How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
|
|
|
- Susan Annabelle Collins
- 5 years ago
- Views:
Transcription

1 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016


2 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423

3 Hypertension often poorly controlled Scottish Health Survey 2009
4 Hypertension targets just got lower SPRINT investigators NEJM :
5 Secondary hypertension 5-10% of essential hypertension cases Clinical clues important Age based approach essential
6 Age group Secondary hypertension according to age % with underlying cause Most common cause Children (<12 years) 70-85% Renal parenchymal disease Coarctation of aorta Adolescents (12-18 years) 10-15% Renal parenchymal disease Coarctation of aorta Young adults (19-39 years) 5% Fibromuscular dysplasia Renal parenchymal disease Middle aged adults (40-65 years) 8-12% Primary Aldosteronism Obstructive Sleep Apnoea Cushing s syndrome Phaeochromocytoma Older adults 17% Atherosclerotic renovascular disease Renal failure hypothyroidism
7 Secondary hypertension 5-10% of essential hypertension cases Clinical clues important Age based approach essential Consider if: Severe or resistant hypertension Child/adolescent Worsening of previously stable hypertension Malignant hypertension No other risk factors identified and age <30
8 Secondary hypertension: investigations Renal function and urinalysis Renal imaging Ultrasound MRA renal arteries Aldosterone to renin ratio (ARR) 24h urine for catecholamines/metanephrines Only if clinical suspicion
9 Case 1: Just another case of hypertension.? 32 y female 3 years of hypertension, well controlled on ramipril But now BP difficult to control (162/95 mm/hg) despite addition of amlodipine UE: Na 136, K 4.1 Cl 95 Ur 4.2 Cr 68 Plasma aldosterone (supine) 420 pmol/l ( ), plasma renin activity (PRC) 1.2 µiu/ml (5-44.9) Aldosterone to renin ratio (ARR) 350
10 The myths of Primary Aldosteronism (PA)? PA is a rare cause of hypertension Serum potassium must be normal All the drugs must be stopped! Making the diagnosis doesn t matter- just lower the blood pressure!
11 Frequency of aldosteronism in hypertension: 4.8% Aldosterone Producing Adenoma 6.4% Idiopathic Hyperaldosteronism
12 The myths of Primary Aldosteronism (PA)? PA is a rare cause of hypertension Serum potassium must be normal All the drugs must be stopped Making the diagnosis doesn t matter- just lower the blood pressure!
13 Hypokalaemia and Primary Aldosteronism Rossi et al. J Am Coll Cardiol 2006
14 The myths of Primary Aldosteronism (PA)? PA is a rare cause of hypertension Serum potassium must be normal All the drugs must be stopped Making the diagnosis doesn t matter- just lower the blood pressure!
15 Drug Effect on aldosterone Medications and ARR Effect on renin Β-blocker Centrally acting Effect on ARR NSAIDs K-wasting diuretics K-sparing diuretics ACEi/ARB Ca channel blockers (DHP)
16 The myths of Primary Aldosteronism (PA)? PA is a rare cause of hypertension Serum potassium must be normal All drugs must be stopped Making the diagnosis doesn t matter- just lower the blood pressure!


17 Lower the blood pressure (Gordon McInnes)
18 % Primary Aldosteronism Essential Hypertension Increased cardiovascular morbidity in Primary Aldosteronism Milliez et al, JACC 2005, 45, OR 1.6 (1-2.5) OR 2.9 ( ) 20 OR 4.2 (2-8.6) 15 OR 12.1 ( ) 10 OR 6.5 ( ) 5 0 CVA MI AF Echo LVH ECG LVH

19 Aldosterone and cardiovascular complications Savard et al Hypertension 2013
20 Diagnosis of PA J Clin Endocrinol Metab 2016
21 Diagnosis of PA: a guideline based approach
22 Diagnosis of PA: a guideline based approach Aldosterone 420 pmol/l PRC 1.2 µiu/ml ARR =350; > 35 merits investigation
23 Diagnosis of PA: a guideline based approach Aldosterone 420 pmol/l PRC 1.2 µiu/ml ARR =350; > 35 merits investigation Saline suppression test 2 litres saline/4 hours: Baseline: PRC 1.1/aldo hours: PRC<0.5/aldo 305

24 Diagnosis of PA: a guideline based approach Aldosterone 420 pmol/l PRC 1.2 µiu/ml ARR =350; > 35 merits investigation Saline suppression test 2 litres saline/4 hours: Baseline: PRC 1.1/aldo hours: PRC<0.5/aldo 305
25 Diagnosis of PA: a guideline based approach Aldosterone 395 pmol/l PRC 1.2 µiu/ml ARR =329; > 35 merits investigation Saline suppression test 2 litres saline/4 hours: Baseline: PRC 1.1/aldo hours: PRC<0.5/aldo 305
26 PA subtype classification- adenoma v hyperplasia CT has insufficient sensitivity and specificity Adrenal vein sampling (AVS) can confirm unilateral aldosterone excess 35 Recommended in all patients > 40 years or in younger patients with no visible adenoma on CT Only performed if surgery indicated
27 Adrenal Vein Sampling (AVS) Technical issues: right adrenal problematic 74% success for right adrenal (384 patients) 97% success rate in Mayo clinic (Rossi JCEM 2001) Lack of operator experience is main determinant of outcome
28 Alternatives to AVS Clinical prediction of aldosterone producing adrenal adenoma: Size ~ 1cm K < 3.5 mmol/l egfr> 100 (Kupers et al, JCEM 2012) 100% specificity 11 C-Metomidate PET CT
29 PA: outcome after surgery BP improves in almost all, serum [K] normalises in 100% Long-term cure rates of hypertension 30-60% Persistent hypertension more likely if: 2 or more anti-hypertensive agents Older age serum creatinine Longer duration of hypertension So, need to manage expectations Coexisting primary hypertension
30 Case 1 outcome: Left adrenalectomy 3 months later: BP 128/82 mm/hg on amlodipine only PRC now 14 µiu/ml Plasma aldosterone: 285 pmol/l
31 Case 2: To stent or not to stent? 28 year old female, referred to MAU with hypertension and headache OCP recently stopped due to BP (ABPM 164/108 mm/hg) PMH: pyelonephritis No FH O/E: Lean. BP 195/130 mm/hg, pulse 92. CV exam normal, femoral pulses palpable Fundoscopy: bilateral flame haemorrhages, no papilloedema Urinalysis: +++ protein; UE: egfr normal, [K] 3.2
32 Malignant (accelerated) hypertension Severe hypertension with bilateral retinal haemorrhages and exudates +/- papilloedema No absolute blood pressure level (usually > 180/120 mm/hg) to confirm or exclude diagnosis Always merits investigation for secondary cause Renal artery stenosis cause of up to 45% cases of malignant hypertension
33 Case 2: continued Plasma renin concentration: 211 µiu/ml (5-44.9) Plasma aldosterone: 507 pmol/l ( ) US renal tract: The right kidney measures 9.6 cm and the left kidney 10.7 cm in length. Both kidneys appear normal with no focal abnormality or hydronephrosis visualised. Next investigation??

34 Renal MR angiogram
35 Renal fibromuscular dysplasia (FMD) Non-inflammatory non-atherosclerotic disorder causing renal artery stenosis Unusual, <1% of cases of hypertension Can involve other arteries Mesenteric arteries most commonly Bilateral in 35-50%
36 Clinical features- renovascular hypertension Hypertension Activation of RAAS Clinical suspicion: Severe/resistant hypertension (esp >55y) Hypertension <35y Sudden rise in BP Significant increase in creatinine after ACEi/ARB without drop in BP Widespread atheroma or asymmetrical kidneys
37 Management of FMD Control blood pressure: ACEi usually ok (watch Cr); only contraindicated in severe bilateral disease But young woman of child-bearing age Stenting of renal artery Usually percutaneous Hypertension cure rates 20-80% Stabilises renal function


38 MR angiogram of case 2 Left renal artery stenosis confirmed BP improved with ACEi and thiazide diuretic Underwent PTA of renal artery May 2016 BP now 125/69 on no treatment
39 Renal artery stenting in atherosclerotic renovascular disease 3 large, randomised clinical trials since 2009 ASTRAL n=806; > 40% stenosis (NEJM : ) STAR n=140; >40% stenosis (Ann Int Med : ) CORAL n=947; >60% stenosis (NEJM 370:13-22) All show NO BENEFIT in renal artery stenting compared to medical therapy in atheromatous reno-vascular disease
40 Case 3: spells, sweating and flushing 39 year old man, ex-professional rugby player Presented with chest pain and hypertension Previous episodes During exercise: grey sweaty and clammy, headache, vomiting On arrival: BP 190/110, ST elevation, positive troponin, pulmonary oedema Treatment: IV metoprolol: BP rose to 230/150

41 Case 3: Coronary angiogram: normal coronary arteries CT abdomen:
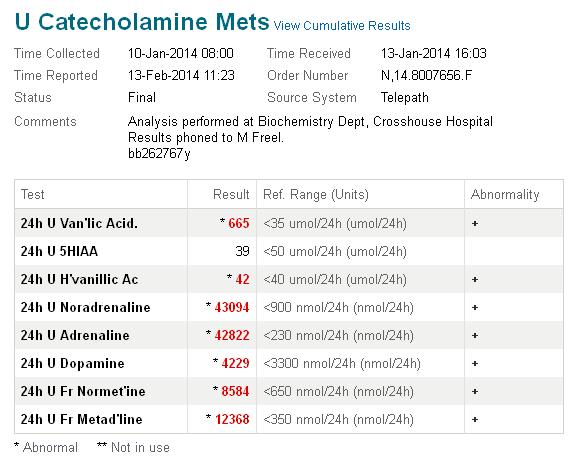
42 Case 3:
43 Phaeochromocytoma Accounts for <0.2% of patients with hypertension Indications for screening: Headache, sweating and tachycardia spells with palpitations, headache, pallor Genetic predisposition Adrenal adenoma
44 Phaeochromocytoma-screening 24h urine fractionated metanephrines 98% sensitivity/specificity Plasma metanephrines From cannula, supine, fasting Very sensitive, less specific (77-85%) Reserve for cases with high clinical suspicion
45 Phaeochromocytoma: false positive results Any acute illness, esp CV/MI/CCF/OSA Tricyclic anti-depressants Decongestant cold remedies Amphetamines/cocaine Buspirone and most psychoactive agents Prochlorperazine Ethanol
46 Imaging in phaeochromocytoma CT or MRI both very sensitive but 70% specificity due to incidentalomas Heterogeneous, vascular, cystic, dense adrenal lesions No concern about use of IV contrast if not alpha-blocked Diagnostic 123 I-MIBG if: Large phaeo (>10 cm) Paraganglioma
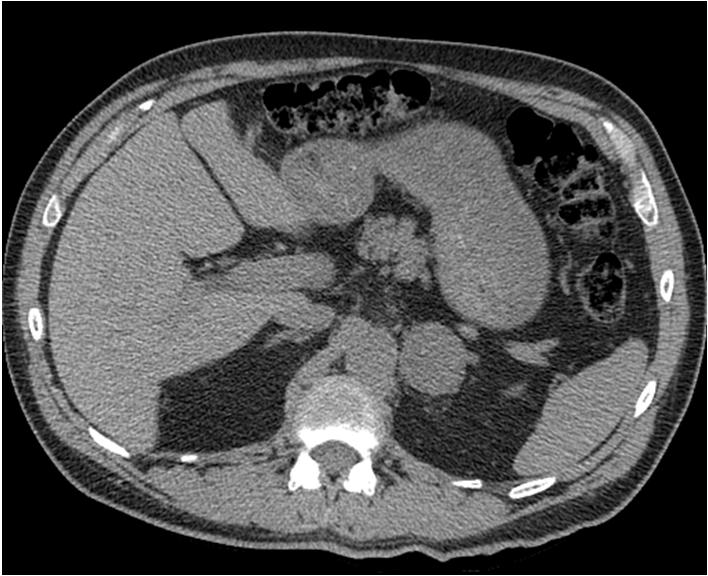


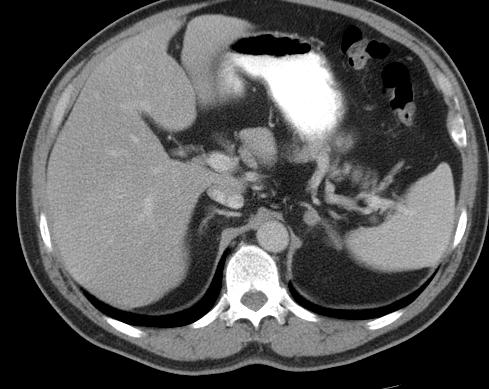
47 Phaeochromocytoma: imaging characteristics
48 Imaging in phaeochromocytoma CT or MRI both very sensitive but 70% specificity due to incidentalomas Heterogeneous, vascular, cystic, dense adrenal lesions No concern about use of IV contrast if not alpha-blocked Diagnostic 123 I-MIBG if: Large phaeo (>10 cm) Paraganglioma
49 Phaeochromocytoma-key points It is not common Beware of interfering medications Pallor and headache are good discriminating symptoms If symptoms present, diagnosis should be straightforward

50 Case 3 outcome Phenoxybenzamine 80 mg bd, labetolol 200 mg tds Laparoscopic adrenalectomy Currently normotensive, normal LV systolic function Genetic screen negative
51 Summary Majority of hypertension is primary Consider screening if: Young Malignant hypertension Resistant hypertension Newly uncontrolled hypertension Main screening tests: ARR (beware but don t be put off by drugs) 24h urinary metanephrines Renal ultrasound Renal doppler or MRA renal arteries
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
Hypertension: Who and How (and Why) to Investigate. Jessica Triay Andy Levy
 to Investigate. Jessica Triay Andy Levy") Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Karim Said. 41 year old farmer. Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy
 Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Renal Artery Disease. None > 65,000,000. Learning objectives: Renal Artery Disease
 Renal Artery Disease Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Financial Disclosure Information Renal Artery Disease Robert McBane, MD None To appreciate: Learning objectives:
Renal Artery Disease Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Financial Disclosure Information Renal Artery Disease Robert McBane, MD None To appreciate: Learning objectives:
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis
 Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Approach to Management of Hypertension. Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc
 Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Audience Response. Hypertension. Case: Mr. J. Measuring BP. Non-pharmacologic intervention. Case: Mr. J. Session ID: HTN411
 Audience Response http://rwpoll.com OR App downloads: Hypertension Chris Knight, MD cknight@uw.edu http://tiny.cc/rwiphone http://tiny.cc/rwdroid Session ID: HTN411 Case: Mr. J 52 y/o male patient comes
Audience Response http://rwpoll.com OR App downloads: Hypertension Chris Knight, MD cknight@uw.edu http://tiny.cc/rwiphone http://tiny.cc/rwdroid Session ID: HTN411 Case: Mr. J 52 y/o male patient comes
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
The real picture. Prorenin (Renin) PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009
 PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009") The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD
The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD
CV Risk in the Young. Dr. Susan Connolly Consultant Cardiologist Western Health and Social Care Trust
 CV Risk in the Young Dr. Susan Connolly Consultant Cardiologist Western Health and Social Care Trust Hypertension Clinics Cardiology Clinics CV Risk Clinic Lipid Clinics Vascular Clinics Endocrinology
CV Risk in the Young Dr. Susan Connolly Consultant Cardiologist Western Health and Social Care Trust Hypertension Clinics Cardiology Clinics CV Risk Clinic Lipid Clinics Vascular Clinics Endocrinology
Southern Derbyshire Shared Care Pathology Guidelines. Secondary Hypertension
 Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON
 When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON Conflict of interest None related to the topic When to look
When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON Conflict of interest None related to the topic When to look
HYPERTENSION CHAT with Colin and Ted AUG 2015
 HYPERTENSION CHAT with Colin and Ted AUG 2015 INTRODUCTION Hypertension has challenged famous physicians for centuries. 1733 - Clergyman Stephen Hales made the 1 st published measurement of blood pressure
HYPERTENSION CHAT with Colin and Ted AUG 2015 INTRODUCTION Hypertension has challenged famous physicians for centuries. 1733 - Clergyman Stephen Hales made the 1 st published measurement of blood pressure
Secondary hypertension is defined as being
 Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Renovascular hypertension in children and adolescents
 Renovascular hypertension in children and adolescents M I E C Z Y S L AW L I T W I N D E P T. O F N E P H R O LO G Y & A R T E R I A L H Y P E R T E N S I O N T H E C H I L D R E N S M E M O R I A L H
Renovascular hypertension in children and adolescents M I E C Z Y S L AW L I T W I N D E P T. O F N E P H R O LO G Y & A R T E R I A L H Y P E R T E N S I O N T H E C H I L D R E N S M E M O R I A L H
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Presentation of hypertensive emergency
 Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
RESISTANT HYPERTENSION
 RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Management of Hypertension and Consequences of non-compliance. Colin Edwards
 Management of Hypertension and Consequences of non-compliance Colin Edwards CARDIOLOGIST AHG May 2016 Outline 1. Consequences of poorly controlled hypertension 2. BP targets and anti-hypertensive drugs
Management of Hypertension and Consequences of non-compliance Colin Edwards CARDIOLOGIST AHG May 2016 Outline 1. Consequences of poorly controlled hypertension 2. BP targets and anti-hypertensive drugs
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
About 20% of the Canadian population
 Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Secondary hypertension How to approach?
 Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Genetic factors. A number of genetic factors or interactions between genes play a major role in essential hypertension.
 Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Renal artery stenosis
 Renal artery stenosis Dr. Alexander Woywodt Consultant Renal Physician, Royal Preston Hospital Preston, 31.10.2007 Menu anatomy of the renal arteries diseases of the large renal arteries atherosclerotic
Renal artery stenosis Dr. Alexander Woywodt Consultant Renal Physician, Royal Preston Hospital Preston, 31.10.2007 Menu anatomy of the renal arteries diseases of the large renal arteries atherosclerotic
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Pediatric Hypertension. Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019
 Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Duplex Ultrasound of the Renal Arteries. Duplex Ultrasound. In the Beginning
 Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Hypertension Cases. Katharine Dahl, MD January 10, 2017
 Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
NT-proBNP: Evidence-based application in primary care
 NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
Blood Pressure. Michelle Bertram- Nephrology- OBH
 Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.
 Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Diagnosis of Renal Artery Stenosis (RAS)
") May 2001 Diagnosis of Renal Artery Stenosis (RAS) Kurt Fink, Harvard Medical School, Year III Epidemiology Hypertension -Affects 60 million Americans Essential HTN >95% of cases Secondary HTN 1-5% of cases
May 2001 Diagnosis of Renal Artery Stenosis (RAS) Kurt Fink, Harvard Medical School, Year III Epidemiology Hypertension -Affects 60 million Americans Essential HTN >95% of cases Secondary HTN 1-5% of cases
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Systemic Hypertension
 BCS Theme Session Cardiovascular Block Pathology of Hypertension Department of Pathology University of Sydney Systemic Hypertension Definition of Systemic hypertension: consistent blood pressure elevation
BCS Theme Session Cardiovascular Block Pathology of Hypertension Department of Pathology University of Sydney Systemic Hypertension Definition of Systemic hypertension: consistent blood pressure elevation
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Mr Patrick Gladding. Specialist General Cardiology and Internal Medicine Auckland
 Mr Patrick Gladding Specialist General Cardiology and Internal Medicine Auckland 16:30-17:25 WS #60: Individualising Hypertension Treatment - Intensive or Not? 17:35-18:30 WS #72: Individualising Hypertension
Mr Patrick Gladding Specialist General Cardiology and Internal Medicine Auckland 16:30-17:25 WS #60: Individualising Hypertension Treatment - Intensive or Not? 17:35-18:30 WS #72: Individualising Hypertension
Renal Artery Stenting
 Renal Artery Stenting J.P. Reilly, MD, FSCAI Ochsner Medical Center Speaker s bureau: Astra Zeneca and Lilly/Diachi Sankyo Prevalence of RAS is high in cath population. Renal artery intervention can help
Renal Artery Stenting J.P. Reilly, MD, FSCAI Ochsner Medical Center Speaker s bureau: Astra Zeneca and Lilly/Diachi Sankyo Prevalence of RAS is high in cath population. Renal artery intervention can help
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
Amlodipine plus Lisinopril Tablets AMLOPRES-L
 Amlodipine plus Lisinopril Tablets AMLOPRES-L COMPOSITION AMLOPRES-L Each uncoated tablet contains: Amlodipine besylate equivalent to Amlodipine 5 mg and Lisinopril USP equivalent to Lisinopril (anhydrous)
Amlodipine plus Lisinopril Tablets AMLOPRES-L COMPOSITION AMLOPRES-L Each uncoated tablet contains: Amlodipine besylate equivalent to Amlodipine 5 mg and Lisinopril USP equivalent to Lisinopril (anhydrous)
Case yr old lady; type 2 Diabetes 10 yrs; PVD; hypertension
 Does this patient have flash pulmonary oedema? Philip A Kalra Professor of Nephrology, Salford Royal Hospital and University of Manchester, UK 73 yr old lady; type 2 Diabetes 1 yrs; PVD; hypertension Acute
Does this patient have flash pulmonary oedema? Philip A Kalra Professor of Nephrology, Salford Royal Hospital and University of Manchester, UK 73 yr old lady; type 2 Diabetes 1 yrs; PVD; hypertension Acute
Diagnosis and treatment of hypertension. Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington
 Diagnosis and treatment of hypertension Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington Outline Epidemiology Diagnosis Evaluation of individuals with
Diagnosis and treatment of hypertension Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington Outline Epidemiology Diagnosis Evaluation of individuals with
Renal Intervention. Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014
 Renal Intervention Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.: Advisory
Renal Intervention Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.: Advisory
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Read the following article and answer the questions that follow. Refer to the Keys section to check your answers.
 ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
Chronic Pediatric Hypertension
 Chronic Pediatric Hypertension Nephrology Grand Round 3/13/2015 Mahmoud Kallash M.D Outline Definition of hypertension (HTN) Challenges in diagnosing HTN Epidemiology Causes and evaluation of HTN Management
Chronic Pediatric Hypertension Nephrology Grand Round 3/13/2015 Mahmoud Kallash M.D Outline Definition of hypertension (HTN) Challenges in diagnosing HTN Epidemiology Causes and evaluation of HTN Management
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension