Biopsy Evaluation of Non- Neoplastic Diseases of the Large Bowel: an algorithmic approach
|
|
|
- Suzanna Boone
- 5 years ago
- Views:
Transcription
1 Biopsy Evaluation of Non- Neoplastic Diseases of the Large Bowel: an algorithmic approach Laura W. Lamps, M.D. Godfrey D. Stobbe Professor and Director of GI Pathology University of Michigan Health System Ann Arbor, MI Medical (lung, GI, liver, kidney, skin) pathology has different challenges from tumor pathology. Nonspecific by definition Infinite variety of insults cause finite variety of tissue reactions Cirrhosis Interstitial fibrosis Lichenoid dermatitis Villous blunting Biopsy Diagnosis of Colitis Clinically Relevant Diagnosis vs. Description 68% of biopsy specimens obtained for non-neoplastic colonic disease showed an abnormal inflammatory process 75% of these could be classified into specific types of colitis based on morphology + available clinical data BUT, 59% were originally given only descriptive diagnoses; reclassified upon review From Tsang and Rotterdam: AJSP 23:423-30,
2 Biopsy Diagnosis of Colitis Clinically Relevant Diagnosis vs. Description Description Acute inflammation Chronic nonspecific inflammation Unspecified colitis, acute/subacute, etiology undetermined Clinically Relevant Diagnosis Active colitis, suggestive of acute infectious-type colitis Chronic, active colitis, consistent with Histologic changes consistent with ischemia Components of a useful medical colitis report Diagnosis or at least useful description Normal vs. inflamed Chronic or not Description They like to know what we see Avoid clinical correlation required Comment/implications Even if there is no specific diagnosis, it s helpful to give them a category of disease, a differential, and something to do General Evaluation of Intestinal Mucosal Biopsies: The Question Oriented Approach (made easier by the advent of widely accessible EMRs) Why was the biopsy done? What are the nature and duration of the patient s symptoms? From EXACTLY where was the biopsy taken? What were the endoscopic findings? 2
3 Fear not the normal biopsy! One of the most common complaints that endoscopists have is that pathologists label all cases mild chronic inflammation. The intestinal tract is constantly bombarded with antigenic stimulation, and thus always contains mild chronic inflammation. The real question is, is enough inflammation seen to explain the patient s symptoms? Riddell, Lewin, and Weinstein, Pathologist-Gastroenterologist Interaction: the changing role of the pathologist. Am J Clin Path 103: S9-S12, General Classification of Inflammatory Disorders of the Colon Chronic Idiopathic IBD Ulcerative colitis Crohn s Infectious Motor Disorders Diverticulitis Prolapse/SRUS Ischemia Iatrogenic Drug associated Radiation Diversion colitis GVHD Neutropenic colitis Other Collagenous colitis Lymphocytic colitis Eosinophilic colitis Diverticular-disease associated colitis Colitis ASLC AITC FAC CHRONICITY Architectural distortion Basal plasmacytosis Left sided Paneth cells Pyloric metaplasia Variant chronic colitides CIIBD Infection NSAID Infection NSAID Rarely Crohn s Tic-associated segmental colitis Diversion colitis Lymphocytic colitis Collagenous colitis Crohn s UC 3


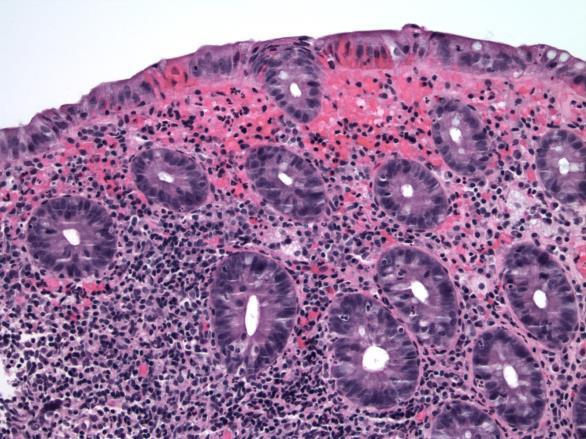
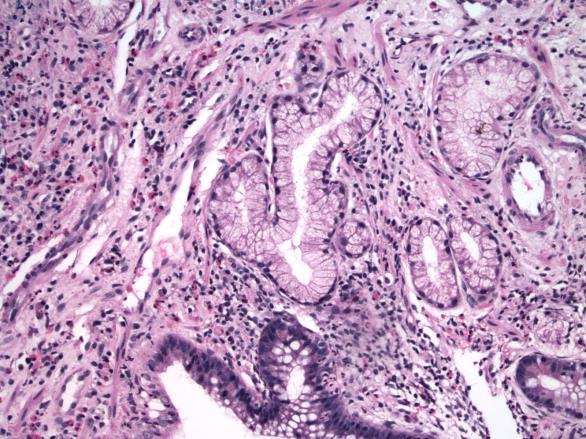
4 The Atypical or Variant Colitides Heterogeneous group of colitides NOT UC or Crohn s Often lack constitutional symptoms Often lack definite laboratory abnormalities Often included are: Collagenous colitis Lymphocytic colitis Diversion colitis Diverticular disease-related segmental colitis 30 year old man with sudden onset of bloody diarrhea-right colon bxs Focal Active Colitis Often has: Lamina propria neutrophils Focal cryptitis Surface injury Should not have: Architectural distortion Basal plasmacytosis Paneth cell metaplasia (left) 4

5 Implications of FAC Infection NSAID Nothing Occasionally Crohn s (less than 10% in adults; around 30% in kids) 1. Greenson et al. The clinical significance of focal active colitis. Hum Pathol 28:729-33, Xin et al. The clinical significance of focal active colitis in pediatric patients. Am J Surg Pathol 27:1134-8, Volk et al. The clinical significance of a biopsy-based diagnosis of focal active colitis: a clinicopathologic study of 31 cases. Mod Pathol 11:789-94, Remember the bowel prep artifacts! Apthous ulcers Cryptitis Superficial hemorrhage Apoptotic debris at surface 5


6 Courtesy Dr. Joel Greenson 6


7 Are there any snakes like this one in Pennsylvania? 43 year old male, 3 month history of diarrhea, crampy abdominal pain; left colon and rectosigmoid bxs Chronic idiopathic inflammatory bowel disease: UC vs. Crohn s Ulcerative colitis Clinical info Imaging Macroscopic findings Pathologic features Crohn s disease 7
 If granulomas,")

8 Classic Features of Untreated Ulcerative Colitis and Crohn s Disease Ulcerative colitis Diffuse continuous disease Rectal involvement Disease worse distally Usually limited to mucosa Ileum spared (except backwash) If granulomas, associated with ruptured crypts Crohn s disease Segmental disease +/- upper tract involvement Variable severity Transmural lymphoid aggregates, other mural changes Granulomas Pyloric metaplasia Perianal disease Ulcerative colitis 8

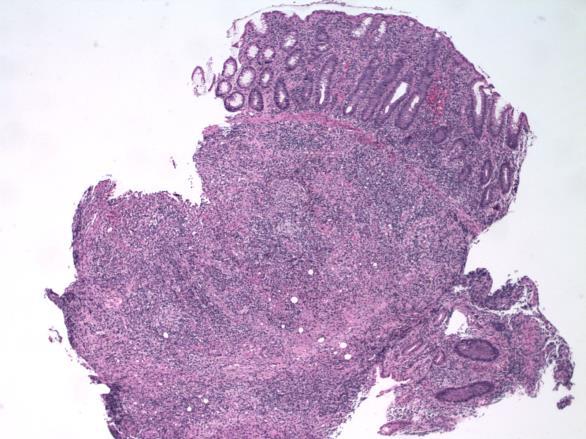
9 Crohn s disease Crohn s diseasenote submucosal infiltrate 9

10 Crohn s disease Pyloric-type metaplasia 10

11 Only if you ve been living right Important Clinical/Endoscopic Information insufficient clinical/radiographic info is most common cause of error in the Crohn s vs. UC scenario Clinical Family hx, PSC, symptoms/signs, serology, prior surgery, perianal disease Radiologic Endoscopic Pathologic Segmental vs diffuse, SB involvement, strictures, fistulas, wall thickness Type/appearance of ulcers, distribution of disease, appearance of ileum Prior biopsies (and resections), ideally pretreatment Courtesy Dr. Rob Odze Indeterminate Colitis Not a distinct entity/disease No diagnostic criteria Should be regarded an interim diagnosis CIIBD, unclassified or a comment is preferred 11


12 UC vs. Crohn s on biopsy: how far can you go? Depending on quality of other information, may get to UC or CD If not, if you can get to CIIBD, then the drugs are the same Most cases of indeterminate disease end up acting like UC, and do well treated as such Don t use indeterminate colitis as a disease entity This lecture has worn me out. When is the break? 65 year old man with diarrhea, crampy abdominal pain; sigmoid biopsies 12
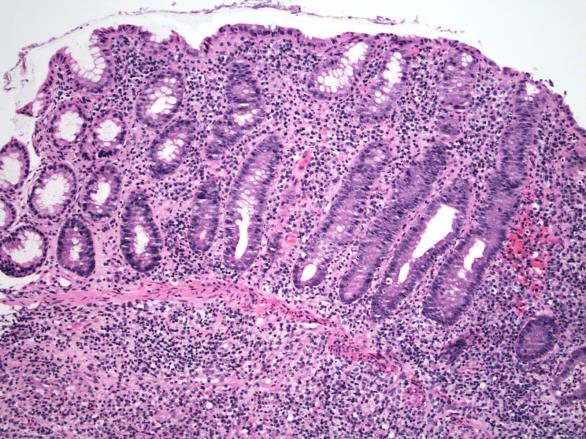
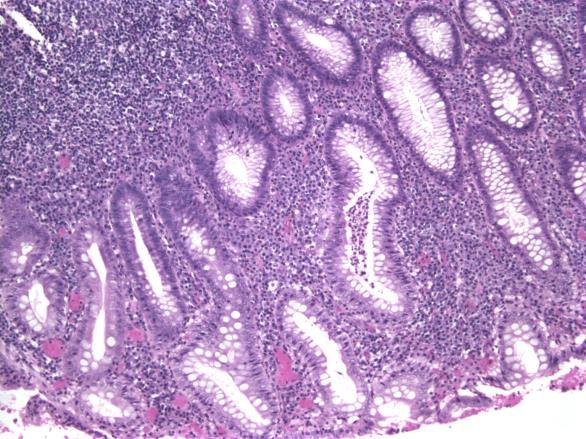
13 Colitis with features of chronicity UC Crohn s Macroscopic appearance Timing/duration of Variant chronic symptoms colitides Laboratory tests Drug history Tic-associated segmental colitis Diversion colitis Lymphocytic colitis Collagenous colitis Infectious Mimics Drug Diverticular-Disease Associated Segmental Colitis Primarily elderly patients Hematochezia, mucus, cramps Colonoscopy: Patchy or confluent hyperemia Accentuated on crests of mucosal folds Mucosal granularity Distribution Descending colon and sigmoid, in area of tics Rectum is virtually always spared! Diverticular-Disease Associated Colitis - Histology Mimics chronic idiopathic inflammatory bowel disease: Cryptitis and crypt abscesses Increased LP mixed inflammatory infiltrate Often basal plasmacytosis Crypt distortion (mimics CIIBD) Granulomas (Crohn s-like variant) Ulceration 13



14 Mucosal lymphoid aggregates are common Cryptitis in DDASC Architectural distortion, crypt abscesses, and basal lymphoid aggregates in DDASC 14
 Gross")

15 DDASC Ulcerative colitis Diverticular-Disease Associated Colitis-Differential Diagnosis Crohn s Involvement of other segments of bowel (upper and lower) Gross features Ulcerative colitis Contiguous disease with rectal involvement DDASC Patients have diverticula Colitis limited to segment of bowel with tics Rectum spared 15
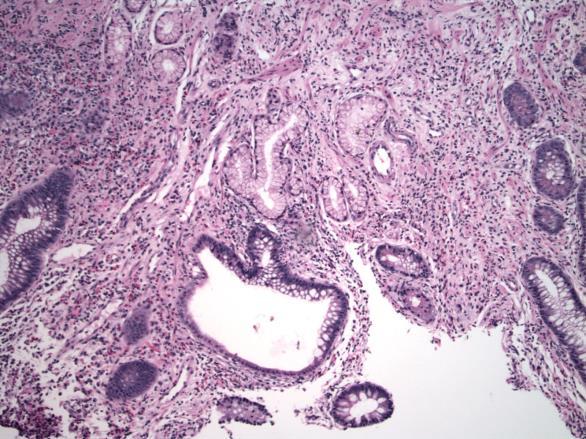
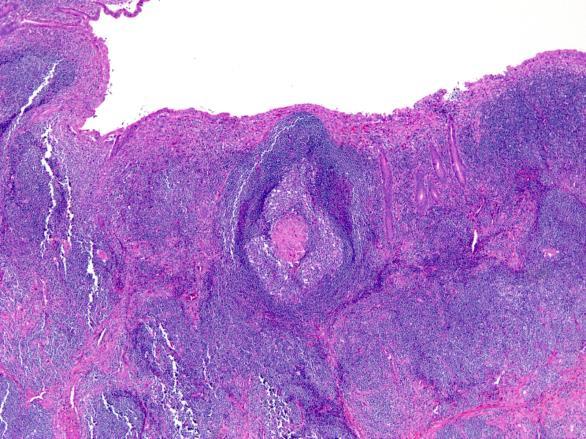
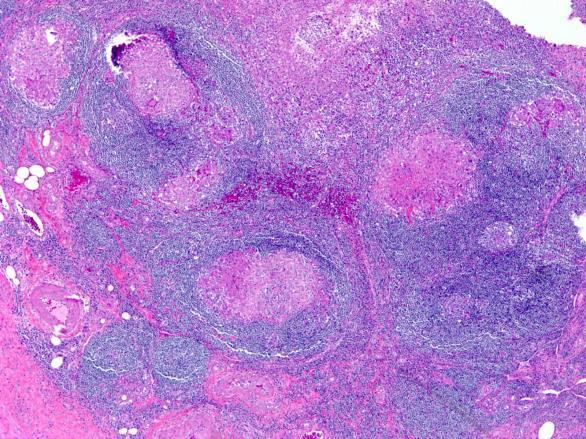
16 Diversion Colitis Found in segments of bowel diverted from the fecal stream Eventually occurs in almost all diversions Cured by surgical reversal of diversion Symptoms occur with increasing duration of diversion: Bloody/mucoid discharge Abdominal pain Tenesmus Diversion Colitis Mimics IBD Need to know that it s diverted, and need to know why they were diverted Diversion Colitis Histology Apthous ulcers Prominent lymphoid follicles Increased inflammation in lamina propria Including neutrophils; granulomas rare Cryptitis and crypt abscesses Crypt architecture usually preserved 16



17 Courtesy Dr. Nathan Lee Prominent lymphoid follicles in diversion colitis Apthous ulcer overlying prominent lymphoid follicle in diversion colitis 17


18 Cryptitis, crypt abscesses, and focal mild architectural distortion in DC 18
19 Diversion Colitis Differential Diagnosis Differential from Idiopathic IBD: History of diversion! Disease in remainder of bowel Histology Lack of significant architectural distortion Milder inflammatory changes May be very difficult if not impossible Resolution of symptoms with surgical correction, fatty acid enemas Drug and Chemical Related Colitis Antibiotics Chemotherapeutic agents Gold NSAIDS Methyldopa Flucytosine Cellsept (mycophenolate) Carbamazepine Cimetidine Retinoids Detergents, etc: Herbal remedies Hydrogen peroxide Sodium hydroxide Alcohols Formalin NSAID-Associated Colitis May occur after only weeks of use Abdominal pain, cramping, bloody stool Commonly involves ileum but can be any area of colon Mucosal erythema, friability, ulcers Strictures/diaphragms Massive bleeding, perforation Risk increases with patient age, duration of use, and use of other concomitant medications 19

20 NSAID-Associated Colitis variable histology Patchy colitis with mixed inflammation, including neutrophils Intraepithelial lymphocytes Superficial erosions Regenerative mucosal changes May be focal architectural disarray but not true distortion Ddx: Crohn s, infection, other drug reactions 20

21 Mycophenolate mofetil (Cellsept) Maintenance immunosuppression, primarily in solid organ transplants Most common side effect is GI toxicity (diarrhea) Mimics GVHD, CIIBD GI toxicity does not appear to be dosedependent More severe if drug started later in the course More toxicity with higher creatinine Mycophenolate mofetil Microscopic Features Prominent apoptosis Crypt atrophy/dropout Crypt distortion Dilated crypts with neutrophils, eosinophils Marked neutrophilic activity, diffuse mixed inflammation usually absent 21



22 Mycophenolate toxicity Significant architectural distortion may be present, mimicking CIIBD Ipilimumab colitis 22


23 Chronic radiation colitis Infectious mimics of chronic idiopathic inflammatory bowel disease Yersinia Aeromonas Shigella Salmonella CMV Amoebiasis 23

24 Yersinia species 24


25 Aeromonas: common food and waterborn pathogen Infections superimposed on CIIBD CMV C. difficile Food-borne enterics 25


26 Utility of CMV Stains in Evaluation of Biopsies from UC Flares Kambham et al, AJSP 2004 Case control study of UC patient with refractory disease 25% of patients with refractory UC had CMV inclusions on immunostain 60% of these had been missed on H&E Recommend using CMV IHC in evaluation of biopsies in these patients CMV commonly superinfects both Crohn s disease and UC patients 26


27 What about microscopic colitis? The presence of histologic abnormalities in the context of an unremarkable colonoscopic examination ( microscopic disease). Don t use microscopic colitis as diagnosis Collagenous colitis Lymphocytic colitis Both patterns associated with olmesartan 27

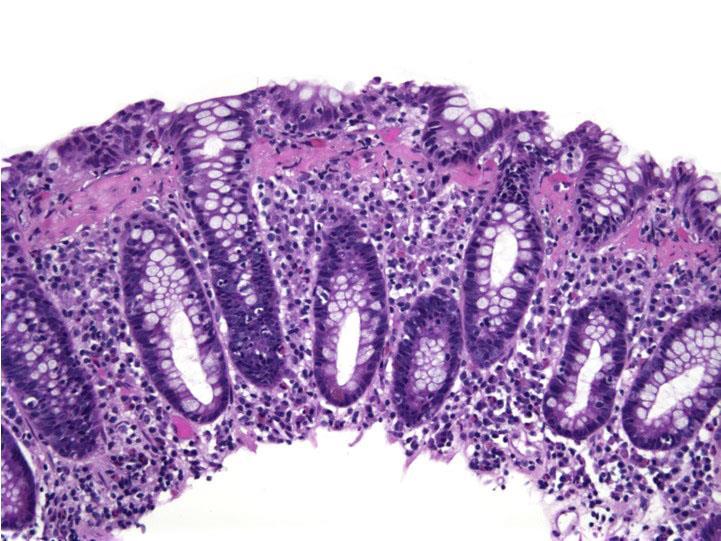
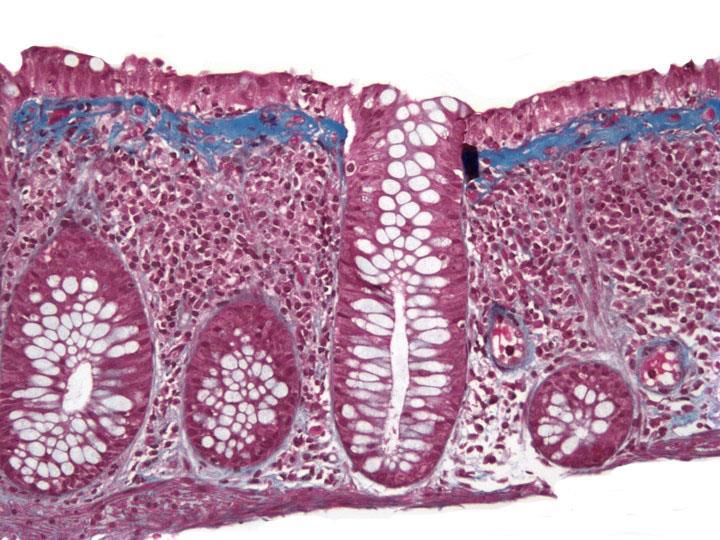
28 What about microscopic colitis? You need: History of long-term chronic watery diarrhea Appropriate histology Normal colonoscopy If any of these don t fit, back off the diagnosis!! Collagenous Colitis Chronic, watery diarrhea Often lasts for years Crampy abdominal pain Normal colonoscopy and radiographs Primarily a disease of middle aged women Male:female ratio 9-20:1 Often coexistent autoimmune disorder?association with NSAIDS Collagenous Colitis Histology Collagen Thickened subepithelial collagen band No numerical cutoff! May abate with treatment Variable, shaggy, with entrapped capillaries Colitis Intraepithelial lymphocytosis Increased mixed LP inflammatory infiltrate Neutrophils should be rare Surface epithelial damage 28


29 Yield of Biopsy Specimens Diagnostic of Collagenous Colitis 70% 83% 78% 66% From: Offner et al, Hum Pathol 30:451-7 Courtesy Dr. Joel Greenson 29

30 30


31 Collagenous Colitis Diagnostic Pitfalls Failure to consider inflammatory component Sole reliance on numerical quantitation of collagen band Misinterpretation of normal structures or other types of fibrosis Tangential orientation Hyperplastic polyps Fibrosis of ischemia, Crohn s Site within colon Lazenby et al, Hum Pathol 21: Normal-Tangential Section Courtesy Dr. Joel Greenson 31

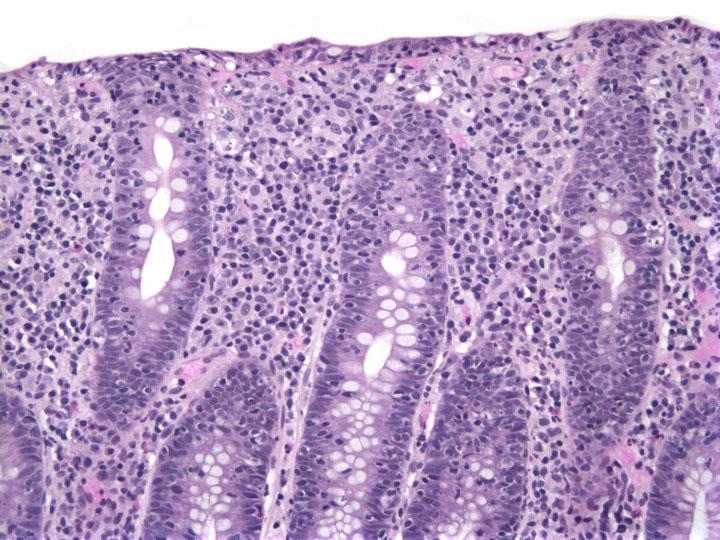
32 Ischemia Courtesy Dr. Joel Greenson Lymphocytic Colitis Symptoms are similar to collagenous colitis Unremarkable colonoscopy Equal male to female distribution Lymphocytic Colitis Histology Increased intraepithelial lymphocytosis Usually greater than 10/100 enterocytes Surface and crypts involved Surface epithelial damage Increased LP inflammatory component Plasma cells common; neutrophils should be rare No abnormal subepithelial collagen band 32


33 33


34 Other things that cause a lymphocytosis: NSAIDs Viral enterocolitis Crohn s Resolving bacterial infection Resolving Infection 34
 Resolving bacterial infection Collagenous vs.")
35 Lymphocytic Colitis Diagnostic Pitfalls Failure to integrate with clinical and endoscopic data Other entities featuring colonic epithelial lymphocytosis: Drug-related colitis (especially NSAID) Celiac disease Crohn s disease Infectious diarrhea (Brainerd diarrhea) Resolving bacterial infection Collagenous vs. Lymphocytic Colitis Similarities: Watery diarrhea Mean age at dx Normal colonoscopy Intraepithelial lymphocytosis Differences: Female to male ratio HLA antigens Increased subepithelial collagen Autoantibodies From Giardello et al, Gastroenterol Clin North Amer 24;717-29, 1995 Alys ponders the diagnostic nuances of inflammatory bowel disease. 35
36 How to stay out of trouble Find out history Know macroscopic findings (e.g., if colitis limited to segment with diverticula or bx from diverted segment) Be aware of drugs and infections that mimic CIIBD Components of a useful medical intestinal biopsy report Diagnosis Normal vs. inflamed Chronic or not How active is it Description They like to know what we see Comment/implications Even if there is no specific diagnosis, we need to give them a category and something to do Report Colon, right, bx: Focal active colitis; sc Comment: Description There are no features of chronicity These features are most commonly seen with self-limited processes such as infection, adverse drug reaction; can recommend drug history, infectious workup 36
37 Report Colon, left, bx: Chronic, active colitis Comment: Description, emphasizing chronicity Features compatible with type of CIIBD, depending on clinical/colonoscopic information Dysplasia designation Report Colon, left, bx: Chronic, active colitis; see comment Give description Note that per endoscopist colitis is present only in region of tics Consistent with DDASC Colitis-unacceptable reporting cryptitis with no comment Chronic inflammation Acute inflammation moderate colitis colitis with a few erosions Not giving a category of disease, and/or recommendations 37

38 Let s go grill! 38
하부위장관비종양성질환의 감별진단 주미인제의대일산백병원
 하부위장관비종양성질환의 감별진단 주미인제의대일산백병원 Solutions for diagnostic problems in Colitis : Please ask yourself five questions Normal or Inflamed? Acute or Chronic? IBD or Other chronic colitis? Ulcerative colitis or
하부위장관비종양성질환의 감별진단 주미인제의대일산백병원 Solutions for diagnostic problems in Colitis : Please ask yourself five questions Normal or Inflamed? Acute or Chronic? IBD or Other chronic colitis? Ulcerative colitis or
11/1/2017. Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota. Cerilli & Greenson
 Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota Acute infectious (self-limited) colitis Focal active colitis Pseudomembranous colitis Ischemic colitis Collagenous
Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota Acute infectious (self-limited) colitis Focal active colitis Pseudomembranous colitis Ischemic colitis Collagenous
Pitfalls in the Diagnosis of Inflammatory Bowel Disease
 Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease
 BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease David A Owen University of British Columbia CAUSES OF DIARRHEA DIARRHEA COLITIS PRESENT COLITIS ABSENT INFECTIOUS NON-INFECTIOUS
BIOPSY DIAGNOSIS OF COLITIS Common and Unusual Forms of Inflammatory Bowel disease David A Owen University of British Columbia CAUSES OF DIARRHEA DIARRHEA COLITIS PRESENT COLITIS ABSENT INFECTIOUS NON-INFECTIOUS
A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue
 A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue UCSF Liver and Gastrointestinal Pathology Update Sept. 4, 2009 How to Go Wrong When Evaluating Small Bowel Biopsies, Based on
A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue UCSF Liver and Gastrointestinal Pathology Update Sept. 4, 2009 How to Go Wrong When Evaluating Small Bowel Biopsies, Based on
IBD. Crohn s. Outline. Ulcerative colitis versus Crohn s disease: is biopsy useful? UC vs. Crohn s? Is it easy? Biopsy settings 21/07/2017 IBD
 Outline Ulcerative colitis versus Crohn s disease: is biopsy useful? Roger Feakins Colorectal biopsies Ileal and upper GI biopsies Special situations New techniques Summary Inflammatory bowel disease (IBD)
Outline Ulcerative colitis versus Crohn s disease: is biopsy useful? Roger Feakins Colorectal biopsies Ileal and upper GI biopsies Special situations New techniques Summary Inflammatory bowel disease (IBD)
Oncologist-induced Disease of the GI tract: New Developments
 Oncologist-induced Disease of the GI tract: New Developments Jeffrey D Goldsmith, MD Children s Hospital Boston, Beth Israel Deaconess Medical Center, Harvard Medical School Boston, MA Everyone s on drugs
Oncologist-induced Disease of the GI tract: New Developments Jeffrey D Goldsmith, MD Children s Hospital Boston, Beth Israel Deaconess Medical Center, Harvard Medical School Boston, MA Everyone s on drugs
Case History B Female patient 1970 Clinical History : crampy abdominal pain and episodes of bloody diarrhea Surgical treatment
 Case History B-1325945 Female patient 1970 Clinical History : crampy abdominal pain and episodes of bloody diarrhea Surgical treatment Case History B-1325945 Pathology Submucosa & Muscularis Endometriosis
Case History B-1325945 Female patient 1970 Clinical History : crampy abdominal pain and episodes of bloody diarrhea Surgical treatment Case History B-1325945 Pathology Submucosa & Muscularis Endometriosis
What is your diagnosis? a. Lymphocytic colitis. b. Collagenous colitis. c. Common variable immunodeficiency (CVID) associated colitis
 associated colitis") Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
GUIDELINES FOR THE INITIAL BIOPSY DIAGNOSIS OF CHRONIC IDIOPATHIC INFLAMMATORY BOWEL DISEASE A STRUCTURED APPROACH TO COLORECTAL BIOPSY ASSESSMENT
 Guidelines for the Initial Biopsy Diagnosis of Chronic Idiopathic Inflammatory Bowel Disease 1 GUIDELINES FOR THE INITIAL BIOPSY DIAGNOSIS OF CHRONIC IDIOPATHIC INFLAMMATORY BOWEL DISEASE A STRUCTURED
Guidelines for the Initial Biopsy Diagnosis of Chronic Idiopathic Inflammatory Bowel Disease 1 GUIDELINES FOR THE INITIAL BIOPSY DIAGNOSIS OF CHRONIC IDIOPATHIC INFLAMMATORY BOWEL DISEASE A STRUCTURED
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
Kids Like to Break the Rules: Gastrointestinal Pathology in Children
 Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
What do we need for diagnosis of IBD
 What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Chronic Colitis Pattern Christina A. Arnold, M.D. The Ohio State University Wexner Medical Center Columbus, Ohio
 Chronic Colitis Pattern Christina A. Arnold, M.D. The Ohio State University Wexner Medical Center Columbus, Ohio Identify this medication resin: A. Bile Acid Sequestrant B. Kayexalate C. Sevelamer D. Renvela
Chronic Colitis Pattern Christina A. Arnold, M.D. The Ohio State University Wexner Medical Center Columbus, Ohio Identify this medication resin: A. Bile Acid Sequestrant B. Kayexalate C. Sevelamer D. Renvela
Original Article. Atypical histological features of ulcerative colitis. Siddharth N Shah, 1 Anjali D Amarapurkar, 1 N Shrinivas, 2 Rathi PM 2 ABSTRACT
 Tropical Gastroenterology 2011;32(2):107 111 Original Article Atypical histological features of ulcerative colitis Siddharth N Shah, 1 Anjali D Amarapurkar, 1 N Shrinivas, 2 Rathi PM 2 ABSTRACT Department
Tropical Gastroenterology 2011;32(2):107 111 Original Article Atypical histological features of ulcerative colitis Siddharth N Shah, 1 Anjali D Amarapurkar, 1 N Shrinivas, 2 Rathi PM 2 ABSTRACT Department
Interpretation of inflammatory colorectal biopsies has
 The of Colitis in Endoscopic Biopsy Specimens A Review Article Lisa A. Cerilli, MD; Joel K. Greenson, MD Context. A variety of inflammatory disorders may affect the colon, with widely differing clinical
The of Colitis in Endoscopic Biopsy Specimens A Review Article Lisa A. Cerilli, MD; Joel K. Greenson, MD Context. A variety of inflammatory disorders may affect the colon, with widely differing clinical
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Frequency and Distribution of Microscopic Findings in Patients with Chronic Non-Bloody Diarrhea and Normal Colonoscopy
 IJMS Vol 33, No 2, June 2008 Original Article Frequency and Distribution of Microscopic Findings in Patients with Chronic Non-Bloody Diarrhea and Normal Colonoscopy H. Tabrizchie, M.J. Zahedie 1, M. Hayatbakhsh
IJMS Vol 33, No 2, June 2008 Original Article Frequency and Distribution of Microscopic Findings in Patients with Chronic Non-Bloody Diarrhea and Normal Colonoscopy H. Tabrizchie, M.J. Zahedie 1, M. Hayatbakhsh
The Spectrum of IBD. Inflammatory Bowel Disease. Symptoms. Epidemiology. Tests for IBD. CD or UC? Inflamatory Bowel Disease. Fernando Vega, M.D.
 The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
12/7/2011. Patterns of mucosal damage=dx. Non IBD-Colitis: How to communicate with the clinicians. Chronic colitis
 Non IBD-Colitis: How to communicate with the clinicians Gregory Y. Lauwers, M.D. Vice Chairman Department of Pathology Director, Gastrointesinal Pathology Service Massachusetts General Hospital Professor
Non IBD-Colitis: How to communicate with the clinicians Gregory Y. Lauwers, M.D. Vice Chairman Department of Pathology Director, Gastrointesinal Pathology Service Massachusetts General Hospital Professor
The Morphologic Profile of Inflammatory Bowel Disease and the Diagnostic Problem of Crohn s Disease versus TB Colitis A Case Series
 OPEN ACCESS CASE REPORT The Morphologic Profile of Inflammatory Bowel Disease and the Diagnostic Problem of Crohn s Disease versus TB Colitis A Case Series Maria Lourdes Tilbe, Francia Victoria De Los
OPEN ACCESS CASE REPORT The Morphologic Profile of Inflammatory Bowel Disease and the Diagnostic Problem of Crohn s Disease versus TB Colitis A Case Series Maria Lourdes Tilbe, Francia Victoria De Los
Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects
 Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects Patient Group Macroscopic examination Ileum Histology Colon/rectum Histology 1 INR Normal Acute and chronic
Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects Patient Group Macroscopic examination Ileum Histology Colon/rectum Histology 1 INR Normal Acute and chronic
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
INTERNATIONAL COURSE ON THE PATHOLOGY OF THE DIGESTIVE SYSTEM VICTOR BABES NATIONAL INSTITUTE OF PATHOLOGY BUCHAREST 7-8 BUCHAREST 2014
 INTERNATIONAL COURSE ON THE PATHOLOGY OF THE DIGESTIVE SYSTEM VICTOR BABES NATIONAL INSTITUTE OF PATHOLOGY BUCHAREST 7-8 BUCHAREST 2014 Endoscopic biopsy samples of naïve colitides patients: Role of basal
INTERNATIONAL COURSE ON THE PATHOLOGY OF THE DIGESTIVE SYSTEM VICTOR BABES NATIONAL INSTITUTE OF PATHOLOGY BUCHAREST 7-8 BUCHAREST 2014 Endoscopic biopsy samples of naïve colitides patients: Role of basal
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS
 MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
Diagnostic difficulties in inflammatory bowel disease pathology
 Histopathology 2006, 48, 116 132. DOI: 10.1111/j.1365-2559.2005.02248.x REVIEW Diagnostic difficulties in inflammatory bowel disease pathology R K Yantiss & R D Odze 1 Departments of Pathology, Weill Medical
Histopathology 2006, 48, 116 132. DOI: 10.1111/j.1365-2559.2005.02248.x REVIEW Diagnostic difficulties in inflammatory bowel disease pathology R K Yantiss & R D Odze 1 Departments of Pathology, Weill Medical
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX
 Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Treating Crohn s and Colitis in the ASC
 Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
Keep microscopic colitis in mind!
 Keep microscopic in mind! Information for gastroenterologists and pathologists D. Aust (Dresden), S. Miehlke (Hamburg) An initiative of the EUROPEAN MICROSCOPIC COLITIS GROUP Microscopic is a chronic inflammatory
Keep microscopic in mind! Information for gastroenterologists and pathologists D. Aust (Dresden), S. Miehlke (Hamburg) An initiative of the EUROPEAN MICROSCOPIC COLITIS GROUP Microscopic is a chronic inflammatory
Patterns of Colonic Involvement at Initial Presentation in Ulcerative Colitis A Retrospective Study of 46 Newly Diagnosed Cases
 Anatomic Pathology / PATTERNS OF INVOLVEMENT IN ULCERATIVE COLITIS Patterns of Colonic Involvement at Initial Presentation in Ulcerative Colitis A Retrospective Study of 46 Newly Diagnosed Cases Marie
Anatomic Pathology / PATTERNS OF INVOLVEMENT IN ULCERATIVE COLITIS Patterns of Colonic Involvement at Initial Presentation in Ulcerative Colitis A Retrospective Study of 46 Newly Diagnosed Cases Marie
ANATOMIC PATHOLOGY Original Article
 ANATOMIC PATHOLOGY Original Article Histology of the Mucosa in Sigmoid Colon Specimens With Diverticular Disease Observations for the Interpretation of Sigmoid Colonoscopic Biopsy Specimens NEAL S. GOLDSTEIN,
ANATOMIC PATHOLOGY Original Article Histology of the Mucosa in Sigmoid Colon Specimens With Diverticular Disease Observations for the Interpretation of Sigmoid Colonoscopic Biopsy Specimens NEAL S. GOLDSTEIN,
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Non-Neoplastic Disorders. of the Intestines. Laura W. Lamps, M.D. University of Arkansas Little Rock, AR
 Non-Neoplastic Disorders Laura W. Lamps, M.D. University of Arkansas Little Rock, AR Audrey J. Lazenby, M.D. University of Alabama Birmingham, AL Joel K. Greenson, M.D. University of Michigan Ann Arbor,
Non-Neoplastic Disorders Laura W. Lamps, M.D. University of Arkansas Little Rock, AR Audrey J. Lazenby, M.D. University of Alabama Birmingham, AL Joel K. Greenson, M.D. University of Michigan Ann Arbor,
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
For the past 40 years, it has been standard practice to obtain
 ORIGINAL ARTICLE: GASTROENTEROLOGY Good Agreement Between Endoscopic Findings and Biopsy Reports Supports Limited Tissue Sampling During Pediatric Colonoscopy Michael A. Manfredi, Hongyu Jiang, Lawrence
ORIGINAL ARTICLE: GASTROENTEROLOGY Good Agreement Between Endoscopic Findings and Biopsy Reports Supports Limited Tissue Sampling During Pediatric Colonoscopy Michael A. Manfredi, Hongyu Jiang, Lawrence
Endoscopy in IBD. F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M.
 Frankfurt/M.") F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases?
 How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
Gastritis (and gastropathy) Dr Ian Brown Envoi Pathology Brisbane, Australia
 Dr Ian Brown Envoi Pathology Brisbane, Australia") Gastritis (and gastropathy) Dr Ian Brown Envoi Pathology Brisbane, Australia ianbrown@envoi.com.au Topics for discussion Classification of gastritis Minimal diagnostic criteria for gastritis H.pylori negative
Gastritis (and gastropathy) Dr Ian Brown Envoi Pathology Brisbane, Australia ianbrown@envoi.com.au Topics for discussion Classification of gastritis Minimal diagnostic criteria for gastritis H.pylori negative
T he distinction between ulcerative colitis
 1233 REVIEW Indeterminate colitis M Guindi, R H Riddell... Indeterminate colitis (IC) originally referred to those 10 15% of cases of inflammatory bowel disease (IBD) in which there was difficulty distinguishing
1233 REVIEW Indeterminate colitis M Guindi, R H Riddell... Indeterminate colitis (IC) originally referred to those 10 15% of cases of inflammatory bowel disease (IBD) in which there was difficulty distinguishing
Mimics of Inflammatory Bowel Disease. Dr Catriona McKenzie Royal Prince Alfred Hospital, Camperdown
 Mimics of Inflammatory Bowel Disease Dr Catriona McKenzie Royal Prince Alfred Hospital, Camperdown Mimics of IBD: Overview Infections Drugs Autoimmune Other Infections Diagnostic Histopathology, 2015 Case
Mimics of Inflammatory Bowel Disease Dr Catriona McKenzie Royal Prince Alfred Hospital, Camperdown Mimics of IBD: Overview Infections Drugs Autoimmune Other Infections Diagnostic Histopathology, 2015 Case
Chapter 12: Training in Pathology. DDSEP Chapter 13: Question 19
 DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
Normal small intestine Variations
 THE HISTOPATHOLOGICAL DIAGNOSIS OF THE TERMINAL ILEUM BIOPSY K. Geboes, MD, PhD, AGAF, dr. H.C. Belgium Normal small intestine Variations Duodenum Ileum 1 Proliferative compartment Normal variations 2
THE HISTOPATHOLOGICAL DIAGNOSIS OF THE TERMINAL ILEUM BIOPSY K. Geboes, MD, PhD, AGAF, dr. H.C. Belgium Normal small intestine Variations Duodenum Ileum 1 Proliferative compartment Normal variations 2
HDF Case CRYPTOSPORIDIOSE
 HDF Case 986949 CRYPTOSPORIDIOSE 45 yo male with severe diarrhea. Known HIV positive. Endoscopic biopsy of duodenum, the colon and ileum. EXUDATIVE CHANGES GRANULAR BASOPHILIC BODIES Colonic biopsy shows
HDF Case 986949 CRYPTOSPORIDIOSE 45 yo male with severe diarrhea. Known HIV positive. Endoscopic biopsy of duodenum, the colon and ileum. EXUDATIVE CHANGES GRANULAR BASOPHILIC BODIES Colonic biopsy shows
The pathology of IBD and its modification by liver disease. Roger Feakins ESP/H-ECCO
 The pathology of IBD and its modification by liver disease Roger Feakins ESP/H-ECCO Enterprise Interest None IBD UC [IBDU] Crohn s IBD: distribution of disease Ulcerative colitis continuous Crohn s colitis
The pathology of IBD and its modification by liver disease Roger Feakins ESP/H-ECCO Enterprise Interest None IBD UC [IBDU] Crohn s IBD: distribution of disease Ulcerative colitis continuous Crohn s colitis
Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy
 Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy M. Perdiki 2, G. Bamias 1, D. Pouloudi 2, H. Gogas 3, I. Delladetsima 2 1 Academic Dpt. of Gastroenterology,
Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy M. Perdiki 2, G. Bamias 1, D. Pouloudi 2, H. Gogas 3, I. Delladetsima 2 1 Academic Dpt. of Gastroenterology,
INFLAMMATORY BOWEL DISEASE
 National University Faculty of Medicine INFLAMMATORY BOWEL DISEASE Gehan M. Osman, MD. MBBS Pediatrician Jaffar Ibn Auf Specialized Hospital EDUCATIONAL OBJECTIVES Definitions and spectrum of (IBD) Epidemiology
National University Faculty of Medicine INFLAMMATORY BOWEL DISEASE Gehan M. Osman, MD. MBBS Pediatrician Jaffar Ibn Auf Specialized Hospital EDUCATIONAL OBJECTIVES Definitions and spectrum of (IBD) Epidemiology
Review Histological evaluation in ulcerative colitis
 Gastroenterology Report 2 (2014) 178 192, doi:10.1093/gastro/gou031 Advance access publication 18 June 2014 Review Histological evaluation in ulcerative colitis Tom C. DeRoche 1, Shu-Yuan Xiao 2 and Xiuli
Gastroenterology Report 2 (2014) 178 192, doi:10.1093/gastro/gou031 Advance access publication 18 June 2014 Review Histological evaluation in ulcerative colitis Tom C. DeRoche 1, Shu-Yuan Xiao 2 and Xiuli
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
CT Evaluation of Bowel Wall Thickening. Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University.
 CT Evaluation of Bowel Wall Thickening By Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University. The CT findings of bowel wall thickening includes 1 Degree of thickening.
CT Evaluation of Bowel Wall Thickening By Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University. The CT findings of bowel wall thickening includes 1 Degree of thickening.
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
IATROGENIC AND DRUG INDUCED PATHOLOGY IN THE SMALL INTESTINE. Claude Cuvelier N. Goormaghtigh Institute of Pathology
 IATROGENIC AND DRUG INDUCED PATHOLOGY IN THE SMALL INTESTINE Claude Cuvelier N. Goormaghtigh Institute of Pathology Content Iatrogenic pathology Radiation Chemotherapy Graft-Versus-Host disease Changes
IATROGENIC AND DRUG INDUCED PATHOLOGY IN THE SMALL INTESTINE Claude Cuvelier N. Goormaghtigh Institute of Pathology Content Iatrogenic pathology Radiation Chemotherapy Graft-Versus-Host disease Changes
Endoscopic mucosal biopsies are useful in distinguishing granulomatous colitis due to Crohn s disease from tuberculosis
 Gut 1999;45:537 541 537 Wellcome Research Unit, Department of Gastrointestinal Sciences, Christian Medical College and Hospital, Vellore 632 004, Tamilnadu, India A B Pulimood B S Ramakrishna G Kurian
Gut 1999;45:537 541 537 Wellcome Research Unit, Department of Gastrointestinal Sciences, Christian Medical College and Hospital, Vellore 632 004, Tamilnadu, India A B Pulimood B S Ramakrishna G Kurian
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT.
 PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
Small Bowel Cases. Introduction. Introduction, Continued 12/7/2011. Lesions Found on endoscopic biopsies Just Like Signing Out
 Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Opportunistic Infections of the Colon in
 Opportunistic Infections of the Colon in Inflammatory Bowel Disease Dr SM Bigby Laboratory Services, Middlemore Hospital, Auckland Second European Consensus on prevention, diagnosis and management of infections
Opportunistic Infections of the Colon in Inflammatory Bowel Disease Dr SM Bigby Laboratory Services, Middlemore Hospital, Auckland Second European Consensus on prevention, diagnosis and management of infections
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
2015 복영증례 51/M C.C. Past Hx: DM, HTN (1998), Lab: WBC (11500/ μl ), CRP (0.71 mg/dl) 순천향서울병원황지영, 홍성숙 APCT (HAD #1) APCT (HAD#1) APCT (HAD #15)
, Lab: WBC (11500/ μl ), CRP (0.71 mg/dl) 순천향서울병원황지영, 홍성숙 APCT (HAD #1) APCT (HAD#1) APCT (HAD #15)") Case 1 2015 복영증례 순천향서울병원황지영, 홍성숙 51/M C.C Abdominal pain and chilling (1 week ago) Diarrhea (a month ago) Past Hx: DM, HTN (1998), Alcoholic liver disease (2008) Lab: WBC (11500/ μl ), CRP (0.71 mg/dl)
Case 1 2015 복영증례 순천향서울병원황지영, 홍성숙 51/M C.C Abdominal pain and chilling (1 week ago) Diarrhea (a month ago) Past Hx: DM, HTN (1998), Alcoholic liver disease (2008) Lab: WBC (11500/ μl ), CRP (0.71 mg/dl)
Ulcerative Colitis after Multidisciplinary Treatment for Colorectal Cancer with Multiple Liver Metastases : A Case Report
 Showa Univ J Med Sci 29 3, 315 319, September 2017 Case Report Ulcerative Colitis after Multidisciplinary Treatment for Colorectal Cancer with Multiple Liver Metastases : A Case Report Kodai TOMIOKA 1
Showa Univ J Med Sci 29 3, 315 319, September 2017 Case Report Ulcerative Colitis after Multidisciplinary Treatment for Colorectal Cancer with Multiple Liver Metastases : A Case Report Kodai TOMIOKA 1
Pouchitis and Cuffitis A bloody mess. Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board
 Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Clinical History. ACCME/Disclosure. Case 5 John Hart, M.D. University of Chicago. Dr. Hart has nothing to disclose 4/13/2016
 Case 5 John Hart, M.D. University of Chicago slide courtesy of Dr. Anthony Sofia Diagnosed with ileocolonic Crohn Disease Discontinued infliximab due to lack of insurance Clinical History Admitted for
Case 5 John Hart, M.D. University of Chicago slide courtesy of Dr. Anthony Sofia Diagnosed with ileocolonic Crohn Disease Discontinued infliximab due to lack of insurance Clinical History Admitted for
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Inflammatory Bowel Disease Ischemic bowel disease
 Inflammatory Bowel Disease Ischemic bowel disease Inflammatory Bowel Disease The two disorders that comprise IBD are: ulcerative colitis Crohn disease The distinction between ulcerative colitis and Crohn
Inflammatory Bowel Disease Ischemic bowel disease Inflammatory Bowel Disease The two disorders that comprise IBD are: ulcerative colitis Crohn disease The distinction between ulcerative colitis and Crohn
Ileocolonoscopy in Seronegative Spondylarthropathy
 GASTROENTEROLOGY 1989;96:339-44 Ileocolonoscopy in Seronegative Spondylarthropathy M. DE vas, c. CUVELIER, H. MIELANTS, E. VEYS, F. BARBIER, and A:ELEWAUT Departments of Gastroenterology, Pathology, and
GASTROENTEROLOGY 1989;96:339-44 Ileocolonoscopy in Seronegative Spondylarthropathy M. DE vas, c. CUVELIER, H. MIELANTS, E. VEYS, F. BARBIER, and A:ELEWAUT Departments of Gastroenterology, Pathology, and
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Digestion: Small and Large Intestines Pathology
 Digestion: Small and Large Intestines Pathology Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified health
Digestion: Small and Large Intestines Pathology Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified health
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL
 NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
How I Handle Mast Cells in GI Biopsies
 How I Handle Mast Cells in GI Biopsies Dora Lam-Himlin, MD Rodger C. Haggitt Gastrointestinal Pathology Society Forum United States and Canadian Academy of Pathologists Seattle, Washington, March 12, 2016
How I Handle Mast Cells in GI Biopsies Dora Lam-Himlin, MD Rodger C. Haggitt Gastrointestinal Pathology Society Forum United States and Canadian Academy of Pathologists Seattle, Washington, March 12, 2016
Allergic Colitis Clinical and Endoscopic Aspects of Infants. with Rectal Bleeding
 Allergic Colitis Clinical and Endoscopic Aspects of Infants. with Rectal Bleeding Allergic Colitis is an inflammatory disorder of the colon which occurs mainly in preschool children. It is caused by an
Allergic Colitis Clinical and Endoscopic Aspects of Infants. with Rectal Bleeding Allergic Colitis is an inflammatory disorder of the colon which occurs mainly in preschool children. It is caused by an
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Chronic diarrhea. Dr.Nasser E.Daryani Professor of Tehran Medical University
 1 Chronic diarrhea Dr.Nasser E.Daryani Professor of Tehran Medical University Timing Acute diarrhea: 4 weeks Definitions Derived from Greek
1 Chronic diarrhea Dr.Nasser E.Daryani Professor of Tehran Medical University Timing Acute diarrhea: 4 weeks Definitions Derived from Greek
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease
 The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Microscopic colitis: Is it a spectrum of inflammatory bowel disease?
 Online Submissions: http://www.wjgnet.com/esps/ wjg@wjgnet.com doi:10.3748/wjg.v19.i26.4252 World J Gastroenterol 2013 July 14; 19(26): 4252-4256 ISSN 1007-9327 (print) ISSN 2219-2840 (online) 2013 Baishideng.
Online Submissions: http://www.wjgnet.com/esps/ wjg@wjgnet.com doi:10.3748/wjg.v19.i26.4252 World J Gastroenterol 2013 July 14; 19(26): 4252-4256 ISSN 1007-9327 (print) ISSN 2219-2840 (online) 2013 Baishideng.
Clinico-pathological study of colonoscopic biopsies in patients with chronic diarrhea
 International Journal of Research in Medical Sciences Bhagyalakshmi A et al. Int J Res Med Sci. 2016 Jul;4(7):2738-2744 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20161942
International Journal of Research in Medical Sciences Bhagyalakshmi A et al. Int J Res Med Sci. 2016 Jul;4(7):2738-2744 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20161942
Lymphocytic Gastritis, Isolated Type Occurring in Family Members. A Case Report.
 Lymphocytic Gastritis, Isolated Type Occurring in Family Members. A Case Report. Alan Shienbaum, DO; AndriyPavlenko, MD; Jun Liu, MD, PhD; Janusz J Godyn, MD. Pathology Department, Kennedy University Hospitals,
Lymphocytic Gastritis, Isolated Type Occurring in Family Members. A Case Report. Alan Shienbaum, DO; AndriyPavlenko, MD; Jun Liu, MD, PhD; Janusz J Godyn, MD. Pathology Department, Kennedy University Hospitals,
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Diseases of the Colon. Jack Bragg, D.O., F.A.C.O.I.
 Diseases of the Colon Jack Bragg, D.O., F.A.C.O.I. I have no disclosures I work for the Curators of the University of Missouri Inflammatory Bowel Disease ULCERATIVE COLITIS CROHN S DISEASE Transmural Inflammation
Diseases of the Colon Jack Bragg, D.O., F.A.C.O.I. I have no disclosures I work for the Curators of the University of Missouri Inflammatory Bowel Disease ULCERATIVE COLITIS CROHN S DISEASE Transmural Inflammation
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis
 doi: 10.2169/internalmedicine.1607-18 http://internmed.jp CASE REPORT A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis Rumiko Tsuboi,
doi: 10.2169/internalmedicine.1607-18 http://internmed.jp CASE REPORT A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis Rumiko Tsuboi,
Jonathan R. Dillman, MD, MSc. Associate Professor Department of Radiology Cincinnati Children s Hospital Medical Center
 MR Enterography in Children: Interpretation & Value-Added Jonathan R. Dillman, MD, MSc Associate Professor Department of Radiology Cincinnati Children s Hospital Medical Center Disclosures Crohn s disease
MR Enterography in Children: Interpretation & Value-Added Jonathan R. Dillman, MD, MSc Associate Professor Department of Radiology Cincinnati Children s Hospital Medical Center Disclosures Crohn s disease
IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis?
 CASE REPORT IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis? Keita Saeki 1, Shigenari Hozawa 1, Naoteru Miyata 1,
CASE REPORT IgG4-Negative Autoimmune Pancreatitis with Sclerosing Cholangitis and Colitis: Possible Association with Primary Sclerosing Cholangitis? Keita Saeki 1, Shigenari Hozawa 1, Naoteru Miyata 1,
8/29/2016 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW. LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES
 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
children Crohn s disease in MR enterography for GI Complications Microscopy Characterization Primary sclerosing cholangitis Anorectal fistulae
 MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
-2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency
 rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency") SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
USCAP Pediatric Pathology Speciality Conference Case 3. S.Ranganathan, MD Children s Hospital of Pittsburgh of UPMC 4/13/2016
 USCAP Pediatric Pathology Speciality Conference - 2016 SPP asks all individuals involved in the development and presentation of Continuing Medical Education (CME) activities to disclose all relationships
USCAP Pediatric Pathology Speciality Conference - 2016 SPP asks all individuals involved in the development and presentation of Continuing Medical Education (CME) activities to disclose all relationships
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Segmental colonoscopic biopsies in the differentiation of ileocolic tuberculosis from Crohn s disease
 Blackwell Science, LtdOxford, UKJGHJournal of Gastroenterology and Hepatology0815-93192005 Blackwell Publishing Asia Pty LtdMay 2005205688696Original ArticleSegmental biopsies in and Crohn s diseaseab
Blackwell Science, LtdOxford, UKJGHJournal of Gastroenterology and Hepatology0815-93192005 Blackwell Publishing Asia Pty LtdMay 2005205688696Original ArticleSegmental biopsies in and Crohn s diseaseab
MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY
 MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY Alberto Fusi Charité Comprehensive Cancer Centre - Berlin St. George s University - London TAO Meeting - Cancer Toxicity Management Paris - 8th-9th December
MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY Alberto Fusi Charité Comprehensive Cancer Centre - Berlin St. George s University - London TAO Meeting - Cancer Toxicity Management Paris - 8th-9th December
INFLAMMATORY BOWEL DISEASE. Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic
 INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing