Antithrombotics and the Gut
|
|
|
- Gwendolyn Griffin
- 6 years ago
- Views:
Transcription
1 Antithrombotics and the Gut Panelists: AR Tagahvi MD, N Nozari MD Moderator: S Nasseri-Moghaddam MD, MPH IAGH monthly meeting Shahrivar 1395 (September 2016 ) IAGH Conference Hall
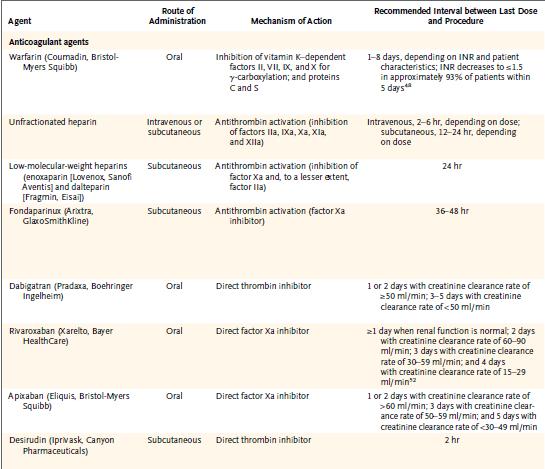
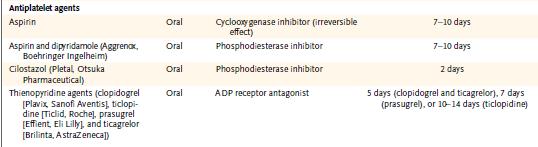
2 Antithrombotic agents Anticoagulants warfarin, Dabigatran, Apixban, heparin, and low molecular weight heparin Antiplatelet agents aspirin, NSAIDs, Thienopyridines (eg, clopidrogrel & ticlopidine), Glycoprotein IIb/IIIa receptor inhibitors.
3 The most common site of significant bleeding in patients receiving oral anticoagulation therapy is the GI tract
4 General concept Low risk procedure for bleeding in high risk pt for thrombosis: Continue anticoagulation High risk procedure for bleeding in low risk pt for thrombosis: Discontinue antithrombotic ASGE: Low risk procedure for bleeding: <1.5% chance High risk procedure for bleeding: >1.5% chance
5 Moderate to high risk thrombosis risk pt undergoing high risk for bleeding procedure Communication between Primary provider Proceduralist Knowledge of: thrombotic risk, procedure-related bleeding risk, concepts of bridging anticoagulation therapy, and timing of cessation and reinitiation of antithrombotic therapy
6 Case-1 A 43 Y/O gentleman w/o any significant past hx presents with substernal pain of 3 hours duration Initial evaluation reveals STEMI (extensive anterior wall) without clinical CHF/dysrhytmias He receives high dose clopidogrel, ASA, & tissue plasminogen activator He undergoes emergency coronary catheterization where a clot is taken out from an occluded LAD and a DES is placed He fares well post-up and is ready for discharge on DET the next day when he feels nauseous and brings up abundant fresh blood
7 Case-1 What will you do for him? Resuscitation and careful management of hydration/hemodynamics Pantoprazole 80mg IV stat followed by 8mg/h Withhold antiplatelets Check Hb q6h Transfuse 2 units of packed RBC Check PT/PTT and if prolonged correct with FFP EGD
8 Before the endoscopy Consider the urgency of the procedure and the risks of Bleeding related solely to antithrombotic therapy, Bleeding related to an endoscopic intervention performed in the setting of antithrombotic medication use, and A thromboembolic event related to interruption of antithrombotic therapy
9 Condition Risk for Thromboembolic Event High Risk Conditions AF with valvular heart disease, prosthetic valves, active congestive heart failure, left ventricular ejection fraction <35%, a history of a thromboembolic event, hypertension, diabetes mellitus, or age >75 y Mechanical valve in the mitral position Mechanical valve in any position and previous thromboembolic event Recently (<1 y) placed coronary stent Acute coronary syndrome Nonstented percutaneous coronary intervention after myocardial infarction Low Risk Conditions Uncomplicated or paroxysmal nonvalvular atrial fibrillation Bioprosthetic valve Mechanical valve in the aortic position Deep vein thrombosis
10 Procedure Risk for Bleeding High Risk Procedures Polypectomy Biliary or pancreatic sphincterotomy Pneumatic or bougie dilation PEG placement Therapeutic balloon-assisted enteroscopy EUS with FNA Enteral stent deployment (without dilation) Endoscopic hemostasis Tumor ablation by any technique Cystogastrostomy Treatment of varices Low Risk Procedures Diagnostic (EGD, colonoscopy, flexible sigmoidoscopy) including biopsy ERCP without sphincterotomy EUS without FNA Enteroscopy and diagnostic balloon-assisted enteroscopy Capsule endoscopy
11 Endoscopic procedures in the acutely bleeding pt on antithrombotics Endoscopic evaluation and therapy in patients who have GIB while using antithrombotic agents is both warranted and safe The most common causes of GIB in these pts: Upper GI tract: Peptic ulcer disease Erosive gastritis/duodenitis/esophagitis Lower GI tract: Diverticular disease
12 Urgent endoscopy in the patient with ACS or a recently placed vascular stent Incidence of GIB in pts with ACS: 1%-3% Mortality in such pts: 4-7 folds The rate of procedural complications may be as high as 12% if done on the same day as the ACS The overall rate of complications associated with EGD: 1-2% Colonoscopy: 1%
13
14 Management of antithrombotic agents in the urgent endoscopic setting
15 Restarting antithrombotic agents after endoscopic hemostasis For aspirin-related PUD with GIB: resumption of aspirin with concurrent proton pump inhibitor therapy is superior to switching to clopidogrel alone Withholding aspirin for 30 days vs resumption at 3-5 days after bleeding associated with: a numerically lower rate of rebleeding (11% vs 19%, P=0.25), 2 months mortality more common (14.5% vs 1.7%, P=.012)
16 Case-2 A 58 Y/O lady has undergone AVR and MVR 20 Y/A (both ball-cage valves) She was maintained on warfarin and metformin (for a recently diagnosed Dm) and did well (INR: 3.5, HbA1c: 6%, creatinine: 0.8mg/dl) Three weeks prior to referral she noted some fresh blood over her stool for the 1 st time The blood was mixed with a formed stool Her bowel habit had not changed She noted another similar episode last week No hx of wt loss, anemia, abdominal pain No family hx of any significant GI disease
17 Case-2 P/E is insignificant except for abdominal obesity and a BMI of 29kg/m 2 The mechanical heart valve sounds appear normal Hb: 13.8 g/dl, MCV: 89 fl, Platelet/WBC/Dif: WNL, INR: 3.6, Creatinine: 0.9mg/dl, HbA1c: 6.2, FBS: 145 mg/dl
18 Case-2 What will you do for her? Considering that the bleeding was not massive, she is stable with mechanical heart valves, & Hb is WNL, treat as hemorrhoids and follow Wait for another episode of hematochezia and if happened then go for colonoscopy Admit her, D/C warfarin, start UFH, schedule for a colonoscopy ASAP Schedule her for an elective colonoscopy
19 Case-2 Hematochezia needs evaluation Careful hx, P/E, and early colonoscopy This case is not urgent and considering her underlying CVD adequate considerations should be given a priori
20 Case-2 She is scheduled for an elective colonoscopy. What will you do now? D/C warfarin 7 days before the procedure, start LMWH and D/C it the day before the procedure Considering the high risk valves for serious thrombotic event, go for the procedure on warfarin and be prepared for management of any bleeding Discuss the case with her cardiologist/cardiac surgeon, D/C warfarin and monitor INR when <2 start LMWH and D/C it the day before the procedure Discuss the case with her cardiologist/cardiac surgeon, D/C warfarin, give 5mg IM vitamin K for 2 successive days and monitor INR when <2 do the procedure Discuss the case with her cardiologist/cardiac surgeon, D/C warfarin and monitor INR when <2 do the procedure
21 Risk of major embolism (causing death, residual neurologic deficit, or peripheral ischemia requiring surgery) in patients with mechanical valves Without antithrombotics: 4/100 pt-yr With antiplatelet therapy: 2.2 per 100 pt-yr With warfarin: 1/100 pt-yr
22 Absolute risk of an embolic event for patients in whom anticoagulation is interrupted for 4-7 days is approximately 1%. Avoid vitamin K to reverse anticoagulation for elective procedures it delays therapeutic anticoagulation once anticoagulants are resumed In patients at low risk of thrombosis: Hold warfarin before the procedure Bridge therapy with heparin usually unnecessary
23 Risk Factors for Thromboembolic Events in Patients with a Mechanical Heart Valve or History of Venous Thromboembolism (<5%/y) (>10%/y)
24 Procedure Risk for Bleeding High Risk Procedures Polypectomy Biliary or pancreatic sphincterotomy Pneumatic or bougie dilation PEG placement Therapeutic balloon-assisted enteroscopy EUS with FNA Enteral stent deployment (without dilation) Endoscopic hemostasis Tumor ablation by any technique Cystogastrostomy Treatment of varices Low Risk Procedures Diagnostic (EGD, colonoscopy, flexible sigmoidoscopy) including biopsy ERCP without sphincterotomy EUS without FNA Enteroscopy and diagnostic balloon-assisted enteroscopy Capsule endoscopy
25 Condition Risk for Thromboembolic Event High Risk Conditions AF with valvular heart disease, prosthetic valves, active congestive heart failure, left ventricular ejection fraction <35%, a history of a thromboembolic event, hypertension, diabetes mellitus, or age >75 y Mechanical valve in the mitral position Mechanical valve in any position and previous thromboembolic event Recently (<1 y) placed coronary stent Acute coronary syndrome Nonstented percutaneous coronary intervention after myocardial infarction Low Risk Conditions Uncomplicated or paroxysmal nonvalvular atrial fibrillation Bioprosthetic valve Mechanical valve in the aortic position Deep vein thrombosis
26 Periprocedural management of warfarin of pts with AF or VHD undergoing elective endoscopy
27 The role of bridge therapy in endoscopy Unfractionated heparin (UFH) and low molecular weight heparin (LMWH) Limited evidence, controversial
28 Continue VKA with a Rxc INR in pts with mechanical heart valves undergoing minor procedures (e.g. as dental extractions or cataract removal) where bleeding is easily controlled. (Level of Evidence: C) Temporarily D/C VKA, w/o bridging agents while the INR is subtherapeutic in pts with a bileaflet mechanical AVR and no other risk factors for thrombosis who are undergoing invasive or surgical procedures. (Level of Evidence: C) Bridging anticoagulation with either IV UFH or subq LMWH with subtherapeutic INR preoperatively in patients who are undergoing invasive or surgical procedures with a: mechanical AVR and any thromboembolic risk factor older-generation mechanical AVR, mechanical MVR. (Level of Evidence: C)
29 D/C anticoagulation (ie, warfarin) in pts with a low risk of thromboembolic events in whom it is safe to do
30
31 Continuing therapeutic anticoagulation with warfarin during the periendoscopic period has a low risk of bleeding in diagnostic EGD/Colonoscopy
32 Bridging anticoagulation: Aims Minimize the risk of thromboembolism in high risk patients when anticoagulation therapy is suspended Minimize the risk of bleeding after high-risk procedures
33 Bridging anticoagulation: Does it help? Older Studies Risk of thrombosis Risk of bleeding Mechanical Heart valves 1.2% 2.7% Atrial Fibrillation 0.9% 2.0% Venous Thrombombolism 1.8% 1.9% SR and metaanalysis (Siegal D et al, 2012): Increased risk of bleeding w/o significant decrease in thromboembolism
34 A new Japanese study Matsumoto et al, BMC gastroenterol 2015 Heparin Bridge Rx: 171 UGI/74 lower GI Controls: 5588 upper GI/6614 lower GI
35 Case-2 She undergoes colonoscopy whith an INR of 1.5. A 2cm pedunculated polyp is identified in midsigmoid and another 15mm sessile one in the distal transverse colon. What will you do? Remove both polyps with snare after injecting beneath them and apply hemoclips Remove both polyps with snare after injecting beneath them Remove the pedunculated one and leave the sessile one for another session when the INR is <1.2 Terminate procedure, achieve an INR<1.2 and then do polypectomies
36 Colonoscopic polypectomy Very low risk of post-polypectomy bleeding even on ASA/NSAIDs (exact risk unknown) Postpolypectomy bleeding risk: increased for patients taking warfarin or resuming warfarin or heparin within 1 week after polypectomy
37 Endoscopic procedures in the acutely bleeding pt on antithrombotics A retrospective study: 52 pts Correcting INR to successful endoscopic Dx & Rx at rates comparable with those achieved in nonanticoagulated pts A larger study (246 pts): 95% of INRs Endoscopic Rx initial success: 94.7% using a variety of hemostatic techniques including injection therapy, heater probe, and hemoclips rebleeding rate: 23% The preprocedure INR was NOT a predictor of rebleeding A retrospective study: INR>4 & INR 2-4: No difference in rates of rebleeding
38 Case-2 The polyps are resected successfully w/o any immediate complication. When will you restart the anticoagulation? Immediately after the procedure The next day with heparin and add warfarin on day 3 Start warfarin within a few hours after the procedure and UFH the next day
39 Re-initiation of antithrombotic agents after elective endoscopy No consensus A study: 94 pts/109 colonoscopies (47% hot biopsy or snare polypectomy) Warfarin restarted the day after the examination. only 1 (0.92%) procedure-related bleeding occurring 7 days after warfarin required hospitalization and transfusion Another study: 173 pts Warfarin restarted within 1w Bleeding risk OR: 5.2 (95% CI: ) AHA/ACC recommendation: Patients with valvular heart disease and a low risk of thromboembolism: restart warfarin within 24 hours Patients with high risk of thromboembolism on UFH or LMWH: restart warfarin as soon as bleeding stability allows and continued until appropriate INR is reached after a therapeutic procedure, UFH may be restarted 2 to 6 hours later. The optimal time to restart LMWH after endoscopy has not been determined.
40 Case-3 A 62 Y/O gentleman who has underwent PCI with placement of two DES 3 months ago refers for follow-up of colon polyps first diagnosed 4 years ago At that time he had 3 polyps 5-25mm in different parts of his colon, all removed and reported to be adenomatous polyps He is diabetic, overweight, and hypertensive on metformin, atorvastatin, ASA, clopidogrel, valsartan, and atenolol Family hx is negative for CRC
41 Case-3 What will you recommend to him? Postpone the colonoscopy till after 12 months has elapsed from his PCI Progress to the colonoscopy +/-polypectomy on his current medication Progress to the colonoscopy +/-polypectomy after D/C Clopidogrel for 5-7 days Progress to the colonoscopy +/-polypectomy after D/C ASA for 3 days Progress to the colonoscopy +/-polypectomy after D/C ASA & Clopidogrel
42 Coronary stents Dual antiplt Rx Premature D/C of Rx increased risk of stent thrombosis and AMI Mortality of 50% Stent type: Bare vs Drug eluting (DES) Highest risk of thrombosis: Bare: within 6 weeks DES: in 3-6 months
43 ENDOSCOPY IN THE PATIENT WITH A VASCULAR STENT OR ACS TAKING ANTITHROMBOTIC DRUGS Postpone endoscopic procedure till at least 12 months after a DES on DAT IF POSSIBLE Thereafter D/C one Which one? Nobody knows exactly? Clopidogrel more effective in prevention of thromosis Good data on safety of polypectomies on ASA
44
45 Management of antithrombotic agents in the elective endoscopic setting
46 Case-4 A 72 Y/O lady undergoes elective CABG Three venous grafts are placed successfully and the pt is doing well in ICU while on heparin and ASA On the second post-op day, she develops painless massive hematochezia with hemodynamic instability which is corrected rapidly with administration of IV fluids Hb 8.5g/dl, PTT: 60s, INR: 1.2, platelet:
47 Case-4 What will you do for her after adequate resuscitation and monitoring? D/C ASA/heparin, prepare the pt for urgent clonoscopy D/C ASA/heparin, start IV PPI, schedule the pt for urgent EGD D/C ASA/heparin, observe the pt carefully and if ongoing bleeding happens or hemodynamic instability recurs go for further Dxc procedures
48 Case-4 The pt is stabilized, undergoes EGD which does not report any significant lesion Is a colonoscopy warranted now? Yes, within the next 7-10 days Yes, can be postponed after 10 days if hemodynamically stable Yes, only if bleeding recurs No, the chances of any significant lower GI pathology is nil considering the massive bleeding & nl EGD No, considering the recent CABG and high risk for any further intervention, finding any pathology in the colon will not affect pt s management
49 Our knowledge is evolving, therefore Strong recommendations regarding the management of particular agents in the periendoscopic period cannot be made at this time Clinicians are encouraged to seek the input of relevant consultants (eg, cardiology and neurology) before discontinuing any antithrombotic agent
50
51 Sphincterotomy and PEG Risk of postsphincterotomy bleeding: 0.3% to 2.0% Withholding aspirin or NSAIDs, even as long as 7 days before sphincterotomy, does not seem to reduce the risk of bleeding Anticoagulation with oral warfarin or intravenous heparin within 3 days after has been shown to increase the risk of postsphincterotomy bleeding PEG placement: 2.5% risk of bleeding complications The risk of bleeding for PEG placement in the patient receiving antithrombotic therapy is unknown
52 ENDOSCOPIC PROCEDURES IN THE ACUTELY BLEEDING PATIENT RECEIVING ANTITHROMBOTIC THERAPY
53 Stopping or reversing antithrombotic agents in the acutely bleeding pt Weigh & individualize the risk of thromboembolic consequences against the risk of continued bleeding by maintaining antithrombotic agents Hold warfarin Give vitamin K (10 mg slow IV) Give (for life-threatening bleeding) or consider FFP (for serious bleeding), prothrombin complex concentrate, or recombinant factor VIIa
54 Procedure Risk for Bleeding High Risk Procedures Polypectomy Biliary or pancreatic sphincterotomy Pneumatic or bougie dilation PEG placement Therapeutic balloon-assisted enteroscopy EUS with FNA Enteral stent deployment (without dilation) Endoscopic hemostasis Tumor ablation by any technique Cystogastrostomy Treatment of varices Low Risk Procedures Diagnostic (EGD, colonoscopy, flexible sigmoidoscopy) including biopsy ERCP without sphincterotomy EUS without FNA Enteroscopy and diagnostic balloon-assisted enteroscopy Capsule endoscopy
55
56 Condition Risk for Thromboembolic Event High Risk Conditions AF with valvular heart disease, prosthetic valves, active congestive heart failure, left ventricular ejection fraction <35%, a history of a thromboembolic event, hypertension, diabetes mellitus, or age >75 y Mechanical valve in the mitral position Mechanical valve in any position and previous thromboembolic event Recently (<1 y) placed coronary stent Acute coronary syndrome Nonstented percutaneous coronary intervention after myocardial infarction Low Risk Conditions Uncomplicated or paroxysmal nonvalvular atrial fibrillation Bioprosthetic valve Mechanical valve in the aortic position Deep vein thrombosis
 Dm")
57 CHADS 2 Scoring System for Assessing the Risk of Stroke among Patients with Non-valvular Atrial Fibrillation CHF HTN Age (75) Dm Stroke
58
59
Peri-Endoscopic Period. Neena S. Abraham MD, MSCE, FACG
 How to Manage Antiplatelet Therapy in the Peri-Endoscopic Period Neena S. Abraham MD, MSCE, FACG Michael E. DeBakey Veterans Affairs Medical Center Sections of Gastroenterology & Health Services Research
How to Manage Antiplatelet Therapy in the Peri-Endoscopic Period Neena S. Abraham MD, MSCE, FACG Michael E. DeBakey Veterans Affairs Medical Center Sections of Gastroenterology & Health Services Research
Oral anti-thrombotic therapy-management in patients requiring endoscopy
 Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Anticoagulation Transitions: Perioperative Care
 Anticoagulation Transitions: Perioperative Care Alan Brush, MD, FACP Clinical Co-Director, Anticoagulation Management Service Harvard Vanguard Medical Associates Four Questions for each Consultation 1.
Anticoagulation Transitions: Perioperative Care Alan Brush, MD, FACP Clinical Co-Director, Anticoagulation Management Service Harvard Vanguard Medical Associates Four Questions for each Consultation 1.
on Anti-coagulants -- Is It Safe? And When to Stop?
 Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Patients on anticoagulant or antiplatelet therapy undergoing elective endoscopic procedures
 This is an official Northern Trust policy and should not be edited in any way Patients on anticoagulant or antiplatelet therapy undergoing elective endoscopic procedures Reference Number: NHSCT/11/454
This is an official Northern Trust policy and should not be edited in any way Patients on anticoagulant or antiplatelet therapy undergoing elective endoscopic procedures Reference Number: NHSCT/11/454
Clinical Practice Guideline for Anticoagulation Management
 Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
Slide 1: Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Endoscopy and the Anticoagulated Patient
 Endoscopy and the Anticoagulated Patient John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Objectives To accurately assess the risk
Endoscopy and the Anticoagulated Patient John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Objectives To accurately assess the risk
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı
 ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
WARFARIN: PERI OPERATIVE MANAGEMENT
 WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Endoscopy in the Era of Anti- Platelet and Anti-Coagulation
 Endoscopy in the Era of Anti- Platelet and Anti-Coagulation Larissa Fujii-Lau, MD Assistant Professor of Medicine University of Hawaii Clinical Updates in Gastroenterology, Hepatology, and Nutrition 1/20/2017
Endoscopy in the Era of Anti- Platelet and Anti-Coagulation Larissa Fujii-Lau, MD Assistant Professor of Medicine University of Hawaii Clinical Updates in Gastroenterology, Hepatology, and Nutrition 1/20/2017
WARFARIN: PERI-OPERATIVE MANAGEMENT
 WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
Peri-endoscopic Management of Antithrombotics & Anticoagulants
 Peri-endoscopic Management of Antithrombotics & Anticoagulants ACG Postgraduate Course, Nashville, TN Dec 5, 2015 Vivek Kaul, MD, FACG Segal-Watson Professor of Medicine Chief of Gastroenterology & Hepatology
Peri-endoscopic Management of Antithrombotics & Anticoagulants ACG Postgraduate Course, Nashville, TN Dec 5, 2015 Vivek Kaul, MD, FACG Segal-Watson Professor of Medicine Chief of Gastroenterology & Hepatology
Expert Consensus Decision Pathway on Peri- Procedural Management of Anticoagulation
 Expert Consensus Decision Pathway on Peri- Procedural Management of Anticoagulation John U Doherty, MD, FACC Anticoagulation Consortium Roundtable Heart House October 24, 2015 Peri-Procedural Management
Expert Consensus Decision Pathway on Peri- Procedural Management of Anticoagulation John U Doherty, MD, FACC Anticoagulation Consortium Roundtable Heart House October 24, 2015 Peri-Procedural Management
Gastroenterology & Hepatology Update 2017 Prevention and Endoscopy: A Balancing Act in Eastern Caribbean CME Cruise Dr.
 Kerri Novak MD University of Calgary www.seacourses.com 1 To review and understand the existing bevy of options for anticoagulation and their mechanism of action Familiarize ourselves with options for
Kerri Novak MD University of Calgary www.seacourses.com 1 To review and understand the existing bevy of options for anticoagulation and their mechanism of action Familiarize ourselves with options for
t. Recommendations for periprocedural anticoagulation are available lhrough the American College of Chest Physicians Clinical Practice Guidelines.
 Name or Policy: Policy Number: 3364-133-116 Department: Approving Officer: Responsible Agent: cope: x Management of Anticoagulation with Invasive Procedures Pharmacy Chief Operating Officer Director of
Name or Policy: Policy Number: 3364-133-116 Department: Approving Officer: Responsible Agent: cope: x Management of Anticoagulation with Invasive Procedures Pharmacy Chief Operating Officer Director of
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K. B. Cosmi
 Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Update on the Management of Anticoagulants and Endoscopy. ACG Eastern Postgraduate Course, Washington, DC June 25, 2016
 Update on the Management of Anticoagulants and Endoscopy ACG Eastern Postgraduate Course, Washington, DC June 25, 2016 Vivek Kaul, MD, FACG Segal-Watson Professor of Medicine Chief of Gastroenterology
Update on the Management of Anticoagulants and Endoscopy ACG Eastern Postgraduate Course, Washington, DC June 25, 2016 Vivek Kaul, MD, FACG Segal-Watson Professor of Medicine Chief of Gastroenterology
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Clinical Practice Committee Anticoagulation Bridging Document
 Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline
 Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline A. Scope (disease/condition, treatment, clinical specialty) 1. Adult patients undergoing a procedure or surgery
Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline A. Scope (disease/condition, treatment, clinical specialty) 1. Adult patients undergoing a procedure or surgery
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
Disclosures. Overview. Have you ever. The Perioperative Management of Anticoagulants. No financial conflicts of interest to disclose
 Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
Peri-Procedural Management of Antithrombotic Agents
 u Peri-Procedural Management of Antithrombotic Agents An Integrated Care Pathway of the Collaborative Care Network Subject Matter Experts: Will Maxted, MD Veronica Kerner, PharmD Pathway Custodian: Pat
u Peri-Procedural Management of Antithrombotic Agents An Integrated Care Pathway of the Collaborative Care Network Subject Matter Experts: Will Maxted, MD Veronica Kerner, PharmD Pathway Custodian: Pat
Bleeding Management Strategies. Aiming for the best Outcomes August 27, Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM
 Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Antiplatelets in cardiac patients with suspected GI bleeding
 Antiplatelets in cardiac patients with suspected GI bleeding Acute GI bleeding is a common major medical emergency. In the 2007 UK-wide audit, overall mortality of patients admitted with acute GI bleeding
Antiplatelets in cardiac patients with suspected GI bleeding Acute GI bleeding is a common major medical emergency. In the 2007 UK-wide audit, overall mortality of patients admitted with acute GI bleeding
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Update in Perioperative Anticoagulation and Antiplatelet management
 Update in Perioperative Anticoagulation and Antiplatelet management Grand Rounds October 31, 2014 Brooke Hall, MD Steve Kornfeld, MD Bruce McLellan, MD Nothing to disclose Objectives Describe the updates
Update in Perioperative Anticoagulation and Antiplatelet management Grand Rounds October 31, 2014 Brooke Hall, MD Steve Kornfeld, MD Bruce McLellan, MD Nothing to disclose Objectives Describe the updates
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now. Bradley A. Hardin, MD Richard F.
 The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
The Role of Oral Anticoagulants in Atrial Fibrillation: What You Need to Know Now Bradley A. Hardin, MD Richard F. Otten, MD, FACC Outline Atrial Fibrillation Overview Overview of New Oral Anticoagulants
Dental Management Considerations for Patients on Antithrombotic Therapy
 Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Perioperative Anticoagulation Management
 Perioperative Anticoagulation Management ACP Delaware Chapter Scientific Meeting Feb 9, 2019 Andrew Dunn, MD, MPH, MACP Chief, Division of Hospital Medicine Mount Sinai Health System, NY DISCLOSURES Desai
Perioperative Anticoagulation Management ACP Delaware Chapter Scientific Meeting Feb 9, 2019 Andrew Dunn, MD, MPH, MACP Chief, Division of Hospital Medicine Mount Sinai Health System, NY DISCLOSURES Desai
CASE IN... Anticoagulation: When to Start,When to Stop. The management of patients who require an. Meet Tracey. Anticoagulation
 Anticoagulation: When to Start,When to Stop Ebtisam Bakhsh, MD; and James D. Douketis, MD, FRCPC Presented at McMaster University s Thrombosis and Hematology Update, October 2006. CASE IN... Anticoagulation
Anticoagulation: When to Start,When to Stop Ebtisam Bakhsh, MD; and James D. Douketis, MD, FRCPC Presented at McMaster University s Thrombosis and Hematology Update, October 2006. CASE IN... Anticoagulation
Perioperative Management of the Anticoagulated Patient
 Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
high thrombotic risk, we recommend continuing aspirin and liaising with a cardiologist about the risk/benefit of discontinuation of P2Y12 receptor
 Guideline 385 Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy
Guideline 385 Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
2010, Metzler Helfried
 Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation
 HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
with Gastrointestinal bleeding and in
 Management of Anticoagulants in patients with Gastrointestinal bleeding and in Elective Endoscopic procedures. S.A.Taghavi M.D., Associate professor of internal Medicine, Shiraz University of Medical Sciences
Management of Anticoagulants in patients with Gastrointestinal bleeding and in Elective Endoscopic procedures. S.A.Taghavi M.D., Associate professor of internal Medicine, Shiraz University of Medical Sciences
Scope of the Problem: DAPT and Triple Therapy after Stenting
 Scope of the Problem: DAPT and Triple Therapy after Stenting Kurt Huber, MD, FESC, FACC 3 rd Medical Department Cardiology & Emergency Medicine Wilhelminenhospital Vienna, Austria Session, August 30, 2010,
Scope of the Problem: DAPT and Triple Therapy after Stenting Kurt Huber, MD, FESC, FACC 3 rd Medical Department Cardiology & Emergency Medicine Wilhelminenhospital Vienna, Austria Session, August 30, 2010,
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation Bridging and Emerging Therapies. Disclosures and Relationships. Objectives. Dr. Cumbler has no conflicts of interest
 Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery. Alex C. Spyropoulos MD, FACP, FCCP, FRCPC
 who Need Elective Surgery. Alex C. Spyropoulos MD, FACP, FCCP, FRCPC") The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery Alex C. Spyropoulos MD, FACP, FCCP, FRCPC Professor of Medicine Hofstra Northwell School of Medicine
The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery Alex C. Spyropoulos MD, FACP, FCCP, FRCPC Professor of Medicine Hofstra Northwell School of Medicine
During Procedures. Neena S. Abraham MD, MSc (EPID), FACG
, FACG") Managing Anticoagulants During Procedures Neena S. Abraham MD, MSc (EPID), FACG Professor of Medicine, Mayo Clinic College of Medicine Associate Medical Director, Mayo Clinic i Robert D. and Patricia i
Managing Anticoagulants During Procedures Neena S. Abraham MD, MSc (EPID), FACG Professor of Medicine, Mayo Clinic College of Medicine Associate Medical Director, Mayo Clinic i Robert D. and Patricia i
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
Anticoagulation Management Around Endoscopy: GI Perspective. Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017
 Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Challenging Anticoagulation Case Studies. Earl J. Hope, M.D. Tower Health Cardiology
 Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients
 4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH
 Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction
 Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved
 . Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved tilladelse Antithrombotic therapy in Atrial Fibrillation
. Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved tilladelse Antithrombotic therapy in Atrial Fibrillation
Colonoscopy and Management of patients under anti-thombotic therapy. Christian BOUSTIERE St Joseph Hospital Marseille, France
 Colonoscopy and Management of patients under anti-thombotic therapy Christian BOUSTIERE St Joseph Hospital Marseille, France INTRODUCTION The use of antithrombotic agents (aspirin, thienopyridines, warfarin,
Colonoscopy and Management of patients under anti-thombotic therapy Christian BOUSTIERE St Joseph Hospital Marseille, France INTRODUCTION The use of antithrombotic agents (aspirin, thienopyridines, warfarin,
Neena S. Abraham, MD, MSCE, FACG
 1B: Hot Topics in Endoscopy and GI Bleeding How to Manage Anti-platelet Therapy in the PeriEndoscopic Period Neena S. Abraham, MD, MSCE, FACG Learning Objectives At the conclusion of this presentation,
1B: Hot Topics in Endoscopy and GI Bleeding How to Manage Anti-platelet Therapy in the PeriEndoscopic Period Neena S. Abraham, MD, MSCE, FACG Learning Objectives At the conclusion of this presentation,
Perioperative Management. Perioperative Management of Cardiovascular Medications
 of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
Primary Care practice clinics within the Edmonton Southside Primary Care Network.
 INR Monitoring and Warfarin Dose Adjustment Last Review: November 2016 Intervention(s) and/or Procedure: Registered Nurses (RNs) adjust warfarin dosage according to individual patient International Normalized
INR Monitoring and Warfarin Dose Adjustment Last Review: November 2016 Intervention(s) and/or Procedure: Registered Nurses (RNs) adjust warfarin dosage according to individual patient International Normalized
Prostate Biopsy Alerts
 Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
Stolling en anesthesie. Erik Vandermeulen MD, PhD Dept. of Anesthesia
 Stolling en anesthesie Erik Vandermeulen MD, PhD Dept. of Anesthesia Preoperative use of anticoagulation Vitamin K-antagonists (VKA) Fenprocoumon (Marcoumar ) Warfarin (Marevan ) Acenocoumarol (Sintrom
Stolling en anesthesie Erik Vandermeulen MD, PhD Dept. of Anesthesia Preoperative use of anticoagulation Vitamin K-antagonists (VKA) Fenprocoumon (Marcoumar ) Warfarin (Marevan ) Acenocoumarol (Sintrom
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR
 MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
Preoperative Management of Patients Receiving Antithrombotics
 Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
2.5 Other Hematology Consult:
 The Warfarin Order Sheet has been approved by the P & T committee to be implemented by pharmacists. These orders are not used to treat patients with serious hemorrhagic complications. WARFARIN TARGET INR
The Warfarin Order Sheet has been approved by the P & T committee to be implemented by pharmacists. These orders are not used to treat patients with serious hemorrhagic complications. WARFARIN TARGET INR
MANAGEMENT OF OVER-ANTICOAGULATION. Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas
 MANAGEMENT OF OVER-ANTICOAGULATION Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas Risk of Intracranial Hemorrhage in Outpatients (From Management of Oral Anticoagulant
MANAGEMENT OF OVER-ANTICOAGULATION Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas Risk of Intracranial Hemorrhage in Outpatients (From Management of Oral Anticoagulant
Alberta Colorectal Cancer Screening Program (ACRCSP) Antithrombotic Management
 Antithrombotic Management") Alberta Colorectal Cancer Screening Program (ACRCSP) Antithrombotic Management Assessment Tools and Suggested Management for the Patient on Antithrombotics Undergoing a Screening-Related Colonoscopy Version
Alberta Colorectal Cancer Screening Program (ACRCSP) Antithrombotic Management Assessment Tools and Suggested Management for the Patient on Antithrombotics Undergoing a Screening-Related Colonoscopy Version
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
DISCLOSURE. What I am Talking About. Rational Use of Antiplatelet Agents. Aspirin. Tom DeLoughery, MD MACP FAWM
 Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Thrombosis Canada Clinical Tools. Perioperative Management of Anticoagulants Antithrombotic Use in Atrial Fibrillation
 Thrombosis Canada Clinical Tools Perioperative Management of Anticoagulants Antithrombotic Use in Atrial Fibrillation Dr. Benjamin Bell, MD FRCPC Staff General Internist North York General Hospital Lecturer,
Thrombosis Canada Clinical Tools Perioperative Management of Anticoagulants Antithrombotic Use in Atrial Fibrillation Dr. Benjamin Bell, MD FRCPC Staff General Internist North York General Hospital Lecturer,
Manuel Castella MD PhD Hospital Clínic, University of
 Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Joost van Veen Consultant Haematologist
 Joost van Veen Consultant Haematologist Bridging anticoagulation - conclusion Aim Questions What is the evidence? Does oral anticoagulation need to be stopped and if so when? When and at what dose is alternative
Joost van Veen Consultant Haematologist Bridging anticoagulation - conclusion Aim Questions What is the evidence? Does oral anticoagulation need to be stopped and if so when? When and at what dose is alternative
Bridging anticoagulation definition
 Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS
: COMPARISON AND FREQUENTLY ASKED QUESTIONS") NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants
 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
Update on Oral Anticoagulation for Mechanical Heart Valves
 Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Nanik Hatsakorzian Pharm.D/MPH
 Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Antithrombotic therapy in difficult clinical conditions
 Antithrombotic therapy in difficult clinical conditions 4 : 5 Pankaj Manoria, PC Manoria, KK Saha, Piyush Manoria, Bhopal Introduction With the development of newer and more potent antithrombotic agents
Antithrombotic therapy in difficult clinical conditions 4 : 5 Pankaj Manoria, PC Manoria, KK Saha, Piyush Manoria, Bhopal Introduction With the development of newer and more potent antithrombotic agents
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥
 Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥 Risk vs Benefit Hemorrhage Thrombosis Hemorrhage rarely fatal, controlled by endoscoic therapeutic measures, TAE, operation Thrombotic
Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥 Risk vs Benefit Hemorrhage Thrombosis Hemorrhage rarely fatal, controlled by endoscoic therapeutic measures, TAE, operation Thrombotic
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015
 in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015") Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin
 To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin Omprakash Pansara, MD Brian Kline, MD St. Joseph s Health Family Medicine Residency Program, Syracuse, NY Case 75yr old male, who
To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin Omprakash Pansara, MD Brian Kline, MD St. Joseph s Health Family Medicine Residency Program, Syracuse, NY Case 75yr old male, who
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy
 Curriculum in Cardiology Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy Syed M. Jafri, MD, FACC Detroit, Mich Patients receiving chronic anticoagulation therapy
Curriculum in Cardiology Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy Syed M. Jafri, MD, FACC Detroit, Mich Patients receiving chronic anticoagulation therapy
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY
 EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised
 DABIGATRAN RECOMMENDED What it is Indications Date decision last revised") Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Triple Therapy: A review of the evidence in acute coronary syndrome. Stephanie Kling, PharmD, BCPS Sanford Health
 Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Anti-thrombotics and Colonoscopy. Anna Rahmani, MD. Ph.D. FRCPC
 Anti-thrombotics and Colonoscopy Anna Rahmani, MD. Ph.D. FRCPC DICLOSURES: consultations fees: Servier and Sanofi Pharmaceuticals Thrombosis Clinic Educational Fund: Servier CONFLICT OF INTEREST: NONE
Anti-thrombotics and Colonoscopy Anna Rahmani, MD. Ph.D. FRCPC DICLOSURES: consultations fees: Servier and Sanofi Pharmaceuticals Thrombosis Clinic Educational Fund: Servier CONFLICT OF INTEREST: NONE
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
Management of Novel Oral Anticoagulants in Gastroenterology
 Management of Novel Oral Anticoagulants in Gastroenterology Breakfast with the Experts, CDDW 2018 February 10, 2018 Toronto, ON Brian Yan, MD FRCPC Associate Professor of Medicine Western University Deborah
Management of Novel Oral Anticoagulants in Gastroenterology Breakfast with the Experts, CDDW 2018 February 10, 2018 Toronto, ON Brian Yan, MD FRCPC Associate Professor of Medicine Western University Deborah