Guidelines for the management of Hypertension
|
|
|
- Caitlin Mosley
- 6 years ago
- Views:
Transcription
1 Guidelines for the management of Hypertension Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the author(s) in conjunction with the paediatric nephrology team at the University Hospital of Wales, Cardiff reviewing available evidence/opinion. They were designed for use by paediatric nephrologists at the University Hospital of Wales, Cardiff for children under their care. They are neither policies nor protocols but are intended to serve only as guidelines. They are not intended to replace clinical judgment or dictate care of individual patients. Responsibility and decision-making (including checking drug doses) for a specific patient lie with the physician and staff caring for that particular patient. Dr Graham Smith May 2017
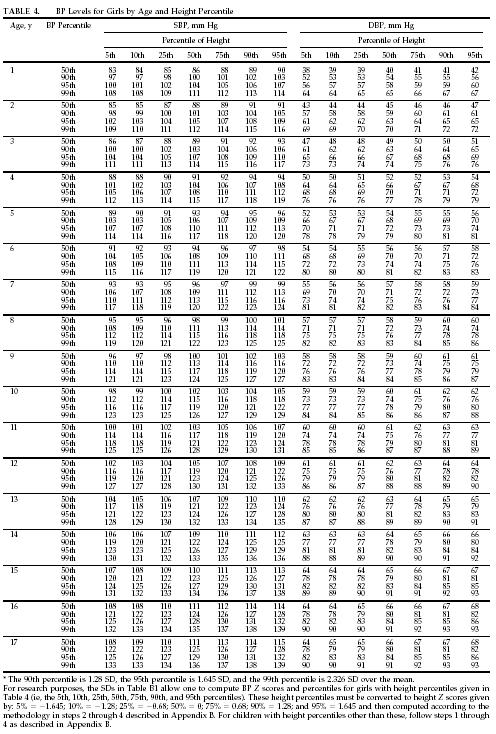
2 Summary These guidelines are aimed at providing the doctors presented with a child with hypertension with information to help identify the underlying problem and to guide treatment. Introduction Measurement of blood pressure should be part of the routine assessment of any child seen as an in patient or out patient. Methods of measuring blood pressure are dealt with in a separate guideline. Hypertension may be secondary to an underlying pathology (usually renal). However with the growing problem of obesity, more children are presenting with primary hypertension. Definitions Blood pressure is a continuous variable and the differentiation between normal and abnormal has been defined statistically. There has also been debate about the relative importance of systolic and diastolic hypertension. It is felt that systolic blood pressure is probably of greater relevance and a value > 95th centile for age and height using appropriate centile charts measured on three occasions defines someone as being hypertensive (see appendix 1). Any measurements taken using an automated device should be confirmed manually and if possible ambulatory measurement should be used to confirm mild hypertension. Severe hypertension is a systolic blood pressure > 95th centile for age and height with symptoms (headache, visual disturbances, neurological disturbances). This requires urgent investigation and management. Aetiology Secondary hypertension is more common than primary hypertension in young children. However primary hypertension is now starting to become the dominant cause of hypertension in children older than 6 years of age as a result of the growing problem of obesity. Underlying causes: Renal disease. Renal parenchymal (most common) and renal vascular disease may cause hypertension. Wilms tumours are commonly associated with hypertension Coartaction of the aorta should be excluded Endocrine causes (Cushings / Conns / Phaeochromocytoma) Rare renal tubular single gene disorders (Gordons, Liddles, apparent mineralocorticoid excess (AME) and glucocorticoid remediable aldosteronism (GRA) can cause hypertension (see below). Elevated Intracranial pressure Pain Monogenic hypertension Hypertension in this group of patients is secondary to salt and water retention which is not a result of primary renal disease, but because of dysfunction of a single gene.
3 Even though rare, these can result in severe hypertension and cause abnormalities in serum potassium levels and alkalosis with suppression of renin and aldosterone. The causes, along with electrolyte and biochemical abnormalities seen in these conditions are listed below: Inheritance pattern Renin Aldosterone K + HCO 3 FE Na Diagnostic indicators AME AR GRA AD CAH AR Liddle syndrome AD Gordon syndrome AD FH II AD N or FGR AD/AR N or Prolonged cortisol half life Urinary cortisol metabolities increased Urinary cortisone metabolities decreased Urinary 18- oxotetrahydrocortisol and 18-ydroxycortisol: tetrahydroaldosterone ratio increased Angiotensin II decreased Ambiguous genitalia/menorrhoea Virilisation/Precocious puberty Family history, clinical and lab findings Family history, clinical and lab findings H-P AD N or AME, syndrome of apparent mineralocorticoid excess; CAH, congenital adrenal hyperplasia; FeNa, fractional excretion of sodium; GRA, glucocorticoid remediable aldosteronism; FGR, familial glucocorticoid resistance; FH II, familial hyperaldosteronism type II; H-P hypertension exacerbated by pregnancy Investigations First line: History and examination, to include palpation of the femoral pulses, comparison of the right arm and lower limb pulse and fundoscopy. Consider stigmata of underlying causes of hypertension (see appendix 2). Urinalysis and early morning urine for protein:creatinine ratio. Urea & Electrolytes / Bone profile / Magnesium / Full Blood Count / Glucose / Bicarbonate / Thyroid Function Tests / Lipid profile / Uric acid Renin and aldosterone (after 30 minutes supine; ideally before starting treatment). Discuss with biochemistry Ultrasound of urinary tract WITH doppler imaging of renal vessels Consider ambulatory BP monitoring. Interpretation needs comparison with an appropriate reference range. A form for use at UHW can be downloaded by clicking here. Further assessment of end organ damage CXR/ECG/ECHO/Ophthalmology Second Line: (discuss with paediatric nephrologist) Urine steroid profile (24 hour collection where practical and random urine if not).
4 Urine or plasma catecholamines. ACE ASOT/autoimmune profile/complement (C3 & C4) / ANCA Random cortisol, DMSA scan MRA / Captopril MAG 3 / Renal angiography MRI / MIBG scan Management Emergency management of severe hypertension: Discuss with paediatric nephrologist Patients may require management on PICU or renal ward Aim for a slow reduction over 72 hours to avoid a sudden drop in perfusion pressure which may cause catastrophic cerebral ischaemia. Aim for one third of overall desired reduction in the 1st 24 hours. Avoid mydriatics for fundoscopy. Site two IV cannulae. One is used to deliver IV antihypertensive agent and the second to deliver a 10ml/kg saline bolus if the blood pressure falls too quickly. The choice of IV agent should be one with which the clinician is familiar. The options include labetalol, nicardipine and sodium nitroprusside. ANother is hydralazine, but this tends to be used more for treatment of neonates. These agents should be administered using a sliding scale to titrate the dose administered with BP, measured every 15 minutes (usually monitored via arterial line in patients on PICU). An arterial line is mandatory when using sodium nitroprusside. Dosages: Labetalol Sodium nitroprusside Nicardipine mg/kg/hr µg/kg/min. Protect from light and should have an arterial line for bp monitoring. Advantage of very short t½. Need to check cyanide level µg/kg/min BNF recommends to infuse at concentration of 0.1mg/ml. Can infuse higher concentrations via a central line. If fluid volume is an issue concentrations up to 0.5mg/ml have been used peripherally [1]. Once control has been established with parenteral agents, convert to oral medications as below. Asymptomatic patients It may be possible to achieve gradual blood pressure reduction with oral therapy using a calcium antagonist. Start with a small dose of nifedipine (0.1 mg/kg) Oral maintenance treatment Aim to maintain BP <95th centile but preferably the 50th centile in patients with renal disease [2]. Choice of oral agents (also see Specific considerations for treatment of hypertension):
5 Angiotensin converting enzyme inhibitors (ACEi; e.g. enalapril / lisinopril) or angiotensin II receptor antagonists (ARB; valsartan, irbesartan) o May cause hyperkalaemia. Monitor serum [K + ]; check levels within 7 days of starting or increasing dose o Avoid if renal artery stenosis suspected o Avoid in the early period after renal transplantation Beta blockers: Metoprolol has selective blockade and non-renal excretion. Use if concerns about the possibility of renal artery stenosis or ACE/ARB contraindicated Calcium channel blockers: Amlodipine/ nifedipine LA Consider diuretics if fluid overload is contributing. First line treatment in acute nephritis. Once daily dosing schedules should improve compliance. Non-pharmacological management Consider the following advice in all children with hypertension Sodium restriction Weight loss Exercise Attention to other cardiovascular risk factors: Control of blood lipids, glycaemic control in diabetes Specific considerations for treatment of hypertension Following renal transplantation. The use of angiotensin converting enzyme inhibitors or angiotensin II receptor antagonists are not generally used in the early post transplant phase due to the difficulty interpreting elevated creatinine. Calcium channel blockers are a sensible choice and there is evidence that use of these agents in the peri-operative period reduce the incidence of post-transplant acute tubular necrosis [3]. Once stable renal function is achieved there are potential benefits from using an ACEi/ARB. Wilms Tumour. Hypertension in Wilms tumour (WT) patients has been reported to be associated with elevated plasma renin levels in 80% of cases [4]. ACE inhibitors should be considered in WT patients with hypertension prior to nephrectomy. Phaeochromocytoma [5, 6]. This is characterised by episodic hypertension/palpitations and sweating. Specific investigations should include: Urine catecholamines: VMA/HVA, abdominal USS, abdominal MRI, MIBG isotope scan. Control of hypertension is required before surgery using alpha and beta blockade. The alpha blocker of choice is phenoxybenzamine and the beta blocker is propanolol. Stop antihypertensives 8-12 before theatre on discussion with the anaesthetist. Renovascular disease [7]. This is characterised by very high renin levels and may be secondary to renal artery stenosis or obstruction to vessels by cysts in polycystic kidney disease. In this situation, intra-glomerular pressure depends on efferent arteriolar constriction and
6 therefore ACE inhibitors or angiotensin II receptor antagonists must be used with caution as these agents cause efferent arteriolar dilatation. Investigations may include: MRA/Angiogarphy. Treatment: metoprolol / amlodipine / other. Neonatal hypertension [8]. Intravenous agents described in the literature are: labetalol, hydralazine and nicardipine. Oral agents in suspensions used in neonates are: propanolol, hydralazine and captopril. If using an ACEi renal function must be carefully monitored as neonates have a greater reliance on the renin-angiotensin system for maintenance of intraglomerular capillary pressure. Rare single gene disorders Glucocorticoid remedial hyperaldosteronism (GRA), Gordons [9], Liddle syndrome [10] and AME (apparent mineralocorticoid excess) are characterised by hypertension due to interruption of the renin-aldosterone axis. They are often associated with hypo- or hyperkalaemia and diagnosis is with a urine steroid profile. Treatment includes the use of potassium sparing diuretics. References 1. Flynn, J. T., Mottes, T. A., Brophy, P. D., Kershaw, D. B., Smoyer, W. E., & Bunchman, T. E. (2001). Intravenous nicardipine for treatment of severe hypertension in children. Journal of Pediatrics, 139(1), Simonetti GD, Santoro L, Ferrarini A, Crosazzo-Franscini L, Fossali E, Bianchetti MG. (2007) Systemic hypertension and proteinuria in childhood chronic renal parenchymal disease: role of antihypertensive drug management. Paediatr Drugs 9: The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics (2004)114: M.H. Maas, K. Cransberg, M. van Grotel, R. Pieters, M.M. van den Heuvel- Eibrink. (2007) Renin-induced hypertension in Wilms tumor patients. Pediatr Blood Cancer. 48(5): Favia G, Lumachi F, Polistina F, D'Amico DF (1998) Pheochromocytoma, a rare cause of hypertension: long-term follow-up of 55 surgically treated patients. World J Surg 22: ; discussion Maher ER, Eng C (2002) The pressure rises: update on the genetics of phaeochromocytoma. Hum Mol Genet 11: Tullus K, Brennan E, Hamilton G, et al. (2008) Renovascular hypertension in children. Lancet 371: Flynn JT (2000) Neonatal hypertension: diagnosis and management. Pediatr Nephrol 14: Kamel KS, Oh MS, Halperin ML (2002) Bartter's, Gitelman's, and Gordon's syndromes. From physiology to molecular biology and back, yet still some unanswered questions. Nephron 92 Suppl 1: Warnock DG (1998) Liddle syndrome: an autosomal dominant form of human hypertension. Kidney Int 53:

7 Appendix 1. Blood pressure centiles based on gender, age, and height
8
9 Appendix 2. Examination findings. Finding Possible Aetiology Vital signs Tachycardia Decreased lower extremity pulses; drop in BP from upper to lower extremities Hyperthyroidism, phaeochromocytoma, neuroblastoma, primary hypertension SPARCstation of the aorta Eyes Retinal changes Severe hypertension, more likely to be associated with secondary hypertension ENT Adenotonsillar hypertrophy Suggests association with sleepdisordered breathing (sleep apnoea), snoring Height / Growth retardation Chronic renal failure weight Obesity (high BMI) Primary hypertension Truncal obesity Cushing syndrome, insulin resistance syndrome Head and Moon facies Cushing syndrome neck Elfin facies Williams syndrome Webbed neck Turner syndrome Thyromegaly Hyperthyroidism Skin Pallor, flushing, diaphoresis Pheochromocytoma Acne, hirsutism, striae Cushing syndrome, anabolic steroid abuse Café-au-lait spots Neurofibromatosis Adenoma sebaceum Tuberous sclerosis Malar rash Systemic lupus erythematosus Acanthrosis nigricans Type 2 diabetes Chest Widely spaced nipples Turner syndrome Heart murmur Coarctation of the aorta Friction rub Systemic lupus erythematosus (pericarditis), collagen-vascular disease, end stage renal disease with uremia Apical heave LVH/chronic hypertension Abdomen Mass Wilms tumor, neuroblastoma, phaeochromocytoma Epigastric/flank bruit Renal artery stenosis Palpable kidneys Polycystic kidney disease, hydronephrosis, multicystic-dysplastic kidney, mass (see above) Genitalia Ambiguous/virilization Adrenal hyperplasia Extremities Joint swelling Systemic lupus erythematosus, collagen vascular disease Muscle weakness Hyperaldosteronism, Liddle syndrome Adapted from Flynn JT. Prog Pediatr Cardiol. 2001;12:
Hypertension in Paediatric Haematology/Oncology
 in Paediatric Haematology/Oncology Overview and aetiology: is a common problem in Paediatric Haematology and Oncology patients. There are a number of causes, some related to the disease itself or the treatment,
in Paediatric Haematology/Oncology Overview and aetiology: is a common problem in Paediatric Haematology and Oncology patients. There are a number of causes, some related to the disease itself or the treatment,
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Hypertension in Paediatrics, Renal Unit, Royal Hospital for Children
 CLINICAL GUIDELINE Hypertension in Paediatrics, Renal Unit, Royal Hospital for Children Please note: The following guidelines have not been assessed according to the AGREE (Appraisal of Guidelines for
CLINICAL GUIDELINE Hypertension in Paediatrics, Renal Unit, Royal Hospital for Children Please note: The following guidelines have not been assessed according to the AGREE (Appraisal of Guidelines for
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Wessex Paediatric Oncology Supportive Care Guidelines: Management of Hypertension.
 Wessex Paediatric Oncology Supportive Care Guidelines: Management of Hypertension. Scope This guideline applies to all paediatric oncology patients in the region. It does not apply to neonates on neonatal
Wessex Paediatric Oncology Supportive Care Guidelines: Management of Hypertension. Scope This guideline applies to all paediatric oncology patients in the region. It does not apply to neonates on neonatal
The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents
 National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children
INTRODUCTION TO RENAL SYSTYEM IN PEDIATRICS
 INTRODUCTION TO RENAL SYSTYEM IN PEDIATRICS ANATOMY & PHYSIOLOGY OF KIDNEY Same as that of an adult but with few differences ; 1. Length approx. 6 cm and weight 24gm in a full term newborn as compared
INTRODUCTION TO RENAL SYSTYEM IN PEDIATRICS ANATOMY & PHYSIOLOGY OF KIDNEY Same as that of an adult but with few differences ; 1. Length approx. 6 cm and weight 24gm in a full term newborn as compared
Secondary hypertension How to approach?
 Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Presentation of hypertensive emergency
 Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Pediatric Hypertension. Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019
 Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Secondary hypertension in the pediatric population
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 12-2015 Secondary hypertension in the pediatric population Ashley M. Gefen Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 12-2015 Secondary hypertension in the pediatric population Ashley M. Gefen Washington University School of Medicine
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
A guideline on Neonatal Hypertension
 A guideline on Neonatal Hypertension Authors: Dr Aravind Shastri, Consultant (Neonatology and Cardiology), Colchester General Hospital For use in: Eastern Neonatal Units Guidance specific to the care of
A guideline on Neonatal Hypertension Authors: Dr Aravind Shastri, Consultant (Neonatology and Cardiology), Colchester General Hospital For use in: Eastern Neonatal Units Guidance specific to the care of
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM
 MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
DIAGNOSIS AND TREATMENT OF HYPERTENSION IN CATS AND DOGS
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk DIAGNOSIS AND TREATMENT OF HYPERTENSION IN CATS AND DOGS Author : Rachel Sant Categories : Vets Date : May 28, 2012 Rachel
Vet Times The website for the veterinary profession https://www.vettimes.co.uk DIAGNOSIS AND TREATMENT OF HYPERTENSION IN CATS AND DOGS Author : Rachel Sant Categories : Vets Date : May 28, 2012 Rachel
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Children with Hypertension in ED
 Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
CLINICAL GUIDELINE. Document No:CG38 *All Sites Management of adult patients referred to South Tees University Hospitals for hypertension.
 GUIDELINE CLINICAL GUIDELINE Document No:CG38 *All Sites Management of adult patients referred to South Tees University Hospitals for hypertension. TITLE Management of adult patients referred to South
GUIDELINE CLINICAL GUIDELINE Document No:CG38 *All Sites Management of adult patients referred to South Tees University Hospitals for hypertension. TITLE Management of adult patients referred to South
Agenda. Management of Accelerated Hypertension (Updated in 2017) Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017
 Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017") Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY
 CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Secondary hypertension is defined as being
 Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI
 DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009
 www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers PROTEINURIA
www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers PROTEINURIA
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
2015/03/11. Dr Patience Sigwadi Paediatric Nephrologist UNITAS NETCARE. Case
 Dr Patience Sigwadi Paediatric Nephrologist UNITAS NETCARE Case 1 Case Report 17-month-old female toddler Presented with hypertensive encephalopathy manifesting with convulsions right hemiparesis and blindness.
Dr Patience Sigwadi Paediatric Nephrologist UNITAS NETCARE Case 1 Case Report 17-month-old female toddler Presented with hypertensive encephalopathy manifesting with convulsions right hemiparesis and blindness.
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
Southern Derbyshire Shared Care Pathology Guidelines. Secondary Hypertension
 Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Genetic factors. A number of genetic factors or interactions between genes play a major role in essential hypertension.
 Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
HYPERTENSION 4.0 Contact Hours Presented by: CEU Professor
 HYPERTENSION 4.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of these materials is
HYPERTENSION 4.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of these materials is
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus
 Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Unilateral renal agenesis does it matter?
 Clinical Research Facility Central Manchester University Hospitals NHS Foundation Trust Unilateral renal agenesis does it matter? Nicholas J A Webb BMedSci DM FRCP FRCPCH Honorary Professor of Paediatric
Clinical Research Facility Central Manchester University Hospitals NHS Foundation Trust Unilateral renal agenesis does it matter? Nicholas J A Webb BMedSci DM FRCP FRCPCH Honorary Professor of Paediatric
Chronic Pediatric Hypertension
 Chronic Pediatric Hypertension Nephrology Grand Round 3/13/2015 Mahmoud Kallash M.D Outline Definition of hypertension (HTN) Challenges in diagnosing HTN Epidemiology Causes and evaluation of HTN Management
Chronic Pediatric Hypertension Nephrology Grand Round 3/13/2015 Mahmoud Kallash M.D Outline Definition of hypertension (HTN) Challenges in diagnosing HTN Epidemiology Causes and evaluation of HTN Management
Amlodipine plus Lisinopril Tablets AMLOPRES-L
 Amlodipine plus Lisinopril Tablets AMLOPRES-L COMPOSITION AMLOPRES-L Each uncoated tablet contains: Amlodipine besylate equivalent to Amlodipine 5 mg and Lisinopril USP equivalent to Lisinopril (anhydrous)
Amlodipine plus Lisinopril Tablets AMLOPRES-L COMPOSITION AMLOPRES-L Each uncoated tablet contains: Amlodipine besylate equivalent to Amlodipine 5 mg and Lisinopril USP equivalent to Lisinopril (anhydrous)
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
0BCore Safety Profile. Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg SE/H/PSUR/0024/003 Date of FAR:
/strength: Film-coated tablet 40, 80, 160, 320 mg SE/H/PSUR/0024/003 Date of FAR:") 0BCore Safety Profile Active substance: Valsartan Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg P-RMS: SE/H/PSUR/0024/003 Date of FAR: 28.02.2013 4.2 Posology and method of administration
0BCore Safety Profile Active substance: Valsartan Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg P-RMS: SE/H/PSUR/0024/003 Date of FAR: 28.02.2013 4.2 Posology and method of administration
Functional vascular disorders
 Functional vascular disorders Raynaud s phenomenon Raynaud s phenomenon Refers to Intermittent,bilateral attacks of ischemia of the fingers or toes, and sometimes ears or nose. It clinically manifests
Functional vascular disorders Raynaud s phenomenon Raynaud s phenomenon Refers to Intermittent,bilateral attacks of ischemia of the fingers or toes, and sometimes ears or nose. It clinically manifests
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
major public health burden
 HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Karim Said. 41 year old farmer. Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy
 Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Over- and underfill: not all nephrotic states are equal. Detlef Bockenhauer
 Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
9/11/2012. Chapter 11. Learning Objectives. Learning Objectives. Endocrine Emergencies. Differentiate type 1 and type 2 diabetes
 Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 9 March 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 March 2011 TAREG 3 mg/ml oral solution B/1 160 ml (CIP code: 491 474-8) Applicant: NOVARTIS PHARMA SAS valsartan
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 March 2011 TAREG 3 mg/ml oral solution B/1 160 ml (CIP code: 491 474-8) Applicant: NOVARTIS PHARMA SAS valsartan
DIRECT RENIN INHIBITOR (DRI) EFFECT ON GFR AND USE IN RENAL ARTERY STENOSIS SCREENING
 EFFECT ON GFR AND USE IN RENAL ARTERY STENOSIS SCREENING") DIRECT RENIN INHIBITOR (DRI) EFFECT ON GFR AND USE IN RENAL ARTERY STENOSIS SCREENING Harold Thomas Pretorius, MD, PhD, Nichole Richards, and Michael Harrell Abstract Objective: A new method using a nuclear
DIRECT RENIN INHIBITOR (DRI) EFFECT ON GFR AND USE IN RENAL ARTERY STENOSIS SCREENING Harold Thomas Pretorius, MD, PhD, Nichole Richards, and Michael Harrell Abstract Objective: A new method using a nuclear
HYPERTENSION (Blood Pressure in Childhood)
") Measurement of Blood Pressure Normal Blood Pressure When should BP be measured? Definition of Hypertension Signs & Symptoms Causes of Transient Hypertension Causes of Sustained Hypertension Investigation
Measurement of Blood Pressure Normal Blood Pressure When should BP be measured? Definition of Hypertension Signs & Symptoms Causes of Transient Hypertension Causes of Sustained Hypertension Investigation
DRUG GUIDELINE. HYDRALAZINE (Intravenous severe hypertension in pregnancy)
") DRUG GUIDELINE HYDRALAZINE (Intravenous severe hypertension SCOPE (Area): FOR USE IN: Labour Ward, HDU, Theatre and ED EXCLUSIONS: Paediatrics (seek Paediatrician advice) and other general wards. SCOPE
DRUG GUIDELINE HYDRALAZINE (Intravenous severe hypertension SCOPE (Area): FOR USE IN: Labour Ward, HDU, Theatre and ED EXCLUSIONS: Paediatrics (seek Paediatrician advice) and other general wards. SCOPE
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
TIP. Documentation and coding guide. Disease definitions* Prevalence and statistics associated with HTN**
 Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and