Categories of BP in Adults*
|
|
|
- Buddy Fleming
- 5 years ago
- Views:
Transcription
1 HYPERTENSION GUIDELINES FOR ADULTS IN PRIMARY CARE [FOR THE DETECTION EVALUATION PREVENTION AND TREATMENT: 2017] [DERIVED FOM JNCH -9 AMERICAN COLLEGE OF CARDIOLOGY RECOMMENDATIONS -2017]. Hypertension has been implicated in the initiation or progression of a number of medical conditions including Cardiac, Stroke, Kidney Disease. It is therefore important that primary care physicians in particular be alert to the prevention, detection, evaluation and treatment of this common medical problem. Normal blood pressure is defined as blood pressure <120/<80 (mm of Hg). Blood pressure is considered ELEVATED if pressure is between /<80. Hypertension is defined in 2 stages: Stage 1: / Stage 2: >=140/>=90 Individuals with blood pressures in two categories should be designated in the higher category. See Table I below. Categories of BP in Adults* BP Category SBP DBP Normal <120 mm Hg and <80 mm Hg Elevated mm Hg and <80 mm Hg Hypertension Stage mm Hg or mm Hg Stage mm Hg or 90 mm Hg *Individuals with SBP and DBP in 2 categories should be designated to the higher BP category. Table 6 Hypertension detection may be further refined by locale, time of day and measurement method. See table below for Clinic; Home; Daytime, Nighttime & 24 Hour ABPM. See Table II below.
2 Corresponding Values of Systolic BP/Diastolic BP for Clinic, Home (HBPM), Daytime, Nighttime, and 24-Hour Ambulatory (ABPM) Measurements. Clinic HBPM Daytime ABPM Nighttime ABPM 24-Hour ABPM 120/80 120/80 120/80 100/65 115/75 130/80 130/80 130/80 110/65 125/75 140/90 135/85 135/85 120/70 130/80 160/ /90 145/90 140/85 145/90 White Coat Hypertension may be suspected in patients not on drug therapy if BP is between >= 130/80 but <160/100 and after3 months of trial of lifestyle modification and with Home BP Monitoring (HBPM) or Daytime Amb. BP Monitoring (ABPM) falls to <130/80. In this scenario ABPM or HBPM should be done annually to detect progression. Masked Hypertension may be suspected in patients, not on drug therapy, if Office BP is /<80 after 3 mo of lifestyle modification and Daytime ABPM or HBPM shows BP of >= 130/80. If BP on monitoring is not >= 130/80 then BP is considered Elevated and life style modification should continue with annual HBPM or ABPM to detect Masked HTN or progression. In both situations of suspicion of White Coat Hypertension and Masked Hypertension if the BP on HBPM or ABPM remains >130/80 then drug therapy should be initiated along with continuation of lifestyle modification. If the patient is on drug therapy and Office BP is above goal by >=5-10 mmhg on 3 agents, then screen for White Coat Effect with HBPM. If BP on HBPM is at goal, then this signifies White Coat Effect and can be confirmed with ABPM. If white Coat Effect is not confirmed, then continue titrating therapy. If the Office BP is at Goal but there is increased CVD risk or target organ damage, then screen for masked uncontrolled hypertension with HBPM. If HBPM is above goal, then investigate further with ABPM and if also above goal then Masked Uncontrolled Hypertension is present and therapy should be intensified. If ABPM is not above goal, then continue current therapy. See diagram below.

3 SCREENING FOR SECONDARY HYPERTENSION If there is new onset or uncontrolled hypertension, then screening should be done for Secondary Hypertension under the following conditions: Abrupt onset Hypertension;
4 Drug-resistant/ induced hypertension; Onset of hypertension at < 30 years old; Onset of diastolic hypertension at age > =65 y.o Disproportionate target organ damage for the degree of hypertension; Unprovoked or excessive hypokalemia; Exacerbation of previously controlled hypertension; Accelerated/ Malignant Hypertension If screening is positive, then referral to clinicians with the specific expertise should be strongly considered. See screening tests and indications in tables below: Causes of Secondary Hypertension with Clinical Indications and Diagnostic Screening Tests Common Causes Prevalence Clinical Indications Physical Exam Screening Tests Additional/ Confirmatory Tests Renal parenchymal disease 1% 2% Urinary tract infections; obstruction, hematuria; urinary frequency and nocturia; analgesic abuse; family history of polycystic kidney disease; elevated serum creatinine; abnormal urinalysis Abdominal mass (polycystic kidney disease); skin pallor Renal ultrasound Tests to evaluate cause of renal disease Renovascular disease 5%-34%* Resistant hypertension; hypertension of abrupt onset or worsening or increasingly difficult to control; lash pulmonary edemam (atherosclerotic); early onset hypertension, especially in women (fibromuscular hyperplasia) Abdominal systolicdiastolic bruit; bruits over other arteries (carotid atherosclerotic or fibromuscular dysplasia), femoral Renal Duplex Doppler ultrasound; MRA; abdominal CT Bilateral selective renal intraarterial angiography Primary 8% 20% aldosteronism Resistant hypertension; hypertension with hypokalemia (spontaneous or diureticinduced); hypertension and muscle cramps or weakness; hypertension and incidentally discovered adrenal mass; hypertension and obstructive sleep apnea; hypertension and family history of early onset hypertension or stroke Arrhythmias (with hypokalemia); especially atrial fibrillation Plasma aldosterone/ renin ratio under standardized conditions (correction of hypokalemia and withdrawal of aldosterone antagonists for 4 6 wk) Oral sodium loading test (prior to 24 h urine aldosterone) or IV saline infusion test with plasma aldosterone at 4 h of infusion. Adrenal CT scan, Adrenal vein sampling. Trial of mineralocorticoid receptor blockers Obstructive sleep apnea 25% 50% Resistant hypertension; snoring fitful sleep; breathing pauses during sleep; daytime sleepiness Obesity, Mallampati class III IV; loss of normal nocturnal BP fall Berlin Questionnaire (8); Epworth Sleepiness Score (9); overnight oximetry Polysomnography
5 Drug- or alcoholinducedii 2% 4% Sodium-containing antacids; caffeine; nicotine (smoking); alcohol; NSAIDs; oral contraceptives; cyclosporine or tacrolimus; sympathomimetics (decongestants, anorectics); cocaine, amphetamines and other illicit drugs; neuro psychiatric agents; erythropoiesis stimulating agents; clonidine withdrawal; herbal agents (MaHuang, ephedra) Fine tremor, tachycardia, sweating (cocaine, ephedrine, MAO inhibitors); acute abdominal pain (cocaine) Urinary drug screen (illicit drugs) Response to withdrawal of suspected agent Uncommon Causes Pheochromocytoma/ paraganglioma 0.1% 0.6% Resistant hypertension; paroxysmal hypertension or crisis superimposed on sustained hypertension; spells, BP lability, headache, sweating, palpitations, pallor; positive family history of pheochromocytoma/ paraganglioma; adrenal incidentaloma Skin stigmata of neurofibromatosis (café-au-lait spots; neurofibromas); orthostatic hypotension 24-h urinary fractionated metanephrines or plasma metanephrines under standard conditions (30 supine position with indwelling IV cannula) CT or MRI scan of abdomen/pelvis Cushing s syndrome <0.1% Rapid weight gain, especially with central distribution; proximal muscle weakness; depression; hyperglycemia Central obesity, moon face, dorsal and supraclavicular fat pads, wide (1 cm) violaceous striae, hirsutism Overnight 1 mg dexamethasone suppression test 24-h urinary free cortisol excretion (preferably multiple); midnight salivary cortisol Hypothyroidism <1% Dry skin; cold intolerance; constipation; hoarseness; weight gain Delayed ankle refex; periorbital puffiness; coarse skin; cold skin; slow movement; goiter Thyroid stimulating hormone; free thyroxine None Hyperthyroidism <1% Warm, moist skin; heat intolerance; nervousness; tremulousness; insomnia; weight loss; diarrhea; proximal muscle weakness Lid lag; fine tremor of the outstretched hands; warm, moist skin Thyroid stimulating hormone, free thyroxine Radioactive iodine uptake and scan Aortic coarctation (undiagnosed or repaired) 0.1% Young patient with hypertension (<30 y of age) BP higher in upper extremities compared to lower extremities; absent femoral pulses; continuous murmur over patient s back, chest, or abdominal bruit; left thoracotomy scar (postoperative) Echocardiogram Thoracic and abdominal CT or MRA Primary hyperparathyroidism Rare Hypercalcemia Usually none Serum calcium Serum parathyroid hormone
6 Uncommon Causes (continued from previous page) Congenital adrenal hyperplasia Rare Hypertension and hypokalemia; virilization (11-beta-hydroxylase deiciency [11-beta-OH]) incomplete masculinization in males and primary amenorrhea in females (17-alphahydroxylase deiciency [17-alpha-OH]) Signs of virilization (11-beta-OH) or incomplete masculinization (17-alpha-OH) Hypertension and hypokalemia with low or normal aldosterone and renin 11-beta-OH: elevated deoxycorticosterone (DOC), 11-deoxycortisol and androgens 17-alpha- OH: decreased androgens and estrogen; elevated deoxycorticosterone and corticosterone Mineralocorticoid excess syndromes other than primary aldosteronism Rare Early onset hypertension; resistant hypertension; hypokalemia or hyperkalemia Arrhythmias (with hypokalemia) Low aldosterone and renin Urinary cortisol metabolites; genetic testing Acromegaly Rare Acral features, enlarging shoe, glove or hat size; headache, visual disturbances; diabetes mellitus Acral features; large hands and feet; frontal bossing Serum growth hormone 1 ng/ml during oral glucose load Elevated age- and sex-matched IGF-1 level; MRI scan of the pituitary *Depending on the clinical situation (hypertension alone, 5%; hypertension starting dialysis, 22%; hypertension and peripheral vascular disease, 28%; hypertension in the elderly with congestive heart failure, 34%). 8% in general population with hypertension; up to 20% in patients with resistant hypertension. Although obstructive sleep apnea is listed as a cause of secondary hypertension, RCTs on the effects of continuous positive airway pressure on lowering BP in patients with hypertension have produced mixed results May treat patients with resistant hypertension with a MRA whether or not primary aldosteronism is present. PREVENTION: Frequently used medications and other substances that may cause elevated blood pressure include: Alcohol, Caffeine, Oral Contraceptives, NSAIDs, Decongestants (eg. Phenylephrine, Pseudoephedrine), Recreational Drugs (eg.cocaine, methamphetamine, bath salts [MDPV], etc), Antidepressants (eg. MAOIs, SNRIs, TCAs), Amphetamines (eg amphetamine, dextroamphetamine, methylphenidate, dexmethylphenidate), Atypical Anti Psychotics (eg Clozapine & Olanzapine), Immunosuppressants (eg Cyclosporine), Herbal Supplements (eg. St John s wort[ with MAO inhibitors yohimbine], Ma Huang [ephedra], Systemic steroids (eg. Prednisone, prednisolone, fluodrocortisone, prednisolone, methylprednisolone) Angiogenesis inhibitor (eg Bevacizumab) Tyrosine kinase inhibitor (eg. sunitinib, sorafenif). Etc.
7 DIAGNOSTIC TESTING: Basic laboratory testing for primary hypertension includes: CBC; serum: -NA, K, Ca, Creatinine with egfr; Fasting blood glucose; Urinalysis; TSH; Lipid Profile. EKG should be done. Other laboratory testing may include Uric Acid and Urinary Albumin/Creatinine ratio. Echocardiogram may be included. PREVENTION AND TREATMENT: Non Pharmacologic Interventions. The proven non pharmacologic interventions for prevention and treatment include: Weight loss (ideal body weight is the goal, expect 1mmHg reduction for each 1 kg reduction in body weight). Healthy diet (rich in fruits, vegetables, whole grain, low fat dairy products with reduced content of saturated and trans I fats). Reduced intake of dietary sodium (<1500 mg/day is goal but at least 1000 mg/day reduction for most.) Enhanced intake of dietary potassium ( mg/day) Physical activity Moderation of alcohol intake (reduction to <= 2 drinks/day for men and <=1 drink/day for women)

8
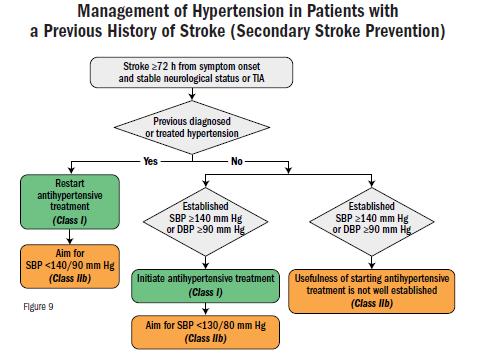
9 PHARMACOLOGIC TREATMENT: As a rule of thumb the goal of therapy is a BP of < 130/80. The exception is (>=65 y.o. noninstutionalized, community living ambulatory adult where the goal is <130 SBP). In most cases therapy is initiated for BP > 130/80 except for patients with no clinical CVD and ASCVD risk of <10% and patients with secondary stroke prevention where the threshold for treatment is >=140/90. BP Thresholds for and Goals of Pharmacologic Therapy in Patients with Hypertension According to Clinical Conditions Clinical Condition (s) BP Threshold mm Hg BP Goal mm Hg General Clinical CVD or 10 year ASCVD risk 10% 130/80 <130/80 No clinical CVD and 10 year ASCVD risk <10% 140/90 <130/80 Older persons ( 65 years of age; non-institutionalized, ambulatory, community-living adults) Specific Comorbidities 130 (SBP) <130 (SBP) Diabetes mellitus 130/80 <130/80 Chronic kidney disease 130/80 <130/80 Chronic kidney disease post-renal transplantation 130/80 <130/80 Heart failure 130/80 <130/80 Stable ischemic heart disease 130/80 <130/80 Secondary stroke prevention 140/90 <130/80 Secondary stroke prevention (lacunar) 130/80 <130/80 Peripheral arterial disease 130/80 <130/80 A list of oral antihypertensive drugs by class, name, usual dosages, usual frequency and important considerations in their usage are listed in the tables below.
10 Class Primary Agents Thiazide or thiazide-type diuretics Drug Oral Antihypertensive Drugs Usual Dose, Range (mg per day)* Daily Frequency Comments Chlorthalidone Chlorthalidone preferred based on prolonged Hydrochlorothiazide half-life and proven trial reduction of CVD Indapamide Monitor for hyponatremia and hypokalemia, uric acid and calcium levels. Metolazone Use with caution in patients with history of acute gout unless patient is on uric acid-lowering therapy. ACE Inhibitors Benazepril Captopril or 2 2 or 3 Do not use in combination with ARBs or direct renin inhibitor Enalapril or 2 Increased risk of hyperkalemia, especially in patients with CKD or in those on K+ supplements Fosinopril or K+-sparing drugs Lisinopril May cause acute renal failure in patients with Moexipril or 2 severe bilateral renal artery stenosis Perindopril Quinapril or 2 Ramipril or 2 Trandolapril Do not use if history of angioedema with ACE inhibitors. Avoid in pregnancy ARBs Azilsartan Candesartan Do not use in combination with ACE inhibitors or direct renin inhibitor Eprosartan or 2 Increased risk of hyperkalemia in CKD or in those on K+ supplements or K+-sparing drugs Irbesartan May cause acute renal failure in patients with Losartan or 2 severe bilateral renal artery stenosis Olmesartan Do not use if history of angioedema with ARBs. Telmisartan Patients with a history of angioedema with an Valsartan ACEI can receive an ARB beginning 6 weeks after ACEI discontinued. Avoid in pregnancy CCB dihydropyridines Amlodipine Avoid use in patients with HFrEF; amlodipine or Felodipine felodipine may be used if required Isradipine Associated with dose-related pedal edema, which is more common in women than men Nicardipine SR Nifedipine LA Nisoldipine CCB nondihydropyridines Diltiazem SR Avoid routine use with beta blockers due to Diltiazem ER increased risk of bradycardia and heart block Do not use in patients with HFrEF Verapamil IR Drug interactions with diltiazem and verapamil Verapamil SR or 2 (CYP3A4 major substrate and moderate inhibitor) Verapamil-delayed onset ER (various forms) (in the evening) Table is continued in the next page
11 Class Secondary Agents Drug Usual Dose, Range (mg per day)* Daily Frequency Comments Diuretics loop Bumetanide Preferred diuretics in patients with symptomatic Furosemide HF. Preferred over thiazides in patients with moderate-to-severe CKD (e.g., GFR <30 ml/min) Torsemide Diuretics potassium sparing Amiloride Triamterene or 2 1 or 2 Monotherapy agents minimally effective antihypertensives Combination therapy of potassium sparing diuretic with a thiazide can be considered in patients with hypokalemia on thiazide monotherapy Avoid in patients with signiicant CKD (e.g., GFR <45 ml/min) Diuretics aldosterone antagonists Eplerenone Spironolactone Preferred agents in primary aldosteronism and resistant hypertension Spironolactone associated with greater risk of gynecomastia and impotence compared to eplerenone Common add-on therapy in resistant hypertension Avoid use with K+ supplements, other K+-sparing diuretics or signiicant renal dysfunction Eplerenone often requires twice daily dosing for adequate BP lowering Beta blockers cardioselective Beta blockers cardioselective and vasodilatory Beta blockers noncardioselective Atenolol Beta blockers are not recommended as irst-line Betaxolol agents unless the patient has IHD or HF Bisorolol Preferred in patients with bronchospastic airway disease requiring a beta blocker Metoprolol tartrate Bisoprolol and metoprolol succinate preferred in Metoprolol patients with HFrEF succinate Avoid abrupt cessation Nebivolol Induces nitric oxide-induced vasodilation Avoid abrupt cessation Nadolol Avoid in patients with reactive airways disease Propranolol IR Propranolol LA Avoid abrupt cessation Beta blockers intrinsic sympathomimetic activity Acebutolol Generally avoid, especially in patients with IHD or HF Carteolol Avoid abrupt cessation Penbutolol Pindolol Table is continued in the next page
12 Class Drug Usual Dose, Range (mg per day)* Secondary Agents (continued from previous page) Beta blockers combined alpha- and beta-receptor Daily Frequency Comments Carvedilol Carvedilol preferred in patients with HFrEF Carvedilol phosphate Labetalol Avoid abrupt cessation Direct renin inhibitor Aliskiren Do not use in combination with ACE inhibitors or ARBs Aliskiren is very long acting Increased risk of hyperkalemia in CKD or in those on K+ supplements or K+ sparing drugs May cause acute renal failure in patients with severe bilateral renal artery stenosis Avoid in pregnancy Alpha-1 blockers Doxazosin Associated with orthostatic hypotension, Prazosin or 3 especially in older adults Terazosin or 2 May consider as second-line agent in patients with concomitant BPH Central alpha1- agonist and other centrally acting drugs Clonidine oral Generally reserved as last-line due to signifcant Clonidine patch weekly CNS adverse effects, especially in older adults Avoid abrupt discontinuation of clonidine, which Methyldopa may induce hypertensive crisis; clonidine must be Guanfacine tapered to avoid rebound hypertension Direct vasodilators Hydralazine or 3 Associated with sodium and water retention and refex tachycardia; use with a diuretic and bet Minoxidil a blocker Hydralazine associated with drug-induced lupuslike syndrome at higher doses Minoxidil associated with hirsutism and requires a loop diuretic. Can induce pericardial effusion *Dosages may vary from those listed in the FDA approved labeling (available at Adapted with permission from Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003; 289: The treatment for hypertension for specific medical conditions including: Heart Failure with Reduced Ejection Fraction, Stable Ischemic Heart Disease, Chronic Kidney Disease, patients with a previous history of stroke (Secondary Stroke Prevention) and Resistant Hypertension, is summarized in the following tables:
13 Heart Failure with Reduced Ejection Fraction (HFrEF) Recommendations for Treatment of Hypertension in Patients with Heart Failure with Reduced Ejection Fraction (HFrEF) Referenced studies that support recommendations are summarized in online Data Supplement 34 COR LOE Recommendations I III: No Benefit C-EO B-R 1. Adults with HFrEF and hypertension should be prescribed GDMT* titrated to attain a BP less than 130/80 mm Hg. 2. Nondihydropyridine CCBs are not recommended in the treatment of hypertension in adults with HFrEF. Heart Failure with Preserved Ejection Fraction (HFpEF) Recommendations for Treatment of Hypertension in Patients with Heart Failure with Preserved Ejection Fraction (HFpEF) Referenced studies that support recommendations are summarized in online Data Supplement 35, 36 COR LOE Recommendations I I C-EO C-LD 1. In adults with HFpEF who present with symptoms of volume overload, diuretics should be prescribed to control hypertension. 2. Adults with HFpEF and persistent hypertension after management of volume overload should be prescribed ACE inhibitors or ARB and beta blockers titrated to attain systolic BP less than 130 mm Hg.

14

15
16

17 Resistant Hypertension: Diagnosis, Evaluation, and Treatment Confirm Treatment Resistance Office SBP/DBP 130/80 mm Hg and Patient prescribed 3 antihypertensive medications at optimal doses, including a diuretic, if possible or Office SBP/DBP <130/80 mm Hg but patient requires 4 antihypertensive medications Exclude Pseudo-Resistance Ensure accurate office BP measurements Assess for nonadherence with prescribed regimen Obtain home, work, or ambulatory BP readings to exclude white coat effect Identify and Reverse Contributing Lifestyle Factors Obesity Physical Inactivity Excessive alcohol ingestion High salt, low-fiber diet Discontinue or Minimize Interfering Substances NSAIDs Sympathomimetic (e.g., amphetamines, decongestants) Stimulants Oral contraceptives Licorice Ephedra Screen for Secondary Causes of Hypertension Primary aldosteronism (elevated aldosterone/renin ratio) CKD (egfr <60 ml/min/1.73 m 2 ) Renal artery stenosis (young female, known atherosclerotic disease, worsening kidney function) Pheochromocytoma (episodic hypertension, palpitations, diaphoresis, headache) Obstructive sleep apnea (snoring, witnessed apnea, excessive daytime sleepiness) Pharmacologic Treatment Maximize diuretic therapy Add a mineralocorticoid receptor antagonist Add other agents with different mechanisms of actions Use loop diuretics in patients with CKD and/or patients receiving potent vasodilators (e.g., minoxidil) Refer to Specialist Refer to appropriate specialist for known or suspected secondary cause(s) of hypertension Refer to hypertension specialist if BP remains uncontrolled after 6 mo of treatment Adapted with permission from Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientifi statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008; 51:
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
2017 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults
 207 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults A Selection of Tables and Figures 207, American College of Cardiology B7206 207 Guideline for the
207 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults A Selection of Tables and Figures 207, American College of Cardiology B7206 207 Guideline for the
2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults
 DETAILED SUMMARY FROM THE 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults A REPORT OF THE American College of Cardiology/ American Heart Association
DETAILED SUMMARY FROM THE 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults A REPORT OF THE American College of Cardiology/ American Heart Association
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups. Lisa Ivy APRN
 Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Guide to the New Hypertension Guidelines
 Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Advanced Practice Pharmacist Crow/Northern Cheyenne Hospital Hypertension St Disclosures None Objectives Describe the new hypertension
Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Advanced Practice Pharmacist Crow/Northern Cheyenne Hospital Hypertension St Disclosures None Objectives Describe the new hypertension
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Guide to the New Hypertension Guidelines. LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital
 Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital Disclosures None Objectives Describe the new hypertension staging and blood pressure goals and
Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital Disclosures None Objectives Describe the new hypertension staging and blood pressure goals and
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety
 New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Andrew Straw, PharmD, BC-ADM
New Hypertension Guidelines: How Lower Blood Pressure Targets Affect Medication Safety Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Andrew Straw, PharmD, BC-ADM
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
HTN talk_l Davis_ /28/2018
 1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
8/20/2018. Objectives. What is hypertension? cont. What is hypertension? Epidemiology cont. Epidemiology
 Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Audience Response. Hypertension. Case: Mr. J. Measuring BP. Non-pharmacologic intervention. Case: Mr. J. Session ID: HTN411
 Audience Response http://rwpoll.com OR App downloads: Hypertension Chris Knight, MD cknight@uw.edu http://tiny.cc/rwiphone http://tiny.cc/rwdroid Session ID: HTN411 Case: Mr. J 52 y/o male patient comes
Audience Response http://rwpoll.com OR App downloads: Hypertension Chris Knight, MD cknight@uw.edu http://tiny.cc/rwiphone http://tiny.cc/rwdroid Session ID: HTN411 Case: Mr. J 52 y/o male patient comes
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Pediatric Hypertension. Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019
 Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Network Hypertension Algorithm
 Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Diagnosis and treatment of hypertension. Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington
 Diagnosis and treatment of hypertension Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington Outline Epidemiology Diagnosis Evaluation of individuals with
Diagnosis and treatment of hypertension Kari Nelson, MD MSHS Division of General Internal Medicine VA Puget Sound, University of Washington Outline Epidemiology Diagnosis Evaluation of individuals with
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
SAURIN GANDHI, AZCOM Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8)
") 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
ASEBP and ARTA TARP Drugs and Reference Price by Categories
 ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
Hypertension Management. complications including stroke, dementia, coronary artery disease, left ventricular dysfunction, kidney
 Hypertension Management Hypertension affects 19.7% of adult Canadians and is one of the most important modifiable risk factors for cardiovascular disease. 1 The prevalence continues to increase with more
Hypertension Management Hypertension affects 19.7% of adult Canadians and is one of the most important modifiable risk factors for cardiovascular disease. 1 The prevalence continues to increase with more
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
New classification of HT Systolic Diastolic Normal <120 <80 Prehypertension Stage1HT Stage 2 HT >160 or >100
 Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Approach to Management of Hypertension. Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc
 Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment
 Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC
 DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment