Percutaneous Transcatheter Treatment of Valvular Disease TAVR and Beyond
|
|
|
- Dwight Baker
- 5 years ago
- Views:
Transcription
1 Percutaneous Transcatheter Treatment of Valvular Disease TAVR and Beyond CREIGHTON W. DON, MD, PHD ASSOCIATE PROFESSOR OF MEDICINE DIRECTOR, INTERVENTIONAL AND STRUCTURAL HEART FELLOWSHIPS DIVISION OF CARDIOLOGY UNIVERSITY OF WASHINGTON

2 TAVR: PARTNER High Risk 5-year Mortality Outcomes Mack MJ. Lancet. 2015
3 PARTNER II: Intermediate Risk TF cohort Stroke Surgery TAVR 30 d 6.1% 5.5% 1 year 8.1% 8.0%


4 TAVR: PIVOTAL High Risk CoreValve New pacemaker 25.8%
5 Intermediate Risk--SURTAVI


6 Event Rate (%) All-cause Mortality at 30 Days RESPOND & Other Real World TAVI Registries Studies FRANCE 2 Registry 1 SAPIEN SOURCE 2 TVT Registry 3 SAPIEN XT SOURCE 4 CoreValve ADVANCE 5 LOTUS RESPOND 6 STS Score: 14.4 NA N: Results from different studies not directly comparable. Information provided for educational purpose only. 1 FRANCE:Gilard, et al. N Engl J Med 2012; 366: SOURCE : Thomas, et al. Circulation. 2010; 122: Mack, et al. JAMA 2013;310: SOURCE XT: Schymik, et al. JACC 2015; 8.5: CoreValve ADVANCE: Linke A, EuroPCR Lotus RESPOND: ACC Boston Scientific Corporation All Rights Reserved. For internal Educational Use only. Do not copy, forward or distribute.

7 Transcatheter aortic valve (TAVR)



8 Transcatheter aortic valve (TAVR)






9 TAVR: Next generation valves Portico Engager Symetis Direct Flow Jenavalve Boston Lotus
 will be nearly as")

10 Where do we go from here? TAVR (native AS) will be nearly as ubiquitous as PCI Valve-in-valve, Extreme-risk TAVR, Aortic Regurgitation Mitral and tricuspid valve therapies
11 TAVR: Ongoing challenges VALVE IN VALVE, CORONARY OBSTRUCTION, EXTREME RISK PATIENTS





12 TAVR: Valve-in-Valve



13 TAVR: Valve-in-Valve



14 Valve-in-Valve 97 yo man with Medtronic 23 mm Hancock AV 4.1 m/s, 42 mmhg

15 Valve-in-Valve 23 Sapien XT
16 Dvir D. Circulation Dvir D. JAMA TAVR Valve-in-valve Global VIV registry 202 Patients with failed aortic bioprostheses (regurg/stenosis)

17 POST-TAVR Mean Gradient Courtesy John Webb, MD

18 TAVR: Valve-in-Valve Date AVA Mean grad Velocity 7/23/ mmhg 4.1 m/s 7/30/ mmhg 2.6 m/s 8/28/ mmhg 3.2 m/s 2/5/ mmhg 3.7 m/s 8/13/ mmhg 3.8 m/s
19 UW Experience 25 patients with valve-in-valve TAVR 3 patients with increasing gradients Goleski P, Don C. CCI 2016.


20 Valve-in-valve: Fracturing Bioprosthetic valve fracturing Saxon JT. Interventional Cardiology Review 2018;13(1):20 6.

21 Valve-in-valve: Fracturing Saxon JT. Interventional Cardiology Review 2018;13(1):20 6.
22 Valve-in-valve: Fracturing Saxon JT. Interventional Cardiology Review 2018;13(1):20 6.

23 Coronary Obstruction


24 BASILICA (Leaflet laceration/coronary obstruction) Khan, J.M. et al. J Am Coll Cardiol. Int. 2018



25 Valve-in-Valve RCA Coronary evaluation LCA
26 TAVR Exteme Risk 65 yo man with severe aortic stenosis in shock On IABP, dobutamine, phenylephrine, norepinephrine, vasopressin Acute renal failure Cr 3.1 Troponin 22 EF 20% Severe mitral regurgitation RA 17, PA 65/30, Wedge 25, CI 2.3 PAPI 2.0


27 Tandem Heart supported TAVR

28 Patient Selection: Emergent TAVR Cardiogenic shock/pressor dependent Cardiac arrest within 24 hrs Unstable ventricular arrhythmia Severe, unrelenting chest pain Mechanical circulatory support Decompensated heart failure requiring intubation
29 TAVR Extreme Risk Emergent/Shock TAVR PARTNER Cohort B 39% 44.1% 51% 33%
30 Survival by timing of MCS placement
31 The next best thing is coming here TRANSCATHETER MITRAL VALVE THERAPIES



32 Mitral Valvuloplasty
33 % Moderate to severe disease % Moderate to severe disease Epidemiology United States 1.7% of US population Olmstead County Nkomo VT. Et al. Lancet Sep 16;368(9540):

34 Heart Failure and Mitral Regurgitation Patients with chronic heart failure in 4 Italian Centers 73% of patients have FMR Rossi. Heart. 2011;97:
:1231-48.")
35 Mitral Valve Anatomy Degenerative Leaflets/chords/papillary Fibrotic/Calcified Leaflets/chords/annulus Functional Dilated ventricle/annulus Papillary muscle tethering Asgar AW et al. J Am Coll Cardiol Mar 31;65(12):





36 Percutaneous Valve Solutions MitraClip Percutaneous Valves TAVR in mitral Tiara (Neovasc), Tendyne, CardiAQ, Twelve
37 Percutaneous Annular Solutions Carillon (Cardiac Dimensions) Cardioband (Valtech) AccuCinch (Ancora Heart) Mitralign
38 Heart Failure and Mitral Regurgitation ATTEND registry (4842 patients) Moderate-Severe functional MR (at discharge) prevalence Preserved EF 18.4% Reduced EF 31.7% Kajimoto K et al. Eur J Heart Fail Aug;18(8):
39 Surgery for functional MR Retrospective propensity matched comparison Patients with severe MR and LVEF <30% Those undergoing MV compared to those medically managed Non-MVA MVA AHA/ACC 2017 Guideline Update Transcatheter mitral valve repair or mitral valve surgery for functional mitral insufficiency with a background of GDMT (IIB) Wu AH et al. J Am Coll Cardiol Feb 1;45(3):381-7.
40 MV surgery and CABG STITCH study Patients with severe mitral regurgitation MVR performed during CABG at operator s discretion CABG only 55 pts CABG/MVR 49 pts Rx 116 pts Grayburn D et al. Circulation (21)
41 Flail Mitral Regurgitation Surgery Mitral Regurgitation International Database ( ) 2097 patients with flail mitral valve leaflets Mean follow-up 10.3 years Suri RM. JAMA Aug 14;310(6):
:1112-7")
42 Progression of MR and LV dysfunction 1 Cioffi G, et al. European Journal of Heart Failure 2005 Dec;7(7):1112-7
43 Mitral valve replacement




44 Tiara Mitral Regurgitation Clinical Trial High risk surgical patients with severe MR Cheung A at al. EuroIntervention. 2016;12;Y70-Y72.
45 TAVR in Mitral Stenosis/Regurg 71 year-old-man XRT germ cell tumor at age 35 Significant coronary artery disease and aortic regurgitation CABG and mechanical AVR at age 62 Known to have moderate mitral regurgitation and stenosis Patient did well for a 6-7 years, starts developing dyspnea and LE edema Diagnosed with severe pulmonary HTN and told he had no options Becomes despondent and stops following up with his physicians 1-year later presents to the hospital with NYHA class 4 symptoms, ascites, and severe LE edema


46 Mixed Mitral Regurgitation/Stenosis Mean gradient 11 mmhg Mod-sev regurgitation PA pressure mmhg


47 Mixed Mitral Regurgitation/Stenosis


48 Severe Mitral Regurgitation/Stenosis


49 Risk of LVOT Obstruction Depth of implant Flaring of device Mitral-LVOT angle Septal hypertrophy Anterior mitral leaflet




50 Parallel vs Conical deployment


51 Anterior mitral leaflet and LVOT


52 CT scan Annular Area 621 mm2 28 mm Annular Perimeter 92 mm 29 mm Aortic-Mitral angle 113 degrees Derived Diameter
-Sapien")
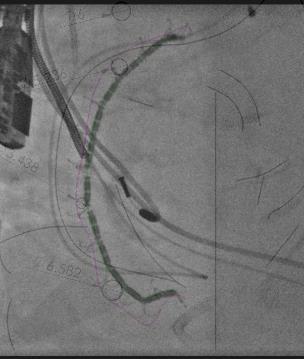
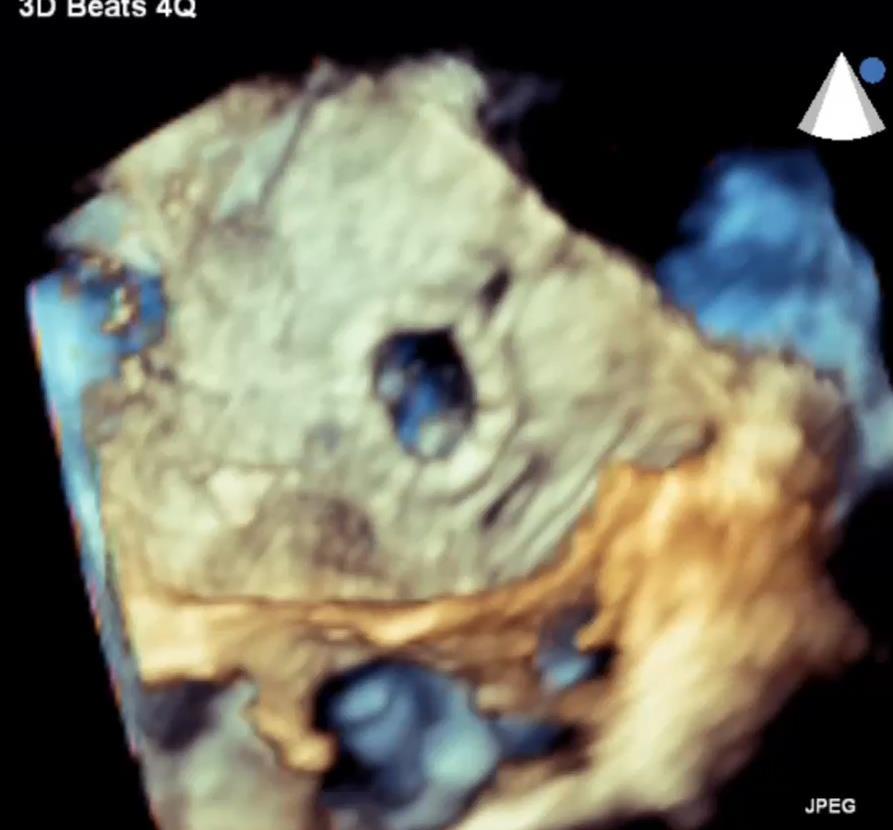
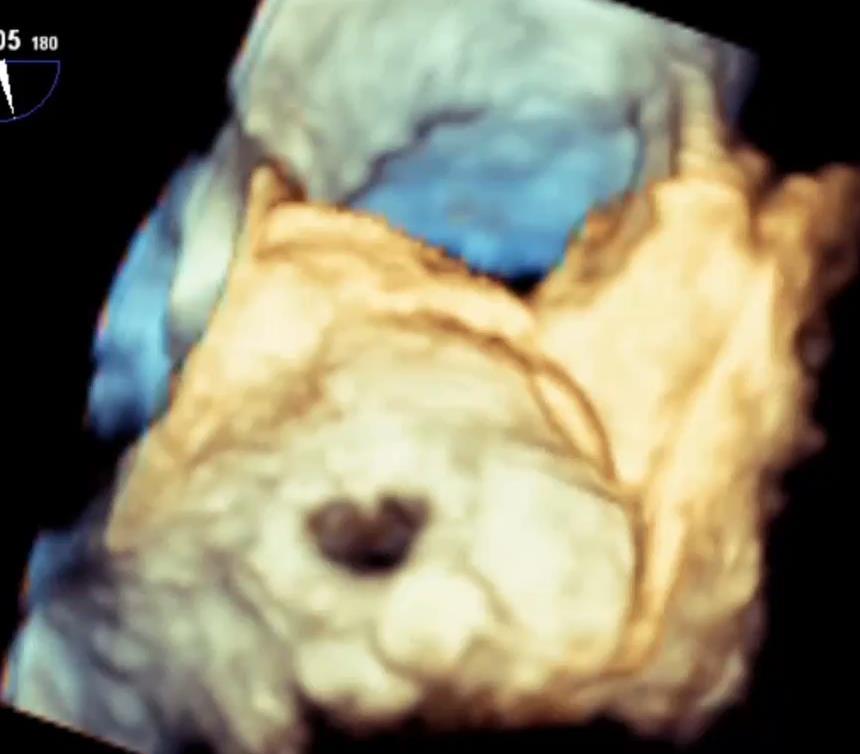
53 Transcatheter Native Mitral Valve Replacement (TMVR)-Sapien XT 29


54 Transcatheter Native Mitral Valve Replacement (TMVR)-Sapien XT 29


55 Transcatheter Native Mitral Valve Replacement (TMVR)-Sapien XT 29


56 Transcatheter Native Mitral Valve Replacement (TMVR)


57 Mean gradient 3 mmhg Mild-moderate regurgitation
58 Hybrid surgical TMVR 81 yo man with severe mitral regurgitation and NYHA class III symptoms. LVEF 50% PMH Severe mitral regurgitation Atrial fibrillation DVT/PE


59 Mitral regurgitation Thickened mitral leaflets (mean gradient 2 mmhg) Decreased posterior leaflet motion Pulmonary venous systolic flow reversal

60 Mitral regurgitation Thickened mitral leaflets (mean gradient 2 mmhg) Decreased posterior leaflet motion Pulmonary venous systolic flow reversal


61 Mitral regurgitation A prior chest CT was evaluated showing significant mitral annular calcification Annular area 826 mm2 Annular diameter 39.8x24.5 mm Aorto-mitral angle 112 degrees

62 Intraoperative TEE Very large annulus Concern for LVOT obstruction

63 Hybrid Surgical Transcatheter TAVR in Mitral Resection of anterior mitral leaflet Six annular sutures were placed Direct deployment of the Edwards Sapien S3 29 mm valve with 4 extra cc s of contrast was performed from the exposed left atrium 80:20 deployment to center the sealing skirt at the annulus level The 6 sutures were then attached to the bottom skirt of the Sapien S3 to secure the valve

64 LVOT obstruction from anterior mitral leaflet Bapat V. Catheter Cardiovasc Interv Oct;86(4):747-60


65 Post-TMV TEE


66 Hybrid surgical-transcatheter TAVR valve for mitral regurgitation Open, direct transcatheter mitral placement using a Sapien S3 valve 80:20 deployment using over-expanded valve Surgical sutures to secure valve and cinch annulus Anterior mitral leaflet resection to avoid LVOT obstruction
67 Mitral valve repair

 5% 10% Feldman T et al. JACC.")
68 EVEREST 5-Year Results Randomized MitraClip v. Surgery MitraClip184 patients Surgery 95 patients 30d Outcome MitraClip Surgery Blood Transfusion 2 u 13% 45% Repeat Surgery 20% 2.2% MACE (excl. bleeding) 5% 10% Feldman T et al. JACC (25)
69 Clinical improvement-mitraclip Transient drop in LVEF, with recovery/improvement at discharge Improved forward stroke volume Reduction in LVEDD/volumes Reduction in PAP Improved quality of life Improved 6-minute walk times Reduction in BNP Auricchio A Et al. JACC (21) Melisurgo G et al. Am J Cardiol 2014; 113: Grayburn et al. Circulation. 2013;128: Glower DD et al. JACC. 2014, Vol.64(2), p Taramasso et al. EuroIntervention. 2014;10: Frazen O et al. European Journal of Heart Failure (2011) 13,


70 Typical MitraClip Case 69 yo man with LVEF 45% multiple hospitalizations for heart failure, NYHA 3-4

71 Posterior prolapse + annular dilation + redundant leaflet


72 Clip rotation and approach


73 Grasping


74 Second clip laterally


75 Final

76 Mitraclip 76 yo woman EF 20%--biv pacer, moderate severe MR hospitalized x 3 weeks

77 Mitraclip 76 yo woman, EF 20% EF 20%--biv pacer, moderate severe MR hospitalized x 3 weeks


78 Mitraclip 76 yo woman, EF 20% Repeat echo 2 months later: Mild MR, EF 29%
 Not treated with GDMT (n=79) All inclusion criteria not met (n=85) Exclusion criteria present (n=34) Echo criteria not met (n=255) Incomplete screening or other (n=419)")
79 COAPT: Study Flow and Follow-up 1576 pts with HF and MR Roll-in cases N=51 at 34 sites Eligible for enrollment N=665 Randomized N=614 at 78 sites Ineligible N=911 Reasons for exclusion Inadequate MR or DMR (n=244) Not treated with GDMT (n=79) All inclusion criteria not met (n=85) Exclusion criteria present (n=34) Echo criteria not met (n=255) Incomplete screening or other (n=419) MitraClip + GDMT N=302 GDMT alone N=312
80 COAPT: Key Inclusion Criteria 1. Ischemic or non-ischemic cardiomyopathy with LVEF 20%-50% and LVESD 70 mm 2. Moderate-to-severe (3+) or severe (4+) secondary MR 3. NYHA functional class II-IVa (ambulatory) despite a stable maximally-tolerated GDMT regimen and CRT (if appropriate) 4. At least one HF hospitalization within 12 months and/or a BNP 300 pg/ml* or a NTproBNP 1500 pg/ml* 5. Not appropriate for mitral valve surgery 6. IC believes secondary MR can be successfully treated by the MitraClip Adjusted by a 4% reduction in the BNP or NT-proBNP cutoff for every increase of 1 kg/m 2 in BMI >20 kg/m 2
81 Baseline Characteristics (ii) HF parameters MitraClip + GDMT (N=302) GDMT alone (N=312) Echo core lab MitraClip + GDMT (N=302) GDMT alone (N=312) Etiology of HF MR severity - Ischemic 60.9% 60.6% - Mod-to-sev (3+) 49.0% 55.3% - Non-ischemic 39.1% 39.4% - Severe (4+) 51.0% 44.7% NYHA class EROA, cm ± ± I 0.3% 0% LVESD, cm 5.3 ± ± II 42.7% 35.4% LVEDD, cm 6.2 ± ± III 51.0% 54.0% LVESV, ml ± ± IV 6.0% 10.6% LVEDV, ml ± ± 72.9 HF hosp w/i 1 year 58.3% 56.1% LVEF, % 31.3 ± ± 9.6 Prior CRT 38.1% 34.9% - 40% 82.2% 82.0% Prior defibrillator 30.1% 32.4% RVSP, mmhg 44.0 ± ± 14.0
82 Cumulative HF Hospitalizations (n) Primary Effectiveness Endpoint All Hospitalizations for HF within 24 months MitraClip + GDMT GDMT alone 283 in 151 pts in 92 pts HR (95% CI] = 0.53 [ ] P<0.001 No. at Risk: MitraClip GDMT Time After Randomization (Months) Median [25%, 75%] FU = 19.1 [11.9, 24.0] mos
83 All-cause Mortality (%) All-cause Mortality 100% 80% 60% 40% MitraClip + GDMT GDMT alone NNT (24 mo) = 5.9 [95% CI 3.9, 11.7] HR [95% CI] = 0.62 [ ] P< % 29.1% 20% No. at Risk: 0% MitraClip + GDMT GDMT alone Time After Randomization (Months)
84 All-cause Mortality or HF Hospitalization (%) Death or HF Hospitalization 100% 80% 60% MitraClip + GDMT GDMT alone HR [95% CI] = 0.57 [ ] P< % 40% 45.7% 20% NNT (24 mo) = 4.5 [95% CI 3.3, 7.2] No. at Risk: MitraClip + GDMT GDMT alone 0% Time After Randomization (Months)
85 24-Month Death or HF Hospitalization Subgroup MitraClip + GDMT GDMT alone HR [95% CI] HR [95% CI] P [Int] All patients Age (median) 74 years (n=317) <74 years (n=297) Sex Female (n=221) Male (n=393) Etiology of cardiomyopathy Ischemic (n=373) Non-ischemic (n=241) Prior CRT Yes (n=224) No (n=390) HF hospitalization within the prior year Yes (n=407) No (n=207) Baseline NYHA class I or II (n=240) III (n=322) IV (n=51) STS replacement score 8% (n=262) <8% (n=352) Surgical risk status* High (n=423) Not high (n=188) Baseline MR grade 3+ (n=320) 4+ (n=293) Baseline LVEF 30% (median; n=301) <30% (median; n=274) >40% (n=103) 40% (n=472) Baseline LVEDV (median) 181 ml (n=288) <181 ml (n=287) 45.7% (129) 52.1% (78) 37.8% (51) 43.2% (39) 47.1% (90) 48.1% (84) 41.1% (45) 50.2% (55) 42.9% (74) 44.7% (86) 47.6% (43) 41.1% (50) 46.6% (67) 68.3% (12) 54.1% (65) 39.2% (64) 49.7% (95) 35.8% (32) 37.5% (51) 53.4% (78) 44.1% (62) 46.4% (56) 49.7% (22) 44.2% (96) 48.9% (43) 41.5% (54) 67.9% (191) 70.2% (100) 65.3% (91) 59.4% (66) 73.0% (125) 70.0% (116) 65.2% (75) 68.4% (69) 67.4% (122) 67.9% (126) 67.8% (65) 66.9% (65) 65.3% (99) 84.4% (26) 71.4% (88) 65.0% (103) 71.5% (140) 58.7% (51) 65.3% (100) 71.4% (91) 61.2% (85) 77.8% (99) 56.2% (27) 71.9% (157) 68.0% (92) 69.5% (92) 0.57 [0.45, 0.71] 0.65 [0.48, 0.88] 0.47 [0.33, 0.66] 0.60 [0.40, 0.89] 0.54 [0.41, 0.71] 0.57 [0.43, 0.76] 0.54 [0.37, 0.78] 0.62 [0.44, 0.89] 0.53 [0.39, 0.71] 0.56 [0.42, 0.73] 0.59 [0.40, 0.86] 0.56 [0.39, 0.81] 0.61 [0.44, 0.83] 0.56 [0.28, 1.12] 0.64 [0.46, 0.88] 0.51 [0.37, 0.70] 0.58 [0.45, 0.75] 0.51 [0.33, 0.80] 0.48 [0.34, 0.67] 0.62 [0.45, 0.83] 0.60 [0.43, 0.84] 0.46 [0.33, 0.64] 0.67 [0.38, 1.17] 0.50 [0.39, 0.65] 0.58 [0.42, 0.80] 0.48 [0.34, 0.67] KM time-to-first event rates *Central eligibility committee assessment Favors MitraClip + GDMT Favors GDMT alone
86 LVEDV (ml) LVEDV change from BL to 12 mo (LSM SE) Change in LVEDV from Baseline to 12 Months GDMT alone MitraClip + GDMT ± Adjusted change* 17.1 ± P< ±76.0 ± ± ± n=174 n=175 n=174 n= Baseline 12 Months -10 *Ancova
87 KCCQ Summary Score KCCQ change from BL to 12 mo (LSM SE) 75 Change in KCCQ from Baseline to 12 Months GDMT alone MitraClip + GDMT 15 Adjusted change* ± ± ±32.0 ± P<0.001 ± ±1.9 n=228 n=236 n=228 n= Baseline 12 Months -6 *Ancova
88 6-Minute Walk Distance (m) 6MWD change from BL to 12 mo (LSM SE) Change in 6MWD from Baseline to 12 Months GDMT alone MitraClip + GDMT ±125.3 ±157.7 ± ± Adjusted change* ± P< n=237 n=229 n=237 n= ±9.0 0 Baseline 12 Months -70 *Ancova
89 24-month rate (%) LVAD or Heart Transplant Within 24 Months GDMT alone (n=312) MitraClip + GDMT (n=302) 7.1 HR [95%CI] = 0.34 [0.13, 0.87] P= HR [95%CI] = 0.35 [0.09, 1.32] P= HR [95%CI] = 0.37 [0.17, 0.81] P= LVAD implant Heart transplant LVAD or HT Stone GW et al. NEJM Sept 23.

90 Death or HF Hospitalization (%) Death or HF Hospitalization (%) COAPT vs. MITRA-FR: 12-Month Death or HF Hosp MITRA-FR COAPT 100% 90% MitraClip + MT MT alone 100% 90% MitraClip + GDMT GDMT alone 80% 70% 60% 50% 40% 30% OR [95% CI]= 1.16 [ ] P= % 51.3% 80% 70% 60% 50% 40% 30% HR [95% CI]= 0.63 [ ] P< % 33.9% 20% 20% 10% 10% 0% 0% No. at Risk: Months No. at Risk: Months Control Group Device Group Control Group Device Group Obadia JF et al. NEJM Aug 27. doi: /NEJMoa Stone GW et al. NEJM Sept 23.


91 Impact of EROA and LVEDV: EROA 30 mm 2 All-cause mortality or HF hospitalization through 12 months 91 LVEDVI >96 ml/m 2 (N=56; 10.2%) LVEDVI 96 ml/m 2 (N=51; 9.3%)
92 Percutaneous Mitral Annuloplasty
93 Percutaneous Annular Solutions Carillon (Cardiac Dimensions) Cardioband (Valtech) AccuCinch (Ancora Heart) Mitralign
 Coronary impingement (1) Coronary impingement and no change in FMR (5) Device fractures (2) Schofer J et al. Circulation. 2009;120:326-333.")
94 Carillon (Cardiac Dimensions) AMADEUS Moderate-severe FMR LVESD > 55, EF < 40% 48 patients, 30 successful implants Distal anchor slipped (3) No change in FMR (4) Coronary impingement (1) Coronary impingement and no change in FMR (5) Device fractures (2) Schofer J et al. Circulation. 2009;120:



95 Carillon TITAN 36 patients with implant 17 patients with recaptured/nondeployed devices Tomasz S et al. Eur J Heart Failure )

96 Cardioband (Valtech) 31 patients with mod/sev FMR 100% successful implant No periprocedural deaths Nickeniq G. JACC Cardiovasc Interv Oct 10;9(19):
 Mitral")

97 Cardioband (Valtech) 31 patients with moderate to severe FMR and depressed LVEF (34 ± 11%) Mitral regurgitation grade NYHA Class at 7-months Nickeniq G. JACC Cardiovasc Interv Oct 10;9(19):




98 Ventricular solutions? AccuCinch Sub-valvular implant

 Apical")
99 TTE 90 Day Apical 4-chamber (Baseline) Apical 4-chamber (90-day)



100 Day CT - Systolic Baseline ml 90 Day ml Change ml Change % Systolic ml -41% Diastolic ml -20% 1 0 0


101 Accucinch: Strain imaging Pre Post
102 EF% Improvement 30 Days n=9 90 Days n=8 6 Months n= Screening 30 Days Screening 90 Days Screening 6-MO EFS Series-3 Paired Data
103 LVESV (ml) 30 Days n=9 90 Days n=8 6 Months n= % % % Screening 30 Days Screening 90 Days Screening 6-MO
104 QoL Improvements 90 Days KCCQ-Overall Clinical Summary n=11 NYHA n=8 6MWT n= % 75% III % III II Screening 90-Days 25% 0% II Screening I 90 Days 50 0 Screening 90-Days NYHA 1 NYHA 2 NYHA 3 NYHA 4 EFS Series-3 Paired Data
105 MR Grade 30 Days n=9 90 Days n=8 6 Months n=4 100% 100% 100% 90% 90% 90% 80% 80% 80% 70% 70% 70% 60% 60% 60% 50% 50% 50% 40% 40% 40% 30% 30% 30% 20% 20% 20% 10% 10% 10% 0% Screening 30-Day 0% Screening 90-Day 0% Screening 6-MO
106 LV Remodeling Therapy Comparisons Enalapril Carvedilol CRT MV Repair MV Replace MitraClip AccuCinch CONSESUS et al Konstam et al. 1 year Doughty et al Packer et al 1 Year Abraham et al 6 months Acker et al. N Eng J Med year Mitra-FR 1 year AccuCinch 1 Month N=9 AccuCinch 3 Months N=8 AccuCinch 6 Months N=4 Δ EF% Δ ESV (ml) Mortality (% risk reduction) 31% 65% 10% Not Evaluated Not Evaluated No Effect TBD TBD TBD Death or HF Hosp 50% 27% 18% Not Evaluated Not Evaluated No Effect TBD TBD TBD
107 And more to come TRICUSPID VALVE THERAPIES

108 Tricuspid regurgitation Trialign


109 Tricuspid Valve

110 Tricuspid Valve Stenosis
111 Paravalvular leak closure

112 Paravalvular Leak Closure


113 Paravalvular leak closure
114 Conclusions MitraClip COAPT Reduction in Morality and HF hospitalizations?less benefit for large LVEDV and <3+ MR LV or annular modifying therapies may benefit Help us enroll patients! Accucinch Any HFrEF patient with or without MR Cardioband Any moderate-severe MR Carillon Any moderate-severe MR
115 Back-up slides

116 AccuCinch Phase I feasibility study 15 patients with moderate-severe FMR NYHA 2-4 High risk surgical candidate Outcomes Procedural/Technical success Safety at 1, 12 mo Hospitalizations, 6 min walk, QOL, NYHA class
117 Thank you Questions? Creighton W Don University of Washington cwdon@uw.edu (cell) VALV
Burden of Mitral Regurgitation (MR) in the US Why is This Important?
 in the US Why is This Important?") Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC
 TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT
 Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream
 Going Mainstream") The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
Outline 9/17/2016. Advances in Percutaneous Mitral Valve Repair and Replacement. Scope of the Problem and Guidelines
 Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
William A. Gray MD System Chief of Cardiovascular Services, Main Line Health President, Lankenau Heart Institute Wynnewood, Pennsylvania USA
 William A. Gray MD System Chief of Cardiovascular Services, Main Line Health President, Lankenau Heart Institute Wynnewood, Pennsylvania USA Mitral Valve Disease Today Mitral regurgitation is the most
William A. Gray MD System Chief of Cardiovascular Services, Main Line Health President, Lankenau Heart Institute Wynnewood, Pennsylvania USA Mitral Valve Disease Today Mitral regurgitation is the most
Update on Transcatheter Mitral Valve Repair and Replacment
 Update on Transcatheter Mitral Valve Repair and Replacment Vinod H. Thourani, MD Professor of Surgery Chair, Department of Cardiac Surgery Medstar Heart and Vascular Washington Hospital Center Georgetown
Update on Transcatheter Mitral Valve Repair and Replacment Vinod H. Thourani, MD Professor of Surgery Chair, Department of Cardiac Surgery Medstar Heart and Vascular Washington Hospital Center Georgetown
Transcatheter Mitral Valve for fmr: The Era of Too Many Options
 Transcatheter Mitral Valve for fmr: The Era of Too Many Options Isaac George, M.D. Surgical Director, Structural Heart & Valve Center Assistant Professor of Surgery Columbia University Medical Center Disclosure
Transcatheter Mitral Valve for fmr: The Era of Too Many Options Isaac George, M.D. Surgical Director, Structural Heart & Valve Center Assistant Professor of Surgery Columbia University Medical Center Disclosure
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL
 PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
Next Generation Therapies: Aortic, Mitral and Beyond
 Next Generation Therapies: Aortic, Mitral and Beyond Scott M Lilly, MD PhD Medical (Interventional) Director, Structural Heart Program Heart Summit, Lima OH August 26 th, 2017 Next Generation Therapies:
Next Generation Therapies: Aortic, Mitral and Beyond Scott M Lilly, MD PhD Medical (Interventional) Director, Structural Heart Program Heart Summit, Lima OH August 26 th, 2017 Next Generation Therapies:
Prognostic Impact of FMR
 Secondary Mitral Valve Regurgitation in Heart Failure, Age 60 Years From Medical Therapy to Surgical Repair to Transcatheter Intervention The Interventionalist s View Samin K Sharma, MD, FACC, FSCAI Director
Secondary Mitral Valve Regurgitation in Heart Failure, Age 60 Years From Medical Therapy to Surgical Repair to Transcatheter Intervention The Interventionalist s View Samin K Sharma, MD, FACC, FSCAI Director
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Mitral Valve Disease. James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN
 Mitral Valve Disease James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN Disclosures Affiliation/Financial Relationship Consulting Fees/Honoraria Speaker Bureau Company Abbott, BSC,
Mitral Valve Disease James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN Disclosures Affiliation/Financial Relationship Consulting Fees/Honoraria Speaker Bureau Company Abbott, BSC,
Percutaneous Mitral Valve Repair
 Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Alec Vahanian,FESC, FRCP (Edin.) Bichat Hospital University Paris VII, Paris, France
 Bichat Hospital University Paris VII, Paris, France") Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Disclosure Statement of Financial Interest Saibal Kar, MD, FACC
 MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
Επεμβατική Καρδιολογία πέραν της Στεφανιαίας Νόσου Το παρόν και το μέλλον. Εμμανουήλ Βαβουρανάκης Καθηγητής Καρδιολογίας ΕΚΠΑ Δ/της Γ ΠΚΚ
 Επεμβατική Καρδιολογία πέραν της Στεφανιαίας Νόσου Το παρόν και το μέλλον Εμμανουήλ Βαβουρανάκης Καθηγητής Καρδιολογίας ΕΚΠΑ Δ/της Γ ΠΚΚ CONFLICT OF INTEREST PROCTOR MEDTRONIC CORE VALVE ΔΙΑΚΑΘΕΤΗΡΙΑΚΗ
Επεμβατική Καρδιολογία πέραν της Στεφανιαίας Νόσου Το παρόν και το μέλλον Εμμανουήλ Βαβουρανάκης Καθηγητής Καρδιολογίας ΕΚΠΑ Δ/της Γ ΠΚΚ CONFLICT OF INTEREST PROCTOR MEDTRONIC CORE VALVE ΔΙΑΚΑΘΕΤΗΡΙΑΚΗ
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Percutaneous Therapy for Mitral Regurgitation: Current and Future Options: Could we do better today?
 Percutaneous Therapy for Mitral Regurgitation: Current and Future Options: Could we do better today? Peter S. Fail, MD, FACC, FACP, FSCAI Director of the Cardiac Catheterization Laboratories and Interventional
Percutaneous Therapy for Mitral Regurgitation: Current and Future Options: Could we do better today? Peter S. Fail, MD, FACC, FACP, FSCAI Director of the Cardiac Catheterization Laboratories and Interventional
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Management of Secondary MR : Insights from CTSN Ischemic MR trial; COAPT and MITRA-FR:
 Management of Secondary MR : Insights from CTSN Ischemic MR trial; COAPT and MITRA-FR: Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute,
Management of Secondary MR : Insights from CTSN Ischemic MR trial; COAPT and MITRA-FR: Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute,
Percutaneous mitral valve repair/replacement. Jan Van der Heyden MD, PhD St.Antonius Hospital Nieuwegein
 Percutaneous mitral valve repair/replacement Jan Van der Heyden MD, PhD St.Antonius Hospital Nieuwegein Mitral Valve anatomy Difference between AoV and MV Aortic Valve Mitral Valve Transcatheter Mitral
Percutaneous mitral valve repair/replacement Jan Van der Heyden MD, PhD St.Antonius Hospital Nieuwegein Mitral Valve anatomy Difference between AoV and MV Aortic Valve Mitral Valve Transcatheter Mitral
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
Aortic Stenosis: Background
 Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Mitral Innovations, Part II. Michael Mack, M.D. Baylor Scott & White Health
 Transcatheter Mitral Innovations, Part II Michael Mack, M.D. Baylor Scott & White Health Conflict of Interest Disclosure Co-PI of the COAPT Trial of MitraClip sponsored by Abbott Vascular Uncompensated
Transcatheter Mitral Innovations, Part II Michael Mack, M.D. Baylor Scott & White Health Conflict of Interest Disclosure Co-PI of the COAPT Trial of MitraClip sponsored by Abbott Vascular Uncompensated
Get Ready for Percutaneous Mitral Valve Approaches
 Get Ready for Percutaneous Mitral Valve Approaches Paul A. Grayburn, MD Baylor Scott and White Healthcare System The Heart Hospital Baylor Plano and Baylor Heart and Vascular Hospital Dallas, TX HOPE Unmet
Get Ready for Percutaneous Mitral Valve Approaches Paul A. Grayburn, MD Baylor Scott and White Healthcare System The Heart Hospital Baylor Plano and Baylor Heart and Vascular Hospital Dallas, TX HOPE Unmet
Mitral Regurgitation
 Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F.
 Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Transcatheter Valve Replacement: Current State in 2017
 Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
SURGICAL AND TRANSCATHETER MITRAL VALVE REPLACEMENT VS. REPAIR: COMPETITION OR SYNERGY
 SURGICAL AND TRANSCATHETER MITRAL VALVE REPLACEMENT VS. REPAIR: COMPETITION OR SYNERGY Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research
SURGICAL AND TRANSCATHETER MITRAL VALVE REPLACEMENT VS. REPAIR: COMPETITION OR SYNERGY Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain
 Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain Device Landscape 2010 PERCUTANEOUS TECHNIQUES Percutaneous indirect annuloplasty Percutaneous direct annuloplasty Edge to Edge ( E-Valve ) Non
Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain Device Landscape 2010 PERCUTANEOUS TECHNIQUES Percutaneous indirect annuloplasty Percutaneous direct annuloplasty Edge to Edge ( E-Valve ) Non
Percutaneous Mitral Valve Repair
 Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation
 Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation Hatim Al Lawati MD, FRCPC, FACC Consultant Interventional Cardiology Sultan Qaboos University
Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation Hatim Al Lawati MD, FRCPC, FACC Consultant Interventional Cardiology Sultan Qaboos University
Transcatheter Mitral Valve Interventions: Clinical Indications. Didier TCHETCHE, MD. Clinique Pasteur, Toulouse, France.
 Transcatheter Mitral Valve Interventions: Clinical Indications Didier TCHETCHE, MD. Clinique Pasteur, Toulouse, France. Conflicts of interest: -Consultant for Medtronic -Consultant for Cephea Anatomy of
Transcatheter Mitral Valve Interventions: Clinical Indications Didier TCHETCHE, MD. Clinique Pasteur, Toulouse, France. Conflicts of interest: -Consultant for Medtronic -Consultant for Cephea Anatomy of
Update on a Tethered Transapical Device for TMVR Vinay Badhwar, MD
 Update on a Tethered Transapical Device for TMVR Vinay Badhwar, MD Gordon F. Murray Professor and Chairman Department of Cardiovascular & Thoracic Surgery WVU Heart and Vascular Institute West Virginia
Update on a Tethered Transapical Device for TMVR Vinay Badhwar, MD Gordon F. Murray Professor and Chairman Department of Cardiovascular & Thoracic Surgery WVU Heart and Vascular Institute West Virginia
Current status: Percutaneous mitral valve therapy
 Current status: Percutaneous mitral valve therapy Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital ESC Stockholm 2010 Disclosures Research Grants Abbott, Edwards Consultant Abbott, Edwards 2 Percutaneous
Current status: Percutaneous mitral valve therapy Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital ESC Stockholm 2010 Disclosures Research Grants Abbott, Edwards Consultant Abbott, Edwards 2 Percutaneous
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Update on Percutaneous Therapies for Structural Heart Disease. William Thomas MD Director of Structural Heart Program Tucson Medical Center
 Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
TAVI and TAVR: Radical and Revolutionary: The Newest Insights for the CV Community and a Panel Discussion
 TAVI and TAVR: Radical and Revolutionary: The Newest Insights for the CV Community and a Panel Discussion Moderator: Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular
TAVI and TAVR: Radical and Revolutionary: The Newest Insights for the CV Community and a Panel Discussion Moderator: Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular
CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ;
 CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ; Επιµορφωτικά Σεµινάρια Ειδικευοµένων Καρδιολογίας 7 Απριλίου 2012 M Chrissoheris MD FACC THV Department HYGEIA Hospital Degenerative MR (DMR) Usually refers to an anatomic
CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ; Επιµορφωτικά Σεµινάρια Ειδικευοµένων Καρδιολογίας 7 Απριλίου 2012 M Chrissoheris MD FACC THV Department HYGEIA Hospital Degenerative MR (DMR) Usually refers to an anatomic
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Transcatheter Mitral Valve Replacement How Close Are We?
 Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Clinical Pearls: Takeaway Points for Aortic Stenosis and Mitral Regurgitation Management in 2014
 Clinical Pearls: Takeaway Points for Aortic Stenosis and Mitral Regurgitation Management in 2014 Hemal Gada, MD, MBA Assistant Professor of Medicine Rutgers Robert Wood Johnson Medical School A Hot 20
Clinical Pearls: Takeaway Points for Aortic Stenosis and Mitral Regurgitation Management in 2014 Hemal Gada, MD, MBA Assistant Professor of Medicine Rutgers Robert Wood Johnson Medical School A Hot 20
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management
 Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Percutaneous mitral valve repair: current techniques and results
 Percutaneous mitral valve repair: current techniques and results Ted Feldman, M.D., FSCAI, FACC Angioplasty Summit April 25-27 th th 2007 Seoul, Korea Ted Feldman MD, FACC, FSCAI Disclosure Information
Percutaneous mitral valve repair: current techniques and results Ted Feldman, M.D., FSCAI, FACC Angioplasty Summit April 25-27 th th 2007 Seoul, Korea Ted Feldman MD, FACC, FSCAI Disclosure Information
Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical. The Houston Aortic Symposium February 23-25, 2017
 James S. Gammie, MD Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical The Houston Aortic Symposium February 2-25, 2017 Disclosure Statement of Financial Interest Within
James S. Gammie, MD Professor and Chief, Division of Cardiac Surgery Chief Medical Officer, Harpoon Medical The Houston Aortic Symposium February 2-25, 2017 Disclosure Statement of Financial Interest Within
GDMT for percutaneous mitral valve repair
 GDMT for percutaneous mitral valve repair Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital The 11th Annual Innovations & Trends in Cardiovascular Care New Brunswick, NJ October 18 th 2014 Ted Feldman
GDMT for percutaneous mitral valve repair Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital The 11th Annual Innovations & Trends in Cardiovascular Care New Brunswick, NJ October 18 th 2014 Ted Feldman
Emerging Mitral Technologies Where Are We Now? MICHAEL MACK, MD BAYLOR SCOTT & WHITE HEALTH DALLAS, TX
 Emerging Mitral Technologies Where Are We Now? MICHAEL MACK, MD BAYLOR SCOTT & WHITE HEALTH DALLAS, TX Conflict of Interest Disclosure Abbott Vascular- Co PI COAPT Trial Medtronic- Executive Committee
Emerging Mitral Technologies Where Are We Now? MICHAEL MACK, MD BAYLOR SCOTT & WHITE HEALTH DALLAS, TX Conflict of Interest Disclosure Abbott Vascular- Co PI COAPT Trial Medtronic- Executive Committee
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
DISCLOSURE. Mitral ViV: why? Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? UW Medicine NONE.
 Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Valvular Heart Disease Transcatheter Valve Therapies. October 2016 Brian Whisenant MD
 Valvular Heart Disease Transcatheter Valve Therapies October 2016 Brian Whisenant MD Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Valvular Heart Disease Transcatheter Valve Therapies October 2016 Brian Whisenant MD Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Percutaneous Treatment of Mitral Insufficiency: Present and Future
 Percutaneous Treatment of Mitral Insufficiency: Present and Future Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine Seattle, WA
Percutaneous Treatment of Mitral Insufficiency: Present and Future Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine Seattle, WA
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Transcatheter Mitral Valve Implantation: Techniques and Early Clinical Outcomes. Dr. T. Modine MD, PhD, MBA Heart team CHRU de Lille
 Transcatheter Mitral Valve Implantation: Techniques and Early Clinical Outcomes Dr. T. Modine MD, PhD, MBA Heart team CHRU de Lille Speaker's name: Thomas Modine I have the following potential conflicts
Transcatheter Mitral Valve Implantation: Techniques and Early Clinical Outcomes Dr. T. Modine MD, PhD, MBA Heart team CHRU de Lille Speaker's name: Thomas Modine I have the following potential conflicts
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
What the Cardiologist needs to know from Medical Images
 What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
Transcatheter Mitral & Tricuspid Therapies. Bernard J. Zovighian Corporate Vice President
 Transcatheter Mitral & Tricuspid Therapies Bernard J. Zovighian Corporate Vice President We Will Lead and Transform Treatment for Patients with Mitral and Tricuspid Diseases Mitral and Tricuspid Diseases
Transcatheter Mitral & Tricuspid Therapies Bernard J. Zovighian Corporate Vice President We Will Lead and Transform Treatment for Patients with Mitral and Tricuspid Diseases Mitral and Tricuspid Diseases
Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ
 Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ Carpentier MV Classification- Leaflet Mobility Normal Increased Decreased Mobility
Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ Carpentier MV Classification- Leaflet Mobility Normal Increased Decreased Mobility
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification. Rheumatic Mitral Stenosis 76yo male
 MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial
 Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial Suzanne V. Arnold, MD, MHA Saint Luke s Mid America
Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial Suzanne V. Arnold, MD, MHA Saint Luke s Mid America
MITRAL (Mitral Implantation of TRAnscatheter valves)
") MITRAL (Mitral Implantation of TRAnscatheter valves) 30-Day Outcomes of Transcatheter MV Replacement in Patients With Severe Mitral Valve Disease Secondary to Mitral Annular Calcification or Failed Annuloplasty
MITRAL (Mitral Implantation of TRAnscatheter valves) 30-Day Outcomes of Transcatheter MV Replacement in Patients With Severe Mitral Valve Disease Secondary to Mitral Annular Calcification or Failed Annuloplasty
Development of a TMVR Device Challenge to Innovators
 Development of a TMVR Device Challenge to Innovators Eberhard Grube MD, FACC, FSCAI, FAPSIC University Bonn, Heart Center, Bonn, Germany Stanford Universuty, School of Medicine, Palo Alto, CA Disclosure
Development of a TMVR Device Challenge to Innovators Eberhard Grube MD, FACC, FSCAI, FAPSIC University Bonn, Heart Center, Bonn, Germany Stanford Universuty, School of Medicine, Palo Alto, CA Disclosure
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Steven F Bolling Professor of Cardiac Surgery University of Michigan
 Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients?
 Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients? David H. Adams, MD Cardiac Surgeon-in-Chief Mount Sinai Health System Marie Josée and Henry R. Kravis Professor and
Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients? David H. Adams, MD Cardiac Surgeon-in-Chief Mount Sinai Health System Marie Josée and Henry R. Kravis Professor and
RANDOMISED TRIALS TAVI WITH SAVR STEPHAN WINDECKER AORTIC VALVE DISEASE COMPARING
 AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients
 Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC
 TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
The Future of Medicine. Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy
 The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S.
 ACC 2015 LBCT Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S. A report from the STS/ACC TVT Registry Paul Sorajja, MD, Saibal Kar, MD, Amanda Stebbins,
ACC 2015 LBCT Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S. A report from the STS/ACC TVT Registry Paul Sorajja, MD, Saibal Kar, MD, Amanda Stebbins,
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
TAVR in 2020: What is Next!!!!
 TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
Organic mitral regurgitation
 The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
Percutaneous Valve in Native With and Without Mitral Valve Calcification: When To Go Hybrid
 Percutaneous Valve in Native With and Without Mitral Valve Calcification: When To Go Hybrid Deborah Tabachnick, MD Cardiac Surgeon The Heart Hospital Baylor Plano Baylor Scott & White Health Disclosures
Percutaneous Valve in Native With and Without Mitral Valve Calcification: When To Go Hybrid Deborah Tabachnick, MD Cardiac Surgeon The Heart Hospital Baylor Plano Baylor Scott & White Health Disclosures
Latest therapies for patients with HF. Dr AIGUL BALTABAEVA PhD, FESC, FRCP RBHT & ASPH
 Latest therapies for patients with HF Dr AIGUL BALTABAEVA PhD, FESC, FRCP RBHT & ASPH ESC HF Guidelines 2016 ESC HF Guidelines 2016: Pharmacological Treatments Pathways blocked by ACE-I, ARB and NI Effect
Latest therapies for patients with HF Dr AIGUL BALTABAEVA PhD, FESC, FRCP RBHT & ASPH ESC HF Guidelines 2016 ESC HF Guidelines 2016: Pharmacological Treatments Pathways blocked by ACE-I, ARB and NI Effect
Advanced Mitral Valve Therapies
 Advanced Mitral Valve Therapies Mahesh Ramchandani MD, FRCS Chief, Section of Cardiac Surgery A Largely Untreated Patient Population Mitral Regurgitation 2009 U.S. Prevalence Total MR Patients 1,2 4,100,000
Advanced Mitral Valve Therapies Mahesh Ramchandani MD, FRCS Chief, Section of Cardiac Surgery A Largely Untreated Patient Population Mitral Regurgitation 2009 U.S. Prevalence Total MR Patients 1,2 4,100,000
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Edwards' solution for patients suffering from tricuspid valve disease
 Edwards' solution for patients suffering from tricuspid valve disease R. S. von Bardeleben, MD Head Structural and Heart Valve Center Heart Center Cardiology I, University Medicine Mainz Germany Potential
Edwards' solution for patients suffering from tricuspid valve disease R. S. von Bardeleben, MD Head Structural and Heart Valve Center Heart Center Cardiology I, University Medicine Mainz Germany Potential
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute
 Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Percutaneous Mitral Valve Therapies
 Percutaneous Mitral Valve Therapies Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical School
Percutaneous Mitral Valve Therapies Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical School
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,