Treatment Options for Chronic Kidney. Goce Spasovski, R. Macedonia
|
|
|
- Dylan Snow
- 6 years ago
- Views:
Transcription


1 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011
2 Session Objectives Definition of the problem of CKD-MBD Clinical relevance and consequences increased morbidity and mortality Current therapeutical options-modification Calcium and phosphate levels (bone) Calcifications (vessels) CVDs (outcome) phosphate binders 2008; 3(3):222-8

3 Mineral & Bone Disorder (MBD) Systemic Complication in CKD Mineral Hormonal Bone abnormalities, Vascular calcifications Soft tissue calcifications CVD, fractures, mortality
 Ca reabs. 1 a hydroxylase FOOD 800 mg/day Absorption 1,25(OH) 2 D 3 1200 mg Daily food -- PO 4 abs. 800 mg 400 mg Faecal excretion INTESTINE Spasovski G et al.")
4 Pathophysiology of CKD - MBD BLOOD VESSEL BONE resorption 200 mg/day Deposition Vascular calcification PARATHYROID GLAND BLOOD 200 mg/day Resorption Ca PO 4 Ca PO mg/day Formation PTH 150 mg/day KIDNEY (RENAL FAILURE) Ca reabs. 1 a hydroxylase FOOD 800 mg/day Absorption 1,25(OH) 2 D mg Daily food -- PO 4 abs. 800 mg 400 mg Faecal excretion INTESTINE Spasovski G et al. Semin Dial 2009; 22(4):
5 FGF-23 Regulation of Phosphorous Homeostasis FGF-23 Bone Serum Phosphorous Kidney P reabsorption 1,25(OH) 2 D 3 P excretion in urine Adapted from Stubbs J, et al. Semin Dial. 2007;20:
6 Mean Log FGF-23* Changes in FGF-23 Levels With Decline in Kidney Function 7 CKD 2 CKD 3 CKD 4 & FGF-23 > < 30 egfr (ml/min/1.73 m 2 ) N = 220 *Normal range for FGF-23 indicated by shaded area; GFR = glomerular filtration rate; egfr = estimated GFR. Adapted from Gutiérrez OM, et al. Circulation. 2009;119:
7 ipth (pg/ml) 1,25(OH) 2 D 3 (pg/ml) Changes in PTH and 1,25(OH) 2 D 3 Levels With Decline in Kidney Function N = 1,814 Median Values of Serum 1,25(OH) 2 D 3 and ipth by GFR 1 CKD 2 CKD 3 CKD 4 & 5 ipth 1,25(OH) 2 D 3 > < 20 GFR (ml/min) ipth = intact PTH; GFR = glomerular filtration rate. Levin A, et al. Kidney Int. 2007; 71:31-38.
8 Mineral Metabolism and Mortality Risk in the DOPPS Disorders of mineral metabolism are associated with increased mortality Prospective observational cohort study patients with ESRD on hemodialysis. Outcomes: Adjusted hazard ratios (HR) for all-cause and cardiovascular mortality using Cox models. Tentori F et al. Am J Kidney Dis 2008;52:
9 K/DOQI* guidelines for Bone Metabolism and Disease / Dislipidemia in Chronic Kidney Disease ( mmol/l) (< 4.4 mmol 2 /l 2 ) (< 2.56 mmol/l) (< 5.12 mmol/l) The K/DOQI guidelines have become widely accepted and are basis of many national treatment guidelines in Eastern Europe National Kidney Foundation K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease. Am J Kidney Dis 2003;42(Suppl 3):S1-S202. National Kidney Foundation K/DOQI Clinical Practice Guidelines for managing Dyslipidemias in Chronic Kidney Disease. Am J Kidney Dis. 2003;41(suppl 3):S1-91.
10 Relative Hazard of Death (95% CI) Mortality Risk Varies According to Number of Laboratory Targets* Achieved Concurrently 1,8 1,6 Three Targets (Reference) Two Targets One Target No Targets 1,51 1,4 1,39 1,37 1,35 1,2 1,21 1,20 1,15 1,0 1,00 0,8 N = 22,937 All ipth & P ipth & Ca Ca & P Groups Defined by Targets Achieved P ipth Ca None Time-dependent model. *Laboratory targets from National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ). KDOQI TM is a trademark of the National Kidney Foundation, Inc. Danese MD, et al. Clin J Am Soc Nephrol. 2008;3:
11 Bone as primary reservoir of calcium & phosphorus Hydroxyapatite % of total body Ca % of total body PO 4 Bone 99 % 29 % Intracellular Interstitial Plasma 0.9 % % % 70 % (exch.) 0.1 % 0.9 % Spasovski G et al. Semin Dial 2009; 22(4):
12 Consequences of Elevated Serum Phosphorus Pi Ca ++ Calcitriol PTH resistance Calcitriol resistance PTH Secretion Parathyroid Cell Growth Increased CaxP & risk of metastatic calcifications HPTH Treatment ABD Morbidity & Mortality Spasovski G et al. Semin Dial 2009; 22(4):
13




14 Bone Histology in ROD Osteitis Fibrosa Mixed lesion Adynamic bone disease Osteomalacia
15 Changing Spectrum of ROD Earliest reports HPTH most prevalent, followed by OM Insufficient treatment of shpth Vitamin D deficiency Al intoxication Last two decades ABD Older age of the patients Diabetes Calcium containing phosphate binder Vitamin D treatment High calcium dialysate concentration
16 Changing spectrum of renal osteodystrophy Adynamic Bone Disease - bone and beyond Evolution of ROD distribution pattern over time Brandenburg VM & Floege J. NDT plus (2008) 3: Malluche HH, Mawad H, Monier-Faugere MC. Nephrol Dial Transpl 2004; 19 Suppl 1: i9-13
17 Changing spectrum of renal osteodystrophy Spectrum of Renal Bone Disease in patients with end-stage renal bone disease not yet in dialysis Osteomalacia 12% Hyperpara 9% N = 84 Adynamic bone 23% Mixed lesion 18% Prospective, Non-randomized, Macedonian Population N = 84 patients Histomorphometric criteria according to: Salusky et al., Kidney Int.,33,1988 Parfitt et al., Calcif Tissue Int 42, 1988 Normal bone 38% GB Spasovski et al. Nephrol Dial Transpl 2003; 18:
18 Physiopathology of Adynamic Bone Al + Fe Mg ++ Better Pi control Diabetes Vit.D treatm. VDR polymorphism Relative hypoparathyroidism VDR expression Down regulation of PTH receptor Insufficient PTH levels Osteoblastic dysfunction Diabetes Older age Older age Male gender Malnourishment Ca receptor expression Decreased BFR Uremic toxins Extracellular Ca ++ Growth factors Al + Fe Ca load: Ca based binders HD & CAPD dialysis fluid Ca conc. Vit.D treatment
19 Clinical Relevance and Consequences Association in CKD patients between: MBD (abnormal mineral metabolism & bone health) & Fractures decreased quality of life VC most important cause of morbidity CVD significant mortality Bone health and vascular calcification relationship in chronic kidney disease Spasovski G. Int Urol Nephrol 2007;39:
 that of age-matched controls. Alem A et al.")
20 CKD - MBD: Bone lose & fracture United States Renal Data System data (300,000 patients) - The relative risk for hip fracture in dialysed patients is 4.4 times (men and women) that of age-matched controls. Alem A et al. Kidney Int 2000, 58: 396-9
21 Disordered bone remodelling can induce vascular calcification High bone turnover Phosphate Calcium Precipitation in vessels and soft tissues Low bone turnover Calcification High bone turnover leads to release of Ca + P from bone. Low bone turnover hinders their emplacement in bone. Result is cardiovascular and soft tissue calcification. London et al. J Am Soc Nephrol 2004;15: ; Spasovski G. Int Urol Nephrol 2007;39:
22 Osteoclast Resorption (%) Double labeled surfaces (%) Osteoblast surface (%) Arterial Calcifications and Bone Histomorphometry in ESRD P = versus P = versus versus Arterial calcification score* n = 58 Arterial calcification score* Osteoclasts (n/mm 2 ) P = versus P = versus Arterial calcification score* Arterial calcification score* *Determined by ultrasonography London GM, J Am Soc Neph 15: , 2004
23 VSMCs can Transdifferentiate into Osteoblasts Ox LDL TNF-a IL-1b TGFb PO 4 AGE MGP OPN Fetuin BMP7 PTH OPG Calcitriol Steroïds Leptin AMPc Calcifying Smooth muscle cells Bone cells Modified from: Shanahan CM. Curr Opin Nephrol Hypertens 2005; 14(4):361-7



 More")
24 CKD - MBD: Vascular calcifications Intimal calcification Media calcification More frequent & early occurrence vs. general population (London G et al. JASN, 2000, 11:778-8) More rapid rate of progression (Tamashiro M et al., AJKD, 2001, 38:64-9)
25 Arterial calcification increases mortality risk Probability of survival arteries calcified 1 artery calcified 2 arteries calcified 3 arteries calcified n=110 p< Duration of follow-up (months) 4 arteries calcified Presence and extent of vascular calcifications predict cardiovascular and allcause mortality in dialysis patients. Prospective trial in 110 dialysis patients assessing cardiovascular (CV) calcifications, mean follow up 53 months. Endpoints: All cause and CV mortality using univariate and multivariate survival analysis. Blacher et al. Hypertension 2001;38:
26 Survival Distribution Function Survival by baseline CACS P= CACS=0 CACS< 400 CACS >= 400 No. at Risk Months Patients with cardiovascular calcifications had a higher mortality risk than non-calcified patients. Follow up of a randomized, prospective, open label, multicenter study over a median of 44 months (RIND). 127 patients randomized to either sevelamer or Ca. Prespecified secondary endpoint. Block GA et al. Kidney Int 2007;71:
27 Annual CVD Mortality (%) Increased CVD Morbidity & Mortality >85 Age (years) GP Male GP Female GP Black GP White Dialysis Male Dialysis Female Dialysis Black Dialysis White CVD = cardiovascular disease GP = general population Foley FN et al. AJKD 1998;32:S112-S119

28 Increased serum phosphorus negatively impacts the mortality of CKD patients not on dialysis. The association between higher phosphate levels and mortality risk was present among patients with absolute serum phosphate levels in the high-normal range. Kestenbaum B, Sampson JN, Rudser KD, et al. Serum phosphate levels and mortality risk among people with chronic kidney disease. J Am Soc Nephrol. 2005;16:
29 Management of Hyperphosphatemia Dietary phosphorus restriction Dialysis Phosphate binders Serum phosphorus not sufficiently controlled through dialysis and diet Almost all dialysis patients need phosphate binders New Strategies in Treatment of MBD and Associated Cardiovascular Disease in Patients with CK Spasovski G, Recent Patents on Cardiovascular Drug Discovery, 2008; 3(3): NKF - K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease. Am J Kidney Dis 2003;42(Suppl 3):S1-S202.
30 K/DOQI* guidelines for Bone Metabolism and Disease / Dislipidemia in Chronic Kidney Disease ( mmol/l) (< 4.4 mmol 2 /l 2 ) (< 2.56 mmol/l) (< 5.12 mmol/l) The K/DOQI guidelines have become widely accepted and are basis of many national treatment guidelines in Eastern Europe National Kidney Foundation K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease. Am J Kidney Dis 2003;42(Suppl 3):S1-S202. National Kidney Foundation K/DOQI Clinical Practice Guidelines for managing Dyslipidemias in Chronic Kidney Disease. Am J Kidney Dis. 2003;41(suppl 3):S1-91.
 Non Ca based Sevelamer remains first line treatment option (Lanthanum, MCI 196) Ca based binders contraindicated in low PTH, high Ca, severe calcifications National Kidney Foundation K/DOQI")
31 K/DOQI* guidelines for Bone Metabolism and Disease in Chronic Kidney Disease (> 1.8 mmol/l) Non Ca based (> 2.7 mmol/l) Non Ca based Sevelamer remains first line treatment option (Lanthanum, MCI 196) Ca based binders contraindicated in low PTH, high Ca, severe calcifications National Kidney Foundation K/DOQI Clinical Practic Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease. Am J Kidney Dis 2003;42(Suppl 3):S1-S202.

32 Calcium restriction in KDIGO Calcification Persistently Low PTH Hypercalcemia ABD 1,2,3 2 2,3,4 51% - 83% 57% 16% - 54% 5 40% CKD 3/ % HD % PD 5 Recommended for Calcium Restriction 1 Russo D, Corrao S, Miranda I, et al. Am J Neph 2007;27: Chertow GM, Burke SK, Raggi P, et al. Kidney Int. 2002;62: Block GA, Spiegel DM, Ehrlich J,et al. Kidney Int. 2005;68: Qunibi W, Moustafa M, Muenz LR, et al. AJKD Andress D. Kidney Int. 2008;73: KDIGO. Kidney Int. 2009; 76 (Suppl 113):S1-S130
 for all-cause and cardiovascular mortality using Cox models. Tentori F et al.")
33 Mineral Metabolism and Mortality Risk in the DOPPS Hyperphosphatemia is the most frequent abnormality. Around 90% of dialysis patients on phosphate binders, still 35% out of KDOQI targets. Prospective observational cohort study patients with ESRD on hemodialysis. Outcomes: Adjusted hazard ratios (HR) for all-cause and cardiovascular mortality using Cox models. Tentori F et al. Am J Kidney Dis. 2008;52:
34 Types of Phosphate Binders Calcium-based Calcium carbonate and acetate (Mg) effective at binding dietary phosphate, but associated with vascular-soft tissue calcification Metal-based - (non-calcium) Aluminium effective at binding dietary phosphate, but long-term toxicity shown Lanthanum systemically absorbed; bone deposition (no toxicity) has been demonstrated Renagel (sevelamer) (non-calcium) Calcium-free, metal-free phosphate binder. The only non-absorbed phosphate binder. Does not expose patients to increased risk of vascular and soft tissue calcification *MCI-196 (non-calcium) Calcium & metal-free non-absorbed phosphate binder. Efficient and safe treatment, no risk of soft and VC Goodman WG et al. NEJM 2000;342: London GM et al. JASN 2004;15: Malluche HH and Mawad H. NDT 2002;17: Locatelli F et al. Drugs 2003;6: Chertow GM et al. KI 2002;62: Block GA et al. KI 2005;68: Spasovski G et al. NDT 2006;21: *Locatelli F et al. NDT 2010;25:
 for all-cause and cardiovascular mortality using Cox models. Tentori F et al.")
35 Mineral Metabolism and Mortality Risk in the DOPPS Disorders of mineral metabolism are associated with increased mortality Prospective observational cohort study patients with ESRD on hemodialysis. Outcomes: Adjusted hazard ratios (HR) for all-cause and cardiovascular mortality using Cox models. Tentori F et al. Am J Kidney Dis 2008;52:

36 Vascular events in healthy older women on calcium supplementation p=0,01 Myocardial infarction and the composite endpoint occurred more frequently in the calcium group Randomized, placebo controlled trial in 1471 healthy postmenopausal women to determine the effect of calcium supplementation on myocardial infarction, stroke, and sudden death in healthy postmenopausal women. Bolland MJ et al. BMJ 2008;336:262-6
37 Risk Factors Associated With Cardiac Calcification in Young Dialysis Patients Coronary No Calcification Calcification Factor (n=14) (n=25) P - value Ca from 6456 ± ± calcium binders (mg/day) Serum Ca (mmol/l) 2.4 ± ± Serum P (mmol/l) 2.2 ± ± Ca P (mmol 2 /L 2 ) 5.2 ± ± Age (years) 26 ± 3 15 ± 5 <0.001 Mean duration of dialysis (years) 14 ± 5 4 ± 4 < HD patients 7 30 years 60 controls years EBT scans at baseline and after months Goodman WG et al. N Engl J Med. 2000; 342:
38 NEW THERAPEUTIC APPROACH PREVENTION OF COMPLICATIONS OF THERAPY... OF HYPERPHOSPHATEMIA & MBD & ROD & VC IN CKD PATIENTS
39 Reducing Calcium Load With a Calcium-free Phosphate Binder Total Elemental Calcium Intake (average g/wk) g/wk Phosphate binder: 3-5 g/day (20-30% resorption) 1300 mg/day Dialysate: 1.25 moll/l - net influx mg calcium / HD Diet: intake 600 mg calcium per day Calcium Binder* 4.3 g/wk Calcium-Free, Metal-Free Binder Binder (dose 5 g/day) Dialysate (2.5 meq/l) Diet (600 mg/day) Bleyer AJ et al. Am J Kidney Dis. 1999;33: Data on file, Genzyme Corporation Hsu CH. Am J Kidney Dis. 1997;29:
40 Mortality effect of coronary calcification and phosphate binder choice Survival Distribution Function 1.00 P= Calcium Renagel Months No. at Risk Calcium Renagel Treatment with sevelamer was associated with a significant survival benefit. There were 11 deaths in the sevelamer and 23 in the Calcium group. Follow up of a randomized, prospective, open label, multicenter study over a median of 44 months (RIND). 127 patients randomized to either sevelamer or Ca. Prespecified secondary endpoint. Block GA et al. Kidney Int 2007;71:
41 Cumulative Incidence of All-Cause Mortality DCOR: All-Cause Mortality Calcium Sevelamer Time on Study (Years) Results of the DCOR trial were inconclusive for the primary end-point of allcause mortality across the entire patient cohort (RR 0.91; p = 0.3) Prospective, randomized trial in 2103 prevalent dialysis patients receiving either sevelamer or Ca-containing phosphate binders. Max. follow up 45 months. Primary endpoint: All cause survival. Secondary endpoints: Cause-specific mortality, all-cause and cause-specific hospitalization, medicare expenditures. Suki W et al. Kidney Int 2007;72:
![DCOR: Mortality risk reduction with Renagel Risk reduction [%] 10 20 30-9% -22% p = 0,02-34% All patients Patients 65 Patients on study 2 yrs A mortality benefit for patients treated with Renagel was](/docs-images/79/79994832/images/42-0.jpg "shown in subgroups: Patients older than 65 (predefined) and patients on study for more than 2 years Prospective, randomized trial in 2103 prevalent dialysis patients receiving either sevelamer or")
42 DCOR: Mortality risk reduction with Renagel Risk reduction [%] % -22% p = 0,02-34% All patients Patients 65 Patients on study 2 yrs A mortality benefit for patients treated with Renagel was shown in subgroups: Patients older than 65 (predefined) and patients on study for more than 2 years Prospective, randomized trial in 2103 prevalent dialysis patients receiving either sevelamer or Ca-containing phosphate binders. Max. follow up 45 months. Primary endpoint: All cause survival. Secondary endpoints: Cause-specific mortality, all-cause and cause-specific hospitalization, medicare expenditures. Suki W et al. Kidney Int 2007; 72:
43 Hospitalisation rate by binder choice Rate per patient-year Sevelamer Calcium HR* p* First hospitalisations 0,96 0,97 ns Multiple hospitalisations 1,70 1,91 0,89 0,02 Days in hospital 12,3 13,9 0,88 0,03 Almost every patient was hospitalised once per year. Renagel treated patients were hospitalized less frequently and spent less time in the hospital. Preplanned secondary analysis of DCOR for mortality, morbidity, and hospitalization end points, using Centers for Medicare & Medicaid Services data. St. Peter WL et al. Am J Kidney Dis 2008;51: *Adjusted for demographic variables and prestudy cardiovascular comorbidity
44 Calcium-treated subjects had decreased bone density Mean change (%) Cortical Trabecular* Cortical Trabecular* sevelamer (S) Calcium (C) The lower time averaged PTH achieved in calcium-treated subjects is a likely explanation for the changes observed in bone attenuation. Post- hoc analysis of a randomized, prospective, open label, multicenter study over one year (Treat to Goal) evaluating EBCT scans of vertebrae. Raggi P et al. J Bone Miner Res. 2005;20: *p=0.01 Sevelamer vs. Calcium, ns
45 Effects of Sevelamer Hydrochloride and Calcium Carbonate on ROD in HD Patients Ferreira A, Frazao J et al. J Am Soc Nephrol 2008; 19:


46 Classification of ROD in LC and CC group Patients with either low bone turnover at baseline and those evolving toward low bone turnover at follow-up in both study groups Evolution of renal bone disease of all patients after one year of treatment with either lanthanum or calcium carbonate D'Haese PC, Spasovski GB et al. Kidney Int 2003; 63: Suppl 85:73-78
47 Evolution of bone and plasma concentration of lanthanum in dialysis patients before, during 1 year treatment with lanthanum carbonate and after two years of follow up. Bone lanthanum concentrations of patients receiving lanthanum carbonate (solid circle) and calcium carbonate treatment (open circle) for 12 months, followed by 2 years of treatment with calcium carbonate. There is a slow release of lanthanum from its bone deposits 2 years after the discontinuation of the treatment and no association with aluminium-like bone toxicity. Spasovski G et al. Nephrol Dial Transpl 2006; 21(8):
 in patients who were treated with lanthanum")

48 Effects of Treatment of Renal Osteodystrophy on Bone Histology 58% 35.5% Baseline 1 year Higher activation frequency (bone turnover) in patients who were treated with lanthanum carbonate after 1 year 28% 9% Baseline 2 years Higher bone volume (tissue volume) in patients who were treated with lanthanum carbonate after 2 years Malluche H et al. Clin Nephrol 2008; 70(4): Malluche H et al. Clin J Am Soc Nephrol 2008; 3: S157 S163
49 Analysis of survival in a 2-year comparative study of lanthanum carbonate vs. standard therapy Figure 1. Survival probability: lanthanum carbonate versus standard therapy. LC, lanthanum carbonate; Standard, standard therapy. Figure 2. Survival probability in patients aged >65 years: lanthanum carbonate versus standard therapy. LC, lanthanum carbonate; Standard, standard therapy. Wilson R, Zhang P, Smyth M, Pratt R. Curr Med Res Opin. 2009; 25(12):
50 New Strategies in Treatment of MBD and Associated CVD in Patients with CKD Spasovski G, Recent Patents on Cardiovascular Drug Discovery, 2008; 3(3):222-8 Cost-effectiveness - Good value for money!? Huybrechts KF, Caro JJ, Wilson DA, O Brien JA. Health and economic consequences of sevelamer use for hyperphosphatemia in patients on hemodialysis. Value Health 2005; 8: Lack of outcome data favorable enough to justify widespread utilisation CA White, J Jaffey, P Magner. Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis patients. Kidney International (2007) 71, The yearly cost of implementation of the K/DOQI guidelines for 416 pts. at this center (University of Ottawa) was estimated at $ (American dollars). Given the significant cost, widespread adoption of the K/DOQI CPGs for Bone Metabolism and Disease should await the publication of compelling data demonstrating significant improved outcomes in patients treated with sevelamer.

51 Type of treatment for hyperphosphataemia and related outcomes

52 Type of treatment for hyperphosphataemia and related outcomes
53
54 Cost-effective Reduction of Calcium Load and possible treatment of ABD as most prevalent ROD type Individualized program
 1.18 0.01 1.15 0.02 NS 1.25 0.02 1.09 0.02 P<0.0001 PO 4 (mm) 1.70 0.12 1.72 0.13 NS 1.89 0.13 1.92 0.14 NS Mg (mm) 1.24 0.06 1.22 0.03 NS 1.21 0.05 1.20 0.")
55 Lowered Dialysate Calcium in PD: Increased PTH and Bone Formation. Haris A et al. Kidney Int 2006; 70(5):931-7 Control Ca Low Ca Before After P-value Before After P-value tca (mm) NS P<0.001 ica (mm) NS P< PO 4 (mm) NS NS Mg (mm) NS NS ALP (U/l) NS NS PTH (pm) NS P< n = 9 n = 14
56 Treatment of ABD with LCD and HCD Improvement of Bone and Mineral Parameters Related to ABD by Diminishing Dialysate Calcium Pre HD param. LCD HCD unit Baseline 3 months 6 months Baseline 3 months 6 months tca Pre HD 2.44 ± ± 0.19 a 2.39 ± ± ± 0.19 a 2.39 ± 0.17 b tca Post HD 2.41 ± ± ± 0.20 b 2.65 ± 0.18 c 2.50 ± 0.17 a,c 2.63 ± 0.19 b,c ica Pre HD 1.10 ± ± 0.12 a 1.07 ± 0.09 b 1.11 ± ± 0.08 c 1.07 ± 0.08 ica Post HD 1.09 ± ± 0.14 a 1.12 ± 0.09 b 1.20 ± 0.08 c 1.16 ± 0.22 c 1.18 ± 0.08 c P 1.50 ± ± ± ± ± 0.46 a 1.58 ± 0.45 a Ca x P ipth pg/ml* TAP U/L* BAP U/L* 3.68 ± ± ± ± ± ± ± ± 43.4 a 78.6 ± 44.7 a 43.5 ± ± ± 29.6 c 59.5 ± ± 26.7 a 84.0 ± 35.4 a 58.0 ± ± ± 25.9 c 23.4 ± ± ± 22.3 a 25.4 ± ± ± 9.7 c Spasovski G et al. Bone 2007; 41:
57 Vitamin K 2 Improves Bone Metabolism in HD pts. with a Low PTH 40 HD pts with low intact PTH levels (<100 pg/ml) randomised into a vitamin K₂ group receiving oral menatetrenone (45 mg/day) for 1 year and a control group without vitamin K₂. Ochiai M, et al. Nephron Clin Pract. 2011; 117(1):c15-9.
 The K/DOQI guidelines have become widely accepted and are basis of many national treatment guidelines in Eastern Europe National Kidney Foundation K/DOQI Clinical Practice Guidelines for")
58 K/DOQI* guidelines for Bone Metabolism and Disease / Dislipidemia in Chronic Kidney Disease ( mmol/l) (< 4.4 mmol 2 /l 2 ) (< 2.56 mmol/l) (< 5.12 mmol/l) The K/DOQI guidelines have become widely accepted and are basis of many national treatment guidelines in Eastern Europe National Kidney Foundation K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease. Am J Kidney Dis 2003;42(Suppl 3):S1-S202. National Kidney Foundation K/DOQI Clinical Practice Guidelines for managing Dyslipidemias in Chronic Kidney Disease. Am J Kidney Dis. 2003;41(suppl 3):S1-91.

59
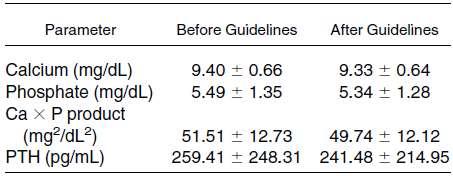
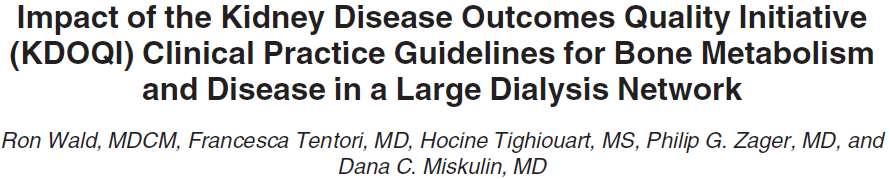
60 K/DOQI guidelines achieved parameters
61 Treatment options
62 Conclusion from the KDOQI based studies The individualisation of the CKD-MBD management may be successful even in the absence of modern new treatment possibilities. Nephrologists should ask for advanced treatment options in accordance with the guidelines at least for a small subset of patients where current standard therapy does not work. Implementation process should be continuous and selfmonitored at least through surveys. Judicious treatment could be a better option than overzealous treatment in order to do no harm for the patients health.
63 Modification of current therapeutic options in pts. with low PTH - ABD Avoid hypoparathyroidism Avoid high-dose vitamin D Avoid high-dose oral calcium Avoid high-calcium dialysate Use low-ca dialysate! Use Vit. K 2!
64 Summary: Treatment of MBD in CKD An aggressive treatment of hyperphosphatemia with Ca based P- binders might lead towards an opposite effect: - hypoparathyroidism, hypercalcemia, calcifications An individualised treatment and prevention of complications of therapy preserving bone and vascular health : Calcium phosphate binders (as less as possible / 1-2 g/day) Low-calcium dialysis bath (1.25 mmol/l) Vitamin K 2 Non Ca-based P binders in pts at risk for fractures&vc&cvd Calcimimetics & Vit.D analogs - no other armamentarium is available

65 Treat the Hyperphosphatemia & Bones in order to save blood vessels & the Heart!
Management of CKD. Goce Spasovski, R. Macedonia
 Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
Treatment Options for Chronic Kidney
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Guidelines and new evidence on CKD - MBD treatment
 Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
IMPLEMENTATION OF THE CKD-MBD PRACTICE. Goce Spasovski, R. Macedonia
 IMPLEMENTATION OF THE CKD-MBD GUIDELINES Introduction INTO CLINICAL to Renagel PRACTICE Goce Spasovski, R. Macedonia Antalya, Turkey, September 16 2012 Session Objectives Guidelines needs and controversy
IMPLEMENTATION OF THE CKD-MBD GUIDELINES Introduction INTO CLINICAL to Renagel PRACTICE Goce Spasovski, R. Macedonia Antalya, Turkey, September 16 2012 Session Objectives Guidelines needs and controversy
Cinacalcet treatment in advanced CKD - is it justified?
 Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary hyperparathyroidism in dialysis patients
 Secondary hyperparathyroidism in dialysis patients ( a critical approach of pharmacological treatments) Dominique JOLY Néphrologie Hôpital NECKER, Paris DFG Finn WF. J Am Soc Nephrol. 24;15:271A. Ca ++
Secondary hyperparathyroidism in dialysis patients ( a critical approach of pharmacological treatments) Dominique JOLY Néphrologie Hôpital NECKER, Paris DFG Finn WF. J Am Soc Nephrol. 24;15:271A. Ca ++
2017 KDIGO Guidelines Update
 2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience
 Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis
 Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis Seoung Woo Lee Div. Of Nephrology and Hypertension, Dept. of Internal Medicine, Inha Unv. College of Medicine, Inchon, Korea
Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis Seoung Woo Lee Div. Of Nephrology and Hypertension, Dept. of Internal Medicine, Inha Unv. College of Medicine, Inchon, Korea
( ) , (Donabedian, 1980) We would not choose any treatment with poor outcomes
 , (Donabedian, 1980) We would not choose any treatment with poor outcomes") ..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
Cardiovascular Mortality: General Population vs ESRD Dialysis Patients
 Cardiovascular Mortality: General Population vs ESRD Dialysis Patients Annual CVD Mortality (%) 100 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age (years) GP Male GP Female GP Black GP
Cardiovascular Mortality: General Population vs ESRD Dialysis Patients Annual CVD Mortality (%) 100 10 1 0.1 0.01 0.001 25-34 35-44 45-54 55-64 66-74 75-84 >85 Age (years) GP Male GP Female GP Black GP
Hyperphosphatemia is associated with a
 TREATMENT OPTIONS IN THE MANAGEMENT OF PHOSPHATE RETENTION * George A. Porter, MD, FACP, and Hartmut H. Malluche, MD, FACP ABSTRACT Hyperphosphatemia is an independent risk factor for mortality and cardiovascular
TREATMENT OPTIONS IN THE MANAGEMENT OF PHOSPHATE RETENTION * George A. Porter, MD, FACP, and Hartmut H. Malluche, MD, FACP ABSTRACT Hyperphosphatemia is an independent risk factor for mortality and cardiovascular
Level 1 Strong We recommendyshould A High Moderate Level 2 Weak We suggestymight C Low Very low. K Hyperphosphatemia has been associated with poor
 chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
Month/Year of Review: September 2012 Date of Last Review: September 2010
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure
 Nephrol Dial Transplant (2002) 17: 340 345 The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure Naseem Amin Genzyme Corporation, Cambridge, MA,
Nephrol Dial Transplant (2002) 17: 340 345 The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure Naseem Amin Genzyme Corporation, Cambridge, MA,
Therapeutic golas in the treatment of CKD-MBD
 Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
CKD-Mineral Bone Disorder (MBD) Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire
 Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire") Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
The CARI Guidelines Caring for Australasians with Renal Impairment. Serum phosphate GUIDELINES
 Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Serum phosphate GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Serum phosphate GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
New biological targets for CKD- MBD: From the KDOQI to the
 New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. E-mail : guillaume-jean-crat@wanadoo.fr
New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. E-mail : guillaume-jean-crat@wanadoo.fr
KDIGO. CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke
 CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke Unité 1088 de l Inserm UFR de Médecine et de Pharmacie Jules Verne University of Picardie Amiens, France Poten2al conflicts of interest Research support:
CKD- MBD: Is the Term S2ll Jus2fied? Tilman B. Drüeke Unité 1088 de l Inserm UFR de Médecine et de Pharmacie Jules Verne University of Picardie Amiens, France Poten2al conflicts of interest Research support:
Benefits and Harms of Phosphate Binders in CKD: A Systematic Review of Randomized Controlled Trials
 Benefits and Harms of Phosphate Binders in CKD: A Systematic Review of Randomized Controlled Trials Sankar D. Navaneethan, MD, MPH, Suetonia C. Palmer, MBChB, Jonathan C. Craig, MBChB, PhD, Grahame J.
Benefits and Harms of Phosphate Binders in CKD: A Systematic Review of Randomized Controlled Trials Sankar D. Navaneethan, MD, MPH, Suetonia C. Palmer, MBChB, Jonathan C. Craig, MBChB, PhD, Grahame J.
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016
 Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Month/Year of Review: May 2014 Date of Last Review: September New Drug Evaluation: Sucrofferic Oxyhydroxide (Velphoro )
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
OPEN. Masahiro Yoshikawa 1,2, Osamu Takase 1,2, Taro Tsujimura
 www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
CKD and CVD. Jamal Salameh, MD, FACP, FASN First Coast Nephrology
 CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015)
 Final Version (01/03/2015)") CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015) Dr Simon Steddon, Consultant Nephrologist, Guy s and St Thomas NHS Foundation Trust, London Dr Edward Sharples,
CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015) Dr Simon Steddon, Consultant Nephrologist, Guy s and St Thomas NHS Foundation Trust, London Dr Edward Sharples,
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE ON MAINTENANCE DIALYSIS THERAPY
 UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
BONE AND MINERAL METABOLISM in the PD PATIENT
 BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
Renal Association Clinical Practice Guideline in Mineral and Bone Disorders in CKD
 Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
A new era in phosphate binder therapy: What are the options?
 http://www.kidney-international.org & 2006 International Society of Nephrology A new era in phosphate binder therapy: What are the options? IB Salusky 1 1 Department of Pediatrics, David Geffen School
http://www.kidney-international.org & 2006 International Society of Nephrology A new era in phosphate binder therapy: What are the options? IB Salusky 1 1 Department of Pediatrics, David Geffen School
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Kobe University Repository : Kernel
 Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
The hart and bone in concert
 The hart and bone in concert Piotr Rozentryt III Department of Cardiology, Silesian Centre for Heart Disease, Silesian Medical University, Zabrze, Poland Disclosure Research grant, speaker`s fee, travel
The hart and bone in concert Piotr Rozentryt III Department of Cardiology, Silesian Centre for Heart Disease, Silesian Medical University, Zabrze, Poland Disclosure Research grant, speaker`s fee, travel
Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD
pth: ein neuer Marker für CKD-MBD") Biomarker der kardio-renalen Achse Mannheim, 20. Januar 2017 Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD Prof. Dr. med. Thomas Bernd Dschietzig Immundiagnostik AG, Bensheim Med. Klinik m.
Biomarker der kardio-renalen Achse Mannheim, 20. Januar 2017 Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD Prof. Dr. med. Thomas Bernd Dschietzig Immundiagnostik AG, Bensheim Med. Klinik m.
CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism
 CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism Pieter Evenepoel Nephrology, Dialysis, and Transplantation University Hospitals Leuven April 2017, FMC Herbeumont Disclosures Research support:
CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism Pieter Evenepoel Nephrology, Dialysis, and Transplantation University Hospitals Leuven April 2017, FMC Herbeumont Disclosures Research support:
Sevelamer hydrochloride: a calcium- and metal-free phosphate binder
 DRUG PROFILE Sevelamer hydrochloride: a calcium- and metal-free phosphate binder Anthony J Bleyer & James Balwit Author for correspondence Wake Forest University School of Medicine, Section on Nephrology,
DRUG PROFILE Sevelamer hydrochloride: a calcium- and metal-free phosphate binder Anthony J Bleyer & James Balwit Author for correspondence Wake Forest University School of Medicine, Section on Nephrology,
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL
 PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
Hemodialysis: slightly beyond basics Dialysate calcium and magnesium concentrations
 Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Kidney-Bone and Beyond: An Academic Career
 Kidney-Bone and Beyond: An Academic Career Isidro B. Salusky, M.D. Distinguished Professor of Pediatrics Chief, Division of Pediatric Nephrology Director, Clinical Translational Research Center Associate
Kidney-Bone and Beyond: An Academic Career Isidro B. Salusky, M.D. Distinguished Professor of Pediatrics Chief, Division of Pediatric Nephrology Director, Clinical Translational Research Center Associate
Bone Markers and Vascular Calcification in CKD-MBD
 Bone Markers and Vascular Calcification in CKD-MBD Pierre Delanaye, MD, PhD Department of Nephrology, Dialysis, Transplantation CHU Sart Tilman University of Liège BELGIUM Bone Markers and Vascular Calcification
Bone Markers and Vascular Calcification in CKD-MBD Pierre Delanaye, MD, PhD Department of Nephrology, Dialysis, Transplantation CHU Sart Tilman University of Liège BELGIUM Bone Markers and Vascular Calcification
ISN Mission: Advancing the diagnosis, treatment and prevention of kidney diseases in the developing and developed world
 ISN Mission: Advancing the diagnosis, treatment and prevention of kidney diseases in the developing and developed world Nutrition in Kidney Disease: How to Apply Guidelines to Clinical Practice? T. Alp
ISN Mission: Advancing the diagnosis, treatment and prevention of kidney diseases in the developing and developed world Nutrition in Kidney Disease: How to Apply Guidelines to Clinical Practice? T. Alp
Velphoro (sucroferric oxyhydroxide)
") STRENGTH DOSAGE FORM ROUTE GPID 500mg chewable tablet oral 36003 MANUFACTURER Fresenius Medical Care North America INDICATION(S) For the control of serum phosphorus levels in patients with chronic kidney
STRENGTH DOSAGE FORM ROUTE GPID 500mg chewable tablet oral 36003 MANUFACTURER Fresenius Medical Care North America INDICATION(S) For the control of serum phosphorus levels in patients with chronic kidney
Protocol GTC : A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients.
 in Chronic Kidney Disease Patients.") Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
Drugs for the treatment of secondary hyperparathyroidism and hyperphosphataemia
 NSW Therapeutic Advisory Group Level 5, 376 Victoria Street PO Box 766 Darlinghurst NSW 2010 Phone: 61 2 8382 2852 Fax: 61 2 8382 3529 Email: nswtag@stvincents.com.au www.nswtag.org.au Drugs for the treatment
NSW Therapeutic Advisory Group Level 5, 376 Victoria Street PO Box 766 Darlinghurst NSW 2010 Phone: 61 2 8382 2852 Fax: 61 2 8382 3529 Email: nswtag@stvincents.com.au www.nswtag.org.au Drugs for the treatment
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality
 Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls
 O. Mehls") Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls Division of Pediatric Nephrology University Hospital for Children and Adolescents Heidelberg, Germany Definition
Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls Division of Pediatric Nephrology University Hospital for Children and Adolescents Heidelberg, Germany Definition
TRANSPARENCY COMMITTEE OPINION. 22 July 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 22 July 2009 PHOSPHOSORB 660 mg, film-coated tablet Container of 200 (CIP: 381 466-0) Applicant: FRESENIUS MEDICAL
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 22 July 2009 PHOSPHOSORB 660 mg, film-coated tablet Container of 200 (CIP: 381 466-0) Applicant: FRESENIUS MEDICAL
THE IMPACT OF SERUM PHOSPHATE LEVELS IN CKD-MBD PROGRESSION
 THE IMPACT OF SERUM PHOSPHATE LEVELS IN CKD-MBD PROGRESSION Mario Cozzolino, MD, PhD, Fellow of the European Renal Association Department of Health Sciences University of Milan Renal Division & Laboratory
THE IMPACT OF SERUM PHOSPHATE LEVELS IN CKD-MBD PROGRESSION Mario Cozzolino, MD, PhD, Fellow of the European Renal Association Department of Health Sciences University of Milan Renal Division & Laboratory
PROTECTING HEART, VESSELS, AND BONE: NEW WAYS TO CONTROL PHOSPHORUS
 PROTECTING HEART, VESSELS, AND BONE: NEW WAYS TO CONTROL PHOSPHORUS This symposium took place on 22 th May 2016 as part of the European Renal Association - European Dialysis and Transplant Association
PROTECTING HEART, VESSELS, AND BONE: NEW WAYS TO CONTROL PHOSPHORUS This symposium took place on 22 th May 2016 as part of the European Renal Association - European Dialysis and Transplant Association
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416)
") Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
New Medicines Profile. December 2013 Issue No. 13/04. Colestilan
 New Medicines Profile December 2013 Issue. 13/04 Concise evaluated information to support the managed entry of new medicines in the NHS Summary (BindRen ) is an oral, non-absorbed, non-calcium, nonmetallic
New Medicines Profile December 2013 Issue. 13/04 Concise evaluated information to support the managed entry of new medicines in the NHS Summary (BindRen ) is an oral, non-absorbed, non-calcium, nonmetallic
K/DOQI-recommended intact PTH levels do not prevent low-turnover bone disease in hemodialysis patients
 http://www.kidney-international.org & 2008 International Society of Nephrology original article see commentary on page 674 K/DOQI-recommended intact PTH levels do not prevent low-turnover bone disease
http://www.kidney-international.org & 2008 International Society of Nephrology original article see commentary on page 674 K/DOQI-recommended intact PTH levels do not prevent low-turnover bone disease
Renal Osteodystrophy. Chapter 6. I. Introduction. Classification of Bone Disease. Eric W. Young
 Chapter 6 Renal Osteodystrophy Eric W. Young I. Introduction Renal osteodystrophy refers to bone disease that occurs in patients with kidney disease. Bone disease occurs across the full spectrum of kidney
Chapter 6 Renal Osteodystrophy Eric W. Young I. Introduction Renal osteodystrophy refers to bone disease that occurs in patients with kidney disease. Bone disease occurs across the full spectrum of kidney
Calcium x phosphate product
 Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Calcium x phosphate product GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL
Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Calcium x phosphate product GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL
Pediatric Nutrition and Kidney Disease
 Pediatric Nutrition and Kidney Disease Loai Eid, MD, MSHS, FAAP Consultant Pediatric Nephrologist Pediatric Nephrology & Hypertension Division Chief Dubai Hospital - DHA 26 th October, 2017 Objectives
Pediatric Nutrition and Kidney Disease Loai Eid, MD, MSHS, FAAP Consultant Pediatric Nephrologist Pediatric Nephrology & Hypertension Division Chief Dubai Hospital - DHA 26 th October, 2017 Objectives
The Parsabiv Beginner s Book
 The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
Outline. The Role of Vitamin D in CKD. Essential Role of Vitamin D. Mechanism of Action of Vit D. Mechanism of Action of Vit D 7/16/2010
 Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.PMN.04 Effective Date: 11.15.17 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: CP.PMN.04 Effective Date: 11.15.17 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy for important
Reversal of adynamic bone disease by lowering of dialysate calcium
 http://www.kidney-international.org & 26 International Society of Nephrology original article Reversal of adynamic bone disease by lowering of dialysate calcium A Haris 1, DJ Sherrard 2 and G Hercz 3 1
http://www.kidney-international.org & 26 International Society of Nephrology original article Reversal of adynamic bone disease by lowering of dialysate calcium A Haris 1, DJ Sherrard 2 and G Hercz 3 1
Calcium, phosphate and parathyroid metabolism in kidney transplanted patients
 DOI 10.1007/s11255-009-9631-0 NEPHROLOGY - ORIGINAL PAPER Calcium, phosphate and parathyroid metabolism in kidney transplanted patients Csaba Ambrus Æ Miklos Zsolt Molnar Æ Maria Eszter Czira Æ Laszlo
DOI 10.1007/s11255-009-9631-0 NEPHROLOGY - ORIGINAL PAPER Calcium, phosphate and parathyroid metabolism in kidney transplanted patients Csaba Ambrus Æ Miklos Zsolt Molnar Æ Maria Eszter Czira Æ Laszlo
Contents. Authors Name: Christopher Wong: Consultant Nephrologist Anne Waddington: Renal Pharmacist Eimear Fegan : Renal Dietitian
 Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
Complications of Chronic Kidney Disease: Anemia, Mineral Metabolism, and Cardiovascular Disease
 Med Clin N Am 89 (2005) 549 561 Complications of Chronic Kidney Disease: Anemia, Mineral Metabolism, and Cardiovascular Disease Shona Pendse, MD, Ajay K. Singh, MB, MRCP(UK)* Renal Division, Brigham and
Med Clin N Am 89 (2005) 549 561 Complications of Chronic Kidney Disease: Anemia, Mineral Metabolism, and Cardiovascular Disease Shona Pendse, MD, Ajay K. Singh, MB, MRCP(UK)* Renal Division, Brigham and
Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism
 The Journal of International Medical Research 2011; 39: 978 987 Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism J NARANDA 1,2, R EKART
The Journal of International Medical Research 2011; 39: 978 987 Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism J NARANDA 1,2, R EKART
Effect of lanthanum carbonate and calcium acetate in the treatment of hyperphosphatemia in patients of chronic kidney disease
 Research Article Effect of lanthanum and calcium acetate in the treatment of hyperphosphatemia in patients of chronic kidney disease P. Thomas Scaria, Reneega Gangadhar 1, Ramdas Pisharody 2 ABSTRACT Departments
Research Article Effect of lanthanum and calcium acetate in the treatment of hyperphosphatemia in patients of chronic kidney disease P. Thomas Scaria, Reneega Gangadhar 1, Ramdas Pisharody 2 ABSTRACT Departments
SCIENTIFIC DISCUSSION
 European Medicines Agency London, 01 June 2007 Product Name : Renagel Procedure No: EMEA/H/C/000254/II/56 SCIENTIFIC DISCUSSION 1/11 1. Introduction Renagel (sevelamer), a non-absorbed, calcium and metal-free
European Medicines Agency London, 01 June 2007 Product Name : Renagel Procedure No: EMEA/H/C/000254/II/56 SCIENTIFIC DISCUSSION 1/11 1. Introduction Renagel (sevelamer), a non-absorbed, calcium and metal-free
The Skeletal Response to Aging: There s No Bones About It!
 The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale. Maurizio Gallieni Università degli Studi di Milano
 Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Sevelamer carbonate in the treatment of hyperphosphatemia in patients with chronic kidney disease on hemodialysis
 REVIEW Sevelamer carbonate in the treatment of hyperphosphatemia in patients with chronic kidney disease on hemodialysis Vincenzo Savica 1,2 Domenico Santoro 1 Paolo Monardo 2 Agostino Mallamace 1 Guido
REVIEW Sevelamer carbonate in the treatment of hyperphosphatemia in patients with chronic kidney disease on hemodialysis Vincenzo Savica 1,2 Domenico Santoro 1 Paolo Monardo 2 Agostino Mallamace 1 Guido
Stefanos K. Roumeliotis. Department of Nephrology, Medical School Democritus University of Thrace, Alexandroupolis, Greece. Stefanos K.
 Department of Nephrology, Medical School Democritus University of Thrace, Alexandroupolis, Greece Passive, degenerative accumulation process of Ca ++ /P +++ without treatment options Active, complex, condition:
Department of Nephrology, Medical School Democritus University of Thrace, Alexandroupolis, Greece Passive, degenerative accumulation process of Ca ++ /P +++ without treatment options Active, complex, condition:
Phosphate binders and metabolic acidosis in patients undergoing maintenance hemodialysis sevelamer hydrochloride, calcium carbonate, and bixalomer
 Hemodialysis International 2015; 19:5459 Phosphate binders and metabolic acidosis in patients undergoing maintenance hemodialysis sevelamer hydrochloride, calcium carbonate, and bixalomer Toru SANAI, 1
Hemodialysis International 2015; 19:5459 Phosphate binders and metabolic acidosis in patients undergoing maintenance hemodialysis sevelamer hydrochloride, calcium carbonate, and bixalomer Toru SANAI, 1
chapter 1 & 2009 KDIGO
 http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
Pediatric CKD-MBD: pathophysiology and management
 Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Improved Assessment of Aortic Calcification in Japanese Patients Undergoing Maintenance Hemodialysis
 ORIGINAL ARTICLE Improved Assessment of Aortic Calcification in Japanese Patients Undergoing Maintenance Hemodialysis Masaki Ohya 1, Haruhisa Otani 2,KeigoKimura 3, Yasushi Saika 4, Ryoichi Fujii 4, Susumu
ORIGINAL ARTICLE Improved Assessment of Aortic Calcification in Japanese Patients Undergoing Maintenance Hemodialysis Masaki Ohya 1, Haruhisa Otani 2,KeigoKimura 3, Yasushi Saika 4, Ryoichi Fujii 4, Susumu
Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis patients
 original article http://www.kidney-international.org & 2007 International Society of Nephrology Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis
original article http://www.kidney-international.org & 2007 International Society of Nephrology Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis
Cardiovascular Disease in CKD. Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center
 Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
02/27/2018. Objectives. To Replace or Not to Replace: Nutritional Vitamin D in Dialysis.
 To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
Original epidemiologic studies 1 have suggested that approximately
 Factors for Increased Morbidity and Mortality in Uremia: Hyperphosphatemia Nathan W. Levin, Frank A. Gotch, and Martin K. Kuhlmann Hyperphosphatemia is a metabolic abnormality present in the majority of
Factors for Increased Morbidity and Mortality in Uremia: Hyperphosphatemia Nathan W. Levin, Frank A. Gotch, and Martin K. Kuhlmann Hyperphosphatemia is a metabolic abnormality present in the majority of
David Ramenofsky, MD Bryan Kestenbaum, MD
 Association of Serum Phosphate Concentration with Vascular Calcification in Patients Free of Chronic Kidney Disease: The Multi Ethnic Study of Atherosclerosis David Ramenofsky, MD Bryan Kestenbaum, MD
Association of Serum Phosphate Concentration with Vascular Calcification in Patients Free of Chronic Kidney Disease: The Multi Ethnic Study of Atherosclerosis David Ramenofsky, MD Bryan Kestenbaum, MD
Normal kidneys filter large amounts of organic
 ORIGINAL ARTICLE - NEPHROLOGY Effect Of Lanthanum Carbonate vs Calcium Acetate As A Phosphate Binder In Stage 3-4 CKD- Treat To Goal Study K.S. Sajeev Kumar (1), M K Mohandas (1), Ramdas Pisharody (1),
ORIGINAL ARTICLE - NEPHROLOGY Effect Of Lanthanum Carbonate vs Calcium Acetate As A Phosphate Binder In Stage 3-4 CKD- Treat To Goal Study K.S. Sajeev Kumar (1), M K Mohandas (1), Ramdas Pisharody (1),
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet:
 Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Literature Scan: Phosphate Binders
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Title:Hyperphosphatemia as an Independent Risk Factor of Coronary Artery Calcification Progression in Peritoneal Dialysis Patients
 Author's response to reviews Title:Hyperphosphatemia as an Independent Risk Factor of Coronary Artery Calcification Progression in Peritoneal Dialysis Patients Authors: Da Shang (sdshangda@163.com) Qionghong
Author's response to reviews Title:Hyperphosphatemia as an Independent Risk Factor of Coronary Artery Calcification Progression in Peritoneal Dialysis Patients Authors: Da Shang (sdshangda@163.com) Qionghong
Metabolic Bone Disease (Past, Present and Future Challenges in the Management)
") Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
TITLE: Sevelamer Hydrochloride for the Treatment of Patients with Chronic Kidney Disease: A Review of the Clinical Effectiveness
 TITLE: Hydrochloride for the Treatment of Patients with Chronic Kidney Disease: A Review of the Clinical Effectiveness DATE: 08 September 2009 CONTEXT AND POLICY ISSUES: Patients with end-stage chronic
TITLE: Hydrochloride for the Treatment of Patients with Chronic Kidney Disease: A Review of the Clinical Effectiveness DATE: 08 September 2009 CONTEXT AND POLICY ISSUES: Patients with end-stage chronic
Chapter 5: Evaluation and treatment of kidney transplant bone disease Kidney International (2009) 76 (Suppl 113), S100 S110; doi: /ki.2009.
 76 (Suppl 113), S100 S110; doi: /ki.2009.") http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD
 The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
Introduction/objective: Adinamic bone disease (ABD) is a common finding in peritoneal. dialysis (PD) and is associated with a
 is a common finding in peritoneal. dialysis (PD) and is associated with a") Original Article Low-calcium peritoneal dialysis solution is effective in bringing PTH levels to the range recommended by current guidelines in patients with PTH levels < 150 pg/dl Authors Thyago Proença
Original Article Low-calcium peritoneal dialysis solution is effective in bringing PTH levels to the range recommended by current guidelines in patients with PTH levels < 150 pg/dl Authors Thyago Proença
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment
 Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Prevalence and Pattern of Mineral Bone Disorder in Chronic Kidney Disease Patients Using Serum
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Prevalence and Pattern of Mineral Bone Disorder in Chronic Kidney Disease Patients Using Serum
Bone impairment in pediatric CKD
 A 16-year old girl arriving in the emergency room for seizures No significant medical past except orthopaedic surgery for bilateral genu valgum without any obvious etiology at the age of 14 years Bone
A 16-year old girl arriving in the emergency room for seizures No significant medical past except orthopaedic surgery for bilateral genu valgum without any obvious etiology at the age of 14 years Bone
An overview on adynamic bone disease clinical and therapeutical approaches
 2014/2015 Mariana Barata Santos Barreira de Jesus An overview on adynamic bone disease clinical and therapeutical approaches março, 2015 Mariana Barata Santos Barreira de Jesus An overview on adynamic
2014/2015 Mariana Barata Santos Barreira de Jesus An overview on adynamic bone disease clinical and therapeutical approaches março, 2015 Mariana Barata Santos Barreira de Jesus An overview on adynamic
Malnutrition and Role of Nutrition in BMD:CKD
 Malnutrition and Role of Nutrition in BMD:CKD PNDS Continuing Nutrition Education Seminar Saturday, 30 th November 2013 Fayza Khan MSC (Foods and Nutrition) R.D President,PNDS Outline Objective Malnutrition
Malnutrition and Role of Nutrition in BMD:CKD PNDS Continuing Nutrition Education Seminar Saturday, 30 th November 2013 Fayza Khan MSC (Foods and Nutrition) R.D President,PNDS Outline Objective Malnutrition
Nutrition and Renal Disease Update
 Nutrition and Renal Disease Update Denis FOUQUE Department of Nephrology Centre de Recherche en Nutrition Humaine University Claude Bernard Lyon - France What have we learned? 1. Chronic kidney disease:
Nutrition and Renal Disease Update Denis FOUQUE Department of Nephrology Centre de Recherche en Nutrition Humaine University Claude Bernard Lyon - France What have we learned? 1. Chronic kidney disease: