CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough
|
|
|
- Eleanore Baldwin
- 5 years ago
- Views:
Transcription

1 Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough

2 DISCLOSURES I have no financial disclosures Presenter name

3 Philip A Davenport, MD, PhD Presenter name
4 Stroke Statistics About 795,000 Americans each year suffer a new or recurrent stroke. That means, on average, a stroke occurs every 40 seconds. Stroke kills more than 129,000 people a year. That's about 1 of every 18 deaths. It is the 5th leading cause of death. Presenter name On average, every 4 minutes someone dies of stroke. Americans paid about $95 billion in 2015 for strokerelated medical costs and disability.

5 PREVALENCE OF ASX DZ It is now estimated that some 6% of Americans over 65 harbor an asymptomatic carotid artery stenosis >50% Presenter name

6 Nat l History of Asymptomatic Disease Presenter name

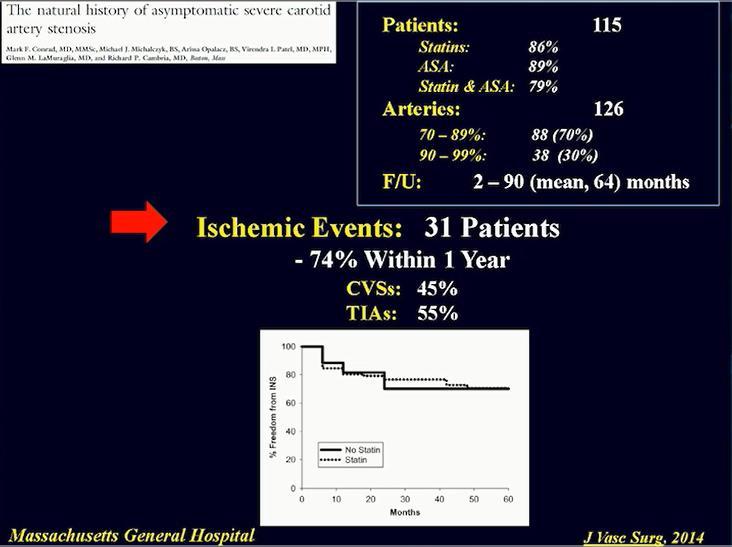
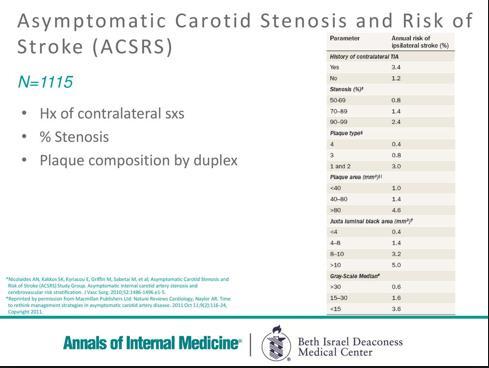
7 Carotid stenosis >70% significantly increases stroke risk irrespective of the Presenter fact that name 70% of this cohort were on statin medications
8
9
10
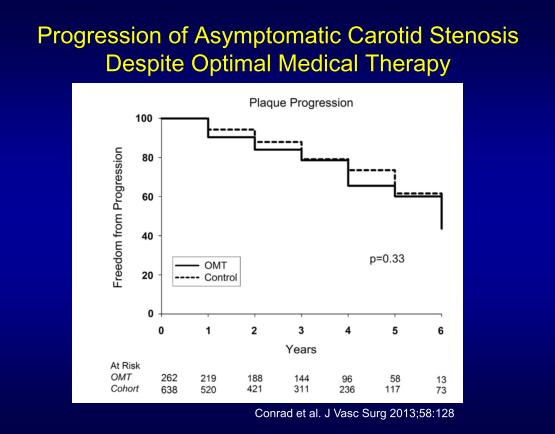
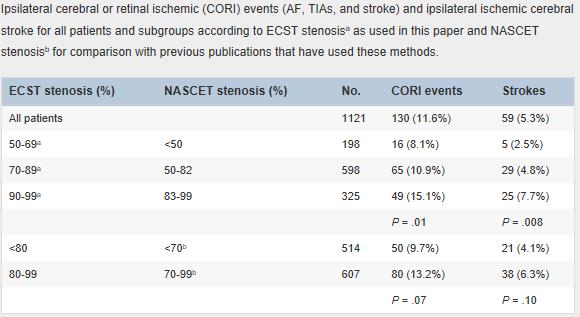
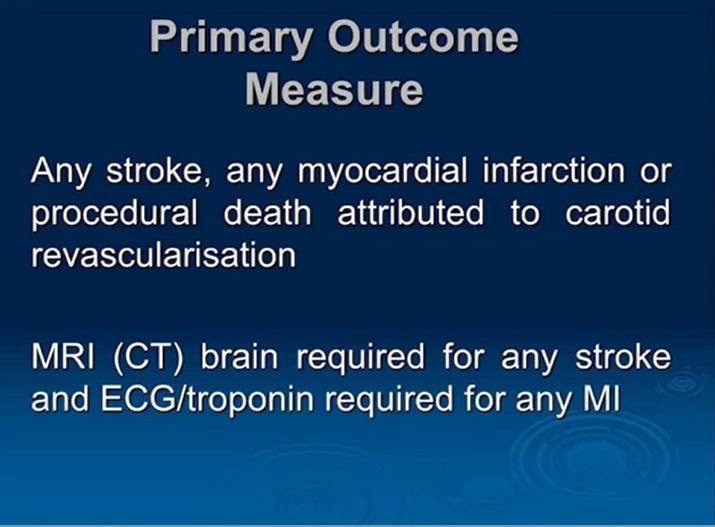
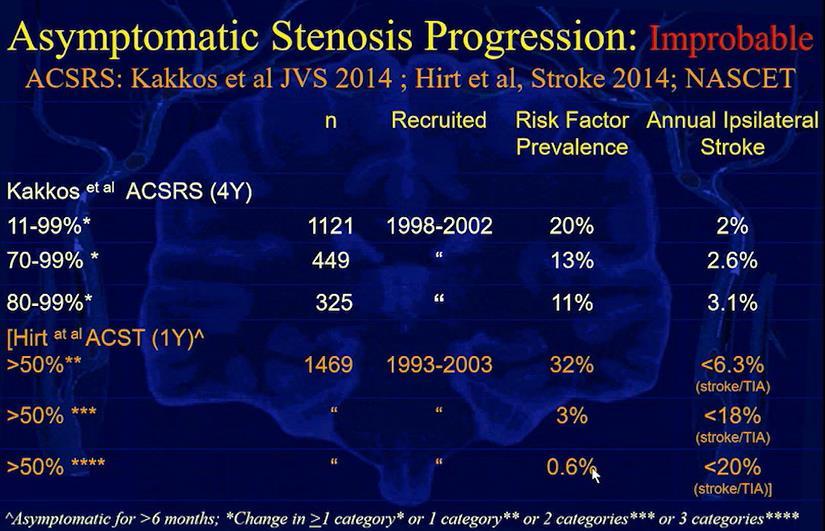
![A total of 1121 patients with asymptomatic carotid stenosis of 50% to 99% in relation to the bulb diameter (European Carotid Surgery Trial [ECST] method) underwent six monthly clinical assessments](/docs-images/82/84888700/images/11-1.jpg "and carotid duplexes for up to 8 years (mean follow-up, 4 years). Regression occurred in 43 (3.8%), no change in 856 (76.4%), and progression in 222 (19.8%) patients.")
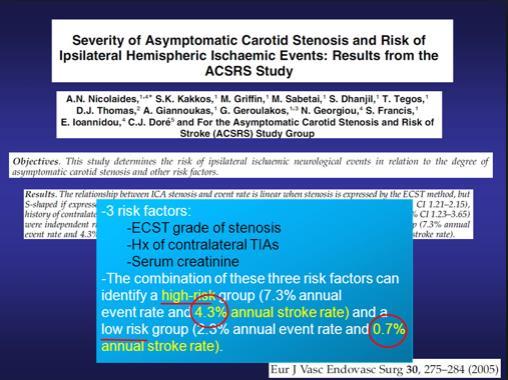
11 A total of 1121 patients with asymptomatic carotid stenosis of 50% to 99% in relation to the bulb diameter (European Carotid Surgery Trial [ECST] method) underwent six monthly clinical assessments and carotid duplexes for up to 8 years (mean follow-up, 4 years). Regression occurred in 43 (3.8%), no change in 856 (76.4%), and progression in 222 (19.8%) patients. For the entire cohort, the 8-year cumulative ipsilateral cerebral ischemic stroke rate was zero in patients with regression, 9% if the stenosis was unchanged, and 16% if there was progression (average annual stroke rates of 0%, 1.1%, and 2.0%, respectively) For patients with baseline stenosis 70% to 99%, in the absence of progression (n = 349), the 8-year cumulative ipsilateral cerebral ischemic stroke rate was 12%. In the presence of progression (n = 77), it was 21% (average annual stroke rates Presenter of 1.5% and 2.6%, name respectively) PROGRESSION IS BAD!!!!
 Asymptomatic Carotid Stenosis and Risk of Stroke")
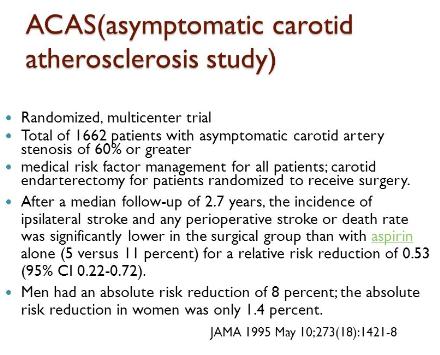
12 ASX TRIALS VA Cooperative Study Group Asx Carotid Atherosclerosis Trial (ACAS) Presenter name Asx Carotid Surgery Trial (ACST) Asymptomatic Carotid Stenosis and Risk of Stroke (ACSRS)
13
14

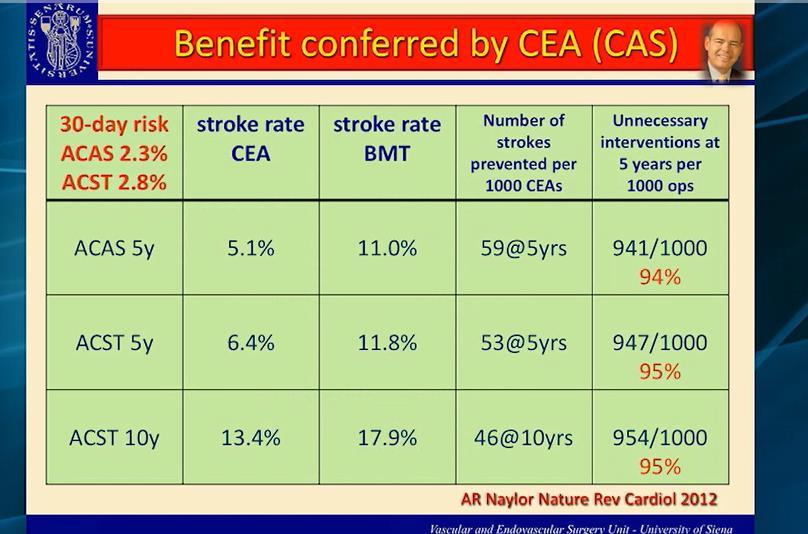
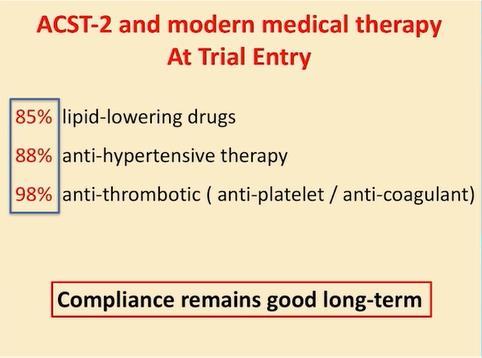
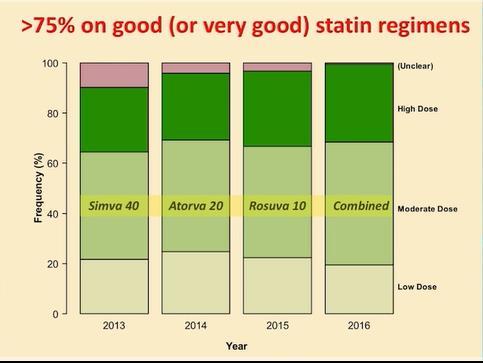
15 ACST (asymptomatic carotid surgery trial) 3120 asx pts w/ >60% stenosis by U/S Randomized b/t immed CEA and indefinite deferral of any CEA and were followed for up to 5 yrs Net five year risk for stroke or periop death in CEA pts was reduced by nearly half Absolute risk reduction over 5 yrs Presenter greater for name men than for women (8.2 vs 4.08) 80% of patients were on statins in latter yrs of study
16
17
18
19

20 CRITICAL STENOSIS, VULNERABLE PLAQUE, PRIOR C/L TIA/CVA IS BAD Presenter name ADDITIVE EFFECT IS WORSE
21
22
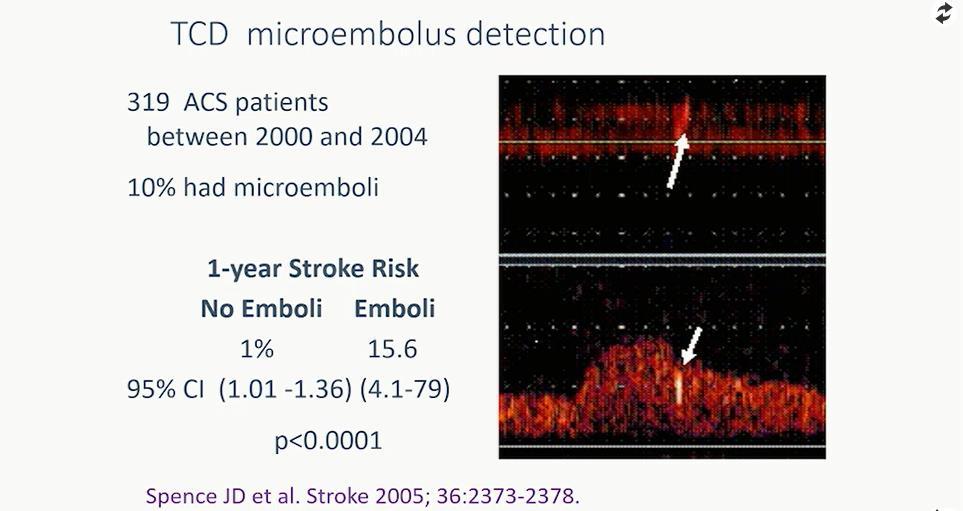
23 3 or more ulcers adds 5% risk to microemboli (greater than equal 2/hr) TCD HITS & MULTIPLE ULCERS ARE BAD Presenter name

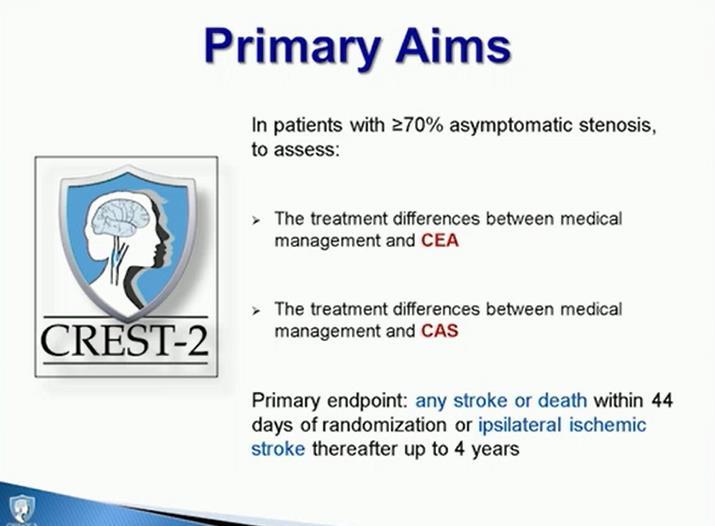
24 WE HAVE TO FIND THIS PLAQUE BEFORE IT FINDS OUR PATIENT S BRAIN
25
26
27
28
29
30
31 GUIDELINNES Presenter name

32
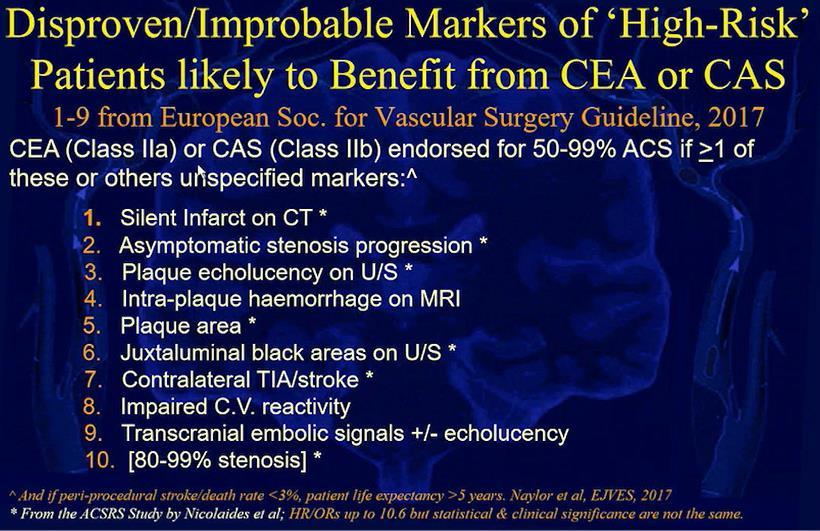
 on computerized plaque analysis, Presenter plaque echolucency, name intra-plaque haemorrhage")
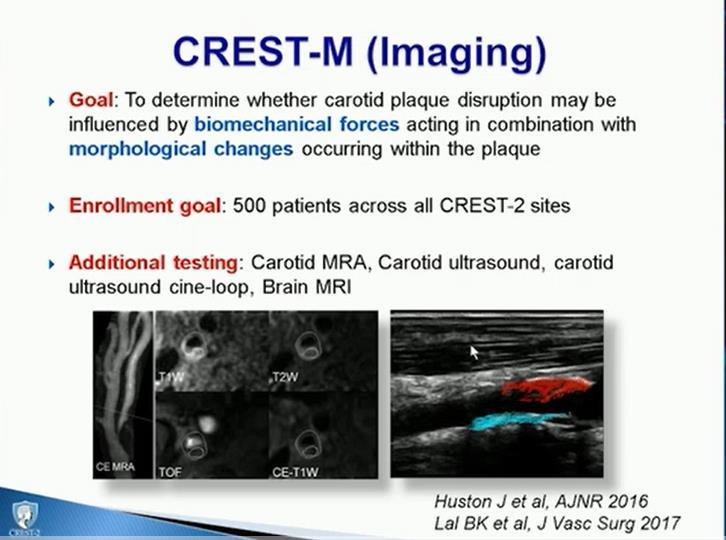
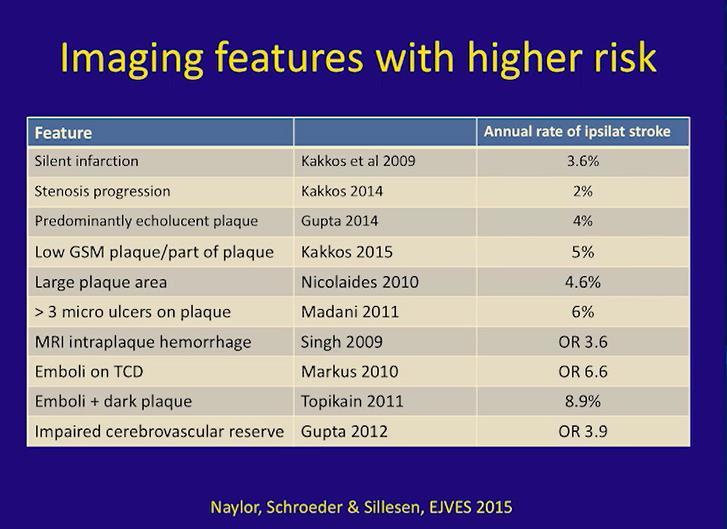
33 While awaiting data from CREST-2, ECST-2, ACST-2, and ACTRIS and the development of validated algorithms for patient selection, the presence of one or more clinical and/or imaging features such as silent infarction on CT/MRI, stenosis progression, large plaque area, large juxta-luminal black area (JBA) on computerized plaque analysis, Presenter plaque echolucency, name intra-plaque haemorrhage on MRI, impaired cerebral vascular reserve (CVR), and spontaneous embolisation on transcranial Doppler (TCD) monitoring, might be useful for selecting higher-risk stroke patients for revascularisation
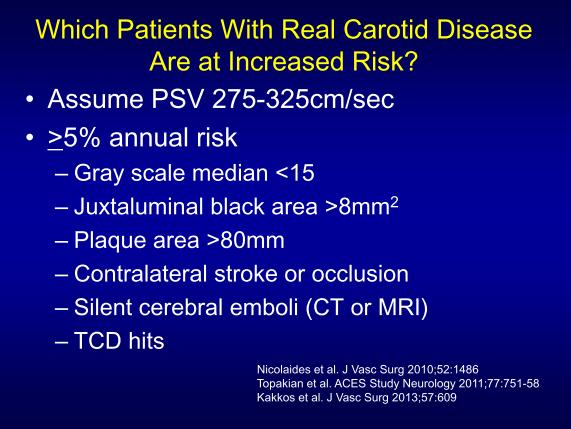
34 RECOMMENDATIONS FOR ASX CAROTID STENOSIS HIGH GRADE LESIONS (80-99%) PROGRESSION OF DISEASE VULNERABLE PLAQUE GSM <15 PLAQUE AREA >80 JUXTA-LUMINAL BLACK AREA > 8 cm² Presenter name CONTRALATERAL CVA or OCCLUSION ( CV RESERVE) MULTIPLE TCD HITS MULTIPLE ULCERATIONS

35



36 ???BIAS??? Presenter name
37
38 Roadster 2 Exclusion Criteria EXCLUSION CRITERIA: Each potential patient must be screened to ensure that they do not meet any of the following exclusion criteria. This screening is to be based on known medical history and data available at the time of eligibility determination and enrollment. Patient has an alternative source of cerebral embolus, including but not limited to: Patient has chronic atrial fibrillation. Patient has had any episode of paroxysmal atrial fibrillation within the past 6 months, or history of paroxysmal atrial fibrillation requiring chronic anticoagulation. Knowledge of cardiac sources of emboli. e.g. left ventricular aneurysm, intracardiac filling defect, cardiomyopathy, aortic or mitral prosthetic heart valve, calcific aortic stenosis, endocarditis, mitral stenosis, atrial septal defect, atrial septal aneurysm, or left atrial myxoma). Recently (<60 days) implanted heart valve (either surgically or endovascularly), which is a known source of emboli as confirmed on echocardiogram. Abnormal angiographic findings: ipsilateral intracranial or extracranial Presenter arterial stenosis (as determined name by angiography or CTA/MRA 6 months prior to index procedure) greater in severity than the lesion to be treated, cerebral aneurysm > 5 mm, AVM (arteriovenous malformation) of the cerebral vasculature, or other abnormal angiographic findings. Patient has a history of spontaneous intracranial hemorrhage within the past 12 months, or has had a recent (<7 days) stroke of sufficient size (on CT or MRI) to place him or her at risk of hemorrhagic conversion during the procedure. Patient had hemorrhagic transformation of an ischemic stroke within the past 60 days. Patient with a history of major stroke attributable to either carotid artery (CVA or retinal embolus) with major neurological deficit (NIHSS 5 OR mrs 3) likely to confound study endpoints within 1 month of index procedure. Patient has an intracranial tumor.
39 Exclusion Criteria Roadster 2 Patient has an evolving stroke. Patient has neurologic illnesses within the past two years characterized by fleeting or fixed neurologic deficit which cannot be distinguished from TIA or stroke, including but not limited to: moderate to severe dementia, partial or secondarily generalized seizures, complicated or classic migraine, tumor or other space-occupying brain lesions, subdural hematoma, cerebral contusion or other posttraumatic lesions, intracranial infection, demyelinating disease, or intracranial hemorrhage). Patient has had a TIA or amaurosis fugax within 48 hrs prior to the procedure. Patient has an isolated hemisphere. Patient had or will have CABG, endovascular stent procedure, valve intervention or vascular surgery within 30 days before or after the intervention. Myocardial Infarction within 72 hours prior to the intervention. Presence of a previous placed intravascular stent in target vessel or ipsilateral CCA or significant CCA inflow lesion. Occlusion or [Thrombolysis In Myocardial Infarction Trial (TIMI 0)] "string sign" >1cm of the ipsilateral common or internal carotid artery. An intraluminal filling defect (defined as an endoluminal lucency surrounded by contrast, seen in multiple angiographic projections, in the absence of angiographic evidence of calcification) whether or not it is associated with an ulcerated target lesion. Ostium of Common Carotid Artery (CCA) requires revascularization. Presenter name Patient has an open stoma in the neck. Female patients who are pregnant or may become pregnant. Patient has history of intolerance or allergic reaction to any of the study medications or stent materials (refer to stent IFU), including aspirin (ASA), ticlopidine, clopidogrel, statin or contrast media (that can't be pre medicated). Patients must be able to tolerate statins and a combination of ASA and ticlopidine or ASA and clopidogrel. Patient must have a life expectancy <3 years without contingencies related to other medical, surgical, or interventional procedures as per the Wallaert Score and patients with primary, recurrent or metastatic malignancy who do not have independent assessment of life expectancy performed by the treating oncologist or an appropriate specialist other than the physician performing TCAR.
40
41

42




43

44 Todd W Gensler MD, FACS twgensle@sentara.com Presenter name
45
46
47
48
49
50
51
52
53
54 Best method TCD microemboli Presenter name
55
56
57
58
59
60
61

62 Abbott says this is best risk stratifier Presenter name
63
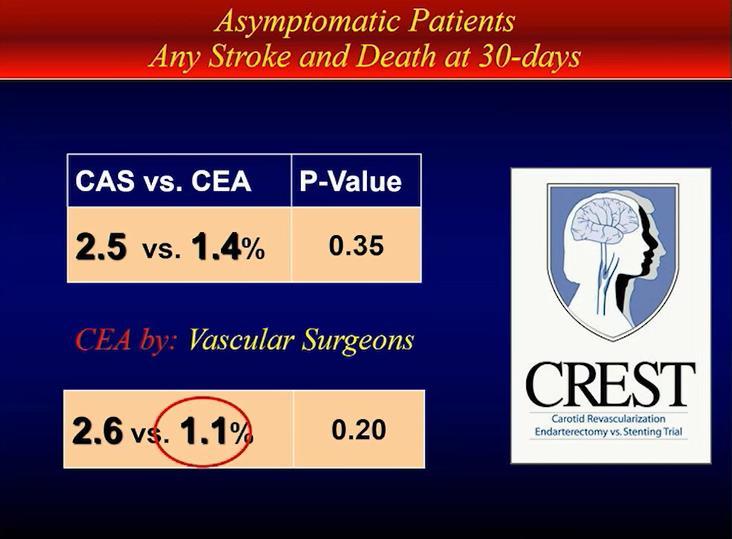
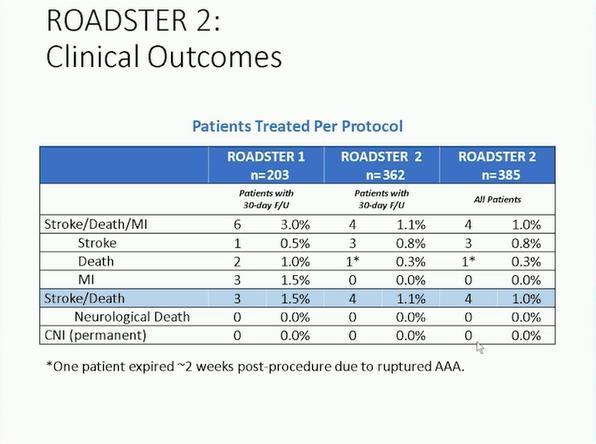
64 1.0% in vascular surgeons Presenter name
65
66
67
68
69

70

71 All asx carotid pts should be on intensive lipid lowering Rx Presenter name
72
73
74
75
76
77
78
79
80
81
82
83
84
85

86 Published in Circulation Presenter name
87

88 How often do stent fx occur? Presenter name
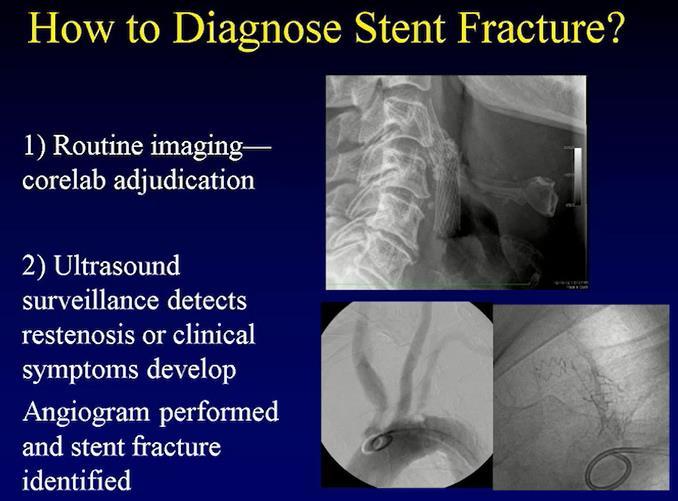
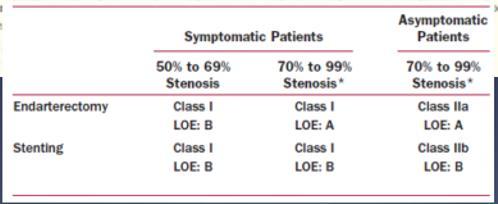
89
90 Peaks yrs 2-3 and does not increase w time Presenter name
91
92
93
94
95
96
97
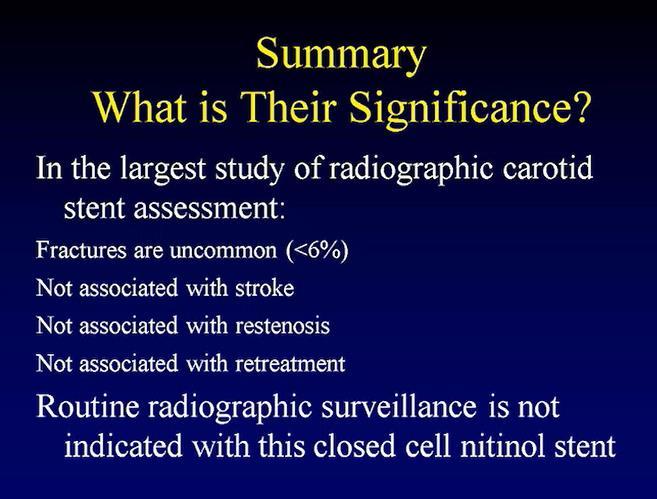
98 <5% benefit Presenter name
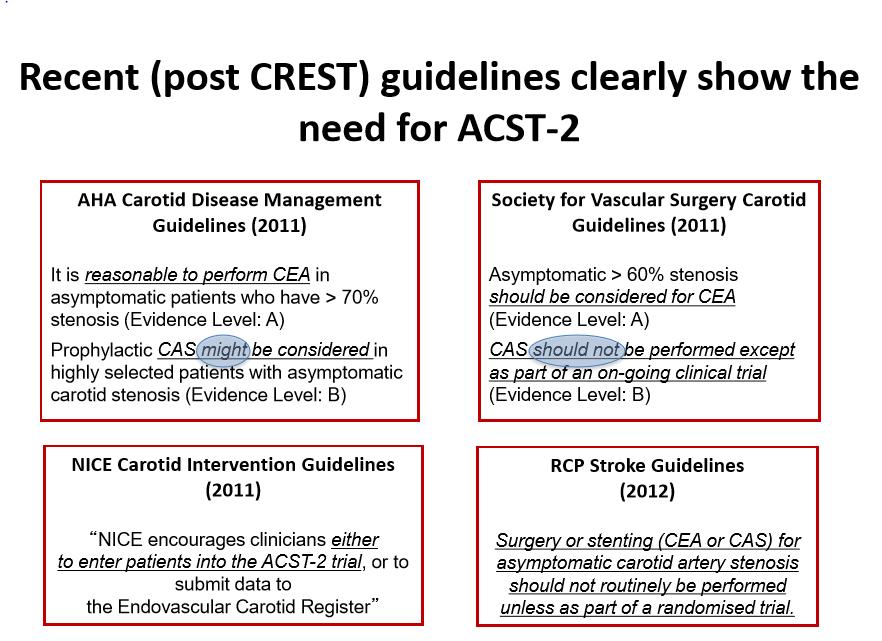
99 Asymptomatic Disease Consensus Guidelines Class 1--Selection of asymptomatic patients for carotid revascularization should be guided by an assessment of comorbid conditions, life expectancy, and other individual factors and should include a thorough discussion of the risks and benefits of the procedure with an understanding of patient preferences. (Level C) Class IIa--It is reasonable to perform CEA in asymptomatic patients who have more than 70% stenosis of the internal carotid artery if the risk of perioperative stroke, MI, and death is low (Level A) Presenter name Class IIb--Prophylactic CAS might be considered in highly selected patients with asymptomatic carotid stenosis (minimum 60% by angiography, 70% by validated Doppler ultrasound), but its effectiveness compared with medical therapy alone in this situation is not well established (Level B)
100 Click to edit Master text styles Second level Third level Fourth level» Fifth level Presenter name
101
102

103 Click to edit Master text styles Second level Third level Fourth level» Fifth level Presenter name
104
105
106

107 Where Do We Draw the Line? Presenter name
108
109
110
111
112
113

114
115


116 Event Rates in Patients With ASX Carotid Artery Stenosis Managed Without Revascularization Presenter name

117
118

119
120
121
122
123
124

125 Click to edit Master text styles Second level Third level Fourth level» Fifth level Presenter name

126 Click to edit Master text styles Second level Third level Fourth level» Fifth level Presenter name
127 Click to edit Master text styles Second level Third level Fourth level» Fifth level Presenter name

128 Click to edit Master text styles Second level Third level Fourth level» Fifth level Presenter name
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
ROADSTER 2. SPONSOR: Silk Road Medical
 ROADSTER 2 CONDITION: Carotid artery disease PI: Jessica Titus, MD CONTACT INFO: Jo Anne Goldman JoAnne.Goldman@allina.com 612-863-3793 DESCRIPTION: The study is intended to evaluate real world usage of
ROADSTER 2 CONDITION: Carotid artery disease PI: Jessica Titus, MD CONTACT INFO: Jo Anne Goldman JoAnne.Goldman@allina.com 612-863-3793 DESCRIPTION: The study is intended to evaluate real world usage of
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
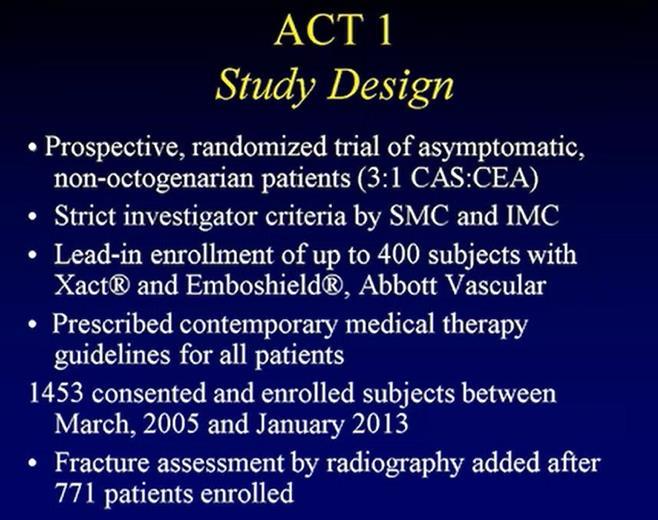
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
ESC Heart & Brain Workshop
 ESC Heart & Brain Workshop The role of vascular surgeon in stroke prevention Barbara Rantner, MD, PhD, Department of Vascular Surgery, Medical University Innsbruck, Innsbruck, Austria Supported by Bayer,
ESC Heart & Brain Workshop The role of vascular surgeon in stroke prevention Barbara Rantner, MD, PhD, Department of Vascular Surgery, Medical University Innsbruck, Innsbruck, Austria Supported by Bayer,
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease
 The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Octogenarians Must Be Treated With CAS
 Some Octogenarians Must Be Treated With CAS LN Hopkins, MD E Levy MD, Adnan Siddiqui,, MD, PhD Rod Samuelson MD J Mocco MD LN Hopkins, MD Potential Conflicts Consultant & research support: Boston Scientific,
Some Octogenarians Must Be Treated With CAS LN Hopkins, MD E Levy MD, Adnan Siddiqui,, MD, PhD Rod Samuelson MD J Mocco MD LN Hopkins, MD Potential Conflicts Consultant & research support: Boston Scientific,
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
LARGE ARTERY DISEASE pathophysiology of ischemic insults. ISCHEMIC STROKE & TIA main etiologies
 תאריך בדיקה- 27.1.04 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
תאריך בדיקה- 27.1.04 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
ISCHEMIC STROKE & TIA main etiologies
 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון תאריך בדיקה- 27.1.04 ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון תאריך בדיקה- 27.1.04 ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Stenting Versus
 Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Approach to the Patient with Carotid Artery Disease
 Approach to the Patient with Carotid Artery Disease Michael R. Jaff, DO, FACP, FACC Director, Vascular Medicine Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Statement Within
Approach to the Patient with Carotid Artery Disease Michael R. Jaff, DO, FACP, FACC Director, Vascular Medicine Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Statement Within
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Direct oral anticoagulants for Embolic Strokes of Undetermined Source? George Ntaios University of Thessaly, Larissa/Greece
 Direct oral anticoagulants for Embolic Strokes of Undetermined Source? George Ntaios University of Thessaly, Larissa/Greece Disclosures Scholarships: European Stroke Organization; Hellenic Society of Atherosclerosis.
Direct oral anticoagulants for Embolic Strokes of Undetermined Source? George Ntaios University of Thessaly, Larissa/Greece Disclosures Scholarships: European Stroke Organization; Hellenic Society of Atherosclerosis.
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Surgical Treatment of Carotid Disease
 Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Management of cervicocephalic arterial dissection. Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery
 Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
DESPITE CURRENT LEVEL 1 EVIDENCE THE OUTLOOK FOR AN UPSURGE IN CAROTID STENTING (CAS) IS BRIGHT FRANK J. VEITH LINC LEIPZIG JANUARY 27, 2015
 IS BRIGHT FRANK J. VEITH LINC LEIPZIG JANUARY 27, 2015") DESPITE CURRENT LEVEL 1 EVIDENCE THE OUTLOOK FOR AN UPSURGE IN CAROTID STENTING (CAS) IS BRIGHT FRANK J. VEITH LINC - 2015 LEIPZIG JANUARY 27, 2015 Disclosure Speaker name: FRANK J. VEITH DESPITE SOME
DESPITE CURRENT LEVEL 1 EVIDENCE THE OUTLOOK FOR AN UPSURGE IN CAROTID STENTING (CAS) IS BRIGHT FRANK J. VEITH LINC - 2015 LEIPZIG JANUARY 27, 2015 Disclosure Speaker name: FRANK J. VEITH DESPITE SOME
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective)
") Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Carotid Artery Disease How the Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient
 Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers
 The study a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers Conflict of interest have the following potential conflicts of interest to report: Consulting
The study a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers Conflict of interest have the following potential conflicts of interest to report: Consulting
True cryptogenic stroke
 True cryptogenic stroke Arne Lindgren, MD, PhD Dept of Clinical Sciences Lund, Neurology, Lund University Dept of Neurology and Rehabilitation Medicine Skåne University Hospital Lund, Sweden Disclosures
True cryptogenic stroke Arne Lindgren, MD, PhD Dept of Clinical Sciences Lund, Neurology, Lund University Dept of Neurology and Rehabilitation Medicine Skåne University Hospital Lund, Sweden Disclosures
Carotid Artery Stent: Is it ready for prime time?
 2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
ASYMPTOMATIC CAROTID STENOSIS WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON SURVIVAL PREDICTIONS
 CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON SURVIVAL PREDICTIONS") WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON S ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON DISCLOSURES INDIVIDUAL None A patient with an asymptomatic 90%
WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON S ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON DISCLOSURES INDIVIDUAL None A patient with an asymptomatic 90%
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis?
 for stroke prevention in patients with asymptomatic carotid stenosis?") How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis? Dorothee Saur Department of Neurology University of Leipzig Disclosure for Dorothee
How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis? Dorothee Saur Department of Neurology University of Leipzig Disclosure for Dorothee
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Carotid Artery Stenting (CAS) Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA
 Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA") Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
FRANK J. VEITH MAC TH MUNICH VASCULAR CONF
 UPDATE ON THE NORTH AMERICAN RCTs CREST 2 & ACST 1: WILL CAS SURVIVE AS AN ALTERNATIVE TO BMT OR CEA? FRANK J. VEITH 6 TH MUNICH VASCULAR CONF MAC - 2016 MUNICH DECEMBER 1, 2016 I HAVE NO FINANCIAL CONFLICTS
UPDATE ON THE NORTH AMERICAN RCTs CREST 2 & ACST 1: WILL CAS SURVIVE AS AN ALTERNATIVE TO BMT OR CEA? FRANK J. VEITH 6 TH MUNICH VASCULAR CONF MAC - 2016 MUNICH DECEMBER 1, 2016 I HAVE NO FINANCIAL CONFLICTS
TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS
 TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS Assistant Professor of Surgery Director of Carotid Interventions Division of Vascular & Endovascular Surgery Stony Brook University
TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS Assistant Professor of Surgery Director of Carotid Interventions Division of Vascular & Endovascular Surgery Stony Brook University
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS
 CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Management of Extracranial Carotid Disease and Intracranial Atherosclerosis Wein T, Gladstone D (Writing Group Chairs) on Behalf of the PREVENTION of STROKE
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Management of Extracranial Carotid Disease and Intracranial Atherosclerosis Wein T, Gladstone D (Writing Group Chairs) on Behalf of the PREVENTION of STROKE
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Current Medical Therapy for
 STROKE Current Medical Therapy for Stroke Prevention and Treatment Endovascular Today engages lipid expert Richard Milani, MD, and stroke expert Roekchai Tulyapronchote, MD, in a rapid-fire Q&A session.
STROKE Current Medical Therapy for Stroke Prevention and Treatment Endovascular Today engages lipid expert Richard Milani, MD, and stroke expert Roekchai Tulyapronchote, MD, in a rapid-fire Q&A session.
Stroke prevention in asymptomatic carotid stenosis. ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ
 Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
Cryptogenic Stroke: What Don t We Know. Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare
 Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS. Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford
 Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford Two BIG questions in carotid research Question #1 Should we
Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford Two BIG questions in carotid research Question #1 Should we
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
ICSS Safety Results NOT for PUBLICATION. June 2009 ICSS ICSS ICSS ICSS. International Carotid Stenting Study: Main Inclusion Criteria
 Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered?
 TCT 2009 San Francisco, California September 22, 2009 The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered? Michael
TCT 2009 San Francisco, California September 22, 2009 The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered? Michael
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH
 ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
Aortic arch pathology. Cerebral ischemia following carotid artery stenosis.
 Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
CEA or CAS for asymptomatic carotid stenosis which patients benefit most?
 CEA or CAS for asymptomatic carotid stenosis which patients benefit most? Alison Halliday Professor of Vascular Surgery University of Oxford Keynote Lecture, MAC, December 6 th 2018 Clinical/imaging characteristics
CEA or CAS for asymptomatic carotid stenosis which patients benefit most? Alison Halliday Professor of Vascular Surgery University of Oxford Keynote Lecture, MAC, December 6 th 2018 Clinical/imaging characteristics
CAROTID ANGIOPLASTY AND STENTING UNDER PROTECTION IS BECOMING THE GOLD STANDARD TREATMENT IN HIGH AND LOW RISK PATIENTS
 CAROTID ANGIOPLASTY AND STENTING UNDER PROTECTION IS BECOMING THE GOLD STANDARD TREATMENT IN HIGH AND LOW RISK PATIENTS M. HENRY* MD, I. HENRY MD A. POLYDOROU MD, A.D. POLYDOROU MD M. HUGEL RN NANCY FRANCE
CAROTID ANGIOPLASTY AND STENTING UNDER PROTECTION IS BECOMING THE GOLD STANDARD TREATMENT IN HIGH AND LOW RISK PATIENTS M. HENRY* MD, I. HENRY MD A. POLYDOROU MD, A.D. POLYDOROU MD M. HUGEL RN NANCY FRANCE
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
I want Medical Therapy for my ASYMPTOMATIC patients with Carotid Disease
 I want Medical Therapy for my ASYMPTOMATIC patients with Carotid Disease Alonso Collar, M.D. F.A.C.S. Chief of Surgery Chair Cardiovascular Surgery Sparrow Hospital Lansing, MI I want Medical Therapy for
I want Medical Therapy for my ASYMPTOMATIC patients with Carotid Disease Alonso Collar, M.D. F.A.C.S. Chief of Surgery Chair Cardiovascular Surgery Sparrow Hospital Lansing, MI I want Medical Therapy for
Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie?
 XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea
 TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea R. Pini, G.L. Faggioli, M. Gargiulo, E. Pisano, A. Pilato, E. Gallitto, C. Mascoli, L.M. Cacioppa, A. Vacirca,
TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea R. Pini, G.L. Faggioli, M. Gargiulo, E. Pisano, A. Pilato, E. Gallitto, C. Mascoli, L.M. Cacioppa, A. Vacirca,
NCDR CARE Registry Carotid Artery Revascularization and Endarterectomy Registry Carotid Artery Stenting Form v1.09
 NCDR CARE Registry Carotid Artery Revascularization and Endarterectomy Registry Carotid Artery Stenting Fm v1.09 A. PARTICIPANT ADMINISTRATION Participant ID 1000 : Participant Name 1010 : Medicare Provider
NCDR CARE Registry Carotid Artery Revascularization and Endarterectomy Registry Carotid Artery Stenting Fm v1.09 A. PARTICIPANT ADMINISTRATION Participant ID 1000 : Participant Name 1010 : Medicare Provider
Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side
 Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side Academician Mitrev Z, Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 History Hippocrates, 400 B.C.
Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side Academician Mitrev Z, Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 History Hippocrates, 400 B.C.
CardioLucca2014. Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee. Fabrizio Tomai
 CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA
 Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy
 13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
ACUTE CENTRAL PERIFERALEMBOLISM
 EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
APPENDIX A NORTH AMERICAN SYMPTOMATIC CAROTID ENDARTERECTOMY TRIAL
 APPENDIX A Primary Findings From Selected Recent National Institute of Neurological Disorders and Stroke-Sponsored Clinical Trials That Have shaped Modern Stroke Prevention Philip B. Gorelick 178 NORTH
APPENDIX A Primary Findings From Selected Recent National Institute of Neurological Disorders and Stroke-Sponsored Clinical Trials That Have shaped Modern Stroke Prevention Philip B. Gorelick 178 NORTH
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Carotid Artery Stenting
 Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Internal carotid artery near-total occlusions: Is it justified to operate on them?
 Internal carotid artery near-total occlusions: Is it justified to operate on them? Christos D. Liapis Professor (Em) of Vascular Surgery Athens University Medical School Director Vascular & Endovascular
Internal carotid artery near-total occlusions: Is it justified to operate on them? Christos D. Liapis Professor (Em) of Vascular Surgery Athens University Medical School Director Vascular & Endovascular
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department