Secondary hyperparathyroidism in dialysis patients
|
|
|
- Rosemary Hudson
- 6 years ago
- Views:
Transcription
1 Secondary hyperparathyroidism in dialysis patients ( a critical approach of pharmacological treatments) Dominique JOLY Néphrologie Hôpital NECKER, Paris
2 DFG Finn WF. J Am Soc Nephrol. 24;15:271A.
3 Ca ++ Phosphates Calcitriol Ca SR? VDR VDR PTH
4 Ca ++ Phosphates Calcitriol Ca SR? VDR VDR PTH Secretion Synthesis Number of cells Hyperplasia Nodules
5 Ca ++ Phosphates Calcitriol Ca SR? VDR VDR PTH Secretion Synthesis Number of cells Hyperplasia Nodules
6 PTH High turnover Low turnover PTH
7 Low turnover PTH Target PTH : 15-3 pg/ml PTH High turnover

8 Low turnover PTH Target PTH : 15-3 pg/ml PTH High turnover Barreto KI. 28;73:771
9 Low turnover PTH Target PTH : 15-3 pg/ml PTH High turnover Fracture-free survival PTH > < 65 (mois) Coco & Rush, AJKD 2;36:1115
10 High turnover PTH Target PTH : 15-3 pg/ml Low turnover PTH
11 Low turnover PTH Target PTH : 15-3 pg/ml PTH High turnover PO -- 4 Ca ++ PO Ca ++ Ca x P elevated
12 Mortality 1.8 * RR of death * * * 1..8 * * *.6. < > * 2. * RR of death * * * < > 9. RR of death *.8.6. < Block J Am Soc Nephrol. 24;15:
13 Mortality 1.8 * RR of death * * * 1..8 * * * < > 11. * Ca RR of death * * * * < > 9. PTH 8 Ph PTHi RR of death * < Block J Am Soc Nephrol. 24;15:
14 Calcifications
15 Calcifications




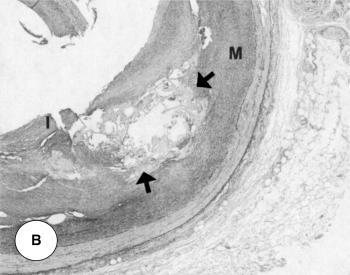
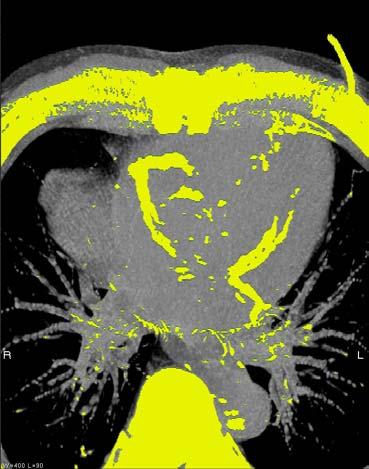
16 Calcifications CAC score (EBCT)
17 CAC Score of dialysis patients
18 CAC Score of dialysis patients (1) Elevated 2,5 2, 1,5 1, 5 Contro l Coronary artery disease On Dialysis Ag e Braun et al. AJKD. 1996;27:
19 CAC Score of dialysis patients (1) Elevated 2,5 2, 1,5 1, 5 Contro l Coronary artery disease On Dialysis Ag e Braun et al. AJKD. 1996;27: Blacher et al. Hypertension. 21;38:938. London et al. NDT 23;18:1731. (2) Predicts mortality SURVIVAL Calcification score: Calcification score: 1 Calcification score: 2 Calcification score: 3.25 Calcification score: mois
20 CAC Score of dialysis patients (3) Increased by hyperca ++ - phosphatemia Braun et al. AJKD. 1996;27: Blacher et al. Hypertension. 21;38:938. London et al. NDT 23;18:1731. Chertow et al. NDT. 24;19: Coronaire (P =.1) s Ph< 5.5 Aorte (P =.16) Ph 5.5 mg/dl
21 CAC Score of dialysis patients (3) Increased by hyperca ++ - phosphatemia Braun et al. AJKD. 1996;27: Blacher et al. Hypertension. 21;38:938. London et al. NDT 23;18:1731. Chertow et al. NDT. 24;19: Block GA et al, KI 25;68: Coronaire (P =.1) s Ph< 5.5 (4) Modified by treatments T Calciu msevelame r 6 m 12 m 18 m Aorte (P =.16) Ph 5.5 mg/dl
22 CAC Score of dialysis patients (3) Increased by hyperca ++ - phosphatemia Braun et al. AJKD. 1996;27: Blacher et al. Hypertension. 21;38:938. London et al. NDT 23;18:1731. Chertow et al. NDT. 24;19: Block GA et al, KI 25;68: Coronaire (P =.1) s Ph< 5.5 (4) Modified by treatments T Calciu msevelame r 6 m 12 m 18 m Aorte (P =.16) Ph 5.5 mg/dl VITAMIN D CINACALCET CONTROL
23 Ca x P Calcifications Mortalite «There is a link» Moe S et al, KI 26;69:

24 Ca x P Calcifications Mortalite «There is a link» Moe S et al, KI 26;69: «Causality?»
25 Ca x P Calcifications Mortalite «There is a link» Moe S et al, KI 26;69: «Causality?» «Intervention studies are necessary» Vitamin D Calcimimetic agents Phosphate binders
 doxercalciferol (Hectorol, 1-αOH-D2) 3 generation : paricalcitol (Zemplar, 19-Nor-1-α-25 (OH) 2")
26 1. Vitamin D Stock (calciferol, ergocalciferol) sun, food 1 generation: calcitriol (1, 25-(OH) 2 -D3) 2 generation : alfacalcidol (1-α OH-D3) doxercalciferol (Hectorol, 1-αOH-D2) 3 generation : paricalcitol (Zemplar, 19-Nor-1-α-25 (OH) 2 -D2) other
27 Calcitriol VDR VDR PTH Synthesis ipth P Ca Ca x P New vitamin D Calcitriol/ Alfacalcidol
28 Do 3 generation vitamins D have a «better biological profile»? (prospective randomized study)
29 Do 3 generation vitamins D have a «better biological profile»? (prospective randomized study) PTH (pg/ml) Calcitriol (n = 133) 1 Paricalcitol (n = 13) % of patients: > 5% reduction of PTH Paricalcitol : quicker Paricalcitol : fewer hypercalcemia / Ca x P w Sprague Kidney Int. 23;63:
30 Are 2 /3 generation vitamin D associated with a better survival in HD patients? (historical cohorts, retrospective, observation of 2-3y mortality, multivariate adjusted)
31 Are 2 /3 generation vitamin D associated with a better survival in HD patients? (historical cohorts, retrospective, observation of 2-3y mortality, multivariate adjusted) HD (prevalent) survival : paricalcitol > calcitriol Paricalcitol => mortality -16 % (,79-,9) Teng, NEJM 23; 349:446-56
 67 399 HD (prevalent) survival : paricalcitol > calcitriol Paricalcitol => mortality -16 %")
32 Are 2 /3 generation vitamin D associated with a better survival in HD patients? (historical cohorts, retrospective, observation of 2-3y mortality, multivariate adjusted) HD (prevalent) survival : paricalcitol > calcitriol Paricalcitol => mortality -16 % (,79-,9) Teng, NEJM 23; 349: HD (incident) survival: «no differences» Tentori, KI 26; 7:
33 Vitamine D use is associated with a reduced all-cause mortality (historical cohorts, retrospective, observation of 2-3y mortality, multivariate adjusted)
34 Vitamine D use is associated with a reduced all-cause mortality (historical cohorts, retrospective, observation of 2-3y mortality, multivariate adjusted) Teng M et al, JASN HD (prevalent) under vitamin D (IV calcitriol or paricalcitol) no vitamine D HR Death =.8 ( ) Tentori, KI 26; 7: HD (incident) 46,9 % no vitamin D (calcitriol or paricalcitol) HR Death =.8 (.7-.9) Melamed, KI 26; 7: HD/DP (incident) HR Death =.74 (.56-1)
35 Vitamine D use is associated with a reduced all-cause mortality (historical cohorts, retrospective, observation of 2-3y mortality, multivariate adjusted) Teng M et al, JASN HD (prevalent) under vitamin D (IV calcitriol or paricalcitol) no vitamine D HR Death =.8 ( ) Tentori, KI 26; 7: HD (incident) 46,9 % no vitamin D (calcitriol or paricalcitol) HR Death =.8 (.7-.9) Melamed, KI 26; 7: HD/DP (incident) HR Death =.74 (.56-1) vitamin D
36 Does vitamin D use explain «better survival of HD black patients?» (prospective cohort of incident HD, 1 y mortality observation, multivariate adjustement) n Mortality (1 y) PTH (pg/ml) 25 OH (ng/ml) Vitamin D active Dose/TT White % ,2 71%,6 µg Black % ,2 88 % 1 µg Black - Hispanic White
37 Does vitamin D use explain «better survival of HD black patients?» (prospective cohort of incident HD, 1 y mortality observation, multivariate adjustement) n Mortality (1 y) PTH (pg/ml) 25 OH (ng/ml) Vitamin D active Dose/TT White % ,2 71%,6 µg Black % ,2 88 % 1 µg Black - Hispanic White
 n Mortality (1 y) PTH (pg/ml) 25 OH (ng/ml) Vitamin D active Dose/TT")
38 Does vitamin D use explain «better survival of HD black patients?» (prospective cohort of incident HD, 1 y mortality observation, multivariate adjustement) n Mortality (1 y) PTH (pg/ml) 25 OH (ng/ml) Vitamin D active Dose/TT White % ,2 71%,6 µg Black % ,2 88 % 1 µg black patients on active VD blancs
39 Vitamin D Pleiotropic effects VDR is ubiquitary Vitamin D deficiency is associated with extra-skeletal complications Insulin-resistance, Diabetes HTA, SRAA Activation, cardiac failure, stroke Cancer (prostate, colon, breast) Wang, circulation 27; 117:53
40 Vitamin D Pleiotropic effects VDR is ubiquitary Vitamin D deficiency is associated with extra-skeletal complications Insulin-resistance, Diabetes HTA, SRAA Activation, cardiac failure, stroke Cancer (prostate, colon, breast) Wang, circulation 27; 117:53 VDR and diabetic nephropathy Progression Zhang, KI 28; 73:163 Glycemia Proteinuria VDR -/- Glomerulosclérosis VDR +/+
41 Vitamin D Ongoing studies OBSERVATION INTERVENTION Native Active VD and Myopathy in HD patients
42 2. Calcimimetic agents Small organic compounds that are administered orally Act as allosteric activators rather than ligands to the CaSR Increase sensitivity of the CaSR to extracellular Ca ions Suppress PTH secretion without elevating serum calcium and phosphorus levels
43 Calcimimetic agents Cinacalcet [Ca 2+ ] Ca SR PTH Secretion Synthesis Number of cells Hyperplasia
44 Calcimimetic agents Cinacalcet [Ca 2+ ] Increase calcium sensitivity 1 Control Cinacalcet Ca SR Serum PTH (% of maximum) Secretion PTH Synthesis Number of cells Hyperplasia Serum ionized calcium (mm) de Francisco, NDT 23 AVRIL 28
45 Calcimimetic agents Cinacalcet [Ca 2+ ] Increase calcium sensitivity 1 Control Cinacalcet Ca SR Serum PTH (% of maximum) Secretion PTH Synthesis Number of cells Hyperplasia Serum ionized calcium (mm) ipth P Ca Ca x P de Francisco, NDT 23 AVRIL 28 Cinacalcet
46 Calcimimetic agents Placebo Cinacalcet Biological Effects PTH KDOQI Target B Week Calcium KDOQI Target B Week Phosphate 65 6 Ca x P KDOQI Target B Week 45 4 KDOQI Target B Week Moe SM, et al. Kidney Int. 25;67:
47 Calcimimetic agents Clinical Effects Changes in relative risk (%)* PTX Fracture -54 Hospitalization CV -39 Mortality Cunningham J et al, KI 25;68:1793-8
48 Calcimimetic agents Clinical Effects Changes in relative risk (%)* PTX Fracture -54 Hospitalization CV -39 Mortality Cunningham J et al, KI 25;68:1793-8
49 Calcimimetic agents Clinical Effects Changes in relative risk (%)* PTX Fracture -54 Hospitalization CV -39 Mortality Cunningham J et al, KI 25;68:1793-8
50 Calcimimetic agents Clinical Effects Changes in relative risk (%)* PTX Fracture -54 Hospitalization CV -39 Mortality -19 DNS Cunningham J et al, KI 25;68:1793-8
51 Calcimimetic agents Clinical Effects Meta-analysis 8 studies comparing cinacalcet vs placebo n = 1429 patients End of treatment values of PTH, Ca, Ph are lower with calcimimetics No significant effects on patient-based endpoints were demonstrated Benefits of calcimimetics remain uncertain until futher RCT become available Strippoli AJKD 26;47:715
52 Calcimimetic agents Clinical Effects IN PROGRESS EVOLVE (Evaluation of Cinacalcet to Lower Clinical Events)
53 Calcimimetic agents Clinical Effects IN PROGRESS EVOLVE (Evaluation of Cinacalcet to Lower Clinical Events) Prevalent HD N=19 PTH > 3 Ca > 2.1 mm N=19 Ca x P > 3.6 mm 2 Placebo ± P binders ± vit D Cinacalcet ± P binders ± vit D
54 Calcimimetic agents Clinical Effects IN PROGRESS EVOLVE (Evaluation of Cinacalcet to Lower Clinical Events) Prevalent HD N=19 PTH > 3 Ca > 2.1 mm N=19 Ca x P > 3.6 mm 2 Placebo ± P binders ± vit D Titration : PTH 15-3 End : 1882 events (± 2.5 years) Death MI/ ACS Pulm oedema Stroke Cinacalcet ± P binders ± vit D
55 Calcimimetic agents Clinical Effects IN PROGRESS EVOLVE (Evaluation of Cinacalcet to Lower Clinical Events) Prevalent HD N=19 PTH > 3 Ca > 2.1 mm N=19 Ca x P > 3.6 mm 2 Placebo ± P binders ± vit D Titration : PTH 15-3 End : 1882 events (± 2.5 years) Cinacalcet ± P binders ± vit D Death MI/ ACS Pulm oedema Stroke %?
56 Calcimimetic agents Clinical Effects While EVOLVE results are awaited I personnaly use calcimimetic agents in selected patients
57 Calcimimetic agents Clinical Effects While EVOLVE results are awaited I personnaly use calcimimetic agents in selected patients M PTH 15 Ca x P > 1 mg 2 /dl 2 Zerbi et al. JCEM


58 Calcimimetic agents Clinical Effects While EVOLVE results are awaited I personnaly use calcimimetic agents in selected patients M Cinacalcet 3-6 mg/j M6 PTH 15 Ca x P > 1 mg 2 /dl Zerbi et al. JCEM

59 3. Phosphorus Hennig Bland (1669) The Discovery of Phosphorus Joseph Wright

60 Phosphate? PTH HD patients General Population 2.2 Risque relatif de décès < > 9. Block JASN 24;15: Dhingra Arch Intern Med 27;167:
61 Phosphate balance in HD patients Intake 1.2 g/kg => 1 mg P Absorption 6% => 42 mg P/w Dialysis Extraction => 8 mg x 3/w Accumulation => 2 mg P /day
62 Phosphate balance in HD patients Intake 1.2 g/kg => 1 mg P Absorption 6% => 42 mg P/w Dialysis Extraction => 8 mg x 3/w Accumulation => 2 mg P /day Diet appropriate diet prevents l hyperparathyroïdism Slatopolski et al, JCI :492

63 Phosphate balance in HD patients Intake 1.2 g/kg => 1 mg P Absorption 6% => 42 mg P/w Dialysis Extraction => 8 mg x 3/w Accumulation => 2 mg P /day Diet Phosphate Binders appropriate diet prevents l hyperparathyroïdism Calcium (carbonate / acetate) Résines Sevelamer Lanthanum Slatopolski et al, JCI :492
64 Phosphate binders Serum P (mg/dl) Ca * Ca *** Sevelamer * Lanthanum ** 5.5 K/DOQI Weeks * TTG: Chertow GM. KI 22 ** Hutchison WCN 3. Berlin *** Qunibi W. Kidney Int : 1914
65 Phosphate binders «CARE Study» The Calcium Acetate Renagel Evaluation Qunibi W. Kidney Int : 1914
66 Phosphate binders «CARE Study» The Calcium Acetate Renagel Evaluation n = 1 HD Double blind 8 weeks Titration : P<5.5 Phosphate Ca x P P < 5.5 mg/dl Calcium Acetate OR = 2.37 CaP < 55 mg 2 /dl 2 Calcium Acetate OR = 2.16 Calcium Hypercalcémie Calcium Acetate OR = 6.1 Qunibi W. Kidney Int : 1914
67 Phosphate binders «CARE Study» The Calcium Acetate Renagel Evaluation n = 1 HD Double blind 8 weeks Titration : P<5.5 PTH DNS HCO3- P <,1 Tolerance DNS
68 Phosphate binders «CARE Study» The Calcium Acetate Renagel Evaluation n = 1 HD Double blind 8 weeks Titration : P<5.5 Calcium Acetate 732 $ Sevelamer 4283 $ «superior efficacy» «in occasional patients»
69 Phosphate binders Treat to Goal 2 prevalent HD Calcium Acetate Calcium Carbonate International Prospective Randomized Open 52 weeks Sevelamer Primary endpoint : Ca x P difference between binders Chertow, et al. KI :
70 Phosphate binders Treat to Goal 2 prevalent HD Calcium Acetate Calcium Carbonate International Prospective Randomized Open 52 weeks Sevelamer Primary endpoint : Ca x P difference between binders Results Primary endpoint not met (no difference between binders) Some secondary endpoints show differences: 1 hypercalcemic episode PTH suppression LDL cholesterol Aorta calcification at 52 weeks Chertow, et al. KI :
71 Phosphate binders Treat to Goal Progression of calcifications Median Percent Change Sevalame r Calcium binders 1 % Aort a Week % Week 52 5 % 28% * Chertow, et al. KI :
72 Phosphate binders Treat to Goal Progression of calcifications «calcium calcifies» Median Percent Change Sevalame r Calcium binders 1 % Aort a Week % Week 52 5 % 28% * Chertow, et al. KI :
73 Phosphate binders Treat to Goal Progression of calcifications «calcium calcifies» Median Percent Change Sevalame r Calcium binders 1 % Aort a Week % Week 52 5 % 28% * «not so sure» In the SEVELAMER group, 1) Calcium intake was probably important in the dialysate as nighttime supplements 2) LDLc was lower Chertow, et al. KI :
74 Phosphate binders Treat to Goal Sevelamer (n=99) Final Calcium (n=11) Final P Phosphorus mg/dl Calcium mg/dl Hypercalcemia % Ca P mg2/dl2 Intact PTH pg/ml LDL-C mg/dl 5.1 ± ±.7 16% 49 ± ± <.1 Chertow, et al. KI :
75 Phosphate binders CARE -2 Calcium Acetate /Sevelamer Evaluation Study 2 23 PREVALENT HD Calcium Acetate USA Prospective Randomized Open 52 weeks Sevelamer Ph mg/dl LDLc <.7 g/l (± atorvastatin)
76 Phosphate binders CARE -2 Calcium Acetate /Sevelamer Evaluation Study 2 23 PREVALENT HD Calcium Acetate USA Prospective Randomized Open 52 weeks Sevelamer Ph mg/dl LDLc <.7 g/l (± atorvastatin) Primary endpoint : CAC score (ECBT at 1 year) Hypothesis : no différence in CAC score progression
77 Phosphate binders CARE -2 Calcium Acetate /Sevelamer Evaluation Study 2 23 PREVALENT HD Calcium Acetate USA Prospective Randomized Open 52 weeks Sevelamer 3 3 % 29% Ph mg/dl LDLc <.7 g/l (± atorvastatin) Median % Change AJKD 28 in press Sevalamer Calcium binders 5 Week 52
78 Phosphate binders RIND study Renagel In New Dialysis Block GA et al, KI 27;71:
79 Phosphate binders RIND study Renagel In New Dialysis 129 INCIDENTS HD Calcium Acetate Calcium Carbonate International Prospective Randomised Open 44 weeks Sevelamer Endpoints: 1) Mortality Block GA et al, KI 27;71:
80 Phosphate binders RIND study Renagel In New Dialysis 129 INCIDENTS HD Calcium Acetate Calcium Carbonate International Prospective Randomised Open 44 weeks Renagel Endpoints: 1) Mortality Crude : 1.6/1 vs 5.3/1 (P=.5) Adjusted : HR 3.1 (p=.16) Block GA et al, KI 27;71:
81 Phosphate binders RIND study Renagel In New Dialysis 129 INCIDENTS HD Calcium Acetate Calcium Carbonate International Prospective Randomised Open 44 weeks Renagel Endpoints: 1) Mortality Crude : 1.6/1 vs 5.3/1 (P=.5) Adjusted : HR 3.1 (p=.16) Block GA et al, KI 27;71:
82 Phosphate binders DCOR «Dialysis Clinical Outcomes Revisited» 213 HD prévalents (75 centres, USA) Renagel (n=153) Calcium(n=15) Acetate 7% Carbonate 3% Suki et al. KI 27
83 Phosphate binders DCOR «Dialysis Clinical Outcomes Revisited» 213 HD prévalents Renagel (n=153) Calcium(n=15) (75 centres, USA) Acetate 7% Carbonate 3% Men 55% Black 47% Diabetes 5% HD vintage 3 y 6 y Suki et al. KI 27
84 Phosphate binders DCOR «Dialysis Clinical Outcomes Revisited» 213 HD prévalents Renagel (n=153) Calcium(n=15) (75 centres, USA) Acetate 7% Carbonate 3% Men 55% Black 47% Diabetes 5% HD vintage 3 y 6 y 45 months Mortality Power >8 % to detect a > 22% mortaliy réduction Suki et al. KI 27
85 Phosphate binders DCOR «Dialysis Clinical Outcomes Revisited» 213 HD prévalents Renagel (n=153) Calcium(n=15) (75 centres, USA) Acetate 7% Carbonate 3% Men 55% Black 47% Diabetes 5% HD vintage 3 y 6 y 45 months Mortality Power >8 % to detect a > 22% mortaliy réduction P <.1 Ca <.1 Ca x P DNS PTH <.1 LDLc <.1 Suki et al. KI 27
86 Phosphate binders DCOR All cause Mortality Cardiovascular Mortality Suki et al. KI 27
87 Phosphate binders DCOR STRATIFICATION : PATIENTS > 65 ans All cause Mortality Cardiovascular Mortality Suki et al. KI 27
88 Phosphate binders Systematic reviews
89 Phosphate binders Systematic reviews Experts opinions

 12.")
90 Phosphate binders Systematic reviews 2 -ANALYSIS AJKD 28 (March) 51 : 445 Experts opinions DCOR : many patients were lost to follow up Intention to treat analysis Using Medicare/Medicaid data Reported by Separate group of investigators Overall mortality DNS Cause specific mortality DNS Morbidity DNS Cause specific hospitalisation DNS First specific hospitalisation DNS Multiple hospitalisation rate 1.7 vs 1.9* Hospital days (patient/year) 12.3 vs 13.9 *


91 HPTX TREATMENTS Ca CLINICALLY RELEVANT RESULTS Morbidity Mortality Phos
92 HPTX TREATMENTS Ca CLINICALLY RELEVANT RESULTS Morbidity Mortality Phos Desappointing Absent Awaited To be confirmed Sevelamer Cinacalcet Vitamin D Lanthanum Nicotinic Acid Calcium / dialysate
( ) , (Donabedian, 1980) We would not choose any treatment with poor outcomes
 , (Donabedian, 1980) We would not choose any treatment with poor outcomes") ..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
New biological targets for CKD- MBD: From the KDOQI to the
 New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. E-mail : guillaume-jean-crat@wanadoo.fr
New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. E-mail : guillaume-jean-crat@wanadoo.fr
Therapeutic golas in the treatment of CKD-MBD
 Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Treatment Options for Chronic Kidney
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
2017 KDIGO Guidelines Update
 2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
Management of CKD. Goce Spasovski, R. Macedonia
 Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis
 Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis Seoung Woo Lee Div. Of Nephrology and Hypertension, Dept. of Internal Medicine, Inha Unv. College of Medicine, Inchon, Korea
Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis Seoung Woo Lee Div. Of Nephrology and Hypertension, Dept. of Internal Medicine, Inha Unv. College of Medicine, Inchon, Korea
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment
 Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Outline. The Role of Vitamin D in CKD. Essential Role of Vitamin D. Mechanism of Action of Vit D. Mechanism of Action of Vit D 7/16/2010
 Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
Month/Year of Review: September 2012 Date of Last Review: September 2010
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE ON MAINTENANCE DIALYSIS THERAPY
 UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Cinacalcet treatment in advanced CKD - is it justified?
 Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Benefits and Harms of Phosphate Binders in CKD: A Systematic Review of Randomized Controlled Trials
 Benefits and Harms of Phosphate Binders in CKD: A Systematic Review of Randomized Controlled Trials Sankar D. Navaneethan, MD, MPH, Suetonia C. Palmer, MBChB, Jonathan C. Craig, MBChB, PhD, Grahame J.
Benefits and Harms of Phosphate Binders in CKD: A Systematic Review of Randomized Controlled Trials Sankar D. Navaneethan, MD, MPH, Suetonia C. Palmer, MBChB, Jonathan C. Craig, MBChB, PhD, Grahame J.
02/27/2018. Objectives. To Replace or Not to Replace: Nutritional Vitamin D in Dialysis.
 To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
Treatment Options for Chronic Kidney. Goce Spasovski, R. Macedonia
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011 Session Objectives Definition of the problem of CKD-MBD
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011 Session Objectives Definition of the problem of CKD-MBD
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
TRANSPARENCY COMMITTEE OPINION. 22 July 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 22 July 2009 PHOSPHOSORB 660 mg, film-coated tablet Container of 200 (CIP: 381 466-0) Applicant: FRESENIUS MEDICAL
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 22 July 2009 PHOSPHOSORB 660 mg, film-coated tablet Container of 200 (CIP: 381 466-0) Applicant: FRESENIUS MEDICAL
Level 1 Strong We recommendyshould A High Moderate Level 2 Weak We suggestymight C Low Very low. K Hyperphosphatemia has been associated with poor
 chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
KDIGO. CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke
 CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke Unité 1088 de l Inserm UFR de Médecine et de Pharmacie Jules Verne University of Picardie Amiens, France Poten2al conflicts of interest Research support:
CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke Unité 1088 de l Inserm UFR de Médecine et de Pharmacie Jules Verne University of Picardie Amiens, France Poten2al conflicts of interest Research support:
The CARI Guidelines Caring for Australasians with Renal Impairment. Serum phosphate GUIDELINES
 Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Serum phosphate GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Serum phosphate GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015)
 Final Version (01/03/2015)") CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015) Dr Simon Steddon, Consultant Nephrologist, Guy s and St Thomas NHS Foundation Trust, London Dr Edward Sharples,
CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015) Dr Simon Steddon, Consultant Nephrologist, Guy s and St Thomas NHS Foundation Trust, London Dr Edward Sharples,
Cardiovascular Mortality: General Population vs ESRD Dialysis Patients
 Cardiovascular Mortality: General Population vs ESRD Dialysis Patients Annual CVD Mortality (%) 100 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age (years) GP Male GP Female GP Black GP
Cardiovascular Mortality: General Population vs ESRD Dialysis Patients Annual CVD Mortality (%) 100 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age (years) GP Male GP Female GP Black GP
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale. Maurizio Gallieni Università degli Studi di Milano
 Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Renal Association Clinical Practice Guideline in Mineral and Bone Disorders in CKD
 Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism
 CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism Pieter Evenepoel Nephrology, Dialysis, and Transplantation University Hospitals Leuven April 2017, FMC Herbeumont Disclosures Research support:
CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism Pieter Evenepoel Nephrology, Dialysis, and Transplantation University Hospitals Leuven April 2017, FMC Herbeumont Disclosures Research support:
Sensipar (cinacalcet)
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure
 Nephrol Dial Transplant (2002) 17: 340 345 The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure Naseem Amin Genzyme Corporation, Cambridge, MA,
Nephrol Dial Transplant (2002) 17: 340 345 The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure Naseem Amin Genzyme Corporation, Cambridge, MA,
Month/Year of Review: May 2014 Date of Last Review: September New Drug Evaluation: Sucrofferic Oxyhydroxide (Velphoro )
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Drugs for the treatment of secondary hyperparathyroidism and hyperphosphataemia
 NSW Therapeutic Advisory Group Level 5, 376 Victoria Street PO Box 766 Darlinghurst NSW 2010 Phone: 61 2 8382 2852 Fax: 61 2 8382 3529 Email: nswtag@stvincents.com.au www.nswtag.org.au Drugs for the treatment
NSW Therapeutic Advisory Group Level 5, 376 Victoria Street PO Box 766 Darlinghurst NSW 2010 Phone: 61 2 8382 2852 Fax: 61 2 8382 3529 Email: nswtag@stvincents.com.au www.nswtag.org.au Drugs for the treatment
Guidelines and new evidence on CKD - MBD treatment
 Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016
 Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 28 March 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 28 March 2012 OSVAREN 435 mg/235 mg, film-coated tablet Bottle of 180 (CIP: 382 886 3) Applicant: FRESENIUS MEDICAL
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 28 March 2012 OSVAREN 435 mg/235 mg, film-coated tablet Bottle of 180 (CIP: 382 886 3) Applicant: FRESENIUS MEDICAL
IMPLEMENTATION OF THE CKD-MBD PRACTICE. Goce Spasovski, R. Macedonia
 IMPLEMENTATION OF THE CKD-MBD GUIDELINES Introduction INTO CLINICAL to Renagel PRACTICE Goce Spasovski, R. Macedonia Antalya, Turkey, September 16 2012 Session Objectives Guidelines needs and controversy
IMPLEMENTATION OF THE CKD-MBD GUIDELINES Introduction INTO CLINICAL to Renagel PRACTICE Goce Spasovski, R. Macedonia Antalya, Turkey, September 16 2012 Session Objectives Guidelines needs and controversy
2.0 Synopsis. ABT-358 M Clinical Study Report R&D/06/099. (For National Authority Use Only) to Item of the Submission: Volume:
 to Item of the Submission: Volume:") 2.0 Synopsis Abbott Laboratories Name of Study Drug: Zemplar Injection Name of Active Ingredient: Paricalcitol Individual Study Table Referring to Item of the Submission: Volume: Page: (For National Authority
2.0 Synopsis Abbott Laboratories Name of Study Drug: Zemplar Injection Name of Active Ingredient: Paricalcitol Individual Study Table Referring to Item of the Submission: Volume: Page: (For National Authority
Protocol GTC : A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients.
 in Chronic Kidney Disease Patients.") Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
2.0 Synopsis. Paricalcitol Capsules M Clinical Study Report R&D/15/0380. (For National Authority Use Only)
") 2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls
 O. Mehls") Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls Division of Pediatric Nephrology University Hospital for Children and Adolescents Heidelberg, Germany Definition
Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls Division of Pediatric Nephrology University Hospital for Children and Adolescents Heidelberg, Germany Definition
Should cinacalcet be used in patients who are not on dialysis?
 Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416)
") Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi
 Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi Mario Cozzolino, MD, PhD, FERA Dipartimento di Scienze della Salute Università di Milano UO Nefrologia e Dialisi Laboratorio
Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi Mario Cozzolino, MD, PhD, FERA Dipartimento di Scienze della Salute Università di Milano UO Nefrologia e Dialisi Laboratorio
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience
 Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Contents. Authors Name: Christopher Wong: Consultant Nephrologist Anne Waddington: Renal Pharmacist Eimear Fegan : Renal Dietitian
 Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
The role of calcimimetics in chronic kidney disease
 http://www.kidney-international.org & 2006 International Society of Nephrology The role of calcimimetics in chronic kidney disease A Gal-Moscovici 1,2 and SM Sprague 1 1 Division of Nephrology and Hypertension,
http://www.kidney-international.org & 2006 International Society of Nephrology The role of calcimimetics in chronic kidney disease A Gal-Moscovici 1,2 and SM Sprague 1 1 Division of Nephrology and Hypertension,
Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis patients
 original article http://www.kidney-international.org & 2007 International Society of Nephrology Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis
original article http://www.kidney-international.org & 2007 International Society of Nephrology Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality
 Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD
pth: ein neuer Marker für CKD-MBD") Biomarker der kardio-renalen Achse Mannheim, 20. Januar 2017 Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD Prof. Dr. med. Thomas Bernd Dschietzig Immundiagnostik AG, Bensheim Med. Klinik m.
Biomarker der kardio-renalen Achse Mannheim, 20. Januar 2017 Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD Prof. Dr. med. Thomas Bernd Dschietzig Immundiagnostik AG, Bensheim Med. Klinik m.
Class Review: Vitamin D Analogs
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
FOCUS ON CARDIOVASCULAR DISEASE
 The Consequences of Vitamin D Deficiency: FOCUS ON CARDIOVASCULAR DISEASE Vitamin D deficiency is a global health problem. With all the medical advances of the century, vitamin D deficiency is still epidemic.
The Consequences of Vitamin D Deficiency: FOCUS ON CARDIOVASCULAR DISEASE Vitamin D deficiency is a global health problem. With all the medical advances of the century, vitamin D deficiency is still epidemic.
OPEN. Masahiro Yoshikawa 1,2, Osamu Takase 1,2, Taro Tsujimura
 www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
Kidney-Bone and Beyond: An Academic Career
 Kidney-Bone and Beyond: An Academic Career Isidro B. Salusky, M.D. Distinguished Professor of Pediatrics Chief, Division of Pediatric Nephrology Director, Clinical Translational Research Center Associate
Kidney-Bone and Beyond: An Academic Career Isidro B. Salusky, M.D. Distinguished Professor of Pediatrics Chief, Division of Pediatric Nephrology Director, Clinical Translational Research Center Associate
ABT-358 (Paricalcitol) M Clinical Study Report R&D/08/333
 M Clinical Study Report R&D/08/333") Subjects who satisfied all inclusion criteria and none of the exclusion criteria were eligible to enroll in this study and were assigned randomly in equal numbers to Sequence Group I or II. The sequences
Subjects who satisfied all inclusion criteria and none of the exclusion criteria were eligible to enroll in this study and were assigned randomly in equal numbers to Sequence Group I or II. The sequences
Vitamin D and Calcium Therapy: how much is enough
 Vitamin D and Calcium Therapy: how much is enough Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco DISCLOSURE Nothing to disclose 1 RECOMMENDATIONS
Vitamin D and Calcium Therapy: how much is enough Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco DISCLOSURE Nothing to disclose 1 RECOMMENDATIONS
2.0 Synopsis. ABT-358/Paricalcitol M Clinical Study Report R&D/09/1255. (For National Authority Use Only) to Part of Dossier: Volume:
 to Part of Dossier: Volume:") 2.0 Synopsis Title of Study: Late Phase II Study of Paricalcitol Injection Dose-response study of paricalcitol injection in chronic kidney disease subjects receiving hemodialysis with secondary hyperparathyroidism
2.0 Synopsis Title of Study: Late Phase II Study of Paricalcitol Injection Dose-response study of paricalcitol injection in chronic kidney disease subjects receiving hemodialysis with secondary hyperparathyroidism
The Endocrine Society Guidelines
 Vitamin D and Calcium Therapy: how much is enough DISCLOSURE Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco Nothing to disclose RECOMMENDATIONS
Vitamin D and Calcium Therapy: how much is enough DISCLOSURE Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco Nothing to disclose RECOMMENDATIONS
Phosphate binders and metabolic acidosis in patients undergoing maintenance hemodialysis sevelamer hydrochloride, calcium carbonate, and bixalomer
 Hemodialysis International 2015; 19:5459 Phosphate binders and metabolic acidosis in patients undergoing maintenance hemodialysis sevelamer hydrochloride, calcium carbonate, and bixalomer Toru SANAI, 1
Hemodialysis International 2015; 19:5459 Phosphate binders and metabolic acidosis in patients undergoing maintenance hemodialysis sevelamer hydrochloride, calcium carbonate, and bixalomer Toru SANAI, 1
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet:
 Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Secondary hyperparathyroidism in chronic kidney disease recent paradigm shift in clinical management
 Secondary hyperparathyroidism in chronic kidney disease recent paradigm shift in clinical management Complete this course and earn 1 CME POINT Dr. HO Chung Ping MBBS (HK), MRCP, FRCP (Glas, Edin), FHKCP,
Secondary hyperparathyroidism in chronic kidney disease recent paradigm shift in clinical management Complete this course and earn 1 CME POINT Dr. HO Chung Ping MBBS (HK), MRCP, FRCP (Glas, Edin), FHKCP,
New Medicines Profile. December 2013 Issue No. 13/04. Colestilan
 New Medicines Profile December 2013 Issue. 13/04 Concise evaluated information to support the managed entry of new medicines in the NHS Summary (BindRen ) is an oral, non-absorbed, non-calcium, nonmetallic
New Medicines Profile December 2013 Issue. 13/04 Concise evaluated information to support the managed entry of new medicines in the NHS Summary (BindRen ) is an oral, non-absorbed, non-calcium, nonmetallic
Original epidemiologic studies 1 have suggested that approximately
 Factors for Increased Morbidity and Mortality in Uremia: Hyperphosphatemia Nathan W. Levin, Frank A. Gotch, and Martin K. Kuhlmann Hyperphosphatemia is a metabolic abnormality present in the majority of
Factors for Increased Morbidity and Mortality in Uremia: Hyperphosphatemia Nathan W. Levin, Frank A. Gotch, and Martin K. Kuhlmann Hyperphosphatemia is a metabolic abnormality present in the majority of
The hart and bone in concert
 The hart and bone in concert Piotr Rozentryt III Department of Cardiology, Silesian Centre for Heart Disease, Silesian Medical University, Zabrze, Poland Disclosure Research grant, speaker`s fee, travel
The hart and bone in concert Piotr Rozentryt III Department of Cardiology, Silesian Centre for Heart Disease, Silesian Medical University, Zabrze, Poland Disclosure Research grant, speaker`s fee, travel
Sensipar. Sensipar (cinacalcet) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Cinacalcet hydrochloride for the treatment of secondary hyperparathyroidism Responses to consultee and commentators on
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Cinacalcet hydrochloride for the treatment of secondary hyperparathyroidism Responses to consultee and commentators on
CKD-Mineral Bone Disorder (MBD) Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire
 Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire") Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW
 NEW PRODUCT SLIDESHOW") Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW Introduction Brand name: Parsabiv Generic name: Etelcalcetide Pharmacological class: Calcimimetic Strength and Formulation: 2.5mg/0.5mL, 5mg/mL, 10mg/2mL;
Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW Introduction Brand name: Parsabiv Generic name: Etelcalcetide Pharmacological class: Calcimimetic Strength and Formulation: 2.5mg/0.5mL, 5mg/mL, 10mg/2mL;
Opinion 23 April 2014
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 23 April 2014 MIMPARA 30 mg, film-coated tablet B/14 (CIP: 365 154 8) B/28 (CIP: 365 155 4) B/30 (CIP: 365 157 7)
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 23 April 2014 MIMPARA 30 mg, film-coated tablet B/14 (CIP: 365 154 8) B/28 (CIP: 365 155 4) B/30 (CIP: 365 157 7)
Clinical Guideline Bone chemistry management in adult renal patients on dialysis
 Clinical Guideline Bone chemistry management in adult renal patients on dialysis This guidance covers how to: Maintain serum phosphate 0.8 to 1.7mmol/L 1 Maintain serum corrected calcium 2.1 to 2.5mmol/L
Clinical Guideline Bone chemistry management in adult renal patients on dialysis This guidance covers how to: Maintain serum phosphate 0.8 to 1.7mmol/L 1 Maintain serum corrected calcium 2.1 to 2.5mmol/L
Hyperphosphatemia is associated with a
 TREATMENT OPTIONS IN THE MANAGEMENT OF PHOSPHATE RETENTION * George A. Porter, MD, FACP, and Hartmut H. Malluche, MD, FACP ABSTRACT Hyperphosphatemia is an independent risk factor for mortality and cardiovascular
TREATMENT OPTIONS IN THE MANAGEMENT OF PHOSPHATE RETENTION * George A. Porter, MD, FACP, and Hartmut H. Malluche, MD, FACP ABSTRACT Hyperphosphatemia is an independent risk factor for mortality and cardiovascular
NDT Advance Access published February 3, 2007
 NDT Advance Access published February 3, 2007 Nephrol Dial Transplant (2007) 1 of 6 doi:10.1093/ndt/gfl840 Original Article Implementation of K/DOQI Clinical Practice Guidelines for Bone Metabolism and
NDT Advance Access published February 3, 2007 Nephrol Dial Transplant (2007) 1 of 6 doi:10.1093/ndt/gfl840 Original Article Implementation of K/DOQI Clinical Practice Guidelines for Bone Metabolism and
BONE AND MINERAL METABOLISM in the PD PATIENT
 BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
APPLYING KDIGO GUIDELINES TO
 Knowledge Exchange 2016 APPLYING KDIGO GUIDELINES TO CLINICAL PRACTICE MARKUS KETTELER, MD, FELLOW OF THE EUROPEAN RENAL ASSOCIATION DIVISION OF NEPHROLOGY, KLINIKUM COBURG COBURG, GERMANY Date of preparalon:
Knowledge Exchange 2016 APPLYING KDIGO GUIDELINES TO CLINICAL PRACTICE MARKUS KETTELER, MD, FELLOW OF THE EUROPEAN RENAL ASSOCIATION DIVISION OF NEPHROLOGY, KLINIKUM COBURG COBURG, GERMANY Date of preparalon:
Achievement of recommended treatment targets for bone and mineral metabolism in haemodialysis patients using paricalcitol: An observational study
 Achievement of recommended treatment targets for bone and mineral metabolism in haemodialysis patients using paricalcitol: An observational study Fernstrom, Anders; Giaever, Jan; Granroth, Barbara; Hylander,
Achievement of recommended treatment targets for bone and mineral metabolism in haemodialysis patients using paricalcitol: An observational study Fernstrom, Anders; Giaever, Jan; Granroth, Barbara; Hylander,
Parathyroid Hormone, Calcium and Phosphorus Levels in Hemodialysis Patients at Al-Shifa Hospital, Gaza-Palestine
 IUG Journal of Natural and Engineering Studies Vol.22,No.1, pp 97-110 2014, ISSN 1726-6807, http://www.iugaza.edu.ps/ar/periodical/ Parathyroid Hormone, Calcium and Phosphorus Levels in Hemodialysis Patients
IUG Journal of Natural and Engineering Studies Vol.22,No.1, pp 97-110 2014, ISSN 1726-6807, http://www.iugaza.edu.ps/ar/periodical/ Parathyroid Hormone, Calcium and Phosphorus Levels in Hemodialysis Patients
Determinants of coronary artery calcification in maintenance hemodialysis patients
 1 Determinants of coronary artery calcification in maintenance hemodialysis patients Yoshiko Nishizawa, MD 1,2, Sonoo Mizuiri, MD, PhD 2, Noriaki Yorioka, MD, PhD 3, Chieko Hamada MD, PhD 1,Yasuhiko Tomino
1 Determinants of coronary artery calcification in maintenance hemodialysis patients Yoshiko Nishizawa, MD 1,2, Sonoo Mizuiri, MD, PhD 2, Noriaki Yorioka, MD, PhD 3, Chieko Hamada MD, PhD 1,Yasuhiko Tomino
Long-term effect of cinacalcet hydrochloride on abdominal aortic calcification in patients on hemodialysis with secondary hyperparathyroidism
 Long-term effect of cinacalcet hydrochloride on abdominal aortic calcification in patients on hemodialysis with secondary hyperparathyroidism Kazunori Nakayama 1, 2, Kazushi Nakao 1, 2, Yuji Takatori 1,
Long-term effect of cinacalcet hydrochloride on abdominal aortic calcification in patients on hemodialysis with secondary hyperparathyroidism Kazunori Nakayama 1, 2, Kazushi Nakao 1, 2, Yuji Takatori 1,
A Randomised Clinical Study of Alfacalcidol and Paricalcitol
 PHD THESIS DANISH MEDICAL JOURNAL A Randomised Clinical Study of Alfacalcidol and Paricalcitol Two vitamin D analogs for treatment of secondary hyperparathyroidism in chronic hemodialysis patients Ditte
PHD THESIS DANISH MEDICAL JOURNAL A Randomised Clinical Study of Alfacalcidol and Paricalcitol Two vitamin D analogs for treatment of secondary hyperparathyroidism in chronic hemodialysis patients Ditte
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Treatment of hyperphosphatemia in hemodialysis patients: The Calcium Acetate Renagel Evaluation (CARE Study)
") Kidney International, Vol. 65 (2004), pp. 1914 1926 Treatment of hyperphosphatemia in hemodialysis patients: The Calcium Acetate Renagel Evaluation (CARE Study) WAJEH Y. QUNIBI,ROBERT E. HOOTKINS,LAVETA
Kidney International, Vol. 65 (2004), pp. 1914 1926 Treatment of hyperphosphatemia in hemodialysis patients: The Calcium Acetate Renagel Evaluation (CARE Study) WAJEH Y. QUNIBI,ROBERT E. HOOTKINS,LAVETA
Corporate Presentation January 2013
 Corporate Presentation January 2013 0 Forward-Looking Statements Certain statements and information included in this presentation are forwardlooking statements under the Private Securities Litigation Reform
Corporate Presentation January 2013 0 Forward-Looking Statements Certain statements and information included in this presentation are forwardlooking statements under the Private Securities Litigation Reform
Vitamin D. Vitamin functioning as hormone. Todd A Fearer, MD FACP
 Vitamin D Vitamin functioning as hormone Todd A Fearer, MD FACP Vitamin overview Vitamins are organic compounds that are essential in small amounts for normal metabolism They are different from minerals
Vitamin D Vitamin functioning as hormone Todd A Fearer, MD FACP Vitamin overview Vitamins are organic compounds that are essential in small amounts for normal metabolism They are different from minerals
Nephrology Subcommittee of PTAC Meeting held 2 December 2014
 Nephrology Subcommittee of PTAC Meeting held 2 December 2014 (minutes for web publishing) Nephrology Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology and
Nephrology Subcommittee of PTAC Meeting held 2 December 2014 (minutes for web publishing) Nephrology Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology and
CKD and CVD. Jamal Salameh, MD, FACP, FASN First Coast Nephrology
 CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
REVIEW. KEYWORDS 1αOH-vitamin D derivatives, calcimimetics, chronic kidney disease, hyperparathyroidism, oral phosphate binders
 Reappraisal of 2003 NKF-K/DOQI guidelines for management of hyperparathyroidism in chronic kidney disease patients Matthieu Monge, Irina Shahapuni, Roxana Oprisiu, Najeh El Esper, Philippe Morinière, Ziad
Reappraisal of 2003 NKF-K/DOQI guidelines for management of hyperparathyroidism in chronic kidney disease patients Matthieu Monge, Irina Shahapuni, Roxana Oprisiu, Najeh El Esper, Philippe Morinière, Ziad
Hemodialysis: slightly beyond basics Dialysate calcium and magnesium concentrations
 Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Original Article. Introduction
 Nephrol Dial Transplant (2006) 21: 1663 1668 doi:10.1093/ndt/gfl006 Advance Access publication 6 February 2006 Original Article Application of NKF-K/DOQI Clinical Practice Guidelines for Bone Metabolism
Nephrol Dial Transplant (2006) 21: 1663 1668 doi:10.1093/ndt/gfl006 Advance Access publication 6 February 2006 Original Article Application of NKF-K/DOQI Clinical Practice Guidelines for Bone Metabolism
Posttransplant Bone Disease. Budapest 2007
 Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
J.Bacchetta has documented that she has received grants for research activities from Amgen, Crinex, Sandoz.
 J.Bacchetta has documented that she has received grants for research activities from Amgen, Crinex, Sandoz. Epidemiological, immune and metabolic aspects of vitamin D in CKD Justine Bacchetta, MD, PhD
J.Bacchetta has documented that she has received grants for research activities from Amgen, Crinex, Sandoz. Epidemiological, immune and metabolic aspects of vitamin D in CKD Justine Bacchetta, MD, PhD
Disclosures. Topics. Staging and GFR. K-DOQI Staging of Chronic Kidney Disease. Definition of Chronic Kidney Disease. Chronic Kidney Disease
 Disclosures Chronic Kidney Disease Consultant: Baxter Healthcare J. Kevin Tucker, M.D. Brigham and Women s Hospital Massachusetts General Hospital Topics Staging of chronic kidney disease (CKD) How to
Disclosures Chronic Kidney Disease Consultant: Baxter Healthcare J. Kevin Tucker, M.D. Brigham and Women s Hospital Massachusetts General Hospital Topics Staging of chronic kidney disease (CKD) How to
A new era in phosphate binder therapy: What are the options?
 http://www.kidney-international.org & 2006 International Society of Nephrology A new era in phosphate binder therapy: What are the options? IB Salusky 1 1 Department of Pediatrics, David Geffen School
http://www.kidney-international.org & 2006 International Society of Nephrology A new era in phosphate binder therapy: What are the options? IB Salusky 1 1 Department of Pediatrics, David Geffen School
Title:Hyperphosphatemia as an Independent Risk Factor of Coronary Artery Calcification Progression in Peritoneal Dialysis Patients
 Author's response to reviews Title:Hyperphosphatemia as an Independent Risk Factor of Coronary Artery Calcification Progression in Peritoneal Dialysis Patients Authors: Da Shang (sdshangda@163.com) Qionghong
Author's response to reviews Title:Hyperphosphatemia as an Independent Risk Factor of Coronary Artery Calcification Progression in Peritoneal Dialysis Patients Authors: Da Shang (sdshangda@163.com) Qionghong
Malnutrition and Role of Nutrition in BMD:CKD
 Malnutrition and Role of Nutrition in BMD:CKD PNDS Continuing Nutrition Education Seminar Saturday, 30 th November 2013 Fayza Khan MSC (Foods and Nutrition) R.D President,PNDS Outline Objective Malnutrition
Malnutrition and Role of Nutrition in BMD:CKD PNDS Continuing Nutrition Education Seminar Saturday, 30 th November 2013 Fayza Khan MSC (Foods and Nutrition) R.D President,PNDS Outline Objective Malnutrition
Metabolic Bone Disease (Past, Present and Future Challenges in the Management)
") Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical