Assessment and Management of Neurologic Complications After Cardiac and Aortic Surgery
|
|
|
- Sophia Lee
- 5 years ago
- Views:
Transcription

1 Assessment and Management of Neurologic Complications After Cardiac and Aortic Surgery Joseph S. Coselli, M.D. Professor and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery Baylor College of Medicine Toronto, Canada Sunday, May 2, 2010
 WL Gore & Associates, Inc (PI: Gore Conformable Descending/Dissection Thoracic Stent Graft Trial, Speaker 2009-10, Consultant")
2 Presenter Disclosure Joseph S. Coselli, MD The following relationships exist related to this presentation: Cook, Inc. (PI: TX2 Thoracic Stent Graft Trial) Medtronic, Inc. (PI: Valor II and THRIVE Stent Graft Trial, Consultant, Speaker 2009) WL Gore & Associates, Inc (PI: Gore Conformable Descending/Dissection Thoracic Stent Graft Trial, Speaker , Consultant ) Vascutek Terumo (Educational Grant, Royalties for Coselli Branched Graft for TAAA repairs, and Consultant )
3 Neurologic Injury Injury Following Cardiac or Aortic Surgery Altered Brain Perfusion Inflammatory Response Dispersed Emboli Hypoperfusion Non-pulsatile Perfusion Organ Specific Diffuse Systemic Atherosclerotic Particulate Lipid Gaseous
4 Neurologic Complications Neurologic complications tend to be associated with specific regions of repair Stroke Heart Ascending aorta Aortic arch Paraplegia Descending thoracic aorta Thoracoabdominal aorta

5 Risk Factors: Diabetes & Atherosclerosis 464 consecutive patients ( ) 372 ascending repair 92 arch repair Examined role of diabetes, atherosclerosis, dissection, coronary artery disease, gender, on poor outcomes Hagl JTCVS 2003;126;1005

6 Risk Factors: Diabetes & Atherosclerosis Ascending Aorta Factor P value Odds Ratio Diabetes Atherosclerosis Dissection Multivariate analysis of 372 ascending patients Diabetes, atherosclerosis, and dissection found to be significant predictors of adverse outcomes Death or stroke Hagl JTCVS 2003;126;1005
7 Risk Factors: Diabetes & Atherosclerosis Aortic Arch Multivariate analysis of Factor P value Odds Ratio Female gender Coronary artery disease + Total cerebral protection time 40 min min > 80 min per minute 92 aortic arch patients Female gender, CAD, and increasing total cerebral protection time found to be significant predictors of adverse outcomes Death or stroke Hagl JTCVS 2003;126;1005

8 Predictors of Outcome Univariate analysis of 531 patients 431 with total arch repair Stroke 2.9% 3.3% total arch repair Transient neurocognitive dysfunction 9.9% Ogino JTCVS 2008;136:641
9 Predictors of Outcome Arch vessel malperfusion (in dissection) Aortic arch atheroma Chronic renal failure Odds Ratio Ogino JTCVS 2008;136:641 P-value < Female gender Identified risks for permanent stroke include female gender, chronic renal failure, malperfusion of arch vessels during dissection, and pressence of aortic arch atheroma
10 Effect of prior brain injury on postoperative neurologic outcome Total Arch Replacement 131 patients 10/131 stroke 30/131 transient neurologic dysfunction Preoperative leukoaraiosis and hippocampal atrophy was assessed Morimoto ATS 2009;136:641

11 Predictors of Outcome A) Mild Leukoaraiosis B) Severe Leukoaraiosis C) Hippocampal atrophy was from coronal views of T1 weighted images Morimoto ATS 2009;136:641
12 Predictors of Outcome Stroke OR P-value Arch atheroma Leukoaraiosis score TND OR P-value Aortic atheroma Hippocampal atrophy score Morimoto ATS 2009;136: Leukoaraiosis score 1.3 <0.001 Effect of prior brain injury on postoperative neurologic outcome 131 patients 10/131 stroke 30/131 transient neurologic dysfunction Preoperative leukoaraiosis and hippocampal atrophy was found predictive

13 Early Aortic Arch Replacement Grafts Interesting approaches towards maintaining perfusion Synthetic grafts allow for creative placement DeBakey et al AMA Arch Surg 1958

14 Propose several perfusion strategies based on location Early Aortic Arch Replacement Grafts In their 1962 summary article, the key problems to replacing the aortic arch are Left ventricular strain Ischemic damage Hypothermia has been abandoned in favor of temporary bypass from CPB DeBakey et al SCNA 1962
15 Cardiopulmonary Bypass Associated with inflammatory response Contact of blood with artificial bypass surfaces Conversion of blood to nonpulsatile flow Activation of leukocyte and endothelial cells following ischemic and reperfusion states Activation of complement, fibrinolytic, and cytokine cascades
16 CPB: Complement Cascade Starts when blood contacts the artificial surfaces of the bypass circuit Inflammation increased cytokines Activation leukocytes Microvascular occlusion as leukocytes and endothelial cells interact Results in distal, end-organ ischemia
17 Therapeutic strategies Mitigate CPB-induced Inflammation Corticosteroids: decrease complement activation But, may increase risk of postoperative infection and delay wound healing Aprotinin: inhibits serine protease Withdrawn from market May 2008 due to concerns of increased adverse events
18 138 patients Early Aortic Arch Replacement Grafts Mortality of repair is improving, but remains nearly 20% Increases greatly with age Over age 60 has at least a 40% mortality rate DeBakey et al SCNA, 1962


19 Improving Arch Repair Single anastomosis approach to simplify and expedite repair Techniques to improve cerebral perfusion Assessing adequacy of perfusion extremely difficult Bloodwell et al Ann Thorac Surg 1968

20 Bloodwell et al Ann Thorac Surg 1968


21 1 st Island Arch Repair Bloodwell et al ATS 1968

22 Options During Circulatory Arrest How should we protect the brain? Hypothermic circulatory arrest alone Retrograde cerebral perfusion Antegrade cerebral perfusion


23 Improving Arch Repair Griepp et al J Thorac Cardiovasc Surg 1975 Hypothermia is revisited Benefits of profound hypothermic circulatory arrest for arch repair established Did not use cerebral perfusion 4 patients 3 survivors Limits of perfusion time not yet understood 60 minutes?
24 Impact of Temperature on Brain Normothermia Irreversible brain damage after 4 minutes of arrest Dissolved oxygen plays a trivial role in cerebral oxygen delivery and metabolism 1-2% of arterial O 2 content Profound hypothermia Hb avidity for O 2 / O 2 solubility Decrease CMRO 2 by 65-87% at 18 C Q 10 average 2-3 on CPB Potential safe arrest period Dexter ATS 1997;63:1725 Greeley JTCVS 1991

25 O2 Extraction ml/dl Oxygen Debt After HCA 1.6 Transcranial O 2 Extraction P <0.001 Arrest leads to a progressive O 2 debt manifest as increased oxygen extraction at the end of HCA. The debt is proportional to the duration of arrest 0 Pre HCA Post HCA Bonser JTCVS 2002;123:943

26 Hypothermic Circulatory Arrest HCA without adjuncts remains an acceptable approach, but has clear limitations. Stroke 7% Mortality 10% HCA used during aortic surgery in 656 patients 40 min increased stroke rate 65 min increased mortality rate Svensson et al J Thorac Cardiovasc Surg 1993

 Ueda et al Ann")
27 Improving Arch Repair Ueda Retrograde Perfusion Nippon Kyobu Geka Gakki Zasshi 1988 [Surgical treatment of the aneurysm or dissection involving the ascending aorta and aortic arch using circulatory arrest and retrograde perfusion] Article in Japanese Introduces concept of retrograde cerebral perfusion in 1988 Presents experience in 249 patients in patients with aneurysm 116 patients with dissection Average duration of RCP was 46 min Overall mortality was 24/249 (10%) Ueda et al Ann Thorac Surg 1999
28 Retrograde Cerebral Perfusion Potential benefits Cerebral metabolic support Maintenance of intracranial hypothermia Flushing of embolic debris and waste metabolites
29 Liver Spleen Kidney Heart Cortical grey Cortical white Hippocampus Cerebellum Medulla oblongata Regional organ blood flow (ml/min/100g) at 18 o C Minimal cerebral blood flow during retrograde cerebral perfusion (Microsphere CBF measurement technique) Antegrade cerebral perfusion Retrograde cerebral perfusion hour HCA / RCP Boeckxstaens et al. Ann Thorac Surg 1995;60:
30 Incidence of neuropsychometric deficit in HCA and HCA + RCP groups 100 p=0.22 % Neuropsychometric deficit p= weeks 12 weeks HCA RCP Harrington et al, J Thorac & Cardiovasc Surg, 2003
31 Mortality and stroke rate HCA ± RCP (479 pts) % event day mortality In-hospital deaths Stroke P< P< P< All patients(n=479) HCA + RCP (n=290) HCA only (n=189) * But HCA Only group had greater incidence of DM, CVA and Aortic dissection p<0.025 Coselli J Card Surg 1997;12(suppl):

32 Retrograde Cerebral Perfusion Widely used in recent past Developing consensus that efficacy is limited Failure to provide metabolic support Use is declining


33 Improving Arch Repair Return to Antegrade Cerebral Perfusion Flexible catheters facilitate use Kazui Antegrade Perfusion Annals of Thoracic Surgery 1992 Selective cerebral perfusion during operation for aneurysm of the aortic arch: a reassessment.

34 Antegrade Cerebral Perfusion Clear potential advantages Popularity of axillary artery cannulation increasing use

35 Improving Arch Repair Cerebral perfusion is revisited 10 patients spanning 1970 to 1985 Simplified CPB with partial brachiocephalic perfusion Moderate cooling Frist et al Ann Thorac Surg 1986

36 Intra-operative Management Use of transcranial Doppler to monitor cerebral perfusion Aortic Arch Surgery: Edmonds Ch


37 Intra-operative Management Use of near infrared spectroscopy to monitor cerebral perfusion

38 Perfusion via Axillary Artery Cannulation Rationale Simplifies delivery of antegrade cerebral perfusion Avoids malperfusion ACP via axillary artery has emerged as the method of choice.

39 Perfusion via Axillary Artery Cannulation
 0 Femoral 26 2 (8%) 2 (8%) Ascending 30 3 (10%) 4 (13%) All 122 7 (6%) 6 (5%) Axillary cannulation was associated with a significantly better outcome (p = 0.")
40 Axillary Cannulation 869 patients with ascending aorta/root repairs From 1995 to 2005 Right axillary cannulation in 451 patients Atherosclerotic aneurysm in 122 patients Cannulation n Death Stroke Axillary 66 2 (3%) 0 Femoral 26 2 (8%) 2 (8%) Ascending 30 3 (10%) 4 (13%) All (6%) 6 (5%) Axillary cannulation was associated with a significantly better outcome (p = 0.05) Etz et al, Ann Thorac Surg 2008
 12 (4%) Direct 1037 91 (9%) 69 (7%) All 1336 112 (8%) 81 (6%) Axillary cannulation was associated with a significantly")
41 Axillary Cannulation 1352 patients repairs with circulatory arrest 415 arch repairs From 1993 to 2003 Axillary or subclavian cannulation plus graft 299 Axillary or subclavian without graft 167 Propensity matched Cannulation n Death Stroke Axillary plus graft (7%) 12 (4%) Direct (9%) 69 (7%) All (8%) 81 (6%) Axillary cannulation was associated with a significantly better outcome (p = 0.09 and p = 0.05 in matched pairs) Svensson et al, Ann Thorac Surg 2004
42 Improving Arch Repair Total Experience As hypothermic circulatory arrest time increases, mortality and stroke increase Experience in 347 arch repairs ( ) Sundt et al Ann Thorac Surg 2008
43 Improving Arch Repair Retrograde CP Antegrade CP Appears to neutralize extended operative times Sundt et al Ann Thorac Surg 2008
, all surgical patients did much better than medical only <70 yrs 21% early death >70 yrs 31% early death Management Total n (All Ages) Mortality n (%) Medical 153 90/153")
44 IRAD Mortality: Acute Type A Dissection Analysis stratified by age Although younger surical patients did better (P=.005), all surgical patients did much better than medical only <70 yrs 21% early death >70 yrs 31% early death Management Total n (All Ages) Mortality n (%) Medical /153 (59%) Surgical /769 (24%) Trimarchi IRAD JTCVS In Press 2010
45 Axillary Artery Cannulation in Surgery For Acute or Subacute Ascending Aortic Dissections Wong, Coselli, Palmero, Bozinovski, Carter, Murariu, LeMaire Purpose: To describe the short- and mid-term results for repair of acute and subacute ascending aortic dissections in patients Dec 2003 April 2007 Wong, Coselli et al Ann Thorac Surg In Press 2010
46 Patients Baseline Patient Characteristics (n = 83) Age (years) 58 (22-84) Previous dissection 10 (12%) Previous stroke 7 (8%) Previous MI 6 (7%) COPD 9 (11%) Renal insufficiency/failure 3 (4%) Visceral ischemia 2 (2%) Wong, Coselli et al Ann Thorac Surg In Press 2010
47 Patients Presenting Disease Characteristics (n = 83) Disease Type Classic dissection 81 (98%) Intramural hematoma 2 (2%) Acuity of Dissection Acute 75 (90%) Subacute (15-60d) 8 (10%) Diseased Aortic Segment Ascending + desc aorta (DeBakey type I) 65 (78%) Ascending aorta only (DeBakey type II) 18 (22%) Wong, Coselli et al Ann Thorac Surg In Press 2010
48 Patients Findings at Presentation (n = 83) Rupture 7 (8%) Pericardial effusion 24 (29%) Cardiac tamponade 4 (5%) Acute neurologic injury Stroke 2 (2%) Transient ischemic attack 3 (4%) Paraplegia/paraparesis 2 (2%) Other 11 (13%) Wong, Coselli et al Ann Thorac Surg In Press 2010
49 Surgical Technique Operative Details (n = 83) Aortic valve replacement 4 (5%) Root replacement 16 (19%) Aortic valve repair 47 (57%) Hemiarch replacement 77 (93%) Elephant trunk arch replacement 3 (4%) Coronary artery bypass 13 (16%) Redo sternotomy 16 (19%) Wong, Coselli et al Ann Thorac Surg In Press 2010
50 Surgical Technique Operative Details (n = 83) CPB time, min 138 Cross-clamp time, min 57 Circulatory arrest time, min 37 Unprotected ischemic time, min 9 Wong, Coselli et al Ann Thorac Surg In Press 2010
51 Results Short-Term Outcomes (n = 83) Death, in-hospital or within 30 days 14 (17%) Stroke (6 with full recovery) 9 (11%) Paraplegia/paraparesis 0 Myocardial infarction 0 Reoperation for bleeding 7 (8%) Wong, Coselli et al Ann Thorac Surg In Press 2010
52 Survival (%) Results 3 Year Actuarial Survival: 63.5 ± 6% Mean follow-up time: 1.6 ± 1.3 yrs Time (years) Wong, Coselli et al Ann Thorac Surg In Press 2010
53 Mortality Acute Type A Dissection Author Year n Mortality Trimarchi IRAD in press (24%) Tsai IRAD (27%) Raghupathy IRAD (23%) Narayan (18%) Knipp NIS (26%) Erwin (23%) Haverich (24%)


54 Trifurcated Graft Technique 2002 Ann Thorac Surg 2002;74:S1810-4
; 7 hospital deaths (4.7%); 6 permanent strokes (4.1%) 7 patients (4.")
 required dialysis for transient renal failure ICU LOS: 3 (1-108) days; Total LOS: 10 (4-108) days")
55 Trifurcated Graft Technique patients over 6 years ( ) Adverse outcomes in 13 (8.7%); 7 hospital deaths (4.7%); 6 permanent strokes (4.1%) 7 patients (4.7%) with temporary neurological dysfunction 9 patients (6.0%) required dialysis for transient renal failure ICU LOS: 3 (1-108) days; Total LOS: 10 (4-108) days Use of technique with HCA and SCP is safe and versatile Ann Thorac Surg 2007;83:S791-5
56 Traditional Partial Arch Group n=165 (68%) 243 Arch Repairs : % Hemi-arch (n=157) Partial Arch with Innominate Graft (n=7)... Patch Repair (n=1)
57 Traditional Total Arch Group n=23 (10%) 243 Arch Repairs: % Arch with Island (n=3). Arch with Branched Arch Graft (n=6) ET with Island (n=14)

 ET with Trifurcated")
58 Trifurcated Graft Group n=55 (23%) 243 Arch Repairs: % Arch with Bifurcated Graft (n=7) Arch with Trifurcated Graft (n=1) ET with Bifurcated Graft (n=40) ET with Trifurcated Graft (n=7)
59

60
61
62
63
64

65
66

67

68
69 Operative Variables Operative Variables for 55 Patients Who Underwent Total Aortic Arch Replacement using the Trifurcated Graft Technique Urgency of Operation: Elective 43 (78%) Urgent 10 (18%) Emergent 2 (4%) Repeat Sternotomy 33 (60%) Concomitant procedures: Aortic valve replacement 12 (22%) Aortic valve repair (commissural plication) 10 (18%) Aortic root replacement 5 (9%)
70 Early Outcomes Early Outcome Characteristics of 55 Patients Who Underwent Total Aortic Arch Replacement using the Trifurcated Graft Technique Operative death: Hospital 0 (0%) Operative death: 30-day 1 (2%)* Bleeding requiring reoperation 4 (7%) Stroke 3 (5%) Myocardial Infarction 1 (2%) Arrhythmia 22 (40%) Atrial arrhythmia 21 (38%) Ventricular arrhythmia 3 (5%) *Pericardial effusion presenting with tamponade 13 days after discharge (21 days postop)
 returned for Stage II Results, Late")
 Endovascular Stage II Repair")
71 46 patients (98%) survived Stage I elephant trunk procedure 30 patients (65%) returned for Stage II Results, Late Outcomes Operative mortality for Stage II was 4% (1 patient) Open Stage II Repair 25/30 (83%) Endovascular Stage II Repair 5/30 (17%)
72 Comparison Outcome Variables Trifurcated Graft Technique (n=55) Traditional Partial Arch Replacement (n=165) Operative death 1 (2%) 10 (6%) 1 (4%) Stroke 3 (5%) 7 (4%) 3 (13%) Renal failure dialysis 3 (5%) 4 (2%) 1 (4%) Reoperation for bleeding 4 (7%) 9 (6%) 3 (13%) Traditional Full Arch Replacement (n=23) Actuarial 1-year survival % % % * p < 0.05 vs. Trifurcated Graft Technique group
73 Can we use Higher Temperatures? Hypothermic Circulatory Arrest: Group 1: Temperature < 20 ºC (16.7±1.7 ºC ) Group 2: Temperature 20 ºC (22.9±1.4 ºC ) Coselli, unpublished data 2010
74 Preoperative Characteristics Group 1 (n = 99) % Group 2 (n = 142) % P Value (χ 2 ) Female gender 34% 32% Age in years 62 ± ± Diabetes mellitus 9% 6% Smoking history 31% 41% Renal insufficiency 14% 14% Hypertension 85% 87% Carotid artery disease 13% 12% Pulmonary disease 24% 38% Coronary artery disease 30% 37% Congestive heart failure 35% 51% NYHA class III or IV 38% 41% History of CVA 7% 12% Acute aortic dissection 15% 13% Coselli, unpublished data 2010
75 Preoperative and Operative Characteristics Medical therapy Group 1 (n = 99) % Group 2 (n = 142) % P Value (χ 2 ) Use of antiplatelet agent 36% 39% Use of β-blocker 66% 70% Use of calcium channel blocker 23% 26% Use of statins 35% 40% Operative characteristics Hemi or partial arch surgery 74% 63% Total arch surgery 26% 37% Emergent surgery 17% 13% Reoperation, prior sternotomy 32% 36% Mean duration HCA, minutes 38 ± ± Mean duration CPB, minutes 154 ± ± Coselli, unpublished data 2010
76 Perioperative Transfusion Group 1 (n = 99) Group 2 (n = 142) P Value (χ 2 ) PRBC units FFP units Platelet aphresis units Coselli, unpublished data 2010
77 Postoperative Outcomes Group 1 (n = 99) % Group 2 (n = 142) % P Value (χ 2 ) Odds Ratio 95% Confidence Intervals 30-day mortality 9.1% 2.1% Hospital death 8.1% 0.7% Stroke 9.1% 2.8% Tracheostomy 23% 23% NS Postoperative RI 1.7% 2.2% NS Postoperative myocardial infarction 2.0% 1.4% NS Atrial fibrillation 36.4% 31.7% NS Sepsis 3.0% 3.3% NS Postoperative dialysis Hospital length of stay, days 5.1% 2.1% NS 18 ± ± Coselli, unpublished data 2010

78



79 Hybrid Approaches Gore TAG endograft 28x10cm distally. Placement of a 34x10 cm Gore TAG endostent proximally to the ascending aorta


80 Hybrid Approaches

81 STROKE RISK

82 Paraplegia Distal perfusion Shunts LHB CPB CPB + HCA Pharmacology Steroids Naloxone No Morphine Hypothermia Regional CPB Intercostal arteries Direct reattachment Preconditioning
83

84
85
86 # of Patients Left Heart Bypass v. No Bypass Paraplegia/Paraparesis in 751 Extent II TAAA % 10.2% Total Patients PAR/PLG p = Left Heart Bypass No Bypass Coselli

87 Cerebrospinal Fluid Drainage CSF pressure s during aortic clamping Blaisdell & Cooley, 1962 Ligation/Pressure studies At least 2 arteries needed Spinal perfusion MAP CSF pressure Goal improve spinal perfusion pressure Widespread use now commonly applied to endovascular approaches DTA/TAAA


88 Incidence of Paraplegia (%) 156 Extent I/II TAAA Repairs: With vs. Without CSF Drainage 20 P = With CSFD Without CSFD Coselli et al J Vasc Surg 2002
 218 patients Mortality 7.3% Paraplegia 4.6% Renal Failure - dialysis 6.")
89 Hypothermic Circulatory Arrest Approaches to TAA Aneurysm Repair Profound Hypothermic Circulatory Arrest Standard use of HCA in TAAA repairs Kouchoukos Ann Thorac Surg 2001 Kouchoukos Ann Thorac Surg 2002 Fehrenbacher Ann Thorac Surg 2007 Aortic Symposium 2010 (C I II III) 218 patients Mortality 7.3% Paraplegia 4.6% Renal Failure - dialysis 6.9%
 [10-33] [0-31%] [0-15%] [0-29%] [0-62%] 5,342 381 (7.1%) 280 (5.2%) 276/4210 (6.6%) 0 [56-2286] [5-17%] [2-9%] [2-12%] P < 0.001 P = 0.")
90 Hybrid Thoracoabdominal Repairs Comparison of Results Hybrid Open No. of Operative Renal Early Patients Mortality Paraplegia Dysfunction Endoleaks (16.7%) 10 (4.5%) 28 (12.6%) 51 (23.0%) [10-33] [0-31%] [0-15%] [0-29%] [0-62%] 5, (7.1%) 280 (5.2%) 276/4210 (6.6%) 0 [ ] [5-17%] [2-9%] [2-12%] P < P = Black 2006 Chiesa 2007 Siegenthaler 2008 Muehling 2009 Resch 2006 Lee 2007 Aguiar Luis 2009 Patel 2009 Zhou 2006 Böckler 2008 Kabanni 2009 Quinones-Baldrich 2009 Kouchoukos 2001 Jacobs 2006 Etz 2008 Schepens 2009 Chiesa 2004 Conrad 2007 Misfeld 2008 Sandmann 2005 Coselli 2007 Patel 2009
91 Early Outcomes in 441 TAAA Patients by Crawford Extent of Repair Crawford Extent of Repair Factor Extent I Extent II Extent III Extent IV (n = 111) (n =138) (n = 84) (n = 108) Early death In-hospital or 30-day death 4 (4%) 9 (7%) 6 (7%) 7 (6%) Permanent paraplegia 1 (1%) 5 (4%) 3 (4%) 1 (1%) Overall rate of permanent paraplegia is 2.3% (10/441) Mesenteric ischemia 0 1 ( 1%) 0 1 (1%) Acute renal dysfunction 11 (10%) 20 (14%) 11 (13%) 13 (12%) Acute renal failure 9 (8%) 14 (10%) 7 (8%) 9 (8%) On dialysis at discharge 2 (2%) 7 (5%) 3 (4%) 8 (7%) Overall rate of permanent renal failure is 4.5% (20/441) Unpublished Coselli Data March 2010
92 Paraplegia in 409 Patients by Crawford Extent of Repair Crawford Extent of Repair Factor Extent I Extent II Extent III Extent IV (n = 102) (n = 126) (n = 79) (n = 102) Paraplegia 7 (7%) 9 (7%) 5 (6%) 2 (2%) Immediate 0 2 (22%) 1(20%) 0 Delayed 7 (100%) 7 (78%) 4 (80%) 2 (100%) At discharge 1 (1%) 5 (4%) 3 (4%) 1(1%) Immediate 0 1 (20%) 1 (33%) 0 Delayed 1 (100%) 4 (80%) 2 (67%) 1 (100%) Most patients with paraplegia had delayed deficits
93 Paraplegia Rescue CSF Pressure 6 10 mmhg Steroids Mannitol Increase Systolic BP Maximize Oxygenation Optimize Hemodnamics and CO Naloxzone
94 Conclusions Early results using trifurcated graft technique compare favorably to traditional approaches Enables effective delivery of SCP Minimizes unprotected cerebral ischemic time Associated with low risk of neurological sequelae Readily adapted to accommodate anatomic variations Possibly reduce temp and operative time
95 Cannulation and Cooling Cannulation Axillary artery Temperature gradient 7 C Perfusion flow L.min-1min-2 Cooling duration minutes Nasopharyngeal temperature 24 C for >5 minutes Jugular bulb O2 saturation 95% Pre-treatment Mannitol 1g.kg-1 Dexamethasone 12mg 20 min pre-arrest Hematocrit 20-30% ph management alpha-stat Glucose management Insulin sliding scale WBG <10mmol.L-1
96 Arrest Period and ACP Position Trendelenberg 15 o C Technique HCA alone for anticipated arrest times 20 minutes ACP for all other cases Cannulation Balloon perfusion catheter via left carotid artery Left subclavian artery Occlusion with embolectomy catheter Perfusate temperature 15 C Hematocrit 20-30% Flow rate ml.kg-1.min-1 LCCA perfusion pressure mmhg without overt manipulation
97 Reperfusion and Rewarming Air Meticulous arch airdrill Perfusion flow L.min -1 min -2 Reperfusion temperature 24 o C for 5 minutes Temperature gradient 7 o C Nasopharyngeal temperature maximum 36.5 o C Arterial outflow temperature maximum 37 o C Rewarming duration Nasopharyngeal temperature 36.5 o C minutes Hematocrit 20-30% ph management alpha-stat Glucose management Insulin sliding scale WBG <10mmol.L -1



98 Thank you!
Aortic Arch/ Thoracoabdominal Aortic Replacement
 Aortic Arch/ Thoracoabdominal Aortic Replacement Joseph S. Coselli, M.D. Vice Chair, Department of Surgery Professor, Chief, and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery Baylor
Aortic Arch/ Thoracoabdominal Aortic Replacement Joseph S. Coselli, M.D. Vice Chair, Department of Surgery Professor, Chief, and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery Baylor
Chairman and O. Wayne Isom Professor Department of Cardiothoracic Surgery Weill Cornell Medicine
 Leonard N. Girardi, M.D. Chairman and O. Wayne Isom Professor Department of Cardiothoracic Surgery Weill Cornell Medicine New York, New York Houston Aortic Symposium Houston, Texas February 23, 2017 weill.cornell.edu
Leonard N. Girardi, M.D. Chairman and O. Wayne Isom Professor Department of Cardiothoracic Surgery Weill Cornell Medicine New York, New York Houston Aortic Symposium Houston, Texas February 23, 2017 weill.cornell.edu
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation
 Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm
 Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Major Aortic Reconstruction; Cerebral protection and Monitoring
 Major Aortic Reconstruction; Cerebral protection and Monitoring N AT H A E N W E I T Z E L M D A S S O C I AT E P R O F E S S O R O F A N E S T H E S I O LO G Y U N I V E R S I T Y O F C O LO R A D O S
Major Aortic Reconstruction; Cerebral protection and Monitoring N AT H A E N W E I T Z E L M D A S S O C I AT E P R O F E S S O R O F A N E S T H E S I O LO G Y U N I V E R S I T Y O F C O LO R A D O S
Total arch replacement with separated graft technique and selective antegrade cerebral perfusion
 Masters of Cardiothoracic Surgery Total arch replacement with separated graft technique and selective antegrade cerebral perfusion Teruhisa Kazui 1,2 1 Hamamatsu University School of Medicine, Hamamatsu,
Masters of Cardiothoracic Surgery Total arch replacement with separated graft technique and selective antegrade cerebral perfusion Teruhisa Kazui 1,2 1 Hamamatsu University School of Medicine, Hamamatsu,
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection: Con
 Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection: Con Thomas G. Gleason, M.D. Ronald V. Pellegrini Professor and Chief Division of Cardiac Surgery University of Pittsburgh Presenter
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection: Con Thomas G. Gleason, M.D. Ronald V. Pellegrini Professor and Chief Division of Cardiac Surgery University of Pittsburgh Presenter
Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist. M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria
 Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Evidence Surgical aortic arch replacement with a Dacron
Aortic Arch Treatment Open versus Endo Evidence versus Zeitgeist M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Evidence Surgical aortic arch replacement with a Dacron
Acute Aortic Dissection: Decision and Outcome
 Acute Aortic Dissection: Decision and Outcome Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Director, Center for Diseases of the Thoracic Aorta Washington University School
Acute Aortic Dissection: Decision and Outcome Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Director, Center for Diseases of the Thoracic Aorta Washington University School
Type II arch hybrid debranching procedure
 Safeguards and Pitfalls Type II arch hybrid debranching procedure Prashanth Vallabhajosyula, Wilson Y. Szeto, Nimesh Desai, Caroline Komlo, Joseph E. Bavaria Division of Cardiovascular Surgery, University
Safeguards and Pitfalls Type II arch hybrid debranching procedure Prashanth Vallabhajosyula, Wilson Y. Szeto, Nimesh Desai, Caroline Komlo, Joseph E. Bavaria Division of Cardiovascular Surgery, University
Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery
 Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery Are Young Patients More Likely to Develop Adverse Aortic Remodeling of the Remnant Aorta Over Time? Suk Jung Choo¹, Jihoon Kim¹,
Remodeling of the Remnant Aorta after Acute Type A Aortic Dissection Surgery Are Young Patients More Likely to Develop Adverse Aortic Remodeling of the Remnant Aorta Over Time? Suk Jung Choo¹, Jihoon Kim¹,
SELECTIVE ANTEGRADE TECHNIQUE OF CHOICE
 SELECTIVE ANTEGRADE CEREBRAL PERFUSION IS THE TECHNIQUE OF CHOICE MARKO TURINA University of Zurich Zurich, Switzerland What is so special about the operation on the aortic arch? Disease process is usually
SELECTIVE ANTEGRADE CEREBRAL PERFUSION IS THE TECHNIQUE OF CHOICE MARKO TURINA University of Zurich Zurich, Switzerland What is so special about the operation on the aortic arch? Disease process is usually
Simple retrograde cerebral perfusion is as good as complex antegrade cerebral perfusion for hemiarch replacement
 Perspective on Cardiac Surgery Page 1 of 7 Simple retrograde cerebral perfusion is as good as complex antegrade cerebral perfusion for hemiarch replacement Akiko Tanaka, Anthony L. Estrera Department of
Perspective on Cardiac Surgery Page 1 of 7 Simple retrograde cerebral perfusion is as good as complex antegrade cerebral perfusion for hemiarch replacement Akiko Tanaka, Anthony L. Estrera Department of
Neurological outcomes and mortality in patients with type A aortic dissection. Impact of intra-operative management
 Neurological outcomes and mortality in patients with type A aortic dissection. Impact of intra-operative management P Santé, M. Buonocore L Majello, A Caiazzo, G Petrone, G Nappi Dept. of Cardiothoracic
Neurological outcomes and mortality in patients with type A aortic dissection. Impact of intra-operative management P Santé, M. Buonocore L Majello, A Caiazzo, G Petrone, G Nappi Dept. of Cardiothoracic
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery
 Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery Type A Dissection Workshop 2014 CCC Vancouver Oct 26 th, 2014 Jehangir Appoo Libin Cardiovascular Institute University of Calgary
Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery Type A Dissection Workshop 2014 CCC Vancouver Oct 26 th, 2014 Jehangir Appoo Libin Cardiovascular Institute University of Calgary
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection
 Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Protecting the brain and spinal cord in aortic arch surgery
 Keynote Lecture Series Protecting the brain and spinal cord in aortic arch surgery Lars G. Svensson Heart & Vascular Institute, Cleveland Clinic, Cleveland, OH, USA Correspondence to: Lars G. Svensson,
Keynote Lecture Series Protecting the brain and spinal cord in aortic arch surgery Lars G. Svensson Heart & Vascular Institute, Cleveland Clinic, Cleveland, OH, USA Correspondence to: Lars G. Svensson,
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Early- and medium-term results after aortic arch replacement with frozen elephant trunk techniques a single center study
 Featured Article Early- and medium-term results after aortic arch replacement with frozen elephant trunk techniques a single center study Sergey Leontyev*, Martin Misfeld*, Piroze Daviewala, Michael A.
Featured Article Early- and medium-term results after aortic arch replacement with frozen elephant trunk techniques a single center study Sergey Leontyev*, Martin Misfeld*, Piroze Daviewala, Michael A.
Ann Thorac Cardiovasc Surg 2018; 24: Online January 26, 2018 doi: /atcs.oa Original Article
 Ann Thorac Cardiovasc Surg 2018; 24: 89 96 Online January 26, 2018 doi: 10.5761/atcs.oa.17-00138 Original Article Selective Cerebral Perfusion with the Open Proximal Technique during Descending Thoracic
Ann Thorac Cardiovasc Surg 2018; 24: 89 96 Online January 26, 2018 doi: 10.5761/atcs.oa.17-00138 Original Article Selective Cerebral Perfusion with the Open Proximal Technique during Descending Thoracic
I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical Department National Taiwan University Hospital
 Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Gelweave TM. Thoracic and Thoracoabdominal Graft Geometries. Ante-Flo TM 4 Branch Plexus. Siena Valsalva TM Trifurcate Arch Graft. Coselli.
 Gelweave TM Thoracic and Thoracoabdominal Graft Geometries Ante-Flo TM 4 Branch Plexus Siena Valsalva TM Trifurcate Arch Graft Coselli Lupiae Product availability subject to local regulatory approval.
Gelweave TM Thoracic and Thoracoabdominal Graft Geometries Ante-Flo TM 4 Branch Plexus Siena Valsalva TM Trifurcate Arch Graft Coselli Lupiae Product availability subject to local regulatory approval.
Advances in the Treatment of Acute Type A Dissection: An Integrated Approach
 Advances in the Treatment of Acute Type A Dissection: An Integrated Approach Joseph E. Bavaria, MD, Derek R. Brinster, MD, Robert C. Gorman, MD, Y. Joseph Woo, MD, Thomas Gleason, MD, and Alberto Pochettino,
Advances in the Treatment of Acute Type A Dissection: An Integrated Approach Joseph E. Bavaria, MD, Derek R. Brinster, MD, Robert C. Gorman, MD, Y. Joseph Woo, MD, Thomas Gleason, MD, and Alberto Pochettino,
Total arch replacement using selective antegrade cerebral perfusion as the neuroprotection strategy
 Featured Article Total arch replacement using selective antegrade cerebral perfusion as the neuroprotection strategy Yutaka Okita, Kenji Okada, Atsushi Omura, Hiroya Kano, Hitoshi Minami, Takeshi Inoue,
Featured Article Total arch replacement using selective antegrade cerebral perfusion as the neuroprotection strategy Yutaka Okita, Kenji Okada, Atsushi Omura, Hiroya Kano, Hitoshi Minami, Takeshi Inoue,
How to manage the left subclavian and left vertebral artery during TEVAR
 How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
ORIGINAL ARTICLE. Systemic Temperature and Paralysis After Thoracoabdominal and Descending Aortic Operations
 ORIGINAL ARTICLE Systemic Temperature and Paralysis After Thoracoabdominal and Descending Aortic Operations Lars G. Svensson, MD, PhD; Lev Khitin, MD; Edward M. Nadolny, CCP; Wendy A. Kimmel, CCP Hypothesis:
ORIGINAL ARTICLE Systemic Temperature and Paralysis After Thoracoabdominal and Descending Aortic Operations Lars G. Svensson, MD, PhD; Lev Khitin, MD; Edward M. Nadolny, CCP; Wendy A. Kimmel, CCP Hypothesis:
debris + 3 debris debris debris Tel: ,3
 13 467 471 2004 debris + 3 13.2 15.47.0 6.5 7.7 0 3 25.012.5 7.0 0 13 467 471 2004 Tel: 075-251-5752 602-8566 463-1 2004 3 7 2004 5 18 30 1 2,3 4 2000 7 debris debris debris 7 13 4 Table 1 Patients profiles
13 467 471 2004 debris + 3 13.2 15.47.0 6.5 7.7 0 3 25.012.5 7.0 0 13 467 471 2004 Tel: 075-251-5752 602-8566 463-1 2004 3 7 2004 5 18 30 1 2,3 4 2000 7 debris debris debris 7 13 4 Table 1 Patients profiles
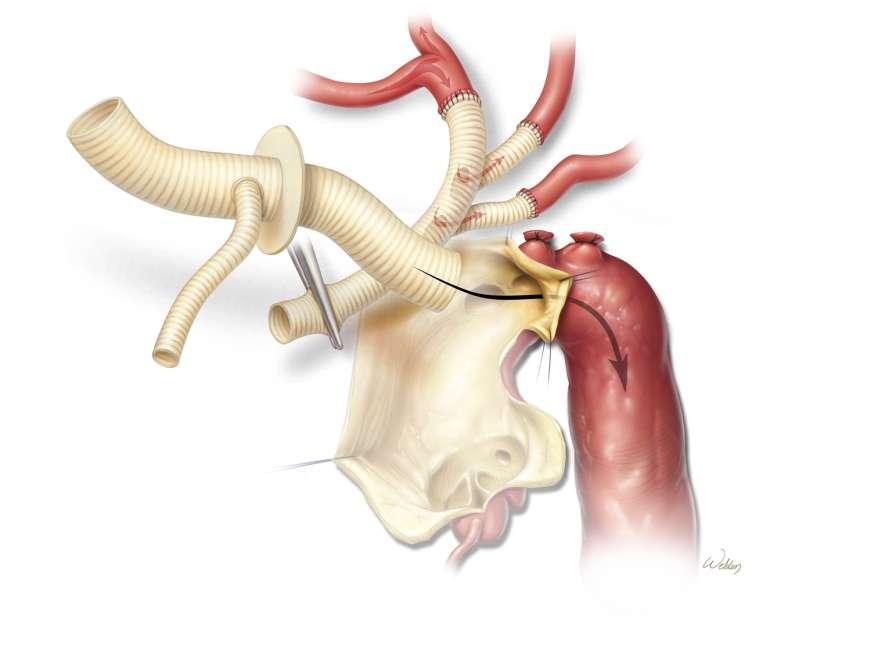
Thoracoabdominal aortic aneurysms by definition traverse
 Thoracoabdominal Aortic Aneurysm Repair: Open Technique Joseph Huh, MD, Scott A. LeMaire, MD, Scott A. Weldon, MA, CMI, and Joseph S. Coselli, MD Thoracoabdominal aortic aneurysms by definition traverse
Thoracoabdominal Aortic Aneurysm Repair: Open Technique Joseph Huh, MD, Scott A. LeMaire, MD, Scott A. Weldon, MA, CMI, and Joseph S. Coselli, MD Thoracoabdominal aortic aneurysms by definition traverse
Management of Acute Aortic Syndromes. M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria
 Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Thoracoabdominal Aneurysm Repair: From Athena to Zeus
 Thoracoabdominal Aneurysm Repair: From Athena to Zeus Joseph S. Coselli, M.D. Vice Chair, Department of Surgery Professor, Chief, and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery,
Thoracoabdominal Aneurysm Repair: From Athena to Zeus Joseph S. Coselli, M.D. Vice Chair, Department of Surgery Professor, Chief, and Cullen Foundation Endowed Chair Division of Cardiothoracic Surgery,
Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device
 Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device Luis A. Sanchez MD Gregorio A. Sicard Distinguished Professor of Surgery & Radiology Chief, Section of Vascular Surgery
Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device Luis A. Sanchez MD Gregorio A. Sicard Distinguished Professor of Surgery & Radiology Chief, Section of Vascular Surgery
Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques
 Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques Tariq Almerey MD, January Moore BA, Houssam Farres MD, Richard Agnew MD, W. Andrew Oldenburg MD, Albert Hakaim MD Department of Vascular
Complex Thoracic and Abdominal Aortic Repair Using Hybrid Techniques Tariq Almerey MD, January Moore BA, Houssam Farres MD, Richard Agnew MD, W. Andrew Oldenburg MD, Albert Hakaim MD Department of Vascular
Thoracoabdominal Aorta: Advances and Novel Therapies
 Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Department of Cardiovascular Surgery, Beijing Anzhen Hospital of Capital Medical University, Beijing Aortic Disease Center, Beijing, China;
 Featured Article Sun s procedure of total arch replacement using a tetrafurcated graft with stented elephant trunk implantation: analysis of early outcome in 398 patients with acute type A aortic dissection
Featured Article Sun s procedure of total arch replacement using a tetrafurcated graft with stented elephant trunk implantation: analysis of early outcome in 398 patients with acute type A aortic dissection
Aortic arch repair under moderate hypothermic circulatory arrest with or without antegrade cerebral perfusion based on the extent of repair
 Original Article Aortic arch repair under moderate hypothermic circulatory arrest with or without antegrade cerebral perfusion based on the extent of repair Sung Jun Park 1 *, Bo Bae Jeon 2 *, Hee Jung
Original Article Aortic arch repair under moderate hypothermic circulatory arrest with or without antegrade cerebral perfusion based on the extent of repair Sung Jun Park 1 *, Bo Bae Jeon 2 *, Hee Jung
Brain Protection Using Antegrade Selective Cerebral Perfusion: A Multicenter Study
 Brain Protection Using Antegrade Selective Cerebral Perfusion: A Multicenter Study Marco Di Eusanio, MD, Marc A. A. M. Schepens, MD, PhD, Wim J. Morshuis, MD, PhD, Karl M. Dossche, MD, PhD, Roberto Di
Brain Protection Using Antegrade Selective Cerebral Perfusion: A Multicenter Study Marco Di Eusanio, MD, Marc A. A. M. Schepens, MD, PhD, Wim J. Morshuis, MD, PhD, Karl M. Dossche, MD, PhD, Roberto Di
SPINAL CORD ISCHEMIA AFTER THORACIC ANEURYSM REPAIR: RISK STRATIFICATION & PREVENTION DISCLOSURES. INDIVIDUAL None
 DISCLOSURES AFTER THORACIC ANEURYSM REPAIR: INDIVIDUAL None RISK STRATIFICATION & PREVENTION INSTITUTIONAL Cook, Inc W. L. Gore, Inc Conrad, J Vasc Surg, 2008 1 Intraoperative Adjuncts Oversew intercostals
DISCLOSURES AFTER THORACIC ANEURYSM REPAIR: INDIVIDUAL None RISK STRATIFICATION & PREVENTION INSTITUTIONAL Cook, Inc W. L. Gore, Inc Conrad, J Vasc Surg, 2008 1 Intraoperative Adjuncts Oversew intercostals
Total Arch Replacement Using Bilateral Axillary Antegrade Selective Cerebral Perfusion
 Original Article Total Arch Replacement Using Bilateral Axillary Antegrade Selective Cerebral Perfusion Satoshi Yamashiro, MD, PhD, Yukio Kuniyoshi, MD, Katsuya Arakaki, MD, Hitoshi Inafuku, MD, Yuji Morishima,
Original Article Total Arch Replacement Using Bilateral Axillary Antegrade Selective Cerebral Perfusion Satoshi Yamashiro, MD, PhD, Yukio Kuniyoshi, MD, Katsuya Arakaki, MD, Hitoshi Inafuku, MD, Yuji Morishima,
SdO 2. p Hypothermic circulatory arrest: HCA n = 6 Continuous retrograde cerebral perfusion: retrograde cerebral perfusion: IRCP
 20 3 49 55 2005 2 24 4 SdO 2 SdO 2 SdO 2 p 0.01 1999 409-3898 1110 2005 4 27 2005 4 27 JW 24 Hypothermic circulatory arrest: HCA n = 6 Continuous retrograde cerebral perfusion: n = 6 Intermittent retrograde
20 3 49 55 2005 2 24 4 SdO 2 SdO 2 SdO 2 p 0.01 1999 409-3898 1110 2005 4 27 2005 4 27 JW 24 Hypothermic circulatory arrest: HCA n = 6 Continuous retrograde cerebral perfusion: n = 6 Intermittent retrograde
To reduce the morbidity and mortality associated with
 Cardiac Surgery Aortic Arch Replacement/ Selective Antegrade Perfusion David Spielvogel, MD*, Steven L. Lansman, MD, PhD, and Randall B. Griepp, MD To reduce the morbidity and mortality associated with
Cardiac Surgery Aortic Arch Replacement/ Selective Antegrade Perfusion David Spielvogel, MD*, Steven L. Lansman, MD, PhD, and Randall B. Griepp, MD To reduce the morbidity and mortality associated with
Modification in aortic arch replacement surgery
 Gao et al. Journal of Cardiothoracic Surgery (2018) 13:21 DOI 10.1186/s13019-017-0689-y LETTER TO THE EDITOR Modification in aortic arch replacement surgery Feng Gao 1,2*, Yongjie Ye 2, Yongheng Zhang
Gao et al. Journal of Cardiothoracic Surgery (2018) 13:21 DOI 10.1186/s13019-017-0689-y LETTER TO THE EDITOR Modification in aortic arch replacement surgery Feng Gao 1,2*, Yongjie Ye 2, Yongheng Zhang
Open surgical repair of thoracoabdominal aneurysms - the Massachusetts General Hospital experience
 Research Highlight Open surgical repair of thoracoabdominal aneurysms - the Massachusetts General Hospital experience Virendra I. Patel, Robert T. Lancaster, Mark F. Conrad, Richard P. Cambria Division
Research Highlight Open surgical repair of thoracoabdominal aneurysms - the Massachusetts General Hospital experience Virendra I. Patel, Robert T. Lancaster, Mark F. Conrad, Richard P. Cambria Division
Total Arch Replacement Under Flow Monitoring During Selective Cerebral Perfusion Using a Single Pump
 Total Arch Replacement Under Flow Monitoring During Selective Cerebral Perfusion Using a Single Pump Hideyuki Shimizu, MD, PhD, Toru Matayoshi, CP, Masanori Morita, CP, Toshihiko Ueda, MD, PhD, and Ryohei
Total Arch Replacement Under Flow Monitoring During Selective Cerebral Perfusion Using a Single Pump Hideyuki Shimizu, MD, PhD, Toru Matayoshi, CP, Masanori Morita, CP, Toshihiko Ueda, MD, PhD, and Ryohei
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy. Johannes Lammer Medical University Vienna, Austria
 Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Cannulation of the femoral artery with retrograde
 PROXIMAL AORTIC PERFUSION FOR COMPLEX ARCH AND DESCENDING AORTIC DISEASE Stephen Westaby, MS, FRCS Takahiro Katsumata, MD Objective: Cannulation of the femoral artery is used routinely for hypothermic
PROXIMAL AORTIC PERFUSION FOR COMPLEX ARCH AND DESCENDING AORTIC DISEASE Stephen Westaby, MS, FRCS Takahiro Katsumata, MD Objective: Cannulation of the femoral artery is used routinely for hypothermic
Minimally Invasive Aortic Arch Surgery:
 Minimally Invasive Aortic Arch Surgery: Where are we? Where are we headed? Jehangir J. Appoo Libin Cardiovascular Institute University of Calgary www.aorta.ca June 15, 2016 Cardiac Masters Day: Minimally
Minimally Invasive Aortic Arch Surgery: Where are we? Where are we headed? Jehangir J. Appoo Libin Cardiovascular Institute University of Calgary www.aorta.ca June 15, 2016 Cardiac Masters Day: Minimally
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients
 Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients A Prospective, Multi-Center, Comparative Study Joseph S. Coselli, Irina V. Volguina, Scott A. LeMaire, Thoralf M. Sundt, Elizabeth
Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients A Prospective, Multi-Center, Comparative Study Joseph S. Coselli, Irina V. Volguina, Scott A. LeMaire, Thoralf M. Sundt, Elizabeth
Circulatory Arrest Under Moderate Systemic Hypothermia and Cold Retrograde Cerebral Perfusion
 ORIGINAL ARTICLES: CARDIOVASCULAR Circulatory Arrest Under Moderate Systemic Hypothermia and Cold Retrograde Cerebral Perfusion Yaron Moshkovitz, MD, Tirone E. David, MD, Michael Caleb, MD, Christopher
ORIGINAL ARTICLES: CARDIOVASCULAR Circulatory Arrest Under Moderate Systemic Hypothermia and Cold Retrograde Cerebral Perfusion Yaron Moshkovitz, MD, Tirone E. David, MD, Michael Caleb, MD, Christopher
Accepted Manuscript. Perioperative renal function and thoracoabdominal aneurysm repair: Where do we go from here? Leonard N. Girardi, M.D.
 Accepted Manuscript Perioperative renal function and thoracoabdominal aneurysm repair: Where do we go from here? Leonard N. Girardi, M.D. PII: S0022-5223(18)31804-X DOI: 10.1016/j.jtcvs.2018.06.057 Reference:
Accepted Manuscript Perioperative renal function and thoracoabdominal aneurysm repair: Where do we go from here? Leonard N. Girardi, M.D. PII: S0022-5223(18)31804-X DOI: 10.1016/j.jtcvs.2018.06.057 Reference:
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D.
 How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D. AATS International Cardiovascular Symposium 2017 Session 6: Technical Aspects of Open Surgery on the Aortic Valve Sao Paulo, Brazil
How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D. AATS International Cardiovascular Symposium 2017 Session 6: Technical Aspects of Open Surgery on the Aortic Valve Sao Paulo, Brazil
AORTIC DISSECTION. DISSECTING ANEURYSMS OF THE AORTA or CLASSIFICATION
 DISSECTING ANEURYSMS OF THE AORTA or AORTIC DISSECTION CLASSIFICATION DeBakey classified aortic dissections into types I, II, and III :- Type I dissection the tear site originates in the ascending aorta,
DISSECTING ANEURYSMS OF THE AORTA or AORTIC DISSECTION CLASSIFICATION DeBakey classified aortic dissections into types I, II, and III :- Type I dissection the tear site originates in the ascending aorta,
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Femoral Versus Aortic Cannulation for Surgery of Chronic Ascending Aortic Aneurysm
 Femoral Versus Aortic Cannulation for Surgery of Chronic Ascending Aortic Aneurysm Fitsum Lakew, MD, Piotr Pasek, MD, Michael Zacher, MD, Anno Diegeler, MD, and Paul P. Urbanski, MD Department of Cardiovascular
Femoral Versus Aortic Cannulation for Surgery of Chronic Ascending Aortic Aneurysm Fitsum Lakew, MD, Piotr Pasek, MD, Michael Zacher, MD, Anno Diegeler, MD, and Paul P. Urbanski, MD Department of Cardiovascular
Midterm Results of Aortic Arch Replacement in a Stanford Type A Aortic Dissection With an Intimal Tear in the Aortic Arch
 ORIGINAL ARTICLE DOI 10.4070 / kcj.2009.39.7.270 Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright c 2009 The Korean Society of Cardiology Midterm Results of Aortic Arch Replacement in a Stanford
ORIGINAL ARTICLE DOI 10.4070 / kcj.2009.39.7.270 Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright c 2009 The Korean Society of Cardiology Midterm Results of Aortic Arch Replacement in a Stanford
Use of carotid subclavian arterial bypass and thoracic endovascular aortic repair to minimize cerebral ischemia in total aortic arch reconstruction
 Xydas et al Evolving Technology/Basic Science Use of carotid subclavian arterial bypass and thoracic endovascular aortic repair to minimize cerebral ischemia in total aortic arch reconstruction Steve Xydas,
Xydas et al Evolving Technology/Basic Science Use of carotid subclavian arterial bypass and thoracic endovascular aortic repair to minimize cerebral ischemia in total aortic arch reconstruction Steve Xydas,
Advances in Treatment of Traumatic Aortic Transection
 Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
OPEN AND ENDOVASCULAR TECHNIQUES IN THE CARDIOTHORACIC SURGEON S HANDS
 4 th Aortic Live Symposium OPEN AND ENDOVASCULAR TECHNIQUES IN THE CARDIOTHORACIC SURGEON S HANDS A/Prof George Matalanis Director Cardiac Surgery Austin Hospital Disclosure I do not have any potential
4 th Aortic Live Symposium OPEN AND ENDOVASCULAR TECHNIQUES IN THE CARDIOTHORACIC SURGEON S HANDS A/Prof George Matalanis Director Cardiac Surgery Austin Hospital Disclosure I do not have any potential
Thoracoabdominal aortic replacement for Crawford extent II aneurysm after thoracic endovascular aortic repair
 Original Article Thoracoabdominal aortic replacement for Crawford extent II aneurysm after thoracic endovascular aortic repair Haiou Hu, Tie Zheng, Junming Zhu, Yongmin Liu, Ruidong Qi, Lizhong Sun Department
Original Article Thoracoabdominal aortic replacement for Crawford extent II aneurysm after thoracic endovascular aortic repair Haiou Hu, Tie Zheng, Junming Zhu, Yongmin Liu, Ruidong Qi, Lizhong Sun Department
OPCAB IS NOT BETTER THAN CONVENTIONAL CABG
 OPCAB IS NOT BETTER THAN CONVENTIONAL CABG Harold L. Lazar, M.D. Harold L. Lazar, M.D. Professor of Cardiothoracic Surgery Boston Medical Center and the Boston University School of Medicine Boston, MA
OPCAB IS NOT BETTER THAN CONVENTIONAL CABG Harold L. Lazar, M.D. Harold L. Lazar, M.D. Professor of Cardiothoracic Surgery Boston Medical Center and the Boston University School of Medicine Boston, MA
Influence of Perioperative Hemodynamics on Spinal Cord Ischemia in Thoracoabdominal Aortic Repair
 Influence of Perioperative Hemodynamics on Spinal Cord Ischemia in Thoracoabdominal Aortic Repair Yujiro Kawanishi, MD, Kenji Okada, MD, Masamichi Matsumori, MD, Hiroshi Tanaka, MD, Teruo Yamashita, MD,
Influence of Perioperative Hemodynamics on Spinal Cord Ischemia in Thoracoabdominal Aortic Repair Yujiro Kawanishi, MD, Kenji Okada, MD, Masamichi Matsumori, MD, Hiroshi Tanaka, MD, Teruo Yamashita, MD,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Predictors of Adverse Outcome and Transient Neurological Dysfunction After Ascending Aorta/Hemiarch Replacement
 Predictors of Adverse Outcome and Transient Neurological Dysfunction After Ascending Aorta/Hemiarch Replacement Marek P. Ehrlich, MD, M. Arisan Ergin, MD, PhD, Jock N. McCullough, MD, Steven L. Lansman,
Predictors of Adverse Outcome and Transient Neurological Dysfunction After Ascending Aorta/Hemiarch Replacement Marek P. Ehrlich, MD, M. Arisan Ergin, MD, PhD, Jock N. McCullough, MD, Steven L. Lansman,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation, radiofrequency, anesthetic considerations for, 479 489 Acute aortic syndrome, thoracic endovascular repair of, 457 462 aortic
Index Note: Page numbers of article titles are in boldface type. A Ablation, radiofrequency, anesthetic considerations for, 479 489 Acute aortic syndrome, thoracic endovascular repair of, 457 462 aortic
Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider
 Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider Matthias Thielmann, MD, PhD, FAHA Thoracic and Cardiovascular Surgery, West-German Heart and Vascular Center
Optimised management of type A aortic dissection with visceral malperfusion concept to reconsider Matthias Thielmann, MD, PhD, FAHA Thoracic and Cardiovascular Surgery, West-German Heart and Vascular Center
Surgical Considerations of TEVAR
 Surgical Considerations of TEVAR University of Alberta, June 14 th, 2013 Jehangir Appoo Libin Cardiovascular Institute University of Calgary, Today: Lesions/Pathology amenable to TEVAR On label Off label
Surgical Considerations of TEVAR University of Alberta, June 14 th, 2013 Jehangir Appoo Libin Cardiovascular Institute University of Calgary, Today: Lesions/Pathology amenable to TEVAR On label Off label
Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques
 Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques Konstadinos A Plestis, MD System Chief of Cardiothoracic and Vascular
Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques Konstadinos A Plestis, MD System Chief of Cardiothoracic and Vascular
THE EVOLUTION OF FET-TECHNIQUE
 4 th Aortic Live Symposium THE EVOLUTION OF FET-TECHNIQUE Heinz Jakob, MD PhD West German Heart andvascular Center, University Duisburg-Essen, Germany Disclosure Speaker name: Heinz Jakob JOTEC GmbH, Hechingen,
4 th Aortic Live Symposium THE EVOLUTION OF FET-TECHNIQUE Heinz Jakob, MD PhD West German Heart andvascular Center, University Duisburg-Essen, Germany Disclosure Speaker name: Heinz Jakob JOTEC GmbH, Hechingen,
H. J. Safit, M. P. Campbell, C. C. Miller III, D. C. Iliopoulos, A. Khoynezhad, G. V. Letsou and P. J. Asimacopoulos
 Eur J Vasc Endovasc Surg 14, 118-124 (1997) Cerebral Spinal Fluid Drainage and Distal Aortic Perfusion Decrease the Incidence of Neurological Deficit: The Results of 343 Descending and Thoracoabdominal
Eur J Vasc Endovasc Surg 14, 118-124 (1997) Cerebral Spinal Fluid Drainage and Distal Aortic Perfusion Decrease the Incidence of Neurological Deficit: The Results of 343 Descending and Thoracoabdominal
EACTS Adult Cardiac Database
 EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication vs Benefit? Mortality? Morbidity?
 Preoperative intraaortic balloon counterpulsation in high-risk CABG Stefan Klotz, M.D. Preoperative IABP in high-risk CABG Questions?? Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication
Preoperative intraaortic balloon counterpulsation in high-risk CABG Stefan Klotz, M.D. Preoperative IABP in high-risk CABG Questions?? Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication
Technique and Outcome of Laser Fenestration For Arch Vessels
 Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Frozen elephant trunk for DeBakey type 1 dissection: the Cleveland Clinic technique
 Masters of Cardiothoracic Surgery Frozen elephant trunk for DeBakey type 1 dissection: the Cleveland Clinic technique Eric E. Roselli, Michael Z. Tong, Faisal G. Bakaeen Aorta Center, Department of Thoracic
Masters of Cardiothoracic Surgery Frozen elephant trunk for DeBakey type 1 dissection: the Cleveland Clinic technique Eric E. Roselli, Michael Z. Tong, Faisal G. Bakaeen Aorta Center, Department of Thoracic
The morbidity and mortality rates associated with the. Outcome of Surgical Treatment in Patients With Acute Type B Aortic Dissection
 Outcome of Surgical Treatment in Patients With Acute Type B Aortic Dissection Tomoki Shimokawa, MD, Kazutaka Horiuchi, MD, Naomi Ozawa, MD, Kenu Fumimoto, MD, Susumu Manabe, MD, Tetsuya Tobaru, MD, and
Outcome of Surgical Treatment in Patients With Acute Type B Aortic Dissection Tomoki Shimokawa, MD, Kazutaka Horiuchi, MD, Naomi Ozawa, MD, Kenu Fumimoto, MD, Susumu Manabe, MD, Tetsuya Tobaru, MD, and
Evolving Strategy and Results of Spinal Cord Protection in Type I and II Thoracoabdominal Aortic Aneurysm Repair
 Original Article Evolving Strategy and Results of Spinal Cord Protection in Type I and II Thoracoabdominal Aortic Aneurysm Repair Norihiko Shiiya, MD, Takashi Kunihara, MD, Kenji Matsuzaki, MD, and Keishu
Original Article Evolving Strategy and Results of Spinal Cord Protection in Type I and II Thoracoabdominal Aortic Aneurysm Repair Norihiko Shiiya, MD, Takashi Kunihara, MD, Kenji Matsuzaki, MD, and Keishu
Among the many challenges presented to the cardiovascular. Impact of Retrograde Cerebral Perfusion on Ascending Aortic and Arch Aneurysm Repair
 Impact of Retrograde Cerebral Perfusion on Ascending Aortic and Arch Aneurysm Repair Hazim J. Safi, MD, George V. Letsou, MD, Dimitrios C. Iliopoulos, MD, Mahesh H. Subramaniam, MS, Charles C. Miller III,
Impact of Retrograde Cerebral Perfusion on Ascending Aortic and Arch Aneurysm Repair Hazim J. Safi, MD, George V. Letsou, MD, Dimitrios C. Iliopoulos, MD, Mahesh H. Subramaniam, MS, Charles C. Miller III,
THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR
 Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Intra-operative Effects of Cardiac Surgery Influence on Post-operative care. Richard A Perryman
 Intra-operative Effects of Cardiac Surgery Influence on Post-operative care Richard A Perryman Intra-operative Effects of Cardiac Surgery Cardiopulmonary Bypass Hypothermia Cannulation events Myocardial
Intra-operative Effects of Cardiac Surgery Influence on Post-operative care Richard A Perryman Intra-operative Effects of Cardiac Surgery Cardiopulmonary Bypass Hypothermia Cannulation events Myocardial
Selective antegrade cerebral perfusion during aortic arch surgery confers survival and neuroprotective advantages
 Selective antegrade cerebral perfusion during aortic arch surgery confers survival and neuroprotective advantages Mohammad Shihata, MD, a Rohan Mittal, a A. Senthilselvan, hd, b David Ross, MD, a Arvind
Selective antegrade cerebral perfusion during aortic arch surgery confers survival and neuroprotective advantages Mohammad Shihata, MD, a Rohan Mittal, a A. Senthilselvan, hd, b David Ross, MD, a Arvind
EVAR follow up: answers to uncertainties Moderators F. Moll, Y. Alimi, M. Bjorck. Inflammatory response after EVAR: causes and clinical implication
 39 th Annual Meeting, Boston, Sept. 2012 EVAR follow up: answers to uncertainties Moderators F. Moll, Y. Alimi, M. Bjorck Inflammatory response after EVAR: causes and clinical implication Christos D. Liapis,
39 th Annual Meeting, Boston, Sept. 2012 EVAR follow up: answers to uncertainties Moderators F. Moll, Y. Alimi, M. Bjorck Inflammatory response after EVAR: causes and clinical implication Christos D. Liapis,
Endovascular Branched Aortic Arch Repair
 Houston Aortic Symposium 2018 Endovascular Branched Aortic Arch Repair Nimesh D. Desai MD PhD Associate Professor of Surgery, University of Pennsylvania Co-Director, Penn Thoracic Aortic Surgery Program
Houston Aortic Symposium 2018 Endovascular Branched Aortic Arch Repair Nimesh D. Desai MD PhD Associate Professor of Surgery, University of Pennsylvania Co-Director, Penn Thoracic Aortic Surgery Program
STS/EACTS LatAm CV Conference 2017
 STS/EACTS LatAm CV Conference 2017 Joseph E. Bavaria, MD Director, Thoracic Aortic Surgery Program Roberts-Measey Professor and Vice Chair of CV Surgery University of Pennsylvania Immediate-Past President
STS/EACTS LatAm CV Conference 2017 Joseph E. Bavaria, MD Director, Thoracic Aortic Surgery Program Roberts-Measey Professor and Vice Chair of CV Surgery University of Pennsylvania Immediate-Past President
Aneurysms that arise in the distal aortic arch and
 Surgical Management of Distal Arch Aneurysm: Another Approach With Improved Results Kenji Minatoya, MD, Hitoshi Ogino, MD, Hitoshi Matsuda, MD, Hiroaki Sasaki, MD, Toshikatsu Yagihara, MD, and Soichiro
Surgical Management of Distal Arch Aneurysm: Another Approach With Improved Results Kenji Minatoya, MD, Hitoshi Ogino, MD, Hitoshi Matsuda, MD, Hiroaki Sasaki, MD, Toshikatsu Yagihara, MD, and Soichiro
Circulatory arrest (CA) is usually necessary for surgical correction of pathologic
 is usually necessary for surgical correction of pathologic") Surgical Techniques Mehmet Unal, MD Oguz Yilmaz, MD Ilker Akar, MD Ilker Ince, MD Cemal Aslan, MD Fatih Koc, MD Haluk Kafali, MD Key words: Aneurysm, dissecting/surgery; aortic aneurysm, thoracic/surgery;
Surgical Techniques Mehmet Unal, MD Oguz Yilmaz, MD Ilker Akar, MD Ilker Ince, MD Cemal Aslan, MD Fatih Koc, MD Haluk Kafali, MD Key words: Aneurysm, dissecting/surgery; aortic aneurysm, thoracic/surgery;
Endo-Bentall: Fact or Fiction?
 Endo-Bentall: Fact or Fiction? Eric E. Roselli, MD Chief, Adult Cardiac Surgery Surgical Director, Aorta Center Heart and Vascular Institute, Cleveland Clinic Disclosures Bolton Cook Cryolife Edwards Gore
Endo-Bentall: Fact or Fiction? Eric E. Roselli, MD Chief, Adult Cardiac Surgery Surgical Director, Aorta Center Heart and Vascular Institute, Cleveland Clinic Disclosures Bolton Cook Cryolife Edwards Gore
Hybrid repair of aortic arch aneurysms: a comprehensive review
 Review Article Hybrid repair of aortic arch aneurysms: a comprehensive review Steve Xydas 1, Christos G. Mihos 2, Roy F. Williams 1, Angelo LaPietra 1, Maurice Mawad 1, S. Howard Wittels 3, Orlando Santana
Review Article Hybrid repair of aortic arch aneurysms: a comprehensive review Steve Xydas 1, Christos G. Mihos 2, Roy F. Williams 1, Angelo LaPietra 1, Maurice Mawad 1, S. Howard Wittels 3, Orlando Santana
Lulu Liu, Chaoyi Qin, Jianglong Hou, Da Zhu, Bengui Zhang, Hao Ma, Yingqiang Guo
 Case Report One-stage hybrid surgery for acute Stanford type A aortic dissection with David operation, aortic arch debranching, and endovascular graft: a case report Lulu Liu, Chaoyi Qin, Jianglong Hou,
Case Report One-stage hybrid surgery for acute Stanford type A aortic dissection with David operation, aortic arch debranching, and endovascular graft: a case report Lulu Liu, Chaoyi Qin, Jianglong Hou,
Comparative Study of Cerebral Protection during Surgery of Thoracic Aortic Aneurysm
 Hiroshima J. Med. Sci. Vol.41, No.2, 31-35, June, 1992 HIJM 41-6 31 Comparative Study of Cerebral Protection during Surgery of Thoracic Aortic Aneurysm Taijiro SUEDA1), Takayuki NOMIMURA1), Tetsuya KAGA
Hiroshima J. Med. Sci. Vol.41, No.2, 31-35, June, 1992 HIJM 41-6 31 Comparative Study of Cerebral Protection during Surgery of Thoracic Aortic Aneurysm Taijiro SUEDA1), Takayuki NOMIMURA1), Tetsuya KAGA
Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology
 Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology Eduard Charchyan MD, PhD, Yurii Belov MD, PhD, Denis Breshenkov, Alexey
Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology Eduard Charchyan MD, PhD, Yurii Belov MD, PhD, Denis Breshenkov, Alexey
Luca Di Marco, Giacomo Murana, Alessandro Leone, Davide Pacini
 Viewpoint on Cardiac Surgery Page 1 of 6 Con debate: short circulatory arrest times in arch reconstructive surgery: is simple retrograde cerebral perfusion or hypothermic circulatory arrest as good or
Viewpoint on Cardiac Surgery Page 1 of 6 Con debate: short circulatory arrest times in arch reconstructive surgery: is simple retrograde cerebral perfusion or hypothermic circulatory arrest as good or
Cardiopulmonary Bypass for Thoracic Aortic Aneurysm: A Report on 488 Cases
 The Journal of The American Society of Extra-Corporeal Technology Cardiopulmonary Bypass for Thoracic Aortic Aneurysm: A Report on 488 Cases Yulong Guan, MD; Jing Yang, MD; Caihong Wan, MD; Meiling He;
The Journal of The American Society of Extra-Corporeal Technology Cardiopulmonary Bypass for Thoracic Aortic Aneurysm: A Report on 488 Cases Yulong Guan, MD; Jing Yang, MD; Caihong Wan, MD; Meiling He;
Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD
 Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD Foeke JH Nauta, MD, PhD Resident Cardiothoracic Surgery, Academic Medical Center, Amsterdam Disclosure
Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD Foeke JH Nauta, MD, PhD Resident Cardiothoracic Surgery, Academic Medical Center, Amsterdam Disclosure
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Treatment of acute type B aortic dissection: Current status
 MEET Cannes, 18. - 21.06.2009 Treatment of acute type B aortic dissection: Current status Christoph A. Nienaber, MD, FACC University of Rostock Department of Internal Medicine, Cardiology christoph.nienaber@med.uni-rostock.de
MEET Cannes, 18. - 21.06.2009 Treatment of acute type B aortic dissection: Current status Christoph A. Nienaber, MD, FACC University of Rostock Department of Internal Medicine, Cardiology christoph.nienaber@med.uni-rostock.de
Table I. Associated diseases
 Thoracic and thoracoabdominal aortic aneurysm repair using cardiopulmonary bypass, profound hypothermia, and circulatory arrest via left side of the chest incision Hazim J. Safi, MD, Charles C. Miller
Thoracic and thoracoabdominal aortic aneurysm repair using cardiopulmonary bypass, profound hypothermia, and circulatory arrest via left side of the chest incision Hazim J. Safi, MD, Charles C. Miller