Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
|
|
|
- Colin York
- 6 years ago
- Views:
Transcription
1 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
2 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018
3 Conflicts of Interest No conflicts of interest
4 Objectives Be able to list the indications and contraindications for stress testing. Appreciate the different modalities available for cardiac stress testing. Appropriately select the optimal cardiac stress test for each patient.
5 Stoll s Words of Wisdom Don t stress patients you think you might kill with the study Don t order a study if you already know the answer If a patient can t exercise, don t order an exercise study If the patient s resting EKG is abnormal, something other than EKG imaging is needed to make it a useful study LBBB and paced rhythms may cause false positive studies in tests that increase HR (exercise or dobutamine stress)
6 More Words of Wisdom Echo imaging is only useful if you can image the endocardium Dobutamine can induce arrhythmias (AF, VT, VF) Adenosine, Persantine, Lexiscan can induce bronchospasm Stress tests are not perfect
7 Case Study A 60 yo man is evaluated for chest pain of 4 months duration. He describes the pain as sharp, located in the left chest, with no radiation or associated symptoms, that occurrs with walking one to two blocks and resolves with rest. Occasionally, the pain improves with continued walking or occurs during the evening hours. He has hypertension. Family history does not include cardiovascular disease in any first-degree relatives. His only medication is amlodipine. On physical examination, he is afebrile, blood pressure is 130/80 mhg, pulse rate is 72/min, and respiration rate is 12/min. BMI is 28. No carotid bruits are present, and a normal S1 and S2 with no murmurs are heard. Lung fields are clear, and distal pulses are normal. EKG showed normal sinus rhythm w/ LBBB.
8 Case Question Which of the following is the most appropriate diagnostic test to perform next? a. Adenosine nuclear perfusion stress test b. Coronary angiography c. Echocardiography d. Exercise treadmill
9 General Overview Stress testing is generally a safe procedure Commonly performed (1998 Medicare data) Treadmill 533,000 Stress Echo 354,000 Stress SPECT 1,362,000 Low risk of MI or death (1 per 2500) Requires appropriate supervision
10 Indications Who to stress? Screening for obstructive CAD Symptoms suggesting angina (low to moderate risk) Acute chest pain Known CAD with change in clinical status Assessment of prognosis and severity of disease
11 Indications Who to stress? Valvular heart disease New heart failure or cardiomyopathy Chronic left ventricular dysfunction and CHD (who are candidates for revascularization) Selected arrhythmias Undergoing non-urgent non-cardiac surgery
12 Contraindications Who NOT to stress? Unstable angina (high risk) Acute myocardial infarction (< 6 days) Known severe LM disease Arrhythmia with hemodynamic instability Aortic dissection
13 Contraindications Who NOT to stress? Symptomatic (critical) aortic stenosis Decompensated heart failure Severe HTN (SBP > 220 mmhg, DBP > 120 mmhg) Pulmonary embolism Myocarditis, Pericarditis
14 Who should get a stress test??
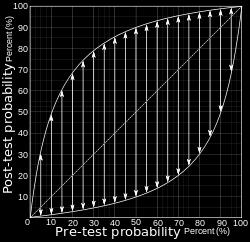
15 Bayes Theorem p(x A)*p(A) p(a X) = P(X A)*p(A) + p(x ~A)*p(~A) Given some phenomenon A that we want to investigate, and an observation X that is evidence about A, we can update the original probability of A, given the new evidence X.
16 Fundamentals of Stress Testing
17 Fundamentals of Stress Testing Positive Negative
18 Fundamentals of Stress Testing Positive Negative
19 Fundamentals of Stress Testing Positive Negative
20 Fundamentals of Stress Testing Positive Negative
21 Fundamentals of Stress Testing Positive Negative
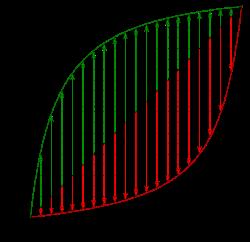
22 Fundamentals of Stress Testing
23 Pre-Test Probability ACC/AHA Guidelines Low probability - <10% - no further testing, except for prognostic information Intermediate probability % - non-invasive testing for diagnosis (exercise ECG as first modality) High probability - >90% - noninvasive testing for prognosis/management prior to cardiac cath
24 Pre-Test Probability Age Nonanginal pain Atypical angina Typical angina Men Women Men Women Men Women % 2% 34% 12% 76% 26% % 3% 51% 22% 87% 55% % 7% 65% 31% 93% 73% % 14% 72% 51% 94% 86%
25 Definitions of Chest Pain Typical angina (definite) Substernal chest discomfort with characteristic quality and duration Provoked by exertion or emotional stress Relieved by NTG or rest Atypical angina (probable) meets 2 of the above Non-anginal chest pain meets 1 or none of the typical characteristics
26 Pre-Test Probability Age Nonanginal pain Atypical angina Typical angina Men Women Men Women Men Women % 2% 34% 12% 76% 26% % 3% 51% 22% 87% 55% % 7% 65% 31% 93% 73% % 14% 72% 51% 94% 86%
27 But which test to order??
28 Anatomy of a Stress Test Each cardiac stress test has two components: Stressing agent: treadmill, dobutamine, or adenosine (or persantine or regadenosine) Imaging agent: EKG, echo, or radionuclide tracer (thallium or technetium)
29 Stress Agents Stressor Pro Con Treadmill Physiologic, simple, less expensive, good for patient who can walk Avoid in patients with SSS or pacemaker Dobutamine No exercise needed Caution in patients with arrhythmias Adenosine/Regadenosine (or dipyridamole) No exercise needed; uncomfortable for some Adenosine may induce bronchospasm caution in COPD and asthma!!
30 Stress Agents Stressor Pro Con Treadmill Physiologic, simple, less expensive, good for patient who can walk Avoid in patients with SSS or pacemaker Dobutamine No exercise needed Caution in patients with arrhythmias Adenosine/Regadenosine (or dipyridamole) No exercise needed; uncomfortable for some Adenosine may induce bronchospasm caution in COPD and asthma!!
31 Stress Agents Stressor Pro Con Treadmill Physiologic, simple, less expensive, good for patient who can walk Avoid in patients with SSS or pacemaker Dobutamine No exercise needed Caution in patients with arrhythmias Adenosine/Regadenosine (or dipyridamole) No exercise needed; uncomfortable for some Adenosine may induce bronchospasm caution in COPD and asthma!!
32 Imaging Agents Imaging Pro Con EKG Echocardiogram Thallium or technetium Simple, less expensive Good if patient has pre-existing EKG abnormalities. More info than EKG. Less expensive than nuclear. Localizes ischemia and infarcted tissue. Less information. May not be able to localize the lesion. Cannot use if there are baseline EKG abnormalities i.e. LBBB, ST-T changes Operator dependent to some extent. May have poor windows due to body habitus. Pre-existing wall motion abnormalities may make interpretation more challenging. Expensive, Radiation exposure

33 EKG Imaging Agents

34 EKG - LBBB Imaging Agents

35 EKG - Paced Rhythm Imaging Agents

36 EKG - Abnormal Baseline Imaging Agents
37 Imaging Agents Imaging Pro Con EKG Echocardiogram Thallium or technetium Simple, less expensive Good if patient has pre-existing EKG abnormalities. More info than EKG. Less expensive than nuclear. Localizes ischemia and infarcted tissue. Less information. May not be able to localize the lesion. Cannot use if there are baseline EKG abnormalities i.e. LBBB, ST-T changes Operator dependent to some extent. May have poor windows due to body habitus. Pre-existing wall motion abnormalities may make interpretation more challenging. Expensive, Radiation exposure
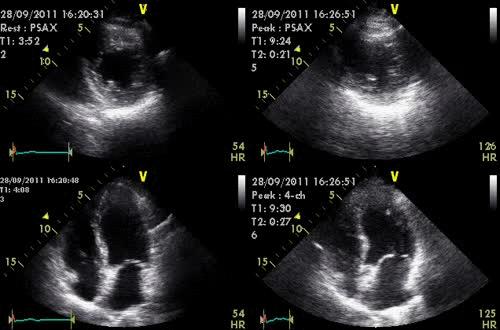
38 Echocardiographic Imaging Agents
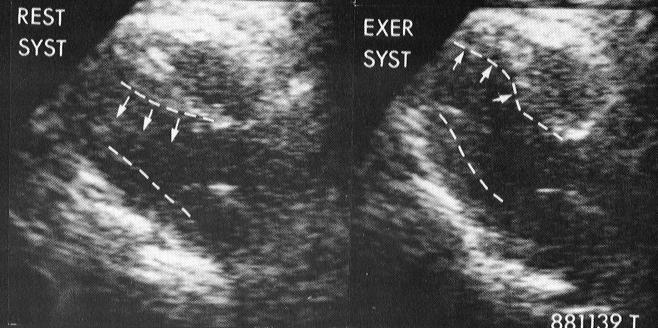
39 Echocardiographic Imaging Agents
40 Imaging Agents Imaging Pro Con EKG Echocardiogram Thallium or technetium Simple, less expensive Good if patient has pre-existing EKG abnormalities. More info than EKG. Less expensive than nuclear. Localizes ischemia and infarcted tissue. Less information. May not be able to localize the lesion. Cannot use if there are baseline EKG abnormalities i.e. LBBB, ST-T changes Operator dependent to some extent. May have poor windows due to body habitus. Pre-existing wall motion abnormalities may make interpretation more challenging. Expensive, Radiation exposure

41 Nuclear Imaging Agents
42 Sensitivity and Specificity Sensitivity Specificity Exercise EKG 68% 77% Stress Echo 76% 88% Nuclear Imaging 79-92% 73-88%
43 Selecting Modalities
44 Selecting Modalities
45 Selecting Modalities
46 Selecting Modalities
47 Selecting Modalities
48 Case Study A 60 yo man is evaluated for chest pain of 4 months duration. He describes the pain as sharp, located in the left chest, with no radiation or associated symptoms, that occurs with walking one to two blocks and resolves with rest. Occasionally, the pain improves with continued walking or occurs during the evening hours. He has hypertension. Family history does not include cardiovascular disease in any first-degree relatives. His only medication is amlodipine. On physical examination, he is afebrile, blood pressure is 130/80 mhg, pulse rate is 72/min, and respiration rate is 12/min. BMI is 28. No carotid bruits are present, and a normal S1 and S2 with no murmurs are heard. Lung fields are clear, and distal pulses are normal. EKG showed normal sinus rhythm w/ LBBB.
49 Case Study A 60 yo man is evaluated for chest pain of 4 months duration. He describes the pain as sharp, located in the left chest, with no radiation or associated symptoms, that occurs with walking one to two blocks and resolves with rest. Occasionally, the pain improves with continued walking or occurs during the evening hours. He has hypertension. Family history does not include cardiovascular disease in any first-degree relatives. His only medication is amlodipine. On physical examination, he is afebrile, blood pressure is 130/80 mhg, pulse rate is 72/min, and respiration rate is 12/min. BMI is 28. No carotid bruits are present, and a normal S1 and S2 with no murmurs are heard. Lung fields are clear, and distal pulses are normal. EKG showed normal sinus rhythm w/ LBBB.
50 Case Question Non-cardiac, Atypical or Typical chest pain? Pretest probability (60 y.o. / Male)? 65-72% Can he exercise? Yes or No Interpretable resting EKG (LBBB)? Yes or No Lung Disease or Obesity (BMI 28)? Yes or No
51 Case Question Which of the following is the most appropriate diagnostic test to perform next? a. Adenosine nuclear perfusion stress test b. Coronary angiography c. Echocardiography d. Exercise treadmill
52 Take-Home Points Know the contraindications for stress testing Stress testing is generally indicated for patients with intermediate pre-test probability Positive test in a low-risk population is frequently false positive Testing in high-risk populations may help determine prognosis Each stress test has two components: an imaging modality and a stress modality When determining which stress test to order, keep in mind the patient s ability to exercise and whether any confounding variables are present
53 Yes ordering the proper stress test does matter!!
54 Questions???
55
Case Question. Evaluation of Chest pain in the Office and Cardiac Stress Testing
 Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Choosing the Right Cardiac Test. Outline
 Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Cardiology Updates: Syncope and Stress Testing. Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
 Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Stress Testing:Which Study is Indicated for My Patient?
 Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test
 Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test Jang-Ho Bae, MD., PhD., FACC. Konyang University Hospital Daejeon, Korea Chest pain in Women ACS Atypical Stable angina F/29
Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test Jang-Ho Bae, MD., PhD., FACC. Konyang University Hospital Daejeon, Korea Chest pain in Women ACS Atypical Stable angina F/29
Patient-centered Imaging in Coronary Artery Disease. Jason H Cole, MD, MS, FACC January 10, 2015
 Patient-centered Imaging in Coronary Artery Disease Jason H Cole, MD, MS, FACC January 10, 2015 Non-invasive coronary imaging Non-invasive cardiac imaging has improved assessment of cardiac function, anatomy,
Patient-centered Imaging in Coronary Artery Disease Jason H Cole, MD, MS, FACC January 10, 2015 Non-invasive coronary imaging Non-invasive cardiac imaging has improved assessment of cardiac function, anatomy,
Contra-indications, Risks, and Safety Precautions for Stress Testing. ACSM guidelines, pg 20 7 ACSM RISK FACTORS. Risk Classifications pg 27
 Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
CHEST PAIN CDU INCLUSION CRITERIA
 CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN
 DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN DISCLOSURES financial or pharmaceutical affiliations related to topic JOSHUA MESKIN, MD, FACC -Medical College of Wisconsin -Associate Professor of
DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN DISCLOSURES financial or pharmaceutical affiliations related to topic JOSHUA MESKIN, MD, FACC -Medical College of Wisconsin -Associate Professor of
Cardiac Stress Testing What Stress is Best?
 Cardiac Stress Testing What Stress is Best? Jennifer Gerryts, Registered Respiratory Therapist Kati Tuomi, Medical Radiation Technologist, Nuclear Medicine Thunder Bay Regional Health Sciences Centre 1
Cardiac Stress Testing What Stress is Best? Jennifer Gerryts, Registered Respiratory Therapist Kati Tuomi, Medical Radiation Technologist, Nuclear Medicine Thunder Bay Regional Health Sciences Centre 1
P F = R. Disorder of the Breast. Approach to the Patient with Chest Pain. Typical Characteristics of Angina Pectoris. Myocardial Ischemia
 Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O.
 CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O. INTRODUCTION Form of imprisonment in 1818 Edward Smith s observations TECHNIQUE Heart rate Blood pressure ECG parameters Physical appearance INDICATIONS
CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O. INTRODUCTION Form of imprisonment in 1818 Edward Smith s observations TECHNIQUE Heart rate Blood pressure ECG parameters Physical appearance INDICATIONS
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
9/2/2016 CARDIOLOGY TESTING WHAT TO ORDER WHEN REFERENCE OBJECTIVES
 CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
Non Invasive Diagnostic Modalities for Coronary Artery Disease. Dr. Amitesh Aggarwal
 Non Invasive Diagnostic Modalities for Coronary Artery Disease Dr. Amitesh Aggarwal Ebers papyrus, ca. 1555 BCE If thou examine a man for illness in his cardia, and he has pains in his arms, in his breasts
Non Invasive Diagnostic Modalities for Coronary Artery Disease Dr. Amitesh Aggarwal Ebers papyrus, ca. 1555 BCE If thou examine a man for illness in his cardia, and he has pains in his arms, in his breasts
Diagnosis of CAD S Richard Underwood
 Diagnosis of CAD S Richard Underwood Professor of Cardiac Imaging Royal Brompton Hospital & Imperial College Faculty of Medicine London, UK The history and diagnosis 89% Non-cardiac chest pain 50% Atypical
Diagnosis of CAD S Richard Underwood Professor of Cardiac Imaging Royal Brompton Hospital & Imperial College Faculty of Medicine London, UK The history and diagnosis 89% Non-cardiac chest pain 50% Atypical
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
Noninvasive Evaluation of Coronary Artery Disease:
 Noninvasive Evaluation of Coronary Artery Disease: Selecting the Right Test for the Right Patient Saurabh Malhotra, MD, MPH Timothy Wong, MD Faculty Saurabh Malhotra, MD, MPH Assistant Professor of Medicine
Noninvasive Evaluation of Coronary Artery Disease: Selecting the Right Test for the Right Patient Saurabh Malhotra, MD, MPH Timothy Wong, MD Faculty Saurabh Malhotra, MD, MPH Assistant Professor of Medicine
High Value Evaluation of Chest Pain. Zoom Tips
 High Value Evaluation of Chest Pain California Quality Collaborative s Cardiology Webinar Series Webinar 1 December 7, 2017 Zoom Tips Attendees are automatically MUTED upon entry Refrain from using the
High Value Evaluation of Chest Pain California Quality Collaborative s Cardiology Webinar Series Webinar 1 December 7, 2017 Zoom Tips Attendees are automatically MUTED upon entry Refrain from using the
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Stress ECG is still Viable in Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh
 Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Which Test When? Avoid the Stress of Stress Testing. Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute
 Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Stress echo workshop STRESSORS
 Stress echo workshop STRESSORS Adham Ahmed, MD Lecturer of Cardiology, Ain Shams Indications of Stress Echo CAD Diagnosis Prognosticat ion 1 Physiologic Basis 1930s: Tennant and Wiggers Relationship between
Stress echo workshop STRESSORS Adham Ahmed, MD Lecturer of Cardiology, Ain Shams Indications of Stress Echo CAD Diagnosis Prognosticat ion 1 Physiologic Basis 1930s: Tennant and Wiggers Relationship between
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why?
 Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Welcome! To submit questions during the presentation: or Text:
 Welcome! To participate in the interactive Q & A please do the following: 1. Download the Socrative Student App 2. Enter Teacher s Room Code: ZD0F3X5Q 3. Select Quiz: Intermountain Cardiac Stress Testing
Welcome! To participate in the interactive Q & A please do the following: 1. Download the Socrative Student App 2. Enter Teacher s Room Code: ZD0F3X5Q 3. Select Quiz: Intermountain Cardiac Stress Testing
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Atypical pain and normal exercise test
 Atypical pain and normal exercise test F. Mut, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history 67-year old male with several coronary risk factors. Atypical
Atypical pain and normal exercise test F. Mut, M. Beretta Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Clinical history 67-year old male with several coronary risk factors. Atypical
Preoperative Management. Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
 Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Chapter 21: Clinical Exercise Testing Procedures
 Publisher link: thepoint http://thepoint.lww.com/book/show/2930 Chapter 21: Clinical Exercise Testing Procedures American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise
Publisher link: thepoint http://thepoint.lww.com/book/show/2930 Chapter 21: Clinical Exercise Testing Procedures American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Risk Stratification for CAD for the Primary Care Provider
 Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Cardiac Stress Test [ ] Procedures. Cardiac Studies Stress Tests (Single Response)
![Cardiac Stress Test [ ] Procedures. Cardiac Studies Stress Tests (Single Response)](/thumbs/82/85301141.jpg "Cardiac Stress Test [ ] Procedures. Cardiac Studies Stress Tests (Single Response)") Cardiac Stress Test [3041300006] Procedures Cardiac Studies Stress Tests (Single Response) ( ) EKG Only Exercise Stress Test - Treadmill Do Not Order if: Baseline ST segment abnormalities on EKG (LBBB,
Cardiac Stress Test [3041300006] Procedures Cardiac Studies Stress Tests (Single Response) ( ) EKG Only Exercise Stress Test - Treadmill Do Not Order if: Baseline ST segment abnormalities on EKG (LBBB,
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Current and Future Imaging Trends in Risk Stratification for CAD
 Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Guideline Number: NIA_CG_024 Last Review Date: January 2011 Responsible Department: Last Revised Date: May 2, 2011 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Subha V. Raman, MD, MSEE, FACC, FAHA
 OSU Cardiovascular MR/CT Update April 27, 2018 Contemporary Approaches to Myocardial Ischemia Subha V. Raman, MD, MSEE, FACC, FAHA Professor and Medical Director, CMR/CCT Disclosures Institutional research
OSU Cardiovascular MR/CT Update April 27, 2018 Contemporary Approaches to Myocardial Ischemia Subha V. Raman, MD, MSEE, FACC, FAHA Professor and Medical Director, CMR/CCT Disclosures Institutional research
Stress tests: How to make a calculated choice Spare your patients unnecessary stress testing by determining their pretest probability for CAD
 PRACTICA MEDICALÅ19 REFERATE GENERALE Stress tests: How to make a calculated choice Spare your patients unnecessary stress testing by determining their pretest probability for CAD DENNIS P. BREEN, MD University
PRACTICA MEDICALÅ19 REFERATE GENERALE Stress tests: How to make a calculated choice Spare your patients unnecessary stress testing by determining their pretest probability for CAD DENNIS P. BREEN, MD University
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Guideline Number: NIA_CG_024 Last Revised Date: August 2011 Responsible Department: Implementation Date: January 2014 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING (aka NUCLEAR CARDIAC IMAGING STUDY) CPT Code: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78499 Original
National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING (aka NUCLEAR CARDIAC IMAGING STUDY) CPT Code: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78499 Original
Chest Pain Wave I. Making Dollars and Sense Out of Stress Testing
 Chest Pain Wave I Making Dollars and Sense Out of Stress Testing Presenters Kristin Newby, MD, FACC Michael Kontos, MD, FACC Disclosures Dr. Newby: None specifically related to this activity All RWI are
Chest Pain Wave I Making Dollars and Sense Out of Stress Testing Presenters Kristin Newby, MD, FACC Michael Kontos, MD, FACC Disclosures Dr. Newby: None specifically related to this activity All RWI are
Cardiac Diagnostics Workshop. Lori Savard NP Cardiology Update 2015
 Cardiac Diagnostics Workshop Lori Savard NP Cardiology Update 2015 Disclosure of Commercial Support Potential for conflict(s) of interest: none Objectives Increase understanding regarding stable IHD and
Cardiac Diagnostics Workshop Lori Savard NP Cardiology Update 2015 Disclosure of Commercial Support Potential for conflict(s) of interest: none Objectives Increase understanding regarding stable IHD and
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
12 Lead EKG Chapter 4 Worksheet
 Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
10/22/16. Lay of the land. Definition of ACS. Why do we worry about ST elevations?
 Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Cardiovascular nuclear imaging employs non-invasive techniques to assess alterations in coronary artery flow, and ventricular function.
 National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA Original Date: October 2015 Page 1 of 9 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes:
National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA Original Date: October 2015 Page 1 of 9 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes:
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease?
 CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease? Madan Mohan MD MRCP FACC CQO, Division of Cardiovascular Medicine University Hospitals Case Medical Center Assistant
CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease? Madan Mohan MD MRCP FACC CQO, Division of Cardiovascular Medicine University Hospitals Case Medical Center Assistant
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Guideline Number: NIA_CG_024 Last Revised Date: August 2011 Responsible Department: Clinical. Implementation Date: January 2014 Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING MYOCARDIAL PERFUSION STUDY CPT Code: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78499 Original Date: October
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING MYOCARDIAL PERFUSION STUDY CPT Code: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78499 Original Date: October
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Family Practice. Stress tests: How to make a calculated choice. For personal use only. Copyright Dowden Health Media
 For mass reproduction, content licensing and permissions contact Dowden Health Media. Family Practice the journal of Stress tests: How to make a calculated choice Spare your patients unnecessary stress
For mass reproduction, content licensing and permissions contact Dowden Health Media. Family Practice the journal of Stress tests: How to make a calculated choice Spare your patients unnecessary stress
CONFUSION IN CARDIAC TESTING. Bilal Aijaz M.D FACC FSCAI
 CONFUSION IN CARDIAC TESTING Bilal Aijaz M.D FACC FSCAI WHY DOES CARDIOLOGY HAVE SO MANY TESTS? to create confusion (of course) to generate more business (maybe?) to accommodate the ever expanding patient
CONFUSION IN CARDIAC TESTING Bilal Aijaz M.D FACC FSCAI WHY DOES CARDIOLOGY HAVE SO MANY TESTS? to create confusion (of course) to generate more business (maybe?) to accommodate the ever expanding patient
Cardiovascular nuclear imaging employs non-invasive techniques to assess alterations in coronary artery flow, and ventricular function.
 National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA CPT4 Codes: Refer to pages 6-9 LCD ID Number: L33960 J 15 = KY, OH Responsible
National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA CPT4 Codes: Refer to pages 6-9 LCD ID Number: L33960 J 15 = KY, OH Responsible
Imaging of the Heart Todd Tessendorf MD FACC
 Imaging of the Heart Todd Tessendorf MD FACC Outline Imaging Modalities for Structural Heart Disease ECHO, MRI Imaging Modalities for Ischemic Heart Disease SPECT, PET, CCTA Show lots of pretty pictures
Imaging of the Heart Todd Tessendorf MD FACC Outline Imaging Modalities for Structural Heart Disease ECHO, MRI Imaging Modalities for Ischemic Heart Disease SPECT, PET, CCTA Show lots of pretty pictures
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
LVHN Cardiac Diagnostic Testing PCP/PCP Office Testing Cheat Sheet. September 2017
 LVHN Cardiac Diagnostic Testing PCP/PCP Office Testing Cheat Sheet September 2017 1. ECHOCARDIOGRAM A (transthoracic) echocardiogram (2D Echo) is a 2-dimensional graphic of the heart s movement, valves
LVHN Cardiac Diagnostic Testing PCP/PCP Office Testing Cheat Sheet September 2017 1. ECHOCARDIOGRAM A (transthoracic) echocardiogram (2D Echo) is a 2-dimensional graphic of the heart s movement, valves
Detection Of Heart. By Dr Gary Mo
 Detection Of Heart Disease By Dr Gary Mo Types Of Heart Disease A. Coronary Heart Disease B. Valvular Heart Disease C. Cardiac Arrhythmia ( Rhythm disturbance ) D. Heart Blocks ( Conduction Abnormalities
Detection Of Heart Disease By Dr Gary Mo Types Of Heart Disease A. Coronary Heart Disease B. Valvular Heart Disease C. Cardiac Arrhythmia ( Rhythm disturbance ) D. Heart Blocks ( Conduction Abnormalities
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
History of Stress Testing. Disclosure. Overview. Stress Echocardiography New Applications. and Comparison with Other Stress.
 Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
There are 3 principle types of stress tests which do not involve the measurement of radiolabelled distribution within the body.
 National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING HEART (CARDIAC) PET SCAN STRESS ECHOCARDIOGRAM (Non-emergent outpatient testing) CPT4 Codes: Refer to pages 11-12 LCD
National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING HEART (CARDIAC) PET SCAN STRESS ECHOCARDIOGRAM (Non-emergent outpatient testing) CPT4 Codes: Refer to pages 11-12 LCD
Bayes Theorem and diagnostic tests with application to patients with suspected angina
 96 Tutorial December 2013 - Issue 2 Bayes Theorem and diagnostic tests with application to patients with suspected angina Andrew Owen PhD, FESC Department of Cardiology, Canterbury Christ Church University,
96 Tutorial December 2013 - Issue 2 Bayes Theorem and diagnostic tests with application to patients with suspected angina Andrew Owen PhD, FESC Department of Cardiology, Canterbury Christ Church University,
Chronic Stable Angina
 1 Chronic Stable Angina Theodore D. Fraker, Stephan D. Fihn, and Raymond J. Gibbons Introduction Classification of angina pectoris Demographics of angina pectoris Patients with new onset or changing anginal
1 Chronic Stable Angina Theodore D. Fraker, Stephan D. Fihn, and Raymond J. Gibbons Introduction Classification of angina pectoris Demographics of angina pectoris Patients with new onset or changing anginal
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
Myocardial Perfusion SPECT How to do it E. Moralidis
 Myocardial Perfusion SPECT How to do it E. Moralidis Aristotelian University AHEPA Hospital Thessaloniki Myocardial perfusion SPECT procedure Stress Imaging Data analysis and reporting Myocardial perfusion
Myocardial Perfusion SPECT How to do it E. Moralidis Aristotelian University AHEPA Hospital Thessaloniki Myocardial perfusion SPECT procedure Stress Imaging Data analysis and reporting Myocardial perfusion
Getting the Most Out of Stress Echo
 Getting the Most Out of Stress Echo Vera H. Rigolin, MD, FASE, FACC, FAHA Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern
Getting the Most Out of Stress Echo Vera H. Rigolin, MD, FASE, FACC, FAHA Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern
STANDARDIZED PROCEDURE CARDIAC STRESS TESTING-EXERCISE TESTING (Adult)
") 1 I. Definition: During the exercise test, the patient exercises on a bike or treadmill while being monitored with a 12 lead ECG, blood pressure device, pulse oximetry oxygen consumption, and perhaps imaging
1 I. Definition: During the exercise test, the patient exercises on a bike or treadmill while being monitored with a 12 lead ECG, blood pressure device, pulse oximetry oxygen consumption, and perhaps imaging
Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018
 Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018 No Disclosures The American Heart Association Evidence-Based Scoring
Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018 No Disclosures The American Heart Association Evidence-Based Scoring
21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease
 21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease Noninvasive Evaluation of Coronary Artery Disease: Anatomical, Functional, Clinical May 5, 2018 Mark Hansen MD FRCPC Cardiologist,
21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease Noninvasive Evaluation of Coronary Artery Disease: Anatomical, Functional, Clinical May 5, 2018 Mark Hansen MD FRCPC Cardiologist,
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Lahey Clinic Internal Medicine Residency Program: Curriculum for Cardiovascular Medicine Rotation
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Cardiovascular Medicine Rotation Faculty representative: David Venesy, MD Resident representative: David Kahan, MD Revision date: June 29,
Lahey Clinic Internal Medicine Residency Program: Curriculum for Cardiovascular Medicine Rotation Faculty representative: David Venesy, MD Resident representative: David Kahan, MD Revision date: June 29,
Khai Pham Gia. Vietnam Cardiovascular Organization Cardiovascular Hospital. Hanoi, Vietnam. Declared no potential conflict of interest.
 Khai Pham Gia Vietnam Cardiovascular Organization Cardiovascular Hospital Hanoi University of Medicine Hanoi, Vietnam Declared no potential conflict of interest. Hypertension in Patients with Coronary
Khai Pham Gia Vietnam Cardiovascular Organization Cardiovascular Hospital Hanoi University of Medicine Hanoi, Vietnam Declared no potential conflict of interest. Hypertension in Patients with Coronary
Maria Angela S. Cruz-Anacleto, MD
 Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Chest Pain: To Cath or Not? Part I
 Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
IAEA International Conference on Integrated Medical Imaging in CV Disease 2013
 IAEA International Conference on Integrated Medical Imaging in CV Disease 2013 How to Stress My Patient Choosing the Proper Stress Test Consultant and Advisory Board for Astellas John J. Mahmarian, MD,
IAEA International Conference on Integrated Medical Imaging in CV Disease 2013 How to Stress My Patient Choosing the Proper Stress Test Consultant and Advisory Board for Astellas John J. Mahmarian, MD,
Anesthesia for Cardiac Patients for Non Cardiac Surgery. Kimberly Westra DNP, MSN, CRNA
 Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
NUCLEAR CARDIOLOGY UPDATE
 Nuclear Cardiology David K. Shelton, Jr., MD NUCLEAR CARDIOLOGY UPDATE No Conflicts. No Disclosures. No Smoking. David K. Shelton UCDMC Nuclear Cardiology Nuclear Cardiology Radionuclide Ventriculography
Nuclear Cardiology David K. Shelton, Jr., MD NUCLEAR CARDIOLOGY UPDATE No Conflicts. No Disclosures. No Smoking. David K. Shelton UCDMC Nuclear Cardiology Nuclear Cardiology Radionuclide Ventriculography
Chest Pain. Dr. Amitesh Aggarwal. Department of Medicine
 Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Chest Pain Dr. Amitesh Aggarwal Department of Medicine BACKGROUND Approx 5% of all ED visits 15 % - AMI 25-30 % - Unstable angina 50-55 % - Other conditions Atypical presentations common 2% of patients
Cardiac Screening with Electrocardiography, Stress Echocardiography, or Myocardial Perfusion Imaging
 Cardiac Screening with Electrocardiography, Stress Echocardiography, or Myocardial Perfusion Imaging A D V I C E F O R H I G H V A L U E C A R E F R O M T H E A M E R I C A N C O L L E G E O F P H Y S
Cardiac Screening with Electrocardiography, Stress Echocardiography, or Myocardial Perfusion Imaging A D V I C E F O R H I G H V A L U E C A R E F R O M T H E A M E R I C A N C O L L E G E O F P H Y S
Stress Echo Cases Sunday, October 8, :10 3:30 PM 20 min
 2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None
, FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None") Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 2,000 Noninvasive Procedures 1,600 Units of Service/ 1,000 Beneficiaries 1,200 800 Evaluation and
Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 2,000 Noninvasive Procedures 1,600 Units of Service/ 1,000 Beneficiaries 1,200 800 Evaluation and
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Specific Basic Standards for Osteopathic Fellowship Training in Cardiology
 Specific Basic Standards for Osteopathic Fellowship Training in Cardiology American Osteopathic Association and American College of Osteopathic Internists BOT 07/2006 Rev. BOT 03/2009 Rev. BOT 07/2011
Specific Basic Standards for Osteopathic Fellowship Training in Cardiology American Osteopathic Association and American College of Osteopathic Internists BOT 07/2006 Rev. BOT 03/2009 Rev. BOT 07/2011
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
2017 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2017 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 15 performance measures that were approved by CMS for use in ASC's 2017 Qualified Clinical Data
2017 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 15 performance measures that were approved by CMS for use in ASC's 2017 Qualified Clinical Data
Conflict Disclosures. Vermont Cardiac Network. Outline. Series Learning Objectives 4/27/2016. Scott E. Friedman April 28, 2016
 Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Cardiac Diagnostic Testing Reference Guide January 2018
 STAT Cardiac Testing is available for inpatients only. ECHOCARDIOGRAM Cardiac Diagnostic Testing A (transthoracic) echocardiogram (2D Echo) is a 2-dimensional graphic of the heart's movement, valves and
STAT Cardiac Testing is available for inpatients only. ECHOCARDIOGRAM Cardiac Diagnostic Testing A (transthoracic) echocardiogram (2D Echo) is a 2-dimensional graphic of the heart's movement, valves and
FFR-CT Not Ready for Primetime
 FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry