Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
|
|
|
- Raymond Parker
- 5 years ago
- Views:
Transcription
1 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1
2 Objectives Definition Why the urgency? Evidence/Guidelines for symptomatic carotid disease (BP, antithrombotics, CEA/CUS) Special situations: Role of heparin Role of acute endovascular management CEA/CUS in women, elderly, while on DAP, with disabling stroke, timing 2
3 Case 58 year-old right-handed woman woke up with new left-sided weakness. PMHX: Diabetes, Hypertension, Hyperlipidemia, TIA 2 years ago. SHX: No bad habits. Home Meds: ASA 81mg daily. No statin. Exam: BP 160/90, CN intact. Left hand and entire leg strength 4/5. Walks without support. Labs: LDL 122, A1c 7.0 3
4 Case: 58yo with left-sided weakness CT/H without acute changes CTA with R ICA 80% stenosis (NASCET criteria), L ICA < 50%, and diffuse mild atherosclerotic disease. Next steps? 4
5 Case: 58yo with left-sided weakness MRI with peri-rolandic R frontal ischemic stroke, about 10 cc in volume. Started on aspirin 81mg daily and clopidogrel 75mg daily Admitted to the neurology floor with acute ischemic stroke order set and frequent neuro checks. Next steps? 5
6 What is the urgency? Why close monitoring, further diagnostics and urgency of intervention? 6
7 Risk of recurrent TIA/stroke after event is front loaded. > 2000 pts with ischemic stroke. Of those, > 500 with prior TIA events. Of strokes preceded by TIA, 43% of strokes happened in first 7 days after TIA. Third of those happened on the day of stroke! Timing of TIAs preceding stroke: Time window for prevention is very short. Neurology Timing of TIAs preceding stroke: Time window for prevention is very short. Neurology
8 The second event was disabling or fatal in half of these patients. Fairhead JF, Mehta Z, Rothwell PM. Population-based study of delays in carotid imaging and surgery and the risk of recurrent stroke. Neurology. 2005;65:
9 Risk of stroke in the hyperacute period after the index TIA in patients with 50 99% carotid stenosis compared with pooled data from the randomized trials. 48 h 72 h 7 d 14 d 5 y ESCT + NASCET + VA (medical therapy) 2 21% Fairhead et al. (2005) 29 20% Purroy et al. (2007) 30 10% Ois et al. (2009) 31 17% 22% 25% Bonifati et al. (2011) 32 8% Johansson et al. (2013) 33 5% 8% 11% Merwick et al. (2013) 34 8% Marnane et al. (2014) 35 5% 9% 9% 16% b Source: Naylor, European Journal of Vascular and Endovascular Surgery June

10 Why is early stroke risk high? CEA performed < 4 weeks of index TIA > 4 weeks Thrombus overlying plaque 66% 21% Naylor, Review Time is Brain 2015; [Harrison, Marshall 1977] 10
11 However, not everyone with TIA or minor stroke ends up with a stroke. Can high-risk patients be identified? Would they be treated differently? 11
12 Transcranial doppler Prevalence of spontaneous emboli on TCD after symptom onset: 42% of patients in < 7 days 22% 8-14 days 16% > 14 days Salem MK, Sayers RD, Bown MJ, Naylor AR. Spontaneous embolisation in asymptomatic and acutely symptomatic patients with TIA/ minor stroke. Eur J Vasc Endovasc Surg 2011;41:

 No signal hyperintensity.")
13 MRI of carotid plaque Axial views of T1-weighted water-selective magnetic resonance imaging to detect plaque hemorrhage of carotid arteries. Hyperintense signals (B D, white arrows) reflect plaque hemorrhage in carotid arteries, black arrows (A) show absence of plaque hemorrhage, and asterisks indicate the lumen of internal carotid artery. (A) No signal hyperintensity. (B) Large moderately hyperintense plaque. (C) Small strongly hyperintense plaque. (D) Large strongly hyperintense plaque. 13

14 Intraplaque hemorrhage predicts outcome Hosseini et al: Carotid Plaque Hemorrhage
15 Management 15
16 Blood pressure Current consensus guidelines recommend treating BP > 220/120 mmhg unless patient has received thrombolytic therapy in which case the maximum permitted BP is 185/110 mmhg. However, hyperacute post-stroke BP often has to be individualized. 16
17 Anti-platelet therapy ASA + Clopidogrel > 50% reduction in microemboli POINT trial ongoing. SOCRATES trial ticagrelor 90mg BID vs ASA 100mg QD after stroke/tia with no significant benefit. However, subgroup analysis showed benefit if ipsilateral carotid disease. Ischemic CVA, MI, Death Ischemic CVA SOCRATES, Lancet
18 TARDIS Anti-platelet triple therapy no benefit over dual therapy More bleeding POINT trial for further data on DAPT The Triple Antiplatelets for Reducing Dependency in Ischemic Stroke (TARDIS) trial,
19 Case: 58yo with left-sided weakness Additional diagnostics TCD w/ emboli monitoring Carotid ultrasound/mri to characterize the carotid plaque Additional management CEA/CAS Heparin gtt 19
20 CEA 20

21 CEA - Timing Naylor, Review Time is Brain 21


22 CEA - Gender Naylor, Review Time is Brain 22
23 CEA Most of the data is based on old medical therapy, TIA/minor stroke and high peri-procedural risk. Current guidelines recommend periprocedural risk of stroke/death < 6% for symptomatic carotid stenosis. Suggested that this be lowered to < 2%. Favors medical mgmt. Favors surgery Sex Female Male Lesion Smooth Ulcerated Sx type Retinal Hemispheric Collaterals Present Absent Comorbidity Present Absent Chaturvedi S, Emergency Medicine
24 Hyperacute CEA How early can we safely do CEA? 24
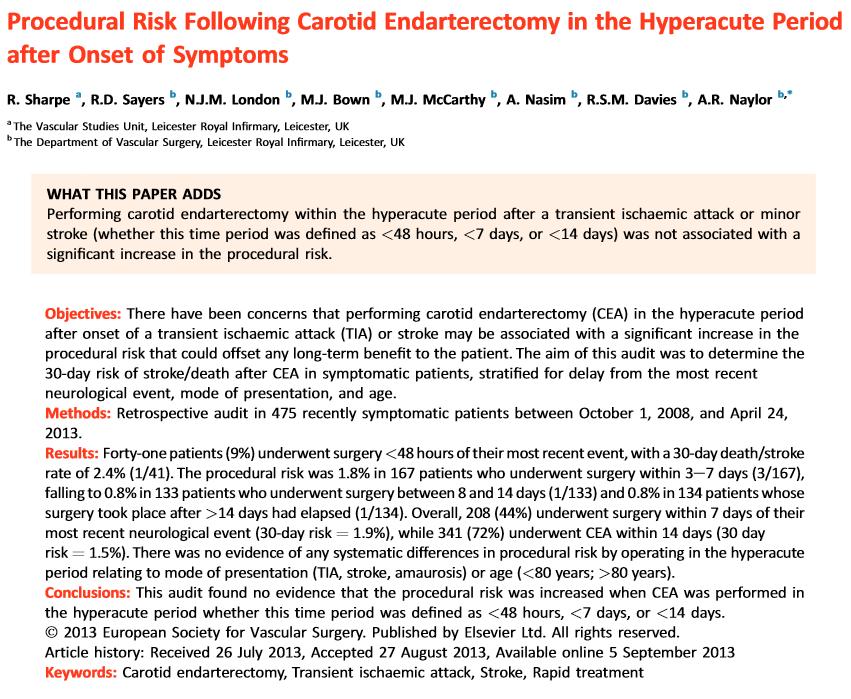
25 Procedural risk of CEA w.r.t. to timing [15 SwedVasc Registry] Very urgent carotid endarterectomy confers increased procedural risk Stroke, 43 (2012), pp [16] Procedural risk following carotid endarterectomy in the hyperacute period after onset of symptoms Eur J Vasc Endovasc Surg, 46 (2013), pp [17] Very urgent carotid endarterectomy does not increase the procedural risk Eur J Vasc Endovasc Surg, 49 (2015), pp
26 26
27 Why lower procedural risk in Leicester study? we attributed our very low procedural risks to an obsessional attention to surgical technique, completion angioscopy/intraoperative TCD, peri-operative dual antiplatelet therapy and written guidelines for treating post-cea hypertension. 27
28 CEA - Elderly Depends on life expectancy. There is post-operative risk and that benefit recouped over the years. However, if they are not alive long, then that benefit cannot be recuperated. 28
29 Debatable Heparin for acute ischemic stroke Severe stroke patients excluded form trials. Would they benefit from intervention? 29
30 Case 75 year old woman with no PMHx woke up with left side weakness. On exam: Left hemiparesis and neglect EKG: normal Symptoms: progressing What antithrombotic medication would you want to use acutely? 30
31 Aspirin 31
32 Heparin 32
33 33

34 Miller Fisher: The Master of Clinicopathologic Correlation. Interview Trobe, Jonathan D. MD JDT: And weren t you responsible for introducing the idea of anticoagulation in TIAs and large extracranial artery stenosis? CMF: Yes. The first patient I anticoagulated with heparin had basilar TIAs. We d turn on the heparin and the TIAs would stop, turn it off and they d start up again. I set up the first anticoagulation trial. Seven centers cooperated. We had so many fatal bleeding accidents that it appeared unlikely that a benefit could be shown. Miller_Fisher The_Master_of_Clinicopathologic.14.aspx 34
35 Multiple trials in use of heparin IST (unfractionated sq heparin) TOAST (danaproid) FisBis (fraxiparin) HAEST (dalteparin) NO overall benefit. 35
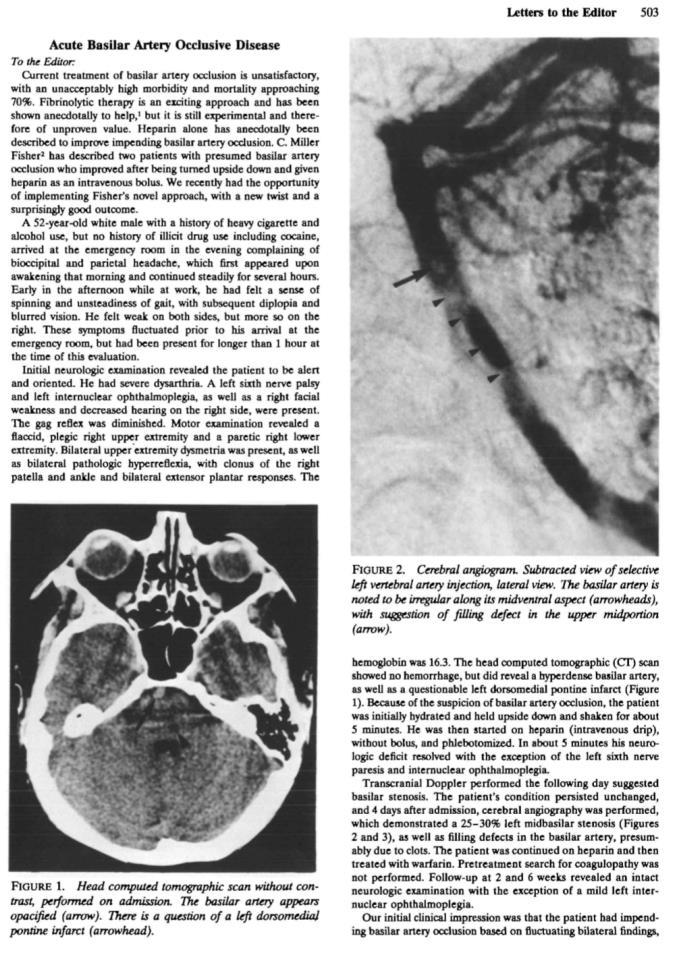
36 Anticoagulation for acute ischemic stroke Guidelines do not support routine use of anticoagulation post-stroke. However, experts consider it in : Conditions with potential high risk of early cardiogenic reembolization Symptomatic dissection of the arteries supplying the brain Symptomatic extracranial or intracranial arteriosclerotic stenosis with crescendo TIAs or early progressive stroke TCDs with embolization/stump Basilar artery occlusion before or after intra-arterial pharmacological or mechanical thrombolysis. Known hypercoagulable states Cerebral venous sinus thrombosis 36
37 Conclusion Post-stroke/TIA recurrence stroke rate is high. Evidence/Guidelines exist for symptomatic carotid disease (BP, antithrombotics, CEA/CUS) Identification of high-risk patients can allow targeted therapies such as hyperacute CEA and anticoagulation. Women have a different risk/benefit profile. 37
38 Extra slides 38
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough
 Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Advances in the treatment of posterior cerebral circulation symptomatic disease
 Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Management of cervicocephalic arterial dissection. Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery
 Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease
 The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Spontaneous embolisation on TCD and carotid plaque features
 Spontaneous embolisation on TCD and carotid plaque features J. David Spence Stroke Prevention & Atherosclerosis Research Centre Robarts Research Institute London, Canada dspence@robarts.ca www.imaging.robarts.ca/sparc
Spontaneous embolisation on TCD and carotid plaque features J. David Spence Stroke Prevention & Atherosclerosis Research Centre Robarts Research Institute London, Canada dspence@robarts.ca www.imaging.robarts.ca/sparc
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Carotid Artery Stenting Versus
 Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
CardioLucca2014. Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee. Fabrizio Tomai
 CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
DESCRIPTION: Percent of asymptomatic patients undergoing CEA who are discharged to home no later than post-operative day #2
 Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Stroke prevention in asymptomatic carotid stenosis. ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ
 Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
MEET Θ symptomatic patients. K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany
 MEET Θ 2006 Why I stent asymptomatic and symptomatic patients K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany Evidence for treating symptomatic patients symptomatic patients
MEET Θ 2006 Why I stent asymptomatic and symptomatic patients K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany Evidence for treating symptomatic patients symptomatic patients
The Great Swedish Debate. Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund
 The Great Swedish Debate Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund My Disclosures Trying to bribe the moderators What do my patients expect? Balanced information
The Great Swedish Debate Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund My Disclosures Trying to bribe the moderators What do my patients expect? Balanced information
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Int J Clin Exp Med 2018;11(9): /ISSN: /IJCEM
: /ISSN: /IJCEM") Int J Clin Exp Med 2018;11(9):10069-10075 www.ijcem.com /ISSN:1940-5901/IJCEM0069372 Case Report Acute cerebral infarction after spontaneous recanalization of extracranial internal carotid artery atherosclerotic
Int J Clin Exp Med 2018;11(9):10069-10075 www.ijcem.com /ISSN:1940-5901/IJCEM0069372 Case Report Acute cerebral infarction after spontaneous recanalization of extracranial internal carotid artery atherosclerotic
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention
 How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention Christopher J. White MD, MSCAI Chief of Medical Services, Professor and Chairman of Medicine Ochsner Medical Center
How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention Christopher J. White MD, MSCAI Chief of Medical Services, Professor and Chairman of Medicine Ochsner Medical Center
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
The argument against revascularization for asymptomatic carotid stenosis
 The argument against revascularization for asymptomatic carotid stenosis Seemant Chaturvedi, MD, FAHA, FAAN Professor of Clinical Neurology Vice-Chair for VA Programs Univ. of Miami Miller School of Medicine
The argument against revascularization for asymptomatic carotid stenosis Seemant Chaturvedi, MD, FAHA, FAAN Professor of Clinical Neurology Vice-Chair for VA Programs Univ. of Miami Miller School of Medicine
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
LARGE ARTERY DISEASE pathophysiology of ischemic insults. ISCHEMIC STROKE & TIA main etiologies
 תאריך בדיקה- 27.1.04 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
תאריך בדיקה- 27.1.04 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
ISCHEMIC STROKE & TIA main etiologies
 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון תאריך בדיקה- 27.1.04 ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון תאריך בדיקה- 27.1.04 ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea
 TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea R. Pini, G.L. Faggioli, M. Gargiulo, E. Pisano, A. Pilato, E. Gallitto, C. Mascoli, L.M. Cacioppa, A. Vacirca,
TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea R. Pini, G.L. Faggioli, M. Gargiulo, E. Pisano, A. Pilato, E. Gallitto, C. Mascoli, L.M. Cacioppa, A. Vacirca,
Emboli detection to evaluate risk of stroke
 Emboli detection to evaluate risk of stroke Background: Improved methods are required to identify patients with asymptomatic carotid stenosis at high risk for stroke. Whether surgery is beneficial for
Emboli detection to evaluate risk of stroke Background: Improved methods are required to identify patients with asymptomatic carotid stenosis at high risk for stroke. Whether surgery is beneficial for
Intracranial Atherosclerosis in Asians
 Intracranial Atherosclerosis in Asians Anthony S. Kim, MD Assistant Clinical Professor of Neurology UCSF Neurovascular Service February 27, 2010 Disclosures Research Support National Institutes of Health
Intracranial Atherosclerosis in Asians Anthony S. Kim, MD Assistant Clinical Professor of Neurology UCSF Neurovascular Service February 27, 2010 Disclosures Research Support National Institutes of Health
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Carotid Stenting and Surgery in 2016 in Russia
 Carotid Stenting and Surgery in 2016 in Russia Novosibirsk research institute of circulation pathology named by Meshalkin, Novosibirsk, Russia Starodubtsev V., Karpenko A., Ignatenko P. Annually in Russia
Carotid Stenting and Surgery in 2016 in Russia Novosibirsk research institute of circulation pathology named by Meshalkin, Novosibirsk, Russia Starodubtsev V., Karpenko A., Ignatenko P. Annually in Russia
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS
 CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Management of Extracranial Carotid Disease and Intracranial Atherosclerosis Wein T, Gladstone D (Writing Group Chairs) on Behalf of the PREVENTION of STROKE
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Management of Extracranial Carotid Disease and Intracranial Atherosclerosis Wein T, Gladstone D (Writing Group Chairs) on Behalf of the PREVENTION of STROKE
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Extracranial Carotid Artery Stenting With or Without Distal Protection Device
 Extracranial Carotid Artery Stenting With or Without Distal Protection Device Eak-Kyun Shin MD. Professor of Medicine Division of Cardiology, Heart Center, Gil Medical Center Gacheon Medical School Incheon,
Extracranial Carotid Artery Stenting With or Without Distal Protection Device Eak-Kyun Shin MD. Professor of Medicine Division of Cardiology, Heart Center, Gil Medical Center Gacheon Medical School Incheon,
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
TIA triage in Not all that glitters is gold
 TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Limitations of Other Embolic Protection Devices - Filters. Carotid Stenting with Flow Reversal. Limitations of Distal Occlusion
 Carotid Stenting with Flow Reversal Marc Schermerhorn, MD Division of Vascular and Endovascular Surgery Beth Israel Deaconess Center Boston, MA Limitations of Other Embolic Protection Devices - Filters
Carotid Stenting with Flow Reversal Marc Schermerhorn, MD Division of Vascular and Endovascular Surgery Beth Israel Deaconess Center Boston, MA Limitations of Other Embolic Protection Devices - Filters
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Surgical Treatment of Carotid Disease
 Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Cryptogenic Stroke: What Don t We Know. Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare
 Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Internal carotid artery near-total occlusions: Is it justified to operate on them?
 Internal carotid artery near-total occlusions: Is it justified to operate on them? Christos D. Liapis Professor (Em) of Vascular Surgery Athens University Medical School Director Vascular & Endovascular
Internal carotid artery near-total occlusions: Is it justified to operate on them? Christos D. Liapis Professor (Em) of Vascular Surgery Athens University Medical School Director Vascular & Endovascular
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia
 GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
Carlo Setacci Chief Department of Surgery Vascular and Endovascular Unit University of Siena
 Which carotid procedures are required to grade the stroke risk? Carlo Setacci Chief Department of Surgery Vascular and Endovascular Unit University of Siena Faculty disclosure Carlo Setacci I have no financial
Which carotid procedures are required to grade the stroke risk? Carlo Setacci Chief Department of Surgery Vascular and Endovascular Unit University of Siena Faculty disclosure Carlo Setacci I have no financial
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Assessment of the procedural etiology of stroke resulting from carotid artery stenting
 Assessment of the procedural etiology of stroke resulting from carotid artery stenting 1. Study Purpose and Rationale: A. Background Stroke is the 3 rd leading cause of death in the United States and carries
Assessment of the procedural etiology of stroke resulting from carotid artery stenting 1. Study Purpose and Rationale: A. Background Stroke is the 3 rd leading cause of death in the United States and carries
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Carotid Artery Stenting
 Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor
 Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017 1 Faculty Disclosure Faculty: Grant Stotts MD, FRCPC Assistant Professor, uottawa Brain and Mind Institute
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017 1 Faculty Disclosure Faculty: Grant Stotts MD, FRCPC Assistant Professor, uottawa Brain and Mind Institute
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Tailored carotid artery stenting
 Tailored carotid artery stenting is associated with a low complication rate 30-day results from the continued TARGET-CAS study in 1133 consecutive procedures. Lukasz Tekieli, Piotr Pieniazek, Piotr Musialek,
Tailored carotid artery stenting is associated with a low complication rate 30-day results from the continued TARGET-CAS study in 1133 consecutive procedures. Lukasz Tekieli, Piotr Pieniazek, Piotr Musialek,