A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
|
|
|
- Lydia Quinn
- 5 years ago
- Views:
Transcription
1 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
2 Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory evaluation showed hypokalemia. Since then, he has been receiving potassium supplement, but his serum potassium has remained low or low normal. He did not experience further episode of weakness. He denied vomiting, diarrhea, palpitation, tremor or excessive sweating. He also denied use of over the counter medications or supplements. PMH: gall bladder polyp, colon polyp, hyperuricemia FH: Father: hypertension, DM, emphysema, angina pectoris, Grandfather: liver cancer Mother: subarachnoid hemorrhage
3 Case SH: occupation: high school teacher, smoking: 20 cigarettes/day (20 y.o. ~ 45 y.o.) alcohol: none Medications: Ursodeoxycol 100mg twice daily Vitamin B 2 Sustained release potassium chloride 2400mg twice daily Allopurinol 100mg once daily
4 Physical Examination Height 163 cm, BW 76 kg Well nourished, not in acute distress BP 136/86 mmhg, HR 66/min, regular Neck: no goiter Lung: clear to auscultation Heart; normal S1, S2 without murmur Abdomen: soft and flat, normal bowel sound, no bruit Extremity: no edema Skin: moist, no rash
5 Question What test is the first step in differential diagnoses of hypokalemia? 1. Plasma renin activity and plasma aldosterone concentration 2. Urine electrolytes 3. Arterial blood gas 4. Thyroid function tests
6 Answer Rule out pseudohypokalemia. Pseudohypokalemia Caused by potassium uptake by cells after venipuncture Usually seen in patients with many metabolically active blood cells, such as patients with acute myeloid leukemia Can be prevented by rapid separation of the plasma from the cells following venipuncture or storage of the blood at 4 before assay.
7 Answer You eventually need to perform all the tests but the first step is to check urine electrolytes to determine if hypokalemia is from renal or extrarenal potassium loss.
8 Laboratory Data ABG Chemistry ph Na 139 meq/l S-Osm 286 mosm/kg pco mmhg K 3.2 meq/l U-Osm 581 mosm/kg HCO mmol/l Cl 99 meq/l TSH 1.80 µu/ml CBC BUN 9 mg/dl Free T ng/dl WBC 8400 /µl Cre 0.88 mg/dl Free T3 3.1 pg/ml Hb 16.8 g/dl Glu 87 mg/dl PRA 6.6 ng/ml/hr Hct 48.7 % Ca 8.8 mg/dl PAC pg/ml Plt /µl P 2.7 mg/dl Mg 1.1 mg/dl U-Na 148 meq/l U-K 48 meq/l U-Cl 145 meq/l U-Cr 34.4 mg/dl
9 Laboratory Data 24 hour urine study Na: 137 meq/day K: 137 meq/day Cl: 199 mea/day Ca: 26 mg/day Cre: 1418 mg/day
10 Question What are the possible causes of his hypokalemia? 1. Primary aldosteronism 2. Hypokalemic periodic paralysis 3. Diarrhea 4. Renal tubular acidosis 5. Diuretic abuse 6. Vomiting 7. Bartter syndrome 8. Gitelman syndrome 9. Liddle syndrome
11 Differential Diagnosis of Hypokalemia Hypokalemia U K < meq/l U K <15-30 mmol/day U K :Ucr<13mEq/gCre or 1.5 meq/mmolcre U K > meq/l UK>15-30 mmol/day U K :Ucr>13mEq/gCre or 1.5 meq/mmolcre Intracellular shift Metabolic alkalosis Insulin Periodic paralysis Hyperadrenergic state Extra-renal potassium loss Diarrhea Burn Renal potassium loss
12 Differential Diagnosis of Hypokalemia Renal potassium loss U Cl <20 meq/l Metabolic alkalosis Vomiting Remote diuretic use Hypertension Next page U Cl >20 meq/l Variable ph Mg deficiency Low~normal BP Metabolic acidosis Renal tubular acidosis Bartter syndrome Gitelman syndrome Diuretics
13 Differential Diagnosis of Hypokalemia U K >20, metabolic alkalosis, U Cl >20, hypertension Low PRA High PAC Primary hyperaldosteronism High PRA Renovascular HTN Malignant HTN Renin-producing tumor Low-normal PAC Glucocorticoid Cushing syndrome Liddle syndrome
14 Answer Step1. His urine potassium was > 20 meq/l, 24 hour urine potassium 137mEq, urine K/Cre 139mEq/gCre renal potassium loss Step2. ABG showed metabolic alkalosis. renal tubular acidosis is unlikely Step3. His urine chloride was > 20 meq/l. vomiting is unlikely Step4. He is not hypertensive. Bartter syndrome, Gitelman syndrome, diuretic abuse are the consideration.
15 Question His PRA was 6.6 ng/ml/hr and PAC was pg/ml. What is the most likely cause of elevated PRA and PAC? 1. He also has primary aldosteronism. 2. He also has renal artery stenosis. 3. He also has renin producing tumor. 4. Secondary aldosteronism from intravascular volume depletion.
16 Answer 4. Secondary aldosteronism from intravascular volume depletion.
17 Plasma renin activity (PRA) and plasma aldosterone concentration(pac) Hypokalemia has to be corrected before measurements (hypokalemia suppress aldosterone). Many medications can affect the results. PAC PRA PAC/PRA ACE-I/ARB β- blockers Direct renin inhibitors Diuretics Aldosterone antagonists
18 Plasma renin activity (PRA) and plasma aldosterone concentration(pac) Mineralcorticoid antagonists (spironolactone, eplerenone) has to be stopped 4-6 weeks before the test ACE, ARB, diuretics, beta-blockers may be acceptable. (See next slide.)
19 Initial aldosterone/renin ratio on antihypertensives among patient with proven aldosterone-producing adenoma AJKD 2001; 37:
20 Sensitivity/Specificity Aldosterone/renin ratio of 40 (ng/dl/ng/ml/hr) gives the sensitivity of 100 % and specificity of 85 % (off diuretics, ACE-I/ARB, betablocker) Be careful of unit for aldosterone. 10pg/ml=1ng/dL J Hypertens 2006; 24:
21 Plasma renin activity (PRA) and plasma aldosterone concentration(pac) The values need to be interpreted in the clinical context.
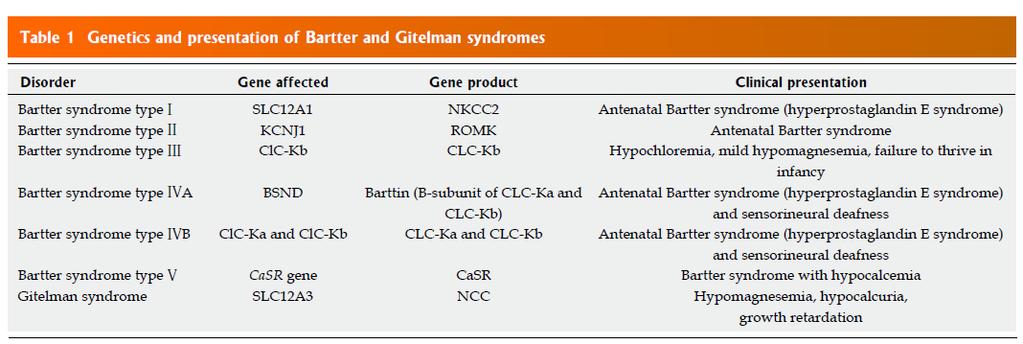
22 Case The patient denied any use of diuretics. He is a school teacher and does not seem to have access to diuretics. Bartter syndrome and Gitelman syndrome are considered. How can you differentiate these two syndromes?
23 Genetic defect in Bartter syndrome Genetic defect in Gitelman syndrome
24
25 Bartter and Gitelman syndrome Patients with Bartter syndrome would not respond to loop diuretics. Patients with Gitelman syndrome would not respond to thiazide diuretics.
26 Furosemide loading tests Furosemide 20mg iv Time Before 20 min 40min 60 min 80 min 100 min 120 min Urine volume (L) Urine Na (meq/l) Urine K (meq/l) Urine Cl (meq/l) Urine Cre (mg/dl)
27 Thiazide loading test Trichlormethiazide 8mg po Time Before 20 min 40 min 60 min 90 min 120 min150 min180 min Urine Volume (L) Urine Na (meq/l) Urine K (meq/l) Urine Cl (meq/l) Urine Cre (mg/dl)
28 Diagnosis Gitelman Syndrome
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Hypokalemia. Etiology of hypokalemia
 Hypokalemia The total body K+ storage: 50~55 meq/kg ( approximately 3000~4000 meq) 98% of the body K+ is located in the cells The net effect is that [K+c] is about 140 meq/l and [K+e] is only 4~5 meq/l
Hypokalemia The total body K+ storage: 50~55 meq/kg ( approximately 3000~4000 meq) 98% of the body K+ is located in the cells The net effect is that [K+c] is about 140 meq/l and [K+e] is only 4~5 meq/l
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Case conference. TAKUGA HINOSHITA 2 nd resident ONMC
 Case conference TAKUGA HINOSHITA 2 nd resident ONMC 38 y/o female, Japanese CC: Dyspnea, Muscle clump, Numbness HPI Since 1 week PTA, she s been complaining of fever around 38, chills, cold sweat and nocturnal
Case conference TAKUGA HINOSHITA 2 nd resident ONMC 38 y/o female, Japanese CC: Dyspnea, Muscle clump, Numbness HPI Since 1 week PTA, she s been complaining of fever around 38, chills, cold sweat and nocturnal
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
Acid/Base Disorders 2015
 Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
TUBULOPATHY Intensive Care Unit Sina Hospital
 TUBULOPATHY Intensive Care Unit Sina Hospital A 13 years old female who is known case of Scoliosis. She was operated 2 months ago for spinal curve repair. PMH:EMG-MCV In 2 years old =>No Motoneuron Disease
TUBULOPATHY Intensive Care Unit Sina Hospital A 13 years old female who is known case of Scoliosis. She was operated 2 months ago for spinal curve repair. PMH:EMG-MCV In 2 years old =>No Motoneuron Disease
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Clinical Approach to the Patient with Potential Acid- Base Disturbances
 Education Article Iran J Ped June 2007, Vol 17 (No 2), Pp:171-178 Clinical Approach to the Patient with Potential Acid- Base Disturbances Farahnak Assadi* 1, MD 1. Pediatric Nephrologist, Rush University
Education Article Iran J Ped June 2007, Vol 17 (No 2), Pp:171-178 Clinical Approach to the Patient with Potential Acid- Base Disturbances Farahnak Assadi* 1, MD 1. Pediatric Nephrologist, Rush University
CASE A 58-year-old woman, office worker CC : fatigue and weakness
 CASE A 58-year-old woman, office worker CC : fatigue and weakness HISTORY OF PRESENT ILLNESS About 7 days before admission, she lost her appetite and had a sensation of thirst. She had difficulties to
CASE A 58-year-old woman, office worker CC : fatigue and weakness HISTORY OF PRESENT ILLNESS About 7 days before admission, she lost her appetite and had a sensation of thirst. She had difficulties to
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
CASE REPORT. Abstract. Introduction. Case Report
 CASE REPORT A Novel Compound Heterozygous Mutation of Gitelman s Syndrome in Japan, as Diagnosed by an Extraordinary Response of the Fractional Excretion Rate of Chloride in the Trichlormethiazide Loading
CASE REPORT A Novel Compound Heterozygous Mutation of Gitelman s Syndrome in Japan, as Diagnosed by an Extraordinary Response of the Fractional Excretion Rate of Chloride in the Trichlormethiazide Loading
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment. Jamie Johnston, MD University of Pittsburgh School of Medicine
 Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Hypertension Cases. Katharine Dahl, MD January 10, 2017
 Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment
 Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/21/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/21/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Hypokalemic Hypertension Leading to a Diagnosis of Autosomal Dominant Polycystic Kidney Disease
 Case Report ISSN 1738-5997 (Print) ISSN 2092-9935 (Online) Electrolyte Blood Press 14:11-15, 2016 http://dx.doi.org/10.5049/ebp.2016.14.1.11 Hypokalemic Hypertension Leading to a Diagnosis of Autosomal
Case Report ISSN 1738-5997 (Print) ISSN 2092-9935 (Online) Electrolyte Blood Press 14:11-15, 2016 http://dx.doi.org/10.5049/ebp.2016.14.1.11 Hypokalemic Hypertension Leading to a Diagnosis of Autosomal
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
2018/6/7 APSN/JSN CME Course Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6
 2018/6/7 APSN/JSN CME Course 2018 Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6 Case1 77F Left leg pain Na 112 Case2 39M Seizure Na 117 Case3 73M General malaise Na 120 Case1
2018/6/7 APSN/JSN CME Course 2018 Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6 Case1 77F Left leg pain Na 112 Case2 39M Seizure Na 117 Case3 73M General malaise Na 120 Case1
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Hyperaldosteronism: Conn's Syndrome
 RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
About 20% of the Canadian population
 Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Acid-Base Imbalance-2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD
 Yanal A. Shafagoj MD. PhD") AcidBase Imbalance2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD Introduction Disturbance in acidbase balance are common clinical problem that range in severity from mild to life threatening, the acute
AcidBase Imbalance2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD Introduction Disturbance in acidbase balance are common clinical problem that range in severity from mild to life threatening, the acute
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
RISK FACTORS AND TREATMENT STRATEGIES FOR URINARY STONES Review of NASA s Evidence Reports on Human Health Risks
 Mayo Clinic O Brien Urology Research Center RISK FACTORS AND TREATMENT STRATEGIES FOR URINARY STONES 2017 Review of NASA s Evidence Reports on Human Health Risks John C Lieske, MD July 27, 2017 What types
Mayo Clinic O Brien Urology Research Center RISK FACTORS AND TREATMENT STRATEGIES FOR URINARY STONES 2017 Review of NASA s Evidence Reports on Human Health Risks John C Lieske, MD July 27, 2017 What types
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
Clinical Significance of Aldosterone Levels and Low Grade Inflammation in Patients with Coronary Vasospasm
 Clinical Significance of Aldosterone Levels and Low Grade Inflammation in Patients with Coronary Vasospasm Department of Cardiology Keiji Inoue Akira Ueoka, Naoki Maruyama, Yoshiaki Shimoda, Eigo Kishita,
Clinical Significance of Aldosterone Levels and Low Grade Inflammation in Patients with Coronary Vasospasm Department of Cardiology Keiji Inoue Akira Ueoka, Naoki Maruyama, Yoshiaki Shimoda, Eigo Kishita,
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN
 Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Mannitol-induced Metabolic Alkalosis
 Electrolyte & Blood Pressure :, 00 ) Mannitolinduced Metabolic Alkalosis Kyung Pyo Kang, M.D., Sik Lee, M.D., Kyung Hoon Lee, M.D., and Sung Kyew Kang, M.D. Department of Internal Medicine, Research Institute
Electrolyte & Blood Pressure :, 00 ) Mannitolinduced Metabolic Alkalosis Kyung Pyo Kang, M.D., Sik Lee, M.D., Kyung Hoon Lee, M.D., and Sung Kyew Kang, M.D. Department of Internal Medicine, Research Institute
Case Studies of Electrolyte Disorders ACOI Board Review Mark D. Baldwin D.O. FACOI
 Case Studies of Electrolyte Disorders ACOI Board Review 2018 Mark D. Baldwin D.O. FACOI Disclosures None, just working for The Man Question 1 The first thing in evaluating a patient who has a disorder
Case Studies of Electrolyte Disorders ACOI Board Review 2018 Mark D. Baldwin D.O. FACOI Disclosures None, just working for The Man Question 1 The first thing in evaluating a patient who has a disorder
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Tables of Normal Values (As of February 2005)
") Tables of Normal Values (As of February 2005) Note: Values and units of measurement listed in these Tables are derived from several resources. Substantial variation exists in the ranges quoted as normal
Tables of Normal Values (As of February 2005) Note: Values and units of measurement listed in these Tables are derived from several resources. Substantial variation exists in the ranges quoted as normal
Diuretics (Saluretics)
") Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
A 20-year-old woman with fatigue and palpitations
 IM BOARD REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will associate electrolyte abnormalities with the specific electrocardiographic abnormalities they can cause CYNTHIA H. HO, MD Department of Pediatrics
IM BOARD REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will associate electrolyte abnormalities with the specific electrocardiographic abnormalities they can cause CYNTHIA H. HO, MD Department of Pediatrics
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Two Little Water Cravers
 Two Little Water Cravers Baby Mo (5mths/M) Chief complaint Repeated vomiting since 2 months old with poor weight gain PMH Gestation 40+6wks, BW 3.375kg Hx of fracture Rt clavicle at birth HbH disease on
Two Little Water Cravers Baby Mo (5mths/M) Chief complaint Repeated vomiting since 2 months old with poor weight gain PMH Gestation 40+6wks, BW 3.375kg Hx of fracture Rt clavicle at birth HbH disease on
Severe electrolyte- and acid-base disorders. GIC oktober 2013
 Severe electrolyte- and acid-base disorders GIC oktober 2013 Case (1) 19-year-old male, 60 kg Fever persisting for 1 month Cough and chest congestion for 10 days Lethargy for 1 week Admitted with diagnosis
Severe electrolyte- and acid-base disorders GIC oktober 2013 Case (1) 19-year-old male, 60 kg Fever persisting for 1 month Cough and chest congestion for 10 days Lethargy for 1 week Admitted with diagnosis
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups. Lisa Ivy APRN
 Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
SMALL GROUP DISCUSSION
 MHD II, Seesion II Student Copy - Page 1 SMALL GROUP DISCUSSION MHD II Session II JANUARY 15, 2014 Recent Review highlighting disease process in Case 2: Fasano A, Catassi, C. NEJM 2012; 367: 2419-26 STUDENT
MHD II, Seesion II Student Copy - Page 1 SMALL GROUP DISCUSSION MHD II Session II JANUARY 15, 2014 Recent Review highlighting disease process in Case 2: Fasano A, Catassi, C. NEJM 2012; 367: 2419-26 STUDENT
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Kidneycentric. Follow this and additional works at:
 Washington University School of Medicine Digital Commons@Becker All Kidneycentric 2014 Gitelman syndrome David Steflik Washington University School of Medicine in St. Louis Follow this and additional works
Washington University School of Medicine Digital Commons@Becker All Kidneycentric 2014 Gitelman syndrome David Steflik Washington University School of Medicine in St. Louis Follow this and additional works
The most current assessment of this problem can be found in the Apex note dated
 Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Acid Base Disorders: Key Core Concepts. Thomas DuBose M.D., MACP, FASN ASN Board Review Course Online Resource Material 2014
 Acid Base Disorders: Key Core Concepts Thomas DuBose M.D., MACP, FASN ASN Board Review Course Online Resource Material 2014 Speaker Disclosure I, Thomas DuBose, M.D., have no financial relationships or
Acid Base Disorders: Key Core Concepts Thomas DuBose M.D., MACP, FASN ASN Board Review Course Online Resource Material 2014 Speaker Disclosure I, Thomas DuBose, M.D., have no financial relationships or
Dr. Suzana Voiculescu
 Dr. Suzana Voiculescu AB balance parameters Extracellular ph (plasmatic ph)= 7.35-7.45 < 7.35= acidosis >7.45= alkalosis Kassirer-Bleich equation [H+] = 24 PCO2/ [HCO3-] predicts that the ratio of dissolved
Dr. Suzana Voiculescu AB balance parameters Extracellular ph (plasmatic ph)= 7.35-7.45 < 7.35= acidosis >7.45= alkalosis Kassirer-Bleich equation [H+] = 24 PCO2/ [HCO3-] predicts that the ratio of dissolved
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
DIURETICS. Assoc. Prof. Bilgen Başgut
 DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Mechanical versus bioprosthetic valve. Intern: Supervisor: VS
 Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6
 Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
HYPERTENSION CHAT with Colin and Ted AUG 2015
 HYPERTENSION CHAT with Colin and Ted AUG 2015 INTRODUCTION Hypertension has challenged famous physicians for centuries. 1733 - Clergyman Stephen Hales made the 1 st published measurement of blood pressure
HYPERTENSION CHAT with Colin and Ted AUG 2015 INTRODUCTION Hypertension has challenged famous physicians for centuries. 1733 - Clergyman Stephen Hales made the 1 st published measurement of blood pressure
NORMAL POTASSIUM DISTRIBUTION AND BALANCE
 NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
Dr. Suzana Voiculescu Discipline of Physiology and Fundamental Neurosciences Carol Davila Univ. of Medicine and Pharmacy
 Dr. Suzana Voiculescu Discipline of Physiology and Fundamental Neurosciences Carol Davila Univ. of Medicine and Pharmacy AB balance parameters Extracellular ph (plasmatic ph)= 7.35-7.45 < 7.35= acidosis
Dr. Suzana Voiculescu Discipline of Physiology and Fundamental Neurosciences Carol Davila Univ. of Medicine and Pharmacy AB balance parameters Extracellular ph (plasmatic ph)= 7.35-7.45 < 7.35= acidosis
Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University
 Metabolic Acidosis Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com
Metabolic Acidosis Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com
Signs & Symptoms Suspected Acid-Base. Laboratory Variable. Disorder Serum Bicarbonate HCO 3. Central Nervous System. Respiratory Acidosis
 H+ Acid base Anion gap Acid base balance Proteins lose or gain H+ according to plasma (ICF) H+ Normally the plasma H+ is very low (40nanoEq/L ie 40 x 10 9 mol/l); this is roughly one millionth the meq/l
H+ Acid base Anion gap Acid base balance Proteins lose or gain H+ according to plasma (ICF) H+ Normally the plasma H+ is very low (40nanoEq/L ie 40 x 10 9 mol/l); this is roughly one millionth the meq/l
SAURIN GANDHI, AZCOM Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8)
") 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive