Esophageal Stents What, Why, When and How?
|
|
|
- Gregory Carr
- 6 years ago
- Views:
Transcription
1 Esophageal Stents What, Why, When and How? Motility Noon Conference Bill Kessler February 1, 2017
2 Disclosure Research support from Merit Medical, Inc.
3 Objectives Background Indications Techniques and What? Why? When? How? What s next???
")
4 What (Who) is (a) stent?
5 History of Stent Development 1859 Dentist Charles T Stent developed dental splint and commercialized the device in Charles Dotter first used coaxial tubes for gradual intraluminal stenting 1986 First human use of Wallstent by Puel st use of SEMS esophageal stent 5
6 History of Stents Continued 1997 Bioabsorbable Esophageal stent 2008 SX Ella BD Stent Commercially Available 2013 Niti S TTS (Through the Scope) stent 2016 Extracellular Matrix + stent

7 7 Illustration courtesy of Todd H Baron, MD Mayo Clinic


8 WHAT?
9 WHY? (Indications) Malignant Locally unresectable Widely Metastatic Poor surgical candidate Poor functional status Preoperative BV Dasari Ann Surg 2014 RK Freeman Ann Thorac Surg 2015 Benign (OFF LABEL) Tracheo Esophageal Fistula Anastamotic Leak Esophagectomy Bariatric (fistula) Esophageal Perforation Boerhaave Iatrogenic Foreign body (EoE) Benign Stricture Extraesophageal CA (extrinsic)
10 Dysphagia Score: Mellow and Pinkas 0 = able to eat normal diet / no dysphagia. 1 = able to swallow some solid foods 2 = able to swallow only semi solid foods 3 = able to swallow liquids only 4 = unable to swallow anything / total dysphagia Knyrim 1993
11 50% of circumference 50% incurable disease Most rapidly rising CA

12 Palliation for Malignant Dysphagia Wilson Cook General Anesthesia Balloon dilation 20 mm 16 mm Prosthesis Wallstent MAC sedation Max dilation 10 mm 16 mm diameter
13 Results
14

15 SX Ella Esoph Stent Saito et al Surgical suture Poly L lactic acid

16 Potential Benefits of SEPS FDA Approved for benign and malignant stricture Less tissue in growth Complete sealing % migration 30% Less stricture formation Increased radial expansion Removable


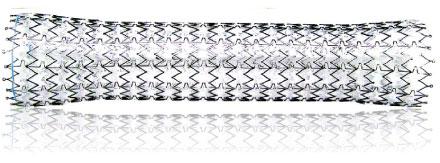
17 Polyflex Fully covered, silicone reinforced ends, proximal flare Radiographic and Endoscopic markings
18 Polyflex Continued
19
20 Summary of Study 30 patients Left in place 52 days (mean) 30% migration rate (1/2 clipped) 30% Immediate pain (1 removed) 90% improvement 47% Required reintervention post removal
21 How about benign conditions? 15 Patients with benign strictures All stented with Polyflex Single migration Remainder with improvement in dysphagia 80% long term (22 months) Repici A GIE 2004
 77/83 (92%) with initial improvement Holm AN et al.")
22 Self expanding plastic stents in treatment of benign esophageal conditions 83/84 stents successfully placed (airway) 77/83 (92%) with initial improvement Holm AN et al. Gastrointest Endosc 2008
23 Immediate Complications Complication # Procedures Chest Pain 23 (27%) Nausea/Vom 8 (9.5%) * Unplanned brief hospital stay In 22 procedures (26%) Airway Comp 3* (3.6%) Dysphonia 2 (2.4%) Perforation 1 (1.2%)
24 Migration Location Frequency Indication Frequency (%) (%) Proximal 30/44 (68) Benign Stricture Mid 3/10 (30) Anast. Stricture Distal 19/27 (70.4) Leak/ Fistula 18/22 (82) 18/25 (72) 13/22 (59) Radiation 4/14 (29)
25 Long Term Results 5/83 (6%) with long term improvement No difference in; Indication Location Size of stent

26 Esophageal Leak post Heller Myotomy
27

28

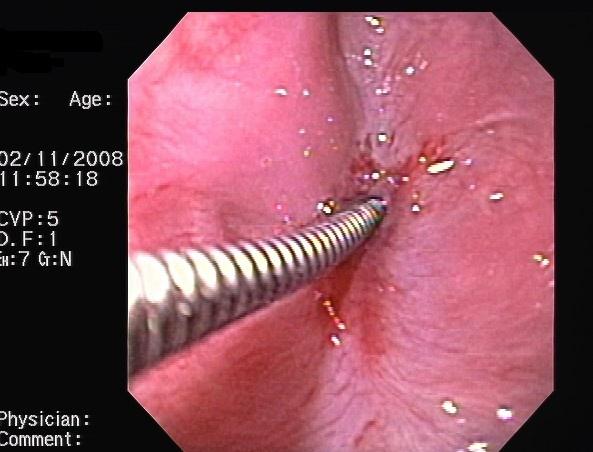
29 Unsuccessful Removal with Rat Tooth

30 Snare used for removal

31 69 yo male with refractory stricture

32 Dilated Fr 18 mm Polyflex Stent Placed

33 Migrated SEPS

34 Stricture Site after Stent Removed

35 Recurrence of symptoms a few weeks later
36
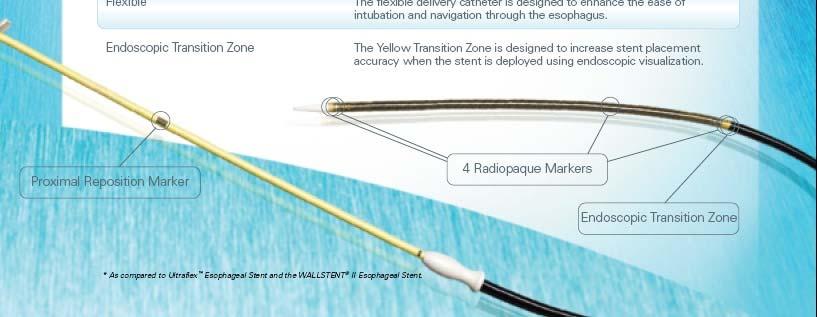

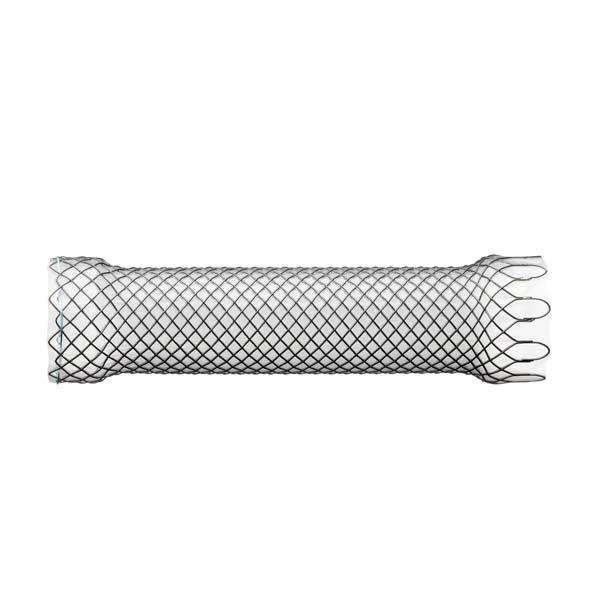
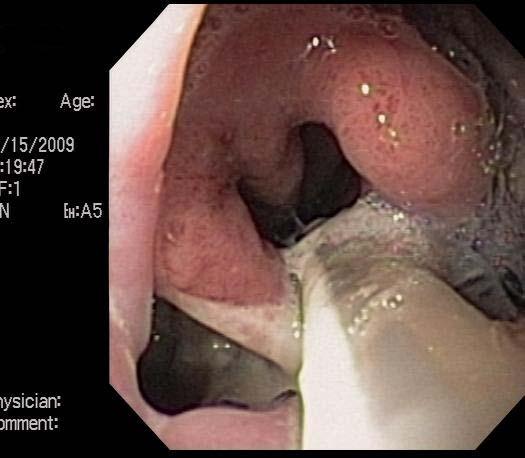
37 Wallflex

38 Alimaxx E Stent
 Tracheo Esophageal Fistula Anastamotic Leak Esophagectomy Bariatric (fistula) Esophageal Perforation Boerhaave Iatrogenic Foreign body (EoE) Benign Stricture Extraesophageal CA")
39 Esophageal Stent Indications Malignant Locally unresectable Widely Metastatic Poor surgical candidate Poor functional status BV Dasari Ann Surg 2014 RK Freeman Ann Thorac Surg 2015 Benign (Off label) Tracheo Esophageal Fistula Anastamotic Leak Esophagectomy Bariatric (fistula) Esophageal Perforation Boerhaave Iatrogenic Foreign body (EoE) Benign Stricture Extraesophageal CA (extrinsic)
 Ann Surg")
40 300 patients: 404 Stents (1/3 FCSEPS only) Ann Surg 2014;259:852-60
41 Primary Outcomes: 91% Technical Success (Metal higher*) 81% Clinic Success healing +/ stent
42 Secondary Outcomes: Migration: 27% Plastic vs. 11% Metal Reintervention: Endoscopic: 22% Plastic vs. 5% Metal Surgical: 6% Plastic vs. 15% Metal Stricture rate: 0.3% Plastic, 3% Metal

43 48 yo male s/p esoph x with leak
44
45

46

47 Leak covered with SEMS

48 Stent Removal

49 Picture after stent removal steven knowles E gram
50 When? How soon should the stent go in? When should it come out?
51 Self expandable metal stents for the treatment of benign upper GI leaks and perforations Retrospective review, single institution 88 patients 65% post operative fistula 15% iatrogenic perforation PC SEMS (Ultraflex, Boston Scientific) Swinnen J et al. GIE 2011;73:890-9
52 Findings Timing is important for perforation 100% closure if immediate (<24 hrs) 50% closure if delayed Is patient infected? Non infectious 100% Infectious 75% ***drain if present Leak closure overall 78% Stricture 21% and migration 11% Stent removal in 97.8%
53 IUH Level One Program Multidisciplinary Team: Esophageal Emergency 30 Month Review Referrals from 45 Hospital Mean Distance : 56 miles (1 163) 80% by ambulance, 20% by air 89% perforation (suspected, diagnosed) 89% of perforations non contained
54 IUH Level One Program Etiology of perforation Ceppa D Esophageal Emergency Program (Submitted)
55 Results
56
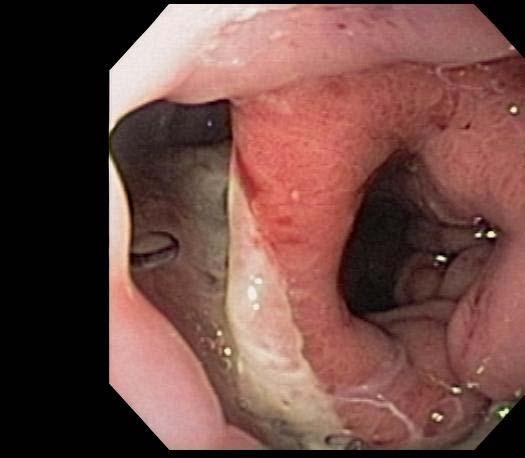
57 Boerhaave s Syndrome 1724 Dr. Hermann Boerhaave describes Large meal + emetic induced vomiting 90% food or alcohol related Men>Women, yo 90% distal esophagus Lack of serosal layer Mortality up to 75% UA Ezenkwele Oct 2016 Medscape
58 Findings in Boerhaave s Syndrome Mackler triad (seen in 50%) Vomiting Acute chest pain Sub cutaneous air Hamman sign (precordial crunch)
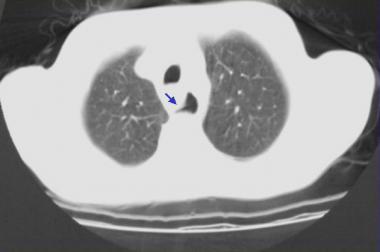
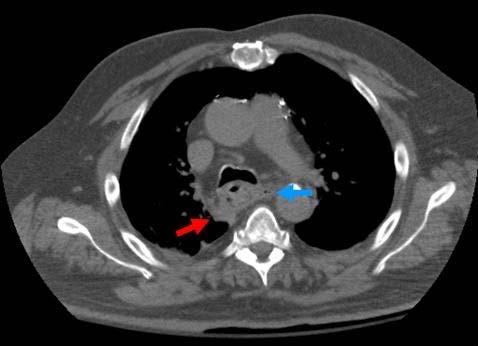
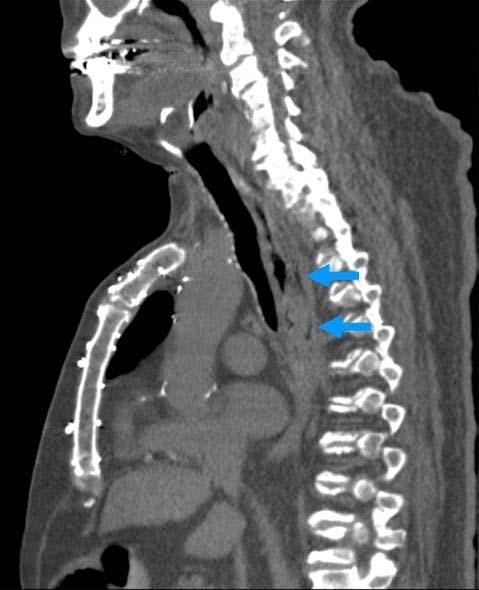
59 Imaging CXR (90% sensitive) Esophagram CT Water soluble (60 75% sensitivity) Barium (90% sensitivity but mediastinitis concern) Mediastinal air Periesophageal fluid Extraluminal contrast Pleural effusion Endoscopy is not typically helpful

60 Esophagram
61
62

63 32/36 yo males EoE Perforation during EGD PCSEMS placed 1 of 2 followed long term
64 What if? (Potential Complications) Airway Compression Fistulization Vascular Structures (Aorta) Airway Migration with SBO Esophageal Necrosis Stent Fracture/Degradation Stuck Stent
65 Informed Consent 0.5 2% Stent Related Mortality Off Label Use of FCSEMS for Benign Indication Diet Aspiration Risk (DD PPI, HOB elevation) Need for Repeat Procedures Chest Pain
66 WHEN (to remove)? Typically 4 8 weeks Monitor for embedding; Q 4 weeks for Partially covered SEMS Q 6 weeks for SEPS/Fully covered SEMS Prolonged Stenting Times (8 16 weeks) Ischemic Injury Strictures <6 12 months after injury Strictures > 5 cm in length Siersema PD Nature Clinical Practice 2009
67 Trends: SEPS with SEMS PC SEMS 8 10 weeks + SEPS 10 days Swinnen J et al. GIE 2011;73:890 9 PC SEMS + SEPS 7 14 days Hirdes MMC et al. Endoscopy 2011;43: perforations with removal (median 29 days)

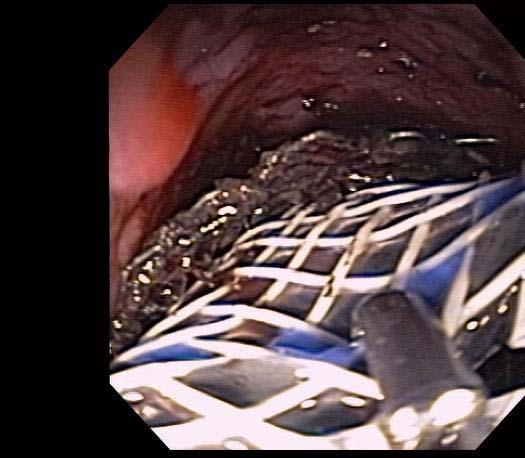
68 SEMS 5 months after deployment

69 SEPS inside SEMS
70

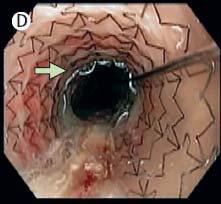
71 After SEPS removed

72 Both Stents removed leak healed

73

74 Ann Thorac Surg 2015
75 Timing of Removal Continued

76 HOW? Migration Prevention?
77 Migration Prevention OTS Clips: Animal data Similar force required to remove as sutures Clips: 44 Patients (50% strictures) 55% vs 13% migration Avg 2.4 clips 12 with retained clip Suture: 37 Patients 55% vs 11.7% migration Hebuterne X Surg Endosc (1)53-9 Surg Endosc (11) Sethi A J Clin Gastroenterol :57-60
78 Sutures to Prevent Migration Sethi A J Clin Gastroenterol :57-60
79 What s next? Valved Esophageal Stent Biodegradable esophageal stent Regenerative stent
80 Valved Stent Anti Reflux Valve Wind Sock Current Study
81 Why Biodegradable? FCSEPS and FCSEMS migrate PCSEMS pose difficulty in removing No need to remove


82 How do they work? Woven polydioxanone monofilament Degrades by hydrolysis, accelerated by ph Strength maintained for 1 month Disintegrates in 3 months
83 Retrospective Study of BD Stents Benign Strictures 10 pts (17 stents) Median F/U 3+ years Dilation Interval (days) Pre: 34 (12 67) Post: 149 (60 244)* No migration One SAE (sepsis) 2/10 required SEMS Malignant Strictures 10 pts (11 stents) Planned XRT/CTX +/ EsophX Median Survival 36 weeks Only 1 patient went to OR Stent Patency Period (month) 6.5 (4.5 9) 5/10 required SEMS (4.5) 1 alive at completion (2 yrs) DE Sigounas Endoscopy International 2016
84 New Frontier?


85 24 yo quadraplegic male s/p MVA 5 years prior Large paraspinal abscess C4 T11 Retrograde endoscopy with Alimaxx bridge KS Dua Lancet 2016
, sutured Platelet rich")
86 3 weeks later.persistent leak Sternocleidomastoid Incision AlloDerm (regenerative tissue matrix), sutured Platelet rich plasma (PRP)+Thrombin+CaCl SCM incision closed Esophogram negative 4 weeks later dysphagia stent bridge
87 Telescoping stents
88 Follow Up Planned removal at 12 weeks Returns with dysphagia at 2 years APC fails FCSEPS for 2 weeks Follow up to 4 years

89
90
91 Summary Stents are useful in a variety of indications Stents have significant potential complications Know what stent you want/need Stents may evolve further in the near future Thank You!
Endoscopic Management of Perforations
 Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City
 Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City Peptic stricture Shtki Schatzki s ring Esophageal cancer Radiation therapy
Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City Peptic stricture Shtki Schatzki s ring Esophageal cancer Radiation therapy
The first stents designed for use in the biliary tree and
 Imaging and Advanced Technology Michael B. Wallace, Section Editor Expandable Gastrointestinal Stents TODD H. BARON Department of Medicine, Division of Gastroenterology & Hepatology, Mayo Clinic, Rochester,
Imaging and Advanced Technology Michael B. Wallace, Section Editor Expandable Gastrointestinal Stents TODD H. BARON Department of Medicine, Division of Gastroenterology & Hepatology, Mayo Clinic, Rochester,
Douglas G. Adler MD. ACG Regional Postgraduate Course - Nashville, TN Copyright 2013 American College of Gastroenterology
 Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Owen Dickinson. Consultant in Endoscopy & Interventional Radiology. Upper GI Stenting. Rotherham Foundation Trust
 Owen Dickinson Consultant in Endoscopy & Interventional Radiology Upper GI Stenting Rotherham Foundation Trust Owen Dickinson Consultant in Endoscopy & Interventional Radiology Rotherham Foundation Trust
Owen Dickinson Consultant in Endoscopy & Interventional Radiology Upper GI Stenting Rotherham Foundation Trust Owen Dickinson Consultant in Endoscopy & Interventional Radiology Rotherham Foundation Trust
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Expandable stents in digestive pathology present use in an emergency hospital
 ORIGINAL ARTICLES Article received on November30, 2015 and accepted for publishing on December15, 2015. Expandable stents in digestive pathology present use in an emergency hospital Mădălina Ilie 1, Vasile
ORIGINAL ARTICLES Article received on November30, 2015 and accepted for publishing on December15, 2015. Expandable stents in digestive pathology present use in an emergency hospital Mădălina Ilie 1, Vasile
Is a Metallic Stent Useful for Non Resectable Esophageal Cancer?
 Original Article Is a Metallic Stent Useful for Non Resectable Esophageal Cancer? Shinsuke Wada, MD, 1 Tsuyoshi Noguchi, MD, 1 Shinsuke Takeno, MD, 1 Hatsuo Moriyama, MD, 1 Tsuyoshi Hashimoto, MD, 1 Yuzo
Original Article Is a Metallic Stent Useful for Non Resectable Esophageal Cancer? Shinsuke Wada, MD, 1 Tsuyoshi Noguchi, MD, 1 Shinsuke Takeno, MD, 1 Hatsuo Moriyama, MD, 1 Tsuyoshi Hashimoto, MD, 1 Yuzo
ESPEN Congress Brussels Stenting of the esophagus and small bowel. Jean-Marc Dumonceau
 ESPEN Congress Brussels 2005 Stenting of the esophagus and small bowel Jean-Marc Dumonceau Stenting of the esophagus and small bowel Jean-Marc Dumonceau, Div. of Gastroenterology Geneva, Switzerland Indication:
ESPEN Congress Brussels 2005 Stenting of the esophagus and small bowel Jean-Marc Dumonceau Stenting of the esophagus and small bowel Jean-Marc Dumonceau, Div. of Gastroenterology Geneva, Switzerland Indication:
ESOPHAGEAL PERFORATION. Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013
 ESOPHAGEAL PERFORATION Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013 OUTLINE Risk factors Diagnosis Management GOALS Make sure you don t miss it If
ESOPHAGEAL PERFORATION Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013 OUTLINE Risk factors Diagnosis Management GOALS Make sure you don t miss it If
Endoscopic Palliation of Malignant Dysphagia
 Endoscopic Palliation of Malignant Dysphagia 1. Scope of the guideline This guidance has been produced to support endoscopic palliation of malignant dysphagia from oesophageal cancer. 2. Guideline background
Endoscopic Palliation of Malignant Dysphagia 1. Scope of the guideline This guidance has been produced to support endoscopic palliation of malignant dysphagia from oesophageal cancer. 2. Guideline background
Stenting for Esophageal Cancer Technical Issues and Outcomes
 Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Стенты «Ella-cs» Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts»
 Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts» A. Esophageal Stenting and related topics 1 AMJG 2009; 104:1329 1330 Letters to Editor Early Tracheal Stenosis Post Esophageal Stent
Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts» A. Esophageal Stenting and related topics 1 AMJG 2009; 104:1329 1330 Letters to Editor Early Tracheal Stenosis Post Esophageal Stent
Polyflex Expandable Stents in the Treatment of Esophageal Disease: Initial Experience
 GENERAL THORACIC Polyflex Expandable Stents in the Treatment of Esophageal Disease: Initial Experience Arjun Pennathur, MD, Andrew C. Chang, MD, Kevin M. McGrath, MD, Gregory Steiner, BS, Miguel Alvelo-Rivera,
GENERAL THORACIC Polyflex Expandable Stents in the Treatment of Esophageal Disease: Initial Experience Arjun Pennathur, MD, Andrew C. Chang, MD, Kevin M. McGrath, MD, Gregory Steiner, BS, Miguel Alvelo-Rivera,
IATROGENIC OESOPHAGEAL PERFORATION
 IATROGENIC OESOPHAGEAL PERFORATION TAOLE MOKOENA DPhil FRCS PROFESSOR OF SURGERY UNIVERSITY OF PRETORIA 17 TH Controversies and Problems in Surgery Symposium 4-5 October 2013 Introduction Perforation of
IATROGENIC OESOPHAGEAL PERFORATION TAOLE MOKOENA DPhil FRCS PROFESSOR OF SURGERY UNIVERSITY OF PRETORIA 17 TH Controversies and Problems in Surgery Symposium 4-5 October 2013 Introduction Perforation of
Biodegradable esophageal stents in benign and malignant strictures a single center experience
 E618 THIEME Biodegradable esophageal stents in benign and malignant strictures a single center experience Authors Institution Dimitrios E. Sigounas, Sandeep Siddhi, John N. Plevris Centre for Liver & Digestive
E618 THIEME Biodegradable esophageal stents in benign and malignant strictures a single center experience Authors Institution Dimitrios E. Sigounas, Sandeep Siddhi, John N. Plevris Centre for Liver & Digestive
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Colorectal stenting. Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy
 Colorectal stenting Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Metal Stents for Obstructing Colorectal Cancer Dohomoto was credited as the first to report
Colorectal stenting Alessandro Repici, MD Digestive Endoscopy Unit IRCCS Istituto Clinico Humanitas Milano, Italy Metal Stents for Obstructing Colorectal Cancer Dohomoto was credited as the first to report
9/18/2015. Disclosures. Objectives. Dysphagia Sherri Ekobena PA-C. I have no relevant financial interests to disclose I have no conflicts of interest
 Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Historically, esophageal stents have been used to palliate
 A Comprehensive Review of Esophageal Stents Pierre Hindy, MD, Jinwha Hong, Yvette Lam-Tsai, MD, and Frank Gress, MD Dr. Hindy is a GI Fellow, Mr. Hong is a Fourth-Year Medical Student, Dr. Lam-Tsai is
A Comprehensive Review of Esophageal Stents Pierre Hindy, MD, Jinwha Hong, Yvette Lam-Tsai, MD, and Frank Gress, MD Dr. Hindy is a GI Fellow, Mr. Hong is a Fourth-Year Medical Student, Dr. Lam-Tsai is
Airway Remodeling: Preliminary Experience with Bio-Absorbable Airway Stents in Adults Jaus MO, Gonfiotti A, Barale D, Macchiarini P
 Airway Remodeling: Preliminary Experience with Bio-Absorbable Airway Stents in Adults Jaus MO, Gonfiotti A, Barale D, Macchiarini P University Hospital Careggi Florence, Italy Disclosure Statement THE
Airway Remodeling: Preliminary Experience with Bio-Absorbable Airway Stents in Adults Jaus MO, Gonfiotti A, Barale D, Macchiarini P University Hospital Careggi Florence, Italy Disclosure Statement THE
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction
 A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
Difficult Esophageal Strictures. Disclosures
 Difficult Esophageal Strictures John A. (Jerry) Evans, MD Ochsner Medical Center New Orleans, LA Disclosures Prior Consultant: Cook Medical Pentax America 1 Format Review of Dilation Options Definition
Difficult Esophageal Strictures John A. (Jerry) Evans, MD Ochsner Medical Center New Orleans, LA Disclosures Prior Consultant: Cook Medical Pentax America 1 Format Review of Dilation Options Definition
Endoscopic stent placement throughout the gastrointestinal tract van den Berg, M.W.
 UvA-DARE (Digital Academic Repository) Endoscopic stent placement throughout the gastrointestinal tract van den Berg, M.W. Link to publication Citation for published version (APA): van den Berg, M. W.
UvA-DARE (Digital Academic Repository) Endoscopic stent placement throughout the gastrointestinal tract van den Berg, M.W. Link to publication Citation for published version (APA): van den Berg, M. W.
Therapeutic Bronchoscopy Etiology - Benign Stenosis Post - intubation Trauma Post - operative Inflammatory Idiopathic
 Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: What is the treatment
: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: What is the treatment
Esophageal injuries. Pre-test /11/10. 新光急診張志華醫師 Facebook.com/jack119. O What is the most common cause of esophageal injuries?
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Endoscopic biodegradable stents as a rescue treatment in the management of post bariatric surgery leaks: acaseseries
 Endoscopic biodegradable stents as a rescue treatment in the management of post bariatric surgery leaks: acaseseries Authors Abed Al Lehibi, Areej Al Balkhi, Abdullah Al Mtawa, Nawaf Al Otaibi Institution
Endoscopic biodegradable stents as a rescue treatment in the management of post bariatric surgery leaks: acaseseries Authors Abed Al Lehibi, Areej Al Balkhi, Abdullah Al Mtawa, Nawaf Al Otaibi Institution
Canena et al. Canena et al. BMC Gastroenterology 2012, 12:70
 A comparison of the temporary placement of 3 different self-expanding stents for the treatment of refractory benign esophageal strictures: a prospective multicentre study Canena et al. Canena et al. BMC
A comparison of the temporary placement of 3 different self-expanding stents for the treatment of refractory benign esophageal strictures: a prospective multicentre study Canena et al. Canena et al. BMC
DYSPHAGIA MANAGEMENT IN OESOPHAGEAL CANCER
 November 2015 DYSPHAGIA MANAGEMENT IN OESOPHAGEAL CANCER 1 Background... 3 2 Dysphagia Grading... 3 3 Dysphagia General Guidelines... 4 4 Modes of Managing Dysphagia... 4 4.1 Modified consistency diet...
November 2015 DYSPHAGIA MANAGEMENT IN OESOPHAGEAL CANCER 1 Background... 3 2 Dysphagia Grading... 3 3 Dysphagia General Guidelines... 4 4 Modes of Managing Dysphagia... 4 4.1 Modified consistency diet...
Author's response to reviews
 Author's response to reviews Title: Fully covered self-expandable metal stents (SEMS), partially covered SEMS and self-expandable plastic stents for the treatment of benign esophageal ruptures and anastomotic
Author's response to reviews Title: Fully covered self-expandable metal stents (SEMS), partially covered SEMS and self-expandable plastic stents for the treatment of benign esophageal ruptures and anastomotic
Esophageal Stent Placement for the Treatment of Acute Intrathoracic Anastomotic Leak After Esophagectomy
 ORIGINAL ARTICLES: SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have either an STS
ORIGINAL ARTICLES: SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have either an STS
Role of stenting in gastrointestinal benign and malignant diseases
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4253/wjge.v7.i5.460 World J Gastrointest Endosc 2015 May 16; 7(5): 460-480 ISSN 1948-5190 (online)
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4253/wjge.v7.i5.460 World J Gastrointest Endosc 2015 May 16; 7(5): 460-480 ISSN 1948-5190 (online)
Evaluation and Management of Refractory Biliary Stricture. J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc.
 Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Per-oral Endoscopic Myotomy
 POEM With the Flexible Scope as a Treatment for Achalasia and Zenker's Diverticulum Abraham Mathew, MD, MSc Professor of Medicine Penn State College of Medicine Penn State Hershey Medical Center Per-oral
POEM With the Flexible Scope as a Treatment for Achalasia and Zenker's Diverticulum Abraham Mathew, MD, MSc Professor of Medicine Penn State College of Medicine Penn State Hershey Medical Center Per-oral
Results of Expandable Metal Stents for Malignant Esophageal Obstruction in 100 Patients: Short-Term and Long-Term Follow-up
 Results of Expandable Metal Stents for Malignant Esophageal Obstruction in 100 Patients: Short-Term and Long-Term Follow-up Neil A. Christie, MD, Percival O. Buenaventura, MD, Hiran C. Fernando, MD, Ninh
Results of Expandable Metal Stents for Malignant Esophageal Obstruction in 100 Patients: Short-Term and Long-Term Follow-up Neil A. Christie, MD, Percival O. Buenaventura, MD, Hiran C. Fernando, MD, Ninh
Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM
 Eosinophilic Esophagitis: Are We There Yet? Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Learning Objectives Understand current definition
Eosinophilic Esophagitis: Are We There Yet? Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Learning Objectives Understand current definition
Departement of Surgery Faculty of Medicine University Sumatera Utara
 SSS EESOPHAGEAL HPOSAGEAL DISORDERS IN SURGICAL PERSPECTIVE Departement of Surgery Faculty of Medicine University Sumatera Utara CONTENT 1. Esophageal Atresia 2. Achalasia 3. Esophageal Rupture 4. Tumor
SSS EESOPHAGEAL HPOSAGEAL DISORDERS IN SURGICAL PERSPECTIVE Departement of Surgery Faculty of Medicine University Sumatera Utara CONTENT 1. Esophageal Atresia 2. Achalasia 3. Esophageal Rupture 4. Tumor
Case Presentation Surgery Grand Round. Amid Keshavarzi, MD UCHSC 4/9/2006
 Case Presentation Surgery Grand Round Amid Keshavarzi, MD UCHSC 4/9/2006 Case Presentation 12 y/o female Presented to OSH after accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not
Case Presentation Surgery Grand Round Amid Keshavarzi, MD UCHSC 4/9/2006 Case Presentation 12 y/o female Presented to OSH after accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not
Esophageal injuries. 新光急診張志華醫師 Facebook.com/jack119
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic Pre-test 2 Which contrast agent
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic Pre-test 2 Which contrast agent
Managing Complications of Bariatric Surgery. Objectives
 Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pritesh Mutha, MD, MPH
 Virginia Commonwealth University Fellow Presentations Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pit Pritesh hm Mutha, MD, MPH Benign Esophageal Stricture Sanjay
Virginia Commonwealth University Fellow Presentations Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pit Pritesh hm Mutha, MD, MPH Benign Esophageal Stricture Sanjay
A Novel Endoscopic Treatment for Achalasia Is the POEM mightier than the sword?
 A Novel Endoscopic Treatment for Achalasia Is the POEM mightier than the sword? Pavlos Kaimakliotis, MD Department of Gastroenterology Lahey Hospital and Medical Center Assistant Professor of Medicine
A Novel Endoscopic Treatment for Achalasia Is the POEM mightier than the sword? Pavlos Kaimakliotis, MD Department of Gastroenterology Lahey Hospital and Medical Center Assistant Professor of Medicine
4/24/2015. History of Reflux Surgery. Recent Innovations in the Surgical Treatment of Reflux
 Recent Innovations in the Surgical Treatment of Reflux Scott Carpenter, DO, FACOS, FACS Mercy Hospital Ardmore Ardmore, OK History of Reflux Surgery - 18 th century- first use of term heartburn - 1934-
Recent Innovations in the Surgical Treatment of Reflux Scott Carpenter, DO, FACOS, FACS Mercy Hospital Ardmore Ardmore, OK History of Reflux Surgery - 18 th century- first use of term heartburn - 1934-
Introduction E178. Background and study aims Fully covered self-expanding
 Original article Treatment of refractory post-esophagectomy anastomotic esophageal strictures using temporary fully covered esophageal metal stenting compared to repeated bougie dilation: results of a
Original article Treatment of refractory post-esophagectomy anastomotic esophageal strictures using temporary fully covered esophageal metal stenting compared to repeated bougie dilation: results of a
EGD. John M. Wo, M.D. University of Louisville July 3, 2008
 EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Duke Masters of Minimally Invasive Thoracic Surgery Orlando, FL. September 17, Session VI: Minimally Invasive Thoracic Surgery: Miscellaneous
 Duke Masters of Minimally Invasive Thoracic Surgery Orlando, FL September 17, 2016 Session VI: Minimally Invasive Thoracic Surgery: Miscellaneous NOTES and POEM James D. Luketich MD, FACS Henry T. Bahnson
Duke Masters of Minimally Invasive Thoracic Surgery Orlando, FL September 17, 2016 Session VI: Minimally Invasive Thoracic Surgery: Miscellaneous NOTES and POEM James D. Luketich MD, FACS Henry T. Bahnson
Dysphagia. Conflicts of Interest
 Dysphagia Bob Kizer MD Assistant Professor of Medicine Creighton University School of Medicine August 25, 2018 Conflicts of Interest None 1 Which patient does not need an EGD as the first test? 1. 50 year
Dysphagia Bob Kizer MD Assistant Professor of Medicine Creighton University School of Medicine August 25, 2018 Conflicts of Interest None 1 Which patient does not need an EGD as the first test? 1. 50 year
Early pain detection and management after esophageal metal stent placement in incurable cancer patients: A prospective observational cohort study
 E89 Early pain detection and management after esophageal metal stent placement in incurable cancer patients: A prospective observational cohort study Authors Institution Agnes N. Reijm, Paul Didden, Marco
E89 Early pain detection and management after esophageal metal stent placement in incurable cancer patients: A prospective observational cohort study Authors Institution Agnes N. Reijm, Paul Didden, Marco
Interventional Endoscopy in PB Malignancy
 Interventional Endoscopy in PB Malignancy 7 th Annual Symposium on GI Cancers St Louis, Missouri Sept 20 th, 2008 David L Carr-Locke MA, MB BChir, DRCOG, FRCP, FACG, FASGE Director, Endoscopy Institute,
Interventional Endoscopy in PB Malignancy 7 th Annual Symposium on GI Cancers St Louis, Missouri Sept 20 th, 2008 David L Carr-Locke MA, MB BChir, DRCOG, FRCP, FACG, FASGE Director, Endoscopy Institute,
Endoscopic incision for the treatment of refractory esophageal anastomotic strictures: outcomes of 13 cases with a minimum follow-up of 12 months
 1130-0108/2016/108/4/196-200 Revista Española de Enfermedades Digestivas Copyright 2016 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid) Vol. 108, N.º 4, pp. 196-200, 2016 ORIGINAL PAPERS Endoscopic incision
1130-0108/2016/108/4/196-200 Revista Española de Enfermedades Digestivas Copyright 2016 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid) Vol. 108, N.º 4, pp. 196-200, 2016 ORIGINAL PAPERS Endoscopic incision
Pulmonary. Pulmonary Endoscopy. Alair Bronchial Thermoplasty System. Transbronchial Aspiration Needles. Cytology Brushes.
 Pulmonary Endoscopy Alair Bronchial Thermoplasty System Alair Bronchial Thermoplasty System... 79 Airway Stents Dynamic (Y) Stent... 79 Polyflex Self-Expanding Silicone Airway Stent... 82 Ultraflex Partially
Pulmonary Endoscopy Alair Bronchial Thermoplasty System Alair Bronchial Thermoplasty System... 79 Airway Stents Dynamic (Y) Stent... 79 Polyflex Self-Expanding Silicone Airway Stent... 82 Ultraflex Partially
Esophageal Diverticulum. Ahmed Hozain, PGY III Kings County Hospital University Hospital of Brooklyn, Surgery Grand Rounds May 18 th, 2017
 Esophageal Diverticulum Ahmed Hozain, PGY III Kings County Hospital University Hospital of Brooklyn, Surgery Grand Rounds May 18 th, 2017 Case Presentation 53 YOF presented to KCHC with sx of dysphagia
Esophageal Diverticulum Ahmed Hozain, PGY III Kings County Hospital University Hospital of Brooklyn, Surgery Grand Rounds May 18 th, 2017 Case Presentation 53 YOF presented to KCHC with sx of dysphagia
Endoscopic Management of the Iatrogenic CBD Injury
 The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
The Foreign Body. Neil H. Stollman, MD, FACG
 The Foreign Body Neil H. Stollman, MD, FACG Associate Clinical Professor of Medicine University of California San Francisco Chief, Division of Gastroenterology Alta Bates Summit Medical Center, Oakland,
The Foreign Body Neil H. Stollman, MD, FACG Associate Clinical Professor of Medicine University of California San Francisco Chief, Division of Gastroenterology Alta Bates Summit Medical Center, Oakland,
DUMON-NOVATECH Y-STENTS: A FOUR-YEAR EXPERIENCE WITH 50 TRACHEOBRONCHIAL TUMORS INVOLVING THE CARINA
 Solunum 3, Özel Sayı 2: 260-264, 2001 DUMON-NOVATECH Y-STENTS: A FOUR-YEAR EXPERIENCE WITH 50 TRACHEOBRONCHIAL TUMORS INVOLVING THE CARINA Jean F DUMON* M C DUMON* SUMMARY This article reports a 4-year
Solunum 3, Özel Sayı 2: 260-264, 2001 DUMON-NOVATECH Y-STENTS: A FOUR-YEAR EXPERIENCE WITH 50 TRACHEOBRONCHIAL TUMORS INVOLVING THE CARINA Jean F DUMON* M C DUMON* SUMMARY This article reports a 4-year
Review Article The Use of Self-Expanding Plastic Stents in the Management of Oesophageal Leaks and Spontaneous Oesophageal Perforations
 Hindawi Publishing Corporation Diagnostic and Therapeutic Endoscopy Volume 2011, Article ID 418103, 6 pages doi:10.1155/2011/418103 Review Article The Use of Self-Expanding Plastic Stents in the Management
Hindawi Publishing Corporation Diagnostic and Therapeutic Endoscopy Volume 2011, Article ID 418103, 6 pages doi:10.1155/2011/418103 Review Article The Use of Self-Expanding Plastic Stents in the Management
Approach to the Biliary Stricture
 Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Title: Use of self-expanding nitinol stents in the pediatric management of refractory esophageal caustic stenosis
 Title: Use of self-expanding nitinol stents in the pediatric management of refractory esophageal caustic stenosis Authors: Verónica Alonso, Devicka Ojha, Harsha Nalluri, Juan Carlos de Agustín DOI: 10.17235/reed.2017.4959/2017
Title: Use of self-expanding nitinol stents in the pediatric management of refractory esophageal caustic stenosis Authors: Verónica Alonso, Devicka Ojha, Harsha Nalluri, Juan Carlos de Agustín DOI: 10.17235/reed.2017.4959/2017
Surgical Evaluation for Benign Esophageal Disease. Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018
 Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Analysis of Unsuccessful Esophageal Stent Placements for Esophageal Perforation, Fistula, or Anastomotic Leak
 Analysis of Unsuccessful Esophageal Stent Placements for Esophageal Perforation, Fistula, or Anastomotic Leak Richard K. Freeman, MD, Anthony J. Ascioti, MD, Theresa Giannini, ARNP, and Raja J. Mahidhara,
Analysis of Unsuccessful Esophageal Stent Placements for Esophageal Perforation, Fistula, or Anastomotic Leak Richard K. Freeman, MD, Anthony J. Ascioti, MD, Theresa Giannini, ARNP, and Raja J. Mahidhara,
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
WallFlex Stents Technique Spotlights
 WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
Disclosures. Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia. Case Presentation. Case Presentation.
 Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Esophageal Stenosis Treatment by Interventional Radiology: Indications, Techniques and complications
 Esophageal Stenosis Treatment by Interventional Radiology: Indications, Techniques and complications Poster No.: C-0437 Congress: ECR 2013 Type: Authors: Keywords: DOI: Educational Exhibit M. Leyva Vásquez-Caicedo,
Esophageal Stenosis Treatment by Interventional Radiology: Indications, Techniques and complications Poster No.: C-0437 Congress: ECR 2013 Type: Authors: Keywords: DOI: Educational Exhibit M. Leyva Vásquez-Caicedo,
Postoperative esophageal leak management with the Polyflex esophageal stent
 Freeman, Ascioti, and Wozniak General Thoracic Surgery Postoperative esophageal leak management with the Polyflex esophageal stent Richard K. Freeman, MD, a Anthony J. Ascioti, MD, a and Thomas C. Wozniak,
Freeman, Ascioti, and Wozniak General Thoracic Surgery Postoperative esophageal leak management with the Polyflex esophageal stent Richard K. Freeman, MD, a Anthony J. Ascioti, MD, a and Thomas C. Wozniak,
34th Annual Toronto Thoracic Surgery Refresher Course
 34th Annual Toronto Thoracic Surgery Refresher Course TREATMENT OPTIONS FOR ACHALASIA Dr. Carmine Simone Director, Intensive Care Unit Head, Division of Critical Care Departments of Medicine and Surgery
34th Annual Toronto Thoracic Surgery Refresher Course TREATMENT OPTIONS FOR ACHALASIA Dr. Carmine Simone Director, Intensive Care Unit Head, Division of Critical Care Departments of Medicine and Surgery
Slide 1. Slide 2. Slide 3 Pancreatic Cancer- Case #1. Endoscopic management of GI malignancy. Endoscopic approaches in GI malignancy- Agenda
 Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Esophageal perforations are challenging to manage and are
 Endoscopic Techniques for the Management of Esophageal Perforation Karen Joanna Dickinson, MBBS, BSc, MD, FRCS, and Shanda H. Blackmon, MD, MPH Esophageal perforations or leaks can be spontaneous, iatrogenic,
Endoscopic Techniques for the Management of Esophageal Perforation Karen Joanna Dickinson, MBBS, BSc, MD, FRCS, and Shanda H. Blackmon, MD, MPH Esophageal perforations or leaks can be spontaneous, iatrogenic,
Managing Foreign Objects in the GI Tract Tips & Tricks
 Managing Foreign Objects in the GI Tract Tips & Tricks STEPHEN LANDRENEAU, MD Take home o Perform emergent endoscopy in cases of: Esophageal obstruction due to food bolus impaction or foreign object. Disk
Managing Foreign Objects in the GI Tract Tips & Tricks STEPHEN LANDRENEAU, MD Take home o Perform emergent endoscopy in cases of: Esophageal obstruction due to food bolus impaction or foreign object. Disk
Biliary Metal Stents MAKING A DIFFERENCE TO HEALTH
 Biliary Metal Stents In a fast paced and maturing market, Diagmed Healthcare s Hanarostent has managed to continue to innovate and add unique and clinically superior features to its already premium range.
Biliary Metal Stents In a fast paced and maturing market, Diagmed Healthcare s Hanarostent has managed to continue to innovate and add unique and clinically superior features to its already premium range.
Endoscopic management of sleeve leaks
 Endoscopic management of sleeve leaks Mr Damien Loh Oesophagogastric and Bariatric Surgeon The Alfred The clinical problem Incidence 0.1-7% Inpatient mortality 2-5% High morbidity Prolonged ICU and in-hospital
Endoscopic management of sleeve leaks Mr Damien Loh Oesophagogastric and Bariatric Surgeon The Alfred The clinical problem Incidence 0.1-7% Inpatient mortality 2-5% High morbidity Prolonged ICU and in-hospital
Spotlight on Esophageal Perforation A multinational study using the Pittsburgh Esophageal Perforation Severity Scoring System
 Spotlight on Esophageal Perforation A multinational study using the Pittsburgh Esophageal Perforation Severity Scoring System Michael Schweigert Department of Thoracic Surgery Objective Esophageal perforation
Spotlight on Esophageal Perforation A multinational study using the Pittsburgh Esophageal Perforation Severity Scoring System Michael Schweigert Department of Thoracic Surgery Objective Esophageal perforation
Management of esophageal anastomotic leaks, perforations, and fistulae with self-expanding plastic stents
 Management of esophageal anastomotic leaks, perforations, and fistulae with self-expanding plastic stents Yiyang Dai, MD, a Sascha S. Chopra, MD, b S oren Kneif, PhD, a and Michael H unerbein, MD, PhD
Management of esophageal anastomotic leaks, perforations, and fistulae with self-expanding plastic stents Yiyang Dai, MD, a Sascha S. Chopra, MD, b S oren Kneif, PhD, a and Michael H unerbein, MD, PhD
A unique case of esophageal perforation caused by prickly pears
 A unique case of esophageal perforation caused by prickly pears Abstract This is a report of a previously healthy 20-yearold male presenting with the sensation of a foreign object being stuck in the throat
A unique case of esophageal perforation caused by prickly pears Abstract This is a report of a previously healthy 20-yearold male presenting with the sensation of a foreign object being stuck in the throat
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
How I Do It? Per-oral Endoscopic Myotomy (POEM) Ping-hong ZHOU, MD. Endoscopy Center, Zhongshan Hospital Fudan University, Shanghai, China
 Ping-hong ZHOU, MD. Endoscopy Center, Zhongshan Hospital Fudan University, Shanghai, China") How I Do It? Per-oral Endoscopic Myotomy (POEM) Ping-hong ZHOU, MD Endoscopy Center, Zhongshan Hospital Fudan University, Shanghai, China The 2 nd World Congress on CONTROVERSIES IN GASTROENTEROLOGY Prof.
How I Do It? Per-oral Endoscopic Myotomy (POEM) Ping-hong ZHOU, MD Endoscopy Center, Zhongshan Hospital Fudan University, Shanghai, China The 2 nd World Congress on CONTROVERSIES IN GASTROENTEROLOGY Prof.
Foreign Body Management
 Foreign Body Management NYSGE Fellows Summer Course Susana Gonzalez, MD Assistant Professor of Medicine 1 Objectives Timing of endoscopy When? Anatomic location Where? High risk objects What? Choosing
Foreign Body Management NYSGE Fellows Summer Course Susana Gonzalez, MD Assistant Professor of Medicine 1 Objectives Timing of endoscopy When? Anatomic location Where? High risk objects What? Choosing
Jennifer Hsieh 1, Amar Thosani 1, Matthew Grunwald 2, Satish Nagula 1, Juan Carlos Bucobo 1, Jonathan M. Buscaglia 1. Introduction
 How We Do It Serial insertion of bilateral uncovered metal stents for malignant hilar obstruction using an 8 Fr biliary system: a case series of 17 consecutive patients Jennifer Hsieh 1, Amar Thosani 1,
How We Do It Serial insertion of bilateral uncovered metal stents for malignant hilar obstruction using an 8 Fr biliary system: a case series of 17 consecutive patients Jennifer Hsieh 1, Amar Thosani 1,
Endoscopic Management of Biliary Strictures. Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center
 Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
Treating Achalasia. When to consider surgery and New options for therapy
 Treating Achalasia When to consider surgery and New options for therapy James B. Wooldridge,Jr., MD Ochsner Medical Center Senior Staff Surgeon General, Laparoscopic, and Bariatric Surgery Disclosures
Treating Achalasia When to consider surgery and New options for therapy James B. Wooldridge,Jr., MD Ochsner Medical Center Senior Staff Surgeon General, Laparoscopic, and Bariatric Surgery Disclosures
When to Refer for OGD and the Work Up of Upper GI Malignancies
 When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
JMSCR Volume 03 Issue 04 Page April 2015
 www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x A Rare Case of Boerhaaves Syndrome Managed Conservatively Authors Dr. Vinaya Ambore 1, Dr. Vikram Wagh 2, Dr. Prashant Turkar 3, Dr. Kapil
www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x A Rare Case of Boerhaaves Syndrome Managed Conservatively Authors Dr. Vinaya Ambore 1, Dr. Vikram Wagh 2, Dr. Prashant Turkar 3, Dr. Kapil
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
ENDOLUMINAL THERAPIES FOR GERD. University of Colorado Department of Surgery Grand Rounds March 31st, 2008
 ENDOLUMINAL THERAPIES FOR GERD University of Colorado Department of Surgery Grand Rounds March 31st, 2008 Overview GERD Healthcare significance Definitions Treatment objectives Endoscopic options Plication
ENDOLUMINAL THERAPIES FOR GERD University of Colorado Department of Surgery Grand Rounds March 31st, 2008 Overview GERD Healthcare significance Definitions Treatment objectives Endoscopic options Plication
GERD DIAGNOSIS & TREATMENT DISCLOSURES 4/18/2018
 GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
Enteral stenting for gastric outlet obstruction and afferent limb syndrome following pancreaticoduodenectomy
 CASE SERIES Annals of Gastroenterology (2014) 27, 1-5 Enteral stenting for gastric outlet obstruction and afferent limb syndrome following pancreaticoduodenectomy Wilson T. Kwong a, Syed M. Fehmi a, Andrew
CASE SERIES Annals of Gastroenterology (2014) 27, 1-5 Enteral stenting for gastric outlet obstruction and afferent limb syndrome following pancreaticoduodenectomy Wilson T. Kwong a, Syed M. Fehmi a, Andrew
ORIGINAL PAPERS. R. Insertion of fully covered self-expanding metal stents in benign biliary diseases. ABSTRACT MATERIALS AND METHODS INTRODUCTION
 ORIGINAL PAPERS Insertion of fully covered self-expanding metal stents in benign biliary diseases Mariana Omodeo, Ignacio Málaga, Dante Manazzoni, Cecilia Curvale, Julio de María, Martín Guidi and Raúl
ORIGINAL PAPERS Insertion of fully covered self-expanding metal stents in benign biliary diseases Mariana Omodeo, Ignacio Málaga, Dante Manazzoni, Cecilia Curvale, Julio de María, Martín Guidi and Raúl
Interventional Pulmonology
 Interventional Pulmonology The Division of Thoracic Surgery Department of Cardiothoracic Surgery New York Presbyterian/Weill Cornell Medical College p: 212-746-6275 f: 212-746-8223 https://weillcornell.org/eshostak
Interventional Pulmonology The Division of Thoracic Surgery Department of Cardiothoracic Surgery New York Presbyterian/Weill Cornell Medical College p: 212-746-6275 f: 212-746-8223 https://weillcornell.org/eshostak
Self-expanding metal stents in postoperative esophageal leaks
 1130-0108/2016/108/3/133-137 Revista Española de Enfermedades Digestivas Copyright 2016 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid) Vol. 108, N.º 3, pp. 133-137, 2016 ORIGINAL PAPERS Self-expanding
1130-0108/2016/108/3/133-137 Revista Española de Enfermedades Digestivas Copyright 2016 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid) Vol. 108, N.º 3, pp. 133-137, 2016 ORIGINAL PAPERS Self-expanding
Lumen-apposing covered self-expanding metal stent for management of benign gastrointestinal strictures
 E96 THIEME Lumen-apposing covered self-expanding metal stent for management of benign gastrointestinal strictures Authors Institution Shounak Majumder, Navtej S. Buttar, Christopher Gostout, Michael J.
E96 THIEME Lumen-apposing covered self-expanding metal stent for management of benign gastrointestinal strictures Authors Institution Shounak Majumder, Navtej S. Buttar, Christopher Gostout, Michael J.
Fully-covered metal stents with endoscopic suturing vs. partiallycovered metal stents for benign upper gastrointestinal diseases: a comparative study
 Fully-covered metal stents with endoscopic suturing vs. partiallycovered metal stents for benign upper gastrointestinal diseases: a comparative study Authors Saowanee Ngamruengphong 1, *, Reem Sharaiha
Fully-covered metal stents with endoscopic suturing vs. partiallycovered metal stents for benign upper gastrointestinal diseases: a comparative study Authors Saowanee Ngamruengphong 1, *, Reem Sharaiha
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Case Report Embedded Pork Bone Causing Esophageal Perforation and an Esophagus-Innominate Artery Fistula
 Case Reports in Gastrointestinal Medicine, Article ID 969862, 4 pages http://dx.doi.org/10.1155/2014/969862 Case Report Embedded Pork Bone Causing Esophageal Perforation and an Esophagus-Innominate Artery
Case Reports in Gastrointestinal Medicine, Article ID 969862, 4 pages http://dx.doi.org/10.1155/2014/969862 Case Report Embedded Pork Bone Causing Esophageal Perforation and an Esophagus-Innominate Artery
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed