ENDOVASCULAR TREATMENT OF SFA
|
|
|
- Hugh Wood
- 5 years ago
- Views:
Transcription



1 ENDOVASCULAR TREATMENT OF SFA WHAT TO DO IN CASE OF DISSECTION, HOW TO REENTER THE LUMEN, WHEN TO STENT, WHEN NOT TO? E.DUCASSE MD PHD FEBVS, CHU DE BORDEAUX 2018
 3 These lesions are often underrepresented in clinical trials 30% of CTOs in most RCTs Subintimal angioplasty was first used in 1987 by Bolia 3 The ability to consistently")
2 ENDOVASCULAR TTT OF SFA NOWDAYS PTA first introduced in the 1960s 1,2 Challenge = passage of guidewire through CTOs Clinical presentations are becoming worse and worse length number of CTOs (up to 50% in daily practice) 3 These lesions are often underrepresented in clinical trials 30% of CTOs in most RCTs Subintimal angioplasty was first used in 1987 by Bolia 3 The ability to consistently cross a CTO takes years of experience and intimate knowledge of the multitude of wires, support catheters, and dedicated CTO crossing devices now available CTOs with a strong calcium component and extensive lesions (>15 cm) are still a factor of failure A crossing rate of 90% is only encountered in expert centers Long CTOs starting in the SFA and reconstituting in a distal tibial vessel may be the most challenging 1. Dotter et al. Circulation 30: Gruntzig et al. Deutsc Med Wochenschr 99: Banerjee et al. Am J Cardiol 104: Bolia et al. Clin Radiol. 1989;40:325.



3 WHAT TO DO IN CASE OF DISSECTION 1/ Antegrade approach Guidewire alone Sometimes dissection is inevitable or even intentional 1,2 ± support catheter or OTW balloon Sliding Technique Drilling Technique Penetration Technique Parallel wire technique Guidewire with polymer + hydrophilic coating Stiff hydrophobic guidewire / non tappered Alternative to the drilling technique Severly calcified lesions/resisting CTOs Super-stiff guidewire / tappered First wire enters false lumen, it is left in place Second wire (typically stiffer and tapered with different tip bend) is passed parallel to the first wire into the true lumen 1. Reekers et al. Eur J Vasc Surg 1994;8: Reekers et al. Eur J Radiol 1998;28:192-8
4 WHAT TO DO IN CASE OF DISSECTION Microchannel Technique majority of CTOs have intraluminal microchannels from 100μm500μm Guidewire alone proximal fibrous cap is first centrally penetrated to 1mm 2mm with very stiff guidewire and support catheter careful injection of undiluted contrast (1mL) immediately distal to proximal cap of CTO identifies and enlarges microchannels creating a pathway between proximal and distal true lumens ± support catheter or OTW balloon Sliding Technique Drilling Technique Penetration Technique Parallel wire technique Guidewire with polymer + hydrophilic coating Stiff hydrophobic guidewire / non tappered Alternative to the drilling technique Severly calcified lesions/resisting CTOs Super-stiff guidewire / tappered First wire enters false lumen, it is left in place Second wire (typically stiffer and tapered with different tip bend) is passed parallel to the first wire into the true lumen
5 WHAT TO DO IN CASE OF DISSECTION 1/ Antegrade approach Guidewire loops over CTO Loop wire technique (Knuckle technique) Standard floppy guidewire + support catheter or OTW balloon Helps for loop creation and control of its length and shape during the recanalization process Helps «Un»looping the guidewire at the end to use its angulation in order to re-entre into the true lumen Helps verify the true lumen re-entry with contrast medium injection Helps exchange guidewires if necessary Gradually choosing stiffer guidewires with higher tip loads Start with hydrophilic, angled Glidewire (Terumo Interventional Systems, Inc., Somerset, NJ) supported by a inch support catheter Change for stiff guidewire for more support Or Terumo Advantage Change for or if necessary

6 HOW TO REENTER THE LUMEN 1/ Antegrade approach Guidewire loops over CTO Loop wire technique (Knuckle technique) Standard floppy guidewire Perforation 5-8% of the cases 1,2 Wire is seen under fluoroscopy as traveling outside the normal course of the arterial anatomy Tip of the wire curls abnormally as it enters the soft tissue planes Angiography may reveal extravasation of contrast material Wire should be withdrawn and an attempt made to find a newsubintimal plane to cross the lesion Isolated wire perforations usually seal with conservative management Worse case scenario Stop the procedure and resume a few weeks later Use a Stent graft if you manage to re-enter 1. Hayes et al. J Endovasc Ther 2002;9: Nasim et al. Eur J Vasc Endovasc Surg 1996;12: Picture from the Rutherford 8th Ed


7 HOW TO REENTER THE LUMEN 2/ Retrograde approach First series by Spinosa et al. JVIR 2005 High risk to damage distal target vessel by continuing antegrade approach while it might be the only landing zone for bypass Inability to re-enter into the true lumen Rupture or loss of the antegrade vessel pathway Inability to correctly identify the origin of peroneal of tibial artery Consider a retrograde approach rapidely after the first re-entry failures rather than engaging in prolonged attempts These procedures are time and energy consuming fur the patient and the team!!
8 HOW TO REENTER THE LUMEN 2/ Retrograde approach First series by Spinosa et al. JVIR 2005 High risk to damage distal target vessel by continuing antegrade approach while it might be the only landing zone for bypass Inability to re-enter into the true lumen Rupture or loss of the antegrade vessel pathway Inability to correctly identify the origin of peroneal of tibial artery Optimal installation is key Sterile preparation of both groins + entire leg Ultrasound guided puncture (ATA+++) Identify target artery in longitudinal view Puncture at 45 in transversal view Verify intraluminal positionning of guidewire in longitudinal view


9 HOW TO REENTER THE LUMEN 2/ Retrograde approach First series by Spinosa et al. JVIR 2005 High risk to damage distal target vessel by continuing antegrade approach while it might be the only landing zone for bypass Inability to re-enter into the true lumen Rupture or loss of the antegrade vessel pathway Inability to correctly identify the origin of peroneal of tibial artery Fluoroscopy guided puncture Optimal installation is key Sterile preparation of both groins + entire leg Simple scopy if calcified If not proximal injection + road-mapping Parallax adjustment +++ Needle and artery must be perfectly aligned R. Ferraresi, CACVS 2014 For ATA, PTA and PA feet attached together in internal rotation For complex vascular anatomy of the foot and plantar arch Foot in abduction + Standard anteroposterior and lateral oblique projections





10 HOW TO REENTER THE LUMEN 2/ Retrograde approach Through the distal tract of the ATA usually the easiest Through the proximal tract of the peroneal artery right between the bones not possible to perform manual compression rare risk of compartment syndrome Through the PTA more difficult, especially around the malleolar area 2017 A systematic review of results with the retrograde tibial approach Which artery? Olaf J. Bakker Vascular Surgeon UMC Utrecht, The Netherlands Results
11 HOW TO REENTER THE LUMEN 2/ Retrograde approach Dedicated material 16-G needle or 21-G micropuncture kit Antispasm Cocktail Wires guidewires / guidewires Wire excalation strategy (stiffer wire) Support catheters or OTW balloon catheters Sheathless +++ SAFARI 3-4F microsheath Guidewire and catheter inserted directly through the skin Only when you need to use a balloon Procedure resumed by antegrade way



12 HOW TO REENTER THE LUMEN 2/ Retrograde approach Sheathless As compared to proximal cap, distal cap is usually less resistant which makes penetration easier 3-4F Micro-Sheath «Rendez-vous» Proximal re-entry is usually not an issue After proximal wire pickup, the procedure can be completed from above antegrade inflation of a low-pressure balloon + manual compression Hemostasis Patency checked by angiography Parallel balloon technique Moderate-sized balloon in the sub-intimal space to create a dissection plane, crack the intima and allow reentry into the lumen either via an antegrade or retrograde approach


13 WHEN TO STENT Definition of Vessel Dissection


14 WHEN TO STENT

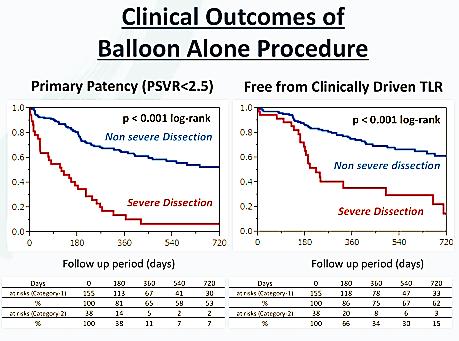
15 WHEN TO STENT


16 WHEN TO STENT SO YES to the «no metallic implant left behind» But only in lesions <10-15 cm AND NOT in CTOs Which are long and calcified lesions Often present with Flow-limiting dissection A Dissection can t heal by itself when the blood-fluid pressure between the two sides of the dissection is >10mmHg And residual stenosis/recoil >50% it s difficult to keep them open for a long time without scaffolding At least in the proximal or distal portion and sometimes we need a full-length stent
17 CLINICAL CASE : 58 YEARS OLD CV risk factors : Active Smoking, DM History : 2008 : CLI right limb over occlusion of right SFA Recnalaization failure of SFA by anterograde & retrograde approach Numerous collaterals coming from th profunda Medical therapy Obese, COPD, CKD-EPI : Cl 36 ml/min Alcoholic cirrhosis waiting for a second liver transplant for ischemic cholangitis CAD with myocardiopathy (stents x 2), ablation of atrial fibrillation in 2016 Clinical Evaluation : Severe claudication of right limb (<100m) Strandness : 70m right calf pain No popliteal or distal pulses ABI : 0.25 right / 0.83 left


18 CTA FRONT BACK


19 ANTEGRADE APPROACH FIRST No SFA Stump PC puncture of left CFA + CROSS OVER Short 6F sheath Glide Terumo guidewire x 180 cm UF catheter Stiff Terumo guidewire x 180 cm Long 6F sheath pushed inside the right CFA
20 ANGIOGRAM


21 ANTEGRADE APPROACH FIRST Glide Terumo guidewire x 180 cm Trailblazer Stiff Terumo guidewire x 180 cm Trailblazer Stiff Terumo guidewire x 180 cm Seeker 0.035



22 RETROGRADE PUNCTURE OF THE POPLITEAL ARTERY IN A SUPINE POSITION 16-Gauge Needle x 83 mm


23 PROCEDURE RESUMED BY ANTEGRADE WAY


24 LENGTH TROUBLE = GUIDEWIRE EXCHANGE Glide Terumo GW x 260mm

25 «TELEPHERIQUE» TECHNIQUE POBA 5 x 100mm

26 GUIDEWIRE PUSHED THROUGH THE POPLITEAL ARTERY Prolonged inflation over retrograde puncture site for hemostasis

 7 x 60mm Post-dilation by 5 x")
27 ANGIOGRAM Long Stenting from distal to proximal part of the dissection : SmartFlex (Cordis) 6 x 150mm SmartFlex (Cordis) 6 x100mm Tigris (Gore) 7 x 60mm Post-dilation by 5 x 100mm balloon

28 FINAL ANGIOGRAM Percutanous closure device : FémoSeal


29 TAKE HOME MESSAGE Endovascular treatment of the SFA is almost always successful in the acute phase BUT experience is definitely required to cross long CTOs it is very important to be closely familiar with all of the guidewires and catheters you should have a good portfolio of devices on hand Subintimal angioplasty may be volontary and even result in a good first-line approach to long CTOs and flush occlusions Antegrade-Retrograde techniques improve even more success rates Stenting is almost always necessary in recanalized CTOs At least in part John Quincy Adams


30 THANK YOU FOR YOUR ATTENTION
In foot treatment : what not to do? clinical experience. E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux
 In foot treatment : what not to do? clinical experience E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux Disclosure Speaker name: Pr E Ducasse I do not have any potential conflict of interest
In foot treatment : what not to do? clinical experience E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux Disclosure Speaker name: Pr E Ducasse I do not have any potential conflict of interest
Lessons for Successful Subintimal Angioplasty in SFA CTO
 Lessons for Successful Subintimal Angioplasty in SFA CTO John R. Laird Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center CTOs in the Periphery Presence of Total Occlusion
Lessons for Successful Subintimal Angioplasty in SFA CTO John R. Laird Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center CTOs in the Periphery Presence of Total Occlusion
Disclosures. Tips and Tricks for Tibial Intervention. Tibial intervention overview
 Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries
 MEET 2013 Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HOSPITAL AND MEDICAL CENTER READING, PA USA Chronic
MEET 2013 Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HOSPITAL AND MEDICAL CENTER READING, PA USA Chronic
UC SF. Introduction: Retrograde Access. Pedal Access: When to Do It How Does it Fare. Introduction: Retrograde Access. Introduction: Retrograde Access
 Introduction: Retrograde Access Pedal Access: When to Do It How Does it Fare Wide spread application of endovascular techniques to infrageniculate arterial occlusive disease Technical failure rate of crossing
Introduction: Retrograde Access Pedal Access: When to Do It How Does it Fare Wide spread application of endovascular techniques to infrageniculate arterial occlusive disease Technical failure rate of crossing
Endovascular Approach to CTOs: Crossing methods and Devices
 Endovascular Approach to CTOs: Crossing methods and Devices Anish J. Thomas, MD FACC FSCAI Interventional Cardiology Vascular/Endovascular Medicine SSM Heart Institute St. Louis, MO Disclosure Consultant:
Endovascular Approach to CTOs: Crossing methods and Devices Anish J. Thomas, MD FACC FSCAI Interventional Cardiology Vascular/Endovascular Medicine SSM Heart Institute St. Louis, MO Disclosure Consultant:
The essentials for BTK procedures: wires, balloons, what else
 A comprehensive approach to diabetic patient Tx The essentials for BTK procedures: wires, balloons, what else Dai-Do Do Clinical and Interventional Angiology Cardiovascular Department Disclosure Speaker
A comprehensive approach to diabetic patient Tx The essentials for BTK procedures: wires, balloons, what else Dai-Do Do Clinical and Interventional Angiology Cardiovascular Department Disclosure Speaker
Copyright HMP Communications
 Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Access strategy for chronic total occlusions (CTOs) is crucial
 is crucial") Learn How Access Strategy Impacts Complex CTO Crossing Arthur C. Lee, MD The Cardiac & Vascular Institute, Gainesville, Florida VASCULAR DISEASE MANAGEMENT 2018;15(3):E19-E23. Key words: chronic total
Learn How Access Strategy Impacts Complex CTO Crossing Arthur C. Lee, MD The Cardiac & Vascular Institute, Gainesville, Florida VASCULAR DISEASE MANAGEMENT 2018;15(3):E19-E23. Key words: chronic total
Annals of Vascular Diseases Advance Published Date: June 2, Horie K, et al.
 2016 Annals of Vascular Diseases doi:10.3400/avd.cr.16-00007 Case Report Recanalization of a Heavily Calcified Chronic Total Occlusion in a Femoropopliteal Artery Using a Wingman Crossing Catheter Kazunori
2016 Annals of Vascular Diseases doi:10.3400/avd.cr.16-00007 Case Report Recanalization of a Heavily Calcified Chronic Total Occlusion in a Femoropopliteal Artery Using a Wingman Crossing Catheter Kazunori
Re-entry into the true lumen from the subintimal space
 VASCULAR AND ENDOVASCULAR TECHNIQUES Peter F. Lawrence, MD, Section Editor Re-entry into the true lumen from the subintimal space Peter A. Schneider, MD, Michael T. Caps, MD, MPH, and Nicolas Nelken, MD,
VASCULAR AND ENDOVASCULAR TECHNIQUES Peter F. Lawrence, MD, Section Editor Re-entry into the true lumen from the subintimal space Peter A. Schneider, MD, Michael T. Caps, MD, MPH, and Nicolas Nelken, MD,
Appropriate Device Selection for Endovascular Procedures
 Appropriate Device Selection for Endovascular Procedures Thomas M. Shimshak, MD Florida Hospital Heartland Medical Center Sebring, Florida Disclosures Speaker s Bureau: Abbott Vascular Boston Scientific
Appropriate Device Selection for Endovascular Procedures Thomas M. Shimshak, MD Florida Hospital Heartland Medical Center Sebring, Florida Disclosures Speaker s Bureau: Abbott Vascular Boston Scientific
There are multiple endovascular options for treatment
 Peripheral Rotablator Atherectomy: The Below-the-Knee Approach to Address Calcium Head On Peripheral Rotablator s front-cutting, diamond-tipped burr provides stable rotation in calcified lesions. BY SONYA
Peripheral Rotablator Atherectomy: The Below-the-Knee Approach to Address Calcium Head On Peripheral Rotablator s front-cutting, diamond-tipped burr provides stable rotation in calcified lesions. BY SONYA
Step by Step : How I treat SFA lesions
 BASIC TECHNIQUES IN PERIPHERAL INTERVENTIONS Step by Step : How I treat SFA lesions Koen Deloose, MD Vascular Surgery, AZ Sint Blasius Dendermonde, Belgium Access to the lesion Common femoral art. Superficial
BASIC TECHNIQUES IN PERIPHERAL INTERVENTIONS Step by Step : How I treat SFA lesions Koen Deloose, MD Vascular Surgery, AZ Sint Blasius Dendermonde, Belgium Access to the lesion Common femoral art. Superficial
Antegrade techniques for CTO recanalization. Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist
 Antegrade techniques for CTO recanalization Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist can CTOs be reliably opened by PCI? Meta-Analysis of 18,061 Patients Patel V, J Am Coll
Antegrade techniques for CTO recanalization Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist can CTOs be reliably opened by PCI? Meta-Analysis of 18,061 Patients Patel V, J Am Coll
Peripheral Arterial Disease: A Practical Approach
 Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step -
 Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
Crossing the Long SFA CTO
 Crossing the Long SFA CTO Techniques and Variables You need to Know Kyoto Katsura Hospital Cardiovascular Center Shigeru Nakamura M.D. Korea Soul 2011.4.28 28 Back ground Superficial femoral artery (SFA)
Crossing the Long SFA CTO Techniques and Variables You need to Know Kyoto Katsura Hospital Cardiovascular Center Shigeru Nakamura M.D. Korea Soul 2011.4.28 28 Back ground Superficial femoral artery (SFA)
Advanced d Techniques and Tools to Treat Below the Knee CTO
 TCTAP 2013, Apr. 23-26, 2013, Seoul, Korea Cardiovascular Center Tokeidai Memorial Hospital Sapporo, Japan Crossing Strategy t for Complex & CTO Lesion - Cross with Confidence - Supported by Educational
TCTAP 2013, Apr. 23-26, 2013, Seoul, Korea Cardiovascular Center Tokeidai Memorial Hospital Sapporo, Japan Crossing Strategy t for Complex & CTO Lesion - Cross with Confidence - Supported by Educational
THE RETROGRADE APPROACH FOR BELOW-THE- KNEE ANGIOPLASTIES:
 THE RETROGRADE APPROACH FOR BELOW-THE- KNEE ANGIOPLASTIES: Massimiliano Fusaro, MD Interventional Cardiologist Hemodynamics and Cardiovascular Interventions Service San Pellegrino Hospital Castiglione
THE RETROGRADE APPROACH FOR BELOW-THE- KNEE ANGIOPLASTIES: Massimiliano Fusaro, MD Interventional Cardiologist Hemodynamics and Cardiovascular Interventions Service San Pellegrino Hospital Castiglione
Successful endovascular treatment for BTK lesion using wire rendezvous technique and retrograde knuckle wire technique by collateral approach
 Successful endovascular treatment for BTK lesion using wire rendezvous technique and retrograde knuckle wire technique by collateral approach Katsutoshi Takayama, MD, Ph.D Department of Radiology and Interventional
Successful endovascular treatment for BTK lesion using wire rendezvous technique and retrograde knuckle wire technique by collateral approach Katsutoshi Takayama, MD, Ph.D Department of Radiology and Interventional
Can t See the Forest for the Trees: Transcollateral Crossing of Chronic Total Occlusions
 Can t See the Forest for the Trees: Transcollateral Crossing of Chronic Total Occlusions Vinayak Subramanian, BS 1 ; George L. Adams, MD, MHS 2 From 1 Department of Biomedical Engineering, North Carolina
Can t See the Forest for the Trees: Transcollateral Crossing of Chronic Total Occlusions Vinayak Subramanian, BS 1 ; George L. Adams, MD, MHS 2 From 1 Department of Biomedical Engineering, North Carolina
Case Report pissn / eissn J Korean Soc Radiol 2016;74(1):
:") Case Report pissn 1738-2637 / eissn 2288-2928 http://dx.doi.org/10.3348/jksr.2016.74.1.37 Target Balloon-Assisted Antegrade and Retrograde Approach for Recanalization of Thrombosed Fem-Pop Bypass Graft
Case Report pissn 1738-2637 / eissn 2288-2928 http://dx.doi.org/10.3348/jksr.2016.74.1.37 Target Balloon-Assisted Antegrade and Retrograde Approach for Recanalization of Thrombosed Fem-Pop Bypass Graft
Access (Antegrade, Retrograde, Pedal)
") Access (Antegrade, Retrograde, Pedal) ARCH St. Louis Craig M. Walker, MD, FACC, FACP Clinical Professor of Medicine Tulane University School of Medicine New Orleans, LA Clinical Professor of Medicine LSU
Access (Antegrade, Retrograde, Pedal) ARCH St. Louis Craig M. Walker, MD, FACC, FACP Clinical Professor of Medicine Tulane University School of Medicine New Orleans, LA Clinical Professor of Medicine LSU
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Novel distal popliteal artery puncture technique in supine position for chronic femoropopliteal arterial occlusion; frontal popliteal puncture
 Novel distal popliteal artery puncture technique in supine position for chronic femoropopliteal arterial occlusion; frontal popliteal puncture Miyazaki Medical Association Hospital Cardiovascular Center
Novel distal popliteal artery puncture technique in supine position for chronic femoropopliteal arterial occlusion; frontal popliteal puncture Miyazaki Medical Association Hospital Cardiovascular Center
Step by step Hybrid procedures in peripheral obstructive disease. Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery
 Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
The Burden of CLI and Crosser Catheter Recanalization Strategies
 , LLC an HMP Communications Holdings Company November 2013 Volume 25/ Supplement D www.invasivecardiology.com The Official Journal of the International Andreas Gruentzig Society The Burden of CLI and Crosser
, LLC an HMP Communications Holdings Company November 2013 Volume 25/ Supplement D www.invasivecardiology.com The Official Journal of the International Andreas Gruentzig Society The Burden of CLI and Crosser
Current Status of Endovascular Therapies for Critical Limb Ischemia
 Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Endovascular intervention for patients with femoro-popliteal and aorto-iliac TASC D lesions
 Endovascular intervention for patients with femoro-popliteal and aorto-iliac TASC D lesions Poster No.: C-2012 Congress: ECR 2014 Type: Educational Exhibit Authors: E. Thomee, W. C. Liong, D. R. Warakaulle;
Endovascular intervention for patients with femoro-popliteal and aorto-iliac TASC D lesions Poster No.: C-2012 Congress: ECR 2014 Type: Educational Exhibit Authors: E. Thomee, W. C. Liong, D. R. Warakaulle;
Leg arteries : MANAGEMENT and STRATEGY
 Leg arteries : MANAGEMENT and STRATEGY Prof E. Ducasse Unit of vascular surgery BORDEAUX ESVB May 14th 2011 BARD Symposium CLI : definition Fontaine Rutherford ABI Symptoms class category Asymptomatic
Leg arteries : MANAGEMENT and STRATEGY Prof E. Ducasse Unit of vascular surgery BORDEAUX ESVB May 14th 2011 BARD Symposium CLI : definition Fontaine Rutherford ABI Symptoms class category Asymptomatic
For Personal Use. Copyright HMP 2013 J INVASIVE CARDIOL 2013;25(5):E96-E100
:E96-E100") Case Report and Brief Review Transcollateral Approach for Percutaneous Revascularization of Complex Superficial Femoral Artery Chronic Total Occlusion Zaheed Tai, DO ABSTRACT: Chronic total occlusions
Case Report and Brief Review Transcollateral Approach for Percutaneous Revascularization of Complex Superficial Femoral Artery Chronic Total Occlusion Zaheed Tai, DO ABSTRACT: Chronic total occlusions
Hydrodynamic boost: a novel re-entry technique in distal BTK vessel: when and how to do it
 Hydrodynamic boost: a novel re-entry technique in distal BTK vessel: when and how to do it Roberto Ferraresi Peripheral Interventional Unit Bergamo Italy Disclosure Roberto Ferraresi, MD I have the following
Hydrodynamic boost: a novel re-entry technique in distal BTK vessel: when and how to do it Roberto Ferraresi Peripheral Interventional Unit Bergamo Italy Disclosure Roberto Ferraresi, MD I have the following
Interventional Cardiology
 r l Interventional Cardiology Intravascular ultrasound findings after knuckle wire technique for superficial femoral artery occlusion Aim: We assessed the wire behavior by using intravascular ultrasound
r l Interventional Cardiology Intravascular ultrasound findings after knuckle wire technique for superficial femoral artery occlusion Aim: We assessed the wire behavior by using intravascular ultrasound
True lumen re-entry devices facilitate subintimal angioplasty and stenting of total chronic occlusions: Initial report
 TECHNICAL NOTE True lumen re-entry devices facilitate subintimal angioplasty and stenting of total chronic occlusions: Initial report Donald L. Jacobs, MD, Raghunandan L. Motaganahalli, MD, Daniel E. Cox,
TECHNICAL NOTE True lumen re-entry devices facilitate subintimal angioplasty and stenting of total chronic occlusions: Initial report Donald L. Jacobs, MD, Raghunandan L. Motaganahalli, MD, Daniel E. Cox,
MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES
 MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES PUSHING BOUNDARIES Terumo Interventional Systems is committed to your success with innovative procedural solutions and ongoing support for your most challenging
MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES PUSHING BOUNDARIES Terumo Interventional Systems is committed to your success with innovative procedural solutions and ongoing support for your most challenging
Guidewire Selection. Making the Most Out of My Guidewire: LINC 2016: Leipzig Interventional Course Leipzig, Germany January 26-29, 2016
 Making the Most Out of My Guidewire: Guidewire Selection LINC 2016: Leipzig Interventional Course Leipzig, Germany January 26-29, 2016 Brian DeRubertis, MD, FACS Associate Professor of Surgery Division
Making the Most Out of My Guidewire: Guidewire Selection LINC 2016: Leipzig Interventional Course Leipzig, Germany January 26-29, 2016 Brian DeRubertis, MD, FACS Associate Professor of Surgery Division
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion
 Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Lets go on a SAFARI and Discover Novel Tactics. Awais Siddique MD Endovascular Interventional Radiology AZH/WAVE Centers Milwaukee WI
 Lets go on a SAFARI and Discover Novel Tactics Awais Siddique MD Endovascular Interventional Radiology AZH/WAVE Centers Milwaukee WI Subintimal Arterial Flossing with Antegrade Retrograde Intervention
Lets go on a SAFARI and Discover Novel Tactics Awais Siddique MD Endovascular Interventional Radiology AZH/WAVE Centers Milwaukee WI Subintimal Arterial Flossing with Antegrade Retrograde Intervention
Chronic Total Occlusion (CTO) Technologies
 Technologies") to receive our latest news and key activities. Chronic Total Occlusion (CTO) Technologies Re-open vital channels LinkedIn page Follow us on CORDIS EMEA OUTBACK LTD Re-Entry Catheter True Lumen Re-Entry
to receive our latest news and key activities. Chronic Total Occlusion (CTO) Technologies Re-open vital channels LinkedIn page Follow us on CORDIS EMEA OUTBACK LTD Re-Entry Catheter True Lumen Re-Entry
Disclosures. Talking Points. An initial strategy of open bypass is better for some CLI patients, and we can define who they are
 An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
Endovascular Intervention BtK Intervention in Patients with Chronic Dialysis
 Endovascular Intervention BtK Intervention in Patients with Chronic Dialysis GB Danzi, MD Ospedale Maggiore Policlinico Milan Italy Disease Pattern in PAD Hypercholesterolemia Age ESRD Current smoking
Endovascular Intervention BtK Intervention in Patients with Chronic Dialysis GB Danzi, MD Ospedale Maggiore Policlinico Milan Italy Disease Pattern in PAD Hypercholesterolemia Age ESRD Current smoking
Fielder XT: Initial and. Department of Cardiology, Asan Medical Center, Ulsan University of college of medicine
 Fielder XT: Initial and Professional Use for CTO Seung-Whan Lee, MD, PhD D t t f C di l A M di l C t Department of Cardiology, Asan Medical Center, Ulsan University of college of medicine Plastic-Jacket
Fielder XT: Initial and Professional Use for CTO Seung-Whan Lee, MD, PhD D t t f C di l A M di l C t Department of Cardiology, Asan Medical Center, Ulsan University of college of medicine Plastic-Jacket
Chronic Total Occlusion (CTO) Technologies. Re-open vital channels
 Technologies. Re-open vital channels") Chronic Total Occlusion (CTO) Technologies Re-open vital channels OUTBACK LTD Re-Entry Catheter True Lumen Re-Entry Technology Get back into the true lumen with ease and precision There are a number of
Chronic Total Occlusion (CTO) Technologies Re-open vital channels OUTBACK LTD Re-Entry Catheter True Lumen Re-Entry Technology Get back into the true lumen with ease and precision There are a number of
Bailout revascularization of chronic femoral artery occlusions with the new outback catheter following failed conventional endovascular intervention
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2009 Bailout revascularization of chronic femoral artery occlusions with the
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2009 Bailout revascularization of chronic femoral artery occlusions with the
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION
 CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
The Safari Technique to Perform Difficult Subintimal Infragenicular Vessels
 CardioVascular and Interventional Radiology ª Springer Science+Business Media, Inc. 2007 Published Online: 10 February 2007 Cardiovasc Intervent Radiol (2007) 30:469 473 DOI: 10.1007/s00270-006-0099-3
CardioVascular and Interventional Radiology ª Springer Science+Business Media, Inc. 2007 Published Online: 10 February 2007 Cardiovasc Intervent Radiol (2007) 30:469 473 DOI: 10.1007/s00270-006-0099-3
Chronic total occlusions (CTOs) are frequently
 are frequently") Specialty Crossing Devices: Understanding the Learning Curve Technical pearls and new devices for crossing peripheral CTOs. y Usman Javed, MD, and John R. Laird, MD (Courtesy of ard Peripheral Vascular,
Specialty Crossing Devices: Understanding the Learning Curve Technical pearls and new devices for crossing peripheral CTOs. y Usman Javed, MD, and John R. Laird, MD (Courtesy of ard Peripheral Vascular,
Utility of Image-Guided Atherectomy for Optimal Treatment of Ambiguous Lesions by Angiography
 Utility of Image-Guided Atherectomy for Optimal Treatment of Ambiguous Lesions by Angiography Jon C. George, MD; Vincent Varghese, DO From the Deborah Heart and Lung Center, Browns Mills, New Jersey. ABSTRACT:
Utility of Image-Guided Atherectomy for Optimal Treatment of Ambiguous Lesions by Angiography Jon C. George, MD; Vincent Varghese, DO From the Deborah Heart and Lung Center, Browns Mills, New Jersey. ABSTRACT:
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA. Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE
 PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
The PIERCE technique for recanalization of heavily calcified arteries in hemodialysis patients.
 The PIERCE technique for recanalization of heavily calcified arteries in hemodialysis patients. Tomoyasu Sato ( tomoyasu_satou@yahoo.co.jp ) Department of interventional and diagnostic Radiology Tsuchiya
The PIERCE technique for recanalization of heavily calcified arteries in hemodialysis patients. Tomoyasu Sato ( tomoyasu_satou@yahoo.co.jp ) Department of interventional and diagnostic Radiology Tsuchiya
Retrograde dorsalis pedis and posterior tibial artery access after failed antegrade angioplasty
 Retrograde dorsalis pedis and posterior tibial artery access after failed antegrade angioplasty Poster No.: C-2067 Congress: ECR 2010 Type: Topic: Authors: Keywords: DOI: Scientific Exhibit Interventional
Retrograde dorsalis pedis and posterior tibial artery access after failed antegrade angioplasty Poster No.: C-2067 Congress: ECR 2010 Type: Topic: Authors: Keywords: DOI: Scientific Exhibit Interventional
Pocket Reference Guide For (CTO) Technologies
 Technologies") to receive our latest news and key activities. Pocket Reference Guide For (CTO) Technologies LinkedIn page Follow us on CORDIS EMEA Table of Contents Essential prescribing information for both FRONTRUNNER
to receive our latest news and key activities. Pocket Reference Guide For (CTO) Technologies LinkedIn page Follow us on CORDIS EMEA Table of Contents Essential prescribing information for both FRONTRUNNER
The Utility of Atherectomy and the Jetstream Atherectomy System
 The Utility of Atherectomy and the Jetstream Atherectomy System William A. Gray, MD Columbia University Medical Center 2014 Boston Scientific Corporation or its affiliates. All rights reserved. IMPORTANT
The Utility of Atherectomy and the Jetstream Atherectomy System William A. Gray, MD Columbia University Medical Center 2014 Boston Scientific Corporation or its affiliates. All rights reserved. IMPORTANT
Guidewires for lower extremity artery angioplasty: a review
 EXPERT REVIEW PERIPHERAL INTERVENTIONS Guidewires for lower extremity artery angioplasty: a review Roberto Lorenzoni 1 *, MD, FESC, FACC; Roberto Ferraresi 2, MD; Marco Manzi 3, MD; Marco Roffi 4, MD,
EXPERT REVIEW PERIPHERAL INTERVENTIONS Guidewires for lower extremity artery angioplasty: a review Roberto Lorenzoni 1 *, MD, FESC, FACC; Roberto Ferraresi 2, MD; Marco Manzi 3, MD; Marco Roffi 4, MD,
My idea on intimal tracking guide wire selection for Pop-BTK treatment
 LINC 2017 Leipzig January 24-27, 2017 My idea on intimal tracking guide wire selection for Pop-BTK treatment Jos C. van den Berg, MD PhD Ospedale Regionale di Lugano, sede Civico Lugano University of Bern
LINC 2017 Leipzig January 24-27, 2017 My idea on intimal tracking guide wire selection for Pop-BTK treatment Jos C. van den Berg, MD PhD Ospedale Regionale di Lugano, sede Civico Lugano University of Bern
Tools and options for recanalisation of long-femoro-popliteal segments
 Tools and options for recanalisation of long-femoro-popliteal segments Pr E Ducasse Unit of Vascular Surgery University of Bordeaux ESVB 2011-may 14th E Ducasse, G Sassoust, D Midy THE ACCESS!! Retrograde
Tools and options for recanalisation of long-femoro-popliteal segments Pr E Ducasse Unit of Vascular Surgery University of Bordeaux ESVB 2011-may 14th E Ducasse, G Sassoust, D Midy THE ACCESS!! Retrograde
Introduction What Causes Peripheral Vascular Disease? How Do Doctors Treat Peripheral Vascular Disease?... 9
 Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Atherectomy with thrombectomy of. Rotarex S : The Leipzig experience
 Atherectomy with thrombectomy of femoropopliteal occlusions with Rotarex S : The Leipzig experience Dr. Bruno Freitas, Prof., MD Department of Interventional Angiology, Universität Leipzig, Germany Santa
Atherectomy with thrombectomy of femoropopliteal occlusions with Rotarex S : The Leipzig experience Dr. Bruno Freitas, Prof., MD Department of Interventional Angiology, Universität Leipzig, Germany Santa
Percutaneous Intervention for totally Occluded Coarctation Of Aorta. John Jose, Vipin Kumar, Ommen K George Dept Of Cardiology
 Percutaneous Intervention for totally Occluded Coarctation Of Aorta John Jose, Vipin Kumar, Ommen K George Dept Of Cardiology Background Coarctation of aorta (CoA) forms 5-7% of congenital heart diseases
Percutaneous Intervention for totally Occluded Coarctation Of Aorta John Jose, Vipin Kumar, Ommen K George Dept Of Cardiology Background Coarctation of aorta (CoA) forms 5-7% of congenital heart diseases
Is there a place for very distal BTK stenting? What are the options for acute PTA failure?
 Is there a place for very distal BTK stenting? What are the options for acute PTA failure? Dr. E. Puras Mallagray Hospital Universitario Quirón Madrid SPAIN Faculty disclosure Enrique Puras I disclose
Is there a place for very distal BTK stenting? What are the options for acute PTA failure? Dr. E. Puras Mallagray Hospital Universitario Quirón Madrid SPAIN Faculty disclosure Enrique Puras I disclose
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of June 4, 2018 Thrombolysis, Thrombectomy & Angioplasty
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of June 4, 2018 Thrombolysis, Thrombectomy & Angioplasty
Introduction 3. What is Peripheral Vascular Disease? 5. What Are Some of the Symptoms of Peripheral Vascular Disease? 6
 Patient Information Table of Contents Introduction 3 What is Peripheral Vascular Disease? 5 What Are Some of the Symptoms of Peripheral Vascular Disease? 6 What Causes Peripheral Vascular Disease? 7 How
Patient Information Table of Contents Introduction 3 What is Peripheral Vascular Disease? 5 What Are Some of the Symptoms of Peripheral Vascular Disease? 6 What Causes Peripheral Vascular Disease? 7 How
Dealing with Calcification in BTK Arteries: Is Lithoplasty the Answer?
 Dealing with Calcification in BTK Arteries: Is Lithoplasty the Answer? Andrew Holden, MBChB, FRANZCR, EBIR Director of Interventional Radiology Auckland, New Zealand LINC 2017 January 25 th 2017 Disclosure
Dealing with Calcification in BTK Arteries: Is Lithoplasty the Answer? Andrew Holden, MBChB, FRANZCR, EBIR Director of Interventional Radiology Auckland, New Zealand LINC 2017 January 25 th 2017 Disclosure
Hydrodynamic boost: a novel re-entry technique in subintimal angioplasty of below-the-knee vessels
 DOI 10.1007/s00330-015-4078-4 VASCULAR-INTERVENTIONAL Hydrodynamic boost: a novel re-entry technique in subintimal angioplasty of below-the-knee vessels Roberto Ferraresi 1 & Meneme Hamade 2 & Vito Gallicchio
DOI 10.1007/s00330-015-4078-4 VASCULAR-INTERVENTIONAL Hydrodynamic boost: a novel re-entry technique in subintimal angioplasty of below-the-knee vessels Roberto Ferraresi 1 & Meneme Hamade 2 & Vito Gallicchio
Endovascular Treatment of Aortoiliac Occlusive Disease: What s in My Toolbox in Jade S. Hiramoto, MD, MAS UCSF Vascular Symposium April 20, 2018
 Endovascular Treatment of Aortoiliac Occlusive Disease: What s in My Toolbox in 2018 Jade S. Hiramoto, MD, MAS UCSF Vascular Symposium April 20, 2018 Disclosures Research support and royalties, Cook Inc.
Endovascular Treatment of Aortoiliac Occlusive Disease: What s in My Toolbox in 2018 Jade S. Hiramoto, MD, MAS UCSF Vascular Symposium April 20, 2018 Disclosures Research support and royalties, Cook Inc.
Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
 Catheterization and Cardiovascular Interventions 78:395 399 (2011) Case Reports Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
Catheterization and Cardiovascular Interventions 78:395 399 (2011) Case Reports Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
TurboHawk. Plaque Excision System
 TurboHawk Plaque Excision System Twelve-month Patency in Diabetics DIABETICS VS. NON-DIABETICS 12-month Primary Patency (%) Diabetic patients show a more positive response to directional atherectomy than
TurboHawk Plaque Excision System Twelve-month Patency in Diabetics DIABETICS VS. NON-DIABETICS 12-month Primary Patency (%) Diabetic patients show a more positive response to directional atherectomy than
Superficial Femoral Artery Intervention: The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA
 : The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA Peripheral arterial disease (PAD) of the superficial femoral artery (SFA) is the most common cause of intermittent claudication
: The gift that keeps on giving! Wm. Britton Eaves,MD WKHSC Bossier City, LA Peripheral arterial disease (PAD) of the superficial femoral artery (SFA) is the most common cause of intermittent claudication
Limitations of the Outback LTD re-entry device in femoropopliteal chronic total occlusions
 From the Society for Clinical Vascular Surgery Limitations of the Outback LTD re-entry device in femoropopliteal chronic total occlusions Susanna H. Shin, MD, Donald Baril, MD, Rabih Chaer, MD, Robert
From the Society for Clinical Vascular Surgery Limitations of the Outback LTD re-entry device in femoropopliteal chronic total occlusions Susanna H. Shin, MD, Donald Baril, MD, Rabih Chaer, MD, Robert
Peripheal artery occlusive disease(from aorta to popliteal) 연세대학교의과대학 심장혈관병원최동훈
 연세대학교의과대학 심장혈관병원최동훈") Peripheal artery occlusive disease(from aorta to popliteal) 연세대학교의과대학 심장혈관병원최동훈 Case 1 Aorta disease -antegrade via brachial artery, subintimal approach, wire retraction, kissing stent- M / 59 # 4268376
Peripheal artery occlusive disease(from aorta to popliteal) 연세대학교의과대학 심장혈관병원최동훈 Case 1 Aorta disease -antegrade via brachial artery, subintimal approach, wire retraction, kissing stent- M / 59 # 4268376
An Extensive, Calcified CTO in the Superficial Femoral Artery
 WHAT WOULD YOU DO? An Extensive, Calcified CTO in the Superficial Femoral Artery MODERATOR: JOHN H. RUNDBACK, MD, FAHA, FSVM, FSIR PANEL: MICHAEL MILLER Jr, MD, FSIR; MIGUEL MONTERO-BAKER, MD; AND VINCENT
WHAT WOULD YOU DO? An Extensive, Calcified CTO in the Superficial Femoral Artery MODERATOR: JOHN H. RUNDBACK, MD, FAHA, FSVM, FSIR PANEL: MICHAEL MILLER Jr, MD, FSIR; MIGUEL MONTERO-BAKER, MD; AND VINCENT
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014
 PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
Elements of CTO PCI. Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center
 Elements of CTO PCI Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center Disclosures Consultant- Bridgepoint Medical Systems Speakers Honorarium- WL Gore Inc.
Elements of CTO PCI Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center Disclosures Consultant- Bridgepoint Medical Systems Speakers Honorarium- WL Gore Inc.
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Below-the-knee (BTK) targeted re-entry using the Outback catheter in subintimal angioplasty: Success rate and complications
 targeted re-entry using the Outback catheter in subintimal angioplasty: Success rate and complications") Below-the-knee (BTK) targeted re-entry using the Outback catheter in subintimal angioplasty: Success rate and complications Poster No.: C-0734 Congress: ECR 2016 Type: Scientific Exhibit Authors: S. M.
Below-the-knee (BTK) targeted re-entry using the Outback catheter in subintimal angioplasty: Success rate and complications Poster No.: C-0734 Congress: ECR 2016 Type: Scientific Exhibit Authors: S. M.
Quick Reference Guide
 Quick Reference Guide Indications for Use The AFX Endovascular AAA System is indicated for endovascular treatment in patients with AAA. The devices are indicated for patients with suitable aneurysm morphology
Quick Reference Guide Indications for Use The AFX Endovascular AAA System is indicated for endovascular treatment in patients with AAA. The devices are indicated for patients with suitable aneurysm morphology
Angioplasty Summit TCTAP Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D
 Angioplasty Summit TCTAP 2010 Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D Introduction CTO-PCI has been technically and technologically evolved over the past two
Angioplasty Summit TCTAP 2010 Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D Introduction CTO-PCI has been technically and technologically evolved over the past two
Ultrasound User Demonstration
 Ultrasound User Demonstration Disclaimer: This presentation is intended to be used as a demonstration educational device to showcase Terumo products. It is NOT intended to be used as a diagnostic device
Ultrasound User Demonstration Disclaimer: This presentation is intended to be used as a demonstration educational device to showcase Terumo products. It is NOT intended to be used as a diagnostic device
Retrograde Endovascular Revascularization of Anterior Tibial Artery via the Dorsal and Plantar Arches
 Case Reportc imedpub Journals www.imedpub.com Journal of Vascular and Endovascular Surgery DOI: 10.21767/2573-4482.100020 Retrograde Endovascular Revascularization of Anterior Tibial Artery via the Dorsal
Case Reportc imedpub Journals www.imedpub.com Journal of Vascular and Endovascular Surgery DOI: 10.21767/2573-4482.100020 Retrograde Endovascular Revascularization of Anterior Tibial Artery via the Dorsal
CTO: Technique and Tools
 CTO: Technique and Tools S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Associate Editor: Cath Cardiov Interventions UT
CTO: Technique and Tools S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Associate Editor: Cath Cardiov Interventions UT
How do I use mechanical debulking for the treatment of arterial occlusions
 How do I use mechanical debulking for the treatment of arterial occlusions Sven Bräunlich, MD Division of Interventional Angiology University-Hospital Leipzig, Germany Disclosure Speaker name: Sven Bräunlich
How do I use mechanical debulking for the treatment of arterial occlusions Sven Bräunlich, MD Division of Interventional Angiology University-Hospital Leipzig, Germany Disclosure Speaker name: Sven Bräunlich
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Interventional Radiology in Peripheral Vascular Disease: How Far Can We Go? Dr. L. F. CHENG Department of Radiology Princess Margaret Hospital
 Interventional Radiology in Peripheral Vascular Disease: How Far Can We Go? Dr. L. F. CHENG Department of Radiology Princess Margaret Hospital History The era of innovation in image-guided intervention
Interventional Radiology in Peripheral Vascular Disease: How Far Can We Go? Dr. L. F. CHENG Department of Radiology Princess Margaret Hospital History The era of innovation in image-guided intervention
Lessons learnt from DES in the SFA is there any ideal concept so far?
 Wednesday, January 25, 2017 - Time: 11:49-11:55 DEEP DIVE SESSION: Lower limb interventions (part II) Lessons learnt from DES in the SFA is there any ideal concept so far? S.Müller-Hülsbeck, MD, EBIR,
Wednesday, January 25, 2017 - Time: 11:49-11:55 DEEP DIVE SESSION: Lower limb interventions (part II) Lessons learnt from DES in the SFA is there any ideal concept so far? S.Müller-Hülsbeck, MD, EBIR,
Page 2 of 9
 OUTBACK LTD re-entry catheter in subintimal superficial femoral artery CTO revascularization: Preliminary data about procedure time, radioscopy time and precision in targeting the expected re-entry site
OUTBACK LTD re-entry catheter in subintimal superficial femoral artery CTO revascularization: Preliminary data about procedure time, radioscopy time and precision in targeting the expected re-entry site
PTA Balloon Dilatation Catheter
 PTA Balloon Dilatation Catheter March 2016 1/6(3214-0) Catalogue number Serial number Lot number Use by Do not reuse Do not resterilize Do not use if package is damaged Consult instructions for use Keep
PTA Balloon Dilatation Catheter March 2016 1/6(3214-0) Catalogue number Serial number Lot number Use by Do not reuse Do not resterilize Do not use if package is damaged Consult instructions for use Keep
Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD Toyohashi Heart Center, Japan
 Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD, Japan Retrograde Approach for Coronary CTO Collateral channels A. bypass graft B. epicardial collateral C. septal perforator Retrograde wiring techniques
Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD, Japan Retrograde Approach for Coronary CTO Collateral channels A. bypass graft B. epicardial collateral C. septal perforator Retrograde wiring techniques
Infrapopliteal endovascular intervention has become a
 Alternative Access for Tibial Intervention Techniques for treating challenging lesions. BY BRET N. WIECHMANN, MD Infrapopliteal endovascular intervention has become a first-line therapy for many patients
Alternative Access for Tibial Intervention Techniques for treating challenging lesions. BY BRET N. WIECHMANN, MD Infrapopliteal endovascular intervention has become a first-line therapy for many patients
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases
 Original paper Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases Sakir Arslan, Isa Oner Yuksel, Erkan Koklu, Goksel
Original paper Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases Sakir Arslan, Isa Oner Yuksel, Erkan Koklu, Goksel
Critical Limb Ischemia A Collaborative Approach to Patient Care. Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017
 Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Recanalization Techniques: Sharp Needle Recanalization. Recanalization Techniques: Sharp Needle Recanalization
 Recanalization of Occluded Central Veins When Conventional Methods Failed: Abigail Falk, MD, FSIR American Access Care New York, NY Conventional Methods of Recanalization Directional 0.035 and 0.018 Guidewires
Recanalization of Occluded Central Veins When Conventional Methods Failed: Abigail Falk, MD, FSIR American Access Care New York, NY Conventional Methods of Recanalization Directional 0.035 and 0.018 Guidewires
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
BTK Case Studies Joseph Cardenas, MD AZ Heart & Vascular, Yuma, AZ
 BTK Case Studies Joseph Cardenas, MD AZ Heart & Vascular, Yuma, AZ 1 Case 1 78 yr. old female Rutherford Class II/III lesion 1 block claudicant 2 Pre Treatment Post Treatment Anterior Tibial Artery Occlusion
BTK Case Studies Joseph Cardenas, MD AZ Heart & Vascular, Yuma, AZ 1 Case 1 78 yr. old female Rutherford Class II/III lesion 1 block claudicant 2 Pre Treatment Post Treatment Anterior Tibial Artery Occlusion
NCVH. What's New on the Vascular Horizons? Craig M. Walker, MD, FACC, FACP. New Cardiovascular Horizons
 What's New on the Vascular Horizons? NCVH New Cardiovascular Horizons KNOW YOUR OPTIONS Craig M. Walker, MD, FACC, FACP Clinical Professor of Medicine Tulane University School of Medicine New Orleans,
What's New on the Vascular Horizons? NCVH New Cardiovascular Horizons KNOW YOUR OPTIONS Craig M. Walker, MD, FACC, FACP Clinical Professor of Medicine Tulane University School of Medicine New Orleans,
Recent Advances in Peripheral Salvage
 Recent Advances in Peripheral Salvage Dr Shaiful Azmi Yahaya, MD, MMed, FNHAM, FAsCC, FAPSIC Consultant Cardiologist and Peripheral Interventionist, Institut Jantung Negara Disclosure I am proctoring for
Recent Advances in Peripheral Salvage Dr Shaiful Azmi Yahaya, MD, MMed, FNHAM, FAsCC, FAPSIC Consultant Cardiologist and Peripheral Interventionist, Institut Jantung Negara Disclosure I am proctoring for
Drug- Coated Balloons for the SFA: Overview of Technology and Results
 Drug- Coated Balloons for the SFA: Overview of Technology and Results NCVH Latin American 2015 Bogota, Colombia April 9-11, 2015 Brian G. DeRubertis, M.D. Associate Professor of Surgery Division of Vascular
Drug- Coated Balloons for the SFA: Overview of Technology and Results NCVH Latin American 2015 Bogota, Colombia April 9-11, 2015 Brian G. DeRubertis, M.D. Associate Professor of Surgery Division of Vascular
Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data)
") Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data) (Angiolite BTK DES, IVascular) P. Goverde MD, K. Taeymans MD, K. Lauwers MD Vascular Clinic ZNA Antwerp,Belgium
Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data) (Angiolite BTK DES, IVascular) P. Goverde MD, K. Taeymans MD, K. Lauwers MD Vascular Clinic ZNA Antwerp,Belgium