Trans-Carotid Artery Revascularization
|
|
|
- Hilary Logan
- 5 years ago
- Views:
Transcription
1 Trans-Carotid Artery Revascularization How I do it John Rollo Clinical Assistant Professor University of Washington Vascular Surgery 6/15/2018
2 DISCLOSURE John Rollo, MD, RPVI Consultant / Advisory Board: Silk Road Medical Speakers Bureau: Silk Road Medical

3 A Victim of the Endovascular Revolution Lead shield Sweaty brow Leaded goggles Lead gown
4 What about cerebrovascular disease?
5 What about cerebrovascular disease? Over 135,000 carotid artery revascularizations per year 90% are performed on asymptomatic disease 11% are catheter-based interventional procedures
6 Choice of revascularization Carotid Endarterectomy (CEA) is safe and effective Carotid artery stenting (CAS) has some advantages
7 Choice of revascularization Some lesions are challenging to treat with CEA High ICA lesions Above C2 Higher risk anatomical Prior neck dissection (redo CEA) Radiation Contralateral ICA disease or occlusion Contralateral laryngeal nerve injury Tracheostomy

8 Trans-Femoral carotid stenting Lesion must be crossed before embolic protection is in place



 DeRubertis et al.")
9 Trans-Femoral carotid stenting Elderly (age >75) - Arch anatomy Strong correlation between age and aortic arch ROC (R 2 =0.60, p<0.0001) DeRubertis et al. SVS Annual Meeting 2013

 for")
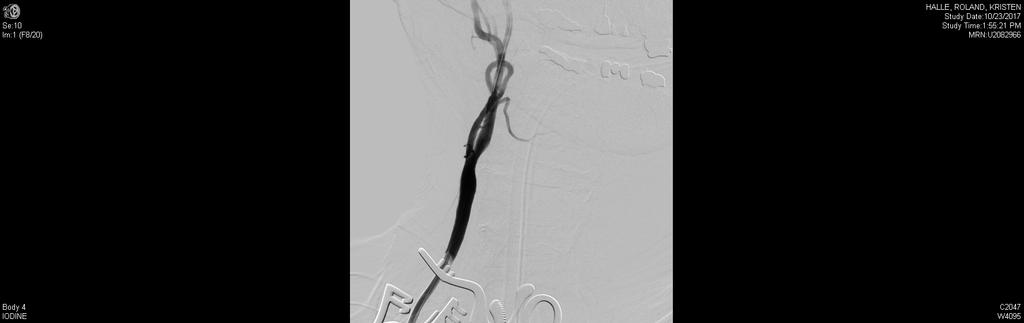
10 Trans-Carotid artery revascularization (TCAR) for high-risk carotid stenosis
11

12 VASCULAR AND ENDOVASCULAR SURGERY 4 weeks 2 weeks
13 Who is a TCAR candidate? Standard CMS coverage for CAS: Symptomatic high surgical risk with cervical carotid stenosis > 70%
14 Who is a TCAR candidate Requires registry data entry Symptomatic with cervical carotid stenosis > 50% ; Asymptomatic > 80% and one of the following: Physiologic high risk Age 75 CHF, EF 35% 2 diseased coronaries Unstable angina MI within 6 weeks Abnormal stress test Need for open heart surgery Need for major surgery (including vascular) Uncontrolled DM Severe Pulmonary disease Anatomic high risk Prior head or neck surgery Prior neck radiation Restenosis s/p CEA Surgically inaccessible lesion Laryngeal palsy Contralateral CN injury Contralateral ICA occlusion Tandem lesions Bilateral stenosis needing treatment.
15 Who is a TCAR candidate? Relative contraindications: Anatomy Clavicle to carotid bifurcation distance < 5cm Heavy calcium and plaque burden in the CCA Stenosis or occlusion of CCA Surgically inaccessible CCA
16 How I Do it: Patient selection 1. Everyone gets a CTA head + neck a. CCA origin evaluation b. Intracranial collateralization c. Tortuosity and accessibility of CCA d. Accurate clavicle CCA distance 2. Avoid heavy CCA disease 3. Assess anesthesia risk a. If low risk for GA and open contralateral ICA, do it 4. Be wary of severe COPD a. Pneumothorax is a risk! 5. Recent stroke, tolerance of flow reversal
17 How I Do it: Pre-operative management 1. Everyone gets dual anti-platelet + statin (minimum 5d pre-op) - Including ASA+Plavix morning of procedure 2. If on anticoagulation, hold prior to operation +/- bridge. 3. Standard pre-surgical preparation and labs 4. Medical pre-op evaluation for high risk medical patients. 5. Thorough neurovascular exam
18 How I Do it: Intra-operative management 1. Hybrid OR team 2. Standard CEA neck prep + bilateral groin prep 3. Propofol sedation for cut-down portion with local anesthesia +/- Cervical block 4. Keep a chest tube set up ready 5. TCAR time-out prior to CCA access - Adequately heparinized ACT > BP elevated - Glycopyrrolate 0.2mg IV - Neuro checks
19 Video!

20 Video!
21 How I Do it: Intra-operative management 6. Limited initial cervical angiogram - confirm lesion, ICA patency - mark the screen for sheath delivery 7. Insert sheath under fluoro - Stabilize the stiff wire and distal CCA - negative traction on the CCA with umbi tape 8. Initiate passive flow reversal and perform definitive cervical and intracranial angiograms 9. Clamp proximal CCA - repeat neuro checks - check flow reversal
22 How I Do it: Intra-operative management 10.Pre-dilate with a 3-4mm rapid exchange balloon 11.Stent sized to the CCA. - Enroute self-expanding open cell nontapered - Err on the side of too long - cover the external if needed 12. Post dilate if needed (typically 5mm) 13. One minute of flow reversal
23 How I Do it: Intra-operative management 14. Repeat cervical angiogram 15. Unclamp. Repeat intracranial angiograms 16. Neuro checks 17. Reverse heparin 18. Close platysma, skin. No drain
24 How I Do it: Post-operative management 1. ICU overnight 2. Arterial line with BP control 3. ASA + Plavix + Statin 4. Discharge POD 1
25 Roadster 2: Clinical Trial 1. Single arm, prospective observational study patients to be enrolled. - 70% of enrollees at new sites from R1 3. Inclusion: Asymptomatic > 80% stenosis, Symptomatic > 50% stenosis with at least one high risk criteria. Life expectancy > 3 years 4. Exclusion: stroke in evolution, proximal carotid stenosis or prior stent, alternative source of cerebral embolus (Afib).
26 Roadster 2: High Risk Criteria Parameter n=486 Age % Female 33.7% Symptomatic 24.9% Both Physiologic & Anatomic Risk Factors 26.8% Top 3 Physiologic Risk Factors Age 75 Years (17.9% as sole criterion) Hx of CAD ( 2 vessel disease) COPD Top 3 Anatomic Risk Factors High Cervical Stenosis Restenosis after CEA Hostile Neck 42.0% 14.7% 5.6% 25.4% 20.0% 17.0%
27 Roadster 2: Procedure Details Parameter ROADSTER 1 n=219 ROADSTER 2 n=486 ROADSTER 1 Operators 100% 17.9% New TCAR Operators 76.2% 82.1% Enrollment by New Operators 65.3% 70.0% Skin-to-Skin Time (median) 70 mins 69 mins Reverse Flow/Clamp Time (median) 9 mins 9 mins Tolerance to High Flow 98.6% 98.6% Tolerance to Low Flow 100% 100%
28 Roadster 2: Results in Surgical High Risk Patients Stroke/Death/MI ROADSTER 1 ROADSTER 2 n=203 n= % 6 1.4% Stroke 1 0.5% 3 0.7% 2 1.0% 1* 0.2% Death MI 3 1.5% 2 0.5% Stroke/Death 3 1.5% 4 0.9% Neurological Death CNI (permanent) 0 0.0% 0 0.0% 0 0.0% 0 0.0%
29 Conclusions TCAR provides a safe and effective method to treat symptomatic and asymptomatic patients with high grade stenosis who are at high risk for CEA Direct carotid access with high rate flow reversal allows for treatment of patients traditionally at increased risk for CAS (symptomatic, age 75)
30 Appendix A: Roadster 2 inclusion/exclusion Study Population Patients with atherosclerotic extracranial internal carotid stenosis (ICA) with or without involvement of the contiguous common artery (CCA) dete Symptomatic: greater than or equal to 50% stenosis or Asymptomatic: greater than or equal to 80% stenosis Criteria INCLUSION CRITERIA: Patient must meet one of the following criteria regarding neurological symptom status and degree of stenosis: Symptomatic: Stenosis must be >50% as determined by an angiogram and the patient has a history of stroke (minor or non-disabling; NIHSS 4 o OR Asymptomatic: Stenosis must be >80% as determined by angiogram without any neurological symptoms within the prior 180 days. Target vessel must meet all requirements for ENROUTE Transcarotid Neuroprotection System and ENROUTE Stent System (refer to IFU for requ Patient has a discrete lesion located in the internal carotid artery (ICA) with or without involvement of the contiguous common carotid artery (CCA Patient is 18 years of age. Patient understands the nature of the procedure and has provided a signed informed consent using a form that has been reviewed and approved b Patient is willing to comply with the protocol requirements and return to the treatment center for all required clinical evaluations. Patient must have a life expectancy 3 years at the time of the index procedure without contingencies related to other medical, surgical or endova Patient meets at least one of the surgical high-risk criteria listed below. Anatomic High Risk Inclusion Criteria: A. Contralateral carotid artery occlusion B. Tandem stenoses >70% C. High cervical carotid artery stenosis D. Restenosis after carotid endarterecto F. Hostile Necks which the Investigator deems safe for transcarotid access including but not limited to: I. Prior neck irradiation II. Radical neck dissection III. Cervical spine immobility Clinical High Risk Inclusion Criteria: G. Patient is > 75 years of age H. Patient has > 2-vessel coronary artery disease and history of angina of any severity I. Patient has a history of angi Canadian Cardiovascular Society (CCS) angina class 3 or 4 or unstable angina J. Patient has congestive heart failure (CHF) - New York Heart Association (NYHA) Functional Class III or IV K. Patient has known severe left ventricular dysfunction LVEF <30%. L. Patient has had a myocardial infarction > 72 hours and < 6 weeks prior to procedure. M. Patient has severe pulmonary disease (COPD) with either: FEV1 <50% predicted or chronic oxygen therapy or resting PO2 of <60 mmhg (room air) N. Patient has permanent contralateral cranial nerve injury O. Patient has chronic renal insufficiency (serum creatinine > 2.5 mg/dl). REMINDER: The following is a list of anatomical considerations that are not suitable for transfemoral CAS with distal protection that are NOT con I. TypeII, III, or Bovine arch II. Arch atheroma or calcification III. Atheroma of the great vessel origins IV. Tortuous distal ICA V. Tortuous or occl
31 Appendix B: Roadster 1 Exclusion Criteria for TCAR ROADSTER 1 trial Afib; recent valve or MI; bleeding Evolving stroke; neuro disorders Occlusion; ostial CCA or intracranial stenosis; string sign; previous stent CCA disease at entry site <5cm clavicle to bifurcation
32 References 1. Ricotta, J.J., Aburahma, A., Ascher, E., Eskandari, M., Faries, P., Lal, B.K., and Society for Vascular Surgery. Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease. ([Erratum in: J Vasc Surg 2012;55:894])J Vasc Surg. 2011; 54: e1 e31 2. North American Symptomatic Carotid Endarterectomy Trial Collab- orators (NASCET). Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North Ameri- can Symptomatic Carotid Endarterectomy Trial Collaborators N Engl J Med 1991;325: Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al. Benefit of carotid endarterectomy in patients with symptom- atic moderate or severe stenosis. North American Symptomatic Ca- rotid Endarterectomy Trial Collaborators. N Engl J Med 1998;339: Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet 1998;351: J Vasc Surg Nov;54(5): doi: /j.jvs Epub 2011 Jun Kwolek CJ, Jaff MR, Leal JI, Hopkins LN, Shah RM, Hanover TM, Macdonald S, Cambria RP. Results of the ROADSTER multicenter trial of transcarotid stenting with dynamic flow reversal. J Vasc Surg Nov;62(5): doi: /j.jvs PubMed PMID:
ROADSTER 2. SPONSOR: Silk Road Medical
 ROADSTER 2 CONDITION: Carotid artery disease PI: Jessica Titus, MD CONTACT INFO: Jo Anne Goldman JoAnne.Goldman@allina.com 612-863-3793 DESCRIPTION: The study is intended to evaluate real world usage of
ROADSTER 2 CONDITION: Carotid artery disease PI: Jessica Titus, MD CONTACT INFO: Jo Anne Goldman JoAnne.Goldman@allina.com 612-863-3793 DESCRIPTION: The study is intended to evaluate real world usage of
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS
 TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS Assistant Professor of Surgery Director of Carotid Interventions Division of Vascular & Endovascular Surgery Stony Brook University
TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS Assistant Professor of Surgery Director of Carotid Interventions Division of Vascular & Endovascular Surgery Stony Brook University
CardioLucca2014. Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee. Fabrizio Tomai
 CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
Surgical Treatment of Carotid Disease
 Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy
 13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
Carotid Artery Stenting
 Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Technical Tips for Safe, Effective TCAR with the ENROUTE System (Silk Road Medical): When is the Procedure Contraindicated
: When is the Procedure Contraindicated") Technical Tips for Safe, Effective TCAR with the ENROUTE System (Silk Road Medical): When is the Procedure Contraindicated William A Gray MD Lankenau Heart Institute Wynnewood PA USA Addressing an Unmet
Technical Tips for Safe, Effective TCAR with the ENROUTE System (Silk Road Medical): When is the Procedure Contraindicated William A Gray MD Lankenau Heart Institute Wynnewood PA USA Addressing an Unmet
Carotid Artery Stenting (CAS) Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA
 Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA") Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
THE CASE FOR TCAR UNDER LOCAL ANESTHESIA. Sumaira Macdonald MD, PhD Vascular Interventional Radiologist & Chief Medical Officer, Silk Road Medical
 THE CASE FOR TCAR UNDER LOCAL ANESTHESIA Sumaira Macdonald MD, PhD Vascular Interventional Radiologist & Chief Medical Officer, Silk Road Medical MUNICH VASCULAR COURSE DECEMBER 2017 1 TCAR EQUIPMENT SUITE
THE CASE FOR TCAR UNDER LOCAL ANESTHESIA Sumaira Macdonald MD, PhD Vascular Interventional Radiologist & Chief Medical Officer, Silk Road Medical MUNICH VASCULAR COURSE DECEMBER 2017 1 TCAR EQUIPMENT SUITE
Carotid Artery Stent: Is it ready for prime time?
 2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Prevention and Management of Cardiac Adverse Event
 Prevention and Management of Cardiac Adverse Event Carlo Cernetti Department of Interventional Cardiology Mirano (Italy) Cannes MEEC 14 June 2007 Are these risks factors of Haemodynamic Instability
Prevention and Management of Cardiac Adverse Event Carlo Cernetti Department of Interventional Cardiology Mirano (Italy) Cannes MEEC 14 June 2007 Are these risks factors of Haemodynamic Instability
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective)
") Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Assessment of the procedural etiology of stroke resulting from carotid artery stenting
 Assessment of the procedural etiology of stroke resulting from carotid artery stenting 1. Study Purpose and Rationale: A. Background Stroke is the 3 rd leading cause of death in the United States and carries
Assessment of the procedural etiology of stroke resulting from carotid artery stenting 1. Study Purpose and Rationale: A. Background Stroke is the 3 rd leading cause of death in the United States and carries
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Tips and Tricks for CAS T-CAR
 Tips and Tricks for CAS T-CAR H.-H. Eckstein, M. Kallmayer Department for Vascular and Endovascular Surgery, Klinikum Rechts der Isar, Technical University of Munich,, Germany Disclosures Collaborator
Tips and Tricks for CAS T-CAR H.-H. Eckstein, M. Kallmayer Department for Vascular and Endovascular Surgery, Klinikum Rechts der Isar, Technical University of Munich,, Germany Disclosures Collaborator
Octogenarians Must Be Treated With CAS
 Some Octogenarians Must Be Treated With CAS LN Hopkins, MD E Levy MD, Adnan Siddiqui,, MD, PhD Rod Samuelson MD J Mocco MD LN Hopkins, MD Potential Conflicts Consultant & research support: Boston Scientific,
Some Octogenarians Must Be Treated With CAS LN Hopkins, MD E Levy MD, Adnan Siddiqui,, MD, PhD Rod Samuelson MD J Mocco MD LN Hopkins, MD Potential Conflicts Consultant & research support: Boston Scientific,
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
CAROTID ARTERY STENTING TECHNICALS ASPECTS. Symposium Abbott Vascular CANNES MEET 2008 Drs V PIRET, P BERGERON
 CAROTID ARTERY STENTING TECHNICALS ASPECTS Symposium Abbott Vascular CANNES MEET 2008 Drs V PIRET, P BERGERON POINTS TO DISCUSS TO CAS INDICATIONS CONTRA INDICATIONS ANATOMICAL CONSIDERATION TECHNICS CAS
CAROTID ARTERY STENTING TECHNICALS ASPECTS Symposium Abbott Vascular CANNES MEET 2008 Drs V PIRET, P BERGERON POINTS TO DISCUSS TO CAS INDICATIONS CONTRA INDICATIONS ANATOMICAL CONSIDERATION TECHNICS CAS
DESPITE CURRENT LEVEL 1 EVIDENCE THE OUTLOOK FOR AN UPSURGE IN CAROTID STENTING (CAS) IS BRIGHT FRANK J. VEITH LINC LEIPZIG JANUARY 27, 2015
 IS BRIGHT FRANK J. VEITH LINC LEIPZIG JANUARY 27, 2015") DESPITE CURRENT LEVEL 1 EVIDENCE THE OUTLOOK FOR AN UPSURGE IN CAROTID STENTING (CAS) IS BRIGHT FRANK J. VEITH LINC - 2015 LEIPZIG JANUARY 27, 2015 Disclosure Speaker name: FRANK J. VEITH DESPITE SOME
DESPITE CURRENT LEVEL 1 EVIDENCE THE OUTLOOK FOR AN UPSURGE IN CAROTID STENTING (CAS) IS BRIGHT FRANK J. VEITH LINC - 2015 LEIPZIG JANUARY 27, 2015 Disclosure Speaker name: FRANK J. VEITH DESPITE SOME
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
Transcervical carotid stenting:
 Transcervical carotid stenting: Patient selection, techniques, & results Peter A. Schneider, MD Kaiser Hospital and Hawaii Permanente Medical Group Honolulu, Hawaii DISCLOSURE Peter A. Schneider Enter
Transcervical carotid stenting: Patient selection, techniques, & results Peter A. Schneider, MD Kaiser Hospital and Hawaii Permanente Medical Group Honolulu, Hawaii DISCLOSURE Peter A. Schneider Enter
FRANK J. VEITH MAC TH MUNICH VASCULAR CONF
 UPDATE ON THE NORTH AMERICAN RCTs CREST 2 & ACST 1: WILL CAS SURVIVE AS AN ALTERNATIVE TO BMT OR CEA? FRANK J. VEITH 6 TH MUNICH VASCULAR CONF MAC - 2016 MUNICH DECEMBER 1, 2016 I HAVE NO FINANCIAL CONFLICTS
UPDATE ON THE NORTH AMERICAN RCTs CREST 2 & ACST 1: WILL CAS SURVIVE AS AN ALTERNATIVE TO BMT OR CEA? FRANK J. VEITH 6 TH MUNICH VASCULAR CONF MAC - 2016 MUNICH DECEMBER 1, 2016 I HAVE NO FINANCIAL CONFLICTS
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
Carlo Setacci Chief Department of Surgery Vascular and Endovascular Unit University of Siena
 Which carotid procedures are required to grade the stroke risk? Carlo Setacci Chief Department of Surgery Vascular and Endovascular Unit University of Siena Faculty disclosure Carlo Setacci I have no financial
Which carotid procedures are required to grade the stroke risk? Carlo Setacci Chief Department of Surgery Vascular and Endovascular Unit University of Siena Faculty disclosure Carlo Setacci I have no financial
CAROTID ARTERY ANGIOPLASTY
 CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
Carotid stenosis management: CAS or CEA? Yaoguo Yang, Chen Zhong Beijing Anzhen Hospital,China
 Carotid stenosis management: CAS or CEA? Yaoguo Yang, Chen Zhong Beijing Anzhen Hospital,China Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting Employment
Carotid stenosis management: CAS or CEA? Yaoguo Yang, Chen Zhong Beijing Anzhen Hospital,China Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting Employment
CAROTID ANGIOPLASTY AND STENTING UNDER PROTECTION IS BECOMING THE GOLD STANDARD TREATMENT IN HIGH AND LOW RISK PATIENTS
 CAROTID ANGIOPLASTY AND STENTING UNDER PROTECTION IS BECOMING THE GOLD STANDARD TREATMENT IN HIGH AND LOW RISK PATIENTS M. HENRY* MD, I. HENRY MD A. POLYDOROU MD, A.D. POLYDOROU MD M. HUGEL RN NANCY FRANCE
CAROTID ANGIOPLASTY AND STENTING UNDER PROTECTION IS BECOMING THE GOLD STANDARD TREATMENT IN HIGH AND LOW RISK PATIENTS M. HENRY* MD, I. HENRY MD A. POLYDOROU MD, A.D. POLYDOROU MD M. HUGEL RN NANCY FRANCE
Internal carotid artery near-total occlusions: Is it justified to operate on them?
 Internal carotid artery near-total occlusions: Is it justified to operate on them? Christos D. Liapis Professor (Em) of Vascular Surgery Athens University Medical School Director Vascular & Endovascular
Internal carotid artery near-total occlusions: Is it justified to operate on them? Christos D. Liapis Professor (Em) of Vascular Surgery Athens University Medical School Director Vascular & Endovascular
SCAFFOLD Study Gore PTFE mesh-covered stent preclinical and clinical data so far. Peter A. Schneider, MD Kaiser Foundation Hospital Honolulu, Hawaii
 SCAFFOLD Study Gore PTFE mesh-covered stent preclinical and clinical data so far Peter A. Schneider, MD Kaiser Foundation Hospital Honolulu, Hawaii Disclosure Peter A. Schneider... I have the following
SCAFFOLD Study Gore PTFE mesh-covered stent preclinical and clinical data so far Peter A. Schneider, MD Kaiser Foundation Hospital Honolulu, Hawaii Disclosure Peter A. Schneider... I have the following
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Carotid Artery Stenting Today: A Few Updating Remarks
 Carotid Artery Stenting Today: A Few Updating Remarks Camilo R. Gomez, MD, MBA Director, Alabama Neurological Institute Birmingham, Alabama Disclaimer & Warning Company Pharmaceutical BMS-Sanofi-Aventis
Carotid Artery Stenting Today: A Few Updating Remarks Camilo R. Gomez, MD, MBA Director, Alabama Neurological Institute Birmingham, Alabama Disclaimer & Warning Company Pharmaceutical BMS-Sanofi-Aventis
Open heart surgery or carotid endarterectomy. Which procedure should be done first?
 Open heart surgery or carotid endarterectomy. Which procedure should be done first? Pedro Pinto Sousa 1, Gabriela Teixeira 2, João Gonçalves 2 ; Luís Vouga 1, Rui Almeida 2 ; Pedro Sá Pinto 2 1 Centro
Open heart surgery or carotid endarterectomy. Which procedure should be done first? Pedro Pinto Sousa 1, Gabriela Teixeira 2, João Gonçalves 2 ; Luís Vouga 1, Rui Almeida 2 ; Pedro Sá Pinto 2 1 Centro
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Fast-track CEA: a 3-year experience
 Fast-track CEA: a 3-year experience Giorgio L. Poletto, MD Milano, Italy 6th ACST-2 Collaborators Meeting, Palau de Congresos, Valencia. 24th and 25th September 2018. Stroke prevention Primary prevention:
Fast-track CEA: a 3-year experience Giorgio L. Poletto, MD Milano, Italy 6th ACST-2 Collaborators Meeting, Palau de Congresos, Valencia. 24th and 25th September 2018. Stroke prevention Primary prevention:
PCI for Renal Artery stenosis
 PCI for Renal Artery stenosis Why should we treat Renal Artery Stenosis? Natural History of RAS RAS is progressive disease Study Follow-up (months) Pts Progression N (%) Total occlusion Wollenweber Meaney
PCI for Renal Artery stenosis Why should we treat Renal Artery Stenosis? Natural History of RAS RAS is progressive disease Study Follow-up (months) Pts Progression N (%) Total occlusion Wollenweber Meaney
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Current Non-Surgical Cardiac Interventions. By Pam Bayles, RN, BSN
 Current Non-Surgical Cardiac Interventions By Pam Bayles, RN, BSN Balloon Angioplasty & DES A balloon-tipped catheter was first used in 1964 to treat a cause of atherosclerotic disease in a patient s leg
Current Non-Surgical Cardiac Interventions By Pam Bayles, RN, BSN Balloon Angioplasty & DES A balloon-tipped catheter was first used in 1964 to treat a cause of atherosclerotic disease in a patient s leg
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Carotid Artery Disease How the Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient
 Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.
 Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Corporate Medical Policy
 Corporate Medical Policy Endovascular Therapies for Extracranial Vertebral Artery Disease File Name: Origination: Last CAP Review: Next CAP Review: Last Review: endovascular_therapies_for_extracranial_vertebral_artery_disease
Corporate Medical Policy Endovascular Therapies for Extracranial Vertebral Artery Disease File Name: Origination: Last CAP Review: Next CAP Review: Last Review: endovascular_therapies_for_extracranial_vertebral_artery_disease
Endovascular vs Surgical Carotid Revascularisation
 Endovascular vs Surgical Carotid Revascularisation Lessons Learned from Clinical Trials and How I Approach it in My Practice Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor of Vascular Surgery
Endovascular vs Surgical Carotid Revascularisation Lessons Learned from Clinical Trials and How I Approach it in My Practice Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor of Vascular Surgery
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Stenting Versus
 Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
PrOspective multicenter study of carotid artery stenting Usinng mer Stent OCEANUS study!!!
 PrOspective multicenter study of carotid artery stenting Usinng mer Stent OCEANUS study!!! Prof Piotr Pieniazek MD PhD Jagiellonian University Institute of Cardiology, John Paul II Hospital Krakow, Poland
PrOspective multicenter study of carotid artery stenting Usinng mer Stent OCEANUS study!!! Prof Piotr Pieniazek MD PhD Jagiellonian University Institute of Cardiology, John Paul II Hospital Krakow, Poland
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Overview of Subclavian & Innominate Artery Interventions
 TCT 2016 Washington, DC, USA Tuesday November 1st, 2016 Peripheral vascular interventions Overview of Subclavian & Innominate Artery Interventions Dr Jacques Busquet Vascular & Endovascular Surgery Paris,
TCT 2016 Washington, DC, USA Tuesday November 1st, 2016 Peripheral vascular interventions Overview of Subclavian & Innominate Artery Interventions Dr Jacques Busquet Vascular & Endovascular Surgery Paris,
Roadsaver the paradigm shift in carotid artery treatment. G. Torsello Münster
 Roadsaver the paradigm shift in carotid artery treatment G. Torsello Münster Disclosure Speaker name:...g. Torsello... I have the following potential conflicts of interest to report: Consulting Employment
Roadsaver the paradigm shift in carotid artery treatment G. Torsello Münster Disclosure Speaker name:...g. Torsello... I have the following potential conflicts of interest to report: Consulting Employment
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
Approach to Intervention in Carotid Artery Disease. Kenneth Rosenfield, M.D. Section Head Vascular Medicine and Intervention MGH Boston, MA
 Approach to Intervention in Carotid Artery Disease Kenneth Rosenfield, M.D. Section Head Vascular Medicine and Intervention MGH Boston, MA Kenneth Rosenfield, MD Additional Disclosure I am a Carotid Stentor,
Approach to Intervention in Carotid Artery Disease Kenneth Rosenfield, M.D. Section Head Vascular Medicine and Intervention MGH Boston, MA Kenneth Rosenfield, MD Additional Disclosure I am a Carotid Stentor,
DESCRIPTION: Percent of asymptomatic patients undergoing CEA who are discharged to home no later than post-operative day #2
 Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
proximal protection with the MO.ma device during carotid stenting
 proximal protection with the MO.ma device during carotid stenting Robert M. Bersin, MD, MPH, FACC, FSCAI Medical Director, Endovascular Services Seattle Cardiology and Swedish Medical Center -1- proximal
proximal protection with the MO.ma device during carotid stenting Robert M. Bersin, MD, MPH, FACC, FSCAI Medical Director, Endovascular Services Seattle Cardiology and Swedish Medical Center -1- proximal
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
More than strokes occur
 Surgery vs Stent: Treatment for Carotid Artery Disease Imad A. Alhaddad, MD ABSTRACT PURPOSE: This article summarizes and compares the roles of surgery and stent in the management of carotid artery disease.
Surgery vs Stent: Treatment for Carotid Artery Disease Imad A. Alhaddad, MD ABSTRACT PURPOSE: This article summarizes and compares the roles of surgery and stent in the management of carotid artery disease.
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
SCAI Fall Fellows Course Subclavian/Innominate Case Presentation
 SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
Approach to the Patient with Carotid Artery Disease
 Approach to the Patient with Carotid Artery Disease Michael R. Jaff, DO, FACP, FACC Director, Vascular Medicine Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Statement Within
Approach to the Patient with Carotid Artery Disease Michael R. Jaff, DO, FACP, FACC Director, Vascular Medicine Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Statement Within
GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY
 GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY Full Title of Guideline: Author (include email and role): Guideline for Recovery Room Management of Patients after Carotid
GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY Full Title of Guideline: Author (include email and role): Guideline for Recovery Room Management of Patients after Carotid
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
NCDR CARE Registry Carotid Artery Revascularization and Endarterectomy Registry Carotid Artery Stenting Form v1.09
 NCDR CARE Registry Carotid Artery Revascularization and Endarterectomy Registry Carotid Artery Stenting Fm v1.09 A. PARTICIPANT ADMINISTRATION Participant ID 1000 : Participant Name 1010 : Medicare Provider
NCDR CARE Registry Carotid Artery Revascularization and Endarterectomy Registry Carotid Artery Stenting Fm v1.09 A. PARTICIPANT ADMINISTRATION Participant ID 1000 : Participant Name 1010 : Medicare Provider
CAROTID ARTERY ANGIOPLASTY
 CAROTID ARTERY ANGIOPLASTY Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
CAROTID ARTERY ANGIOPLASTY Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
Issam D. Moussa, MD. Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, FL
 Carotid Technologies and Protection Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, FL Disclosure Statement
Carotid Technologies and Protection Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, FL Disclosure Statement
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease
 The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device
 Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device Luis A. Sanchez MD Gregorio A. Sicard Distinguished Professor of Surgery & Radiology Chief, Section of Vascular Surgery
Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device Luis A. Sanchez MD Gregorio A. Sicard Distinguished Professor of Surgery & Radiology Chief, Section of Vascular Surgery
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Techniques for Carotid Interventon
 Techniques for Carotid Interventon Jay S. Yadav MD Cleveland, Ohio Disclosures Inventor of Angioguard; fixed and recurring payments from JNJ Advisor: JNJ, Guidant Understand the Patient What is the Cause
Techniques for Carotid Interventon Jay S. Yadav MD Cleveland, Ohio Disclosures Inventor of Angioguard; fixed and recurring payments from JNJ Advisor: JNJ, Guidant Understand the Patient What is the Cause
Update on Carotid Disease
 Update on Carotid Disease L. Nelson Hopkins, MD Elad Levy, MD Adnan Siddiqui, MD,PhD Ken Snyder, MD,PhD Gates Vascular Institute LN Hopkins, MD I disclose the following financial relationship(s): President,
Update on Carotid Disease L. Nelson Hopkins, MD Elad Levy, MD Adnan Siddiqui, MD,PhD Ken Snyder, MD,PhD Gates Vascular Institute LN Hopkins, MD I disclose the following financial relationship(s): President,
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough
 Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
2/28/2010. Speakers s name: Paul Chiam. I have the following potential conflicts of interest to report: NONE. Antegrade transvenous transseptal route
 Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Update on Carotid Stenting. John R. Laird Cardiovascular Research Institute Washington Hospital Center
 Update on Carotid Stenting John R. Laird Cardiovascular Research Institute Washington Hospital Center Carotid Stenting What a Crazy Idea! Pathogenesis of stroke Does it make sense to think that expansion
Update on Carotid Stenting John R. Laird Cardiovascular Research Institute Washington Hospital Center Carotid Stenting What a Crazy Idea! Pathogenesis of stroke Does it make sense to think that expansion
Contemporary management of brachiocephalic occlusive disease. TM Sullivan Minneapolis, MN
 Contemporary management of brachiocephalic occlusive disease TM Sullivan Minneapolis, MN WL Gore & Associates Disclosures Meeting organizer (SOAR) CR Bard Chair, CEC Bolster trial Veryan National PI, MIMICS
Contemporary management of brachiocephalic occlusive disease TM Sullivan Minneapolis, MN WL Gore & Associates Disclosures Meeting organizer (SOAR) CR Bard Chair, CEC Bolster trial Veryan National PI, MIMICS
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Management of combined coronary & carotid disease
 Management of combined coronary & carotid disease Combined Carotid and coronary artery diseases Frequent combination Fear of imminent death psychologically traumatic for the patients and their families
Management of combined coronary & carotid disease Combined Carotid and coronary artery diseases Frequent combination Fear of imminent death psychologically traumatic for the patients and their families
New concepts for filter protection during CAS: double filtration. Alberto Cremonesi MD, FESC
 New concepts for filter protection during CAS: double filtration Alberto Cremonesi MD, FESC First Experience with the PALADIN Carotid Post-Dilation Balloon with Integrated Embolic Protection Alberto Cremonesi
New concepts for filter protection during CAS: double filtration Alberto Cremonesi MD, FESC First Experience with the PALADIN Carotid Post-Dilation Balloon with Integrated Embolic Protection Alberto Cremonesi
Review of clinical carotid stent procedural & long-term outcomes in. symptomatic asymptomatic. patients
 Review of clinical carotid stent procedural & long-term outcomes in symptomatic asymptomatic patients 1 Conflict of Interest Statement Within the past 12 months, I or my spouse have had a financial interest/arrangement
Review of clinical carotid stent procedural & long-term outcomes in symptomatic asymptomatic patients 1 Conflict of Interest Statement Within the past 12 months, I or my spouse have had a financial interest/arrangement
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
Decision Memo for Percutaneous Transluminal Angioplasty (PTA) of the Carotid Artery Concurrent with Stenting (CAG-00085R6)
 of the Carotid Artery Concurrent with Stenting (CAG-00085R6)") Decision Memo for Percutaneous Transluminal Angioplasty (PTA) of the Carotid Artery Concurrent with Stenting (CAG-00085R6) Decision Memo TO: FROM: Administrative File:CAG-00085R6 Percutaneous Transluminal
Decision Memo for Percutaneous Transluminal Angioplasty (PTA) of the Carotid Artery Concurrent with Stenting (CAG-00085R6) Decision Memo TO: FROM: Administrative File:CAG-00085R6 Percutaneous Transluminal
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Surgical Procedures for. Symptomatic Post-CAS Carotid. Restenosis: Experiences and. Mid-Term Outcomes. Lefeng Qu M.D., Ph.D. Professor of Surgery
 Surgical Procedures for Symptomatic Post-CAS Carotid Restenosis: Experiences and Mid-Term Outcomes Lefeng Qu M.D., Ph.D. Professor of Surgery Department of Vascular and Endovascular Surgery, Changzheng
Surgical Procedures for Symptomatic Post-CAS Carotid Restenosis: Experiences and Mid-Term Outcomes Lefeng Qu M.D., Ph.D. Professor of Surgery Department of Vascular and Endovascular Surgery, Changzheng