J.
Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI ISAR-REACT 4 Trial Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität, Munich, Germany On behalf of F.-J.
DRUGS USED IN COAGULATION DISORDERS
 DRUGS USED IN COAGULATION DISORDERS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 1, 2010 Materials on: Exam #6 Required reading: Katzung, Chapter 34 1 DISORDERS OF COAGULATION
DRUGS USED IN COAGULATION DISORDERS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 1, 2010 Materials on: Exam #6 Required reading: Katzung, Chapter 34 1 DISORDERS OF COAGULATION
In recent years, an increasing number of anticoagulants
 Anticoagulation Strategies for Patients Undergoing Percutaneous Coronary Intervention: Unfractionated Heparin, Low-Molecular-Weight Heparins, and Direct Thrombin Inhibitors Spyros Kokolis, Erdal Cavusoglu,
Anticoagulation Strategies for Patients Undergoing Percutaneous Coronary Intervention: Unfractionated Heparin, Low-Molecular-Weight Heparins, and Direct Thrombin Inhibitors Spyros Kokolis, Erdal Cavusoglu,
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Blood Thinner Agent. Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy
 Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Antiplatelet therapy and Coronary Interventions. Georgios I. Papaioannou, MD Hartford Hospital Grand Rounds 4/22/2003
 Antiplatelet therapy and Coronary Interventions Georgios I. Papaioannou, MD Hartford Hospital Grand Rounds 4/22/2003 Objectives Pharmacology of GP IIb/IIIa inhibitors and Monitoring of Platelet Inhibition
Antiplatelet therapy and Coronary Interventions Georgios I. Papaioannou, MD Hartford Hospital Grand Rounds 4/22/2003 Objectives Pharmacology of GP IIb/IIIa inhibitors and Monitoring of Platelet Inhibition
Update on the management of STEMI. Elliot Rapaport, M.D. San Francisco, CA December 14, 2007
 Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Manual of Interventional Cardiology
 782 PLATELET GLYCOPROTEIN IIb/IIIa RECEPTOR ANTAGONISTS (Tables 34.15, 34.16) Activation of the platelet glycoprotein (GP) IIb/IIIa receptor complex constitutes the final common pathway for platelet aggregation,
782 PLATELET GLYCOPROTEIN IIb/IIIa RECEPTOR ANTAGONISTS (Tables 34.15, 34.16) Activation of the platelet glycoprotein (GP) IIb/IIIa receptor complex constitutes the final common pathway for platelet aggregation,
Journal of the American College of Cardiology Vol. 51, No. 18, by the American College of Cardiology Foundation ISSN /08/$34.
 Journal of the American College of Cardiology Vol. 51, No. 18, 2008 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.12.052
Journal of the American College of Cardiology Vol. 51, No. 18, 2008 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.12.052
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
The Myth of Class Effect Antithrombotics Christopher Cannon, MD
 The Myth of Class Effect Antithrombotics Christopher Cannon, MD Cardiovascular Division Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Senior Investigator, TIMI Study
The Myth of Class Effect Antithrombotics Christopher Cannon, MD Cardiovascular Division Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Senior Investigator, TIMI Study
Journal of the American College of Cardiology Vol. 52, No. 22, by the American College of Cardiology Foundation ISSN /08/$34.
 Journal of the American College of Cardiology Vol. 52, No. 22, 2008 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2008.08.021
Journal of the American College of Cardiology Vol. 52, No. 22, 2008 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2008.08.021
Acute Coronary Syndromes: Selective vs Early Invasive Strategies
 Acute Coronary Syndromes: Selective vs Early Invasive Strategies WilliamE.Boden,MD,FACCandVipulGupta,MBBS,MPH Division of Cardiovascular Medicine, University at Buffalo Schools of Medicine and Public Health,
Acute Coronary Syndromes: Selective vs Early Invasive Strategies WilliamE.Boden,MD,FACCandVipulGupta,MBBS,MPH Division of Cardiovascular Medicine, University at Buffalo Schools of Medicine and Public Health,
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anti-thrombotic management in interventional cardiology
 Chapter 8 Anti-thrombotic management in interventional cardiology James Tcheng, Steve Kindsvater Introduction Since the dawn of the interventional age, the need for anti-thrombotic therapy during percutaneous
Chapter 8 Anti-thrombotic management in interventional cardiology James Tcheng, Steve Kindsvater Introduction Since the dawn of the interventional age, the need for anti-thrombotic therapy during percutaneous
Prevention of Coronary Stent Thrombosis and Restenosis
 Prevention of Coronary Stent Thrombosis and Restenosis Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea 9/12/03 Coronary
Prevention of Coronary Stent Thrombosis and Restenosis Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea 9/12/03 Coronary
Antiplatelet Therapy. Briain Mac Neill
 Antiplatelet Therapy Briain Mac Neill Galway University Hospital & National University of Ireland Galway Milestones in ACS Management Anti-Thrombin Rx Heparin LMWH Bivalirudin Anti-Platelet Rx Aspirin
Antiplatelet Therapy Briain Mac Neill Galway University Hospital & National University of Ireland Galway Milestones in ACS Management Anti-Thrombin Rx Heparin LMWH Bivalirudin Anti-Platelet Rx Aspirin
Horizon Scanning Centre November 2012
 Horizon Scanning Centre November 2012 Cangrelor to reduce platelet aggregation and thrombosis in patients undergoing percutaneous coronary intervention99 SUMMARY NIHR HSC ID: 2424 This briefing is based
Horizon Scanning Centre November 2012 Cangrelor to reduce platelet aggregation and thrombosis in patients undergoing percutaneous coronary intervention99 SUMMARY NIHR HSC ID: 2424 This briefing is based
Do We Need Platelet Function Assays?
 Do We Need Platelet Function Assays? Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic, La Jolla, CA The Antiplatelet Effect of Clopidogrel Varies Widely Among Individuals
Do We Need Platelet Function Assays? Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic, La Jolla, CA The Antiplatelet Effect of Clopidogrel Varies Widely Among Individuals
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Platelet glycoprotein IIb/IIIa inhibition in acute coronary syndromes
 European Heart Journal (00) 3, 1441 1448 doi:10.1053/euhj.00.3160, available online at http://www.idealibrary.com on Platelet glycoprotein IIb/IIIa inhibition in acute coronary syndromes Gradient of benefit
European Heart Journal (00) 3, 1441 1448 doi:10.1053/euhj.00.3160, available online at http://www.idealibrary.com on Platelet glycoprotein IIb/IIIa inhibition in acute coronary syndromes Gradient of benefit
Thrombosis. Jeffrey Jhang, M.D.
 Thrombosis Jeffrey Jhang, M.D. Introduction The human hemostatic system has evolved to maintain blood flow under normal physiologic conditions while remaining primed to rapidly respond to vascular injury
Thrombosis Jeffrey Jhang, M.D. Introduction The human hemostatic system has evolved to maintain blood flow under normal physiologic conditions while remaining primed to rapidly respond to vascular injury
Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis Alaide Chieffo
 Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis 11.45-12.07 Alaide Chieffo San Raffaele Scientific Institute, Milan, Italy Historical Perspective 25 20 15 10 5 0 Serruys 1991
Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis 11.45-12.07 Alaide Chieffo San Raffaele Scientific Institute, Milan, Italy Historical Perspective 25 20 15 10 5 0 Serruys 1991
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib!
 Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib! Roxana Mehran, MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Research support
Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib! Roxana Mehran, MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Research support
Defining the Optimal Activated Clotting Time During Percutaneous Coronary Intervention
 Defining the Optimal Activated Clotting Time During Percutaneous Coronary Intervention Aggregate Results From 6 Randomized, Controlled Trials Derek P. Chew, MBBS; Deepak L. Bhatt, MD; A. Michael Lincoff,
Defining the Optimal Activated Clotting Time During Percutaneous Coronary Intervention Aggregate Results From 6 Randomized, Controlled Trials Derek P. Chew, MBBS; Deepak L. Bhatt, MD; A. Michael Lincoff,