Hypertension Management Focus on new RAAS blocker. Disclosure
|
|
|
- Rosanna Bishop
- 6 years ago
- Views:
Transcription
1 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay pharmaceuticals
2 JNC 7 blood pressure classification in adults aged 18 years BP Classification SBP (mm HG) DBP (mm HG) Normal <120 and <80 Prehypertension or Stage 1 hypertension Stage 2 hypertension or or 100 National Heart, Lung, and Blood Institute. JNC 7 Express. The Seventh Report of the Joint National Committee Hypertension on the Online Prevention, Detection, Evaluation and Treatment of High Blood Pressure % Prevalence of Hypertension in the United States by Age Group * Hypertension Prevalence Age 80% 60% 40% 20% 0% 6% 16% 31% 48% 65% 78% *Based on data from the National Health and Nutrition Examination Survey. Hypertension is defined as blood pressure 140/90 mm Hg or as receiving antihypertensive treatment. Low reliability due to large relative error. Fields LE, et al. Hypertension. 2004;44:

3 Lifetime Risk of Developing Hypertension Among Adults at 65 Years of Age * Risk of Hypertension (%) Men Years *Residual lifetime risk of developing hypertension among adults at 65 years of age with a blood pressure <140/90 mm Hg. Women Vasan RS, et al. JAMA. 2002;287:

4 Adults (%) Hypertension Control Rates Are Slowly Improving (NHANES Data) *Controlled blood pressure was defined as <140/90 mm Hg and expressed as a % of all hypertensives. NHANES = National Health and Nutrition Examination Survey. Chobanian AV, et al. JAMA. 2003;289: ; Ong KL, et al. Hypertension. 2007;49: Treatment Controlled*

5 Cardiovascular Mortality Risk Cardiovascular Mortality Risk Increases as Blood Pressure Rises * 2x 4x 8x 115/75 135/85 155/95 175/105 Systolic/Diastolic Blood Pressure (mm Hg) * Measurements taken in individuals aged years, beginning with a blood pressure of 115/75 mm Hg. Lewington S, et al. Lancet. 2002;360: ; Chobanian AV, et al. JAMA. 2003;289:













6 Complications of Hypertension: End-Organ Damage Hypertension Hemorrhage, Stroke LVH, CHD, CHF Retinopathy CHD = coronary heart disease CHF = congestive heart failure LVH = left ventricular hypertrophy Chobanian AV, et al. JAMA. 2003;289: Peripheral Vascular Disease Renal Failure, Proteinuria Relationship of Hypertension to Its Comorbidities Comorbidity Coronary artery disease Left ventricular hypertrophy Ischemic stroke Chronic kidney disease Diabetes Peripheral artery disease Relationship to Hypertension 50% of patients with coronary artery disease have hypertension 15% to 20% of hypertensive adults have an increased left ventricular mass 77% of patients who have a first stroke have a blood pressure >140/90 mm Hg 8% to 15% of hypertensive adults have decreased renal function 75% of added cardiovascular risk in diabetic patients is attributable to hypertension 74% of patients with peripheral artery disease have hypertension Diamond JA, Phillips RA. Hypertens Res. 2005;28: ;El-Atat F, et al. Curr Hypertens Rep. 2004;6: ; Pepine CJ. Am J Cardiol. 1998;82(3A):21H- 24H; Rosamond W, et al. Circulation. 2007;115:69-171; Segura J, et al. Curr Opin Nephrol Hypertens. 2004;13: ; Selvin E, Erlinger P. Circulation. 2004;110:
 <120 120 139 140 159 160 179 180 199 200 Systolic Blood Pressure (mm Hg) MRFIT = Multiple Risk Factor Intervention Trial Stamler J, et al. Diabetes Care.")
7 Diabetes Increases Hypertension-Related Cardiovascular Risk: MRFIT Cardiovascular Mortality Rate per 10,000 Person-Years Nondiabetic Men (n = 342,815) Diabetic Men (n = 5,163) < Systolic Blood Pressure (mm Hg) MRFIT = Multiple Risk Factor Intervention Trial Stamler J, et al. Diabetes Care. 1993;16:
8 Current Blood Pressure Targets for Various Chronic Conditions Uncomplicated Hypertension Systolic Blood Pressure Chronic Kidney Disease Coronary Artery Disease Diabetes Diastolic Blood Pressure mm Hg American Diabetes Association. Diabetes Care. 2003;26:S80-S82; Hansson L, et al. Lancet. 1998;351: ; National Kidney Foundation. Am J Kidney Dis. 2002;39(2 Suppl 1):S1-S266; Rosendorff C, et al. Circulation. 2007;115: Patient Evaluation Evaluation of patients with documented HTN has three objectives: 1. Assess lifestyle and identify other CV risk factors or concomitant disorders that affects prognosis and guides treatment. 2. Reveal identifiable causes of high BP. 3. Assess the presence or absence of target organ damage and CVD.
9 Target Organ Damage Heart Left ventricular hypertrophy Angina or prior myocardial infarction Prior coronary revascularization Heart failure Brain Stroke or transient ischemic attack Chronic kidney disease Peripheral arterial disease Retinopathy Laboratory Tests Routine Tests Electrocardiogram Urinalysis Blood glucose, and hematocrit Serum potassium, creatinine, or the corresponding estimated GFR, and calcium Lipid profile, after 9- to 12-hour fast, that includes high-density and low-density lipoprotein cholesterol, and triglycerides Optional tests Measurement of urinary albumin excretion or albumin/creatinine ratio More extensive testing for identifiable causes is not generally indicated unless BP control is not achieved


10 Development of Antihypertensive Therapies Classes of Antihypertensive Drugs Aldosterone receptor antagonists (blockers) Angiotensin II antagonists Angiotensin-converting enzyme inhibitors α-blockers α 1 -Selective Nonselective β-blockers β-1/β-2 β-1 predominant α/β Intrinsic sympathomimetic activity Calcium channel antagonists Nondihydropyridine Dihydropyridine Central α 2 agonists Direct renin inhibitors Direct vasodilators Diuretics Thiazide-type Loop-type Potassium-sparing Ganglionic blockers
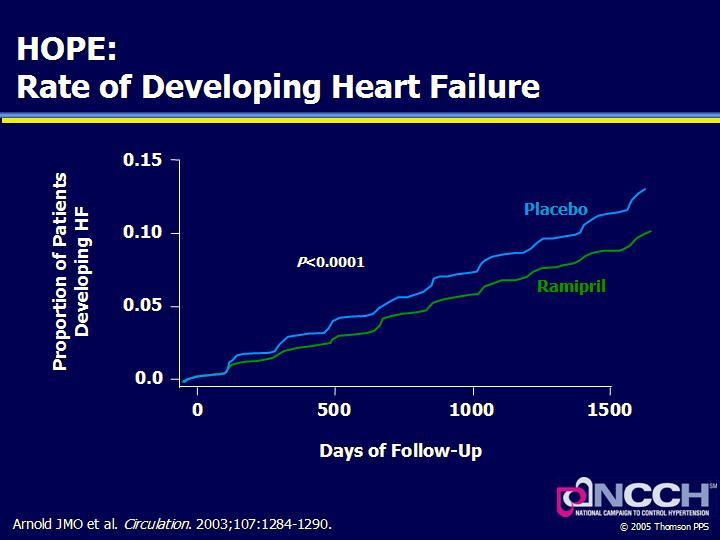
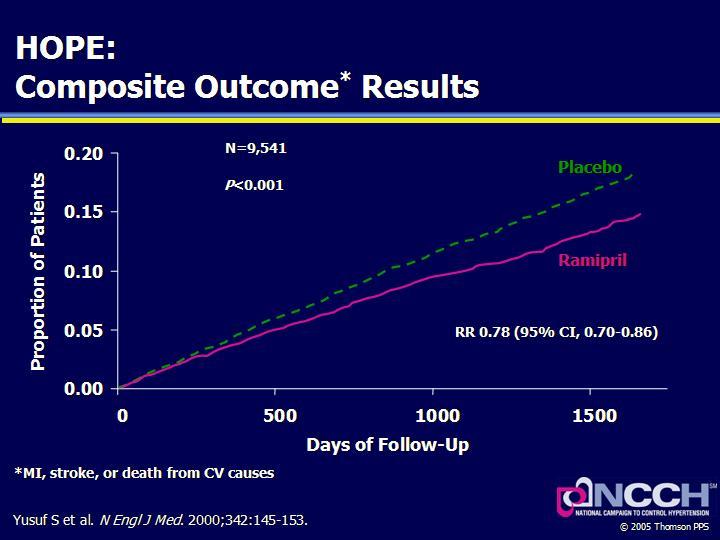
11 Antihypertensive Drug Classes: Action Sites Blood Pressure = Cardiac Output Total Peripheral Resistance Antihypertensive Drug Classes β-blockers Non-DHP CCBs Diuretics β-blockers ACE Inhibitors AT 1 Blockers Direct renin inhibitors α 1 -Blockers α 2 -Agonists All CCBs Diuretics Sympatholytics Vasodilators ACE = angiotensin-converting enzyme; AT 1 = angiotensin type 1; CCBs = calcium channel blockers; DHP = dihydropyridine Compelling Indications for Individual Drug Classes Compelling Indication Initial Therapy Options Clinical Trial Basis Heart failure Postmyocardial infarction High CAD risk THIAZ, BB, ACEI, ARB, ALDO ANT BB, ACEI, ALDO ANT THIAZ, BB, ACE, CCB ACC/AHA Heart Failure Guideline, MERIT-HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, ValHEFT, RALES ACC/AHA Post-MI Guideline, BHAT, SAVE, Capricorn, EPHESUS ALLHAT, HOPE, ANBP2, LIFE, CONVINCE
12 Compelling Indications for Individual Drug Classes Compelling Indication Initial Therapy Options Clinical Trial Basis Diabetes Chronic kidney disease THIAZ, BB, ACE, ARB, CCB ACEI, ARB NKF-ADA Guideline, UKPDS, ALLHAT NKF Guideline, Captopril Trial, RENAAL, IDNT, REIN, AASK Recurrent stroke prevention THIAZ, ACEI PROGRESS JNC-7 7 Report: Treatment Algorithm Initial Drug Choices No Compelling Indication Stage 1 HTN SBP mm Hg, DBP mm Hg Usually thiazide-type diuretic Also consider ACEI, ARB, BB, or CCB alone or in combination Stage 2 HTN SBP 160 mm Hg, DBP 100 mm Hg 2-drug combination Usually thiazide-type diuretic and ACEI, ARB, BB, or CCB ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; BB = β-blocker; CCB = calcium channel blocker; DBP = diastolic blood pressure; HTN = hypertension; JNC = Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure; SBP = systolic blood pressure Chobanian AV, et al. JAMA. 2003;289:
13 Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP <140/90 mmhg or BP <130/80 mmhg in patients with diabetes or chronic kidney disease. Achieve SBP goal especially in persons >50 years of age. Lifestyle Modification Modification Weight reduction Adopt DASH eating plan Dietary sodium reduction Physical activity Approximate SBP reduction (range) 5 20 mmhg/10 kg weight loss 8 14 mmhg 2 8 mmhg 4 9 mmhg Moderation of alcohol consumption 2 4 mmhg
14 Benefits of Lowering BP Average Percent Reduction Stroke incidence 35 40% Myocardial infarction 20 25% Heart failure 50% Causes of Resistant Hypertension Improper BP measurement Excess sodium intake Inadequate diuretic therapy Medication Inadequate doses Drug actions and interactions (e.g., nonsteroidal anti-inflammatory (NSAIDs), illicit drugs, sympathomimetics, oral contraceptives) Over-the-counter (OTC) drugs and herbal supplements Excess alcohol intake Identifiable causes of HTN drugs

15 Physiology of RAAS Bradykinin ACE Angiotensinogen Angiotensin I Angiotensin II Renin Aldosterone Angiotensin III Angiotensin IV Angiotensin II Receptor Goodfriend et al. N Engl J Med ;334: PRA is Correlated With RAAS Activation Plasma renin activity (PRA) is a measure of the conversion of angiotensinogen to ANG1 Elevated PRA is correlated to increased levels of ANG 1 and ANG 2 and therefore is a marker for RAAS activation
16 Consequences of Overactivation of RAAS ANG II is the metabolically active end product of RAAS Increases vasoconstrictiom Increases renal sodium reabsorption Stimulates aldosterone and antidiuretic hormone secretion Angiotensin II as a Cardiac and Renal Toxin Angiotensin Renin Chymase Cathepsin G Carboxypeptidase ARB Ang I Ang II ACEI Bradykinin Inactive Fragments AT 1 R Aldosterone Reactive O 2 Species Cell Growth Sympathetic Activation Renal Na +, H 2 O Vasoconstriction Cardiac, Vascular, Collagen CHF Renal Hypertrophy Carey et al. Endocr Rev ;24:
:S9-S17; S17; Engeli et al. Int J Biochem Cell Biol.")
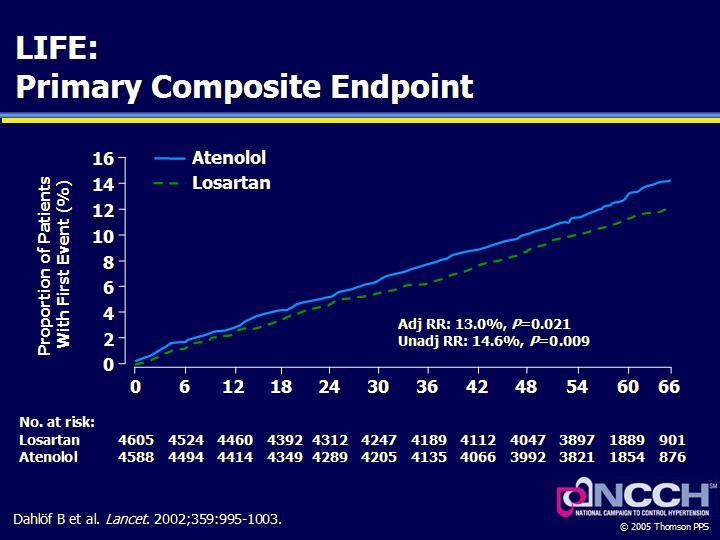
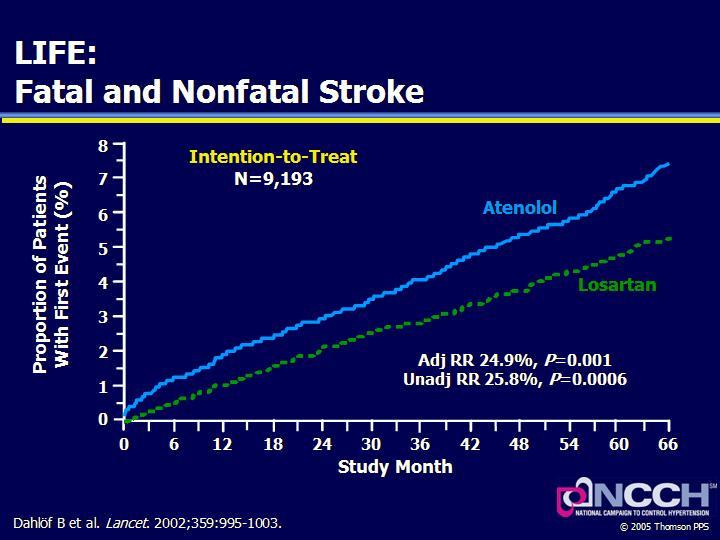
17 Inappropriate RAAS Activation as a Cause of Impaired Vascular and Metabolic Health Angiotensin II Endothelial Dysfunction Vascular Remodeling Impaired Adipogenesis Elevated BP Atherosclerosis Glucose Intolerance Brasier et al. Arterioscler Thromb Vasc Biol. 2002;22: ; 1266; Dzau. J Hypertens. 2005;23(suppl 1):S9-S17; S17; Engeli et al. Int J Biochem Cell Biol. 2003;35: ; 825; Taniyama et al. Hypertension ;43: Studies investigating effects of RAAS manipulation on CV disease outcomes ACE inhibition Angiotensin receptor blockade GISSI-3 ISIS-4 Myocardial ischemia Coronary thrombosis Myocardial Infarction LV Dysfunction Arrhythmia AIRE SAVE SOLVD-Prevention TRACE CHARM-Preserved OPTIMAAL VALIANT HOPE EUROPA CAD Remodeling ALLHAT ANBP2 ASCOT INVEST LIFE VALUE Atherosclerosis LVH Hypertension Adapted from: Dzau V, et al. Am Heart J. 1991;121: End-stage heart disease Ventricular dilation Heart failure SOLVD-Treat CHARM-Added CHARM-Alternative ELITE II Val-HeFT CONSENSUS
18
19
20

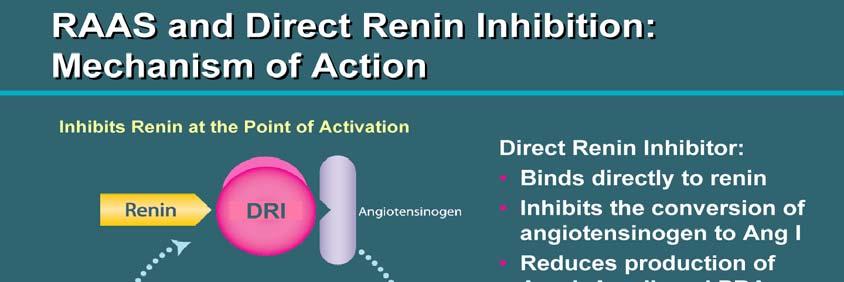
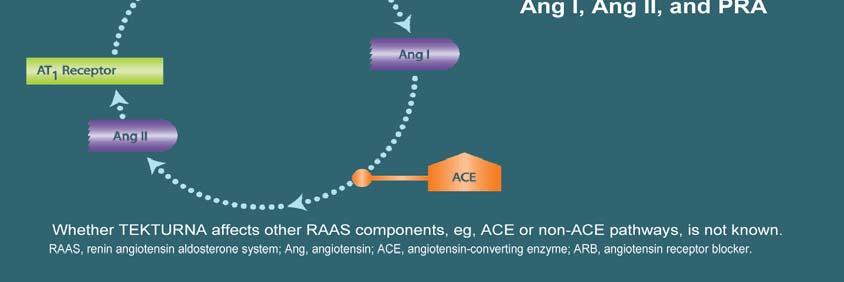
21 RAAS and Direct Renin Inhibition: Mechanism of Action



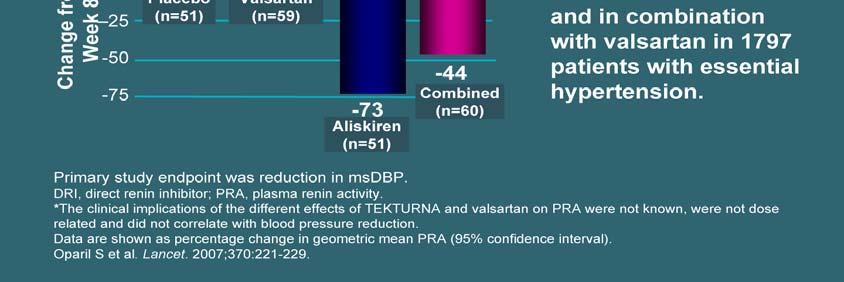
22 Aliskiren Reduced PRA, Alone and in Combination With Ramipril* Aliskiren Reduced PRA Alone and in Combination With Valsartan*




23 TEKTURNA Monotherapy: Powerful BP Reductions (at 8 Weeks) TEKTURNA 300 mg Combined With HCTZ 25 mg: 50% More SBP Efficacy




24 TEKTURNA Combined With Ramipril: Study Trial Design TEKTURNA Combined With Ramipril: Study Results




25 TEKTURNA Combined With an ARB: Study Trial Design TEKTURNA Combined With an ARB: 30% Greater Efficacy With Combination Therapy


26 Summary of Clinical Experience to Date With TEKTURNA Conclusion Benefits of reducing blood pressure on risks of major cardiovascular disease are well established Commonly used antihypertensive medications reduce major CV events by % Large blood pressure reductions correlate with larger reductions of major CV events.
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Strategies for Managing Hypertension
 Strategies for Managing Hypertension by Marsha K. Millonig, MBA, RPh President,Catalyst Enterprises, LLC E.L.F. Publications, Inc. is accredited by the Accreditation Council for Pharmacy Education as a
Strategies for Managing Hypertension by Marsha K. Millonig, MBA, RPh President,Catalyst Enterprises, LLC E.L.F. Publications, Inc. is accredited by the Accreditation Council for Pharmacy Education as a
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension and Diabetes Will Controversies Help Our Patients? Insights of JNC Report Jorge De Jesús MD FACE
 Hypertension and Diabetes Will Controversies Help Our Patients? Insights of JNC8 2013 Report Jorge De Jesús MD FACE Disclosures Dr Jorge De Jesús has received honorariums as speaker for the following pharmaceutical
Hypertension and Diabetes Will Controversies Help Our Patients? Insights of JNC8 2013 Report Jorge De Jesús MD FACE Disclosures Dr Jorge De Jesús has received honorariums as speaker for the following pharmaceutical
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Management of Hypertension in the Diabetic Patient:
 Management of Hypertension in the Diabetic Patient: Nicolas W. Shammas, MS, MD Research Director, Cardiovascular Medicine, PC Presentation Objectives To review: The relationship between HTN, insulin resistance
Management of Hypertension in the Diabetic Patient: Nicolas W. Shammas, MS, MD Research Director, Cardiovascular Medicine, PC Presentation Objectives To review: The relationship between HTN, insulin resistance
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Hypertension in Clinical Practice. Abeer Al Saweer, MBBS, Arab Board*
 1 Bahrain Medical Bulletin, Vol. 33, No. 1, March 2011 Education-Family Physician Corner Hypertension in Clinical Practice Abeer Al Saweer, MBBS, Arab Board* The global incidence of hypertension is growing.
1 Bahrain Medical Bulletin, Vol. 33, No. 1, March 2011 Education-Family Physician Corner Hypertension in Clinical Practice Abeer Al Saweer, MBBS, Arab Board* The global incidence of hypertension is growing.
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Στόχοι αρτηριακής πίεσης σε ειδικούς πληθυσµούς και επιλογή φαρµάκων
 Στόχοι αρτηριακής πίεσης σε ειδικούς πληθυσµούς και επιλογή φαρµάκων Εύα Καρπάνου Δ/ντρια Αντιυπερτασικού Ιατρείου Α ΚΚ Ωνάσειου ΚΚ Θεσσαλονίκη, 14/2/13 Η µελέτη δεν υποστηρίχθηκε από φαρµακευτικές εταιρείες
Στόχοι αρτηριακής πίεσης σε ειδικούς πληθυσµούς και επιλογή φαρµάκων Εύα Καρπάνου Δ/ντρια Αντιυπερτασικού Ιατρείου Α ΚΚ Ωνάσειου ΚΚ Θεσσαλονίκη, 14/2/13 Η µελέτη δεν υποστηρίχθηκε από φαρµακευτικές εταιρείες
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials -
 Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Management of The Patients with Hypertension and High Risk Cardiovascular Disease
 Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University CVD and Hypertension: Worldwide Morbidity and Mortality
Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University CVD and Hypertension: Worldwide Morbidity and Mortality
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Rationale for the use of Single Pill Combination. Yong Jin Kim, MD Seoul National University Hospital
 Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
An Epidemiological Overview
 An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ
 ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ CAD: Statistics CAD is the largest killer of American males and females 13 million Americans have CAD 1.1 million MI s per year Every 26 seconds an American
ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ CAD: Statistics CAD is the largest killer of American males and females 13 million Americans have CAD 1.1 million MI s per year Every 26 seconds an American
47 Hypertension in Elderly
 47 Hypertension in Elderly YOU DO NOT HEAL OLD AGE; YOU PROTECT IT; YOU PROMOTE IT; YOU EXTEND IT Sir James Sterling Ross Abstract: The prevalence of hypertension rises with age and the complications secondary
47 Hypertension in Elderly YOU DO NOT HEAL OLD AGE; YOU PROTECT IT; YOU PROMOTE IT; YOU EXTEND IT Sir James Sterling Ross Abstract: The prevalence of hypertension rises with age and the complications secondary
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
Hypertension is a major risk factor for
 OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Cardiovascular Protection and the RAS
 Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
An Epidemiological Overview
 An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Hypertension and the Challenge of Adherence. Geneva Clark Briggs, Pharm.D., BCPS
 Hypertension and the Challenge of Adherence Geneva Clark Briggs, Pharm.D., BCPS Outline Brief overview of HTN and pharmacologic therapies Role of pharmacists in collaboration with patients and physicians
Hypertension and the Challenge of Adherence Geneva Clark Briggs, Pharm.D., BCPS Outline Brief overview of HTN and pharmacologic therapies Role of pharmacists in collaboration with patients and physicians
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
Cardiac Protection across the cardiac continuum. Dong-Ju Choi, MD, PhD College of Medicine Seoul National University
 Cardiac Protection across the cardiac continuum Dong-Ju Choi, MD, PhD College of Medicine Seoul National University Renin Angiotensin Cascade Nitric oxide (NO) Bradykinin Degradation products ACE ACEI
Cardiac Protection across the cardiac continuum Dong-Ju Choi, MD, PhD College of Medicine Seoul National University Renin Angiotensin Cascade Nitric oxide (NO) Bradykinin Degradation products ACE ACEI
Since the initial description of angiotensin II mediated
 CLINICAL CARDIOLOGY: PHYSICIAN UPDATE Manipulation of the Renin-Angiotensin System Michael M. Givertz, MD Since the initial description of angiotensin II mediated hypertension 40 years ago, basic and clinical
CLINICAL CARDIOLOGY: PHYSICIAN UPDATE Manipulation of the Renin-Angiotensin System Michael M. Givertz, MD Since the initial description of angiotensin II mediated hypertension 40 years ago, basic and clinical
Special Situations in Hypertension Management
 Compelling Indications Hypertension may exist in association with other conditions in which there are compelling indications for use of a particular treatment based on clinical trial data demonstrating
Compelling Indications Hypertension may exist in association with other conditions in which there are compelling indications for use of a particular treatment based on clinical trial data demonstrating
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Managing the Complicated Hypertensive Patient
 Managing the Complicated Hypertensive Patient Cheryl L. Laffer, MD, PhD, FAHA Associate Professor of Medicine, Texas A&M HSC College of Medicine Senior Staff, S&W Hypertension - Internal Medicine Vice
Managing the Complicated Hypertensive Patient Cheryl L. Laffer, MD, PhD, FAHA Associate Professor of Medicine, Texas A&M HSC College of Medicine Senior Staff, S&W Hypertension - Internal Medicine Vice
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
How Low Do We Go? Update on Hypertension
 How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
The Therapeutic Potential of Novel Approaches to RAAS. Professor of Medicine University of California, San Diego
 The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?
 Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction
 The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction Cardiovascular Center, Korea University Guro Hospital 2007. 4. 20 Seung-Woon Rha, MD, PhD Introduction 1.
The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction Cardiovascular Center, Korea University Guro Hospital 2007. 4. 20 Seung-Woon Rha, MD, PhD Introduction 1.
Valsartan Amlodipine HCT Combination: Control To Goal. Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI. Prof of cardiology Ain Shams University
 Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Abbreviations Cardiology I
 Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Prevention of Cardiovascular Events in Hypertension and CAD & Management of Hypertension in HF of Ischemic origin
 "Insight Heart" is also available at www.squarepharma.com.bd Vol: 911 No: 4; 4; 2012 2015 Prevention of Cardiovascular Events in Hypertension and CAD Drug-eluting & Management of Hypertension in HF of
"Insight Heart" is also available at www.squarepharma.com.bd Vol: 911 No: 4; 4; 2012 2015 Prevention of Cardiovascular Events in Hypertension and CAD Drug-eluting & Management of Hypertension in HF of