Endoscopy in the Era of Anti- Platelet and Anti-Coagulation
|
|
|
- Bertha Walton
- 6 years ago
- Views:
Transcription
1 Endoscopy in the Era of Anti- Platelet and Anti-Coagulation Larissa Fujii-Lau, MD Assistant Professor of Medicine University of Hawaii Clinical Updates in Gastroenterology, Hepatology, and Nutrition 1/20/2017
2 Objectives Discuss 3 key questions to ask when managing antithrombotic agents in patients undergoing endoscopic procedures Review the newer antithrombotic agents Overview of antidotes & reversal agents Summarize recommendations on when to restart antithrombotics
3 Case 1 78M w/ nonvalvular atrial fibrillation (CHA 2 DS 2 -VASc score of 4) on dabigatran (Pradaxa) presents to the ICU with hypotension secondary to cholangitis. As the GI consult team, what would you recommend for management? No ERCP, just medical management ERCP w/ sphincterotomy ERCP w/o sphincterotomy ERCP w/ sphincterotomy if PT is normal
4 Case 2 62M w/ CAD on dual therapy w/ ASA + Prasugrel (Effient) for DES placed 13 months ago is found to have a pancreatic mass for which EUS FNA is anticipated. What would you recommend for his antiplatelet medications? Continue both ASA & Prasugrel Stop both ASA & Prasugrel Continue ASA, stop Prasugrel 5 days prior to EUS Continue ASA, stop Prasugrel 7 days prior to EUS
5 General Principles Individualized If in doubt, contact cardiologist or PCP Weigh risk of thromboembolism and bleeding Thromboembolic events are life-threatening, while GI bleeding can typically be treated Management differs for emergent & elective procedures

6
7 Key Questions to Ask in Every Patient 1) Is this a high or low risk procedure (for bleeding)? 2) Is this a high or low risk patient (for thromboembolism)? 3) Is bridging therapy required?
8 3 Key Questions to Ask in Every Patient 1) Is this a high or low risk procedure (for bleeding)? 2) Is this a high or low risk patient (for thromboembolism)? 3) Is bridging therapy required?
9 High vs Low Risk Procedures High Risk (>1.5% risk of bleed) ERCP w/ sphincterotomy EUS w/ FNA Therapeutic BAE Variceal treatment EMR/ESD Polypectomy Tumor ablation Cyst gastrostomy PEG/J placement Endoscopic hemostasis Ampullary resection Pneumatic/bougie dilation Low Risk ( 1.5% risk of bleed) ERCP w/o sphincterotomy EUS w/o FNA Push enteroscopy or diagnostic BAE Diagnostic EGD, FS, colonoscopy ± mucosal biopsy Capsule endoscopy Enteral stent deployment w/o dilation (controversial) APC Barrett s ablation ASGE Guidelines 2016
10 Controversies Studies of bleeding risk exclude patients on complex antithrombotics Controversial procedures Nonachalasia balloon dilation Enteral stenting ( % risk)
11 3 Key Questions to Ask in Every Patient 1) Is this a high or low risk procedure (for bleeding)? 2) Is this a high or low risk patient (for thromboembolism)? 3) Is bridging therapy required?
12 High Risk Patients Valvular atrial fibrillation Nonvalvular atrial fibrillation CHADS2 or CHA2DS2-VASC score 2 Mechanical heart valves Venous thromboembolism Coronary artery disease ASGE guidelines 2016, AHA Guidelines 2009
13 High Risk Patients Valvular atrial fibrillation Nonvalvular atrial fibrillation CHADS2 or CHA2DS2-VASC score 2 Mechanical heart valves Type of prosthesis- caged-ball valve, tilting disc Site- mitral valve Number- 2 Other- h/o CVA/TIA, cardiac thrombi Venous thromboembolism <3 months Underlying thrombophilia or active cancer Unprovoked Coronary artery disease Acute coronary syndrome Nonstented PCI after MI Stents- BMS < 4 weeks or DES < 12 months CHA2DS2-VASc: CHF- 1 point Htn- 1 point Age 75-2 points DM- 1 point Stroke- 2 points Vascular dz- 1 point Age point Female- 1 point ASGE guidelines 2016, AHA Guidelines 2009
14 Cardiac Stent Occlusion Risk factors for stent occlusion >12 mths out Prior stent occlusion Active ACS STEMI Multivessel PCI DM Renal failure Diffuse CAD
15 Low Risk Patients Uncomplicated or paroxysmal nonvalvular Afib Bioprosthetic valve Mechanical bileaflet aortic valve Venous thromboembolism >12 mths prior
16 Key Questions to Ask in Every Patient 1) Is this a high or low risk procedure (for bleeding)? 2) Is this a high or low risk patient (for thromboembolism)? 3) Is bridging therapy required?
17 Who Requires Bridging Therapy? Procedure Risk Patient Risk Discontinue Antithrombotic Low Low High High Low High Low High Bridging
18 Who Requires Bridging Therapy? Procedure Risk Patient Risk Discontinue Antithrombotic Low Low No Low High No High Low Yes High High Yes Bridging
19 Who Requires Bridging Therapy? Procedure Risk Patient Risk Discontinue Antithrombotic Bridging Low Low No No Low High No Yes High Low Yes No High High Yes Yes
20 Controversial Newer evidence showing higher risk of bleeding with no difference in thromboembolic events BRUISE CONTROL study High risk patients (>5% annual risk) PPM or ICD surgery RCT- continue warfarin vs heparin bridge Thromboembolism uncommon Bleeding more common (16% vs 3.5%) in heparin BRIDGE investigators RCT- LMWH bridge vs placebo Arterial thromboembolism uncommon (0.3% vs 0.4%) Major bleeding more common (3.2% vs 1.3%) in LMWH Birnie et al NEJM 2013, Douketis et al. NEJM 2015
21
22 Basic Principles Results of standard hemostatic tests do not reflect the degree of anticoagulation Vary in responsiveness to the new agents Useful if normal to indicate absence of effect To limit risk of bleeding, 3 t 1/2 is the minimum amt of time to wait before the procedure ~10% of drug concentration 5 t 1/2 is safer
23 Warfarin Inhibits vitamin K dependent clotting factors II, VII, IX, & X and proteins C & S Activity is measured with INR INR decreases to 1.5 in 93% of patients within 5 days of discontinuation ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016
24 Heparins Activate antithrombin III and inhibit factor Xa Unfractionated heparin Half life of mins Effects dissipate 3-4 hrs after discontinuation Low molecular weight heparins (LMWH): Ardeparin, dalteparin, enoxaparin, tinzaparin Duration of action is hrs Last dose should be given 24 hrs before the anticipated procedure at 50% of the total daily dose ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016
25 New Anticoagulant Medications Baron TH. CGH 2014;12:187.
26 Direct Factor Xa Inhibitors Agents: PO- rivaroxaban (Xarelto), apixaban (Eliquis), edoxaban (Savaysa) SQ- fondaparinux (Arixtra) Lab monitoring: None Anti-factor Xa assays correlate w/ levels PT, aptt are insensitive Normal test rule out high circulating drug levels Ceiling effect of aptt, so do not use in toxic levesl ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016
27 Rivaroxaban (Xarelto) Apixaban (Eliquis) Edoxaban (Savaysa) Fondaparinux (Arixtra) Route Use Pharmcokinetics PO PO PO SQ Afib, DVT, THA Afib, THA, VTE Afib, VTE THA, DVT, PE Onset: 1-3 h Peak: 2-4 h T 1/2 : 7-11 h Onset: 1-3 h Peak: 1-3 h T 1/2 : 8-15 h Onset: 1-2 h T 1/2 : h Discontinuation CrCl >90: 1 d CrCl 60-90: 2 d CrCl 30-59: 3 d CrCl 15-29: 4d CrCl >60: 1-2 d CrCl 30-59: 3 d CrCl 15-29: 4 d At least 24 hrs; no data on CrCl <15 Notes 66% renal excretion Avoid in cirrhosis 25% renal excretion Peak- 2h 36 hrs High affinity for antithrombin III ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016
28 Direct Thrombin Inhibitors Agents PO- Dabigatron (Pradaxa) IV- Bivalirudin (Angiomax) SQ- Desirudin (Iprivask) Lab monitoring Thrombin generation time (not available in USA) PT & aptt vary in their sensitivities Normal aptt effectively rules out a clinically significant circulating drug level ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016
29 Route Indication Pharmacokinetics Discontinuation Notes Dabigatran (Pradaxa) PO Afib Onset: 1-3 hrs T 1/2 : hrs High risk procedure CrCl >80: 2-3 d CrCl 50-80: 2-3 d CrCl 30-49: 3-4 d CrCl 29: 4-6 d 80% renal excretion Shorter times in lower risk procedures Bivalirudin (Angiomax) IV HIT Onset: mins T 1/2 : 30 mins Immediately before anesthesia induction Desirudin (Iprivask) SQ DVT proph s/p THA 10 hrs ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016


30
31 Antiplatelet Medications
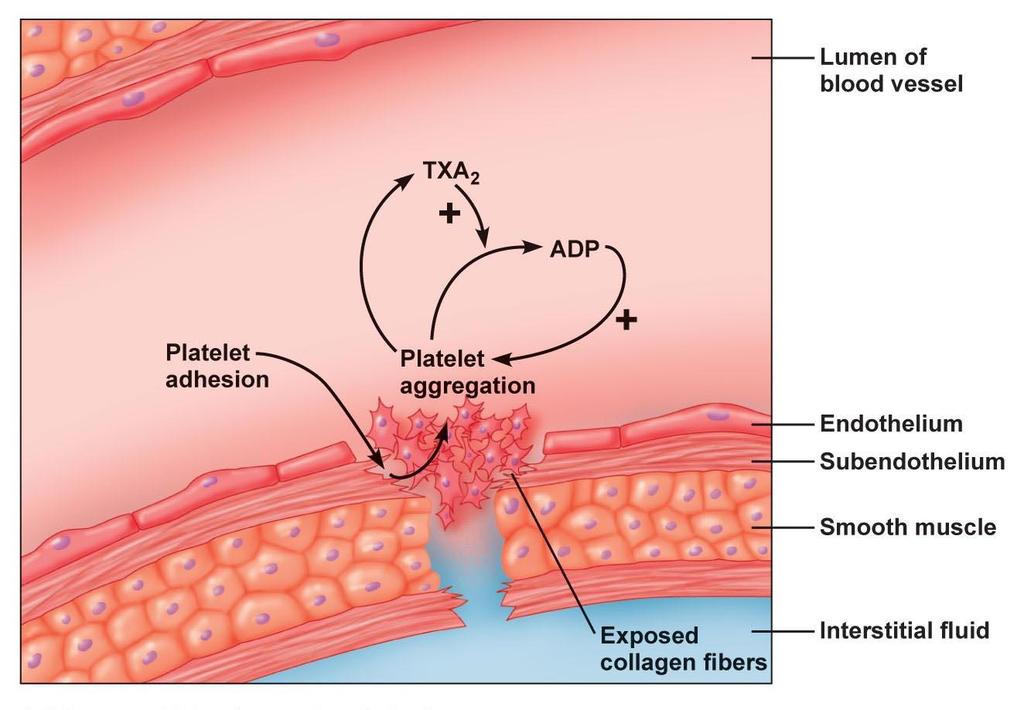
32 COX inhibitors Aspirin: irreversibly inactivates plt COX suppression of thromboxane A2 dependent aggregation Effect lasts for plt s life (7-10 days) NSAIDS: reversible inhibition May be continued safely in perioperative period In the absence of a pre-existing bleeding disorder ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016
33 Thienopyridines Bind to P2Y12 component of ADP receptors on plt surface prevents activation of the GPIIb/IIIa receptor complex plt activation Only inhibits 40-60% of ADP-induced plt activation Indications: ACS ± PCI, CVA, PVD Medications 1 st generation: ticlopidine (Ticlid) 2 nd generation: clopidogrel (Plavix) 3 rd generation: prasugrel (Effient), ticagrelor (Brilinta) ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016
34 Ticlopidine (Ticlid) Clopidogrel (Plavix) Prasugrel (Effient) Ticagrelor (Brilinta) Notes Hematologic side effects (neutropenia, TTP, HUS) limit its use Prodrug that requires mutistep activation Dependent on ABCB1 and CYP2C19 genotypes for activation Prodrug requiring activation in 1 step x more potent then clopidogrel FDA black box warning: should not be used in pt s with active bleeding, h/o TIA/CVA, or likely to undergo urgent CABG Reversible Quickly absorbed Does not require activation Rapid effect that closely parallels drugexposure levels Avoid in hepatic impairment Half-life Discontinuation 7-8 hrs 5-7 days 2-15 hours 5-7 days hrs 3-5 days ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016
35 Vorapaxar (Zontivity) Competitive & selective inhibitor of PAR-1 Major thrombin receptor on human plts Inhibits plt aggregation Indications: MI, PAD risk of MI, CVA, CV death, need for revascularization procedures FDA approved 1/2014 Black box warning- high risk of bleeding Contraindications- h/o CVA/TIA, intracranial hemorrhage Effect remains up to 4 weeks after stopping ASGE guidelines 2016
36
37 Basic Principles Consider waiting to do the higher risk aspects at a later date (i.e. sphincterotomy, polypectomy) Minor bleeding Hold antithrombotic Moderate-severe bleeding Administer antidote if available Transfuse blood components Emergent hemostasis Life-threatening bleeding Consider rapidly reversing agents (i.e. FFP, PCC) Di Minno A. Thrombosis Research. 2015; 136:1074
38 Antidotes: Anticoagulants Warfarin Direct Xa inhibitors Direct thrombin inhibitors Antidote Vitamin K (5-10 mg IV) Activated charcoal (if overdosed within 1-2 hrs prior) Andexanet alfa (only in clinical trials) Others in development: aripazine, anivamersen Dabigatran- idarucizumab, HD ASGE guidelines 2016, Greenwald DA. Best Prac Research Clin Gastroenterol 2016, Di Minno A. Thrombosis Research 2015,Pollack CV. NEJM 2015
39 Goal INR INR level prior to endoscopy has not been shown to be a predictor of rebleeding Effective hemostasis is achieved with moderately elevated INR ASGE guidelines: INR <2.5 is reasonable goal Normalizing INR does not reduce rebleeding Lower goals delay time to endoscopy ASGE guidelines 2016
40 Reversal Agents: Warfarin Recombinant factor VIIa (rfviia) Restrict use to major GIB not adequately controlled by supportive care & endoscopy Prothrombin complex concentrates Clotting factors from pooled/concentrated plasma 3-factor PCCs (Bebulin, Profilnine): II, IX, X With low dose rfviia if 4-factor PCC not available 4-factor PCCs (Kcentra): II, VII, IX, X + protein C, protein S, antithrombin Less volume than FFP (consider in CHF/renal dz to reverse effects of warfarin) ASGE guidelines 2016
41 Reversal Agents: DOAC No proven reversal agents 4-factor PCCs, rfviia Used Unclear role No guarantee benefit Factor VIII inhibitor bypass activity (FEIBA) Used for reversal of dabigatran ASGE guidelines 2016, DiMinno A. Thrombosis Research. 2015
42 Reversal Agents: Antiplatelets Platelet transfusion

43
44 Resumption of Anticoagulants UFH: 2-6 hrs LMWH: hrs if high risk procedure Coumadin: within 24 hrs DOACs: no recommendations Rapid onset and offset of action No good reversal agents Consider 48 hours if low risk of bleeding, longer if higher risk of bleeding ASGE guidelines 2016
45 Resumption of Antiplatelets Reinitiate as soon as hemostasis is achieved If aspirin was discontinued, resume ASAP Studies showing increased risk in 30-day mortality when aspirin not resumed No increase in postprocedural bleeding May consider the use of PPIs Patients with risk factor for GI bleed ASGE guidelines 2016
46 Case 1 78M w/ nonvalvular atrial fibrillation (CHADS2 score 4) on dabigatran (Pradaxa) presents to the ICU with cholangitis. As the GI consult team, what would you recommend for management? No ERCP, just medical management ERCP w/ sphincterotomy ERCP w/o sphincterotomy ERCP w/ sphincterotomy if PT is normal
47 Case 2 62M w/ CAD on dual therapy w/ ASA + Prasugrel (Effient) for DES placed 13 months ago is found to have a pancreatic mass for which EUS FNA is anticipated. What would you recommend for his antiplatelet medications? Continue both ASA & Prasugrel Stop both ASA & Prasugrel Continue ASA, stop Prasugrel 5 days prior to EUS Continue ASA, stop Prasugrel 7 days prior to EUS
48 Summary Always ask yourself the 3 questions when approaching antithrombotic agents Is the procedure high/low risk (bleeding) Is the patient high/low risk (thrombotic events) Is bridging required Thromboembolic events are life-threatening, while bleeding can usually be treated No good lab monitoring for newer agents No proven reversal agents If high risk patient, use older agents

49 Questions?
50 References ASGE Standards of Practice Committee. The management of antithrombotic agents for patients undergoing GI endoscopy. GIE 2016;83:3-16. Baron TH, Kamath PS, and McBane RD. Management of antithrombotic therpay in patients undergoing invasive procedures. NEJM. 2013;368: Baron TH, Kamath PS, and McBane RD. New anticoagulant and antiplatelet agents: A primer for the gastroenterologist. CGH. 2014;12: Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation. NEJM 2013;368: Di Minno A, Spadarella G, Spadarella E, et al. Gastrointestinal bleeding in patients receiving oral anticoagulation: current treatment and pharmacological perspectives. Thrombosis Research. 2015;136: Douketis JD, Spyropoulous AC, Kaatz S, et al. Perioperative bridging anticoagulation in patients with atrial fibrillation. NEJM. 2015;373: Greenwald DA. Managing antithrombotic agents during endsocopy. Best Prac & Researc Clin Gastroenterol. 2016;30: Parekh PJ, Merrell J, Clary M, et al. New anticoagulants and antiplatelet agents: A primer for the clinical gastroenterologist. Am J Gastro. 2014;109:9-19. Pollack Jr CV, Reilly PA, Eikelboom J, et al. Idarucizumab for dabigatran reversal. NEJM. 2015;373:
Endoscopy and the Anticoagulated Patient
 Endoscopy and the Anticoagulated Patient John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Objectives To accurately assess the risk
Endoscopy and the Anticoagulated Patient John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Objectives To accurately assess the risk
on Anti-coagulants -- Is It Safe? And When to Stop?
 Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Anticoagulation Management Around Endoscopy: GI Perspective. Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017
 Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol
 Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Perioperative Anticoagulation Management
 Perioperative Anticoagulation Management ACP Delaware Chapter Scientific Meeting Feb 9, 2019 Andrew Dunn, MD, MPH, MACP Chief, Division of Hospital Medicine Mount Sinai Health System, NY DISCLOSURES Desai
Perioperative Anticoagulation Management ACP Delaware Chapter Scientific Meeting Feb 9, 2019 Andrew Dunn, MD, MPH, MACP Chief, Division of Hospital Medicine Mount Sinai Health System, NY DISCLOSURES Desai
Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥
 Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥 Risk vs Benefit Hemorrhage Thrombosis Hemorrhage rarely fatal, controlled by endoscoic therapeutic measures, TAE, operation Thrombotic
Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥 Risk vs Benefit Hemorrhage Thrombosis Hemorrhage rarely fatal, controlled by endoscoic therapeutic measures, TAE, operation Thrombotic
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Oral anti-thrombotic therapy-management in patients requiring endoscopy
 Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Peri-endoscopic Management of Antithrombotics & Anticoagulants
 Peri-endoscopic Management of Antithrombotics & Anticoagulants ACG Postgraduate Course, Nashville, TN Dec 5, 2015 Vivek Kaul, MD, FACG Segal-Watson Professor of Medicine Chief of Gastroenterology & Hepatology
Peri-endoscopic Management of Antithrombotics & Anticoagulants ACG Postgraduate Course, Nashville, TN Dec 5, 2015 Vivek Kaul, MD, FACG Segal-Watson Professor of Medicine Chief of Gastroenterology & Hepatology
Prostate Biopsy Alerts
 Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Disclosures. Overview. Have you ever. The Perioperative Management of Anticoagulants. No financial conflicts of interest to disclose
 Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Challenging Anticoagulation Case Studies. Earl J. Hope, M.D. Tower Health Cardiology
 Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults
 Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults Purpose: To be used as a common tool for all practitioners involved in the care of patients
Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults Purpose: To be used as a common tool for all practitioners involved in the care of patients
Antiplatelets and Anticoagulants. Helen Leung, PharmD PGY1 Pharmacy Resident Memorial Hermann-Texas Medical Center
 Antiplatelets and Anticoagulants Helen Leung, PharmD PGY1 Pharmacy Resident Memorial Hermann-Texas Medical Center Mechanism 2 http://www.medicinehack.com/2011/07/virchows-triad.html Mechanism 3 http://drtedwilliams.net/kb/index.php?pagename=coagulation%20cascade
Antiplatelets and Anticoagulants Helen Leung, PharmD PGY1 Pharmacy Resident Memorial Hermann-Texas Medical Center Mechanism 2 http://www.medicinehack.com/2011/07/virchows-triad.html Mechanism 3 http://drtedwilliams.net/kb/index.php?pagename=coagulation%20cascade
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Peri-Procedural Management of Antithrombotic Agents
 u Peri-Procedural Management of Antithrombotic Agents An Integrated Care Pathway of the Collaborative Care Network Subject Matter Experts: Will Maxted, MD Veronica Kerner, PharmD Pathway Custodian: Pat
u Peri-Procedural Management of Antithrombotic Agents An Integrated Care Pathway of the Collaborative Care Network Subject Matter Experts: Will Maxted, MD Veronica Kerner, PharmD Pathway Custodian: Pat
Nanik Hatsakorzian Pharm.D/MPH
 Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Peri-Endoscopic Period. Neena S. Abraham MD, MSCE, FACG
 How to Manage Antiplatelet Therapy in the Peri-Endoscopic Period Neena S. Abraham MD, MSCE, FACG Michael E. DeBakey Veterans Affairs Medical Center Sections of Gastroenterology & Health Services Research
How to Manage Antiplatelet Therapy in the Peri-Endoscopic Period Neena S. Abraham MD, MSCE, FACG Michael E. DeBakey Veterans Affairs Medical Center Sections of Gastroenterology & Health Services Research
WARFARIN: PERI OPERATIVE MANAGEMENT
 WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI-OPERATIVE MANAGEMENT
 WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update in Perioperative Anticoagulation and Antiplatelet management
 Update in Perioperative Anticoagulation and Antiplatelet management Grand Rounds October 31, 2014 Brooke Hall, MD Steve Kornfeld, MD Bruce McLellan, MD Nothing to disclose Objectives Describe the updates
Update in Perioperative Anticoagulation and Antiplatelet management Grand Rounds October 31, 2014 Brooke Hall, MD Steve Kornfeld, MD Bruce McLellan, MD Nothing to disclose Objectives Describe the updates
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Disclosure Slide. Controversies in Anticoagulation. Presenter Disclosure Information. Challenges in Anticoagulation
 1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
ADVOCATE HEALTHCARE GUIDELINE FOR ANTITHROMBOTIC REVERSAL
 Minimal clinical evidence exists to support the efficacy of nonspecific procoagulant therapies that promote thrombin formation and antifibrinolytics in the setting of antithrombotic-related bleeding. Hemostatic
Minimal clinical evidence exists to support the efficacy of nonspecific procoagulant therapies that promote thrombin formation and antifibrinolytics in the setting of antithrombotic-related bleeding. Hemostatic
Update on the Management of Anticoagulants and Endoscopy. ACG Eastern Postgraduate Course, Washington, DC June 25, 2016
 Update on the Management of Anticoagulants and Endoscopy ACG Eastern Postgraduate Course, Washington, DC June 25, 2016 Vivek Kaul, MD, FACG Segal-Watson Professor of Medicine Chief of Gastroenterology
Update on the Management of Anticoagulants and Endoscopy ACG Eastern Postgraduate Course, Washington, DC June 25, 2016 Vivek Kaul, MD, FACG Segal-Watson Professor of Medicine Chief of Gastroenterology
Antithrombotics and the Gut
 Antithrombotics and the Gut Panelists: AR Tagahvi MD, N Nozari MD Moderator: S Nasseri-Moghaddam MD, MPH IAGH monthly meeting Shahrivar 1395 (September 2016 ) IAGH Conference Hall Antithrombotic agents
Antithrombotics and the Gut Panelists: AR Tagahvi MD, N Nozari MD Moderator: S Nasseri-Moghaddam MD, MPH IAGH monthly meeting Shahrivar 1395 (September 2016 ) IAGH Conference Hall Antithrombotic agents
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Reversal Agents for Anticoagulants Understanding the Options. Katisha Vance, MD, FACP Alabama Oncology January 28, 2017
 Reversal Agents for Anticoagulants Understanding the Options Katisha Vance, MD, FACP Alabama Oncology January 28, 2017 Objectives Appropriately recommend reversal agents for Vitamin K antagonists Appropriately
Reversal Agents for Anticoagulants Understanding the Options Katisha Vance, MD, FACP Alabama Oncology January 28, 2017 Objectives Appropriately recommend reversal agents for Vitamin K antagonists Appropriately
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
During Procedures. Neena S. Abraham MD, MSc (EPID), FACG
, FACG") Managing Anticoagulants During Procedures Neena S. Abraham MD, MSc (EPID), FACG Professor of Medicine, Mayo Clinic College of Medicine Associate Medical Director, Mayo Clinic i Robert D. and Patricia i
Managing Anticoagulants During Procedures Neena S. Abraham MD, MSc (EPID), FACG Professor of Medicine, Mayo Clinic College of Medicine Associate Medical Director, Mayo Clinic i Robert D. and Patricia i
Emergent Anticoagulation Reversal
 U N C M E D I C A L C E N T E R G U I D E L I N E Emergent Anticoagulation Reversal I. PURPOSE: The purpose of these instructions is to provide guidelines for the reversal of or management of bleeding
U N C M E D I C A L C E N T E R G U I D E L I N E Emergent Anticoagulation Reversal I. PURPOSE: The purpose of these instructions is to provide guidelines for the reversal of or management of bleeding
Clinical Practice Guideline for Anticoagulation Management
 Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
Managing Perioperative Anticoagulation. Edie Shen MD
 Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Anticoagulation Task Force
 Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Patients on anticoagulant or antiplatelet therapy undergoing elective endoscopic procedures
 This is an official Northern Trust policy and should not be edited in any way Patients on anticoagulant or antiplatelet therapy undergoing elective endoscopic procedures Reference Number: NHSCT/11/454
This is an official Northern Trust policy and should not be edited in any way Patients on anticoagulant or antiplatelet therapy undergoing elective endoscopic procedures Reference Number: NHSCT/11/454
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı
 ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA
 Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Post-procedure dose ok after hours. 12 hours (q 24h dosing only) assuming surgical hemostasis; second dose 24 hours after first dose.
 assuming surgical hemostasis; second dose 24 hours after first dose.") Medication Time to wait after last dose Post-procedure dose ok after hours Can pull catheter hours after last dose Can give next dose hours after pulling catheter Enoxaparin (Lovenox) Prophylactic dose
Medication Time to wait after last dose Post-procedure dose ok after hours Can pull catheter hours after last dose Can give next dose hours after pulling catheter Enoxaparin (Lovenox) Prophylactic dose
Gastroenterology & Hepatology Update 2017 Prevention and Endoscopy: A Balancing Act in Eastern Caribbean CME Cruise Dr.
 Kerri Novak MD University of Calgary www.seacourses.com 1 To review and understand the existing bevy of options for anticoagulation and their mechanism of action Familiarize ourselves with options for
Kerri Novak MD University of Calgary www.seacourses.com 1 To review and understand the existing bevy of options for anticoagulation and their mechanism of action Familiarize ourselves with options for
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K. B. Cosmi
 Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Bleeding Management Strategies. Aiming for the best Outcomes August 27, Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM
 Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Reversal of Novel Oral Anticoagulants. Angelina The, MD March 22, 2016
 Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Stolling en anesthesie. Erik Vandermeulen MD, PhD Dept. of Anesthesia
 Stolling en anesthesie Erik Vandermeulen MD, PhD Dept. of Anesthesia Preoperative use of anticoagulation Vitamin K-antagonists (VKA) Fenprocoumon (Marcoumar ) Warfarin (Marevan ) Acenocoumarol (Sintrom
Stolling en anesthesie Erik Vandermeulen MD, PhD Dept. of Anesthesia Preoperative use of anticoagulation Vitamin K-antagonists (VKA) Fenprocoumon (Marcoumar ) Warfarin (Marevan ) Acenocoumarol (Sintrom
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
ADMINISTRATIVE CLINICAL Page 1 of 6
 ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
VENOUS THROMBOEMBOLISM PHARMACOLOGY. University of Hawai i Hilo DNP Program NURS 603 Advanced Clinical Pharmacology Danita Narciso Pharm D
 VENOUS THROMBOEMBOLISM PHARMACOLOGY University of Hawai i Hilo DNP Program NURS 603 Advanced Clinical Pharmacology Danita Narciso Pharm D LEARNING OBJECTIVES Know what factors anticoagulant medications
VENOUS THROMBOEMBOLISM PHARMACOLOGY University of Hawai i Hilo DNP Program NURS 603 Advanced Clinical Pharmacology Danita Narciso Pharm D LEARNING OBJECTIVES Know what factors anticoagulant medications
high thrombotic risk, we recommend continuing aspirin and liaising with a cardiologist about the risk/benefit of discontinuation of P2Y12 receptor
 Guideline 385 Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy
Guideline 385 Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy
THROMBOTIC DISORDERS: The Final Frontier
 THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Anticoagulation Transitions: Perioperative Care
 Anticoagulation Transitions: Perioperative Care Alan Brush, MD, FACP Clinical Co-Director, Anticoagulation Management Service Harvard Vanguard Medical Associates Four Questions for each Consultation 1.
Anticoagulation Transitions: Perioperative Care Alan Brush, MD, FACP Clinical Co-Director, Anticoagulation Management Service Harvard Vanguard Medical Associates Four Questions for each Consultation 1.
Direct Oral Anticoagulant Reversal
 08 June 2018 No. 08 Direct Oral Anticoagulant Reversal M Khattab Moderator: E Hodgson School of Clinical Medicine Discipline of Anaesthesiology and Critical Care CONTENTS INTRODUCTION... 3 Pharmacokinetics
08 June 2018 No. 08 Direct Oral Anticoagulant Reversal M Khattab Moderator: E Hodgson School of Clinical Medicine Discipline of Anaesthesiology and Critical Care CONTENTS INTRODUCTION... 3 Pharmacokinetics
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH
 Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
Holy Crap! Why is a Cardiologist Speaking at a GI Meeting? Jonathan A. Rapp, MD, FACC, FSCAI Cardiologist, Mercy Heart Institute Cincinnati, OH Goals and Objectives Discuss cardiac considerations for patients
ANTICOAGULATION: THE DO'S AND DON'TS OF BRIDGE THERAPY
 ANTICOAGULATION: THE DO'S AND DON'TS OF BRIDGE THERAPY SATURDAY/11:30AM-12:30PM ACPE UAN: 0107-9999-17-236-L01-P 0.1 CEU/1.0 hr Activity Type: Application-Based Learning Objectives for Pharmacists: Upon
ANTICOAGULATION: THE DO'S AND DON'TS OF BRIDGE THERAPY SATURDAY/11:30AM-12:30PM ACPE UAN: 0107-9999-17-236-L01-P 0.1 CEU/1.0 hr Activity Type: Application-Based Learning Objectives for Pharmacists: Upon
Challenges in Coagulation
 Challenges in Coagulation Michael H. Rosove, MD Clinical Professor of Medicine UCLA Division of Hematology-Oncology April 30, 2016 Vitamin K Deficiency Vitamin K1 source from diet Vitamin K2 source from
Challenges in Coagulation Michael H. Rosove, MD Clinical Professor of Medicine UCLA Division of Hematology-Oncology April 30, 2016 Vitamin K Deficiency Vitamin K1 source from diet Vitamin K2 source from
Reversal of Anticoagulants at UCDMC
 Reversal of Anticoagulants at UCDMC Introduction: Bleeding complications are a common concern with the use of anticoagulant agents. In selected situations, reversing or neutralizing the effects of an anticoagulant
Reversal of Anticoagulants at UCDMC Introduction: Bleeding complications are a common concern with the use of anticoagulant agents. In selected situations, reversing or neutralizing the effects of an anticoagulant
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Updates in Coagulation Thrombophilia testing and direct oral anticoagulants. Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017
 Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017 No conflicts of interest Introduction to thrombosis Hemostasis
Updates in Coagulation Thrombophilia testing and direct oral anticoagulants Kevin Y. Chen, MD Hematology and Medical Oncology October 13, 2017 No conflicts of interest Introduction to thrombosis Hemostasis
Xarelto (rivaroxaban) Prescriber Guide
 Prescriber Guide") Xarelto (rivaroxaban) Prescriber Guide October 2018 PP-XAR-IE-0031 Contents Patient Alert Card 4 Dosing Recommendations 4 Stroke prevention in adult patients with non-valvular atrial fibrillation 4 Patients
Xarelto (rivaroxaban) Prescriber Guide October 2018 PP-XAR-IE-0031 Contents Patient Alert Card 4 Dosing Recommendations 4 Stroke prevention in adult patients with non-valvular atrial fibrillation 4 Patients
3/25/2016. Objectives for Pharmacists. Stop the Bleeding! New Reversal Agents. Objectives for Pharmacy Technicians. Assessment Pre-test
 Objectives for Pharmacists Stop the Bleeding! New Reversal Agents Gary D Peksa, Pharm.D., BCPS Clinical Pharmacy Specialist, Emergency Medicine Rush University Medical Center Review current strategies
Objectives for Pharmacists Stop the Bleeding! New Reversal Agents Gary D Peksa, Pharm.D., BCPS Clinical Pharmacy Specialist, Emergency Medicine Rush University Medical Center Review current strategies
Chapter 1 The Reversing Agents
 Available Strategies to Reverse Anticoagulant Medications Michael L. Smith, Pharm. D., BCPS, CACP East Region Pharmacy Clinical Manager Hartford HealthCare Objectives: Describe the pharmacological agents
Available Strategies to Reverse Anticoagulant Medications Michael L. Smith, Pharm. D., BCPS, CACP East Region Pharmacy Clinical Manager Hartford HealthCare Objectives: Describe the pharmacological agents
A Cascade of Updates: Hot Topics in Anticoagulation
 A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Slide 1: Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Alberta Colorectal Cancer Screening Program (ACRCSP) Antithrombotic Management
 Antithrombotic Management") Alberta Colorectal Cancer Screening Program (ACRCSP) Antithrombotic Management Assessment Tools and Suggested Management for the Patient on Antithrombotics Undergoing a Screening-Related Colonoscopy Version
Alberta Colorectal Cancer Screening Program (ACRCSP) Antithrombotic Management Assessment Tools and Suggested Management for the Patient on Antithrombotics Undergoing a Screening-Related Colonoscopy Version
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Challenges in Anticoagulation Bridging and Emerging Therapies. Disclosures and Relationships. Objectives. Dr. Cumbler has no conflicts of interest
 Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
DISCLOSURE. What I am Talking About. Rational Use of Antiplatelet Agents. Aspirin. Tom DeLoughery, MD MACP FAWM
 Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Acute Coronary Syndrome refers to any
 IMPACTING THE CLOTTING CASCADE: PRACTICE IMPLICATIONS FOR ANTICOAGULANT AND ANTIPLATELET PHARMACOLOGY Cynthia L. Webner DNP, CCNS, ACNPC-AG, CCRN-CMC, CHFN NTI Class Code A75m462 Acute Coronary Syndrome
IMPACTING THE CLOTTING CASCADE: PRACTICE IMPLICATIONS FOR ANTICOAGULANT AND ANTIPLATELET PHARMACOLOGY Cynthia L. Webner DNP, CCNS, ACNPC-AG, CCRN-CMC, CHFN NTI Class Code A75m462 Acute Coronary Syndrome
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Bridging anticoagulation definition
 Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
MANAGEMENT OF OVER-ANTICOAGULATION. Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas
 MANAGEMENT OF OVER-ANTICOAGULATION Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas Risk of Intracranial Hemorrhage in Outpatients (From Management of Oral Anticoagulant
MANAGEMENT OF OVER-ANTICOAGULATION Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas Risk of Intracranial Hemorrhage in Outpatients (From Management of Oral Anticoagulant
Disclosure and Conflict of Interest
 A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
A Cascade of Updates: Hot Topics in Anticoagulation Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Golden L. Peters, PharmD, BCPS Associate
New Age Anticoagulants: Bleeding Considerations
 Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
OLD AND NEW ANTIPLATELET DRUGS
 OLD AND NEW ANTIPLATELET DRUGS Franklin A. Bontempo, M.D October 19, 2017 Update in Internal Medicine Associate Professor of Medicine Division of Hematology/Oncology University of Pittsburgh School of
OLD AND NEW ANTIPLATELET DRUGS Franklin A. Bontempo, M.D October 19, 2017 Update in Internal Medicine Associate Professor of Medicine Division of Hematology/Oncology University of Pittsburgh School of
Xarelto (rivaroxaban)
") Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Use of Anticoagulant Reversal Agents
 Use of Anticoagulant Reversal Agents Lori Shutter, MD shutterla@upmc.edu Vice Chair of Education Director, Neurocritical Care Program Professor, Critical Care Medicine, Neurology & Neurosurgery University
Use of Anticoagulant Reversal Agents Lori Shutter, MD shutterla@upmc.edu Vice Chair of Education Director, Neurocritical Care Program Professor, Critical Care Medicine, Neurology & Neurosurgery University
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery. Alex C. Spyropoulos MD, FACP, FCCP, FRCPC
 who Need Elective Surgery. Alex C. Spyropoulos MD, FACP, FCCP, FRCPC") The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery Alex C. Spyropoulos MD, FACP, FCCP, FRCPC Professor of Medicine Hofstra Northwell School of Medicine
The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery Alex C. Spyropoulos MD, FACP, FCCP, FRCPC Professor of Medicine Hofstra Northwell School of Medicine
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation
 HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
Perioperative Management of the Anticoagulated Patient
 Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of Warfarin Interruption
 Perioperative Management of Warfarin Interruption Victoria Lambert, PharmD, CACP Medication Management Pharmacist William W. Backus Hospital Faculty Disclosures There are no actual or potential conflicts
Perioperative Management of Warfarin Interruption Victoria Lambert, PharmD, CACP Medication Management Pharmacist William W. Backus Hospital Faculty Disclosures There are no actual or potential conflicts
with Gastrointestinal bleeding and in
 Management of Anticoagulants in patients with Gastrointestinal bleeding and in Elective Endoscopic procedures. S.A.Taghavi M.D., Associate professor of internal Medicine, Shiraz University of Medical Sciences
Management of Anticoagulants in patients with Gastrointestinal bleeding and in Elective Endoscopic procedures. S.A.Taghavi M.D., Associate professor of internal Medicine, Shiraz University of Medical Sciences
Dr Calum Young Cardiologist Tauranga
 Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated) GPCME 2016: Anticoagulation
Dr Calum Young Cardiologist Tauranga 8:30-9:25 WS #93: New Oral Anticoagulant Drugs and Management of AF 9:35-10:30 WS #105: New Oral Anticoagulant Drugs and Management of AF (Repeated) GPCME 2016: Anticoagulation
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
Perioperative Management of Novel Oral Anticoagulants (NOACs) Hardy Shah PharmD NEANA March 2017
 Hardy Shah PharmD NEANA March 2017") Perioperative Management of Novel Oral Anticoagulants (NOACs) Hardy Shah PharmD NEANA March 2017 Disclosures Presenter has no actual or potential conflicts of interest in relation to this program Question
Perioperative Management of Novel Oral Anticoagulants (NOACs) Hardy Shah PharmD NEANA March 2017 Disclosures Presenter has no actual or potential conflicts of interest in relation to this program Question
Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants
 Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants Van Hellerslia, PharmD, BCPS, CACP Clinical Assistant Professor Temple University School of Pharmacy Over 4 million
Ischemic and hemorrhagic strokes in the context of the direct acting oral anticoagulants Van Hellerslia, PharmD, BCPS, CACP Clinical Assistant Professor Temple University School of Pharmacy Over 4 million
Who uses these medications? Assessing Patients Who Take Blood-Altering Medications. 3 Types of Acute Coronary Syndromes. Platelet-Related Fatalities
 Assessing Patients Who Take Blood-Altering Medications Ann Eshenaur Spolarich, RDH, PhD Herman Ostrow School of Dentistry of USC; Arizona School of Dentistry and Oral Health; University of Maryland Dental
Assessing Patients Who Take Blood-Altering Medications Ann Eshenaur Spolarich, RDH, PhD Herman Ostrow School of Dentistry of USC; Arizona School of Dentistry and Oral Health; University of Maryland Dental