American Heart Association (AHA) Mission: Lifeline
|
|
|
- Andrew Thompson
- 5 years ago
- Views:
Transcription

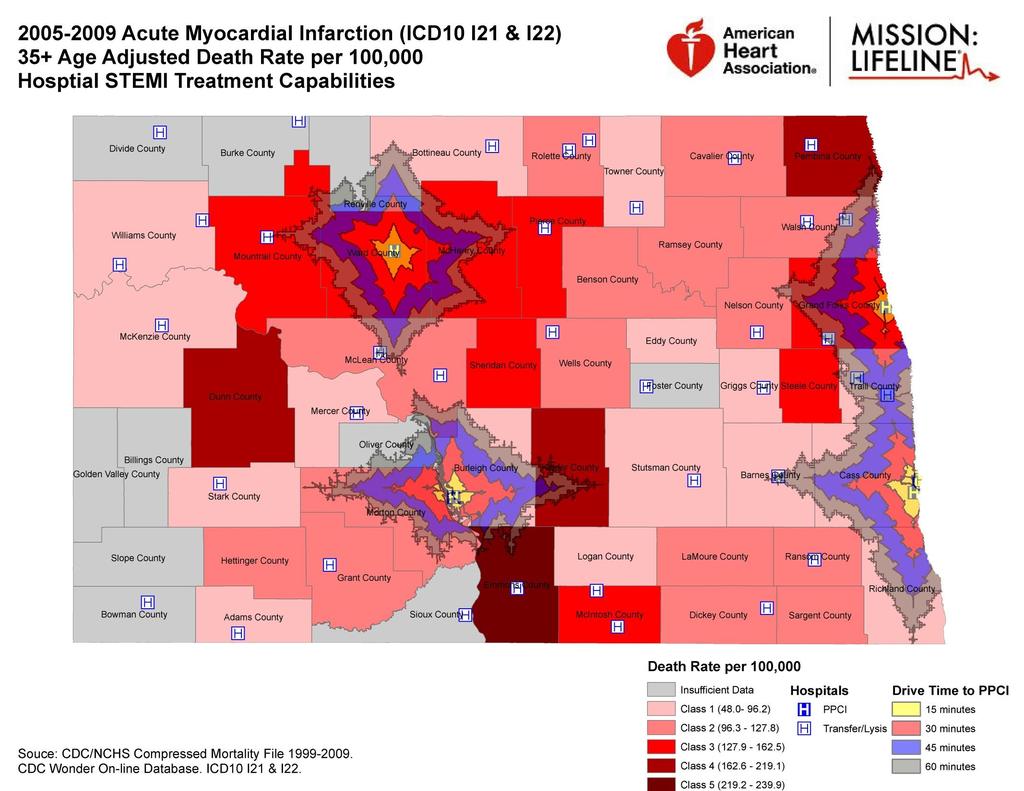
1 American Heart Association (AHA) Mission: Lifeline Optimizing STEMI systems in Rural and Resource Limited Environments: North Dakota - Reperfusion decision making: Lytic vs. PCI, ND Case Scenarios Audio: Toll Free: Participant passcode: LIFELINE Webinar: URL: Conference number: RG Audience passcode: LIFELINE Participants can join the event directly at: , American Heart Association 1
 or thrombolytic therapy Of those who receive PCI, only 40% are treated within the door-to-balloon timeframe of 90 minutes, recommended by the American Heart Association Of those")
2 National Mission: Lifeline STEMI Statistics Almost 250,000 Americans experience STEMI, the deadliest form of heart attack, each year 30% STEMI patients fail to receive percutaneous coronary intervention (PCI) or thrombolytic therapy Of those who receive PCI, only 40% are treated within the door-to-balloon timeframe of 90 minutes, recommended by the American Heart Association Of those who receive thrombolytic therapy, fewer the half are treated within the recommended door-to-needle timeframe of 30 minutes 70% of those patients who aren t eligible for thrombolytic therapy fail to receive PCI, the only other option to restore blood flow to blocked arteries 5/9/ , American Heart Association 2

3 Point Of Entry Protocol : GOAL Less than 90 Minutes Improving the System of Care for STEMI Patients 3



4 ND STEMI Statistics In ND 43% of adults have 3 or more risk factors for Cardiovascular disease. CV disease is the #1 leading cause of death in ND. 5/9/2014 Heart Disease and Stroke Statistic 2011 Update: A Report From the American Heart Association Statistics 4 Committee and Stroke Statistics Subcommittee. Circulation 2011;123:e18-e209.
5 ND Demographics ND Geography: 68,975 sq. miles 680,000 people Frontier counties (37) majority of ND territory Population density of < 6 people/mile = 21% ND residents Rural counties (10): < 5000 residents Population density of > 6/mile = 15% ND residents Urban counties (4): 1 city of at least 15,000 = 63 % ND residents 5

6 6

7 7
8

9 5/9/2014 9

10 5/9/


11 ND Mission: Lifeline 7.1 Million August The Leona M. and Harry B. Helmsley Charitable Trust State of ND Otto Bremer Dakota Medical Foundation American Heart Association 6 PCI Receiving Hospitals Anonymous private donor Improving the System of Care for STEMI Patients 11
12 North Dakota Mission Lifeline Regional Report Qtr.4,
13 STEMI Diagnosis ND State Nation First ECG obtained Pre-Hospital (EMS Arr.) Direct 89% 73% Transfer 51% 34% STEMI Noted on first ECG Direct 87% 86% Transfer 90% 86%
14 Mode of Arrival ND State Nation Private Vehicle -Direct 50% 36% Transfer 73% 74% EMS Direct 49% 61% Transfer 27% 26%
15 Median Time to Reperfusion ND State Nation Primary PCI Direct Presentation in minutes Transfer Fibrinolysis Administration (Ref. Hosp.) minutes Reperfusion Method ND State Nation Primary PCI Overall 70% 85% Direct Presentation 94% 90% Transfers 51% 74% Fibrinolytics Transfer 47% 18%
16 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and Interventions American College of Cardiology Foundation and American Heart Association, Inc.
17 Citation This slide set is adapted from the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction (Journal of the American College of Cardiology). Published on December 17, 2012, available at: The full-text guidelines are also available on the following Web sites: ACC ( and AHA (my.americanheart.org)
18 Slide Set Editors Patrick T. O Gara, MD, FACC, FAHA Frederick G. Kushner, MD, FACC, FAHA, FSCAI The STEMI Writing Committee Members Patrick T. O Gara, MD, FACC, FAHA, Chair Frederick G. Kushner, MD, FACC, FAHA, FSCAI Vice Chair Deborah D. Ascheim, MD, FACC Donald E. Casey, Jr, MD, MPH, MBA, FACP, FAHA Mina K. Chung, MD, FACC, FAHA* James A. de Lemos, MD, FACC* Steven M. Ettinger, MD, FACC* James C. Fang, MD, FACC, FAHA* Francis M. Fesmire, MD, FACEP* Barry A. Franklin, PhD, FAHA Christopher B. Granger, MD, FACC, FAHA* Harlan M. Krumholz, MD, SM, FACC, FAHA* David X. Zhao, MD, FACC* Jane A. Linderbaum, MS, CNP-BC David A. Morrow, MD, MPH, FACC, FAHA* L. Kristin Newby, MD, MHS, FACC, FAHA* Joseph P. Ornato, MD, FACC, FAHA, FACP, FACEP* Narith Ou, PharmD Martha J. Radford, MD, FACC, FAHA Jacqueline E. Tamis-Holland, MD, FACC Carl L. Tommaso, MD, FACC, FAHA, FSCAI# Cynthia M. Tracy, MD, FACC, FAHA Y. Joseph Woo, MD, FACC, FAHA ACCF/AHA representative; ACP representative; ACCF/AHA Task Force on Practice Guidelines liaison; ACCF/AHA Task Force on Performance Measures liaison; ACEP representative; #SCAI representative.


19 Classification of Recommendations and Levels of Evidence A recommendation with Level of Evidence B or C does not imply that the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Although randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective. *Data available from clinical trials or registries about the usefulness/ efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use. For comparative effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
20 Guideline for STEMI Onset of Myocardial Infarction
21 Onset of Myocardial Infarction Community Preparedness and System Goals for Reperfusion Therapy
22 Onset of Myocardial Infarction Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to-Treatment Goals
.")
23 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure initially seen at a non PCI-capable hospital should be transferred for cardiac catheterization and revascularization as soon as possible, irrespective of time delay from MI onset (Class I, LOE: B). Angiography and revascularization should not be performed within the first 2 to 3 hours after administration of fibrinolytic therapy.
24 Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to-Treatment Goals I IIa IIb III All communities should create and maintain a regional system of STEMI care that includes assessment and continuous quality improvement of EMS and hospital-based activities. Performance can be facilitated by participating in programs such as Mission: Lifeline and the D2B Alliance. I IIa IIb III Performance of a 12-lead ECG by EMS personnel at the site of FMC is recommended in patients with symptoms consistent with STEMI.
25 Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to- Treatment Goals I IIa IIb III Reperfusion therapy should be administered to all eligible patients with STEMI with symptom onset within the prior 12 hours. I IIa IIb III I IIa IIb III Primary PCI is the recommended method of reperfusion when it can be performed in a timely fashion by experienced operators. EMS transport directly to a PCI-capable hospital for primary PCI is the recommended triage strategy for patients with STEMI with an ideal FMC-to-device time system goal of 90 minutes or less.* *The proposed time windows are system goals. For any individual patient, every effort should be made to provide reperfusion therapy as rapidly as possible.
26 Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to- Treatment Goals I IIa IIb III Immediate transfer to a PCI-capable hospital for primary PCI is the recommended triage strategy for patients with STEMI who initially arrive at or are transported to a non PCI-capable hospital, with an FMC-to-device time system goal of 120 minutes or less.* I IIa IIb III In the absence of contraindications, fibrinolytic therapy should be administered to patients with STEMI at non PCI-capable hospitals when the anticipated FMC-to-device time at a PCI-capable hospital exceeds 120 minutes because of unavoidable delays. *The proposed time windows are system goals. For any individual patient, every effort should be made to provide reperfusion therapy as rapidly as possible.
27 Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to- Treatment Goals I IIa IIb III When fibrinolytic therapy is indicated or chosen as the primary reperfusion strategy, it should be administered within 30 minutes of hospital arrival.* I IIa IIb III Reperfusion therapy is reasonable for patients with STEMI and symptom onset within the prior 12 to 24 hours who have clinical and/or ECG evidence of ongoing ischemia. Primary PCI is the preferred strategy in this population. *The proposed time windows are system goals. For any individual patient, every effort should be made to provide reperfusion therapy as rapidly as possible.
28 Guideline for STEMI Reperfusion at a Non PCI- Capable Hospital
29 Reperfusion at a Non PCI-Capable Hospital Fibrinolytic Therapy When There Is an Anticipated Delay to Performing Primary PCI Within 120 Minutes of FMC
30 Fibrinolytic Therapy When There Is an Anticipated Delay to Performing Primary PCI Within 120 Minutes of FMC I IIa IIb III I IIa IIb III I IIa IIb III Harm In the absence of contraindications, fibrinolytic therapy should be given to patients with STEMI and onset of ischemic symptoms within the previous 12 hours when it is anticipated that primary PCI cannot be performed within 120 minutes of FMC. In the absence of contraindications and when PCI is not available, fibrinolytic therapy is reasonable for patients with STEMI if there is clinical and/or ECG evidence of ongoing ischemia within 12 to 24 hours of symptom onset and a large area of myocardium at risk or hemodynamic instability. Fibrinolytic therapy should not be administered to patients with ST depression except when a true posterior (inferobasal) MI is suspected or when associated with ST elevation in lead avr.

31 Indications for Fibrinolytic Therapy When There Is a >120-Minute Delay From FMC to Primary PCI
32 Reperfusion at a Non PCI-Capable Hospital Adjunctive Antithrombotic Therapy With Fibrinolysis
33 Adjunctive Antiplatelet Therapy With Fibrinolysis I IIa IIb III Aspirin (162- to 325-mg loading dose) and clopidogrel (300-mg loading dose for patients 75 years of age, 75-mg dose for patients >75 years of age) should be administered to patients with STEMI who receive fibrinolytic therapy.
34 Adjunctive Antiplatelet Therapy With Fibrinolysis I IIa IIb III In patients with STEMI who receive fibrinolytic therapy: aspirin should be continued indefinitely and I IIa IIb III clopidogrel (75 mg daily) for at least 14 days I IIa IIb III o and up to 1 year
35 Adjunctive Antiplatelet Therapy With Fibrinolysis I IIa IIb III It is reasonable to use aspirin 81 mg per day in preference to higher maintenance doses after fibrinolytic therapy.
36 Reperfusion at a Non PCI-Capable Hospital Adjunctive Anticoagulant Therapy With Fibrinolysis
37 Adjunctive Anticoagulant Therapy With Fibrinolysis I IIa IIb III I IIa IIb III I IIa IIb III I IIa IIb III Patients with STEMI undergoing reperfusion with fibrinolytic therapy should receive anticoagulant therapy for a minimum of 48 hours, and preferably for the duration of the index hospitalization, up to 8 days or until revascularization if performed. Recommended regimens include: a. UFH administered as a weight-adjusted intravenous bolus and infusion to obtain an activated partial thromboplastin time of 1.5 to 2.0 times control, for 48 hours or until revascularization; b. Enoxaparin administered according to age, weight, and creatinine clearance, given as an intravenous bolus, followed in 15 minutes by subcutaneous injection for the duration of the index hospitalization, up to 8 days or until revascularization; or c. Fondaparinux administered with initial intravenous dose, followed in 24 hours by daily subcutaneous injections if the estimated creatinine clearance is greater than 30 ml/min, for the duration of the index hospitalization, up to 8 days or until revascularization.

38 Adjunctive Antithrombotic Therapy to Support Reperfusion With Fibrinolytic Therapy

39 Adjunctive Antithrombotic Therapy to Support Reperfusion With Fibrinolytic Therapy (cont.)
40 Reperfusion at a Non PCI-Capable Hospital Transfer to a PCI-Capable Hospital After Fibrinolytic Therapy
41 Reperfusion at a Non PCI-Capable Hospital Transfer of Patients With STEMI to a PCI-Capable Hospital for Coronary Angiography After Fibrinolytic Therapy
42 Transfer of Patients With STEMI to a PCI- Capable Hospital for Coronary Angiography After Fibrinolytic Therapy I IIa IIb III I IIa IIb III Immediate transfer to a PCI-capable hospital for coronary angiography is recommended for suitable patients with STEMI who develop cardiogenic shock or acute severe HF, irrespective of the time delay from MI onset. Urgent transfer to a PCI-capable hospital for coronary angiography is reasonable for patients with STEMI who demonstrate evidence of failed reperfusion or reocclusion after fibrinolytic therapy.
43 Transfer of Patients With STEMI to a PCI- Capable Hospital for Coronary Angiography After Fibrinolytic Therapy I IIa IIb III Transfer to a PCI-capable hospital for coronary angiography is reasonable for patients with STEMI who have received fibrinolytic therapy even when hemodynamically stable* and with clinical evidence of successful reperfusion. Angiography can be performed as soon as logistically feasible at the receiving hospital, and ideally within 24 hours, but should not be performed within the first 2 to 3 hours after administration of fibrinolytic therapy. *Although individual circumstances will vary, clinical stability is defined by the absence of low output, hypotension, persistent tachycardia, apparent shock, high-grade ventricular or symptomatic supraventricular tachyarrhythmias, and spontaneous recurrent ischemia.

44 Indications for Transfer for Angiography After Fibrinolytic Therapy *Although individual circumstances will vary, clinical stability is defined by the absence of low output, hypotension, persistent tachycardia, apparent shock, high-grade ventricular or symptomatic supraventricular tachyarrhythmias, and spontaneous recurrent ischemia.


45 ND M:L EMS Transport Guideline 5/9/


46 Mission: Lifeline ND STEMI Inter- Hospital Transfer Guideline Improving the System of Care for STEMI Patients 46

47 Improving the System of Care for STEMI Patients 47

48 Improving the System of Care for STEMI Patients 48
49 6 STEMI Physician Champion s sign on behalf of all 6 ND PCI Receiving Improving the System of Care for STEMI Patients 49
50 ND Case Reviews STEMI Feedback Report Referring Hospital: 100 miles by ground from PCI Receiving Facility Indicator Actual Time Goal Goal Met Door to 1 st ECG 2 <5 minutes Door to One Call 17 <10 minutes Door to Lytic administration 32 < 30 minutes Door-in to Door-out 117 < 115 minutes Transport time 56 < 55 minutes Sanford Health Door to PCI 16 <20 minutes JRMC Door to PCI 189 < 190 minutes STEMI Medications given prior to CCL: Aspirin, Heparin, TNKase Feedback/Follow-up: This 54 year old female presented to the ED at 0558 with c/o chest pain x 1 ½ hours. A 12L ECG was performed at 0600 and showed anterior ST elevation. The on-call cardiologist was consulted via One Call at The decision was made to administer lytic therapy, and TNKase was given at Plans were made to transfer the patient via helicopter, and they were dispatched at The helicopter was unable to fly, so fixed wing was used. Fixed wing arrived at the patient s beside at 0746 and departed at The patient continued to have slight chest discomfort and ST elevation en route to Sanford, and was therefore admitted directly to the cath lab at Coronary angiography was performed at This revealed a 90% LAD lesion. Thanks to the use of lytic therapy the vessel had TIMI 3 flow (normal) despite the 90% blockage. A PCI was performed at 0907 with good angiographic results. The patient s EF was 50% per an echo performed that same day. The patient did well post PCI and was discharged home on Excellent work ED staff in quickly performing a 12L ECG and recognizing ST elevation. Also, this patient s young age and relatively quick presentation made her a great candidate for lytic therapy. The benefits of lytics were very clear in this case given the fact that she had TIMI 3 flow in the vessel when she arrived in the cath lab. The ED staff administered lytics within 32 minutes after arrival which is great. Unfortunately the Life Flight helicopter was not able to fly and fixed wing had to be used. This results in significantly longer DIDO and transfer times, and makes the use of lytic therapy that much more important! *See below for images Goal met Goal not met 50

51 51

52 52

53 53
54 STEMI Feedback Report Referring Hospital: central ND 100 miles from PCI receiving facility Indicator Actual Time Goal Goal Met Door-in to 1 st ECG unk <5 minutes unk Door-in to One Call 14 <10 minutes Door-in to Lytic 30 < 30 minutes Door-in to Door-out 103 < 100 minutes Transport time 55 < 55 minutes STEMI Medications given prior to CCL: Aspirin, Heparin, Plavix Feedback/Follow-up: This 70 year old female started experiencing left arm pain at approximately She presented to the CAH Hospital ED at A 12L ECG was performed shortly after her arrival which showed anterolateral ST elevation. The on-call cardiologist was consulted via One Call at The decision was made to administer lytic therapy per the ACC/AHA guidelines, as the expected Door to PCI time was greater than 120 minutes, and the patient did not have any obvious contraindications. The helicopter was also dispatched at this time. They arrived at the patient s bedside at 1500 and departed at En route to PCI receiving hospital, the patient experienced a significant mental status change and required intubation. It was also noted that the she had concerning pupillary changes. The patient arrived at Sanford at 1605, and was taken immediately to CT scanning. The CT scan revealed severe intracranial hemorrhage involving the brain stem and mid brain. Cryoprecipitate and FFP were given in an attempt to reverse the thrombolytics. Neurosurgery was consulted for a possible surgical intervention, however, it was determined that this was a non-salvageable injury. The decision was made per the family to withdraw treatment and provide comfort cares only. The patient currently remains on comfort measures. It is very unfortunate that thrombolytics carry the risk of intracranial hemorrhage. The likelihood of this happening is actually very low, at approximately 1%. It is much more likely that lytics will result in a favorable outcome for STEMI patients. Given the patient s relatively early presentation to the ED and lack of contraindications, she appeared to be a good candidate for lytic therapy. Sadly, we can t always know what will be the outcome for patients, and have to do make choices based on what is most likely to produce the best results. Goal met Goal not met 54

55 55
56 STEMI Feedback Report PCI Referring Facility 110 miles from PCI Receiving Facility Indicator Actual Time in minutes Goal Goal Met Door to ECG 0 <5 minutes Door to One Call 3 <10 minutes Door to transport dispatch 28 <5 minutes Door-in to Door-out (includes transfer time to airport and transfer of care to NM Helicopter) 129 <60 minutes Transport time 43 <45 minutes Sanford Health Door to PCI 25 <20 minutes Referral Door to PCI 197 <105 minutes STEMI Medications given prior to CCL: Aspirin, Heparin, Lopressor, Heparin Feedback/Follow-up: This 52 year old male started experiencing chest pain and SOB at approximately 1800 while doing dishes. He presented to the ED at 1807, where a 12L ECG was performed immediately. The ECG showed anterior ST elevation, and One Call was notified at 1810 regarding the need to transfer a STEMI patient. A Helicopter was dispatched at 1839 to transfer the patient. The patient was transferred to the local airport by ground ambulance to meet the helicopter. The helicopter departed the airport at 2016, and the patient arrived in the cath lab at Coronary angiography revealed a 100% occluded proximal LAD. Thrombectomy and stenting was performed on this vessel. The patient s EF was decreased to 35% at the time of the angiogram. Excellent work ED staff in obtaining a 12L ECG without delay and notifying One Call within 3 minutes! There was a delay in dispatching transport. Perhaps this had to do with difficulty arranging a flight service? Also, NM Helicopter arrived at the airport at 1927, however they didn t depart until Presumably this time was spent waiting for the patient to arrive via ground ambulance. Timing out the arrival time of NM Helicopter and the patient at the airport could potentially have saved >40 minutes of infarct time for this patient. Lastly, the AHA/ACC guidelines suggest administering lytic therapy if the expected Door to PCI is >120 minutes. It is virtually impossible for TRF to meet the 120 minute timeframe when transferring to Fargo. Therefore TNKase should always be used if contraindications are not present. *See below for images Goal met Goal not met 56

57 57

58 58
59
60 Case Study #1-Short DIDO 45 yo male CP onset at PMH: No Hx, No meds, current smoker Employed as truck driver in Oil industry Arrival 1819 EKG 1826 (7 min) Anterior Lytics 1844 (25 minutes) Transport Dispatched 1837 (18 min) Door in Door out (39 min) Arrival PCI Center 2004 Cath lab 2004 Wire Cross % LAD Occlusion- DES

61

62
63 Case Study #2- EMS Bypass 60 miles from PCI 37 yo Male, symptom onset 1200 PMH: CAD (previous Inf. Wall MI), Obesity, HTN, Family hx No medications Quit smoking after earlier AMI EMS Dispatch: 1356 Contact: 1407 EKG: 1424 (28 min) Anterior Arrival to PCI Center: 1512 CL: 1530 Wire: 1602 FMC to Reperfusion: 115 minutes Location from PCI

64
65 Case Study #3-Female/Inferior 72 yo Female, onset of CP 2245 PMH: HTN, IDDM, CVA Medications: Insulin, Statin, ASA, Verapamil, Dypyridamole Arrival CAH: 2322 EKG: 2336 (14 min) Inferior Thrombolytics: 0020 (58 min) Transport Dispatch: 0013 DIDO: 0058 (96 min) Arrival PCI Center: 0141 CL 0141 Wire 0228 (100% RCA) Patient coded upon arrival to cath lab and expired

66
67 Case Study #4 TNKase no Heparin 48 yo Male CP onset 0130 PMH: MI X 2, Dyslipidemia, current smoker Non-compliant, not taking medications Arrival CAH: 0238 EKG: 0246 (8 min) Thrombolytics: 0321 (43 min) Transport Dispatch: 0257 (19 min) DIDO: 0401 (83 min) Coded enroute Vfib, multiple shocks Arrival PCI Center: 0456 CL: 0520 Wire: 0538 (RCA 100%)
68 Questions?? Mindy Cook, RN BSN Director Mission: Lifeline North Dakota, Minnesota American Heart Association, Midwest Affiliate Contact Information: 4701 W. 77th St. Minneapolis, MN Office: Fax: /9/
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki. 2013, American Heart Association
 NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: Executive Summary
 Journal of the American College of Cardiology Vol. 61, No. 4, 2013 2013 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/$36.00 Published by Elsevier
Journal of the American College of Cardiology Vol. 61, No. 4, 2013 2013 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/$36.00 Published by Elsevier
Sanford Chest Pain Network: Improving Rural STEMI Outcomes
 Sanford Chest Pain Network: Improving Rural STEMI Outcomes Naveen Rajpurohit, MD Cardiovascular Fellow Sanford Cardiovascular Institute Sanford Heart Hospital The University of South Dakota Sioux Falls,
Sanford Chest Pain Network: Improving Rural STEMI Outcomes Naveen Rajpurohit, MD Cardiovascular Fellow Sanford Cardiovascular Institute Sanford Heart Hospital The University of South Dakota Sioux Falls,
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
 A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Rural Minnesota STEMI Systems of Care
 CARDIOVASCULAR HEALTH UNIT Rural Minnesota STEMI Systems of Care Almost 250,000 Americans experience ST-elevation Myocardial Infarction (STEMI), the deadliest form of heart attack, each year. Of approximately
CARDIOVASCULAR HEALTH UNIT Rural Minnesota STEMI Systems of Care Almost 250,000 Americans experience ST-elevation Myocardial Infarction (STEMI), the deadliest form of heart attack, each year. Of approximately
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
ACTION Registry GWTG Research and Publications Update
 ACTION Registry GWTG Research and Publications Update Dr. Michael Kontos Director, Coronary Intensive Care Unit Pauley Heart Center, Virginia Commonwealth University The following relationships exist:
ACTION Registry GWTG Research and Publications Update Dr. Michael Kontos Director, Coronary Intensive Care Unit Pauley Heart Center, Virginia Commonwealth University The following relationships exist:
REFERRAL HOSPITAL. The Importance of Door In Door Out Time DIDO
 REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Jean Skonhovd,RN,BSN,MSAS Emergency Department Director Avera Heart Hospital of South Dakota Time to Treatment is critical for STEMI patients
REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Jean Skonhovd,RN,BSN,MSAS Emergency Department Director Avera Heart Hospital of South Dakota Time to Treatment is critical for STEMI patients
Transfer in D2B. Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland. The Problem
 Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
Know the Quality of our Care at Every Step. Kansas City ACS Summit BI-State Cardiovascular Education Consortium
 Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
ST Elevated Myocardial Infarction- Latest AHA recommendations
 ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
4. Which survey program does your facility use to get your program designated by the state?
 STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
New STEMI Guidelines
 New STEMI Guidelines L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society of Cardiovascular Patient Care Conflict
New STEMI Guidelines L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society of Cardiovascular Patient Care Conflict
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Improving the Outcomes of
 Improving the Outcomes of STEMI Shelley Valaire, ACP; and Robert Welsh, MD, FRCPC Presented at the University of Alberta s 6th Annual Cardiology Update for General Practitioners and Internists, Edmonton,
Improving the Outcomes of STEMI Shelley Valaire, ACP; and Robert Welsh, MD, FRCPC Presented at the University of Alberta s 6th Annual Cardiology Update for General Practitioners and Internists, Edmonton,
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
2013, American Heart Association
 2013, American Heart Association Mission: Lifeline - Data, Reports and ACTION Registry - GWTG THE MISSION: BETTER HEART ATTACK CARE FOR YOUR COMMUNITY THE LIFELINE: THE AMERICAN HEART ASSOCIATION AND YOU
2013, American Heart Association Mission: Lifeline - Data, Reports and ACTION Registry - GWTG THE MISSION: BETTER HEART ATTACK CARE FOR YOUR COMMUNITY THE LIFELINE: THE AMERICAN HEART ASSOCIATION AND YOU
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Frans Van de Werf, MD, PhD Leuven, Belgium
 STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
Presenters: Disclaimer. Definitions. Deanna Jones, RN, CCRN. Annmarie Keck, RN, CEN
 Presenters: Deanna Jones, RN, CCRN Cardiac Level 1 Coordinator, Providence Sacred Heart Medical Center and Children s Hospital, Spokane, WA Annmarie Keck, RN, CEN Clinical Outreach Educator Northwest MedStar,
Presenters: Deanna Jones, RN, CCRN Cardiac Level 1 Coordinator, Providence Sacred Heart Medical Center and Children s Hospital, Spokane, WA Annmarie Keck, RN, CEN Clinical Outreach Educator Northwest MedStar,
The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network:
 The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network: Nathaniel Niles, MD CREST Symposium November 7th, 28 STEMI = Acute Coronary Thrombosis STEMI
The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network: Nathaniel Niles, MD CREST Symposium November 7th, 28 STEMI = Acute Coronary Thrombosis STEMI
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Mission: Lifeline Addressing the System of STEMI Care
 Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
Dashboard and Outcomes Report with Case Studies
 Dashboard and Outcomes Report with Case Studies Kim Hustler Clinical Quality Consultant, American College of Cardiology The following relationships exist: Kim Hustler: No Disclosures Section F- Procedures
Dashboard and Outcomes Report with Case Studies Kim Hustler Clinical Quality Consultant, American College of Cardiology The following relationships exist: Kim Hustler: No Disclosures Section F- Procedures
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Data Elements and Definitions with Case Studies. Interpreting Your Outcomes Reports. Kim Hustler, Clinical Quality Consultant, NCDR
 Data Elements and Definitions with Case Studies Interpreting Your Outcomes Reports Kim Hustler, Clinical Quality Consultant, NCDR Beth Pruski, Program Manager, NCDR The following relationships exist: Beth
Data Elements and Definitions with Case Studies Interpreting Your Outcomes Reports Kim Hustler, Clinical Quality Consultant, NCDR Beth Pruski, Program Manager, NCDR The following relationships exist: Beth
Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences
 Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences Dr. Henry H. Ting, Mayo Clinic College of Medicine Dr. James G. Jollis,, Duke University Medical Center Mayo Clinic STEMI System for Transferred
Regional STEMI Transfer Systems: the Mayo and NC RACE Experiences Dr. Henry H. Ting, Mayo Clinic College of Medicine Dr. James G. Jollis,, Duke University Medical Center Mayo Clinic STEMI System for Transferred
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Update on STEMI Guidelines. Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center
 Update on STEMI Guidelines Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center All Rights Reserved, Duke Medicine 2008 Disclosures Research Grants: NHLB, AHRQ, AstraZeneca,
Update on STEMI Guidelines Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center All Rights Reserved, Duke Medicine 2008 Disclosures Research Grants: NHLB, AHRQ, AstraZeneca,
STEMI ST Elevation Myocardial Infarction
 STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
Management of STEMI in era of Reperfusion. Eagles Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police
 Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
ACCF/AHA Guideline ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 Circulation is available at http://circ.ahajournals.org ACCF/AHA Guideline 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction A Report of the American College of Cardiology
Circulation is available at http://circ.ahajournals.org ACCF/AHA Guideline 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction A Report of the American College of Cardiology
Controversies on Primary angioplasty in STEMI
 Controversies on Primary angioplasty in STEMI 원주의대이승환 Case ( 51/M) CC C.C: ongoing squeezing chest pain D : for 2 hours Risk factors Current smoker ( 40 PYs) Hypercholesterolemia (+) Case ( 51/M) Physical
Controversies on Primary angioplasty in STEMI 원주의대이승환 Case ( 51/M) CC C.C: ongoing squeezing chest pain D : for 2 hours Risk factors Current smoker ( 40 PYs) Hypercholesterolemia (+) Case ( 51/M) Physical
Update Guidelines in STEMI Management: Focus on Logistic and System Approach to Reperfusion Therapy
 March 14 th, 2018 The First Asia Forum in Emergency Medicine BNH Hospital, Bangkok, Thailand Update Guidelines in STEMI Management: Focus on Logistic and System Approach to Reperfusion Therapy Wacin Buddhari,
March 14 th, 2018 The First Asia Forum in Emergency Medicine BNH Hospital, Bangkok, Thailand Update Guidelines in STEMI Management: Focus on Logistic and System Approach to Reperfusion Therapy Wacin Buddhari,
The American College of Cardiology/American Heart
 ACC/AHA/SCAI Practice Guideline ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention Summary Article A Report of the American College of Cardiology/American Heart Association Task
ACC/AHA/SCAI Practice Guideline ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention Summary Article A Report of the American College of Cardiology/American Heart Association Task
STEMI, Non-STEMI, Chest Pain?
 Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Level One STEMI Connecting the Dots changing Points of Care into Systems of Care
 Level One STEMI Connecting the Dots changing Points of Care into Systems of Care Myron Bloom MD MMM Medical Director Rural Healthcare Quality Network RHQN.org drmbloom@msn.com The Eastern Washington Level
Level One STEMI Connecting the Dots changing Points of Care into Systems of Care Myron Bloom MD MMM Medical Director Rural Healthcare Quality Network RHQN.org drmbloom@msn.com The Eastern Washington Level
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome (ACS) Initial Evaluation and Management
 Initial Evaluation and Management") Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
EMS Recognition Webinar August 24, 2017
 EMS Recognition Webinar August 24, 2017 Today s objectives: Provide you with some rationale regarding the importance of reducing FMC to device time Provide you with an overview of the 2017 Mission: Lifeline
EMS Recognition Webinar August 24, 2017 Today s objectives: Provide you with some rationale regarding the importance of reducing FMC to device time Provide you with an overview of the 2017 Mission: Lifeline
2008, American Heart Association. All rights reserved.
 AHA 2008 Cocaine-Associated Chest Pain and Myocardial Infarction Slide Set Based on the AHA 2008 Scientific Statement for Management of Cocaine-Associated Chest Pain and Myocardial Infarction George J.
AHA 2008 Cocaine-Associated Chest Pain and Myocardial Infarction Slide Set Based on the AHA 2008 Scientific Statement for Management of Cocaine-Associated Chest Pain and Myocardial Infarction George J.
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 Journal of the American College of Cardiology Vol. 61, No. 4, 2013 2013 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/$36.00 Published by Elsevier
Journal of the American College of Cardiology Vol. 61, No. 4, 2013 2013 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/$36.00 Published by Elsevier
Identification and pre-notification using 12-Lead. Why this so important to our STEMI System
 Identification and pre-notification using 12-Lead Why this so important to our STEMI System Jim Smith, MD Great Plains Health, North Platte Chair, NE State EMS Board Medical Director, Emergency Services,
Identification and pre-notification using 12-Lead Why this so important to our STEMI System Jim Smith, MD Great Plains Health, North Platte Chair, NE State EMS Board Medical Director, Emergency Services,
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Coronary Catheterization and Percutaneous Coronary Intervention in China 10-Year Results From the China PEACE-Retrospective CathPCI Study
 Coronary Catheterization and Percutaneous Coronary Intervention in China 10-Year Results From the China PEACE-Retrospective CathPCI Study Xin Zheng, MD, PhD; Jeptha P. Curtis, MD; Shuang Hu, PhD; YongfeiWang,
Coronary Catheterization and Percutaneous Coronary Intervention in China 10-Year Results From the China PEACE-Retrospective CathPCI Study Xin Zheng, MD, PhD; Jeptha P. Curtis, MD; Shuang Hu, PhD; YongfeiWang,
Appropriate Timing for Coronary Revascularization Post - MI. Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center
 Appropriate Timing for Coronary Revascularization Post - M Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center Disclosures nterventional cardiologist Clinical Cardiovascular
Appropriate Timing for Coronary Revascularization Post - M Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center Disclosures nterventional cardiologist Clinical Cardiovascular
Treatment of ST-elevation myocardial infarction in China: Where are we?
 Treatment of ST-elevation myocardial infarction in China: Where are we? Associate Professor, Yihong Sun, MD Peking University People s Hospital Beijing, China Disclosure conflict of Interest The Challenges
Treatment of ST-elevation myocardial infarction in China: Where are we? Associate Professor, Yihong Sun, MD Peking University People s Hospital Beijing, China Disclosure conflict of Interest The Challenges
When the learner has completed this module, she/he will be able to:
 Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
King County EMS STEMI Patients Receiving PCI at King County Hospitals in 2012
 King County EMS STEMI Patients Receiving PCI at King County Hospitals in 2012 Objective The goal of this report is to evaluate demographics, pre hospital and hospital response times and outcomes of ST
King County EMS STEMI Patients Receiving PCI at King County Hospitals in 2012 Objective The goal of this report is to evaluate demographics, pre hospital and hospital response times and outcomes of ST
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Acute Coronary Syndrome
 Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
2018 Acute Coronary Syndrome. Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute
 2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
Therapies for ACS The Articles You ve Got to Know!!
 Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ
 William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ PROBLEM: blood supply to the heart has been compromised and heart
William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ PROBLEM: blood supply to the heart has been compromised and heart
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Marcin Dada, MD December 03, 2013
 STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
STEMI Network. Joseph L. Fredi, M.D., FACC. The median D2B time for patients presenting to the Vanderbilt ED was 55 minutes.
 STEMI Network STEMI News By Joseph Fredi, M.D., FACC, and Carol R. Scott, B.S.N., M.S.N., coordinators, STEMI Network, Vanderbilt Heart and Vascular Institute Even with the great success our STEMI Network
STEMI Network STEMI News By Joseph Fredi, M.D., FACC, and Carol R. Scott, B.S.N., M.S.N., coordinators, STEMI Network, Vanderbilt Heart and Vascular Institute Even with the great success our STEMI Network
 KEARNEY NEBRASKA Clinic Visits Performed per Year: 23,000 Diagnostic Angiograms: 1,600 PCI: 720 (778 DES, 247 BMS) CV Surgery: 325 Carotid Artery Stents: 85 Peripheral Interventions: 220 Implantable
KEARNEY NEBRASKA Clinic Visits Performed per Year: 23,000 Diagnostic Angiograms: 1,600 PCI: 720 (778 DES, 247 BMS) CV Surgery: 325 Carotid Artery Stents: 85 Peripheral Interventions: 220 Implantable
MI MANAGEMENT: ACS Guideline Review. Ben Ochoa BS, RCIS, RCS
 MI MANAGEMENT: ACS Guideline Review en Ochoa S, RCIS, RCS Objectives Discuss management of patients with Non-ST-Elevation Acute Coronary Syndromes. Discuss management of patients with ST-Elevation Acute
MI MANAGEMENT: ACS Guideline Review en Ochoa S, RCIS, RCS Objectives Discuss management of patients with Non-ST-Elevation Acute Coronary Syndromes. Discuss management of patients with ST-Elevation Acute
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI?
 SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD
 Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD Should PCI center activate the cathlab off EMS field interpretation of ECG? Is this happening consistently in New Mexico? What is acceptable rate
Mark C. Bieniarz, MD Andrew Harrell, MD Peter Berger, MD Should PCI center activate the cathlab off EMS field interpretation of ECG? Is this happening consistently in New Mexico? What is acceptable rate
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
KCS Congress: Impact through collaboration
 STEMI IN A NEW INTERVENTIONAL ENVIRONMENT Harun A Otieno, FACC June 29th, 2017 KCS Congress: Impact through collaboration Disclosures I have no conflicts of interest for this talk I have no relationships
STEMI IN A NEW INTERVENTIONAL ENVIRONMENT Harun A Otieno, FACC June 29th, 2017 KCS Congress: Impact through collaboration Disclosures I have no conflicts of interest for this talk I have no relationships
Name Authentication Date (Position or Committee) Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee
 Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee") Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
HAAD quality KPI; waiting time
 Type: Waiting Time Indicator Indicator Number: WT001 Primary Care Appointment- Outpatient Setting Time to see a HAAD licensed family physician or member of their team (GP) Time of request (walk-in or by
Type: Waiting Time Indicator Indicator Number: WT001 Primary Care Appointment- Outpatient Setting Time to see a HAAD licensed family physician or member of their team (GP) Time of request (walk-in or by
STEMI in the State of Jefferson ASSET - 5 Years Later. Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center
 STEMI in the State of Jefferson ASSET - 5 Years Later Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center Sept 22, 2008 Percent # Procedures Performed Coronary
STEMI in the State of Jefferson ASSET - 5 Years Later Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center Sept 22, 2008 Percent # Procedures Performed Coronary
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
PPCI in STEMI. ESC at the 22nd Annual Conference of the Saudi Heart Association February 21th, 2011
 PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Reperfusion Strategies for the STEMI Patient - PCI versus Thrombolysis
 Reperfusion Strategies for the STEMI Patient - PCI versus Thrombolysis Scott Mikesell, DO, FACC, FSCAI, FSVM STEMI Program Director Cardiac Catheterization Laboratory Director St. Luke s Hospital, Duluth,
Reperfusion Strategies for the STEMI Patient - PCI versus Thrombolysis Scott Mikesell, DO, FACC, FSCAI, FSVM STEMI Program Director Cardiac Catheterization Laboratory Director St. Luke s Hospital, Duluth,
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/21543 holds various files of this Leiden University dissertation Author: Dharma, Surya Title: Perspectives in the treatment of cardiovascular disease :
Cover Page The handle http://hdl.handle.net/1887/21543 holds various files of this Leiden University dissertation Author: Dharma, Surya Title: Perspectives in the treatment of cardiovascular disease :
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee