SOB. A Complaint With Many Faces
|
|
|
- Christian Benedict Dixon
- 6 years ago
- Views:
Transcription



1 SOB A Complaint With Many Faces Presented by : Dr. Chris Lee - PGY 2 ER Dr. Matthew Davis - Staff ER Physician, Interim Medical Director for Education
2 2 Shortness of Breath
3 Objectives Upon completion of this presentation, the paramedic should be able to: Describe comprehensive pre-hospital differential diagnoses of SOB, Distinguish between the common causes of SOB, and Apply pre-hospital SOB treatments to various patient care scenarios according to the Advanced Life Care Patient Care Standards. 3
4 Outline Outline common pitfalls when assessing SOB Develop a structured approach to SOB in the pre-hospital setting Review protocols available to treat SOB 4
5 Case 1 76 y/o F Hx of angina, COPD, MI with stent, DM Type 2 Has been getting progressively SOB since the holidays started Has trouble lying down, sleeps in a recliner, SOB always worse at night Still smokes 1/2 pack per day, puffers don t help T: 36.8, HR: 98, BP: 104/78, RR: 24, O2: 91% Auscultation: wheezes bilaterally *Wheezes = COPD* 5
6 Case 2 81 y/o M Hx of HTN, CAD, dyslipidemia, MI, stroke 6 months ago with speech/swallowing deficits Acutely SOB while eating dinner Has some pain with respirations, took nitro without any benefit T: 37.0, HR: 92, BP: 147/93, RR: 20, O2: 94% Auscultation: crackles at bases *Crackles = CHF* 6
7 Case 3 9 y/o M SOB for the past day or so Has been feeling generally unwell for a couple days, worst today, feels increasingly SOB Parents called because very fatigued, N/V, confused, complains of thirst Looks dehydrated, drowsy, hyperpneic T: 37.6, HR: 128, BP: 102/66, RR: 34, O2: 99% Auscultation: Normal breath sounds *Many causes of SOB* 7
8 Shortness of Breath Dyspnea Sensation of breathlessness and the patient s reaction to that sensation. 1 Imbalance of the perceived need to breathe, and the perceived ability to breathe. 2 8
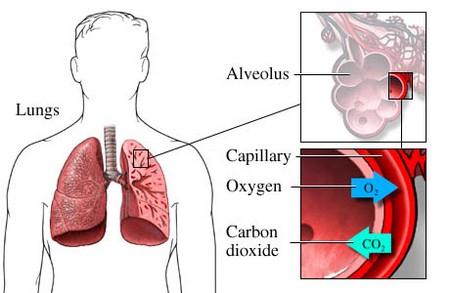
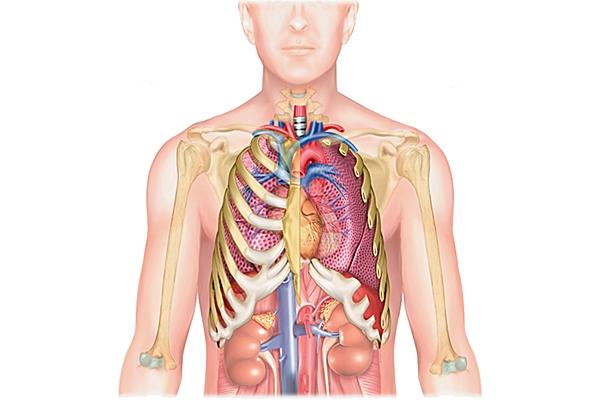
9 O2 in Carotid Bodies Thoracic Cage Protection, inhalation, stretch receptors Diaphragm Inhalation 9

10 10 Negative pressure
11 11
12 O2 in Carotid Bodies CO2 out Medulla Oblongata Trachea Conduit, vocal structures Lungs Gas exchange Thoracic Cage Protection, inhalation, stretch receptors Heart Pump Diaphragm Inhalation 12
13 Foreign body Supraglottitis Vocal Cord Paralysis Croup Trauma Anaphylaxis Trachea Rib Fractures Flail Chest Thoracic Cage Metabolic DKA Renal Failure Electrolyte abnormalities Metabolic Acidosis Thyroid disease Obesity Pregnancy Ascites Intraabdominal infection/sepsis Abdomen Pulmonary Embolus Pneumothorax Asthma Aspiration Pneumonia Pleural Effusion Neoplasm COPD Inhalation injury ARDS Pulmonary Contusion Heart Lungs Pulmonary Edema Myocardial Infarction Cardiac Tamponade Pericarditis Valvular Disease Cardiomyopathies Dysrhythmia Diaphragm Ruptured Diaphragm Hiatus Hernia Diaphragm paralysis Hematologic CO Poisoning Acute Chest Syndrome Anemia 13
14 Treatable (pre-hospital) causes of dyspnea Trachea Foreign Body Croup Anaphylaxis Heart Cardiogenic Pulmonary Edema Cardiac Ischemia/Myocardial Infarction Dysrhythmia Lungs Pneumothorax Asthma COPD 14
15 Trachea Foreign Body Croup Anaphylaxis Child: not watched, missing objects Adult: while eating, taking pills Stridor, audible wheeze, coughing, vomiting, possible decreased BS *Stridor* *High risk story* Children, late fall/winter, 6 mo - 6 yrs, Viral illness prodrome Seal-bark cough, hoarse voice, stridor *Stridor* *Seal-bark cough* History of allergy, GI, Skin complaints, Possible exposure Angioedema, Urticaria, N/V, Possible shock, Wheezing, Cough, stridor *High-risk story* *Cluster of symptoms* 15
16 Trachea Foreign Body Croup Anaphylaxis BLS maneuvers if awake If arrested, can attempt removal If severe respiratory distress: Nebulized epinephrine IM epinephrine IV/IM diphenhydramine If arrested after removal, run medical cardiac arrest 16
17 Lungs Pneumothorax Blunt or penetrating thoracic trauma Spontaneous in tall, young men, also COPD Tension: accumulating air, compression of mediastinum Usually acute onset Chest pain, decreased BS unilaterally *Tension* ++ acutely ill, cyanotic, hypotensive *Acute, high risk story* *decreased BS unilaterally* Asthma History of atopy, Puffer use, Worse at night, Triggers: allergens, exercise, stress Cough, WOB, Air entry Diaphoresis, Wheezing *High-risk story* *wheeze* COPD Long pre-morbid course, Smoking, SOBOE, Chronic cough Cough, WOB, Air entry Wheezing, crackles Auto-PEEP, unwell appearance *High-risk story* *wheeze* 17
18 Lungs Pneumothorax Asthma COPD If tension: Needle thoracostomy *NO* CPAP MDI/Nebulized Ventolin CPAP MDI/Nebulized Ventolin 18
19 Heart Pulmonary Edema (Cardiogenic) MANY causes: Infarction, cardiomyopathies, valvular dysfunction, dysrhythmia, volume overload, ) Hx of: Heart issues, orthopnea, PND, SOBOE Often worse at night Auscultation: Crackles, wheezes, extra heart sounds, if R-sided failure: JVP, leg edema *High-risk story* *Crackles bilaterally* Dysrhythmia Brady Tachy Hx of conduction problems SOB, syncope EKG changes (SSS, AV blocks, ) *EKG* Hx of similar episodes SOB, Palpitations EKG changes (A.Fib/Flutter, AVNRT, ) *EKG* Cardiac Ischemia Chest pain, associated SOB, worse with exertion History of angina, nitro CVS and Resp N, may have extra heart sounds EKG changes possible *High-risk story* *EKG* 19
20 Heart Pulmonary Edema (Cardiogenic) SL Nitroglycerin If in setting of STEMI and shock: IV Saline IV Dopamine Dysrhythmia Brady Tachy If unstable: Atropine BHP guidance: Transcut. Pacing Dopamine AVNRT/AVRT Valsalva Adenosine BHP guidance: Widecomplex Amiodaro ne Lidocaine Cardiovers ion Cardiac Ischemia PO ASA SL Nitroglycerin IV Morphine If in setting of STEMI and shock: IV Saline IV Dopamine 20
21 21 History, History, History
22 22
23 Start with history Start with protocols 23
24 Case 4 68 y/o M Hx of COPD, CABGx3, anxiety, HTN, DM2 Cough, SOB x 2 weeks, now spiking fever Greenish sputum, wife calls because now confused, GP 5 days ago put him on unknown antibiotic T: 38.6, HR: 117, BP: 96/74, RR: 25, O2: 89% Auscultation: crackles and air entry RLL, wheezes B/L *Multiple diagnoses can coexist* 24
25 25 Questions?
26 References 1. Marx JA, Hockberger RS, Walls RM, Adams JG, Barsan WG, Biros MH, et al., editors. Rosen s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia: Mosby Elsevier; Rawy A. Dyspnea [internet]. [Update Jul 2008, Cited Mar 2013] Available online from: 26
April 2011 CE. Site code # E The Patient With Heart Failure; CPAP as an Intervention
 April 2011 CE Site code # 107200E-1211 The Patient With Heart Failure; CPAP as an Intervention Prepared by: Lt. Bill Hoover, Medical Officer Wauconda Fire District Reviewed/revised by Sharon Hopkins, RN,
April 2011 CE Site code # 107200E-1211 The Patient With Heart Failure; CPAP as an Intervention Prepared by: Lt. Bill Hoover, Medical Officer Wauconda Fire District Reviewed/revised by Sharon Hopkins, RN,
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
STS: Circulatory/Pulmonary
 STS: Circulatory/Pulmonary September 27, 2017 You have a 50 y/o male who is complaining of excruciating pain in his chest. You find him sitting down on a bench, arms in a tripod position, breathing heavily.
STS: Circulatory/Pulmonary September 27, 2017 You have a 50 y/o male who is complaining of excruciating pain in his chest. You find him sitting down on a bench, arms in a tripod position, breathing heavily.
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Chest Pain 101: Fine Tuning Your Differential in the Outpatient Setting. Krysten Pilkington MNSc, APRN, AG-ACNP-BC
 Chest Pain 101: Fine Tuning Your Differential in the Outpatient Setting Krysten Pilkington MNSc, APRN, AG-ACNP-BC Where do we start? Onset Location Duration Characteristics Aggravating & Alleviating factors
Chest Pain 101: Fine Tuning Your Differential in the Outpatient Setting Krysten Pilkington MNSc, APRN, AG-ACNP-BC Where do we start? Onset Location Duration Characteristics Aggravating & Alleviating factors
Change in Practice PCP Autonomous IV OBHG Education Subcommittee
 Change in Practice PCP Autonomous IV Intravenous and Fluid Therapy Medical Directive Auxiliary Ability to initiate IV access and Ability to administer fluid and fluid boluses in general IV Therapy Actual
Change in Practice PCP Autonomous IV Intravenous and Fluid Therapy Medical Directive Auxiliary Ability to initiate IV access and Ability to administer fluid and fluid boluses in general IV Therapy Actual
Firefighter Pre-Hospital Care Program Recruit Presentation. Respiratory Emergencies
 Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
MEDICAL KIT - ALGORITHMS
 MEDICAL KIT - ALGORITHMS Page 2 : BRONCHOSPASM / ASTHMA Page 3 : TENSION PNEUMOTHORAX Page 4 : Page 5 : Page 6 : CONGESTIVE HEART FAILURE/ PULMONARY EDEMA ANAPHYLACTIC SHOCK / ALLERGIC REACTION ANGINA
MEDICAL KIT - ALGORITHMS Page 2 : BRONCHOSPASM / ASTHMA Page 3 : TENSION PNEUMOTHORAX Page 4 : Page 5 : Page 6 : CONGESTIVE HEART FAILURE/ PULMONARY EDEMA ANAPHYLACTIC SHOCK / ALLERGIC REACTION ANGINA
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Unit 4 Problems of Cardiac Output and Tissue Perfusion
 Unit 4 Problems of Cardiac Output and Tissue Perfusion Lemone and Burke Ch 30-32 Objectives Review the anatomy and physiology of the cardiovascular system. Identify normal heart sounds and relate them
Unit 4 Problems of Cardiac Output and Tissue Perfusion Lemone and Burke Ch 30-32 Objectives Review the anatomy and physiology of the cardiovascular system. Identify normal heart sounds and relate them
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Do I or Don t I??? Wade Woelfle, MD, FAAEM Assistant Professor Dept. of EM UW Emergency Care Conference 2015
 Do I or Don t I??? Wade Woelfle, MD, FAAEM Assistant Professor Dept. of EM UW Emergency Care Conference 2015 ASA 65 yo female CP for 45 minutes radiating to left arm Dyspneic, diaphoretic HR: 95, RR 20,
Do I or Don t I??? Wade Woelfle, MD, FAAEM Assistant Professor Dept. of EM UW Emergency Care Conference 2015 ASA 65 yo female CP for 45 minutes radiating to left arm Dyspneic, diaphoretic HR: 95, RR 20,
Cardiovascular and Respiratory Disorders
 Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular History Taking. Dr. Amitesh Aggarwal Assistant Professor Department of Medicine
 Cardiovascular History Taking Dr. Amitesh Aggarwal Assistant Professor Department of Medicine Overview Patient details Presenting Complaint History of Presenting Complaint Past Medical History Medications
Cardiovascular History Taking Dr. Amitesh Aggarwal Assistant Professor Department of Medicine Overview Patient details Presenting Complaint History of Presenting Complaint Past Medical History Medications
Interviewing and Health History
 Interviewing and Health History Core Curriculum for CV Clinicians Heart House 2016 Jane A. Linderbaum MS, ARNP, AACC Assistant Professor or Medicine, Mayo Clinic, Associate Medical Editor, AskMayoExpert
Interviewing and Health History Core Curriculum for CV Clinicians Heart House 2016 Jane A. Linderbaum MS, ARNP, AACC Assistant Professor or Medicine, Mayo Clinic, Associate Medical Editor, AskMayoExpert
Pathogenesis of pulmonary symptoms Dr. Rehab F. Gwada
 Pathogenesis of pulmonary symptoms Dr. Rehab F. Gwada Objectives of the lectures Identify main symptoms of pulmonary diseases & their pathogeneses Outline the graded of dyspnea Differentiate between bronchial
Pathogenesis of pulmonary symptoms Dr. Rehab F. Gwada Objectives of the lectures Identify main symptoms of pulmonary diseases & their pathogeneses Outline the graded of dyspnea Differentiate between bronchial
EMS Subspecialty Certification Review Course
 EMS Subspecialty Certification Review Course 1.3.1 1.3.1.1 Shortness of Breath 1.3.1.1.1 Use of portable non invasive ventilation devices 1.3.1.1.2 Field Identification of COPD 1.3.1.1.3 Assisted Ventilation
EMS Subspecialty Certification Review Course 1.3.1 1.3.1.1 Shortness of Breath 1.3.1.1.1 Use of portable non invasive ventilation devices 1.3.1.1.2 Field Identification of COPD 1.3.1.1.3 Assisted Ventilation
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
LeMone & Burke Ch 30-32
 LeMone & Burke Ch 30-32 2 Right side- Low oxygenation Low pressure Light workload Goes toward the lungs Left side High oxygenation Thick walled high pressure Heavier workload Carries oxygenation blood
LeMone & Burke Ch 30-32 2 Right side- Low oxygenation Low pressure Light workload Goes toward the lungs Left side High oxygenation Thick walled high pressure Heavier workload Carries oxygenation blood
NITROGLYCERIN A NEW LOOK FOR AN OLD FRIEND. Casey Patrick MD Jordan Anderson LP, CCP-C Texas EMS November 19, 2018
 NITROGLYCERIN A NEW LOOK FOR AN OLD FRIEND Casey Patrick MD Jordan Anderson LP, CCP-C Texas EMS November 19, 2018 OBJECTIVES Review pathophysiology of CHF Differentiate between acute pulmonary edema (APE),
NITROGLYCERIN A NEW LOOK FOR AN OLD FRIEND Casey Patrick MD Jordan Anderson LP, CCP-C Texas EMS November 19, 2018 OBJECTIVES Review pathophysiology of CHF Differentiate between acute pulmonary edema (APE),
Algorithm Focus. Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Perspective regarding the EMT- Intermediate algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
For more information about how to cite these materials visit
 Project: Ghana Emergency Medicine Collaborative Document Title: Approach to the Dyspenic Adult Patient Author(s): Randall Ellis, MD MPH (Vanderbilt University) License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: Approach to the Dyspenic Adult Patient Author(s): Randall Ellis, MD MPH (Vanderbilt University) License: Unless otherwise noted, this material
Evaluation of Chest Pain in the Primary Care Setting. Joseph Hackler, DO. Disclosures
 Evaluation of Chest Pain in the Primary Care Setting Joseph Hackler, DO Disclosures I have no relevant relationships with commercial interests to disclose. 1 Objectives 1. Discuss the different etiologies
Evaluation of Chest Pain in the Primary Care Setting Joseph Hackler, DO Disclosures I have no relevant relationships with commercial interests to disclose. 1 Objectives 1. Discuss the different etiologies
Anatomy. The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs.
 Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Conscious Sedation Permit Evaluation. General Comments Emergency Algorithms
 General Comments Emergency Algorithms These algorithms delineate appropriate responses to the simulated emergencies listed in Article 5, Section 1043.4c of the California Code of Regulations. Each algorithm
General Comments Emergency Algorithms These algorithms delineate appropriate responses to the simulated emergencies listed in Article 5, Section 1043.4c of the California Code of Regulations. Each algorithm
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Region VIII EMS Systems July 2016
 Region VIII EMS Systems July 2016 Introduction SME video of the month Review of Respiratory SOPs Three scenarios Announcements Region-None System- New SOP s In Effect July 1 st Dyspnea Common type of emergency
Region VIII EMS Systems July 2016 Introduction SME video of the month Review of Respiratory SOPs Three scenarios Announcements Region-None System- New SOP s In Effect July 1 st Dyspnea Common type of emergency
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Simulation and Clinical Learning Tillamook Healthcare Simulation Program Simulation Scenario CO2 Narcosis Code
 Simulation and Clinical Learning Tillamook Healthcare Simulation Program Simulation Scenario CO2 Narcosis Code Simulation Objective: Demonstrate behaviors necessary to respond in a cardiac arrest caused
Simulation and Clinical Learning Tillamook Healthcare Simulation Program Simulation Scenario CO2 Narcosis Code Simulation Objective: Demonstrate behaviors necessary to respond in a cardiac arrest caused
2
 1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
AIRWAY & HEART ANOTOMY
 Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Bronchoconstriction is also treated with medications that inhibit bronchiolar constriction such as: Ipratropium (Atrovent)
") Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
Chest Pain. Dr. Amitesh Aggarwal. Department of Medicine
 Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
MICHIGAN. State Protocols. General Treatment Protocols Table of Contents
 MICHIGAN State Protocols Protocol Number 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 1.10 1.11 1.12 1.13 General Treatment Protocols Table of Contents Protocol Name General Pre-hospital Care Abdominal Pain Nausea
MICHIGAN State Protocols Protocol Number 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 1.10 1.11 1.12 1.13 General Treatment Protocols Table of Contents Protocol Name General Pre-hospital Care Abdominal Pain Nausea
Cardiac Emergencies. A Review of Cardiac Compromise. Lawrence L. Lambert
 Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Contra-indications, Risks, and Safety Precautions for Stress Testing. ACSM guidelines, pg 20 7 ACSM RISK FACTORS. Risk Classifications pg 27
 Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
2/12/2011 Statistics Cardiovascular Emergencies time is myocardium! Cardiovascular disease (CVD) claimed over 1 million lives in CVD has been th
 claimed over 1 million lives in CVD has been th") Statistics Cardiovascular Emergencies time is myocardium! Cardiovascular disease (CVD) claimed over 1 million lives in 2004. CVD has been the leading cause of death for Americans since 1900. Sudden cardiac
Statistics Cardiovascular Emergencies time is myocardium! Cardiovascular disease (CVD) claimed over 1 million lives in 2004. CVD has been the leading cause of death for Americans since 1900. Sudden cardiac
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
MICHIGAN. Table of Contents. State Protocols. Adult Treatment Protocols
 MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
PALS PRETEST. PALS Pretest
 PALS PRETEST 1. A child with a fever, immune system compromise, poor perfusion and hypotension is most likely to be experiencing which type of shock A. cardiogenic B. Neurogenic C. Septic D. Hypovolemic
PALS PRETEST 1. A child with a fever, immune system compromise, poor perfusion and hypotension is most likely to be experiencing which type of shock A. cardiogenic B. Neurogenic C. Septic D. Hypovolemic
APNA 25th Annual Conference October 19, 2011
 Managing Acute and Chronic Illnesses: What Every Psych Nurse Needs to Know SARA BARR GILBERT, RN, CEN, MACP, SANE-A CHESHIRE MEDICAL CENTER, KEENE NH SGILBERT10@MSN.COM Chest Pain/MI MONA (Morphine, Oxygen,
Managing Acute and Chronic Illnesses: What Every Psych Nurse Needs to Know SARA BARR GILBERT, RN, CEN, MACP, SANE-A CHESHIRE MEDICAL CENTER, KEENE NH SGILBERT10@MSN.COM Chest Pain/MI MONA (Morphine, Oxygen,
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
2
 1 2 3 4 5 6 7 8 Please check regional policy on Tetracaine and Morgan Lens this may be optional in your region. *Ketamine and Fentanyl must be added to your controlled substance license if required by
1 2 3 4 5 6 7 8 Please check regional policy on Tetracaine and Morgan Lens this may be optional in your region. *Ketamine and Fentanyl must be added to your controlled substance license if required by
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Respiratory System Anatomy Respiratory system: all the structures that contribute to
 1 2 3 4 5 6 7 8 Chapter 15 Respiratory Emergencies Respiratory Distress Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine.
1 2 3 4 5 6 7 8 Chapter 15 Respiratory Emergencies Respiratory Distress Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine.
EMS Report Writing. Principles and Elements of Quality PCR Reports. David Ghilarducci MD FACEP
 EMS Report Writing Principles and Elements of Quality PCR Reports David Ghilarducci MD FACEP Outline For This Session Role of the EMS PCR The Narrative Section w SOAPP Format Why We Write Reports Patient
EMS Report Writing Principles and Elements of Quality PCR Reports David Ghilarducci MD FACEP Outline For This Session Role of the EMS PCR The Narrative Section w SOAPP Format Why We Write Reports Patient
August 2013 CE. Site code # E-1213
 August 2013 CE Site code # 107200E-1213 Caring for the Patient with CHF or COPD Objectives by Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422
August 2013 CE Site code # 107200E-1213 Caring for the Patient with CHF or COPD Objectives by Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422
In accordance with protocols, this patient should be transported to which medical facility?
 NOTE: Please select the most appropriate answer based on the Westchester Regional On-Line Medical Control Physician (OLMC) Regional System Overview, as well as current regional and state EMS protocols
NOTE: Please select the most appropriate answer based on the Westchester Regional On-Line Medical Control Physician (OLMC) Regional System Overview, as well as current regional and state EMS protocols
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
Respiratory Emergencies
 29698_CH11_Q_p001_012 4/12/05 2:03 PM Page 1 MEDICAL EMERGENCIES S E C T I O N 4 C H A P T E R Respiratory Emergencies 11 Workbook Activities The following activities have been designed to help you. Your
29698_CH11_Q_p001_012 4/12/05 2:03 PM Page 1 MEDICAL EMERGENCIES S E C T I O N 4 C H A P T E R Respiratory Emergencies 11 Workbook Activities The following activities have been designed to help you. Your
Congestive Heart Failure Patient Profile. Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption
 Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
This is my lecture about breathing
 This is my lecture about breathing CHRISTI BARTLETT, MD MAY 18, 2017 Objectives Review pulmonary HTN and discontinuation of PH meds at end of life. Review and understand different causes of dyspnea in
This is my lecture about breathing CHRISTI BARTLETT, MD MAY 18, 2017 Objectives Review pulmonary HTN and discontinuation of PH meds at end of life. Review and understand different causes of dyspnea in
Contra Costa County Emergency Medical Services Drug Reference. Indication Dosing Cautions Comments
 Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
DIASTOLOGY DON T BE SUCH A STIFF
 DIASTOLOGY DON T BE SUCH A STIFF Michael Mallin, MD University of Utah Director Emergency Ultrasound www.ultrasoundpodcast.com Warning: The education found within this presentation is not approved by anyone
DIASTOLOGY DON T BE SUCH A STIFF Michael Mallin, MD University of Utah Director Emergency Ultrasound www.ultrasoundpodcast.com Warning: The education found within this presentation is not approved by anyone
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Pediatric Assessment Triangle
 Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Cardiac Emergencies *** CME Version *** Aaron J. Katz, AEMT-P, CIC
 Cardiac Emergencies *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Mechanical structure Atria Ventricles One way valves Pulmonary arteries Pulmonary veins Aorta Coronary arteries Provide
Cardiac Emergencies *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Mechanical structure Atria Ventricles One way valves Pulmonary arteries Pulmonary veins Aorta Coronary arteries Provide
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
VACCINE-RELATED ALLERGIC REACTIONS
 VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis Public Health Immunization Program June 2018 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever,
VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis Public Health Immunization Program June 2018 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever,
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pneumothorax and Chest Tube Problems
 Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
Chapter 13. Respiratory Emergencies
 Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Assessment and Diagnosis of Heart Failure
 Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Critical Care Monitoring. Indications. Pleural Space. Chest Drainage. Chest Drainage. Potential space. Contains fluid lubricant
 Critical Care Monitoring Indications 1-2- 2 Pleural Space Potential space Contains fluid lubricant Can fill with air, blood, plasma, serum, lymph, pus 3 1 Pleural Space Problems when contain abnormal substances:
Critical Care Monitoring Indications 1-2- 2 Pleural Space Potential space Contains fluid lubricant Can fill with air, blood, plasma, serum, lymph, pus 3 1 Pleural Space Problems when contain abnormal substances:
Transfusion Reactions
 Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
For The Critters Present
 For The Critters Present Be sure to Sepsis Sepsis secondary to UTI Bacteremia SIRS secondary to infection For More Info-Contact Your Documentation Specialist Pat Spadaro, R.N. 6796 Rosanne Garofano, R.N.
For The Critters Present Be sure to Sepsis Sepsis secondary to UTI Bacteremia SIRS secondary to infection For More Info-Contact Your Documentation Specialist Pat Spadaro, R.N. 6796 Rosanne Garofano, R.N.
Chapter 39. Objectives. Objectives 01/09/2013. Geriatrics
 Chapter 39 Geriatrics Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 39 Geriatrics Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
EMS Subspecialty Certification Review Course. Learning Objectives. Upon the completion of this program participants will be able to:
 EMS Subspecialty Certification Review Course 1.3.1 1.3.1.1 Shortness of Breath 1.3.1.1.1 Use of portable non invasive ventilation devices 1.3.1.1.2 Field Identification of COPD 1.3.1.1.3 Assisted Ventilation
EMS Subspecialty Certification Review Course 1.3.1 1.3.1.1 Shortness of Breath 1.3.1.1.1 Use of portable non invasive ventilation devices 1.3.1.1.2 Field Identification of COPD 1.3.1.1.3 Assisted Ventilation
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Respiratory Distress/Failure - General
 Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
Respiratory Distress/Failure - General Criteria: Dyspnea WITHOUT a clear etiology O 2 V/S and SpO 2 (with and without Oxygen therapy if possible) Blood glucose analysis: if less than 80 mg/dl, refer to
1. What additional information needs to be collected to properly treat this client?
 CASE 1 A 45-year-old male presents to the emergency department with a complaint of chest pain for the past two hours. 1. What additional information needs to be collected to properly treat this client?
CASE 1 A 45-year-old male presents to the emergency department with a complaint of chest pain for the past two hours. 1. What additional information needs to be collected to properly treat this client?
SAUDI FELLOWSHIP TRAINING PROGRAM. Adult Cardiology. Final Written Examination 2019
 SAUDI FELLOWSHIP TRAINING PROGRAM Adult Cardiology Final Written Examination 2019 Objectives 1. Determine the trainee has sufficient competency related to the required specialty. 2. Determine the eligibility
SAUDI FELLOWSHIP TRAINING PROGRAM Adult Cardiology Final Written Examination 2019 Objectives 1. Determine the trainee has sufficient competency related to the required specialty. 2. Determine the eligibility
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Chapter 15 - Respiratory Emergencies
 1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 National EMS Education Standard Competencies (1 of 5) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory