Cerebral Revascularization Microsurgical Approach on Stroke Prevention. 16 May 2017 Yuen Shing Chau Neurosurgery Tuen Mun Hospital
|
|
|
- Giles Young
- 6 years ago
- Views:
Transcription
1 Cerebral Revascularization Microsurgical Approach on Stroke Prevention 16 May 2017 Yuen Shing Chau Neurosurgery Tuen Mun Hospital
2 Carotid Endarterectomy and EC-IC bypass CEREBRAL REVASCULARIZATION
3 Carotid Endarterectomy CAROTID STENOSIS
4 Landmark paper





5 SJ Peerless Professor and Chairman of the Division of Neurosurgery in the Department of Clinical Neurological Sciences GG Ferguson Chief of Neurosurgery at University Hospital, Professor of Neurosurgery and Medical Biophysics University of Western Ontario (University Hospital and St Joseph s Heath Center)

6 The term carotid derived from Greek word karos meaning deep sleep Carotid artery

7 Carotid stenosis Cerebral ischemia /infarction due to carotid stenosis: Embolism with platelet aggregates, thrombi or fragments from atheroma plagues at carotid bifurcation Flow reduction because of the arterial narrowing/occlusion
8 2 SYMPTOMATIC CASES




9 M/54 HT, DM Transient left side weakness and Left homonymous hemianopia MRI: Acute infarct over right watershed and occipital region Medical Rx Aspirin, plavix, insulin, zocor Recurrent symptoms within a week and readmitted


10 M/54 DSA revealed severe stenosis


11 LHCS M/54 CEA under GA Intra-operative monitor: EEG SSEP Uneventful surgery
12 The procedure CAROTID ENDARTERECTOMY
13 ECA ICA CCA

14 Clips application in sequence: ICA, CCA, ECA

15 Arteriotomy and endarterectomy

16
17

18 Backflow from ICA

19 Clips off sequence: ECA, CCA, ICA

20

 Density")
21 EEG monitoring in Carotid endarterectomy (G.A.) Raw EEG Compressed Spectral Array (CSA) Density Spectral Array (DSA)



22 Changes at clamping Clamps on Rt Clamps off Clamps on Lt Clamps off

23 SSEP summary No significant change throughout the procedure

24 CEA (G.A.) EEG signal changed after cross clamping Left Right

25 EEG signal changed after cross clamping, required shunting/ by-pass


26 Shunt if EEG/SSEP depressed in clamping Shunt placement
27 SECOND CASE


28 M/69 Chronic smoker Good past health Sudden onset left side weakness MRI: acute infarct over MCA territory Medical Rx Antiplatelet, antilipid Power improved over 4 weeks MBI: 67->88 ADLi


29 M/69 Tight stenosis at proximal ICA CEA under RA

30

31 TKS M/69 CEA under RA Uneventful surgery




32

33
34 Landmark paper
35 Benefit of CEA in symptomatic patients in North American Symptomatic Carotid Endarterectomy Trial % stenosis Nonsurgical Stroke risk Surgical Stroke risk Absolute risk reduction 50-69% 22.2% 15.7% 6.5% at 5 years % 26% 9% 17% at 2 years 8 NNT

36 Severe symptomatic carotid stenosis

37 Moderate symptomatic carotid stenosis
38 Risk of stroke in moderate vs severe stenosis
39 Surgical performance of the study Centers with 50 CEA cases performed in 24 months Surgeons with <6% peri-operative complication rate Performance of surgeons continuously evaluated by principal surgical investigators Majority done under GA Surgical time hours 40% shunt rate Median unshunted clamp time: 32min Majority of arteriotomy closed by simple closure
40 Recommedations from American Stroke Association Indication of Carotid endarterectomy in symptomatic stenosis: Severe carotid stenosis 70-99% Recent TIA or ischemic stroke within 6 months Perioperative mortality and morbidity <6% Moderate carotid stenosis 50-69% with favorable patient factors: age, gender, comorbidities, and severity of initial symptoms Operation ideally done within 2 weeks
41 Asymptomatic patients?


42 Asymptomatic carotid stenosis Advancement of current medical therapy reducing stroke risk in asymptomatic stenosis patients improved over years
43 Identification of high risk patients in asymptomatic stenosis Silent infarct on CT/MRI Cerebrovascular reserve Progressive stenosis on FU Contralateral carotid occlusion Microemboli on transcranial doppler Plaque related factors Severe stenosis Lipid rich Intra-plaque hemorrhage
44 Asymptomatic carotid stenosis Indications of CEA High risk patients with severe stenosis >70% Performed by centers with <3% morbidity and mortality
45 CEA in recent 8 years ( ) in Tuen Mun Neurosurgery Department 63 patients Age: M:F 55:8 GA: RA 24:39 (1 from RA to GA) Shunt bypass: 6 (9.5%) Peri-operative complications: 1 transient ischemia*(1.6% 30 day peri-operative risk) 2 wound haematoma 1 transient hoarseness 1 TIA (8 months after CEA) No recurrent stroke No re-stenosis (carotid doppler, CTA) 4 mortality unrelated to stroke ( 1 Ca rectum, 1 Ca lung, 1 HCC, 1 pneumonia) No myocardial infarct


46 Alternative intervention Carotid stenting Radiation induced stenosis Poor medical condition Restenosis after CEA Prior radical neck surgery Contralateral ICA occlusion ICA clip first

47 Stenosed irregular lumen
48 Natural history of carotid stenosis Asymptomatic <70% Symptomatic 70% Asymptomatic 70% Asymptomatic carotid stenosis with contralateral occlusion Progressive asymptomatic stenosis Risk of stroke 0.5%/ year 10% first 3 months, 5-6%/year 3-3.5%/year 5-6%/ year 4-5%/ year Trial Data-Intervention Risk of Stroke CREST, ICSS, NEJM, Neurology Angioplasty % Endarterectomy %
49 Guidelines for performance of Carotid Endarterectomy Appropriate patients Symptomatic 70-99% stenosis Uncertain patients ( careful patient selection + low perioperative risk center) Symptomatic 50-69% stenosis Asymptomatic 60-99% stenosis Inappropriate patients <50% symptomatic stenosis <60% asymptomatic stenosis Unstable medical or neurological status Recent large cerebral infarction Decreased level of consciousness Surgically inaccessible stenosis
50 Extracranial-Intracranial(EC-IC) bypass CEREBRAL REVASCULARIZATION
51 M/72 Chronic smoker Chronic drinker Right eye blind Sudden onset of left side weakness with partial recovery Limb side limb power Gr 4 ADL independent Carotid doppler revealed severe right cervical ICA occlusion/stenosis DSA: right cervical ICA occlusion

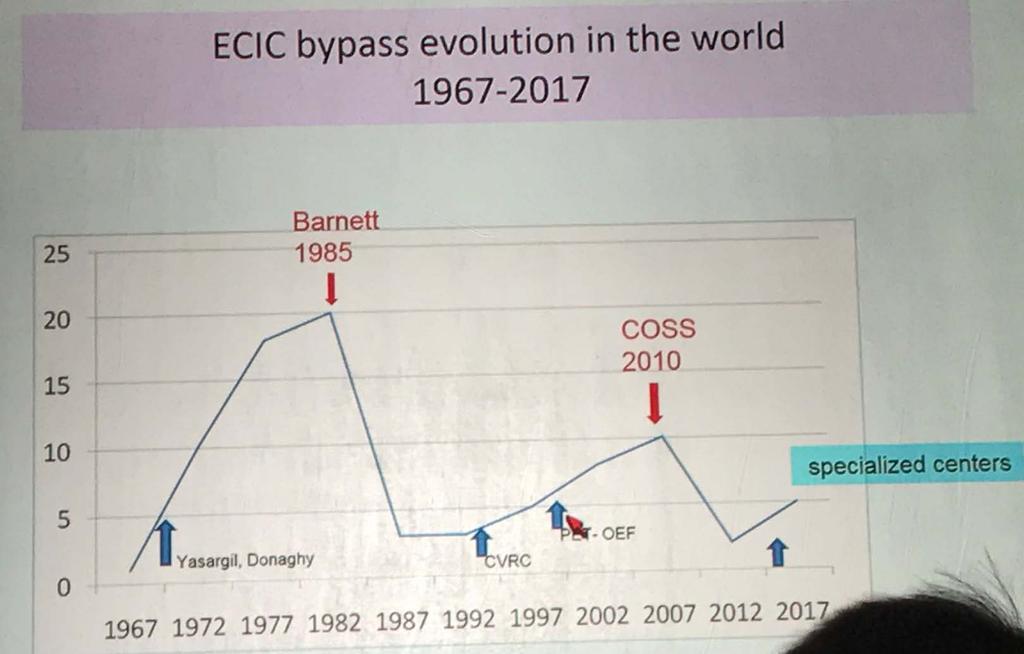
52 EC-IC bypass The STA MCA bypass is the procedure first successfully performed by M. G. Yasargil in the treatment of occlusive cerebrovascular disease in 1967 In late 1960s, EC-IC bypass widely performed in ischemic stroke

53 From: Extracranial-Intracranial Bypass Surgery for Stroke Prevention in Hemodynamic Cerebral Ischemia: The Carotid Occlusion Surgery Study Randomized Trial A and B, Anatomical relationships of the superficial temporal artery and middle cerebral artery. C, Intraoperative view showing completed anastomosis prior to closure of the dura, replacement of the bone flap, and closure of the soft tissues. The temporalis fascia, periosteum, subcutaneous fat, and dura are not depicted.
54 EC-IC bypass In mid 1980s, Barnett (EC-IC bypass Trial) questioned the true efficacy of the bypass procedure to decrease the risk of ischemic stroke A small subgroup of patients despite having optimal medical treatment still have ischemic symptoms referable to the vascular territory with underperfused and poor collateral supply More sophisticated investigations to select patient for revascularization

55

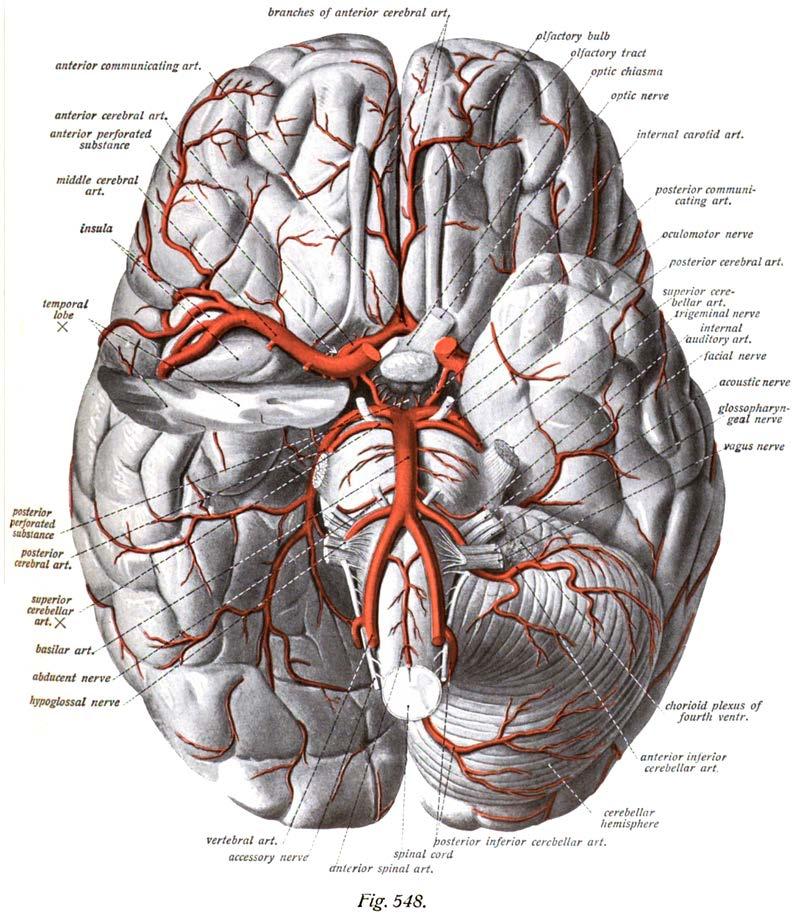
56 Circle of Willis
57 Collateral circulation Figure 1. Cerebral arterial circulation(a) Extracranial arterial collateral circulation. Shown are anastomoses from the facial (1), maxillary (2), and middle meningeal (3) arteries to the ophthalmic artery, and dural arteriolar anastomoses from the middle meningeal artery (4) and occipital artery through the mastoid foramen (5) and parietal foramen (6). Intracranial arterial collateral circulation in frontal (B) and lateral (C) views. Shown are the posterior communicating artery (1); leptomeningeal anastomoses between anterior and middle cerebral arteries (2) and between posterior and middle cerebral arteries (3); the tectal plexus between posterior cerebral and superior cerebellar arteries (4); anastomoses of distal cerebellar arteries (5); and the anterior communicating artery (6).
58 Assessment of collateral circulation Anatomical Imaging Cerebral Angiogram CT Angiogram MR Angiogram Physiologic imaging CT Perfusion MR Perfusion Positron Emission Tompography (PET)


59 CT perfusion Perfusion maps calculated by computer software after rapid bolus of iodinated contrast injection Mean transit time,mtt Time taken for blood to traverse a given brain region; sec Cerebral blood flow, CBF Volume of blood traversing a brain region per unit time; ml/100g/min Cerebral blood volume,cbv Total amount of blood flowing through a brain region at any one time: ml/100g
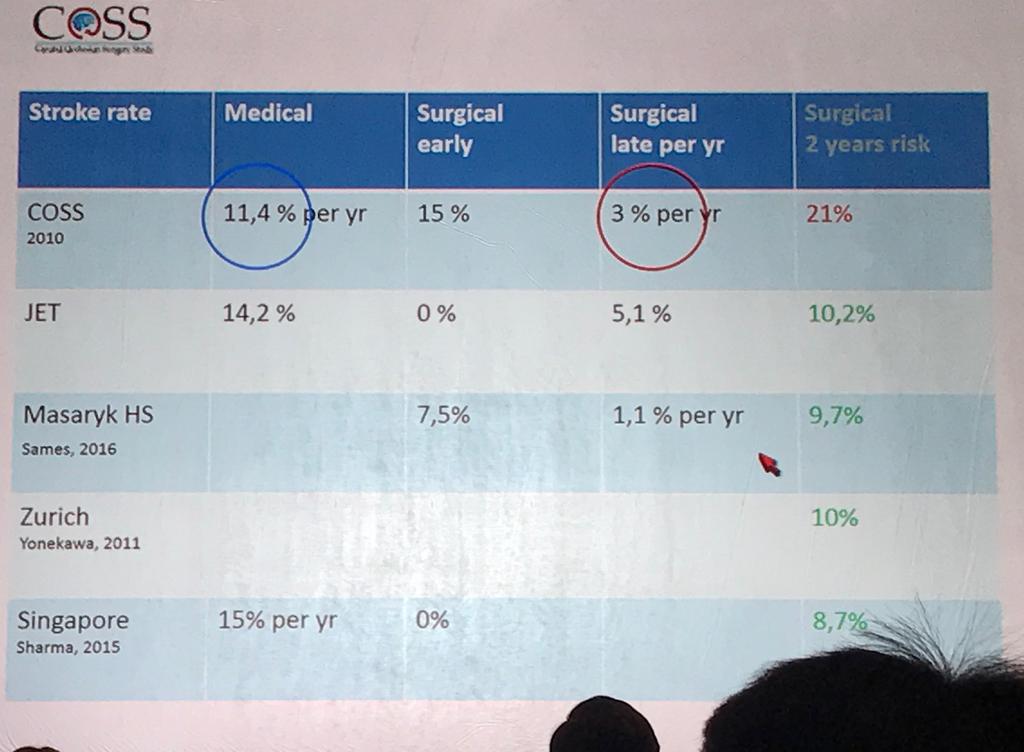
60 Cerebral vascular reserve Cerebral vasodilator Acetazolamine Pre-ECIC After acetazolamine Example: CTP revealed poor left cerebral perfusion and reserve Left STA-MCA bypass Sep2011 FU CTP showed marked improvement Post-ECIC After acetazolamine
61 CT perfusion interpretation CT perfusion parameters Normal Stenosis/occlu sion with good collateral Oligemic tissue that likely to survive Oligemic tissue at risk Tissue irreversibly damaged MTT Normal Prolonged Prolonged Prolonged Marked prolonged CBF Normal Normal Mild Reduction CBV Normal Normal Normal/Mild reduction Intervention Not indicated Acetazolamide challenge Marked reduction Moderate reduction Severely reduced Severely reduced Most useful Not useful
62 Anatomical localization Cervical ICA occlusion Intracranial arterial occlusion/stenosis Petrous or cavernous ICA occlusion Supraclinoid ICA stenosis or occlusion MCA stenosis or occlusion Moyamoya Disease Vertebrobasilar insufficiency
63 Cervical ICA occlusion >80% tolerate unilateral occlusion without suffering a significant ischemic event Small percentage become symptomatic during hypotension or high hemodynamic stress Older Symptoms due to watershed hypoperfusion Carotid Occlusion Surgery Study Trial
64 Carotid Occlusion Surgery Study
65 Carotid Occlusion Surgery Study ECIC bypass + Medical Rx vs Medical Rx only Patients with symptomatic atherosclerotic internal carotid artery occlusion (AICAO) and hemodynamic cerebral ischemia
66 Results The trial was terminated early for futility. Two-year rates for the primary end point were 21.0% (95% CI, 12.8% to 29.2%; 20 events) for the surgical group and 22.7% (95% CI, 13.9% to 31.6%; 20 events) for the nonsurgical group (P =.78, Z test), a difference of 1.7% (95% CI, 10.4% to 13.8%). Thirty-day rates for ipsilateral ischemic stroke were 14.4% (14/97) in the surgical group and 2.0% (2/98) in the nonsurgical group, a difference of 12.4% (95% CI, 4.9% to 19.9%).
67 From: Extracranial-Intracranial Bypass Surgery for Stroke Prevention in Hemodynamic Cerebral Ischemia: The Carotid Occlusion Surgery Study Randomized Trial The primary end point is defined in the footnote to Table 3. The number of participants who remained event free and available for follow-up evaluation at each 90-day interval is shown. EC-IC indicates extracranial-intracranial.
68 Comments on COSS High peri-operative morbidity 14.4% in COSS 0% in the Japanese EC-IC bypass Trial (JET) Outcome at 2 years are not significantly different, a continuation of the curves could result in a crossover benefiting surgery Mean time from symptoms to enrollment in COSS was about 72 days, the enrollees were more stable patients PET failed to identify the right candidates for bypass
69 From: Extracranial-Intracranial Bypass Surgery for Stroke Prevention in Hemodynamic Cerebral Ischemia: The Carotid Occlusion Surgery Study Randomized Trial Medical 11.4% Surgery 3% 5 years The primary end point is defined in the footnote to Table 3. The number of participants who remained event free and available for follow-up evaluation at each 90-day interval is shown. EC-IC indicates extracranial-intracranial.
70
71
72 EC-IC bypass in TMH ( ) 37 procedures (3 patients with bilateral procedures) Age: M:F 24:10 Pre-operative Ix: All symptomatic with DSA+CTP Pathology: Atherosclerosis: 31 (6 with RT) Moya Moya Disease: 6 Anatomic locations: Extracranial ICA 22 Intracranial arterial stenosis 13 Posterior circulation 2
73 EC-IC bypass in TMH ( ) 30 days peri-operative complications: 2 (5.4%) cerebrovascular events: 1 (2.7%) new cerebral infarct, 1 IVH at D26 4 epilepsy 2 subdural hematoma (treated conservatively) 1 pseudomeningocele ( LP) Cerebrovascular events beyond 30 days: 4 more cases: 3 TIA, 1 IVH(MMD) 4 mortality unrelated to stroke( 1 Ca lung, 1 HCC, 2 pneumonia) Bypass patency confirmed in 27 cases CT perfusion improved in 20 cases
74 Results Rough comparison with COSS TMH ECIC ECIC (- MMD) 4.8% (1 event) 6.67%(1/15) 2.7% (1/37) 3.2%(1/31) Cannot directly compare the 2 year stroke rate: 13 patients not reached 2 years FU, only 21 patients included
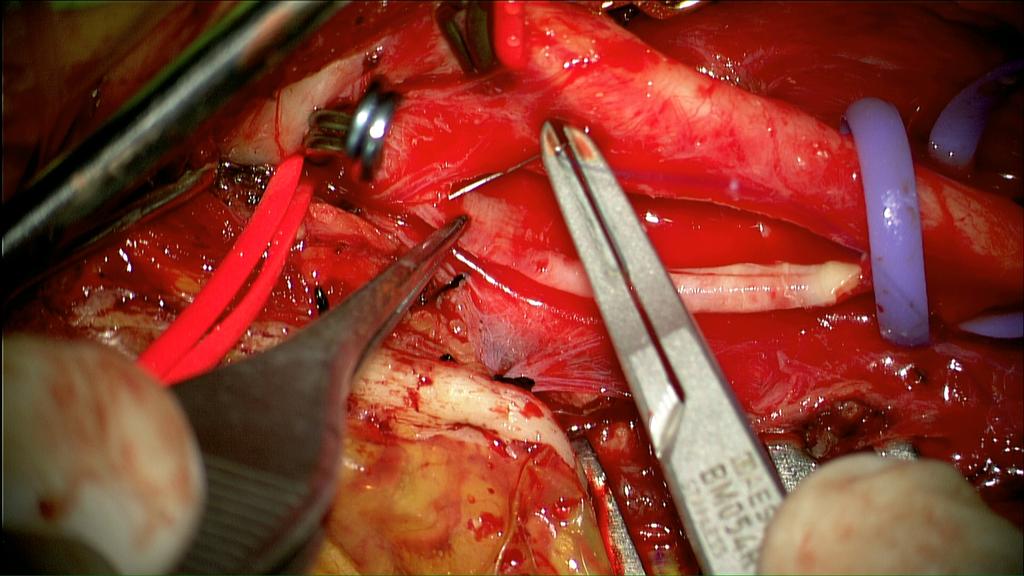
75 The Procedure STA-MCA BYPASS
 bypass 1.")

76 Superficial temporal artery middle cerebral artery (STA-MCA) bypass 1. Isolate STA 2. Craniotomy and identify the MCA branch 3. Anastomosis

77 MCA segment temporary clipped

78 Arteriotomy on MCA

79 MCA lumen irrigated

80 End to side anastomosis


81 Patency checked after anastomosis ICG angiography Anastomosis completed


82 Cervical ICA Occlusion M/72 Chronic smoker Chronic drinker Right eye blind Sudden onset of left side weakness with partial recovery Limb side limb power Gr 4 ADL independent Carotid doppler revealed severe right cervical ICA occlusion/stenosis DSA: right cervical ICA occlusion

83 M/72 Pre-ECIC CTP: impaired right cerebral perfusion and reserve Right STA-MCA bypass Dec2011 Postop CTP revealed improved perfusion and reserve No ischemic event, ADLi, Walks unaided Post-ECIC
84 Anatomical localization Cervical ICA occlusion Intracranial arterial occlusion/stenosis Petrous or cavernous ICA occlusion Supraclinoid ICA stenosis or occlusion MCA stenosis or occlusion Moyamoya Disease Vertebrobasilar insufficiency
85 Supraclinoid ICA stenosis or occlusion Younger Pathology often dissection rather than atherosclerotic Bypass is extremely effective especially occlusion is above the Pcom origin


86 Distal ICA Occlusion M/55 Chronic smoker Sudden onset right side weakness and aphasia with partial recovery Residual limb weakness and expressive dysphasia Right limb power Gr4 Walks unaided with hemiparetic gait DSA revealed occlusion of terminal ICA
87 Supraclinoid ICA occlusion

88 M/55 CTP revealed poor left cerebral perfusion and reserve Pre-ECIC Left STA-MCA bypass Sep2011 FU CTP showed marked improvement Post-ECIC



89 Pre-ECIC M/55 Postop DSA: STA hypertrophy Post-ECIC
90 Anatomical localization Cervical ICA occlusion Intracranial arterial occlusion/stenosis Petrous or cavernous ICA occlusion Supraclinoid ICA stenosis or occlusion MCA stenosis or occlusion Moyamoya Disease Vertebrobasilar insufficiency
91 MCA stenosis or occlusion Dangerous Collateral only from leptomenigeal vesels from ACA and PCA Older patient; MCA occlusion or stenosis either cause severe injury or adequate collateral Young patients due to acute or subacute dissection with fluctuating ischemic symptoms; good candidate for bypass


92 Bilateral MCA stenosis F/50 Construction site worker EX-smoker Hx of transient right side weakness and slurring speech 4 years ago Transient left side weakness Expressive dysphasia Limb power normal MRI, MRA revealed left parietal old infarct ; Right MCA stenosis and left MCA occlusion
93 MCA occlusion




94 F/50 DSA confirmed the MRA findings; early Moyamoya phenomenon
95 Pre-ECIC F/50 CTP revealed decreased perfusion in bilateral MCA territories and inadequate reserve Left STA-MCA bypass Mar2011 Postop CTP: improvement in left MCA and impaired right MCA perfusion and reserve Post- left ECIC





96 F/50 Postop DSA: Patent left STA-MCA bypass; Right MCA occlusion and moyamoya phenomenon Pre-ECIC Post-ECIC

97 F/50 Pre-ECIC CTP revealed decreased perfusion in bilateral MCA territories and inadequate reserve Bilateral EC-IC performed Postop CTA: patent bilateral bypass Post-ECIC
98 Moyamoya disease Classically affecting young children and young adults All ages and all ethnic group Direct/indirect bypass

99 Moya Moya Disease F/22 Sudden onset of headache and collapse in England Found to have ventricular hemorrhage and hydrocephalus Resuscitated with ventricular drainage and managed in London Transferred back to HK after 2 months Good neurological recovery with full GCS Right side limb weakness

100 F/22 Pre-ECIC CTP CTP and DSA showed Moya Moya Disease and impaired perfusion Bilateral STA-MCA bypass Good recovery in limb power Back to full time job 4 months later Post-ECIC CTP

101 Right hemisphere post-ecic Right ECA Right ICA

102 F/22 Bilateral STA-MCA bypass Good recovery in limb power Back to full time job 4 months later

103 Left hemisphere post-ecic Left ECA Left ICA
104 Anatomical localization Cervical ICA occlusion Intracranial arterial occlusion/stenosis Petrous or cavernous ICA occlusion Supraclinoid ICA stenosis or occlusion MCA stenosis or occlusion Moyamoya Disease Vertebrobasilar insufficiency
105 Vertebrobasilar disease Old patients with severe atherosclerotic disease Cervical vertebral artery with angioplasty and stenting Bypass: OA-PICA,STA-SCA, STA-PCA bypass
106 Vertebral artery occlusion



107 Bilateral VA Occlusion M/59 Ex-smoker, ex-drinker NPC RT 2001 Old TB Recurrent generalized weakness and dizziness for months Bilateral deafness Impaired gag reflex Impaired tandem gait Limb power normal MRI/MRA: pontine infarct, left vertebral artery occlusion, right VA and basilar artery stenosis




108 M/59 DSA : Complete occlusion of both VA, right PICA supplied by muscular branches at C1 level Posterior circulation supplied by anterior circulation through Pcom What next?


109 M/59 Left occipital artery PICA bypass Oct2011 CTA: patent bypass Dizziness improved
110 Conclusion Neurosurgery plays a significant role in management of ischemic stroke New imaging techniques useful in selecting suitable candidates for surgery Microsurgical procedures, endarterectomy and EC-IC bypass, are feasible and safe for preventing major strokes

111 Thank you TUEN MUN HOSPITAL
112 Ischemic Stroke M/47 History of infective endocarditis Sudden left hemiplegia Deteriorating conscious level: GCS15->13



113 Ischemic Stroke M/47 History of infective endocarditis Sudden left hemiplegia Deteriorating conscious level: GCS15->13 Decompressive craniectomy and duroplasty

114

115


116 Right CEA Baseline, left > right perfusion Bipolar EEG - EEG F4-C4 : 93% : 7b/m : 1:11 Raw EEG C4-C4 : 90% : 8b/m : 1:9 F8-T6 : 96% : 3b/m : 1:19 F3-C3 : 57% : 16b/m : 13: C3-C3 : 68% : 15b/m : 19:41 F7-T5 : 90% : 8b/m : 1: Rt Rt Rt Lt Lt Compressed spectral array Density spectral array
117 SSEP baseline Lt stim 20mA, Rt stim 30mA Lt SEP - Average N20 N20 C4 -Fpz - (Avg) (BL) C4 -Fpz - (3) Rt SEP - Average N20 N20 (BL) C3 -Fpz - (1) C3 -Fpz - (Avg) P24 P24 P24 P24 N9 N9 Lt Erb-Rt Erb - (Avg) (BL) Lt Erb-Rt Erb - (3) N9 N9 a a a a Rt Erb-Lt Erb - (Avg) (BL) Rt Erb-Lt Erb - (1) 1 5 5


118 The procedure: Carotid endarterectomy




119 M/61 Chronic smoker Repeated LOC No limb weakness PE: Left carotid bruit Carotid doppler revealed bilateral carotid stenosis DSA revealed bilateral carotid stenosis, more on the left side Right ICA Left ICA



120 M/61 Left carotid endarterectomy Nov2011 Postop CTA significant R ICA stenosis No symptom after left CEA What next? LR R
121 M/61 CTP revealed impaired cerebrovascular perfusion and reserve over right side watershed region Right CEA Aug 2012 Remain asymptomatic


122 F/81 DM, HT Recurrent left TIA Admitted for right side weakness and slurring speech in 2009 DSA: bilateral proximal carotid severe stenosis(>90%) AP Lat


123 F/81 Left CEA performed under RA Intra-operative finding: strong adhesion of plaque to ECA orifice preventing atheroma removal at ECA Noticed to have decreased conscious level and increased right side weakness shortly after operation Urgent DSA: ECA occlusion, patent ICA




124 F/81 Urgent DSA: left middle cerebral artery thrombo-embolism Urgent intra-arterial thrombolysis performed with successful recanalization Power and conscious level returned to pre-morbid state Pre-IA Post-IA No recurrent TIA/ stroke on FU(2014) Pre-IA Post-IA
125 Factors Influencing Risk & Benefit of CEA Factors favoring CEA Hemispheric TIA Male Recent symptoms(<30 days) Comorbidities well controlled Severe stenosis(>80%) Ulceration or intraluminal thrombus Silent ipsilateral infarct Contralateral stenosis/occlusion Intracranial (tandem) atherosclerosis Factors favoring medical treatment Amaurosis fugax Female Remote symptoms Comorbidities uncontrolled Advanced age Asymptomatic
126 Carotid endarterectomy by neurosurgeon NASCET cases primarily performed by neurosurgeons Dedicated team in awake surgery (Awake craniotomy) Routine electro-physiological monitoring in GA cases Procedure performed under microscope Intensive post-operative neurological monitoring and management Close cooperation with neuro-radiological interventional team Cerebrovascular perfusion study in equivocal cases
127 M/72 Chronic smoker Chronic drinker Right eye blind Sudden onset of left side weakness with partial recovery Limb side limb power Gr 4 ADL independent Carotid doppler revealed severe right cervical ICA occlusion/stenosis DSA: right cervical ICA occlusion

128 Cervical ICA occlusion

129 CREST No significant difference between CEA vs Stenting Periprocedural stroke Myocardial infarction Death Ipsilateral stroke Postprocedural stroke

130

131
132 Periprocedure stroke -more in stenting Myocardial infarction -more in endarterectomy
133 Carotid Occlusion Surgery Study Patients with symptomatic atherosclerotic internal carotid artery occlusion (AICAO) and hemodynamic cerebral ischemia are at high risk for subsequent stroke when treated medically. Objective To test the hypothesis that extracranialintracranial (EC-IC) bypass surgery, added to best medical therapy, reduces subsequent ipsilateral ischemic stroke in patients with recently symptomatic AICAO and hemodynamic cerebral ischemia
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
History of revascularization
 History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
TABLES. Table 1 Terminal vessel aneurysms. Table. Aneurysm location. Bypass flow** Symptoms Strategy Bypass recipient. Age/ Sex.
 Table TABLES Table 1 Terminal vessel aneurysms Age/ Sex Aneurysm location Symptoms Strategy Bypass recipient Recipient territory Recipient territory flow* Cut flow Bypass flow** Graft Patent postop F/U
Table TABLES Table 1 Terminal vessel aneurysms Age/ Sex Aneurysm location Symptoms Strategy Bypass recipient Recipient territory Recipient territory flow* Cut flow Bypass flow** Graft Patent postop F/U
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid artery stenting for long CTO and pseudo occlusion of carotid artery -2 case reports-
 Carotid artery stenting for long CTO and pseudo occlusion of carotid artery -2 case reports- Katsutoshi Takayama, MD, Ph.D Department of Radiology and Interventional Neuroradiology Ishinkai Yao General
Carotid artery stenting for long CTO and pseudo occlusion of carotid artery -2 case reports- Katsutoshi Takayama, MD, Ph.D Department of Radiology and Interventional Neuroradiology Ishinkai Yao General
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature
 Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA
 Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al.
 ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al. visualization of the posterior inferior cerebellar artery. The patient, now 11 months post-operative, has shown further neurological improvement since
ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al. visualization of the posterior inferior cerebellar artery. The patient, now 11 months post-operative, has shown further neurological improvement since
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke
 Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke Tetsuyoshi Horiuchi, Junpei Nitta, Shigetoshi Ishizaka, Kohei Kanaya, Takao Yanagawa, and Kazuhiro Hongo. Department of Neurosurgery,
Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke Tetsuyoshi Horiuchi, Junpei Nitta, Shigetoshi Ishizaka, Kohei Kanaya, Takao Yanagawa, and Kazuhiro Hongo. Department of Neurosurgery,
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION
 TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie?
 XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Double STA-MCA Anatomosis for Bilateral Carotid Occlusion
 Double STA-MCA Anatomosis for Bilateral Carotid Occlusion -Case Report and Literature Review- Sandra vuignier 1, Kenji Kanamaru 2, Tomohiro Araki 2 1 Department of Neurosurgery, Nagoya University School
Double STA-MCA Anatomosis for Bilateral Carotid Occlusion -Case Report and Literature Review- Sandra vuignier 1, Kenji Kanamaru 2, Tomohiro Araki 2 1 Department of Neurosurgery, Nagoya University School
Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side
 Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side Academician Mitrev Z, Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 History Hippocrates, 400 B.C.
Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side Academician Mitrev Z, Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 History Hippocrates, 400 B.C.
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Cerebral revascularization: past, present and future
 Cerebral revascularization: past, present and future Tomás Funes 1 MD, Asis Lorente Muñoz 2 MD, Federico Fernández Molina 3 MD, Paula Ypa 3 MD, Francisco Mannara 4 MD, Luis González Martínez 2 MD, PhD
Cerebral revascularization: past, present and future Tomás Funes 1 MD, Asis Lorente Muñoz 2 MD, Federico Fernández Molina 3 MD, Paula Ypa 3 MD, Francisco Mannara 4 MD, Luis González Martínez 2 MD, PhD
Case Report INTRODUCTION
 Journal of Cerebrovascular and Endovascular Neurosurgery pissn 2234-8565, eissn 2287-3139, https//doi.org/10.7461/jcen.2018.20.2.127 Case Report Revision Superficial Temporal Artery-Middle Cerebral Artery
Journal of Cerebrovascular and Endovascular Neurosurgery pissn 2234-8565, eissn 2287-3139, https//doi.org/10.7461/jcen.2018.20.2.127 Case Report Revision Superficial Temporal Artery-Middle Cerebral Artery
Assessment Of Collateral Pathways In Acute Ischemic Cerebrovascular Stroke Using A Mansour Grading Scale; A New Scale, A Pilot Study
 ISPUB.COM The Internet Journal of Interventional Medicine Volume 3 Number 1 Assessment Of Collateral Pathways In Acute Ischemic Cerebrovascular Stroke Using A Mansour Grading Scale; A New Scale, A Pilot
ISPUB.COM The Internet Journal of Interventional Medicine Volume 3 Number 1 Assessment Of Collateral Pathways In Acute Ischemic Cerebrovascular Stroke Using A Mansour Grading Scale; A New Scale, A Pilot
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Clinical Study Endovascular Recanalization for Chronic Symptomatic Intracranial Vertebral Artery Total Occlusion
 Minimally Invasive Surgery, Article ID 949585, 6 pages http://dx.doi.org/10.1155/2014/949585 Clinical Study Endovascular Recanalization for Chronic Symptomatic Intracranial Vertebral Artery Total Occlusion
Minimally Invasive Surgery, Article ID 949585, 6 pages http://dx.doi.org/10.1155/2014/949585 Clinical Study Endovascular Recanalization for Chronic Symptomatic Intracranial Vertebral Artery Total Occlusion
A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur.
 A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur. 6 year old school going child. Apparently normal till 3 yrs when she developed
A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur. 6 year old school going child. Apparently normal till 3 yrs when she developed
Moyamoya. Moyamoya Disease Double Trouble. Epidemiology 1/16/2015
 Moyamoya Moyamoya Disease Double Trouble Jan Boerke, ACNP AACN Brunch January 24, 2015 Moyamoya - puff of smoke in Japanese Describes the look of the tangle of tiny vessels formed to compensate for the
Moyamoya Moyamoya Disease Double Trouble Jan Boerke, ACNP AACN Brunch January 24, 2015 Moyamoya - puff of smoke in Japanese Describes the look of the tangle of tiny vessels formed to compensate for the
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Posterior Cerebral Artery Aneurysms with Common Carotid Artery Occlusion: A Report of Two Cases
 Journal of Neuroendovascular Therapy 2017; 11: 371 375 Online March 3, 2017 DOI: 10.5797/jnet.cr.2016-0114 Posterior Cerebral Artery Aneurysms with Common Carotid Artery Occlusion: A Report of Two Cases
Journal of Neuroendovascular Therapy 2017; 11: 371 375 Online March 3, 2017 DOI: 10.5797/jnet.cr.2016-0114 Posterior Cerebral Artery Aneurysms with Common Carotid Artery Occlusion: A Report of Two Cases
CASE REPORT AIR VENT OF VEIN GRAFT IN EXTRACRANIAL-INTRACRANIAL BYPASS SURGERY
 Nagoya J. Med. Sci. 74. 339 ~ 345, 2012 CASE REPORT AIR VENT OF VEIN GRAFT IN EXTRACRANIAL-INTRACRANIAL BYPASS SURGERY HIROFUMI OYAMA, AKIRA KITO, HIDEKI MAKI, KENICHI HATTORI, TOMOYUKI NODA and KENTARO
Nagoya J. Med. Sci. 74. 339 ~ 345, 2012 CASE REPORT AIR VENT OF VEIN GRAFT IN EXTRACRANIAL-INTRACRANIAL BYPASS SURGERY HIROFUMI OYAMA, AKIRA KITO, HIDEKI MAKI, KENICHI HATTORI, TOMOYUKI NODA and KENTARO
This quiz is being published on behalf of the Education Committee of the SNACC.
 Quiz 48 Cerebrovascular Atherosclerotic Disease Shobana Rajan, M.D. Associate Director of Neuroanesthesia, Vice Chair of Education, Allegheny Health Network. Quiz team; Suneeta Gollapudy M.D, Angele Marie
Quiz 48 Cerebrovascular Atherosclerotic Disease Shobana Rajan, M.D. Associate Director of Neuroanesthesia, Vice Chair of Education, Allegheny Health Network. Quiz team; Suneeta Gollapudy M.D, Angele Marie
Cerebral hyperperfusion syndrome after carotid angioplasty
 case report Cerebral hyperperfusion syndrome after carotid angioplasty Zoran Miloševič 1, Bojana Žvan 2, Marjan Zaletel 2, Miloš Šurlan 1 1 Institute of Radiology, 2 University Neurology Clinic, University
case report Cerebral hyperperfusion syndrome after carotid angioplasty Zoran Miloševič 1, Bojana Žvan 2, Marjan Zaletel 2, Miloš Šurlan 1 1 Institute of Radiology, 2 University Neurology Clinic, University
Extracranial to intracranial bypass for intracranial atherosclerosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
collaterals offset ischemia
 Imaging of Intracranial Stenosis objectives & next steps collaterals offset ischemia systematic evaluation of collaterals hemodynamic impact, not % stenosis develop fractional flow measures collateral
Imaging of Intracranial Stenosis objectives & next steps collaterals offset ischemia systematic evaluation of collaterals hemodynamic impact, not % stenosis develop fractional flow measures collateral
Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke
 Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Corporate Medical Policy
 Corporate Medical Policy Endovascular Therapies for Extracranial Vertebral Artery Disease File Name: Origination: Last CAP Review: Next CAP Review: Last Review: endovascular_therapies_for_extracranial_vertebral_artery_disease
Corporate Medical Policy Endovascular Therapies for Extracranial Vertebral Artery Disease File Name: Origination: Last CAP Review: Next CAP Review: Last Review: endovascular_therapies_for_extracranial_vertebral_artery_disease
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Advances in the treatment of posterior cerebral circulation symptomatic disease
 Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Carotid Artery Stent: Is it ready for prime time?
 2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
The National Institute of Neurological Disorders and Stroke
 ORIGINAL RESEARCH A. Srinivasan M. Goyal P. Stys M. Sharma C. Lum Microcatheter Navigation and Thrombolysis in Acute Symptomatic Cervical Internal Carotid Occlusion BACKGROUND AND PURPOSE: The treatment
ORIGINAL RESEARCH A. Srinivasan M. Goyal P. Stys M. Sharma C. Lum Microcatheter Navigation and Thrombolysis in Acute Symptomatic Cervical Internal Carotid Occlusion BACKGROUND AND PURPOSE: The treatment
Management of cervicocephalic arterial dissection. Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery
 Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Surgical Procedures for. Symptomatic Post-CAS Carotid. Restenosis: Experiences and. Mid-Term Outcomes. Lefeng Qu M.D., Ph.D. Professor of Surgery
 Surgical Procedures for Symptomatic Post-CAS Carotid Restenosis: Experiences and Mid-Term Outcomes Lefeng Qu M.D., Ph.D. Professor of Surgery Department of Vascular and Endovascular Surgery, Changzheng
Surgical Procedures for Symptomatic Post-CAS Carotid Restenosis: Experiences and Mid-Term Outcomes Lefeng Qu M.D., Ph.D. Professor of Surgery Department of Vascular and Endovascular Surgery, Changzheng
Ultrasound Imaging of The Posterior Circulation
 Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Neurosurg Focus 5 (5):Article 4, 1998
:Article 4, 1998") Neurosurg Focus 5 (5):Article 4, 1998 Multiple combined indirect procedure for the surgical treatment of children with moyamoya disease. A comparison with single indirect anastomosis with direct anastomosis
Neurosurg Focus 5 (5):Article 4, 1998 Multiple combined indirect procedure for the surgical treatment of children with moyamoya disease. A comparison with single indirect anastomosis with direct anastomosis
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective)
") Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
R ECENTLY, we reported a combined series of extracranial
 J Neurosurg 70:207-211, 1989 Complications of intracranial bypass for vertebrobasilar insufficiency LEO N. HOPKINS, M.D., AND JAMES L. BUDNY, M.D. Department of Neurosurgery, State University of New York
J Neurosurg 70:207-211, 1989 Complications of intracranial bypass for vertebrobasilar insufficiency LEO N. HOPKINS, M.D., AND JAMES L. BUDNY, M.D. Department of Neurosurgery, State University of New York
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP
 Case # 1 Hx 57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP show left PCA occlusion, some basilar stenosis,
Case # 1 Hx 57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP show left PCA occlusion, some basilar stenosis,
010050,Inner Mongolia, China
 Possible factors influencing postoperative temporary neurologic deterioration following standard superficial temporal artery-middle cerebral artery (STA-MCA) bypass surgery: diameter of STA and MCA (M4)
Possible factors influencing postoperative temporary neurologic deterioration following standard superficial temporal artery-middle cerebral artery (STA-MCA) bypass surgery: diameter of STA and MCA (M4)
Aortic arch pathology. Cerebral ischemia following carotid artery stenosis.
 Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Extracranial-to-Intracranial Bypass Using Radial Artery Grafting for Complex Skull Base Tumors: Technical Note
 Extracranial-to-Intracranial Bypass Using Radial Artery Grafting for Complex Skull Base Tumors: Technical Note Saleem I. Abdulrauf, M.D., F.A.C.S. 1 ABSTRACT The management of complex skull base tumors
Extracranial-to-Intracranial Bypass Using Radial Artery Grafting for Complex Skull Base Tumors: Technical Note Saleem I. Abdulrauf, M.D., F.A.C.S. 1 ABSTRACT The management of complex skull base tumors
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Int J Clin Exp Med 2018;11(9): /ISSN: /IJCEM
: /ISSN: /IJCEM") Int J Clin Exp Med 2018;11(9):10069-10075 www.ijcem.com /ISSN:1940-5901/IJCEM0069372 Case Report Acute cerebral infarction after spontaneous recanalization of extracranial internal carotid artery atherosclerotic
Int J Clin Exp Med 2018;11(9):10069-10075 www.ijcem.com /ISSN:1940-5901/IJCEM0069372 Case Report Acute cerebral infarction after spontaneous recanalization of extracranial internal carotid artery atherosclerotic
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease
 The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
Intracranial vascular anastomosis using the microanastomotic system
 J Neurosurg 89:676 681, 1998 Intracranial vascular anastomosis using the microanastomotic system Technical note DAVID W. NEWELL, M.D., ANDREW T. DAILEY, M.D., AND STEPHEN L. SKIRBOLL, M.D. Department of
J Neurosurg 89:676 681, 1998 Intracranial vascular anastomosis using the microanastomotic system Technical note DAVID W. NEWELL, M.D., ANDREW T. DAILEY, M.D., AND STEPHEN L. SKIRBOLL, M.D. Department of
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
Occlusion of All Four Extracranial Vessels With Minimal Clinical Symptomatology. Case Report
 Occlusion of All Four Extracranial Vessels With Minimal Clinical Symptomatology. Case Report BY JIRI J. VITEK, M.D., JAMES H. HALSEY, JR., M.D., AND HOLT A. McDOWELL, M.D. Abstract: Occlusion of All Four
Occlusion of All Four Extracranial Vessels With Minimal Clinical Symptomatology. Case Report BY JIRI J. VITEK, M.D., JAMES H. HALSEY, JR., M.D., AND HOLT A. McDOWELL, M.D. Abstract: Occlusion of All Four
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Overview Blood supply of the brain What is moyamoya disease? > 1
 Moyamoya Disease Overview Moyamoya disease is caused by blocked arteries at the base of the brain. The name "moyamoya" means "puff of smoke" in Japanese and describes the appearance of tiny vessels that
Moyamoya Disease Overview Moyamoya disease is caused by blocked arteries at the base of the brain. The name "moyamoya" means "puff of smoke" in Japanese and describes the appearance of tiny vessels that