CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism
|
|
|
- Morgan Marshall
- 5 years ago
- Views:
Transcription


1 CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism Pieter Evenepoel Nephrology, Dialysis, and Transplantation University Hospitals Leuven April 2017, FMC Herbeumont
2 Disclosures Research support: Amgen, Tecomedical, Diasorin Advisory Board/Consulting: Sanofi, Amgen, Shire Speakers bureau: Amgen, VIFOR Fresenius

3 CKD-MBD
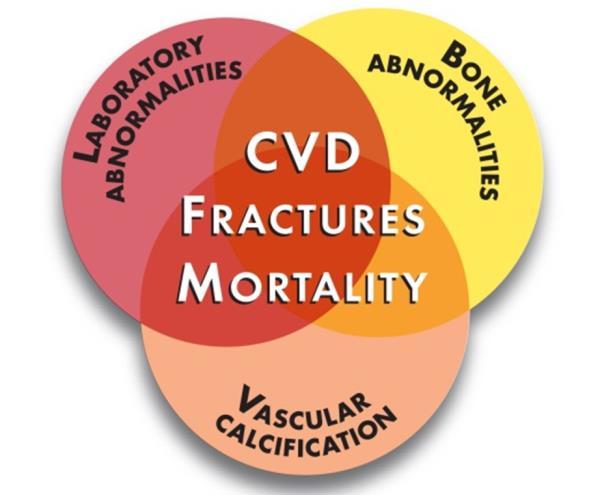
4 CKD-MBD - Calcium - Phosphorus - 1,25(OH)2D Lab - FGF-23 Abnormalities - Alkaline phosphatase Secondary HPT Bone Disease Abnormal bone morphology - Turnover - Mineralization - Volume - Linear growth - Strength FRACTURES Vascular Calcification Vascular calcification Soft-tissue calcification Arterial stiffness FGF-23 = fibroblast growth factor-23. Kidney Disease: Improving Global Outcomes (KDIGO) CKD MBD Work Group. Kidney Int. 2009;76 (Suppl 113):S1 S130. MORTALITY
5 Secondary hyperparathyroidism Epidemiology Pathogenesis Consequences Treatment options Challenges
6 Secondary hyperparathyroidism Epidemiology Pathogenesis Consequences Treatment options Challenges
, at time of Tx: n=518 Parathyroidectomy")
7 PTH: temporal trends in Flanders Flanders, Renal transplant recipients ( ), at time of Tx: n=518 Parathyroidectomy (%)

8 PTH: temporal trends in the world phase 1, ; phase 2, ; phase 3, ; phase 4, ; phase 5, Tentori F et al. CJASN 2015;10:98-109
9 Parathyroidectomy rate (per 1000 patient years) PTX: temporal trends in the world phase 1, ; phase 2, ; phase 3, ; phase 4, ; phase 5, PTX rate shows a declining trend: Less stringent PTH target range Increased uses of acitve Vitamin D/Cinacalcet Francesca Tentori et al. CJASN 2015;10:98-109
10 Secondary hyperparathyroidism Epidemiology Pathogenesis Consequences Treatment options Challenges
11 Pathogenesis of shpt: evolving concepts 2000 calcium-centric paradigm adapted from Isakova and Wolf Kidney Int 2010

12 Pathogenesis of shpt: evolving concepts FGF23 increases precede PTH Chronic Renal Insufficiency Cohort (CRIC), n=3879, CKD stage 2-4 Prevalence rates Cubic spline functions Isakova et al. Kidney Int 2011 Evenepoel et al. CJASN 2010
13 Pathogenesis of shpt: evolving concepts calcium-centric paradigm phosphate-centric paradigm adapted from Isakova and Wolf Kidney Int 2010
14 Pathogenesis of shpt: evolving concepts PTH increases precede FGF23 and calcitriol changes SKIPOGH study, n=1128, general population, Switserland Dhayat et al. Kidney Int 2016
, at time of Tx: n=518 USA, HD, ArMORR, n=825 France, Renal transplant recipients (2004-2006), at time of Tx: n=143 11 ± 10 pg/ml 9.")
15 Pathogenesis of shpt: evolving concepts shpt is universal despite normal active vitamin D levels Flanders, Renal transplant recipients ( ), at time of Tx: n=518 USA, HD, ArMORR, n=825 France, Renal transplant recipients ( ), at time of Tx: n= ± 10 pg/ml 9.3 ± 8.9 pg/ml
16 Vitamin D metabolism in CKD Seatle Kidney Study Decreased production Decreased catabolism Bosworth et al. Kidney Int 2012 CKD is a state of stagnant Vitamin D metabolism


17 Pathogenesis of shpt: evolving concepts ? adapted from Isakova and Wolf Kidney Int 2010
18 Secondary hyperparathyroidism Pathogenesis Epidemiology Consequences Treatment options Challenges
")
19 PTH and bone phenotype(s)

20 Fracture risk in CKD RR Fracture risk CKD1-2 CKD3 CKD4-5 CKD5D Tx Yr1 Yr10 Nickolas et al. JASN 2006; Jadoul et al. Kidney Int 2006; Alem et al. Kidney Int 2000; Chen et al. Osteoporosis int 2014 Vautour et al. Osteop Int 2004; Abbott et al. Ann Epidemiol 2001; Ball et al. JAMA 2002
21 PTH & fractures in CKD Author Population Size Main finding(s) Stehman-Breen et al. KI 2000 Coco et al. AJKD 2000 Fishbane et al. CJASN 2016 CKD5D, USRDS ( ) NO association between PTH and hip fracture CKD5D ( ) Low PTH (<195 pg/ml) associates with hip fractures CKD5D FMC ( ) Low PTH (and Ca) associates with hip and femur fractures Jadoul et al. KI 2006 CKD5D (HD) DOPPS ( ) High PTH (>900 pg/ml) associates with incident (all) fractures Goldmith et al. AJKD 2009 CKD5D Systematic review High PTH ( >900 pg/ml RR 1,7) associates with fractures Perin et al. AJT 2013 Danese et al. AJKD 2006 Atusumi et al. AJKD 1999 CKD-T 143 High PTH associates with fractures CKD5D, DMMS ( ) U-shaped relationship between PTH and (hip/vertebral/pelvic) fractures CKD5D 178 U-shaped relationship between PTH and fractures, with low PTH significantly associated with vertebral fractures

22 PTH & fractures in CKD 5 Fishbane et al. CJASN 2016
 is a Major Risk Factor for Fractures in the 5 Years After Kidney Transplantation (n=143) Giannini et al. JBMR 2010 Perrin et al. AJT 2013")
23 PTH & fractures in CKD-T High PTH levels are associated with an increased vertebral fracture risk in RTRs (n=125) Persistent Hyperparathyroidism (PTH > 130 ng/l at 3 months) is a Major Risk Factor for Fractures in the 5 Years After Kidney Transplantation (n=143) Giannini et al. JBMR 2010 Perrin et al. AJT 2013




24 Pathophysiology Low PTH High PTH Low bone turnover High bone turnover Microstructural abnormalities Low cancellous bone volume Reduced trabecular thickness Reduced toughness Bone Quality Fracture Material and nanomechanical abnormalities (low mineral-to-matrix ratio) Malluche et al. JASN 2012; Ng et al. JBMR 2015; Moorthi and Moe Kidney Int 2013

25 Thoughness The toughness of bone is at least partly related to the ability of its microstructure to dissipate deformation energy without propagation of the crack

26 PTH and vascular phenotype(s)

 Temmar et al.")

27 Vascular calcification progression in CKD controversy Fox et al. KI 2004 (Framingham Heart Study) Budoff et al. AJKD 2011 (CRIC) Temmar et al. J Hypertension 2010 Russo et al. KI 2007 Shroff et al. Circulation 2008 Evenepoel et al. JCEM 2015 CKD1-2 CKD3 CKD4-5 CKD5D Tx Yr1 Yr10
 levels greater than 450 pg/ml. Malluche et al.")
28 PTH & calcification progression Higher CAC progression in patients with parathyroid hormone (PTH) levels greater than 450 pg/ml. Malluche et al. JASN 2015 (epub)
29 PTH & mortality Francesca Tentori et al. CJASN 2015;10:98-109
30 Outcome PTH and outcomes: summary KDIGO KDOQI PTH (X UNL) PTH (ng/ml)

31 Secondary hyperparathyroidism Epidemiology Pathogenesis Consequences Treatment options Challenges
 data Pharmaco-economical aspects (bundled payment plans, reimbursement")
32 ? Which target? Commercial influences RCTs Observational (conflicting) data Pharmaco-economical aspects (bundled payment plans, reimbursement restrictions..) Guidelines Which PTH level to target? Soomo and Goldfarb CJASN 2015 Tentori et al. CJASN 2015
33 How? Suppress PTH Calcimimetics Vitamin D(analogs) Parathyroidectomy PTH Systemic Toxicity Ca PTH Bone Disease Control Calcium Control intake Adjust dialysate calcium Use calcium supplements or vitamin D therapy Vit D P Increase Vitamin D Levels Nutritional/active VitD Lower Elevated Serum Phosphate Control dietary intake (additives!) Use phosphate binders a Treatment approach = vitamin D + phosphate binders used as first-line therapy; cinacalcet used later in the course of therapy. Tomasello S. Diabetes Spectrum. 2008;21:19-25
34 How?
35 How? Suppress PTH Calcimimetics Vitamin D(analogs) Parathyroidectomy PTH Systemic Toxicity Ca PTH Bone Disease Control Calcium Control intake Adjust dialysate calcium Use calcium supplements or vitamin D therapy Vit D P Increase Vitamin D Levels Nutritional/active VitD Lower Elevated Serum Phosphate Control dietary intake (additives!) Use phosphate binders a Treatment approach = vitamin D + phosphate binders used as first-line therapy; cinacalcet used later in the course of therapy. Tomasello S. Diabetes Spectrum. 2008;21:19-25

36 Calcimimetics Ca ++ Parathyroid Gland Chief Cell CaSR AMG 416 Cinacalcet Cinacalcet 1,2 Calcimimetic Small organic molecule; molecular weight = g/mol Interacts with membrane-spanning segments of CaSR and enhances signal transduction, thereby reducing PTH secretion AMG 416 3,4,8 Calcimimetic Synthetic 7-amino acid peptide linked to L-cysteine; molecular weight = g/mol Peptide agonist of the CaSR that interacts with and activates the receptor thereby reducing PTH secretion G Proteins Daily oral IV at the end of dialysis Increased Intracellular Signaling Cartoon representation. Nucleus IV = intravenous; CaSR = calcium-sensing receptor; Da = Dalton; ESRD = end-stage renal disease; PTH = parathyroid hormone Regulation and Decreased Secretion of PTH 1. Cinacalcet product label. 2. Goodman WG. Adv Ren Replace Ther. 2002;9: Cunningham J, et al. Presented at the 52 nd ERA-EDTA Congress; May 2015; London, UK (Data on file, Amgen). 4. Chen P, et al. J Clin Pharmacol. 2015;55: Goodman WG, et al. Kidney Int. 2008;74: Moallem E, et al. J Biol Chem. 1998;273: Brown EM. Rev Endocr Metab Disord. 2000;1: Walter S, et al., J Pharmacol Exp Ther. 2013;346: Reactive Use Only. Do not copy or distribute.
37 Etelecalcetide (AMG416): pharmacokinetics Martin K et al. Kidney Int 2014
38 Cinacalcet and CKD-MBD Block et al. NEJM 2004 BONAFIDE Behets et al. Kidney Int 2015 EVOLVE Moe et al. Circulation Lab Abnormalities Bone Disease Secondary HPT FRACTURES ADVANCE Raggi et al. NDT 2011 Vascular Calcification EVOLVE Chertow et al. NEJM 2013 Moe et al. JASN 2015 MORTALITY
39 Etelcalcetide and CKD-MBD Block et al. JAMA 2017 Lab Abnormalities Bone Disease Secondary HPT FRACTURES Vascular Calcification MORTALITY
40 Head-to-Head Study: Etelcalcetide Vs Cinacalcet Study Design Screening (8 weeks) Randomization Etelcalcetide: Cinacalcet (N = 683) 1:1 TIW IV Etelcalcetide + Daily Oral Placebo (n = 340) Etelcalcetide starting dose was 5 mg and could be increased at Weeks 5, 9, 13, and 17 to maximum dose of 15 mg Daily Oral Cinacalcet + TIW IV Placebo (n = 343) Cinacalcet starting dose was 30 mg and could be increased at Weeks 5, 9, 13, and 17 to maximum dose of 180 mg Follow-up 30 days Day 1 (first dose) Dose titration 16 weeks Maintenance 10 weeks 26 weeks (last dose) Target PTH was 100 and 300 pg/ml. No dose increase for ongoing AEs, cca < 8.3, or PTH < 300 pg/ml was observed. IP could not be increased after week 17. AE = adverse event; cca = corrected calcium; IP = investigational product; PTH = parathyroid hormone; TIW = thrice weekly. Martin KJ, et al. Poster Presented at the 2015 ASN Annual Meeting; November 3-8, 2015;San Diego, CA (# SA-PO1115) Block et al., JAMA. 2017;317(2): doi: /jama
 P, etelecalcetide vs. cinacalcet EAP was defined as weeks 20 27. EAP = efficacy assessment phase; PTH = parathyroid hormone.")
41 Head-to-Head Study: Etelcalcetide Vs Cinacalcet Etelcalcetide Was Superior to Cinacalcet in the Proportion of Patients With a > 30% Reduction From Baseline in Mean Serum PTH During the EAP P = Proportion of Patients With > 30% Mean PTH Reduction From Baseline (%) P, etelecalcetide vs. cinacalcet EAP was defined as weeks EAP = efficacy assessment phase; PTH = parathyroid hormone. (n = 198) (n = 232) 1. Martin KJ, et al. Abstract Presented at the 2015 ASN Annual Meeting; November 3-8, 2015;San Diego, CA. 2. Martin KJ, et al. Poster Presented at the 2015 ASN Annual Meeting; November 3-8, 2015;San Diego, CA (# SA-PO1115). Block et al., JAMA. 2017;317(2): doi: /jama
42 Mean cca (mg/dl) Head-to-Head Study: Etelcalcetide Vs Cinacalcet Mean cca Concentrations Over Time Treatment with etelcalcetide resulted in a greater reduction from baseline in mean cca compared to cinacalcet 10.0 Etelcalcetide Cinacalcet Baseline Study Week Etelcalcetide n = Cinacalcet n = cca = corrected calcium; IP = investigational product; SE = standard error. On-treatment approach: data collected on or prior to the last on-missing dose of IP were summarized by visit. Vertical lines represent SE. Martin KJ, et al. Poster Presented at the 2015 ASN Annual Meeting; November 3-8, 2015;San Diego, CA (# SA-PO1115). Block et al., JAMA. 2017;317(2): doi: /jama
 ( 42, 13) ( 76, 25) ( 50, 2) ( 57, 6) ( 87, 26) BSAP = bone-specific alkaline phosphatase; CTX = type 1")
43 Percent Change Head-to-Head Study: Etelcalcetide Vs Cinacalcet Changes in Biomarkers: FGF-23, BSAP, and CTX (Median Percent Change From Baseline to Week 27) Etelcalcetide was associated with greater reductions in FGF-23, BSAP, and CTX from baseline to week 27 compared with cinacalcet ( 40, 20) ( 42, 13) ( 76, 25) ( 50, 2) ( 57, 6) ( 87, 26) BSAP = bone-specific alkaline phosphatase; CTX = type 1 collagen C-telopeptide; FGF = fibroblast growth factor; SE = standard error. Martin KJ, et al. Poster Presented at the 2015 ASN Annual Meeting; November 3-8, 2015;San Diego, CA (# SA-PO1115). Block et al., JAMA. 2017;317(2): doi: /jama
44 Head-to-Head Study: Etelcalcetide Vs Cinacalcet Summary of Safety and Efficacy Treatment with etelcalcetide achieved a > 50% and a > 30% reduction in PTH in more patients compared to cinacalcet, while nausea and vomiting did not differ There was a numerical imbalance in cardiac failure, for which a causal relationship to etelcalcetide could not be established Hypocalcemia was seen more tine.velghe@skynet.be often with etelcalcetide IV etelcalcetide is more efficacious than oral cinacalcet for the treatment of SHPT in patients on hemodialysis AE = adverse event Martin KJ, et al. Poster Presented at the 2015 ASN Annual Meeting; November 3-8, 2015;San Diego, CA (# SA-PO1115). Block et al., JAMA. 2017;317(2): doi: /jama

 Use phosphate binders a Treatment approach = vitamin D + phosphate binders used as first-line therapy; cinacalcet used later in the")
45 Targeting PTH Suppress PTH Calcimimetics Vitamin D(analogs) Parathyroidectomy PTH Systemic Toxicity Ca PTH Bone Disease Control Calcium Control intake Adjust dialysate calcium Use calcium supplements or vitamin D therapy Vit D P Increase Vitamin D Levels Nutritional/active VitD Lower Elevated Serum Phosphate Control dietary intake (additives!) Use phosphate binders a Treatment approach = vitamin D + phosphate binders used as first-line therapy; cinacalcet used later in the course of therapy. Tomasello S. Diabetes Spectrum. 2008;21:19-25
46 Parathyroidectomy (PTX) and fractures Rudser et al. JASN 2007
47 Parathyroidectomy (PTX) and morbidity Event rates in the 1 year before and 1 year after parathyroidectomy. Areef Ishani et al. CJASN 2015;10:90-97
48 Secondary hyperparathyroidism Pathogenesis Epidemiology Consequences Treatment options Challenges Limitations of PTH as outcome biomarker and target of therapy Uncontrolled secondary hyperparathyroidism

49 Outcome PTH as outcome biomarker in CKD Complex Imprecise PTH Palmer et al. JAMA 2011
50 How to explain imprecise association? Biological variability of PTH Gardham et al. CJASN 2010 Cavalier et al. AJKD Variable PTH resistance PTH1R desensitization PTH1R dysfunction Evenepoel, Bover, Urena KI 2016
51 PTH as target of therapy is imperfect Meta-Analysis: Drug effects on serum PTH are weakly and imprecisely correlated with all-cause and cardiovascular death in the setting of CKD.PTH is unsuitable as indicator of drug efficacy. Palmer et al. AJKD 2015
52 FGF23 Of note, patients with a > 30% decline of FGF23 were characterized by significantly higher BAP levels, indicating higher bone turnover. Thus cinacalcet may confer highest benefit in patients with high BAP Moe et al. Circulation 2015
53 Secondary hyperparathyroidism Pathogenesis Epidemiology Consequences Treatment options Challenges Limitations of PTH as outcome biomarker and target of therapy Uncontrolled secondary hyperparathyroidism




54 Uncontrolled secondary hyperparathyroidism Therapeutic nihilism Non-adherence Low efficacy Side effects High cost
55 shpt 2017: trends and challenges Pathogenesis: remains incompletely understood; initial tigger? Epidemiology: PTH levels are on the rise Consequences: shpt in an integral component of CKD-MBD Treatment options: expanding armamentarium allows treatment choices Challenges: PTH as a biomarker is under siege; caution against therapeutic nihilism
56 shpt 2017: Opportunities Diagnosis-Monitoring Treatment PTH Cinacalcet? Biomarker (panel) Imaging Etelcalcetide Bone histomorphometry

57
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416)
") Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Cinacalcet treatment in advanced CKD - is it justified?
 Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Sensipar. Sensipar (cinacalcet) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
( ) , (Donabedian, 1980) We would not choose any treatment with poor outcomes
 , (Donabedian, 1980) We would not choose any treatment with poor outcomes") ..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW
 NEW PRODUCT SLIDESHOW") Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW Introduction Brand name: Parsabiv Generic name: Etelcalcetide Pharmacological class: Calcimimetic Strength and Formulation: 2.5mg/0.5mL, 5mg/mL, 10mg/2mL;
Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW Introduction Brand name: Parsabiv Generic name: Etelcalcetide Pharmacological class: Calcimimetic Strength and Formulation: 2.5mg/0.5mL, 5mg/mL, 10mg/2mL;
The Parsabiv Beginner s Book
 The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
KDIGO. CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke
 CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke Unité 1088 de l Inserm UFR de Médecine et de Pharmacie Jules Verne University of Picardie Amiens, France Poten2al conflicts of interest Research support:
CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke Unité 1088 de l Inserm UFR de Médecine et de Pharmacie Jules Verne University of Picardie Amiens, France Poten2al conflicts of interest Research support:
CKD-Mineral Bone Disorder (MBD) Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire
 Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire") Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE ON MAINTENANCE DIALYSIS THERAPY
 UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
02/27/2018. Objectives. To Replace or Not to Replace: Nutritional Vitamin D in Dialysis.
 To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1
 Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1 Not an actual Parsabiv vial. The displayed vial is for illustrative
Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1 Not an actual Parsabiv vial. The displayed vial is for illustrative
Secondary hyperparathyroidism in dialysis patients
 Secondary hyperparathyroidism in dialysis patients ( a critical approach of pharmacological treatments) Dominique JOLY Néphrologie Hôpital NECKER, Paris DFG Finn WF. J Am Soc Nephrol. 24;15:271A. Ca ++
Secondary hyperparathyroidism in dialysis patients ( a critical approach of pharmacological treatments) Dominique JOLY Néphrologie Hôpital NECKER, Paris DFG Finn WF. J Am Soc Nephrol. 24;15:271A. Ca ++
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
2017 KDIGO Guidelines Update
 2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Treatment Options for Chronic Kidney
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016
 Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Sensipar (cinacalcet)
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
New biological targets for CKD- MBD: From the KDOQI to the
 New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. E-mail : guillaume-jean-crat@wanadoo.fr
New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. E-mail : guillaume-jean-crat@wanadoo.fr
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Guidelines and new evidence on CKD - MBD treatment
 Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale. Maurizio Gallieni Università degli Studi di Milano
 Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Bone Disease after Kidney Transplantation
 Bone Disease after Kidney Transplantation BTS March 2018 Dr Arif Khwaja PhD, FRCP Sheffield Kidney Institute Clinical case 47 year old female FSGS DBD 2007 egfr 25mls/min. Sirolimus, Azathioprine and prednisolone
Bone Disease after Kidney Transplantation BTS March 2018 Dr Arif Khwaja PhD, FRCP Sheffield Kidney Institute Clinical case 47 year old female FSGS DBD 2007 egfr 25mls/min. Sirolimus, Azathioprine and prednisolone
Therapeutic golas in the treatment of CKD-MBD
 Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Renal Association Clinical Practice Guideline in Mineral and Bone Disorders in CKD
 Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Should cinacalcet be used in patients who are not on dialysis?
 Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
Outline. The Role of Vitamin D in CKD. Essential Role of Vitamin D. Mechanism of Action of Vit D. Mechanism of Action of Vit D 7/16/2010
 Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Swiss Summary of the Risk Management Plan (RMP) for Parsabiv (Etelcalcetide)
 for Parsabiv (Etelcalcetide)") Swiss Summary of the Risk Management Plan (RMP) for Parsabiv (Etelcalcetide) RMP Summary: Version 1, November 2017 EU RMP: Version 1.0, November 2016 Page 1 of 6 The Risk Management Plan (RMP) is a comprehensive
Swiss Summary of the Risk Management Plan (RMP) for Parsabiv (Etelcalcetide) RMP Summary: Version 1, November 2017 EU RMP: Version 1.0, November 2016 Page 1 of 6 The Risk Management Plan (RMP) is a comprehensive
Management of mineral and bone disorders in renal transplant recipients
 Nephrology 22, Suppl. 2 (2017) 65 69 Management of mineral and bone disorders in renal transplant recipients MATTHEW J DAMASIEWICZ 1,3 and PETER R EBELING 2,3,4 Departments of 1 Nephrology, and 2 Endocrinology,
Nephrology 22, Suppl. 2 (2017) 65 69 Management of mineral and bone disorders in renal transplant recipients MATTHEW J DAMASIEWICZ 1,3 and PETER R EBELING 2,3,4 Departments of 1 Nephrology, and 2 Endocrinology,
What Are the Targets in CKD-MBD?
 Knowledge Exchange 2016 Paris, France, September 30, 2016 Date of preparation: Nov 2016 Item job code: INTSP/C-ANPROM/FOS/16/0025 Cristina Ortiz Jorge B Cannata-Andía Bone and Mineral Research Unit Hospital
Knowledge Exchange 2016 Paris, France, September 30, 2016 Date of preparation: Nov 2016 Item job code: INTSP/C-ANPROM/FOS/16/0025 Cristina Ortiz Jorge B Cannata-Andía Bone and Mineral Research Unit Hospital
2.0 Synopsis. Paricalcitol Capsules M Clinical Study Report R&D/15/0380. (For National Authority Use Only)
") 2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD
pth: ein neuer Marker für CKD-MBD") Biomarker der kardio-renalen Achse Mannheim, 20. Januar 2017 Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD Prof. Dr. med. Thomas Bernd Dschietzig Immundiagnostik AG, Bensheim Med. Klinik m.
Biomarker der kardio-renalen Achse Mannheim, 20. Januar 2017 Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD Prof. Dr. med. Thomas Bernd Dschietzig Immundiagnostik AG, Bensheim Med. Klinik m.
Management of CKD. Goce Spasovski, R. Macedonia
 Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
chapter 1 & 2009 KDIGO
 http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment
 Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis
 Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis Seoung Woo Lee Div. Of Nephrology and Hypertension, Dept. of Internal Medicine, Inha Unv. College of Medicine, Inchon, Korea
Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis Seoung Woo Lee Div. Of Nephrology and Hypertension, Dept. of Internal Medicine, Inha Unv. College of Medicine, Inchon, Korea
Pediatric CKD-MBD: pathophysiology and management
 Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Treatment Options for Chronic Kidney. Goce Spasovski, R. Macedonia
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011 Session Objectives Definition of the problem of CKD-MBD
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011 Session Objectives Definition of the problem of CKD-MBD
Posttransplant Bone Disease. Budapest 2007
 Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
Bone Markers and Vascular Calcification in CKD-MBD
 Bone Markers and Vascular Calcification in CKD-MBD Pierre Delanaye, MD, PhD Department of Nephrology, Dialysis, Transplantation CHU Sart Tilman University of Liège BELGIUM Bone Markers and Vascular Calcification
Bone Markers and Vascular Calcification in CKD-MBD Pierre Delanaye, MD, PhD Department of Nephrology, Dialysis, Transplantation CHU Sart Tilman University of Liège BELGIUM Bone Markers and Vascular Calcification
Chapter 5: Evaluation and treatment of kidney transplant bone disease Kidney International (2009) 76 (Suppl 113), S100 S110; doi: /ki.2009.
 76 (Suppl 113), S100 S110; doi: /ki.2009.") http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015)
 Final Version (01/03/2015)") CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015) Dr Simon Steddon, Consultant Nephrologist, Guy s and St Thomas NHS Foundation Trust, London Dr Edward Sharples,
CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015) Dr Simon Steddon, Consultant Nephrologist, Guy s and St Thomas NHS Foundation Trust, London Dr Edward Sharples,
PARSABIV (etelcalcetide)
") PARSABIV (etelcalcetide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
PARSABIV (etelcalcetide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
APPLYING KDIGO GUIDELINES TO
 Knowledge Exchange 2016 APPLYING KDIGO GUIDELINES TO CLINICAL PRACTICE MARKUS KETTELER, MD, FELLOW OF THE EUROPEAN RENAL ASSOCIATION DIVISION OF NEPHROLOGY, KLINIKUM COBURG COBURG, GERMANY Date of preparalon:
Knowledge Exchange 2016 APPLYING KDIGO GUIDELINES TO CLINICAL PRACTICE MARKUS KETTELER, MD, FELLOW OF THE EUROPEAN RENAL ASSOCIATION DIVISION OF NEPHROLOGY, KLINIKUM COBURG COBURG, GERMANY Date of preparalon:
OPEN. Masahiro Yoshikawa 1,2, Osamu Takase 1,2, Taro Tsujimura
 www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
Kobe University Repository : Kernel
 Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
The CARI Guidelines Caring for Australasians with Renal Impairment. Serum phosphate GUIDELINES
 Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Serum phosphate GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Serum phosphate GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Research. JAMA Original Investigation. chronic kidney disease. parathyroid hormone (PTH) concentrations in patients receiving hemodialysis.
 concentrations in patients receiving hemodialysis.") Research JAMA Original Investigation Effect of vs on Serum Parathyroid Hormone in Patients Receiving Hemodialysis With Secondary Hyperparathyroidism Two Randomized Clinical Trials Geoffrey A. Block, MD;
Research JAMA Original Investigation Effect of vs on Serum Parathyroid Hormone in Patients Receiving Hemodialysis With Secondary Hyperparathyroidism Two Randomized Clinical Trials Geoffrey A. Block, MD;
Hemodialysis: slightly beyond basics Dialysate calcium and magnesium concentrations
 Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Contents. Authors Name: Christopher Wong: Consultant Nephrologist Anne Waddington: Renal Pharmacist Eimear Fegan : Renal Dietitian
 Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD
 The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
Month/Year of Review: September 2012 Date of Last Review: September 2010
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The role of calcimimetics in chronic kidney disease
 http://www.kidney-international.org & 2006 International Society of Nephrology The role of calcimimetics in chronic kidney disease A Gal-Moscovici 1,2 and SM Sprague 1 1 Division of Nephrology and Hypertension,
http://www.kidney-international.org & 2006 International Society of Nephrology The role of calcimimetics in chronic kidney disease A Gal-Moscovici 1,2 and SM Sprague 1 1 Division of Nephrology and Hypertension,
Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi
 Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi Mario Cozzolino, MD, PhD, FERA Dipartimento di Scienze della Salute Università di Milano UO Nefrologia e Dialisi Laboratorio
Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi Mario Cozzolino, MD, PhD, FERA Dipartimento di Scienze della Salute Università di Milano UO Nefrologia e Dialisi Laboratorio
BONE AND MINERAL METABOLISM in the PD PATIENT
 BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
The hart and bone in concert
 The hart and bone in concert Piotr Rozentryt III Department of Cardiology, Silesian Centre for Heart Disease, Silesian Medical University, Zabrze, Poland Disclosure Research grant, speaker`s fee, travel
The hart and bone in concert Piotr Rozentryt III Department of Cardiology, Silesian Centre for Heart Disease, Silesian Medical University, Zabrze, Poland Disclosure Research grant, speaker`s fee, travel
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Prevalence and Pattern of Mineral Bone Disorder in Chronic Kidney Disease Patients Using Serum
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Prevalence and Pattern of Mineral Bone Disorder in Chronic Kidney Disease Patients Using Serum
KDOQI COMMENTARY VOL 55, NO 5, MAY 2010
 VOL 55, NO 5, MAY 2010 KDOQI COMMENTARY KDOQI US Commentary on the 2009 KDIGO Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of CKD Mineral and Bone Disorder (CKD-MBD) Katrin
VOL 55, NO 5, MAY 2010 KDOQI COMMENTARY KDOQI US Commentary on the 2009 KDIGO Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of CKD Mineral and Bone Disorder (CKD-MBD) Katrin
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis
 IAMHD HOME HEMODIALYSIS CLINICAL PRACTICE STANDARDS AND PROCEDURES Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis PRINTED copies of Clinical Practice Standards and
IAMHD HOME HEMODIALYSIS CLINICAL PRACTICE STANDARDS AND PROCEDURES Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis PRINTED copies of Clinical Practice Standards and
Ultrasound examination in diagnosis of morphological variants of parathyroid hyperplasia in patients with secondary hyperparathyroidism
 Ultrasound examination in diagnosis of morphological variants of parathyroid hyperplasia in patients with secondary hyperparathyroidism Poster No.: C-0304 Congress: ECR 2015 Type: Authors: Keywords: DOI:
Ultrasound examination in diagnosis of morphological variants of parathyroid hyperplasia in patients with secondary hyperparathyroidism Poster No.: C-0304 Congress: ECR 2015 Type: Authors: Keywords: DOI:
qthis medicinal product is subject to additional monitoring. This will allow quick identification of new safety
 Parsabiv q (etelcalcetide) Frequently Asked Questions qthis medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals
Parsabiv q (etelcalcetide) Frequently Asked Questions qthis medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience
 Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Level 1 Strong We recommendyshould A High Moderate Level 2 Weak We suggestymight C Low Very low. K Hyperphosphatemia has been associated with poor
 chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations
 Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations Nancy E. Lane, MD Director, Center for Musculoskeletal Health Endowed Professor of Medicine and Rheumatology University
Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations Nancy E. Lane, MD Director, Center for Musculoskeletal Health Endowed Professor of Medicine and Rheumatology University
THE IMPACT OF SERUM PHOSPHATE LEVELS IN CKD-MBD PROGRESSION
 THE IMPACT OF SERUM PHOSPHATE LEVELS IN CKD-MBD PROGRESSION Mario Cozzolino, MD, PhD, Fellow of the European Renal Association Department of Health Sciences University of Milan Renal Division & Laboratory
THE IMPACT OF SERUM PHOSPHATE LEVELS IN CKD-MBD PROGRESSION Mario Cozzolino, MD, PhD, Fellow of the European Renal Association Department of Health Sciences University of Milan Renal Division & Laboratory
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet:
 Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Patients with end-stage renal disease (ESRD) have a
 have a") At a Glance Original Research Practical Implications e25 Author Information e32 Web Exclusive Costs of Treatment and Clinical Events for Secondary Hyperparathyroidism Andrew Lee, PhD; Vasily Belozeroff,
At a Glance Original Research Practical Implications e25 Author Information e32 Web Exclusive Costs of Treatment and Clinical Events for Secondary Hyperparathyroidism Andrew Lee, PhD; Vasily Belozeroff,
Bone impairment in pediatric CKD
 A 16-year old girl arriving in the emergency room for seizures No significant medical past except orthopaedic surgery for bilateral genu valgum without any obvious etiology at the age of 14 years Bone
A 16-year old girl arriving in the emergency room for seizures No significant medical past except orthopaedic surgery for bilateral genu valgum without any obvious etiology at the age of 14 years Bone
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine
 Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
Clinical and Practical Use of Calcimimetics in Dialysis Patients With Secondary Hyperparathyroidism
 In-Depth Review Clinical and Practical Use of Calcimimetics in Dialysis Patients With Secondary Hyperparathyroidism Jordi Bover,* Pablo Ure~na, César Ruiz-García,* Iara dasilva,* Patricia Lescano,* Jacqueline
In-Depth Review Clinical and Practical Use of Calcimimetics in Dialysis Patients With Secondary Hyperparathyroidism Jordi Bover,* Pablo Ure~na, César Ruiz-García,* Iara dasilva,* Patricia Lescano,* Jacqueline
THE FIELD OF mineral metabolism and
 SPECIAL REPORT Controversies in Bone and Mineral Metabolism in Chronic Kidney Disease A Bridge to Improving Healthcare Outcomes and Quality of Life Sharon M. Moe, MD, FACP, and Tilman B. Drüeke, MD, FRCP
SPECIAL REPORT Controversies in Bone and Mineral Metabolism in Chronic Kidney Disease A Bridge to Improving Healthcare Outcomes and Quality of Life Sharon M. Moe, MD, FACP, and Tilman B. Drüeke, MD, FRCP
Effects of Diabetes Mellitus, Age, and Duration of Dialysis on Parathormone in Chronic Hemodialysis Patients. Hamid Nasri 1, Soleiman Kheiri 2
 Saudi J Kidney Dis Transplant 2008;19(4):608-613 2008 Saudi Center for Organ Transplantation Saudi Journal of Kidney Diseases and Transplantation Original Article Effects of Diabetes Mellitus, Age, and
Saudi J Kidney Dis Transplant 2008;19(4):608-613 2008 Saudi Center for Organ Transplantation Saudi Journal of Kidney Diseases and Transplantation Original Article Effects of Diabetes Mellitus, Age, and
Hyperphosphatemia is associated with a
 TREATMENT OPTIONS IN THE MANAGEMENT OF PHOSPHATE RETENTION * George A. Porter, MD, FACP, and Hartmut H. Malluche, MD, FACP ABSTRACT Hyperphosphatemia is an independent risk factor for mortality and cardiovascular
TREATMENT OPTIONS IN THE MANAGEMENT OF PHOSPHATE RETENTION * George A. Porter, MD, FACP, and Hartmut H. Malluche, MD, FACP ABSTRACT Hyperphosphatemia is an independent risk factor for mortality and cardiovascular
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality
 Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
OSTEOMALACIA UPDATE. Nothing to Disclose. Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco
 OSTEOMALACIA UPDATE Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco Nothing to Disclose 1 Case History 59 YO WM referred for evaluation of diffuse
OSTEOMALACIA UPDATE Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco Nothing to Disclose 1 Case History 59 YO WM referred for evaluation of diffuse
IMPLEMENTATION OF THE CKD-MBD PRACTICE. Goce Spasovski, R. Macedonia
 IMPLEMENTATION OF THE CKD-MBD GUIDELINES Introduction INTO CLINICAL to Renagel PRACTICE Goce Spasovski, R. Macedonia Antalya, Turkey, September 16 2012 Session Objectives Guidelines needs and controversy
IMPLEMENTATION OF THE CKD-MBD GUIDELINES Introduction INTO CLINICAL to Renagel PRACTICE Goce Spasovski, R. Macedonia Antalya, Turkey, September 16 2012 Session Objectives Guidelines needs and controversy
Cost-Effectiveness of Early versus Late Cinacalcet Treatment in Addition to Standard Care for Secondary Renal Hyperparathyroidism in the USA
 Volume 11 Number 5 2008 VALUE IN HEALTH Cost-Effectiveness of Early versus Late Cinacalcet Treatment in Addition to Standard Care for Secondary Renal Hyperparathyroidism in the USA Joshua A. Ray, MSc,
Volume 11 Number 5 2008 VALUE IN HEALTH Cost-Effectiveness of Early versus Late Cinacalcet Treatment in Addition to Standard Care for Secondary Renal Hyperparathyroidism in the USA Joshua A. Ray, MSc,
Month/Year of Review: May 2014 Date of Last Review: September New Drug Evaluation: Sucrofferic Oxyhydroxide (Velphoro )
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Drugs for the treatment of secondary hyperparathyroidism and hyperphosphataemia
 NSW Therapeutic Advisory Group Level 5, 376 Victoria Street PO Box 766 Darlinghurst NSW 2010 Phone: 61 2 8382 2852 Fax: 61 2 8382 3529 Email: nswtag@stvincents.com.au www.nswtag.org.au Drugs for the treatment
NSW Therapeutic Advisory Group Level 5, 376 Victoria Street PO Box 766 Darlinghurst NSW 2010 Phone: 61 2 8382 2852 Fax: 61 2 8382 3529 Email: nswtag@stvincents.com.au www.nswtag.org.au Drugs for the treatment
Clinical Policy: Cinacalcet (Sensipar) Reference Number: CP.PHAR.61 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.61 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Sensipar) Reference Number: CP.PHAR.61 Effective Date: 05.01.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Sensipar) Reference Number: CP.PHAR.61 Effective Date: 05.01.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
J.Bacchetta has documented that she has received grants for research activities from Amgen, Crinex, Sandoz.
 J.Bacchetta has documented that she has received grants for research activities from Amgen, Crinex, Sandoz. Epidemiological, immune and metabolic aspects of vitamin D in CKD Justine Bacchetta, MD, PhD
J.Bacchetta has documented that she has received grants for research activities from Amgen, Crinex, Sandoz. Epidemiological, immune and metabolic aspects of vitamin D in CKD Justine Bacchetta, MD, PhD
Technology appraisal guidance Published: 28 June 2017 nice.org.uk/guidance/ta448
 Etelcalcetide for treating secondary hyperparathyroidism Technology appraisal guidance Published: 28 June 2017 nice.org.uk/guidance/ta448 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Etelcalcetide for treating secondary hyperparathyroidism Technology appraisal guidance Published: 28 June 2017 nice.org.uk/guidance/ta448 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Bone strength is proportional to bone mass, measured with DXA. Bone turnover markers indicate the status of bone quality.
 Bone strength is proportional to bone mass, measured with DXA Bone quality depend on bone architecture, rate of bone turnover, quality of bone matrix. Bone turnover markers indicate the status of bone
Bone strength is proportional to bone mass, measured with DXA Bone quality depend on bone architecture, rate of bone turnover, quality of bone matrix. Bone turnover markers indicate the status of bone
Class Review: Vitamin D Analogs
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Opinion 23 April 2014
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 23 April 2014 MIMPARA 30 mg, film-coated tablet B/14 (CIP: 365 154 8) B/28 (CIP: 365 155 4) B/30 (CIP: 365 157 7)
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 23 April 2014 MIMPARA 30 mg, film-coated tablet B/14 (CIP: 365 154 8) B/28 (CIP: 365 155 4) B/30 (CIP: 365 157 7)
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.PMN.04 Effective Date: 11.15.17 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: CP.PMN.04 Effective Date: 11.15.17 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy for important
Assessment of Osteoporosis Risk Factors in Low Socioeconomic Status Hemodialysis Patients in Jeddah
 World Journal of Medical Sciences 1 (4): 438-443, 015 ISSN 1817-3055 IDOSI Publications, 015 DOI: 10.589/idosi.wjms.015.1.4.1154 Assessment of Osteoporosis Risk Factors in Low Socioeconomic Status Hemodialysis
World Journal of Medical Sciences 1 (4): 438-443, 015 ISSN 1817-3055 IDOSI Publications, 015 DOI: 10.589/idosi.wjms.015.1.4.1154 Assessment of Osteoporosis Risk Factors in Low Socioeconomic Status Hemodialysis
Cardiovascular Mortality: General Population vs ESRD Dialysis Patients
 Cardiovascular Mortality: General Population vs ESRD Dialysis Patients Annual CVD Mortality (%) 100 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age (years) GP Male GP Female GP Black GP
Cardiovascular Mortality: General Population vs ESRD Dialysis Patients Annual CVD Mortality (%) 100 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age (years) GP Male GP Female GP Black GP
Setting the standard
 SCLEROSTIN in NEPHROLOGY MOST REFERENCED OPTIMIZED FOR CLINICAL SAMPLES Setting the standard for clinical research. SCLEROSTIN A BONE-RELATED PROTEIN URINE PROTOCOL AVAILABLE Sclerostin ELISA - Assay Characteristics
SCLEROSTIN in NEPHROLOGY MOST REFERENCED OPTIMIZED FOR CLINICAL SAMPLES Setting the standard for clinical research. SCLEROSTIN A BONE-RELATED PROTEIN URINE PROTOCOL AVAILABLE Sclerostin ELISA - Assay Characteristics
Prof. Michel Jadoul Cliniques universitaires St-Luc Université Catholique de Louvain Brussels, Belgium. Slide 1
 Phosphate and cardiovascular disease beyond CKD: is phosphate a new cholesterol? Michel Jadoul, Brussels, Belgium Chairs: Pablo Urena Torres, Saint-Ouen, France Carmine Zoccali, Reggio Calabria, Italy
Phosphate and cardiovascular disease beyond CKD: is phosphate a new cholesterol? Michel Jadoul, Brussels, Belgium Chairs: Pablo Urena Torres, Saint-Ouen, France Carmine Zoccali, Reggio Calabria, Italy
2.0 Synopsis. ABT-358/Paricalcitol M Clinical Study Report R&D/09/1255. (For National Authority Use Only) to Part of Dossier: Volume:
 to Part of Dossier: Volume:") 2.0 Synopsis Title of Study: Late Phase II Study of Paricalcitol Injection Dose-response study of paricalcitol injection in chronic kidney disease subjects receiving hemodialysis with secondary hyperparathyroidism
2.0 Synopsis Title of Study: Late Phase II Study of Paricalcitol Injection Dose-response study of paricalcitol injection in chronic kidney disease subjects receiving hemodialysis with secondary hyperparathyroidism
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL
 PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
Vitamin D and Calcium Therapy: how much is enough
 Vitamin D and Calcium Therapy: how much is enough Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco DISCLOSURE Nothing to disclose 1 RECOMMENDATIONS
Vitamin D and Calcium Therapy: how much is enough Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco DISCLOSURE Nothing to disclose 1 RECOMMENDATIONS