Surgical Indications of Infective Endocarditis in Children
|
|
|
- Janice Harvey
- 6 years ago
- Views:
Transcription
1 2016 Annual Spring Scientific Conference of the KSC April 15-16, 2016 Surgical Indications of Infective Endocarditis in Children Cheul Lee, MD Pediatric and Congenital Cardiac Surgery Seoul St. Mary s Hospital College of Medicine, The Catholic University of Korea
2 Increasing Role of Surgery in Infective Endocarditis The proportion of infective endocarditis patients undergoing surgery has increased over time to reach approximately 50%. Circulation 2015;132:

3 Native Valve Endocarditis

4 Prosthetic Valve Endocarditis

5 Catheter Related Endocarditis
6 Surgical Considerations for Infective Endocarditis Indications for surgery Timing of surgery Surgical procedures
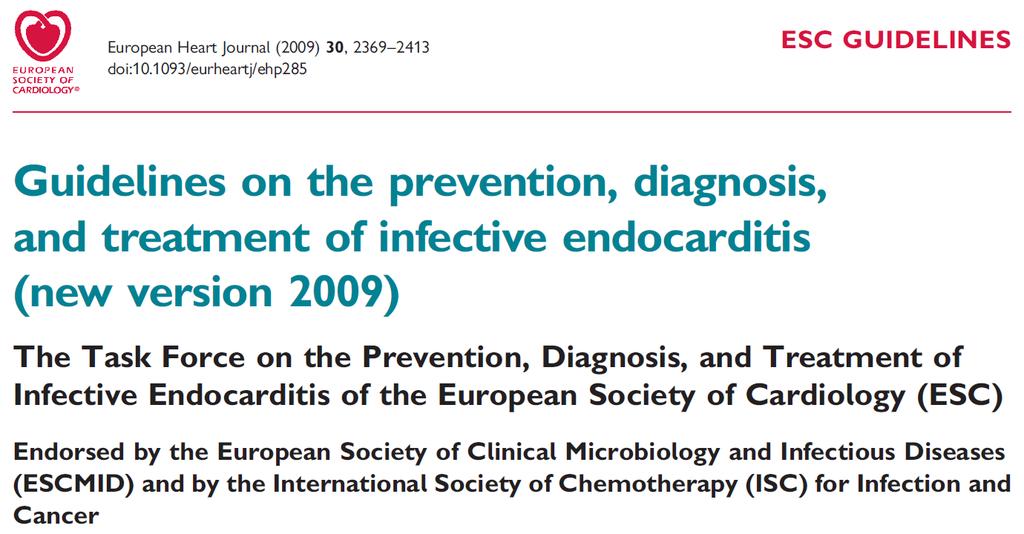
7 Indications for Surgery Heart failure Uncontrolled infection Prevention of embolism
8 Timing of Surgery Emergency: within 24 hours Urgent: within a few days Elective: after 1-2 weeks of antibiotic therapy
9 Goals of Surgery Complete removal of infected tissues Restoration of hemodynamic abnormality
10 Available Guidelines AHA guideline for infective endocarditis in adults (2015) AHA guideline for infective endocarditis in childhood (2015) AHA/ACC guideline for the management of patients with valvular heart disease (2014) ESC guidelines on the prevention, diagnosis, and treatment of infective endocarditis (2009) STS clinical practice guideline for surgical management of endocarditis (2011)
11 J Am Coll Cardiol 2014;63:
12 The First Step Cardiothoracic surgical consultation should be obtained rapidly after the diagnosis of infective endocarditis. Decisions about timing of surgical intervention should be made by a multispecialty Heart Valve Team of cardiology, cardiothoracic surgery, and infectious disease specialists. J Am Coll Cardiol 2014;63:
13 J Am Coll Cardiol 2014;63:
14 Circulation 2015;132:
15 Valve Surgery in Patients With Right-Sided Infective Endocarditis Surgical intervention is reasonable for patients with certain complications (Class IIa; Level C). Valve repair rather than replacement should be performed when feasible (Class I; Level C). If valve replacement is performed, then an individualized choice of prosthesis by the surgeon is reasonable (Class IIa; Level C). It is reasonable to avoid surgery when possible in patients who are injection drug users (Class IIa; Level C). Circulation 2015;132:
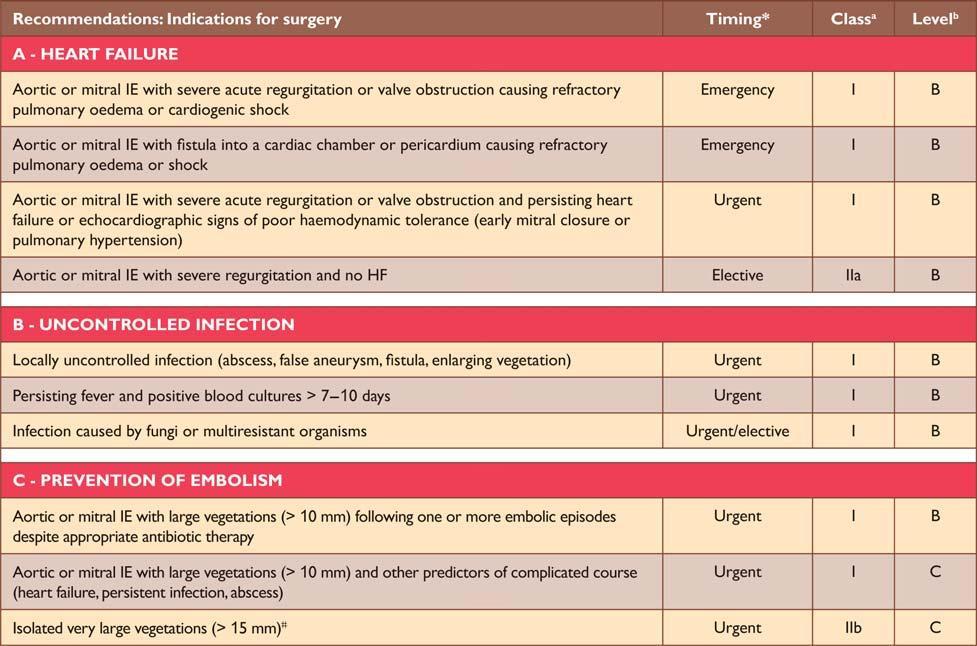
16 Valve Surgery in Patients With Prior Emboli/Hemorrhage/Stroke Valve surgery may be considered in IE patients with stroke or subclinical cerebral emboli and residual vegetation without delay if intracranial hemorrhage has been excluded by imaging studies and neurological damage is not severe (ie, coma) (Class IIb; Level B). In patients with major ischemic stroke or intracranial hemorrhage, it is reasonable to delay valve surgery for at least 4 weeks (Class IIa; Level B). Circulation 2015;132:
17 AHA Scientific Statement Infective Endocarditis in Childhood: 2015 Update A Scientific Statement From the American Heart Association Robert S. Baltimore, MD, Chair; Michael Gewitz, MD, FAHA, Vice Chair; Larry M. Baddour, MD, FAHA; Lee B. Beerman, MD; Mary Anne Jackson, MD; Peter B. Lockhart, DDS; Elfriede Pahl, MD, FAHA; Gordon E. Schutze, MD; Stanford T. Shulman, MD; Rodney Willoughby, Jr, MD; on behalf of the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young and the Council on Cardiovascular and Stroke Nursing In 2002, the American Heart Association (AHA) published Unique Features of Infective Endocarditis in Childhood, 1 which reviewed epidemiology, pathogenesis, diagnosis, clinical and laboratory findings, treatment, and prevention of infective endocarditis (IE) with particular attention to children. Since that time, other AHA reports have focused on new recommendations for treatment of IE in adults (in ) and on major changes Circulation 2015;132: Classification of Recommendations In pediatrics, there are not likely to be any randomized controlled trials for treatment of IE, which posed a challenge for the writing group in compiling recommendations. Therefore, many of the indications are based on consensus. In cases of strong consensus that an intervention be considered as standard-ofcare practice with scientific evidence, interventions were des-
18 Infective Endocarditis in Childhood: 2015 Update Prophylactic surgery to prevent a primary embolic event is not recommended given the lack of proven benefit and long-term risks of valve replacement in childhood (Class III; Level C). Surgery may be considered for patients with relapsing prosthetic valve endocarditis even if valvar function remains intact after prolonged medical therapy (Class IIb; Level B). Circulation 2015;132:
19
20 Eur Heart J 2009;30:
21 N Engl J Med 2012;366:
22 N Engl J Med 2012;366:
23 Eur Heart J 2009;30:
24 Eur Heart J 2009;30:
25 Ann Thorac Surg 2011;91:2012-9
26 Native Aortic Valve Endocarditis A mechanical or stented tissue valve is reasonable in native aortic valve endocarditis. (Class IIa, Level B) A homograft may be considered in native aortic valve endocarditis. (Class IIb, Level B) Ann Thorac Surg 2011;91:2012-9
27 Prosthetic Aortic Valve Endocarditis In patients with aortic PVE limited to the prosthesis without aortic root abscess, and no annular destruction, it is reasonable to implant a mechanical or stented tissue valve. (Class IIa, Level B) A homograft can be beneficial in aortic PVE when periannular abscess or extensive ventricular-aortic discontinuity is present, or when aortic root replacement/reconstruction is necessary because of annular destruction or destruction of anatomical structures. (Class IIa, Level B) Ann Thorac Surg 2011;91:2012-9
28 Native Mitral Valve Endocarditis When technically feasible, mitral valve repair is recommended to treat native mitral valve endocarditis. (Class I, Level B) When surgery is indicated, mechanical or stented tissue valves can be useful for mitral valve replacement. (Class IIa, Level B) Ann Thorac Surg 2011;91:2012-9
29 Prosthetic Mitral Valve Endocarditis When surgery is indicated for prosthetic mitral valve endocarditis, either mechanical or stented tissue valves may be considered for valve replacement. (Class IIb, Level C) Ann Thorac Surg 2011;91:2012-9
30
31 Chicago Experience N = 34 Mean age of 10.7 years 60% congenital heart disease MV > AV > TV > RV-PA conduit Native > prosthetic Replacement > repair > Ross 15% operative mortality (infants, prematurity, fungus) Ann Thorac Surg 2013;96:171-5
32
33 Texas Experience N = 46 Median age of 8.7 years 54% congenital heart disease TV > MV > AV > RV-PA conduit Native > prosthetic 76% early surgery (< 7 days of the diagnosis) Repair > replacement > Ross 2% operative mortality 10-year survival of 81% J Thorac Cardiovasc Surg 2013;146:506-11
34 J Thorac Cardiovasc Surg 2016;151:432-41
35 RV-PA Conduit Endocarditis Bovine jugular vein grafts (Contegra) are associated with a 9-fold greater risk of late endocarditis compared with other RV-PA conduits. J Thorac Cardiovasc Surg 2016;151:432-41
36
37 Percutaneous PV Endocarditis There is a higher incidence of endocarditis in patients with percutaneous pulmonary valve (Melody) implantation compared with surgical pulmonary valves. When analyzing the type of valves regardless of the implantation technique, IE was more frequent in patients with bovine jugular vein valves (ie, Contegra and Melody) compared with others. J Thorac Cardiovasc Surg 2014;148:2253-9
38 Summary 1. Guidelines for surgical management of pediatric IE are mostly an extension of guidelines for management of adult IE. 2. Decisions regarding surgery for IE are complex and should be determined by a multispecialty team with expertise in cardiology, imaging, cardiothoracic surgery, and infectious diseases. 3. Proper patient selection and optimal surgical timing are crucial for improved outcomes. 4. There is an increased risk of endocarditis in patients receiving a bovine jugular vein valve either surgically (Contegra) or by the transcatheter technique (Melody).
General management of infective endocarditis
 General management of infective endocarditis Team approach in infective endocarditis Gilbert Habib La Timone Hospital Marseille - France Eurovalves Barcelona 2017 The echolab «Heart Team" Infective Endocarditis
General management of infective endocarditis Team approach in infective endocarditis Gilbert Habib La Timone Hospital Marseille - France Eurovalves Barcelona 2017 The echolab «Heart Team" Infective Endocarditis
Update on the prevention, diagnosis and management of Infective Endocarditis (IE)
") Update on the prevention, diagnosis and management of Infective Endocarditis (IE) Dr.Ahmed Yahya Mohammed Alarhabi MD, MsC,FcUSM,FACC,MAHA Consultant Interventional Cardiologist Head of Cardiac Center
Update on the prevention, diagnosis and management of Infective Endocarditis (IE) Dr.Ahmed Yahya Mohammed Alarhabi MD, MsC,FcUSM,FACC,MAHA Consultant Interventional Cardiologist Head of Cardiac Center
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Heart on Fire: Infective Endocarditis. Objectives. Disclosure 8/27/2018. Mary McGreal DNP, RN, ANP-c, CCRN
 Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
IE with cerebral hemorrhage
 IE with cerebral hemorrhage Gilbert Habib / Patrizio Lancellotti La Timone Hospital Marseille - France Palermo, 26 April 2018 Case report: aortic bioprosthetic IE History of the disease 75 year-old man
IE with cerebral hemorrhage Gilbert Habib / Patrizio Lancellotti La Timone Hospital Marseille - France Palermo, 26 April 2018 Case report: aortic bioprosthetic IE History of the disease 75 year-old man
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
Case Studies in Complex Endocarditis
 Case Studies in Complex Endocarditis Vera H. Rigolin, MD Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern Memorial Hospital
Case Studies in Complex Endocarditis Vera H. Rigolin, MD Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern Memorial Hospital
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Re-do aortic valve replacement after previous homograft aortic root replacement
 Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
April 16, 09:00-09:15 중앙대학교 윤신원
 April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
PRINCIPLES OF ENDOCARDITIS
 015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kang D-H, Kim Y-J, Kim S-H, et al. Early surgery versus conventional
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kang D-H, Kim Y-J, Kim S-H, et al. Early surgery versus conventional
Management of complex CHD in adults
 Management of complex CHD in adults Victor Tsang Society of Thoracic Surgeons of Thailand 2016 The impact of infant cardiac surgery Over 90 % of infants born with CHD will reach adulthood By 2010, adults
Management of complex CHD in adults Victor Tsang Society of Thoracic Surgeons of Thailand 2016 The impact of infant cardiac surgery Over 90 % of infants born with CHD will reach adulthood By 2010, adults
A Loeys-Dietz Patient with a Trans-Atlantic Odyssey. Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4
 1 2 3 A Loeys-Dietz Patient with a Trans-Atlantic Odyssey Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4 5 6 7 8 9 Thierry Carrel 1, Florian Schoenhoff 1 and Duke Cameron
1 2 3 A Loeys-Dietz Patient with a Trans-Atlantic Odyssey Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4 5 6 7 8 9 Thierry Carrel 1, Florian Schoenhoff 1 and Duke Cameron
Endocardite infectieuse
 Endocardite infectieuse 1. Raccourcir le traitement: jusqu où? 2. Proposer un traitement ambulatoire: à partir de quand? Endocardite infectieuse A B 90 P = 0.014 20 P = 0.0005 % infective endocarditis
Endocardite infectieuse 1. Raccourcir le traitement: jusqu où? 2. Proposer un traitement ambulatoire: à partir de quand? Endocardite infectieuse A B 90 P = 0.014 20 P = 0.0005 % infective endocarditis
Valve Endocarditis Indications and Timing of Surgery
 Valve Endocarditis Indications and Timing of Surgery Michele Di Mauro, MD, PhD Cardiac Surgeon and Cardiologist Heart Department,SS Annunziata H, Chieti, Italy What do the guidelines say? Heart Failure
Valve Endocarditis Indications and Timing of Surgery Michele Di Mauro, MD, PhD Cardiac Surgeon and Cardiologist Heart Department,SS Annunziata H, Chieti, Italy What do the guidelines say? Heart Failure
Indications chirurgicales dans l endocardite infectieuse
 Indications chirurgicales dans l endocardite infectieuse Bruno Hoen ICE AEPEI Agenda Indications of surgery in IE: current guidelines Impact of early valve surgery (EVS) on the prognosis of IE: is the
Indications chirurgicales dans l endocardite infectieuse Bruno Hoen ICE AEPEI Agenda Indications of surgery in IE: current guidelines Impact of early valve surgery (EVS) on the prognosis of IE: is the
Modifiers of the clinical course of infective endocarditis
 Modifiers of the clinical course of infective endocarditis Ulrika Snygg-Martin M.D., Ph.D. Infectious Diseases Clinic Sahlgrenska University Hospital Gothenburg, Sweden Infective endocarditis : modifiers
Modifiers of the clinical course of infective endocarditis Ulrika Snygg-Martin M.D., Ph.D. Infectious Diseases Clinic Sahlgrenska University Hospital Gothenburg, Sweden Infective endocarditis : modifiers
Endocarditis and Its Complications: The Role of Echocardiography
 Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
(Ann Thorac Surg 2008;85:845 53)
") I Made Adi Parmana The utility of intraoperative TEE has become increasingly more evident as anesthesiologists, cardiologists, and surgeons continue to appreciate its potential application as an invaluable
I Made Adi Parmana The utility of intraoperative TEE has become increasingly more evident as anesthesiologists, cardiologists, and surgeons continue to appreciate its potential application as an invaluable
Endocarditis: Medical vs. Surgical Treatment. Nabin K. Shrestha, MD, MPH Infectious Diseases
 Endocarditis: Medical vs. Surgical Treatment Nabin K. Shrestha, MD, MPH Infectious Diseases Conflicts of interest Nothing to disclose 2 Complications of infective endocarditis Local complications Heart
Endocarditis: Medical vs. Surgical Treatment Nabin K. Shrestha, MD, MPH Infectious Diseases Conflicts of interest Nothing to disclose 2 Complications of infective endocarditis Local complications Heart
TRANSCATHETER VALVE IMPLANTATION IN THE RIGHT HEART
 TRANSCATHETER VALVE IMPLANTATION IN THE RIGHT HEART Dr Aphrodite Tzifa, MD(Res), FRCPCH Director, Paediatric and GUCH Cardiologist, Mitera Children's Hospital, Athens, Greece September 10, 2003 FAILURE
TRANSCATHETER VALVE IMPLANTATION IN THE RIGHT HEART Dr Aphrodite Tzifa, MD(Res), FRCPCH Director, Paediatric and GUCH Cardiologist, Mitera Children's Hospital, Athens, Greece September 10, 2003 FAILURE
Percutaneous Tricuspid Valve Therapies: The Next Frontier? Is the Tricuspid Valve Relevant? Data and Guidelines for TV Interventions
 Percutaneous Tricuspid Valve Therapies: The Next Frontier? Scott M Lilly, MD PhD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Outline Is the Tricuspid Valve Relevant? Data
Percutaneous Tricuspid Valve Therapies: The Next Frontier? Scott M Lilly, MD PhD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Outline Is the Tricuspid Valve Relevant? Data
TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE (PPVI)
") TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE (PPVI) BASIL D. THANOPOULOS MD, PhD Director Interventional Cardiology of CHD Euroclinic ATHENS - GREECE TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE
TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE (PPVI) BASIL D. THANOPOULOS MD, PhD Director Interventional Cardiology of CHD Euroclinic ATHENS - GREECE TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE
TAVR and Cardiac Surgeons
 TAVR and Cardiac Surgeons TAVR and Cardiac Surgeons Ragheb Hasan Consultant and Clinical Lead Cardiothoracic Surgeon Manchester Royal Infirmary, Oxford Road, Manchester UK Aortic Stenosis Is A Growing
TAVR and Cardiac Surgeons TAVR and Cardiac Surgeons Ragheb Hasan Consultant and Clinical Lead Cardiothoracic Surgeon Manchester Royal Infirmary, Oxford Road, Manchester UK Aortic Stenosis Is A Growing
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Transcatheter Mitral Valve Replacement How Close Are We?
 Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
MEDICAL POLICY SUBJECT: CARDIAC REHABILITATION
 MEDICAL POLICY PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Daniel C. DeSimone, MD Assistant Professor of Medicine
 Daniel C. DeSimone, MD Assistant Professor of Medicine Faculty photo will be placed here Desimone.Daniel@mayo.edu 2015 MFMER 3543652-1 Infective Endocarditis Mayo School of Continuous Professional Development
Daniel C. DeSimone, MD Assistant Professor of Medicine Faculty photo will be placed here Desimone.Daniel@mayo.edu 2015 MFMER 3543652-1 Infective Endocarditis Mayo School of Continuous Professional Development
Debate in CHD - When Should We
 Debate in CHD - When Should We Replace Pulmonary Valve? Lee, Jae Young Dept. of Pediatrics, Seoul Saint Mary s Hospital The Catholic University of Korea 14 yr/m, TOF repair (1yr) FC I PR Fraction - 48
Debate in CHD - When Should We Replace Pulmonary Valve? Lee, Jae Young Dept. of Pediatrics, Seoul Saint Mary s Hospital The Catholic University of Korea 14 yr/m, TOF repair (1yr) FC I PR Fraction - 48
Pulmonary Valve Replacement
 Indications/Timing and Type of Interventions: Pulmonary Valve Replacement Lars Sondergaard, MD, DMSc Professor of Cardiology Rigshospitalet Copenhagen, Denmark Case 15 years old girl with tetralogy of
Indications/Timing and Type of Interventions: Pulmonary Valve Replacement Lars Sondergaard, MD, DMSc Professor of Cardiology Rigshospitalet Copenhagen, Denmark Case 15 years old girl with tetralogy of
The pulmonary valve is the most common heart valve
 Biologic versus Mechanical Valve Replacement of the Pulmonary Valve After Multiple Reconstructions of the RVOT Tract S. Adil Husain, MD, and John Brown, MD Indiana University School of Medicine, Department
Biologic versus Mechanical Valve Replacement of the Pulmonary Valve After Multiple Reconstructions of the RVOT Tract S. Adil Husain, MD, and John Brown, MD Indiana University School of Medicine, Department
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Tricuspid Valve: The Not So Forgotten Valve. Manuel J Antunes Cardiothoracic Surgery Coimbra, Portugal
 The Tricuspid Valve: The Not So Forgotten Valve Manuel J Antunes Cardiothoracic Surgery Coimbra, Portugal No Conflicts of Interest to declare with regards to this subject 2 INCIDENCE OF TRICUSPID REGURGITATION
The Tricuspid Valve: The Not So Forgotten Valve Manuel J Antunes Cardiothoracic Surgery Coimbra, Portugal No Conflicts of Interest to declare with regards to this subject 2 INCIDENCE OF TRICUSPID REGURGITATION
Original Policy Date
 MP 7.01.111 Transcatheter Pulmonary Valve Implantation Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to
MP 7.01.111 Transcatheter Pulmonary Valve Implantation Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to
Challenging clinical situation
 Challenging clinical situation A young patient with prosthetic aortic valve endocarditis Gilbert Habib La Timone Hospital Marseille - France October 25 th 2014 Case report History of the disease Clinical
Challenging clinical situation A young patient with prosthetic aortic valve endocarditis Gilbert Habib La Timone Hospital Marseille - France October 25 th 2014 Case report History of the disease Clinical
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve
 Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
PROSTHETIC VALVE ENDOCARDITIS Dr Bernard Prendergast DM FRCP EUROVALVE CONGRESS MADRID NOVEMBER 2013
 PROSTHETIC VALVE ENDOCARDITIS Dr Bernard Prendergast DM FRCP EUROVALVE CONGRESS MADRID NOVEMBER 2013 Prosthetic Valve Endocarditis A Dangerous Disease Affects 1-6% of prosthetic valves Mechanical and biological
PROSTHETIC VALVE ENDOCARDITIS Dr Bernard Prendergast DM FRCP EUROVALVE CONGRESS MADRID NOVEMBER 2013 Prosthetic Valve Endocarditis A Dangerous Disease Affects 1-6% of prosthetic valves Mechanical and biological
Right-Sided Bacterial Endocarditis
 New Concepts in the Treatment of the Uncontrollable Infection Agustin Arbulu, M.D., Ali Kafi, M.D., Norman W. Thorns, M.D., and Robert F. Wilson, M.D. ABSTRACT Our experience with 25 patients with right-sided
New Concepts in the Treatment of the Uncontrollable Infection Agustin Arbulu, M.D., Ali Kafi, M.D., Norman W. Thorns, M.D., and Robert F. Wilson, M.D. ABSTRACT Our experience with 25 patients with right-sided
Surgical Options to Prevent and Treat Tricuspid Valve Regurgitation in Heart Transplant Recipients
 Surgical Options to Prevent and Treat Tricuspid Valve Regurgitation in Heart Transplant Recipients Alejandro Bertolotti, MD Favaloro Foundation Argentina Disclosure: Conflict Of Interest Nothing to disclose
Surgical Options to Prevent and Treat Tricuspid Valve Regurgitation in Heart Transplant Recipients Alejandro Bertolotti, MD Favaloro Foundation Argentina Disclosure: Conflict Of Interest Nothing to disclose
Diagnostic strategy. Dr Pilar Tornos Hospital Vall d Hebron Barcelona
 Diagnostic strategy Dr Pilar Tornos Hospital Vall d Hebron Barcelona Faculty disclosure Pilar Tornos I disclose the following financial relationships: Paid speaker for Recordati, Edwards. Diagnosis of
Diagnostic strategy Dr Pilar Tornos Hospital Vall d Hebron Barcelona Faculty disclosure Pilar Tornos I disclose the following financial relationships: Paid speaker for Recordati, Edwards. Diagnosis of
The changing landscape of infective endocarditis (IE)in congenital heart disease (CHD)
in congenital heart disease (CHD)") The changing landscape of infective endocarditis (IE)in congenital heart disease (CHD) Rekwan Sittiwangkul,MD Department of Pediatrics. Chiang Mai University Hospital, 24 th March 2018 Infective endocarditis
The changing landscape of infective endocarditis (IE)in congenital heart disease (CHD) Rekwan Sittiwangkul,MD Department of Pediatrics. Chiang Mai University Hospital, 24 th March 2018 Infective endocarditis
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
An anterior aortoventriculoplasty, known as the Konno-
 The Konno-Rastan Procedure for Anterior Aortic Annular Enlargement Mark E. Roeser, MD An anterior aortoventriculoplasty, known as the Konno-Rastan procedure, is a useful tool for the cardiac surgeon. Originally,
The Konno-Rastan Procedure for Anterior Aortic Annular Enlargement Mark E. Roeser, MD An anterior aortoventriculoplasty, known as the Konno-Rastan procedure, is a useful tool for the cardiac surgeon. Originally,
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease
 2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
Mitral valve infective endocarditis (IE) is the most
 is the most") Mitral Valve Replacement for Infective Endocarditis With Annular Abscess: Annular Reconstruction Gregory J. Bittle, MD, Murtaza Y. Dawood, MD, and James S. Gammie, MD Mitral valve infective endocarditis
Mitral Valve Replacement for Infective Endocarditis With Annular Abscess: Annular Reconstruction Gregory J. Bittle, MD, Murtaza Y. Dawood, MD, and James S. Gammie, MD Mitral valve infective endocarditis
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
MitraClip: Why, How, and For Whom?
 MitraClip: Why, How, and For Whom? Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief, JAMA Cardiology
MitraClip: Why, How, and For Whom? Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief, JAMA Cardiology
Clinical Practice Guidelines and the Under Treatment of Concomitant AF Vinay Badhwar, MD
 Clinical Practice Guidelines and the Under Treatment of Concomitant AF Vinay Badhwar, MD Gordon F. Murray Professor and Chairman Department of Cardiovascular & Thoracic Surgery WVU Heart and Vascular Institute
Clinical Practice Guidelines and the Under Treatment of Concomitant AF Vinay Badhwar, MD Gordon F. Murray Professor and Chairman Department of Cardiovascular & Thoracic Surgery WVU Heart and Vascular Institute
The Journal of Thoracic and Cardiovascular Surgery
 Accepted Manuscript The Ross procedure: time to re-evaluate the guidelines Martin Misfeld, MD PhD, Michael A. Borger, MD PhD PII: S0022-5223(18)31853-1 DOI: 10.1016/j.jtcvs.2018.07.014 Reference: YMTC
Accepted Manuscript The Ross procedure: time to re-evaluate the guidelines Martin Misfeld, MD PhD, Michael A. Borger, MD PhD PII: S0022-5223(18)31853-1 DOI: 10.1016/j.jtcvs.2018.07.014 Reference: YMTC
TREATMENT OF ENDOCARDITIS: Destruction and Reconstruction of the Fibrous Skeleton. Gösta B. Pettersson, M.D., Ph.D. No relationships to disclose!
 TREATMENT OF ENDOCARDITIS: Destruction and Reconstruction of the Fibrous Skeleton Gösta B. Pettersson, M.D., Ph.D. The Cleveland Clinic Foundation No relationships to disclose! Adult Cardiac Surgery Symposium
TREATMENT OF ENDOCARDITIS: Destruction and Reconstruction of the Fibrous Skeleton Gösta B. Pettersson, M.D., Ph.D. The Cleveland Clinic Foundation No relationships to disclose! Adult Cardiac Surgery Symposium
THE VALVE CLINIC VALVE CONFERENCE
 VALVE CLINIC THE VALVE CLINIC Houston Methodist DeBakey Valve Clinic combines outstanding clinical care, advanced imaging and surgical excellence to offer coordinated evaluation and treatment options for
VALVE CLINIC THE VALVE CLINIC Houston Methodist DeBakey Valve Clinic combines outstanding clinical care, advanced imaging and surgical excellence to offer coordinated evaluation and treatment options for
Valvular heart disease (VHD) is present in 2.5% of the
 is present in 2.5% of the") 2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
Outcomes of Surgical Therapy for Infective Endocarditis in a Pediatric Population: A 21-Year Review
 ORIGINAL ARTICLES: SURGERY SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://www.annalsthoracicsurgery.org/cme/ home. To take the CME activity related to this article, you
ORIGINAL ARTICLES: SURGERY SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://www.annalsthoracicsurgery.org/cme/ home. To take the CME activity related to this article, you
Late secondary TR after left sided heart disease correction: is it predictibale and preventable
 Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
SURGICAL ABLATION OF ATRIAL FIBRILLATION DURING MITRAL VALVE SURGERY THE CARDIOTHORACIC SURGICAL TRIALS NETWORK
 SURGICAL ABLATION OF ATRIAL FIBRILLATION DURING MITRAL VALVE SURGERY THE CARDIOTHORACIC SURGICAL TRIALS NETWORK Marc Gillinov, M.D. For the CTSN Investigators ACC Late Breaking Clinical Trials March 16,
SURGICAL ABLATION OF ATRIAL FIBRILLATION DURING MITRAL VALVE SURGERY THE CARDIOTHORACIC SURGICAL TRIALS NETWORK Marc Gillinov, M.D. For the CTSN Investigators ACC Late Breaking Clinical Trials March 16,
Emergency Intraoperative Echocardiography
 Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Management of Heart Failure in Adult with Congenital Heart Disease
 Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Outline 9/17/2016. Advances in Percutaneous Mitral Valve Repair and Replacement. Scope of the Problem and Guidelines
 Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
TAVI and Valve Replacement Thromboprophylaxis. Warren Prokopiw Pharmacy Resident
 TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Atrioventricular valve repair: The limits of operability
 Atrioventricular valve repair: The limits of operability Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart
Atrioventricular valve repair: The limits of operability Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart
Early Surgery versus Conventional Treatment for Infective Endocarditis
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Early Surgery versus Treatment for Infective Endocarditis Duk-Hyun Kang, M.D., Ph.D., Yong-Jin Kim, M.D., Ph.D., Sung-Han Kim, M.D.,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Early Surgery versus Treatment for Infective Endocarditis Duk-Hyun Kang, M.D., Ph.D., Yong-Jin Kim, M.D., Ph.D., Sung-Han Kim, M.D.,
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
CONGENITAL HEART DEFECTS IN ADULTS
 CONGENITAL HEART DEFECTS IN ADULTS THE ROLE OF CATHETER INTERVENTIONS Mario Carminati CONGENITAL HEART DEFECTS IN ADULTS CHD in natural history CHD with post-surgical sequelae PULMONARY VALVE STENOSIS
CONGENITAL HEART DEFECTS IN ADULTS THE ROLE OF CATHETER INTERVENTIONS Mario Carminati CONGENITAL HEART DEFECTS IN ADULTS CHD in natural history CHD with post-surgical sequelae PULMONARY VALVE STENOSIS
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Prophylaxis against Endocarditis: A Brave New World
 Prophylaxis against Endocarditis: A Brave New World Ann Bolger MD FACC FAHA University of California, San Francisco Nothing to disclose PREVENTION OF INFECTIVE ENDOCARDITIS: GUIDELINES FROM THE AMERICAN
Prophylaxis against Endocarditis: A Brave New World Ann Bolger MD FACC FAHA University of California, San Francisco Nothing to disclose PREVENTION OF INFECTIVE ENDOCARDITIS: GUIDELINES FROM THE AMERICAN
Echocardiography in Endocarditis
 Echocardiography in Endocarditis Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Demographics of IE Incidence is 1.4 12.7/100,000
Echocardiography in Endocarditis Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Demographics of IE Incidence is 1.4 12.7/100,000
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
Ischemic Mitral Valve Disease: Repair, Replace or Ignore?
 Ischemic Mitral Valve Disease: Repair, Replace or Ignore? Fabio B. Jatene Full Professor of Cardiovascular Surgery, Medical School, University of São Paulo, Brazil DISCLOSURE I have no financial relationship
Ischemic Mitral Valve Disease: Repair, Replace or Ignore? Fabio B. Jatene Full Professor of Cardiovascular Surgery, Medical School, University of São Paulo, Brazil DISCLOSURE I have no financial relationship
Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study
 Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study Meagan Sullivan, PharmD PGY2 Cardiology Pharmacy Resident University of Chicago Medicine
Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study Meagan Sullivan, PharmD PGY2 Cardiology Pharmacy Resident University of Chicago Medicine
MEDICAL POLICY SUBJECT: CARDIAC REHABILITATION. POLICY NUMBER: CATEGORY: Therapy/ Rehabilitation
 MEDICAL POLICY SUBJECT: CARDIAC REHABILITATION, 08/25/17 PAGE: 1 OF: 6 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product,
MEDICAL POLICY SUBJECT: CARDIAC REHABILITATION, 08/25/17 PAGE: 1 OF: 6 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product,
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Transcatheter Pulmonary Valve Implantation
 Transcatheter Pulmonary Valve Implantation Policy Number: 7.01.131 Last Review: 2/2014 Origination: 2/2012 Next Review: 2/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Transcatheter Pulmonary Valve Implantation Policy Number: 7.01.131 Last Review: 2/2014 Origination: 2/2012 Next Review: 2/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Dayer MJ, Jones S, Prendergast B, et al. Incidence
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Dayer MJ, Jones S, Prendergast B, et al. Incidence
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin. Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong
 Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
Infectious complications of new cardiovascular devices Emanuele Durante Mangoni, MD PhD
 Infectious complications of new cardiovascular devices Emanuele Durante Mangoni, MD PhD Naples, Italy Disclosure of potential conflicts of interest Emanuele Durante Mangoni, MD PhD My Institution has received
Infectious complications of new cardiovascular devices Emanuele Durante Mangoni, MD PhD Naples, Italy Disclosure of potential conflicts of interest Emanuele Durante Mangoni, MD PhD My Institution has received
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Congenital Heart Disease and Critical Neurological Injury: Do Our Patients Belong in a Neurocritical Care Unit?
 Congenital Heart Disease and Critical Neurological Injury: Do Our Patients Belong in a Neurocritical Care Unit? Shriprasad R Deshpande, MBBS MS Assistant Professor of Pediatrics Medical Director, Mechanical
Congenital Heart Disease and Critical Neurological Injury: Do Our Patients Belong in a Neurocritical Care Unit? Shriprasad R Deshpande, MBBS MS Assistant Professor of Pediatrics Medical Director, Mechanical
Native valve, Conduit stenosis or leakage? How can the interventionalist help?
 Complications in Congenital Heart Diseases -with a little help of our friends Native valve, Conduit stenosis or leakage? How can the interventionalist help? P. Ewert German Heart Center Munich Lausanne
Complications in Congenital Heart Diseases -with a little help of our friends Native valve, Conduit stenosis or leakage? How can the interventionalist help? P. Ewert German Heart Center Munich Lausanne
In spite of the evolution of antimicrobial therapy and
 FROM STS WORKFORCE ON EVIDENCE BASED SURGERY Surgical Management of Endocarditis: The Society of Thoracic Surgeons Clinical Practice Guideline John G. Byrne, MD, Katayoun Rezai, MD, Juan A. Sanchez, MD,
FROM STS WORKFORCE ON EVIDENCE BASED SURGERY Surgical Management of Endocarditis: The Society of Thoracic Surgeons Clinical Practice Guideline John G. Byrne, MD, Katayoun Rezai, MD, Juan A. Sanchez, MD,
Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
 Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical. The Houston Aortic Symposium February 23-25, 2017
 James S. Gammie, MD Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical The Houston Aortic Symposium February 2-25, 2017 Disclosure Statement of Financial Interest Within
James S. Gammie, MD Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical The Houston Aortic Symposium February 2-25, 2017 Disclosure Statement of Financial Interest Within
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Interventional solutions for atrial fibrillation in patients with heart failure
 Interventional solutions for atrial fibrillation in patients with heart failure Advances in Cardiovascular Arrhythmias Great Innovations in Cardiology Matteo Anselmino, MD PhD Division of Cardiology Department
Interventional solutions for atrial fibrillation in patients with heart failure Advances in Cardiovascular Arrhythmias Great Innovations in Cardiology Matteo Anselmino, MD PhD Division of Cardiology Department
Surgical options for tetralogy of Fallot
 Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,