Anal Sphincter Injuries: Acute Management
|
|
|
- Morgan Warner
- 6 years ago
- Views:
Transcription
1 Anal Sphincter Injuries: Acute Management Dr Stephen Jeffery Urogynaecology Consultant Department of Obstetrics & Gynaecology Groote Schuur Hospital

2 Colorectal Surgeons Gynaecologists
3 Gynaecologists Colorectal Surgeons
4
5 Audit Ø Do you routinely perform an epiotomy when doing an instrumental delivery? l Yes 5 (27%) l No 13 (73%)
6 Audit Ø Who supervised your first episiotomy repair? l Midwife 10 (55%) l MO 2 (11%) l Registrar 5 (27%) l Consultant 1 (6%)
 l MO 1 (6%) l Registrar 14 (77%) l Consultant 2")
7 Audit Ø Who supervised your first third degree tear repair? l Midwife 1 (6%) l MO 1 (6%) l Registrar 14 (77%) l Consultant 2 (11%)
8 Audit Ø Classification l 3A & 3B 5 (28%) l 3A, 3B, 3C 6 (33%) l 3A, 3B, 3C, 3D 3 (17%) l Don t know 3 (17%)
9 Background Diagnosed clinically at time of delivery in 0.6-9% of cases Two-thirds of registrars and consultants in the UK have expressed a lack of or unsatisfactory training in the management of OASI. Adams et al Guideline No. 29 London, UK: RCOG; 200I Fernando et al. BMC Health Services Research. 2002, 2:9
10 Most common causes of complaint and litigation arising in labour ward practice Fetal death or injury as a consequence of: o Mismanagement of labour o Failure to recognise CTG abnormalities and act on them o Mismanagement of operative vaginal delivery or shoulder dystocia Maternal injury as a consequence of o o Failure to recognise injury to the anal sphincter and repair it Rupture of the uterus Clements RV. Risk Management and Litigation in Obstetrics and Gynaecology 2001 p240
11 Most common causes of complaint and litigation arising in labour ward practice Fetal death or injury as a consequence of: o Mismanagement of labour o Failure to recognise CTG abnormalities and act on them o Mismanagement of operative vaginal delivery or shoulder dystocia Maternal injury as a consequence of o o Failure to recognise injury to the anal sphincter and repair it Rupture of the uterus Clements RV. Risk Management and Litigation in Obstetrics and Gynaecology 2001 p240
12 Nomenclature Every obstetric text in RCOG library (Sultan and Thakar) o o 17% no mention of classification 22% classified anal sphincter injury as second degree BMC Health Services Research (2002) o o 672 practicing Consultant obstetricians 33% classified Complete or Partial external sphincter tear as Second Degree



13 Classification of Perineal Lacerations Ø First Degree l Laceration of the vaginal epithelium or perineal skin only Ø Second Degree l Involvement of the vaginal epithelium, perineal skin and muscles but not the anal sphincter
14 Classification of Perineal Lacerations Ø Third degree l Disruption of the vaginal epithelium, perineal skin, perineal body & internal anal sphincter (IAS) &/or external anal sphincter (EAS) l 3a: <50% EAS torn 3b: >50% EAS torn 3c: IAS torn
 without the involvement of the anal sphincter is rare & not included in this")
15 Classification of Perineal Lacerations Ø Fourth Degree l Extension into the rectal mucosa l Rectal mucosal tear (buttonhole) without the involvement of the anal sphincter is rare & not included in this classification



16 Risk Factors for Sphincter Injury Ø Forceps Ø Primiparity Ø Large fetus (>4kg) Ø Shoulder dystocia Ø Persistant OP position

17 Risk Factors for Sphincter Injury
18 Risk Factors for Sphincter Injury N= 5044 SVD 4.2% sphincter defect Univariate analysis low parity prolonged 1 st and 2 nd stage high birth weight episiotomy forceps Hudelist et al. Am J Obstet Gynecol 2005; 192(3):875-81
19 Risk Factors for Sphincter Injury N= 5044 SVD 4.2% sphincter defect Univariate analysis low parity prolonged 1 st and 2 nd stage high birth weight episiotomy forceps Multivariate analysis Hudelist et al. Am J Obstet Gynecol 2005; 192(3):875-81
20 Risk Factors for Sphincter Injury Occipitoposterior Position n = 393 Occipitoanterior OASI 22% Occipitoposterior OASI 46% Odds ratio 2.5 ( ) Logistic Regression Analysis BMI race nulliparity second stage length episiotomy Birth weight HC OP four X higher chance of sphincter injury Wu JM etal. Am J Obstet Gynecol 2005, 193(2):
21 Recognition of Obstetric Anal Sphincter Injury (OASI) All Vaginal deliveries o Systematic examination of perineum and vagina to assess severity of trauma o Rectal examination if episiotomy or any tear Instrumental Delivery or Extensive Perineal Injury (esp those that extend to anal verge) o Examined by an experienced obstetrician trained in the recognition and management of perineal tears RCOG guidelines July 2001

22 Technique of anal sphincter closure 1.End-to-end 2. Overlap
23 Technique of repair OASI Considerable variation in management Coloproctologist Obstetric Consultants End to end 11.1% 47% 35% Overlap 88% 50% 55% Obstetric Trainees Don t know 2.1% 8.8% Fernando et al. BMC Health Services Research. 2002, 2:9
24 Technique of repair OASI Up to studies (n= 2000) no faecal incontinence!!!! Sultan and Thakar (2002) o 20 studies since 1982 o 37% (15-59%) mean prevalence of incontinence following primary repair Sultan AH, Thakar R. Bailiere s Best Pract Res Clin Obstet Gynecol; 2002: 16,
25 Technique of repair OASI Up to studies (n= 2000) no faecal incontinence!!!! Sultan and Thakar (2002) o 20 studies since 1982 o 37% (15-59%) mean prevalence of incontinence following primary repair Sultan AH, Thakar R. Bailiere s Best Pract Res Clin Obstet Gynecol; 2002: 16,
26 Technique of repair OASI Overlap Technique o Favoured by colorectal surgeons o 21 Prospective Studies o Secondary repair % success o Poorer 5 year outcomes of about 50% Jorge and Wexner. Dis Colon Rectum 1993;36:77-97
27 Technique of repair OASI Overlap Technique for Primary Repair o Pilot study (matched controls) o Described additional repair of IAS o Reduction in incontinence from 41% to 8% o Possibly operator influence??? Sultan et al. Br J Obstet Gynaecol 1999; 106:
28 Technique of repair OASI Overlap Technique for Primary Repair o RCT (Fitzpatrick et al) o 112 primiparas o No difference between groups o No separate IAS repair Fitzpatrick et al. Am J Obstet Gynecol 2000; 183:



29 Technique of repair OASI: Which Method? Fernando et al. o RCT, n=64, 1 year follow up o Only 3b, 3c, 4 th degree tears End-to-end Overlap Faecal Incontinence 24% 0 p=0.009 Faecal Urgency 32% 3.7% p=0.02 Dyspareunia Equal Equal QOL Equal Equal Perineal Pain 20% 0% p=0.04 Fernando et al. Obstet Gynecol 2006; 107:1261-6
30 Methods of repair for obstetric anal sphincter injury R Fernando, AH Sultan, C Kettle, R Thakar, S Radley Cochrane Database of Systematic Reviews 2006 Issue 3 (Status: New) Copyright 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd / CD pub2 This version first published online: 19 July 2006 in Issue 3, 2006 Date of Most Recent Substantive Amendment: 7 April 2006 Objectives To compare the effectiveness of overlap repair versus end-to-end repair following OASIS in reducing subsequent anal incontinence, perineal pain, dyspareunia and improving quality of life.
31 Main results Three eligible trials, of grade A quality, involving 279 women, were included. There was considerable heterogeneity in the outcome measures, time points and reported results. Meta-analyses showed that there was no statistically significant difference in perineal pain (relative risk (RR) 0.08, 95% confidence interval (CI) 0.00 to 1.45, one trial, 52 women), dyspareunia (RR 0.62, 95% CI 0.11 to 3.39, one trial, 52 women), flatus incontinence (RR 0.93, 95% CI 0.26 to 3.31, one trial, 52 women) and faecal incontinence (RR 0.07, 95% CI 0.00 to 1.21, one trial, 52 women) between the two repair techniques at 12 months but showed a statistically significantly lower incidence in faecal urgency (RR 0.12, 95% CI 0.02 to 0.86, one trial, 52 women) and lower anal incontinence score (weighted mean difference -1.70, 95% CI to -0.37) in the overlap group. Overlap technique was also associated with a statistically significant lower risk of deterioration of anal incontinence symptoms over 12 months (RR 0.26, 95% CI 0.09 to 0.79, one trial, 41 women). There was no significant difference in quality of life
32 Main results Three eligible trials, of grade A quality, involving 279 women, were included. There was considerable heterogeneity in the outcome measures, time points and reported results. Meta-analyses showed that there was no statistically significant difference in perineal pain (relative risk (RR) 0.08, 95% confidence interval (CI) 0.00 to 1.45, one trial, 52 women), dyspareunia (RR 0.62, 95% CI 0.11 to 3.39, one trial, 52 women), flatus incontinence (RR 0.93, 95% CI 0.26 to 3.31, one trial, 52 women) and faecal incontinence (RR 0.07, 95% CI 0.00 to 1.21, one trial, 52 women) between the two repair techniques at 12 months but showed a statistically significantly lower incidence in faecal urgency (RR 0.12, 95% CI 0.02 to 0.86, one trial, 52 women) and lower anal incontinence score (weighted mean difference -1.70, 95% CI to -0.37) in the overlap group. Overlap technique was also associated with a statistically significant lower risk of deterioration of anal incontinence symptoms over 12 months (RR 0.26, 95% CI 0.09 to 0.79, one trial, 41 women). There was no significant difference in quality of life
33 Main results Three eligible trials, of grade A quality, involving 279 women, were included. There was considerable heterogeneity in the outcome measures, time points and reported results. Meta-analyses showed that there was no statistically significant difference in perineal pain (relative risk (RR) 0.08, 95% confidence interval (CI) 0.00 to 1.45, one trial, 52 women), dyspareunia (RR 0.62, 95% CI 0.11 to 3.39, one trial, 52 women), flatus incontinence (RR 0.93, 95% CI 0.26 to 3.31, one trial, 52 women) and faecal incontinence (RR 0.07, 95% CI 0.00 to 1.21, one trial, 52 women) between the two repair techniques at 12 months but showed a statistically significantly lower incidence in faecal urgency (RR 0.12, 95% CI 0.02 to 0.86, one trial, 52 women) and lower anal incontinence score (weighted mean difference -1.70, 95% CI to -0.37) in the overlap group. Overlap technique was also associated with a statistically significant lower risk of deterioration of anal incontinence symptoms over 12 months (RR 0.26, 95% CI 0.09 to 0.79, one trial, 41 women). There was no significant difference in quality of life
34 Main results Three eligible trials, of grade A quality, involving 279 women, were included. There was considerable heterogeneity in the outcome measures, time points and reported results. Meta-analyses showed that there was no statistically significant difference in perineal pain (relative risk (RR) 0.08, 95% confidence interval (CI) 0.00 to 1.45, one trial, 52 women), dyspareunia (RR 0.62, 95% CI 0.11 to 3.39, one trial, 52 women), flatus incontinence (RR 0.93, 95% CI 0.26 to 3.31, one trial, 52 women) and faecal incontinence (RR 0.07, 95% CI 0.00 to 1.21, one trial, 52 women) between the two repair techniques at 12 months but showed a statistically significantly lower incidence in faecal urgency (RR 0.12, 95% CI 0.02 to 0.86, one trial, 52 women) and lower anal incontinence score (weighted mean difference -1.70, 95% CI to -0.37) in the overlap group. Overlap technique was also associated with a statistically significant lower risk of deterioration of anal incontinence symptoms over 12 months (RR 0.26, 95% CI 0.09 to 0.79, one trial, 41 women). There was no significant difference in quality of life
35 Main results Three eligible trials, of grade A quality, involving 279 women, were included. There was considerable heterogeneity in the outcome measures, time points and reported results. Meta-analyses showed that there was no statistically significant difference in perineal pain (relative risk (RR) 0.08, 95% confidence interval (CI) 0.00 to 1.45, one trial, 52 women), dyspareunia (RR 0.62, 95% CI 0.11 to 3.39, one trial, 52 women), flatus incontinence (RR 0.93, 95% CI 0.26 to 3.31, one trial, 52 women) and faecal incontinence (RR 0.07, 95% CI 0.00 to 1.21, one trial, 52 women) between the two repair techniques at 12 months but showed a statistically significantly lower incidence in faecal urgency (RR 0.12, 95% CI 0.02 to 0.86, one trial, 52 women) and lower anal incontinence score (weighted mean difference -1.70, 95% CI to -0.37) in the overlap group. Overlap technique was also associated with a statistically significant lower risk of deterioration of anal incontinence symptoms over 12 months (RR 0.26, 95% CI 0.09 to 0.79, one trial, 41 women). There was no significant difference in quality of life
36 Authors' conclusions The limited data available show that compared to immediate primary end-toend repair of OASIS, early primary overlap repair appears to be associated with lower risks for faecal urgency and anal incontinence symptoms. As the experience of the surgeon is not addressed in the three studies reviewed, it would be inappropriate to recommend one type of repair in favour of another
37 Technique of repair OASI GUIDELINES (Sultan et al) 1. Performed by an experienced operator 2. Operating theatre 3. GA or Spinal 4. Grade injury 5. Anal epithelium repaired with Vicryl 3/0 or Vicryl rapide 6. Sphincters with 3/0 PDS 7. IAS end to end Andrews, Sultan and Thakar. Reviews in Gynaecological Practice.
38 Technique of repair OASI: GUIDELINES (Sultan et al) 8. External Sphincter End to End Grasp ends with Allis forceps Figure 8 Andrews, Sultan and Thakar. Reviews in Gynaecological Practice.
39 End-to-end repair
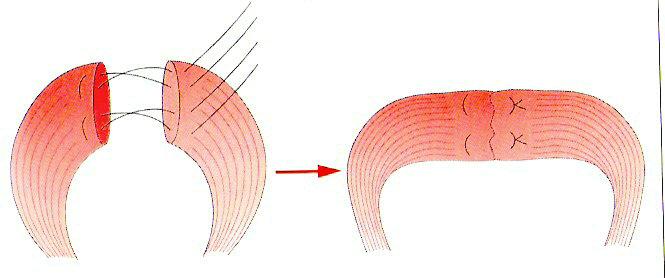
40 Technique of repair OASI GUIDELINES (Sultan et al) 8. External Sphincter Overlap Grasp ends with Allis forceps Mobilisation and dissection from ishcio-anal fat laterally Full width of muscle identified Double breast overlap technique Andrews, Sultan and Thakar. Reviews in Gynaecological Practice.

41 Overlap repair
42
43
44
45 Technique of repair OASI GUIDELINES (Sultan et al) 9. Rectovaginal exam 10. IV antibiotics 11. Foley catheter 24 hrs 12. Detailed notes 13. Laxatives 14. EXPLAIN & DEBRIEF Andrews, Sultan and Thakar. Reviews in Gynaecological Practice.
46 RCT : Diagnosis of anal sphincter tears using U/S N= 752 (not clinically evident sphincter injury) Randomised to scan /no scan With u/s 5.6% injury Outcome = faecal 3 /12 - ultrasound group 3.3% - no ultrasound group 8.7% 1 year - ultrasound group 3.2% - no ultrasound group 6.7% (p=0.03) NNT =29 Faltin DL et al. Obstet Gynecol 2005, 106(1): 61-13
47 Postnatal Care RCT: Laxatives vs Laxatives + Bulking agents (n=i47) o Lactulose alone or Lactulose + Fybogel o Similar pain score o Incontinence in immediate post natal period: o One agent I8% o Two agents 32% p=0.03 Eogan et al. BJOG 2007;II4:

48 The bottom line


49 Who Should all acute tears be repaired by colorectal surgeons? Ø Not shown to have better outcomes Ø Fernando et al l l l 60% had never performed an acute tear 30% had performed <5 in a year Only 19% felt that they should be involved in the acute management of OASI Fernando et al. BMC Health Services Research. 2002, 2:9
50 Occult anal sphincter injury and previous repair o o o Prospective cohort study 100 women with vaginal delivery of 1 st child Incontinence of flatus & stool at 3 & 30 months ASD 2 nd delivery Incontinent (%) RR (95% CI) No No 1/129 (3) 1 No Yes Yes No 1/10(10) 4/25 (16) Yes Yes 5/13 (38) 11.2 Faltin et al (2001)
51 Thank you
Appendix B Protocol for management of obstetric anal sphincter injury THE MANAGEMENT OF THIRD- AND FOURTH-DEGREE PERINEAL TEARS
 Appendix B Protocol for management of obstetric anal sphincter injury Document Type: THE MANAGEMENT OF THIRD- AND FOURTH-DEGREE PERINEAL TEARS PURPOSE & SCOPE To provide a guideline that will assist in
Appendix B Protocol for management of obstetric anal sphincter injury Document Type: THE MANAGEMENT OF THIRD- AND FOURTH-DEGREE PERINEAL TEARS PURPOSE & SCOPE To provide a guideline that will assist in
Obstetric Anal Sphincter Injury- A guideline. Mr David Sim Ms Patricia McStay. Dr Martina Hogan Dept./Division Only: YES-IMWH Directorate Only: NO
 CLINICAL GUIDELINES ID TAG Title: Obstetric Anal Sphincter Injury- A guideline Author: Dr Foteini Verani Designation: Specialist Doctor Speciality / Division: Obstetrics-IMWH Directorate: Acute Services
CLINICAL GUIDELINES ID TAG Title: Obstetric Anal Sphincter Injury- A guideline Author: Dr Foteini Verani Designation: Specialist Doctor Speciality / Division: Obstetrics-IMWH Directorate: Acute Services
Obstetric Anal Sphincter Injury. An update on best practices. Objectives
 Obstetric Anal Sphincter Injury An update on best practices Erin Crosby MD Assistant Professor Department of OB/Gyn Division of FPMRS 1 Objectives Describe the anatomy of the anal sphincter complex Discuss
Obstetric Anal Sphincter Injury An update on best practices Erin Crosby MD Assistant Professor Department of OB/Gyn Division of FPMRS 1 Objectives Describe the anatomy of the anal sphincter complex Discuss
The Perineal Clinic: - the management of women following OASI
 The Perineal Clinic: - the management of women following OASI Miss Gillian Fowler Consultant Urogynaecologist MBChB, MD, MRCOG Liverpool Women s Hospital. Margie Polden University Memorial of Liverpool
The Perineal Clinic: - the management of women following OASI Miss Gillian Fowler Consultant Urogynaecologist MBChB, MD, MRCOG Liverpool Women s Hospital. Margie Polden University Memorial of Liverpool
Dr Anne Sneddon Director of Obstetrics and Gynaecology Lecturer, ANU Medical School The Canberra Hospital
 Dr Anne Sneddon Director of Obstetrics and Gynaecology Lecturer, ANU Medical School The Canberra Hospital Capital city of Australia Population 350,000 but surrounding region of 500,000 Seat of government
Dr Anne Sneddon Director of Obstetrics and Gynaecology Lecturer, ANU Medical School The Canberra Hospital Capital city of Australia Population 350,000 but surrounding region of 500,000 Seat of government
EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May Dr. Annie Leong MBBS, FRANZCOG, CU
 EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May 2011 Dr. Annie Leong MBBS, FRANZCOG, CU Restore normal perineal anatomy Achieve good haemostasis Avoid infection and wound breakdown Avoid coital
EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May 2011 Dr. Annie Leong MBBS, FRANZCOG, CU Restore normal perineal anatomy Achieve good haemostasis Avoid infection and wound breakdown Avoid coital
Third & Fourth Degree Tears guideline (GL926)
") Third & Fourth Degree Tears guideline (GL926) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Chair, Maternity Clinical Governance
Third & Fourth Degree Tears guideline (GL926) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Chair, Maternity Clinical Governance
Clinical Guideline for: The Management of Perineal Trauma following Childbirth
 For Use in: By: For: Division responsible for document: Key words: Name of document author: Job title of document author: Name of document author s Line Manager: Job title of author s Line Manager: Supported
For Use in: By: For: Division responsible for document: Key words: Name of document author: Job title of document author: Name of document author s Line Manager: Job title of author s Line Manager: Supported
Vincent Letouzey, MD, PhD
 How to protect the perineum and prevent obstetric perineal trauma Standards of OASIS diagnosis: Primary (clinical) and Secondary (ultrasound) Vincent Letouzey, MD, PhD Obst/Gyne Dept Nîmes University Hospital
How to protect the perineum and prevent obstetric perineal trauma Standards of OASIS diagnosis: Primary (clinical) and Secondary (ultrasound) Vincent Letouzey, MD, PhD Obst/Gyne Dept Nîmes University Hospital
Risk factors and management of obstetric perineal injury
 Risk factors and management of obstetric perineal injury Ruwan J Fernando Abstract Perineal injury sustained during childbirth is a major aetiological factor in the development of perineal pain, sexual
Risk factors and management of obstetric perineal injury Ruwan J Fernando Abstract Perineal injury sustained during childbirth is a major aetiological factor in the development of perineal pain, sexual
Hands-on Workshop. Cape Town, South Africa 3 August Chairpersons
 Hands-on Workshop www.perineum.net Cape Town, South Africa 3 August 2016 Chairpersons Mr Abdul H Sultan, MB.ChB (Natal), MD, FRCOG Consultant Obstetrician & Urogynaecologist Miss Ranee Thakar, MB.BS, MD,
Hands-on Workshop www.perineum.net Cape Town, South Africa 3 August 2016 Chairpersons Mr Abdul H Sultan, MB.ChB (Natal), MD, FRCOG Consultant Obstetrician & Urogynaecologist Miss Ranee Thakar, MB.BS, MD,
Secondary Repair of Third Degree Perineal Tear Leading to Fecal Incontinence in 2 Cases
 CASE REPORT Secondary Repair of Third Degree Perineal Tear Leading to Fecal Incontinence in 2 Cases Vasant Kawade 1 and Abhijit Ambike 2 Professor and Head, Department of OBGY, B.K.L.Walawakarl Rural Medical
CASE REPORT Secondary Repair of Third Degree Perineal Tear Leading to Fecal Incontinence in 2 Cases Vasant Kawade 1 and Abhijit Ambike 2 Professor and Head, Department of OBGY, B.K.L.Walawakarl Rural Medical
Royal College of Obstetricians and Gynaecologists
 Royal College of Obstetricians and Gynaecologists Consent Advice No. 9 June 2010 REPAIR OF THIRD- AND FOURTH-DEGREE PERINEAL TEARS FOLLOWING CHILDBIRTH This is the first edition of this guidance. This
Royal College of Obstetricians and Gynaecologists Consent Advice No. 9 June 2010 REPAIR OF THIRD- AND FOURTH-DEGREE PERINEAL TEARS FOLLOWING CHILDBIRTH This is the first edition of this guidance. This
Repair of vaginal tears and episiotomy guidelines
 Repair of vaginal tears and episiotomy guidelines Purpose These guidelines assist practitioners in the repair of vaginal and perineal tears including the reasons for, and the techniques of performing an
Repair of vaginal tears and episiotomy guidelines Purpose These guidelines assist practitioners in the repair of vaginal and perineal tears including the reasons for, and the techniques of performing an
Occult anal sphincter injuries myth or reality?
 DOI: 10.1111/j.1471-0528.2006.00799.x www.blackwellpublishing.com/bjog Intrapartum care Occult anal sphincter injuries myth or reality? Vasanth Andrews, a Abdul H Sultan, a Ranee Thakar, a Peter W Jones
DOI: 10.1111/j.1471-0528.2006.00799.x www.blackwellpublishing.com/bjog Intrapartum care Occult anal sphincter injuries myth or reality? Vasanth Andrews, a Abdul H Sultan, a Ranee Thakar, a Peter W Jones
OBSTETRICALLY-CAUSED ANAL SPHINCTER INJURY PREDICTION, MANAGEMENT, PREVENTION
 OBSTETRICALLY-CAUSED ANAL SPHINCTER INJURY PREDICTION, MANAGEMENT, PREVENTION COLM O HERLIHY, MD Professor and Chair University College Dublin Department of Obstetrics and Gynaecology National Maternity
OBSTETRICALLY-CAUSED ANAL SPHINCTER INJURY PREDICTION, MANAGEMENT, PREVENTION COLM O HERLIHY, MD Professor and Chair University College Dublin Department of Obstetrics and Gynaecology National Maternity
Childbirth Trauma & Its Complications 23/ Mr Stergios K. Doumouchtsis
 Mr Stergios K. Doumouchtsis Consultant Obstetrician Gynaecologist & Urogynaecologist Childbirth Trauma & Its Complications Over eighty per cent of women sustain some degree of perineal trauma during childbirth.
Mr Stergios K. Doumouchtsis Consultant Obstetrician Gynaecologist & Urogynaecologist Childbirth Trauma & Its Complications Over eighty per cent of women sustain some degree of perineal trauma during childbirth.
How to repair an anal sphincter injury after vaginal delivery: results of a randomised controlled trial
 DOI: 10.1111/j.1471-0528.2006.00806.x www.blackwellpublishing.com/bjog Intrapartum care How to repair an anal sphincter injury after vaginal delivery: results of a randomised controlled trial Abimbola
DOI: 10.1111/j.1471-0528.2006.00806.x www.blackwellpublishing.com/bjog Intrapartum care How to repair an anal sphincter injury after vaginal delivery: results of a randomised controlled trial Abimbola
Title: A modified surgical approach to women with obstetric anal sphincter tears
 Reviewer's report Title: A modified surgical approach to women with obstetric anal sphincter tears Version: 3 Date: 27 January 2010 Reviewer: Stig S Norderval Reviewer's report: Review on manuscript entitled:
Reviewer's report Title: A modified surgical approach to women with obstetric anal sphincter tears Version: 3 Date: 27 January 2010 Reviewer: Stig S Norderval Reviewer's report: Review on manuscript entitled:
Postpartum Complications
 ACOG Postpartum Toolkit Postpartum Complications Introduction The effects of pregnancy on many organ systems begin to resolve spontaneously after birth of the infant and delivery of the placenta. The timeline
ACOG Postpartum Toolkit Postpartum Complications Introduction The effects of pregnancy on many organ systems begin to resolve spontaneously after birth of the infant and delivery of the placenta. The timeline
Obstetrical Anal Sphincter Injuries (OASIS): Prevention, Recognition, and Repair
: Prevention, Recognition, and Repair") SOGC CLINICAL PRACTICE GUIDELINE No. 330, December 2015 Obstetrical Anal Sphincter Injuries (OASIS): Prevention, Recognition, and Repair This clinical practice guideline has been prepared by the Urogynaecology
SOGC CLINICAL PRACTICE GUIDELINE No. 330, December 2015 Obstetrical Anal Sphincter Injuries (OASIS): Prevention, Recognition, and Repair This clinical practice guideline has been prepared by the Urogynaecology
Guideline for Management and Repair of Perineal Trauma
 Guideline for Management and Repair of Perineal Trauma Author: Labour Ward Forum Specialty: Maternity Date Approved: September 2014 Approved by: W&CH Clinical Governance Committee Date for Review: August
Guideline for Management and Repair of Perineal Trauma Author: Labour Ward Forum Specialty: Maternity Date Approved: September 2014 Approved by: W&CH Clinical Governance Committee Date for Review: August
Obstetric anal sphincter injury is the most common
 Repair Techniques for Obstetric Anal Sphincter Injuries A Randomized Controlled Trial Ruwan J. Fernando, MD, MRCOG, Abdul H. Sultan, MD, FRCOG, Christine Kettle, PhD, Simon Radley, MD, FRCS, Peter Jones,
Repair Techniques for Obstetric Anal Sphincter Injuries A Randomized Controlled Trial Ruwan J. Fernando, MD, MRCOG, Abdul H. Sultan, MD, FRCOG, Christine Kettle, PhD, Simon Radley, MD, FRCS, Peter Jones,
Immediate or delayed repair of obstetric anal sphincter tears a randomised controlled trial*
 DOI: 10.1111/j.1471-0528.2008.01726.x www.blackwellpublishing.com/bjog General obstetrics Immediate or delayed repair of obstetric anal sphincter tears a randomised controlled trial* J Nordenstam, a,b
DOI: 10.1111/j.1471-0528.2008.01726.x www.blackwellpublishing.com/bjog General obstetrics Immediate or delayed repair of obstetric anal sphincter tears a randomised controlled trial* J Nordenstam, a,b
2/5/2016. Evolving Surgical Treatment Approaches for Fecal Incontinence in Women: An Evidence and Cased-Based Approach
 Evolving Surgical Treatment Approaches for Fecal Incontinence in Women: An Evidence and Cased-Based Approach Holly E Richter, PhD, MD, FACOG, FACS J Marion Sims Professor Obstetrics and Gynecology Professor
Evolving Surgical Treatment Approaches for Fecal Incontinence in Women: An Evidence and Cased-Based Approach Holly E Richter, PhD, MD, FACOG, FACS J Marion Sims Professor Obstetrics and Gynecology Professor
Effect of subsequent vaginal delivery on bowel symptoms and anorectal function in women who sustained a previous obstetric anal sphincter injury
 International Urogynecology Journal (2018) 29:1579 1588 https://doi.org/10.1007/s00192-018-3601-y ORIGINAL ARTICLE Effect of subsequent vaginal delivery on bowel symptoms and anorectal function in women
International Urogynecology Journal (2018) 29:1579 1588 https://doi.org/10.1007/s00192-018-3601-y ORIGINAL ARTICLE Effect of subsequent vaginal delivery on bowel symptoms and anorectal function in women
Urinary incontinence after obstetric anal sphincter injuries (OASIS) is there a relationship?
 is there a relationship?") DOI 10.1007/s00192-007-0431-8 ORIGINAL ARTICLE Urinary incontinence after obstetric anal sphincter injuries (OASIS) is there a relationship? Inka Scheer & Vasanth Andrews & Ranee Thakar & Abdul H. Sultan
DOI 10.1007/s00192-007-0431-8 ORIGINAL ARTICLE Urinary incontinence after obstetric anal sphincter injuries (OASIS) is there a relationship? Inka Scheer & Vasanth Andrews & Ranee Thakar & Abdul H. Sultan
Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF)
") Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF) Blair B. Washington MD, MHA Urogynecology & Reconstructive Pelvic Surgery Virginia Mason Medical Center Disclosures
Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF) Blair B. Washington MD, MHA Urogynecology & Reconstructive Pelvic Surgery Virginia Mason Medical Center Disclosures
Long-term ailments due to anal sphincter rupture caused by delivery - a hidden problem
 Eur. J. Obstet. Gynecol. Reprod. Biol., 27 (1988) 27-32 Elsevier 27 EJO 00556 Long-term ailments due to anal sphincter rupture caused by delivery - a hidden problem Knut Haadem, Sten Ohrlander and G6ran
Eur. J. Obstet. Gynecol. Reprod. Biol., 27 (1988) 27-32 Elsevier 27 EJO 00556 Long-term ailments due to anal sphincter rupture caused by delivery - a hidden problem Knut Haadem, Sten Ohrlander and G6ran
THE PELVIC FLOOR, EPISIOTOMY AND PERINEAL REPAIR AND VAGINAL/RECTAL MEDICATIONS
 THE PELVIC FLOOR, EPISIOTOMY AND PERINEAL REPAIR AND VAGINAL/RECTAL MEDICATIONS MID2010 LEARNING OBJECTIVE 1 - REVIEW THE ANATOMY OF THE PELVIC FLOOR Superficial layers cavernosus Deep layer Coccygeus
THE PELVIC FLOOR, EPISIOTOMY AND PERINEAL REPAIR AND VAGINAL/RECTAL MEDICATIONS MID2010 LEARNING OBJECTIVE 1 - REVIEW THE ANATOMY OF THE PELVIC FLOOR Superficial layers cavernosus Deep layer Coccygeus
Doctor s assessment and evaluation of the pelvic floor in antenatal and postpartum women: routine or???
 Doctor s assessment and evaluation of the pelvic floor in antenatal and postpartum women: routine or??? Dr Barry O Reilly Head of department of Urogynaecology Cork University Maternity Hospital Ireland
Doctor s assessment and evaluation of the pelvic floor in antenatal and postpartum women: routine or??? Dr Barry O Reilly Head of department of Urogynaecology Cork University Maternity Hospital Ireland
AN INTERNATIONAL CONTINENCE SOCIETY (ICS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR CHILDBIRTH TRAUMA
 / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR CHILDBIRTH TRAUMA") AN INTERNATIONAL CONTINENCE SOCIETY (ICS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR CHILDBIRTH TRAUMA NEED FOR A WORKING GROUP ON CHILDBIRTH TRAUMA A: Background
AN INTERNATIONAL CONTINENCE SOCIETY (ICS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR CHILDBIRTH TRAUMA NEED FOR A WORKING GROUP ON CHILDBIRTH TRAUMA A: Background
Anal Incontinence After Vaginal Delivery: A Five-Year Prospective Cohort Study
 ORIGINAL RESEARCH Anal Incontinence After Vaginal Delivery: A Five-Year Prospective Cohort Study Johan Pollack, MD, Johan Nordenstam, MD, Sophia Brismar, MD, Annika Lopez, MD, PhD, Daniel Altman, MD, and
ORIGINAL RESEARCH Anal Incontinence After Vaginal Delivery: A Five-Year Prospective Cohort Study Johan Pollack, MD, Johan Nordenstam, MD, Sophia Brismar, MD, Annika Lopez, MD, PhD, Daniel Altman, MD, and
2/25/2013. Speaker Disclosure. Learning Objectives. Ob/Gyn Conference Series: Urinary and Fecal Incontinence After Vaginal Childbirth
 Ob/Gyn Conference Series: Urinary and Fecal Incontinence After Vaginal Childbirth Jaime Sepulveda-Toro MD FACS FACOG Female Pelvic Medicine and Reconstructive Pelvic Surgery South Miami Hospital Speaker
Ob/Gyn Conference Series: Urinary and Fecal Incontinence After Vaginal Childbirth Jaime Sepulveda-Toro MD FACS FACOG Female Pelvic Medicine and Reconstructive Pelvic Surgery South Miami Hospital Speaker
Repair of Perineal trauma, including 3 rd and 4 th degree tear
 MATERNITY GUIDELINES Repair of Perineal trauma, including 3 rd and 4 th degree tear Navigation Guidance document in the contents page the Press Ctrl on your keyboard and click on a heading to navigate
MATERNITY GUIDELINES Repair of Perineal trauma, including 3 rd and 4 th degree tear Navigation Guidance document in the contents page the Press Ctrl on your keyboard and click on a heading to navigate
Pregnancy and childbirth: the effects on pelvic floor muscles
 Page 1 of 9 Pregnancy and childbirth: the effects on pelvic floor muscles 26 February, 2009 Stress incontinence can follow childbirth as pelvic floor muscles are damaged AUTHOR Julia Herbert, MSc, MCSP,
Page 1 of 9 Pregnancy and childbirth: the effects on pelvic floor muscles 26 February, 2009 Stress incontinence can follow childbirth as pelvic floor muscles are damaged AUTHOR Julia Herbert, MSc, MCSP,
anal incontinence; endoanal ultrasonography; grading systems; obstetric sphincter tears; three-dimensional
 Ultrasound Obstet Gynecol 2012; 40: 207 214 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.10154 Incontinence after primary repair of obstetric anal sphincter tears
Ultrasound Obstet Gynecol 2012; 40: 207 214 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.10154 Incontinence after primary repair of obstetric anal sphincter tears
Anal incontinence after childbirth is more common than was previously believed. Anal incontinence after childbirth. Methods
 Anal incontinence after childbirth Research Recherche From *the Department of Obstetrics and Gynecology, University of Ottawa, Ottawa, Ont.; the Departments of Family Medicine and Social and Preventive
Anal incontinence after childbirth Research Recherche From *the Department of Obstetrics and Gynecology, University of Ottawa, Ottawa, Ont.; the Departments of Family Medicine and Social and Preventive
Midline episiotomy and anal incontinence: retrospective cohort study
 Obstetrics and Gynecology Epidemiology Center, Brigham and Women s Hospital, Harvard Medical School, 221 Longwood Avenue, Boston, MA 02115, Lisa B Signorello study coordinator Bernard L Harlow associate
Obstetrics and Gynecology Epidemiology Center, Brigham and Women s Hospital, Harvard Medical School, 221 Longwood Avenue, Boston, MA 02115, Lisa B Signorello study coordinator Bernard L Harlow associate
Faecal incontinence after childbirth
 Britisb Journal of Obstetrics and Gynaecology January 1997, Vol. 104, pp. 4650 Faecal incontinence after childbirth *Christine MacArthur Reader (Maternal and Child Epidemiology), *Debra E. Bick Research
Britisb Journal of Obstetrics and Gynaecology January 1997, Vol. 104, pp. 4650 Faecal incontinence after childbirth *Christine MacArthur Reader (Maternal and Child Epidemiology), *Debra E. Bick Research
Faecal incontinence persisting after childbirth: a 12 year longitudinal
 Author Posting. The Authors 2013. This is the authors version of the work. It is posted here for personal use, not for redistribution. The definitive version was published in British Journal of Obstetrics
Author Posting. The Authors 2013. This is the authors version of the work. It is posted here for personal use, not for redistribution. The definitive version was published in British Journal of Obstetrics
Obstetric anal sphincter injuries: Incidence, risk factors, consequences and prevention
 Obstetric anal sphincter injuries: Incidence, risk factors, consequences and prevention Katariina Laine, MD PhD thesis 2013 Katariina Laine, MD Department of Obstetrics Oslo University Hospital, Ullevål
Obstetric anal sphincter injuries: Incidence, risk factors, consequences and prevention Katariina Laine, MD PhD thesis 2013 Katariina Laine, MD Department of Obstetrics Oslo University Hospital, Ullevål
Perineal Tears. Obstetrics & Gynaecology Women & Children s Group
 Perineal Tears Obstetrics & Gynaecology Women & Children s Group This leaflet has been designed to give you important information about your condition / procedure, and to answer some common queries that
Perineal Tears Obstetrics & Gynaecology Women & Children s Group This leaflet has been designed to give you important information about your condition / procedure, and to answer some common queries that
Care of your Perineum following 3 rd and 4 th degree tears
 Maternity Services Care of your Perineum following 3 rd and 4 th degree tears Introduction This leaflet aims to give you information about the repair and aftercare of the third or fourth degree tear you
Maternity Services Care of your Perineum following 3 rd and 4 th degree tears Introduction This leaflet aims to give you information about the repair and aftercare of the third or fourth degree tear you
Postoperative Care for Pelvic Fistulae. Peter Jeppson, MD October 3, 2017
 Postoperative Care for Pelvic Fistulae Peter Jeppson, MD October 3, 2017 No Disclosures Rational for Postoperative Care Intraoperative injury may be managed by: Identification Closure Continuous post-operative
Postoperative Care for Pelvic Fistulae Peter Jeppson, MD October 3, 2017 No Disclosures Rational for Postoperative Care Intraoperative injury may be managed by: Identification Closure Continuous post-operative
Marietta Mahendeka, M.D. Obstetrician and Gynaecologist Bugando Medical Centre Tanzania. Tutor: Dr Luc de Bernis, WHO
 A COMPARATIVE STUDY OF THE MANAGEMENT OF VESICO AND/OR RECTO-VAGINAL FISTULAE AT BUGANDO MEDICAL CENTRE, MWANZA, TANZANIA, EAST AFRICA: A RETROSPECTIVE STUDY Marietta Mahendeka, M.D. Obstetrician and Gynaecologist
A COMPARATIVE STUDY OF THE MANAGEMENT OF VESICO AND/OR RECTO-VAGINAL FISTULAE AT BUGANDO MEDICAL CENTRE, MWANZA, TANZANIA, EAST AFRICA: A RETROSPECTIVE STUDY Marietta Mahendeka, M.D. Obstetrician and Gynaecologist
Natural progression of anal incontinence after childbirth
 Int Urogynecol J (2009) 20:1029 1035 DOI 10.1007/s00192-009-0901-2 ORIGINAL ARTICLE Natural progression of anal incontinence after childbirth Johan Nordenstam & Daniel Altman & Sophia Brismar & Jan Zetterström
Int Urogynecol J (2009) 20:1029 1035 DOI 10.1007/s00192-009-0901-2 ORIGINAL ARTICLE Natural progression of anal incontinence after childbirth Johan Nordenstam & Daniel Altman & Sophia Brismar & Jan Zetterström
SUTURING AN EPISIOTOMY/GENITAL LACERATION
 WOMEN AND NEWBORN HEALTH SERVICE CLINICAL GUIDELINES SECTION B : GUIDELINES RELEVANT TO OBSTETRICS AND MIDWIFERY 5 INTRAPARTUM CARE 5.15 PERINEAL REPAIR Authorised by: OGCCU 5.15.1 SUTURING AN EPISIOTOMY/GENITAL
WOMEN AND NEWBORN HEALTH SERVICE CLINICAL GUIDELINES SECTION B : GUIDELINES RELEVANT TO OBSTETRICS AND MIDWIFERY 5 INTRAPARTUM CARE 5.15 PERINEAL REPAIR Authorised by: OGCCU 5.15.1 SUTURING AN EPISIOTOMY/GENITAL
Perineal Suturing and Surgical Drapes/Gowns
 Date of Search: 11 January 2017 Sources Searched: Medline, Embase, CINAHL, TRIP Database, Cochrane Library Perineal Suturing and Surgical Drapes/Gowns Summary Surgical site infection has been estimated
Date of Search: 11 January 2017 Sources Searched: Medline, Embase, CINAHL, TRIP Database, Cochrane Library Perineal Suturing and Surgical Drapes/Gowns Summary Surgical site infection has been estimated
UNDERSTANDING EPISIOTOMY C-SECTION AND RECTOCELE. Our suture portfolio meets all your procedural needs
 UNDERSTANDING EPISIOTOMY C-SECTION AND RECTOCELE Our suture portfolio meets all your procedural needs GYNECOLOGY Episiotomy A surgically planned incision on the perineum and the posterior vaginal wall,
UNDERSTANDING EPISIOTOMY C-SECTION AND RECTOCELE Our suture portfolio meets all your procedural needs GYNECOLOGY Episiotomy A surgically planned incision on the perineum and the posterior vaginal wall,
Physiotherapy advice following your third or fourth degree perineal tear
 Further sources of information NHS Choices: www.nhs.uk/conditions Our website: www.sfh-tr.nhs.uk INFORMATION FOR PATIENTS Patient Experience Team (PET) PET is available to help with any of your compliments,
Further sources of information NHS Choices: www.nhs.uk/conditions Our website: www.sfh-tr.nhs.uk INFORMATION FOR PATIENTS Patient Experience Team (PET) PET is available to help with any of your compliments,
Impact of Delivery Types on Women s Postpartum Sexual Health
 Reproduction & Contraception (2003) 14 (4):237~242 Impact of Delivery Types on Women s Postpartum Sexual Health Huan-ying WANG 1, Xiao-yang XU 2, Zhen-wei YAO 1, Qin ZHOU 1 Key words: postpartum; sexual
Reproduction & Contraception (2003) 14 (4):237~242 Impact of Delivery Types on Women s Postpartum Sexual Health Huan-ying WANG 1, Xiao-yang XU 2, Zhen-wei YAO 1, Qin ZHOU 1 Key words: postpartum; sexual
Incidence and Audit of Treatment on Third and Fourth Grade Perineal Tear
 January 2017 Incedence and audit of treatment on perineal tear 35 Research Article Incidence and Audit of Treatment on Third and Fourth Grade Perineal Tear Insidensi dan Audit dari Tata Laksana Ruptur
January 2017 Incedence and audit of treatment on perineal tear 35 Research Article Incidence and Audit of Treatment on Third and Fourth Grade Perineal Tear Insidensi dan Audit dari Tata Laksana Ruptur
The Pelvic Floor: Expecting (and Delivering!) Susan Barr, MD Assistant Professor Saint Louis University Division of Urogynecology
 Susan Barr, MD Assistant Professor Saint Louis University Division of Urogynecology") The Pelvic Floor: What She Can Expect After Expecting (and Delivering!) Susan Barr, MD Assistant Professor Saint Louis University Division of Urogynecology Objectives Understand risk factors and treatment
The Pelvic Floor: What She Can Expect After Expecting (and Delivering!) Susan Barr, MD Assistant Professor Saint Louis University Division of Urogynecology Objectives Understand risk factors and treatment
for a review under the Accident Compensation Act
 FairWay Resolution Limited Tā te Hinengaro Tōkeke Whakatau Review numbers: Application by for a review under the Accident Compensation Act Held at Date of hearing 2 November 2016, adjourned part-heard;
FairWay Resolution Limited Tā te Hinengaro Tōkeke Whakatau Review numbers: Application by for a review under the Accident Compensation Act Held at Date of hearing 2 November 2016, adjourned part-heard;
Diabetes in pregnancy
 Diabetes in pregnancy Patient information This leaflet provides information about gestational diabetes during pregnancy and delivery. Sometimes women who are not known to have diabetes develop it during
Diabetes in pregnancy Patient information This leaflet provides information about gestational diabetes during pregnancy and delivery. Sometimes women who are not known to have diabetes develop it during
Pelvic Floor Ultrasound Imaging. Prof HP Dietz (Sydney) A/Prof KL Shek (Sydney) Dr R Guzman Rojas (Santiago de Chile) Dr Kamil Svabik (Prague)
 A/Prof KL Shek (Sydney) Dr R Guzman Rojas (Santiago de Chile) Dr Kamil Svabik (Prague)") Pelvic Floor Ultrasound Imaging Workshop IUGA 2015 Nice Faculty: Prof HP Dietz (Sydney) A/Prof KL Shek (Sydney) Dr R Guzman Rojas (Santiago de Chile) Dr Kamil Svabik (Prague) The use of translabial ultrasound
Pelvic Floor Ultrasound Imaging Workshop IUGA 2015 Nice Faculty: Prof HP Dietz (Sydney) A/Prof KL Shek (Sydney) Dr R Guzman Rojas (Santiago de Chile) Dr Kamil Svabik (Prague) The use of translabial ultrasound
Number of pages: This policy and procedure guideline applies to all obstetrics and gynecology medical and midwifery staff.
 Saudi Society of Obstetrics and Gynaecology Policy and Procedure Title/Description: REPAIR OF PERINEAL TRAUMA Effective Date: 1st July 2016 1. PURPOSE Department: Obstetrics and Gynecology (Labour & Birth)
Saudi Society of Obstetrics and Gynaecology Policy and Procedure Title/Description: REPAIR OF PERINEAL TRAUMA Effective Date: 1st July 2016 1. PURPOSE Department: Obstetrics and Gynecology (Labour & Birth)
Traumatic injury to the anal sphincter sustained in a thirdor
 Obstetric Anal Sphincter Injuries: A Survey of Clinical Practice Among Canadian Obstetricians Carolyn Best, BSc, MD, FRCSC, Harold P. Drutz, MD, FRCSC, May Alarab, MBChB, MRCOG, MRCPI, MSc Division of
Obstetric Anal Sphincter Injuries: A Survey of Clinical Practice Among Canadian Obstetricians Carolyn Best, BSc, MD, FRCSC, Harold P. Drutz, MD, FRCSC, May Alarab, MBChB, MRCOG, MRCPI, MSc Division of
Bladder care postpartum including bladder care for women with epidural analgesia (GL792)
") Bladder care postpartum including bladder care for women with epidural analgesia (GL792) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children's Services Clinical Governance Committee
Bladder care postpartum including bladder care for women with epidural analgesia (GL792) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children's Services Clinical Governance Committee
Maternity Information Leaflet. Care of the Perineum (including Pelvic Floor Exercises) Version 2
 Version 2") Maternity Information Leaflet Care of the Perineum (including Pelvic Floor Exercises) Version 2 Pelvic Floor Exercises The pelvic floor muscles are located between your legs, and run from your pubic bone
Maternity Information Leaflet Care of the Perineum (including Pelvic Floor Exercises) Version 2 Pelvic Floor Exercises The pelvic floor muscles are located between your legs, and run from your pubic bone
Childbirth and prolapse: long-term associations with the symptoms and objective measurement of pelvic organ prolapse
 DOI: 10.1111/1471-0528.12075 www.bjog.org Epidemiology Childbirth and prolapse: long-term associations with the symptoms and objective measurement of pelvic organ prolapse C Glazener, a A Elders, a C MacArthur,
DOI: 10.1111/1471-0528.12075 www.bjog.org Epidemiology Childbirth and prolapse: long-term associations with the symptoms and objective measurement of pelvic organ prolapse C Glazener, a A Elders, a C MacArthur,
POSTGRADUATE TRAINING AND ASSESSMENT IN OBSTETRICS AND GYNAECOLOGY LOG BOOK
 POSTGRADUATE TRAINING AND ASSESSMENT IN OBSTETRICS AND GYNAECOLOGY LOG BOOK Approved by The UEMS Section of Obstetrics and Gynaecology and The European Board and College of Obstetrics and Gynaecology (EBCOG)
POSTGRADUATE TRAINING AND ASSESSMENT IN OBSTETRICS AND GYNAECOLOGY LOG BOOK Approved by The UEMS Section of Obstetrics and Gynaecology and The European Board and College of Obstetrics and Gynaecology (EBCOG)
ENTRY INTO SPECIALTY TRAINING USING THE CESR (CP) ROUTE DETAILS OF PREVIOUS POSTS IN OBSTETRICS & GYNAECOLOGY PRIOR TO APPOINTMENT TO NTN
 ROUTE DETAILS OF PREVIOUS POSTS IN OBSTETRICS & GYNAECOLOGY PRIOR TO APPOINTMENT TO NTN") ENTRY INTO SPECIALTY TRAINING USING THE CESR (CP) ROUTE DETAILS OF PREVIOUS POSTS IN OBSTETRICS & GYNAECOLOGY PRIOR TO APPOINTMENT TO NTN PERSONAL DETAILS Trainee name Surname Forename(s) NTN Details NTN
ENTRY INTO SPECIALTY TRAINING USING THE CESR (CP) ROUTE DETAILS OF PREVIOUS POSTS IN OBSTETRICS & GYNAECOLOGY PRIOR TO APPOINTMENT TO NTN PERSONAL DETAILS Trainee name Surname Forename(s) NTN Details NTN
period, cesarean delivery is thought to protect against anal incontinence, 3 albeit incompletely. In this study, we investigated anal incontinence
 Obstetrical anal sphincter laceration and anal incontinence 5-10 years after childbirth Emily C. Evers, MPH; Joan L. Blomquist, MD; Kelly C. McDermott, BS; Victoria L. Handa, MD, MHS OBJECTIVE: The purpose
Obstetrical anal sphincter laceration and anal incontinence 5-10 years after childbirth Emily C. Evers, MPH; Joan L. Blomquist, MD; Kelly C. McDermott, BS; Victoria L. Handa, MD, MHS OBJECTIVE: The purpose
Does delayed child-bearing increase the risk of levator injury in labour?
 Australian and New Zealand Journal of Obstetrics and Gynaecology 2007; 47: 491 495 Blackwell Publishing Asia Original Article Delayed child-bearing and levator injury Does delayed child-bearing increase
Australian and New Zealand Journal of Obstetrics and Gynaecology 2007; 47: 491 495 Blackwell Publishing Asia Original Article Delayed child-bearing and levator injury Does delayed child-bearing increase
Urinary and faecal incontinence following delayed primary repair of obstetric genital fistula
 BJOG: an International Journal of Obstetrics and Gynaecology July 2002, Vol. 109, pp. 828 832 Urinary and faecal incontinence following delayed primary repair of obstetric genital fistula Christine Murray,
BJOG: an International Journal of Obstetrics and Gynaecology July 2002, Vol. 109, pp. 828 832 Urinary and faecal incontinence following delayed primary repair of obstetric genital fistula Christine Murray,
Stapled transanal rectal resection for obstructed defaecation syndrome
 Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Pelvic Floor Disorders. Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon
 Consultant Colorectal and General Surgeon") Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Urogynaecology & Prolapse. Alexander Denning and Leifa Jennings
 + Urogynaecology & Prolapse Alexander Denning and Leifa Jennings + Contents What even is prolapse / urogynaecology? Pelvic floor anatomy Prolapse Urinary incontinence Prevention The end (woot) + Urogynaecology
+ Urogynaecology & Prolapse Alexander Denning and Leifa Jennings + Contents What even is prolapse / urogynaecology? Pelvic floor anatomy Prolapse Urinary incontinence Prevention The end (woot) + Urogynaecology
PROTOCOL FOR BLADDER CARE MANAGEMENT DURING INTRAPARTUM AND POSTNATAL PERIOD
 PROTOCOL FOR BLADDER CARE MANAGEMENT DURING INTRAPARTUM AND POSTNATAL PERIOD Specialty: Obstetrics Date Approved: Revised September 2015 Approved by: Labour Ward Forum Date for Review: September 2018 Overview
PROTOCOL FOR BLADDER CARE MANAGEMENT DURING INTRAPARTUM AND POSTNATAL PERIOD Specialty: Obstetrics Date Approved: Revised September 2015 Approved by: Labour Ward Forum Date for Review: September 2018 Overview
Rectal analgesia for the relief of perineal pain after childbirth: a randomised controlled trial of diclofenac suppositories
 BJOG: an International Journal of Obstetrics and Gynaecology October 2004, Vol. 111, pp. 1059 1064 DOI: 10.1111/j.1471-0528.2004.00156.x Rectal analgesia for the relief of perineal pain after childbirth:
BJOG: an International Journal of Obstetrics and Gynaecology October 2004, Vol. 111, pp. 1059 1064 DOI: 10.1111/j.1471-0528.2004.00156.x Rectal analgesia for the relief of perineal pain after childbirth:
PERINEAL REPAIR: COMPARISON OF SUTURE MATERIALS AND SUTURING TECHNIQUES
 ORIGINAL ARTICLE PERINEAL REPAIR: COMPARISON OF SUTURE MATERIALS AND SUTURING TECHNIQUES FOUZIA PERVEEN, TEHMINA SHABBIR ABSTRACT Objective Study design Place & Duration of study To compare the outcome
ORIGINAL ARTICLE PERINEAL REPAIR: COMPARISON OF SUTURE MATERIALS AND SUTURING TECHNIQUES FOUZIA PERVEEN, TEHMINA SHABBIR ABSTRACT Objective Study design Place & Duration of study To compare the outcome
Operative Vaginal Delivery and Pelvic Floor Trauma. Anna Padoa, MD Urogynecology Service Dept of Ob & Gyn Assaf Harofe Medical Center
 + Operative Vaginal Delivery and Pelvic Floor Trauma Anna Padoa, MD Urogynecology Service Dept of Ob & Gyn Assaf Harofe Medical Center + Vaginal birth and the pelvic floor Mechanisms of injury Damage to
+ Operative Vaginal Delivery and Pelvic Floor Trauma Anna Padoa, MD Urogynecology Service Dept of Ob & Gyn Assaf Harofe Medical Center + Vaginal birth and the pelvic floor Mechanisms of injury Damage to
Do Unsutured Second-Degree Perineal Lacerations Affect Postpartum Functional Outcomes?
 Do Unsutured Second-Degree Perineal Lacerations Affect Postpartum Functional Outcomes? Lawrence M. Leeman, MD, Rebecca G. Rogers, MD, Betsy Greulich, CNM, and Leah L. Albers, DrPH Background: To compare
Do Unsutured Second-Degree Perineal Lacerations Affect Postpartum Functional Outcomes? Lawrence M. Leeman, MD, Rebecca G. Rogers, MD, Betsy Greulich, CNM, and Leah L. Albers, DrPH Background: To compare
Papers. Abstract. Introduction. Methods
 Conservative management of persistent postnatal urinary and faecal incontinence: randomised controlled trial Topic: 66;68;159;161 Cathryn M A Glazener, G Peter Herbison, P Don Wilson, Christine MacArthur,
Conservative management of persistent postnatal urinary and faecal incontinence: randomised controlled trial Topic: 66;68;159;161 Cathryn M A Glazener, G Peter Herbison, P Don Wilson, Christine MacArthur,
K. Jundt 1, I. scheer 2, v. von Bodungen 1, F. Krumbachner 1, K. Friese 1, U. M. Peschers 3
 362 EU Ro PE an JoUR nal of MED I cal RE search Eur J Med Res (2010) 15: 362-366 I. Holzapfel Publishers 2010 WHat HaRM DoEs a second DElIvERy to the PElvIc FlooR? K. Jundt 1, I. scheer 2, v. von Bodungen
362 EU Ro PE an JoUR nal of MED I cal RE search Eur J Med Res (2010) 15: 362-366 I. Holzapfel Publishers 2010 WHat HaRM DoEs a second DElIvERy to the PElvIc FlooR? K. Jundt 1, I. scheer 2, v. von Bodungen
Post operative voiding dysfunction and the Value of Urodynamics. Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist
 Post operative voiding dysfunction and the Value of Urodynamics Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist Learning objectives: v Pathophysiology of post op voiding dysfunction.
Post operative voiding dysfunction and the Value of Urodynamics Dr Salwan Al-Salihi Urogynaecologist Obstetrician and Gynaecologist Learning objectives: v Pathophysiology of post op voiding dysfunction.
Perineal and Anal Sphincter Trauma
 Perineal and Anal Sphincter Trauma Abdul H. Sultan, Ranee Thakar and Dee E. Fenner (Eds) Perineal and Anal Sphincter Trauma Diagnosis and Clinical Management Abdul H. Sultan, MB ChB, MD, FRCOG Consultant
Perineal and Anal Sphincter Trauma Abdul H. Sultan, Ranee Thakar and Dee E. Fenner (Eds) Perineal and Anal Sphincter Trauma Diagnosis and Clinical Management Abdul H. Sultan, MB ChB, MD, FRCOG Consultant
Birth Trauma. H. P. Dietz. University of Sydney, Nepean Campus. Penrith, Australia
 Birth Trauma H. P. Dietz University of Sydney, Nepean Campus Penrith, Australia Procedures in US (2010): 1.6 Prolapse Urinary Incontinence Fecal Incontinence Prolapse 200.000 Urinary Incontinence 120.000
Birth Trauma H. P. Dietz University of Sydney, Nepean Campus Penrith, Australia Procedures in US (2010): 1.6 Prolapse Urinary Incontinence Fecal Incontinence Prolapse 200.000 Urinary Incontinence 120.000
Patient Advice for Third & Fourth Degree Tears
 Patient Advice for Third & Fourth Degree Tears Please read this leaflet carefully. It is important that you take note of any instructions or advice given. If you have any questions or problems that are
Patient Advice for Third & Fourth Degree Tears Please read this leaflet carefully. It is important that you take note of any instructions or advice given. If you have any questions or problems that are
Taking care of your perineum before, during and after birth
 Taking care of your perineum before, during and after birth A Parent Information Leaflet Where is is my my perineum and and what what happens happens during childbirth? during childbirth? Your perineum
Taking care of your perineum before, during and after birth A Parent Information Leaflet Where is is my my perineum and and what what happens happens during childbirth? during childbirth? Your perineum
A retrospective postal survey of women s experiences of physiotherapy management following a third- or fourth-degree perineal tear
 Journal of the Association of Chartered Physiotherapists in Women s Health, Spring 2008, 102, 25 35 CLINICAL PAPER A retrospective postal survey of women s experiences of physiotherapy management following
Journal of the Association of Chartered Physiotherapists in Women s Health, Spring 2008, 102, 25 35 CLINICAL PAPER A retrospective postal survey of women s experiences of physiotherapy management following
Maternity Services. Comment / Changes / Approval. First draft of new guidelines. Comments included after consultation.
 Bladder Care v4.0 Nov 2016 for public website FINAL NOV16 Document Control Title Bladder Care Guideline Author Directorate Women and Children s Version Date Issued Status 0.1 Jun Draft 2009 0.2 July 2009
Bladder Care v4.0 Nov 2016 for public website FINAL NOV16 Document Control Title Bladder Care Guideline Author Directorate Women and Children s Version Date Issued Status 0.1 Jun Draft 2009 0.2 July 2009
Post-partum Anal Incontinence in SA: A myth or reality?
 Post-partum Anal Incontinence in SA: A myth or reality? TD Naidoo Consultant and Honorary Lecturer, Department of Obstetrics and Gynaecology, Grey s Hospital, Pietermaritzburg Metropolitan Hospitals Complex,
Post-partum Anal Incontinence in SA: A myth or reality? TD Naidoo Consultant and Honorary Lecturer, Department of Obstetrics and Gynaecology, Grey s Hospital, Pietermaritzburg Metropolitan Hospitals Complex,
Episiotomy and obstetric outcomes among women living with type 3 female genital mutilation: a secondary analysis
 Rodriguez et al. Reproductive Health (2016) 13:131 DOI 10.1186/s12978-016-0242-9 RESEARCH Open Access Episiotomy and obstetric outcomes among women living with type 3 female genital mutilation: a secondary
Rodriguez et al. Reproductive Health (2016) 13:131 DOI 10.1186/s12978-016-0242-9 RESEARCH Open Access Episiotomy and obstetric outcomes among women living with type 3 female genital mutilation: a secondary
Training matrix. Annual expectation of educational progression ST1 to ST7 in O&G for
 Training matrix Annual expectation of educational progression ST1 to ST7 in O&G for 2016-17 1 These standards represent the minimum required. Trainees are encouraged to exceed these requirements. Please
Training matrix Annual expectation of educational progression ST1 to ST7 in O&G for 2016-17 1 These standards represent the minimum required. Trainees are encouraged to exceed these requirements. Please
FACTORS ASSOCIATED WITH URINARY STRESS INCONTINENCE IN PRIMIPARAS
 P.L. Chou, et al ORIGINAL ARTICLE FACTORS ASSOCIATED WITH URINARY STRESS INCONTINENCE IN PRIMIPARAS Pei-Ling Chou, Fang-Ping Chen*, Li-Fen Teng Department of Obstetrics and Gynecology, Keelung Chang Gung
P.L. Chou, et al ORIGINAL ARTICLE FACTORS ASSOCIATED WITH URINARY STRESS INCONTINENCE IN PRIMIPARAS Pei-Ling Chou, Fang-Ping Chen*, Li-Fen Teng Department of Obstetrics and Gynecology, Keelung Chang Gung
The circumferential obstetric fistula: characteristics, management and outcomes
 DOI: 10.1111/j.1471-0528.2007.01329.x www.blackwellpublishing.com/bjog Short communication The circumferential obstetric fistula: characteristics, management and outcomes A Browning Barhirdar Hamlin Fistula
DOI: 10.1111/j.1471-0528.2007.01329.x www.blackwellpublishing.com/bjog Short communication The circumferential obstetric fistula: characteristics, management and outcomes A Browning Barhirdar Hamlin Fistula
Guest Editorial Seeing the future by appreciating the past
 Volume 2, Issue 3 SEPTEMBER 2014 Editorial Peter de Jong Congratulations to Etienne Henn who produced this Edition of the SAUGA Newsletter. Short and to the point as always. His editorial is appropriate
Volume 2, Issue 3 SEPTEMBER 2014 Editorial Peter de Jong Congratulations to Etienne Henn who produced this Edition of the SAUGA Newsletter. Short and to the point as always. His editorial is appropriate
Birth trauma: short and long term effects of forceps delivery compared with spontaneous delivery on various pelvic floor parameters
 British Journal of Obstetrics and Gynaecology November 2000, Vol107, pp. 1360-1365 Birth trauma: short and long term effects of forceps delivery compared with spontaneous delivery on various pelvic floor
British Journal of Obstetrics and Gynaecology November 2000, Vol107, pp. 1360-1365 Birth trauma: short and long term effects of forceps delivery compared with spontaneous delivery on various pelvic floor
NEW POSTNATAL URINARY INCONTINENCE : OBSTETRIC AND OTHER RISK FACTORS IN PRIMIPARAE. New postnatal urinary incontinence in primiparae
 Author Posting. The Authors 2006. This is the author s version of the work. It is posted here for personal use, not for redistribution. The definitive version was published in BJOG, 113(2):208-17. doi:10.1111/j.1471-0528.2005.00840.x
Author Posting. The Authors 2006. This is the author s version of the work. It is posted here for personal use, not for redistribution. The definitive version was published in BJOG, 113(2):208-17. doi:10.1111/j.1471-0528.2005.00840.x
Tertiary, regional and local pelvic floor service providers: the future. model? Andrew Williams
 Tertiary, regional and local pelvic floor service providers: the future Andrew Williams model? Pelvic Floor Unit Guy s and St Thomas NHS Foundation Trust Background 23% women suffer at least one pelvic
Tertiary, regional and local pelvic floor service providers: the future Andrew Williams model? Pelvic Floor Unit Guy s and St Thomas NHS Foundation Trust Background 23% women suffer at least one pelvic
A Comparison Study on Chlorhexidine and Normal Saline for Perineal Wound Cleansing
 A Comparison Study on Chlorhexidine and Normal Saline for Perineal Wound Cleansing Department of Obstetrics & Gynaecology Kwong Wah Hospital Sin Ming TAI, Amy KM YEUNG, Karen KL YU, Pui I LOU, Alice SY
A Comparison Study on Chlorhexidine and Normal Saline for Perineal Wound Cleansing Department of Obstetrics & Gynaecology Kwong Wah Hospital Sin Ming TAI, Amy KM YEUNG, Karen KL YU, Pui I LOU, Alice SY
CURRICULUM VITAE. Fida F Asali. M.B, B.S, MSc, MRCOG, DFSRH
 CURRICULUM VITAE Fida F Asali M.B, B.S, MSc, MRCOG, DFSRH Assistant Professor in Obstetrics and Gynaecology Consultant in Obstetrics and Gynaecology Faculty of Medicine The Hashemite University 1 Personal
CURRICULUM VITAE Fida F Asali M.B, B.S, MSc, MRCOG, DFSRH Assistant Professor in Obstetrics and Gynaecology Consultant in Obstetrics and Gynaecology Faculty of Medicine The Hashemite University 1 Personal
5 DIAGNOSIS. History taking
 5 DIAGNOSIS All of the photographs in Chapter 4 were taken in theatre before operation. This chapter deals with how one can recognize the type of fistula by history taking and examination. (Note that the
5 DIAGNOSIS All of the photographs in Chapter 4 were taken in theatre before operation. This chapter deals with how one can recognize the type of fistula by history taking and examination. (Note that the
Outcomes of Laparoscopic Hysterectomy in Glangwili Hospital
 Outcomes of Laparoscopic Hysterectomy in Glangwili Hospital Anuja Joshi, Mugahid Abbasher, Islam Abdelrahman PRESENTED BY: DR ANUJA JOSHI MTI TRAINEE GLANGWILI HOSPITAL Overview Abdominal Hysterectomy
Outcomes of Laparoscopic Hysterectomy in Glangwili Hospital Anuja Joshi, Mugahid Abbasher, Islam Abdelrahman PRESENTED BY: DR ANUJA JOSHI MTI TRAINEE GLANGWILI HOSPITAL Overview Abdominal Hysterectomy
Guide to Pelvic Floor Multicompartment Scanning
 Guide to Pelvic Floor Multicompartment Scanning These guidelines have been prepared by Giulio A. Santoro, MD, PhD, Head Pelvic Floor Unit, Section of Anal Physiology and Ultrasound, Coloproctology Service,
Guide to Pelvic Floor Multicompartment Scanning These guidelines have been prepared by Giulio A. Santoro, MD, PhD, Head Pelvic Floor Unit, Section of Anal Physiology and Ultrasound, Coloproctology Service,
2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL)
") 2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL) SECTION B PART 1 - SERVICE SPECIFICATIONS Service Specification No. Service
2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL) SECTION B PART 1 - SERVICE SPECIFICATIONS Service Specification No. Service