Calcium Channel Blockers in Management of Hypertension. Yong-Jin Kim, MD Seoul National University Hospital
|
|
|
- Lesley Pearson
- 5 years ago
- Views:
Transcription
1 Calcium Channel Blockers in Management of Hypertension Yong-Jin Kim, MD Seoul National University Hospital
2 Contents Clinical significance of hypertension CCB: Brief introduction Evidences of CCB s in HT and CAD Review on beyond BP lowering effect Practical usefulness of CCB s

3 Headlines of the St. Louis Post-Dispatch, April 13, 1945

4 FDR s Final Picture (April 11, 1945)

5 FDR s BP recorded April 1944
6 Global Burden of CHD Cause Millions (%) Millions (%) CHD Stroke Other CVD TOTAL CVD All Cause Death WHO:WHF
7 Rank Order of Disability (DALYs) 1999 Disease or Injury 2020 Disease or Injury 1. Acute lower respiratory infections 1. Coronary heart disease 2. HIV/AIDS 2. Unipolar major depression 3. Perinatal conditions 3. Road traffic accidents 4. Diarrhoeal diseases 4. Cerebrovascular disease 5. Unipolar major depression 5. COPD 6. Coronary heart disease 6. Lower respiratory infections 7. Cerebrovascular disease 7. Tuberculosis 8. Malaria 8. War 9. Traffic accidents 9. Diarrhoeal diseases 10. COPD 10. HIV
8 HT: A Risk Factor for CV Disease 50 Coronary disease 45.4 Stroke Peripheral artery disease Heart failure Biennial Age- Adjusted Rate per 1000 Patients Risk ratio Men Women Kannel WB. JAMA. 1996;275: Men 3.8 Women 2.6 Normotensive Men 2.0 Women 3.7 Men 4.0 Hypertensive Women 3.0
9 CV Mortality Risk with BP Increment CV Mortality Risk x 4x 2x 115/75 135/85 155/95 175/105 SBP/DBP (mm Hg) *Individuals aged 40 to 69 years, starting at blood pressure 115/75 mm Hg Chobanian AV et al. JAMA. 2003;289: Lewington S et al. Lancet. 2002;360:

10 Small Difference Produces Big Impact Meta-analysis of 61 observational studies 1 million adults For every 2 mm Hg decrease in mean SBP 7% reduction in CHD mortality 10% reduction in stroke mortality Lewington S et al. Lancet. 2002;360:
11 Individual Risk vs Proportional Attributable Risk 5% People with low risk level 70% People with average risk level 25% People with high risk level Individual risk of CHD Distribution of cases
12 Treatment of Hypertension β-blocker JNC 1 JNC Chlorothiazide α-blocker CCB ACEI ARB
13 Contents Clinical significance of hypertension CCB: Brief introduction Evidences of CCB s in HT and CAD Review on beyond BP lowering effect Practical usefulness of CCB s

![[K + ] 140 mm [Na + ] 10 mm [Ca ++ ] 1 µm 0 mv Electrical Gradient [K +](/docs-images/83/87660121/images/14-2.jpg "] 4 mm [Na + ] 140 mm Concentration Gradient [Cl - ] 140 mm [Ca ++ ] 2")
14 Ion Channels and Ion Gradients Ion channel Cl - OH - Ion Exchangers Ca ++ Na + Ca ++ Ion pump ATP Na + HCO - Cl - 3 Ca ++ [Cl - ] 15 mm - 90 mv [K + ] 140 mm [Na + ] 10 mm [Ca ++ ] 1 µm 0 mv Electrical Gradient [K + ] 4 mm [Na + ] 140 mm Concentration Gradient [Cl - ] 140 mm [Ca ++ ] 2 mm



15 Voltage-Dependent Ca ++ Channels Calcium Binding Sites Ca ++ Ca ++ Ca ++ Ca ++ Extracellular Ca ++ Ca ++ Ca ++ Selectivity filter Ca ++ Phosphorylation Site Ca ++ Activation Gate Intracellular P Inactivation Gate



16 Excitation-Contraction Coupling α 2 Actin-myosin interaction Ca ++ -Troponin relieves inhibition on contractile apparatus β VOC δ SR Contraction Ca ++ -induced Ca ++ release L-type Ca ++ channels open at a level of depol. of ~-60 mv. The entry of small Ca ++ triggers Ca ++ release from SR.
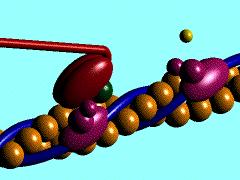
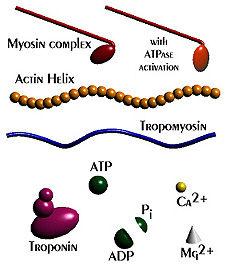
17 Excitation-Contraction Coupling
18 Types of Calcium Channels Channel Blockers Properties Location/Role L type Calcium Large, long-lasting Cardiac & smooth m. antagonists current with neurons; excitationslow activation contraction, excitation-secretion coupling T type Amiloride Tiny, transient SA & Purkinje cell; current pacemaker activity N type Conotoxin Neither L or T Neurons; neurotransmitter release
19 First Observation about CCB in 1964 Developed Tension (g) Developed Tension (g) [Ca ++ ]= 2.4 mm [Ca ++ ]= 0 mm [Ca ++ ]= 2.4 mm [Ca ++ ]= 2.4 mm Verapamil 1 µm Isoproterenol 1µM
20 Classes of L-Type CCB Class I (diphenylalkylamine) Verapamil Isoptin Class II (1,4-dihydropyridines) Amlodipine Felodipine Isradipine Nicardipine Nifedipine Nimodipine Nisoldipine Norvasc, Lotrel Plendil, Lexxel Dynacirc Cardene Adalat, Procardia Nimotop Sular Class III (benzothiazepine) Diltiazem Angizem, Altiazem Class IV (miscellaneous) Bepridil Vascor Class V (T-type blocker) Mibefradil (withdrawn)
21 Pharmacodynamic Effects of CCBs Phenylalkylamine Dihydropyridines Benzothiazepine (Verapamil) (Nifedipine)(Nimodipine) (Diltiazem) Vasodilation peripheral coronary cerebral Heart rate -- SA node AV node Contractility --
22 Classification of CCB s Group First Second generation Third (specificity) generation generation New active principles and/or novel formulations Dihydropyridine Nifedipine Nifedipine Benidipine Amlodipine (artery > cardiac) Nicardipine SR/GITS Isradipine Lacidipine Felodipine ER Manidipine Nicardipine SR Nilvadipine Nimodipine Nisoldipine Nitrendipine Benzothiazepine Diltiazem Diltiazem SR (artery = cardiac) Phenylalkylamine Verapamil Verapamil SR (artery < cardiac) Gallopamil Abbreviations: ER = extended release; GITS = gastrointestinal therapeutic system; SR = sustained release Zanchetti, 1997
23 Contents Clinical significance of hypertension CCB: Brief introduction Evidences of CCB s in HT and CAD Review on beyond BP lowering effect Practical usefulness of CCB s

24 CCB Controversy in 1990 s Circulation 1995
25 Evidences of CCB s in HT, CAD CCB vs Placebo Syst-EUR nitrendipine, Lancet 1997 PREVENT amlodipine, Circulation 2000 ACTION nifedipine GITS, Lancet 2004
26 Syst-EUR Nitrendipine reduces CV events -5% Stroke MI HF All CV events Reduction (%) -15% -25% -35% -30% -29% -31% -45% -42% 4695 Elderly (> 60yr) pts with ISH: SBP>160, DBP<95) Systolic Hypertension in Europe. Staessen et al, Lancet, 1997.
27 Mean Change (mm) PREVENT: Primary QCA Endpoint symptomatic CAD with 3yr f/u Change in Minimum Lumen Diameter (MLD) Primary QCA Endpoint Amlodipine Placebo 30% >30% to 50% >50% All Segments * Values are mean ± SE, adjusted for segment, clinic, and PTCA during baseline angiogram. P=NS for all comparisons of amlodipine versus placebo. Pitt et al. Circulation ;102:
28 PREVENT: Vascular Event or Procedure 30.0 Cumulative Event/ Procedure Rate (%) Placebo (n=408) Amlodipine (n=417) 31% P= Months of Follow-up Pitt et al. Circulation ;102:
29 Evidences of CCB s in HT, CAD CCB vs Active control ABCD nisoldipine vs ACEI, NEJM1998 STOP-2 felodipine or isradipine vs ACEI or diuretic/bb, Lancet 1999 INSIGHT nifedipine GITS vs diuretics, Lancet 2000 ALLHAT amlodipine vs diuretics vs ACEI, JAMA 2002 AASK amlodipine vs BB vs ACEI, JAMA 2002 CONVINCE verapamil vs diuretic/bb, JAMA 2003 CAMELOT amlodipine vs ACEI, JAMA 2004 VALUE amlodipine vs ARB, Lancet 2004
30 Number of Patients International Nifedipine Study enrolled 6321 randomised, eligible for intention-to-treat analysis Long-acting calcium antagonist Nifedipine GITS Diuretic combination: Hydrochlorothiazide & Amiloride ( Active control )
31 International Nifedipine Study 31 Antihypertensive Efficacy Mean Blood Pressure mmhg Nifedipine GITS Hydrochlorothiazide & Amiloride mmhg mmhg Systolic Week 99 mmhg 82 mmhg Diastolic Year 1 Year 2 Year 3 Year 4
32 International Nifedipine Study 32 Sympathetic System Heart Rate 100 Nifedipine GITS Hydrochlorothiazide & Amiloride 80 Beats per Minute Week -4-2/ End Year Year 1 2 Year 3 Year 4
33 International Nifedipine Study 33 Main Clinical Outcome Kaplan Meier Curves Cumulative Proportion Surviving Cumulative Proportion Surviving p = ,200 1,600 2,000 p = ,200 1,600 2,000 Time (Days) Nifedipine GITS Hydrochlorothiazide & Amiloride Myocardial Infarction, Sudden Death, Stroke, Heart Failure, Other Cardiovascular Death (Primary Endpoints) All Cardiovascular Morbidity and All-Cause Mortality (Sum of Primary and Secondary Endpoints)
34 International Nifedipine Study 34 Overview: Individual and Combined Endpoints Relative Risk and 95% Confidence Interval Stroke Myocardial Infarction 0.17 Sudden Death 0.43 Other Cardiovascular Death Heart Failure All Primary Endpoints p All Cardiovascular Morbidity and All-Cause Mortality All Primary and Secondary Endpoints Nifedipine GITS better Hydrochlorothiazide & Amiloride better 1.8

35 Emergence of New Diseases* % of Patients International Nifedipine Study Gout 1 Peripheral Vascular Disorder 1 p < 0.01 p < 0.01 Nifedipine GITS Hydrochlorothiazide & Amiloride Diabetes 2 p = 0.02 *or Recurrence; 1 Reported by investigator; 2 WHO definition of random glucose measurement >11.0 mmol/l or use of anti-diabetic drugs
36 Randomized Design of ALLHAT High-risk hypertensive patients Consent/ Randomize (42,448) Amlodipine besylate mg (n=9048) Chlorthalidone mg (n=15,255) Doxazosin mg (n=9067)* Lisinopril mg (n=9054) Eligible for lipid-lowering lowering Not eligible for lipid-lowering lowering Consent/Randomize (10,355) Pravastatin Usual care Follow for CHD and other outcomes until death or end of study (up p to 8 years). *In January 2000, the National Heart, Lung, and Blood Institute decided d to discontinue the doxazosin arm of the antihypertensive trial and report results. ALLHAT Collaborative Research Group. JAMA ;283: ALLHAT Collaborative Research Group. JAMA ;288:
37 ALLHAT: BP by Treatment Group 150 Chlorthalidone Amlodipine besylate Lisinopril % <140/90 mm Hg 68.2% 66.3% 61.2% 90 mm Hg Systolic BP mm Hg Diastolic BP Years Compared with chlorthalidone: SBP significantly higher in the amlodipine group (0.8 mm Hg) and the lisinopril group (2 mm Hg) at 5 years Years Compared with chlorthalidone: DBP significantly lower in the amlodipine group (0.8 mm Hg) at 5 years ALLHAT Collaborative Research Group. JAMA. 2002;288:
38 ALLHAT: Fatal CHD or Nonfatal MI Cumulative CHD Event Rate Number at Risk: Chlorthalidone Amlodipine Lisinopril , A/C L/C 14, RR (95% CI) 0.98 ( ) 0.99 ( ) Chlorthalidone Amlodipine besylate Lisinopril 13, P Value Years to CHD Event 13, , ALLHAT Collaborative Research Group. JAMA. 2002;288:
39 Rollover from previous therapy (92%) VALUE: Design HT pt with elective e titration to target BP Valsartanbased regimen V 80 mg A 5 mg Amlodipinebased regimen V 160 mg A 10 mg V 160 mg + HCTZ 12.5 mg A 10 mg + HCTZ 12.5 mg V 160 mg + HCTZ 25 mg A 10 mg + HCTZ 25 mg V 160 mg + HCTZ 25 mg + "Free" add-on A 10 mg + HCTZ 25 mg + "Free" add-on Month * 72 Screening Randomisation *Patient visits every 6 months for months Julius S et al. Lancet.. June 2004;363. End of treatment adjustment period
40 VALUE: Primary Composite Endpoint Proportion of Patients With First Event (%) Number at risk Julius et al. Lancet.. June 2004; Valsartan-based regimen Amlodipine besylate -based regimen HR=1.03; 95% CI : P= Time (months) Valsartan Amlodipine besylate
41 VALUE: Fatal and Non-Fatal MI Proportion of Patients With First Event (%) Valsartan-based regimen Amlodipine besylate-based based regimen HR=1.19; 95% CI ; 1.38; P= Time (months) Number at risk Valsartan Amlodipine besylate % Julius S et al. Lancet.. June 2004;363.
42 VALUE: Fatal and Non-fatal Stroke Proportion of Patients With First Event (%) Valsartan-based regimen Amlodipine besylate-based based regimen HR=1.15; 95% CI ; P=0.08 Number at risk Time (months) Valsartan Amlodipine besylate Julius S et al. Lancet.. June 2004;
43 VALUE: Systolic BP in Study mmhg mmhg Julius S et al. Lancet.. June 2004;363. Sitting SBP by Time and Treatment Group Valsartan (N=7649) Amlodipine besylate (N=7596) 135 Baseline Months (or final visit) Difference in SBP Between Valsartan and Amlodipine besylate Months (or final visit)
44 VALUE: Outcome and SBP Differences Time Interval SBP (months) mm Hg Overall study Study end 1.7 PRIMARY ENDPOINT Odds Ratios and 95% CIs Favours valsartan Favours amlodipine besylate Julius S et al. Lancet.. June 2004;363.

45 VALUE: Outcome and SBP Differences

46 New ESC Guideline: Early Treatment
47 BP-Lowering Treatment Trialists Comparisons of Active Treatments and Control BP Difference (mm Hg) Relative Risk Favors Favors Active Control Blood Pressure Lowering Treatment Trialists Collaboration. Lancet ;362: RR (95% CI) Stroke ACEI vs placebo -5/ 5/ (0.64, 0.81) CA vs placebo -8/ 8/ (0.47, 0.82) Coronary heart disease ACEI vs placebo -5/ 5/ (0.73, 0.88) CA vs placebo Heart failure ACEI vs placebo -8/ 8/-4-5/ 5/ (0.62, 0.99) 0.82 (0.69, 0.98) CA vs placebo -8/ 8/ (0.93, 1.58) Major CV events ACEI vs placebo -5/ 5/ (0.73, 0.83) CA vs placebo -8/ 8/ (0.71, 0.95) CV mortality ACEI vs placebo -5/ 5/ (0.71, 0.89) CA vs placebo -8/ 8/ (0.61, 1.00) Total mortality ACEI vs placebo -5/ 5/ (0.81, 0.96) CA vs placebo -8/ 8/ (0.75, 1.05)
48 Stroke CHD HF BP-Lowering Treatment Trialists Comparisons of Different Active Treatments BP Difference (mm Hg) ACE Inhibitor vs D/BB 2/0 CA vs D/BB 1/0 ACE Inhibitor vs CA 1/1 ACE Inhibitor vs D/BB 2/0 CA vs D/BB 1/0 ACE Inhibitor vs CA 1/1 ACE Inhibitor vs D/BB 2/0 Relative Risk 0.5 Favors 1.0 Favors 2.0 First Listed Second Listed RR (95% CI) 1.09 (1.00, 1.18) 0.93 (0.86, 1.01) 1.12 (1.01, 1.25) 0.98 (0.91, 1.05) 1.01 (0.94, 1.08) 0.96 (0.88, 1.05) 1.07 (0.96, 1.19) CA vs D/BB 1/ (1.21, 1.47) ACE Inhibitor vs CA 1/ (0.73, 0.92) Blood Pressure Lowering Treatment Trialists Collaboration. Lancet ;362:
49 BP-Lowering Treatment Trialists Comparisons of Different Active Treatments BP Difference (mm Hg) Relative Risk RR (95% CI) Major CV events ACEI vs D/BB CA vs D/BB ACEI vs CA CV mortality ACEI vs D/BB CA vs D/BB ACEI vs CA Total mortality ACEI vs D/BB CA vs D/BB ACEI vs CA 2/0 1/0 1/1 2/0 1/0 1/1 2/0 1/0 1/ (0.98, 1.07) 1.04 (0.99, 1.08) 0.97 (0.92, 1.03) 1.03 (0.95, 1.11) 1.05 (0.97, 1.13) 1.03 (0.94, 1.13) 1.00 (0.95, 1.05) 0.99 (0.95, 1.04) 1.04 (0.98, 1.10) Blood Pressure Lowering Treatment Trialists 0.5 Favors 1.0 Favors 2.0 First Listed Second Listed Trialists Collaboration. Lancet ;362:
50 Contents Clinical significance of hypertension CCB: Brief introduction Evidences of CCB s in HT and CAD Review on beyond BP lowering effect Practical usefulness of CCB s
51 HOPE Trial 9,297 pt with CAD or DM plus 1 RF (no CHF, LV dysfxn) 75% Aspirin, 40% beta-blocker, 30% statin Ramipril 10mg/day n=4,645 Placebo n=4,652 Primary Endpoint Composite of cardiac death, MI, or stroke follow-up: 5 years The HOPE investigators. N Engl J Med 2000 ; 342 :
52 HOPE: Primary Endpoint cardiac death, MI, or stroke Primary endpoints (%) RRR = 28% p < Placebo Ramipril days The HOPE investigators. N Engl J Med 2000 ; 342 :
53 HOPE: Events per Patient Group Events per Patient Group (%) RR=22% P< RR=26% P< Placebo RR=20% P< RR=32% P< Ramipril RR=0% P=NS RR=16% P= Primary CV Outcome Death *MI, stroke, or CV death. Yusuf et al. N Engl J Med ;342: MI Stroke Non- CV Death Total Mortality
54 Ambulatory BP in HOPE Trial BP (mm Hg) SBP baseline DBP baseline Svensson et al. Hypertension. 2001;38:e28-e32. e32. SBP year 1 DBP year 1 Ramipril Group (n=20) Night =17/8 mm Hg (P<.001)( 24-h =10/4 mm Hg (P<.03)( Time (hours)
55 EUROPA Trial 12,218 patients with stable angina without CHF 90% Aspirin, 60% beta-blocker, 60% statin Perindopril 8mg/day n=6,110 Placebo n=6,108 Primary Endpoint Composite of cardiac death, MI, or cardiac arrest mean follow-up: 4.2 years Lancet 2003; 362:

56 EUROPA: Primary Endpoint % CV death, MI or cardiac arrest Placebo annual event rate : 2.4% Placebo Perindopril % 12% 14% RRR: 20% p = Years Lancet 2003; 362:
57 CAD Mortality and Usual BP by Age Systolic BP Diastolic BP IHD Mortality (Floating Absolute Risk and 95% CI) years years years years years years years years years years Usual Systolic BP (mm Hg) Usual Diastolic BP (mm Hg) Prospective Studies Collaboration. Lancet ;360:
58 Stroke Mortality and Usual BP by Age Systolic BP Diastolic BP Stroke Mortality (Floating Absolute Risk and 95% CI) years years years years years years years years Usual Systolic BP (mm Hg) Usual Diastolic BP (mm Hg) Prospective Studies Collaboration. Lancet ;360:
59 Odds Ratio for CV Events & SBP Difference Odds Ratio (Experimental/Reference) Difference (reference minus experimental) in Systolic BP (mm Hg) Staessen et al. J Hypertens ;21: Recent trials Older trials placebo Older trials active HOPE P<.0001 Recent AASK L vs H ABCD/NT L vs H ALLHAT/Aml Aml ALLHAT/Lis ALLHAT/Lis 65 ALLHAT/Lis Blcks ANBP2 CONVINCE DIABHYCAR ELSA IDNT2 LIFE/ALL LIFE/DM NICOLE PREVENT SCOPE Older ALLHAT/Dox ATMH EWPHE HEP HOPE HOT HOT M vs H INSIGHT MIDAS/NICS/VHAS L vs H MRC MRC2 PART2/SCAT PATS PROGRESS/Per PROGRESSION/Com RCT70-80 RENAAL SHEP STONE STOP 1 STOP2/CCBs STOP2/ACEIs Syst-China Syst-Eur UKPDS C vs A UKPDS L vs H
60 Odds Ratio for CV Events & SBP Difference Odds Ratio (Experimental/Reference) Recent trials Older trials placebo Older trials active EUROPA P< Difference (reference minus experimental) in Systolic BP (mm Hg) Recent AASK L vs H ABCD/NT L vs H ALLHAT/Aml Aml ALLHAT/Lis ALLHAT/Lis 65 ALLHAT/Lis Blcks ANBP2 CONVINCE DIABHYCAR ELSA IDNT2 LIFE/ALL LIFE/DM NICOLE PREVENT SCOPE Fox. Lancet. 2003;362: ; 788; Staessen et al. J Hypertens ;21: Older ALLHAT/Dox ATMH EWPHE HEP HOPE HOT HOT M vs H INSIGHT MIDAS/NICS/VHAS L vs H MRC MRC2 PART2/SCAT PATS PROGRESS/Per PROGRESSION/Com RCT70-80 RENAAL SHEP STONE STOP 1 STOP2/CCBs STOP2/ACEIs Syst-China Syst-Eur UKPDS C vs A UKPDS L vs H
61 Target BP in HT JNC 7, /90-130/80: DM, renal disease ESC guideline, /90-130/80: DM, established CV ds ( stroke, MI, renal ds)
62 BP-Lowering Treatment Trialists 1.50 Stroke CHD A B C D E F G A B C D E F G 1.50 RR of Outcome Event RR of Outcome Event SBP Difference Between (mm Hg) SBP Difference Between (mm Hg) A = CA vs placebo; B = ACE inhibitor vs placebo; C = more intensive vs less intensive blood- pressure- lowering; D = ARB vs control; E = ACE inihibitor vs CA; F = CA vs diuretic or β-blocker; G = ACE inhibitor vs diuretic and β-blocker. Blood Pressure Lowering Treatment Trialists Collaboration. Lancet ;362:
63 BP-Lowering Treatment Trialists 1.50 Heart Failure A B C D E F G RR of Outcome Event SBP Difference Between Groups (mm Hg) A = CA vs placebo; B = ACE inhibitor vs placebo; C = more intensive vs less intensive blood- pressure- lowering; D = ARB vs control; E = ACE inihibitor vs CA; F = CA vs diuretic or β-blocker; G = ACE inhibitor vs diuretic and β-blocker. Blood Pressure Lowering Treatment Trialists Collaboration. Lancet ;362:
64 Regimens based on each of the most commonly used drug classes produce reductions in the risk of major cardiovascular events that appear to be roughly proportional to the size of the blood pressure reductions achieved With the exception of heart failure, the intensity of blood pressure lowering appears to be a more important determinant of outcome than the choice of drug class. BP Lowering Treatment Trialists Collaboration, The Lancet (2003)

65 Target BP lowering in ALLHAT
66 Adequate BP Control First!

67 Adequate BP Control First! source: National health and nutrition examination survey, 2005
68 CVD Survival in Treated HT Untreated BP <140/90 mm Hg Untreated BP 140/90 mm Hg Treated BP at goal <140/90 mm Hg Treated BP not at goal 140/90 mm Hg 1 Survival (%) P=.03 P<.0001 P= Follow-up (Years) Benetos et al. J Hypertens ;21:
69 Contents Clinical significance of hypertension CCB: Brief introduction Evidences of CCB s in HT and CAD Review on beyond BP lowering effect Practical usefulness of CCB s
70 No. of agents to Achieve BP Goal UKPDS (<85 mm Hg, diastolic) MDRD (<92 mm Hg, MAP) HOT (<80 mm Hg, diastolic) AASK (<92 mm Hg, MAP) RENAAL (<140/90 mm Hg) IDNT ( 135/85 mm Hg) 1 2 Number of BP Medications 3 4 Bakris et al. Am J Kidney Dis ;36: ; 661; Bakris et al. Arch Intern Med. 2003;163: ; 1565; Lewis et al. N Engl J Med ;345:
71 Combination Therapy in Korea >4 drugs drugs 2 drugs Monotherapy Note: * Consider small base number for implementation especially when n<30
72 Effect of CCB for Add-on Therapy 0 No Previous Therapy (n=421) ACEI/ARB (n=117) β-blocker (n=70) Diuretic (n=119) ACE/ARB + diuretic (n=165) β-blocker + diuretic (n=47) SBP mm Hg SBP mm Hg *The DHP CCB was Norvasc (amlodipine besylate). P<.001 vs baseline. McLaughlin et al. Am J Hypertens ;16:123A. Abstract P-237. P

73 Guideline on Combination Therapy Thiazide BB ARB Alpha CCB ACEI ESC guideline 2007
74 Summary CCB: strong evidences in management in HT Benefit of HT drugs: mainly from BP lowering effect Early initiation of HT drug: high risk patients Importance of BP lowering at goal
75

76 Thank You for Your Attention!
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
How to Achieve Better Cardiovascular Outcome in Hypertensive Patients. Seoul National University Hospital
 How to Achieve Better Cardiovascular Outcome in Hypertensive Patients t Yong-Jin Kim, MD Seoul National University Hospital Global Burden of CV Disease Cause 1990 2020 Millions (%) Millions (%) CHD 6.2
How to Achieve Better Cardiovascular Outcome in Hypertensive Patients t Yong-Jin Kim, MD Seoul National University Hospital Global Burden of CV Disease Cause 1990 2020 Millions (%) Millions (%) CHD 6.2
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Received 23 March 2003 Revised 6 April 2003 Accepted 9 April 2003
 Original article 1055 Cardiovascular prevention and blood pressure reduction: a quantitative overview updated until 1 March 2003 Jan A. Staessen, Ji-Guang Wang and Lutgarde Thijs Background In a meta-analysis
Original article 1055 Cardiovascular prevention and blood pressure reduction: a quantitative overview updated until 1 March 2003 Jan A. Staessen, Ji-Guang Wang and Lutgarde Thijs Background In a meta-analysis
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
Blood Pressure Targets in Diabetes
 Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Large therapeutic studies in elderly patients with hypertension
 (2002) 16 (Suppl 1), S38 S43 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh Large therapeutic studies in elderly patients with hypertension Centro Clinico Profesional
(2002) 16 (Suppl 1), S38 S43 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh Large therapeutic studies in elderly patients with hypertension Centro Clinico Profesional
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management
 Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Drug Class Review on Calcium Channel Blockers FINAL REPORT
 Drug Class Review on Calcium Channel Blockers FINAL REPORT September 2003 TABLE OF CONTENTS Introduction 5 Scope and Key Questions 6 Methods 6 Literature Search 6 Study Selection 6 Data Abstraction 7 Validity
Drug Class Review on Calcium Channel Blockers FINAL REPORT September 2003 TABLE OF CONTENTS Introduction 5 Scope and Key Questions 6 Methods 6 Literature Search 6 Study Selection 6 Data Abstraction 7 Validity
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Drug Class Review on Calcium Channel Blockers
 Drug Class Review on UPDATED FINAL REPORT #1 April 2004 Marian S. McDonagh, PharmD Karen B. Eden, PhD Kim Peterson, MS Oregon Evidence-based Practice Center Oregon Health & Science University Table of
Drug Class Review on UPDATED FINAL REPORT #1 April 2004 Marian S. McDonagh, PharmD Karen B. Eden, PhD Kim Peterson, MS Oregon Evidence-based Practice Center Oregon Health & Science University Table of
Abbreviations Cardiology I
 Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
CCB Reappraisal CCB as the first line for the East-Asians
 CCB Reappraisal CCB as the first line for the East-Asians Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School 일본의국화 ( 國花 ) 는? www.themegallery.com LOGO 일본 ( 日本
CCB Reappraisal CCB as the first line for the East-Asians Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School 일본의국화 ( 國花 ) 는? www.themegallery.com LOGO 일본 ( 日本
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Rationale for the use of Single Pill Combination. Yong Jin Kim, MD Seoul National University Hospital
 Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
BLOOD PRESSURE-LOWERING TREATMENT
 BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
GOING BEYOND HYPERTENSION CONTROL
 From bench to practice: hypertension control GOING BEYOND HYPERTENSION CONTROL Prof. Dr. Maria DOROBANTU, FESC,FACC CAROL DAVILA UNIVERSITY OF MEDICINE OF BUCHAREST EMERGENCY HOSPITAL OF BUCHAREST, CARDIOLOGY
From bench to practice: hypertension control GOING BEYOND HYPERTENSION CONTROL Prof. Dr. Maria DOROBANTU, FESC,FACC CAROL DAVILA UNIVERSITY OF MEDICINE OF BUCHAREST EMERGENCY HOSPITAL OF BUCHAREST, CARDIOLOGY
Ferrari R, Fox K, Bertrand M, Mourad J.J, Akkerhuis KM, Van Vark L, Boersma E.
 Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Can Anti-hypertension Therapy Reverse Vascular Aging and Dementia?
 2012. 4. 20-21 춘계심장학회 _ 부산 Can Anti-hypertension Therapy Reverse Vascular Aging and Dementia? Jeong Bae Park, MD, PhD Cardiology, Cheil General Hospital, Kwandong University, Seoul, Korea The Pulse : revived
2012. 4. 20-21 춘계심장학회 _ 부산 Can Anti-hypertension Therapy Reverse Vascular Aging and Dementia? Jeong Bae Park, MD, PhD Cardiology, Cheil General Hospital, Kwandong University, Seoul, Korea The Pulse : revived
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS
 HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Caring for Australians with Renal Impairment. BP lowering and CVD
 Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
First line treatment of primary hypertension
 First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico
 Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
The target blood pressure in patients with diabetes is <130 mm Hg
 Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
47 Hypertension in Elderly
 47 Hypertension in Elderly YOU DO NOT HEAL OLD AGE; YOU PROTECT IT; YOU PROMOTE IT; YOU EXTEND IT Sir James Sterling Ross Abstract: The prevalence of hypertension rises with age and the complications secondary
47 Hypertension in Elderly YOU DO NOT HEAL OLD AGE; YOU PROTECT IT; YOU PROMOTE IT; YOU EXTEND IT Sir James Sterling Ross Abstract: The prevalence of hypertension rises with age and the complications secondary
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
HYPERTENSION IN THE ELDERLY A BALANCED APPROACH. Barry Goldlist October 31, 2014
 HYPERTENSION IN THE ELDERLY A BALANCED APPROACH Barry Goldlist October 31, 2014 DISCLOSURE I have not accepted any money for myself from any pharmaceutical company in the 21 st century I have accepted
HYPERTENSION IN THE ELDERLY A BALANCED APPROACH Barry Goldlist October 31, 2014 DISCLOSURE I have not accepted any money for myself from any pharmaceutical company in the 21 st century I have accepted
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Amlodipine and cardiovascular outcomes in hypertensive patients: meta-analysis comparing amlodipine-based versus other antihypertensive therapy
 ORIGINAL ARTICLE Korean J Intern Med 2014;29:315-324 and cardiovascular outcomes in hypertensive patients: meta-analysis comparing amlodipine-based versus other antihypertensive therapy Seung-Ah Lee 1,
ORIGINAL ARTICLE Korean J Intern Med 2014;29:315-324 and cardiovascular outcomes in hypertensive patients: meta-analysis comparing amlodipine-based versus other antihypertensive therapy Seung-Ah Lee 1,
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey