Standard terminology and good urodynamic practices. International Continence Society Adrian Wagg, Hong Kong Continence Society 2014
|
|
|
- Millicent Riley
- 5 years ago
- Views:
Transcription
1 Standard terminology and good urodynamic practices International Continence Society Adrian Wagg, Hong Kong Continence Society 2014
2 The Standardisation of Terminology of Lower Urinary Tract Function: Report from the Standardisation Subcommittee of the International Continence Society & An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic Floor Dysfunction Neurourology and Urodynamics 21: (2002) & Neurourology and Urodynamics 29:4 20 (2010)
3
4 An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic Floor Dysfunction The terminology for women, due to the absence of specific diagnoses as well as other female- specific terminology, may not have been advantaged by a single report Standardized terminology in female pelvic floor dysfunction to enable accurate communication for clinical and research purposes
5 Principles: User friendly Clinically based Symptoms Signs Urodynamic investigations Other investigations Common diagnoses
6 Symptoms Patient or caregiver reported Lower urinary tract symptoms Storage Voiding Post micturition Associated with sexual intercourse Associated with pelvic organ prolapse Genital / lower urinary tract pain The subjective indicator of a disease or change in condition as perceived by the patient, caregiver or partner and may lead him/her to seek help from health care professionals. Any morbid phenomenon or departure from the normal in structure, function, or sensation, experienced by the woman and indicative of disease, or a health problem. Symptoms are either volunteered by, or elicited from the individual, or may be described by the individual s caregiver.
7 Symptoms: Storage Increased daytime frequency Nocturia Urgeny Urinary incontinence Stress urinary incontinence Urge urinary incontinence Mixed urinary incontinence Enuresis Nocturnal enuresis Continuous urinary incontinence Other types of urinary incontinence (giggle /intercourse)
8 Symptoms: Storage contn d Bladder sensation Normal Increased Reduced Absent Non-specific
9 Symptoms Voiding Slow stream Splitting spraying Intermittent stream (intermittency) Hesitancy Straining Terminal dribble
10 Symptoms Post micturition Feeling of Incomplete emptying Post micturition dribble
11 ICS/IUGA (added) Associated with intercourse Associated with pelvic organ prolapse Genital / lower urinary tract pain (exactly) where; when; how much Pain syndromes Painful bladder syndrome (Interstitial cystitis not ICS) Other pain regions Vulva Vagina Scrotum Perineum
12 UIGA / ICS FEMALE Urinary Incontinence Symptoms (added) Postural urinary incontinence Insensible urinary incontinence Coïtal incontinence Voiding Symptoms (added) Position dependent micturition Dysuria Urinary retention Pelvic organ prolapse symptoms Vaginal bulging Pelvic pressure Bleeding discharge infection Splinting /digitation Low backache
13 ICS/ IUGA (added) Dyspareunia Superficial Deep Obstructed intercourse Vaginal laxity Anal dysfunction Faecal incontinence Flatal Faecal urgency Straining to defaecate Feeling of incomplete emptying Diminished rectal sensation Constipation Rectal prolapse Rectal bleeding/mucus
14 Pain Bladder pain: Complaint of suprapubic or retropubic pain, pressure, or discomfort, related to the bladder, and usually increasing with bladder filling. It may persist or be relieved after voiding.3 xi Urethral pain: Complaint of pain felt in the urethra and the woman indicates the urethra as the site.3 Vulval pain: Complaint of pain felt in and around the vulva. 3 Vaginal pain: Complaint of pain felt internally within the vagina, above the introitus.3
15 Pain Perineal pain: Complaint of pain felt between the posterior fourchette (posterior lip of the introitus) and the anus. 3 Pelvic pain: The complaint of pain perceived to arise in the pelvis, not associated with symptoms suggestive of lower urinary tract, sexual, bowel, or gynecological dysfunction. It is less well defined than the above types of localized pain. Cyclical (menstrual) pelvic pain: Cyclical pelvic pain related to menses that raises the possibility of a gynecological cause. Pudendal neuralgia: Burning vaginal or vulval (anywhere between anus and clitoris) pain associated with tender- ness over the course of the pudendal nerves.
16 Signs (suggestive of LUTD) 2002 Are observed by the physician, including simple means, to verify symptoms and quantify them 2010 Any abnormality indicative of disease or a health problem, discoverable on examination of the patient; an objective indication of disease
17 Urinary incontinence: Observation of involuntary loss of urine on examination: this may be urethral or extraurethral Stress (urinary) incontinence (clinical stress leakage): Observation of involuntary leakage from the urethra synchronous with effort or physical exertion, or on sneezing or coughing. Urgency (urinary) incontinence: Observation of involuntary leakage from the urethra synchronous with the sensation of a sudden, compelling desire to void that is difficult to defer. Extraurethral incontinence: Observation of urine leakage through channels other than the urethral meatus, for example, fistula. Stress incontinence on prolapse reduction (occult or latent stress incontinence): Stress incontinence only observed after the reduction of co-existent prolapse Uncategorised incontinence is the observation of involuntary leakage that cannot be classified into one of the above categories on the basis of signs and symptoms. 2002
18 Signs (suggestive of LUTD) Measuring frequency Micturition time chart Frequency volume chart Bladder diary Daytime frequency Nocturia 24-hour frequency 24-hour production Polyuria (>2.8L/24h) Nocturnal urine volume» Nocturnal polyuria >1/3 Maximum voided volume
19 Signs Physical examination Abdomen Perineum Genital Pelvic floor muscle function Rectal Pad testing allows the description of 2002 observed and palpable anatomical abnormalities and is the easiest method of assessing pelvic floor muscle function in children and men. In addition, rectal examination is essential in children with urinary incontinence to rule out faecal inpaction. Normal pelvic floor muscles: 2010 Overactive pelvic floor muscles: Underactive pelvic floor muscles: Non-functioning pelvic floor muscles: Examination for levator (puborectalis) injury: Rectal examination 2010 Anal sphincter tone and strength: Anal sphincter tear: Confirm presence or absence of rectocele Diagnose perineal body deficiency. Other rectal lesions: Anal lesions: Other perianal lesions:
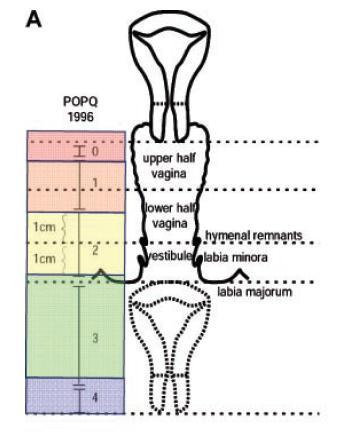
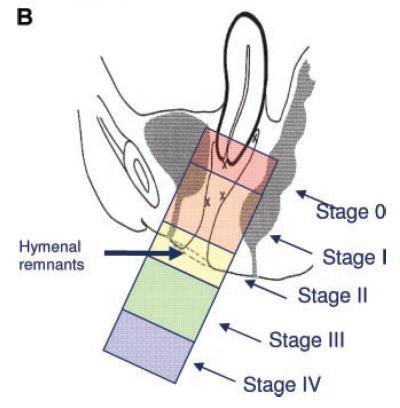
20 Prolapse
21 Anterior vaginal wall prolapse: Observation of descent of the anterior vaginal wall. Posterior vaginal wall prolapse: Observation of descent of the posterior vaginal wall.
22 Other relevant examination Neurological signs: For patients with possible neurogenic lower urinary tract or pelvic floor dysfunction, there should be particular note of those neurological signs related to S2 S4, but these should be complemented by a more general neurological examination as indicated. Abdominal signs: Bladder fullness/retention Other abdominal masses or distension Scars Renal area: Examination for tenderness, masses. 2010
23 Urodynamic technique Conventional urodynamic studies normally take place in the urodynamic laboratory and usually involve artificial bladder filling Artificial bladder filling is defined as filling the bladder, via a catheter, with a specified liquid at a specified rate natural filling means that the bladder is filled by the production of urine rather than by an artificial medium Ambulatory urodynamic studies are defined as a functional test of the lower urinary tract, utilising natural filling, and reproducing the subject s every day activities
24 Intravesical pressure is the pressure within the bladder Abdominal pressure is taken to be the pressure surrounding the bladder. The simultaneous measurement of abdominal pressure is essential for the interpretation of the intravesical pressure trace Detrusor pressure is that component of intravesical pressure that is created by forces in the bladder wall (passive and active). It is estimated by subtracting abdominal pressure from intravesical pressure
25 Filling Cystometry the method by which the pressure/volume relationship of the bladder is measured during bladder filling. The filling phase starts when filling commences and ends when the patient and urodynamicist decide that permission to void has been given. Bladder and urethral function, during filling, need to be defined separately. The rate at which the bladder is filled is divided into: Physiological filling rate is defined as a filling rate less than the predicted maximum - predicted maximum body weight in kg divided by 4, expressed as ml/min Non-physiological filling rate is defined as a filling rate greater than the predicted maximum filling rate - predicted maximum body weight in kg divided by 4 expressed as ml/min
26 Bladder sensation First sensation of bladder filling is the feeling the patient has when he/she first becomes aware of the bladder filling First desire to void the feeling that would lead the patient to pass urine at the next convenient moment, but voiding can be delayed if necessary. Strong desire to void a persistent desire to void with- out the fear of leakage.
27 Increased bladder sensation an early first sensation of bladder filling (or an early desire to void) and/or an early strong desire to void, which occurs at low bladder volume and which persists. Reduced bladder sensation diminished sensation throughout bladder filling. Absent bladder sensation the individual has no bladder sensation. Non-specific bladder sensations may make the individual aware of bladder filling, for example, abdominal fullness or vegetative symptoms
28 Bladder pain during filling cystometry, is a self explanatory term and is an abnormal finding Urgency is a sudden compelling desire to void which is difficult to defer The vesical/urethral sensory threshold defined as the least current which consistently produces a sensation perceived by the subject during stimulation at the site under investigation
29 Bladder capacity during filling cystometry Cystometric capacity: Bladder volume at the end of filling cystometry, when permission to void is usually given by the urodynamicist. Maximum cystometric capacity: In patients with normal sensation, this is the bladder volume when he/she can no longer delay micturition.
30 Detrusor function during filling cystometry: Normal (previously stable ) detrusor function: little or no change in detrusor pressure with filling. There are no involuntary phasic contractions despite provocation with activities such as postural changes, coughing, hearing the sound of running water, hand- washing. Detrusor overactivity: involuntary detrusor contractions during filling cystometry. These contractions, which may be spontaneous or provoked, produce a wave form on the cystometrogram, of variable duration and amplitude. The contractions may be phasic or terminal. Symptoms, for example, urgency and/or urgency incontinence may or may not occur. If a relevant neurological cause is present, then neurogenic detrusor overactivity is noted, otherwise idiopathic detrusor overactivity should be the term used (Fig. 6). Neurogenic detrusor overactivity: This is where there is detrusor overactivity and there is evidence of a relevant neurological disorder.
31 Compliance Compliance is calculated by dividing the volume change (ΔV) by the change in detrusor pressure (ΔPdet) during that change in bladder volume Compliance is expressed as ml per cmh2o. Bladder compliance can be affected by: Bladder filling: Faster filling is more provocative. An artifact may be produced which settles when filling is interrupted. Contractile/relaxant properties of the detrusor 2010 Starting point for compliance calculations3: Usually the detrusor pressure & volume at the start of bladder filling (usually zero). End point for compliance calculations: The detrusor pressure (and volume) at cystometric capacity or immediately before the start of any detrusor contraction that causes significant leakage (and therefore causes the bladder volume to decrease, affecting compliance calculations). Both points are measured excluding any detrusor contraction.
32 Urodynamic conditions / observations The urethral closure mechanism during storage may be competent or incompetent. Normal urethral closure mechanism maintains a positive urethral closure pressure during bladder filling even in the presence of increased abdominal pressure, although it may be overcome by detrusor overactivity Incompetent urethral closure mechanism one which allows leakage of urine in the absence of a detrusor contraction Urethral relaxation incontinence leakage due to urethral relaxation in the absence of raised abdominal pressure or detrusor overactivity Urodynamic stress incontinence involuntary leakage of urine during increased abdominal pressure, in the absence of a detrusor contraction.
33 Leak point pressures The pressure values at leakage should be measured at the moment of leakage. Detrusor leak point pressure (detrusor LPP): the lowest value of the detrusor pressure at which leakage is observed in the absence of increased abdominal pressure or a detrusor contraction Abdominal leak point pressure (abdominal LPP): the lowest value of the intentionally increased intravesical pressure that provokes urinary leakage in the absence of a detrusor contraction. The increase in pressure can be induced by a cough (cough LPP) or Valsalva (Valsalva LPP). Multiple estimates at a fixed bladder volume ( ml) are desirable. Catheter size will influence LPP values and should be standardized.
34 Flow Studies Pressure flow studies of voiding are the method by which the relationship between pressure in the bladder and urine flow rate is measured during bladder emptying The voiding phase starts when permission to void is given or when uncontrollable voiding begins, and ends when the patient considers voiding has finished.
35 Urine flow is defined either as continuous, that is without interruption, or as intermittent, when an individual states that the flow stops and starts during a single visit to the bathroom in order to void. The continuous flow curve is defined as a smooth arc shaped curve or fluctuating when there are multiple peaks during a period of continuous urine flow. Flow rate the volume of fluid expelled via the urethra per unit time. It is expressed in ml/s. Voided volume the total volume expelled via the urethra Maximum flow rate the maximum measured value of the flow rate after correction for artefacts.
36 Voiding time total duration of micturition, i.e. includes interruptions. When voiding is completed without interruption, voiding time is equal to flow time. Flow time the time over which measurable flow actually occurs. Average flow rate voided volume divided by flow time. The average flow should be interpreted with caution if flow is interrupted or there is a terminal dribble. Time to maximum flow the elapsed time from onset of flow to maximum flow.
37 Pressure flow studies Premicturition pressure recorded immediately before the initial isovolumetric contraction Opening pressure recorded at the onset of urine flow (consider time delay). (ORIGINAL) Opening time the elapsed time from initial rise in detrusor pressure to onset of flow. This is the initial isovolumetric contraction period of micturition. Flow measurement delay should be taken into account when measuring opening time. Maximum pressure maximum value of the measured pressure
38 Pressure at maximum flow lowest pressure recorded at maximum measured flow rate. (ORIGINAL) Closing pressure pressure measured at the end of measured flow. (ORIGINAL) Minimum voiding pressure minimum pressure during measurable flow. This is not necessarily equal to either the opening or closing pressures. Flow delay time delay between a change in bladder pressure and the corresponding change in measured flow rate.
39 Detrusor function during voiding 2002: Normal voiding is achieved by a voluntarily initiated continuous detrusor contraction that leads to complete bladder emptying within a normal time span, and in the absence of obstruction.for a given detrusor contraction, the magnitude of the recorded pressure rise will depend on the degree of outlet resistance. 2010: Normal voiding in women is achieved by an initial (voluntary) reduction in intraurethral pressure (urethral relaxation).this is generally followed by a continuous detrusor contraction that leads to complete bladder emptying within a normal time span. Many women will void successfully by urethral relaxation alone, without much of a rise in detrusor pressure. The amplitude of the detrusor contraction will tend to increase to cope with any degree of bladder outflow obstruction
40 eabnormal detrusor activity Detrusor underactivity is defined as a contraction of x reduced strength and/or duration, resulting in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span 2002: Acontractile detrusor is one that cannot be demonstrated to contract during urodynamic studies 2010: Acontractile detrusor: The detrusor cannot be observed to contract during urodynamic studies resulting in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span, where there is a neurological cause use neurogenic acontractile detrusor. Post void residual (PVR) is defined as the volume of urine left in the bladder at the end of micturition.
41 Urethral Function During Voiding Cystometry Normal urethra function a urethra that opens, and is continuously relaxed to allow the bladder to be emptied at a normal pressure. Abnormal urethra function due to either obstruction to urethral overactivity, or a urethra that cannot open due to anatomic abnormality, such as an enlarged prostate or a urethral stricture. Bladder outlet obstruction generic term for obstruction during voiding and is characterised by increased detrusor pressure and reduced urine flow rate. It is usually diagnosed by studying the synchronous values of flowrate and detrusor pressure. Dysfunctional voiding an intermittent and/or fluctuating flow rate due to involuntary intermittent contractions of the periurethral striated muscle during voiding, in neurologically normal individuals Detrusor sphincter dyssynergia a detrusor contraction concurrent with an involuntary contraction of the urethral and/or periurethral striated muscle. Occasionally flow may be prevented altogether Non-relaxing urethral sphincter obstruction usually occurs in individuals with a neurological lesion and is characterised by a non-relaxing, obstructing urethra resulting in reduced urine flow
42 Acute retention of urine Conditions a painful, palpable or percussable bladder, when the patient is unable to pass any urine Chronic retention of urine a non-painful bladder, which remains palpable or percussable after the patient has passed urine Benign prostatic obstruction may be diagnosed when the cause of outlet obstruction is known to be benign prostatic enlargement, due to histologic benign prostatic hyperplasia Benign prostatic hyperplasia the typical histological pattern which defines the disease Benign prostatic enlargement prostatic enlargement due to histologic benign prostatic hyperplasia. The term prostatic enlargement should be used in the absence of prostatic histology.
43 Bladder Oversensitivity DIAGNOSES diagnosis made by symptoms and urodynamic investigations, is more likely to occur in women with symptoms of frequency and nocturia, and a voiding diary showing a clearly reduced average voided volume. Recurrent Urinary Tract Infections diagnosis by clinical history assisted by the results of diagnostic tests involves the determination of the occurrence of at least three symptomatic and medically diagnosed UTIs over the previous 12 months
44 Ultrasound Perineal Introïtal Transvaginal Transabdominal Intercurrent pelvic pathology Position of pelvic organs Postoperative findings Pelvic floor Bladder Urethra
45 Radiological Videocystourethrography Intravenous urography Micturating cystogram Defecography Colporecto-cystourethrography MRI
46 Rehabilitation Pelvic floor training Biofeedback Behavioural modification Electrical stimulation Catheterisation Intermittent Clean intermittent Aseptic intermittent Indwelling Reflex triggering Expression (credé)
47 Good urodynamic practice
48 The committee Werner Schafer Paul Abrams Limin Liao Anders Mattiasson Francesco Pesce, Anders Spangberg Arthur M. Sterling Norman R. Zinner, Philip van Kerrebroeck Neurourol.Urodynamics 2002;21: ,
49 Principles A clear indication for and appropriate selection of relevant test measurements and procedures Precise measurement with data quality control and complete documentation Accurate analysis and critical reporting of results
50 RECORDING MICTURITIONS AND SYMPTOMS Micturition Time Chart records the time of each micturition Frequency Volume Chart time of micturition & voided volumes are recorded Bladder Diary Records time of micturition & voided volumes, relevant symptoms and events such as urgency, pain, incontinence episodes, and pad usage
51 Recording for a minimum of 2 days is recommended. now 3/7 minimally accepted From the recordings, the average voided volume, voiding frequency, and day/night urine production and nocturia can be determined. Provides objective verification of the patient s symptoms, and values for plausibility control for subsequent urodynamic studies.
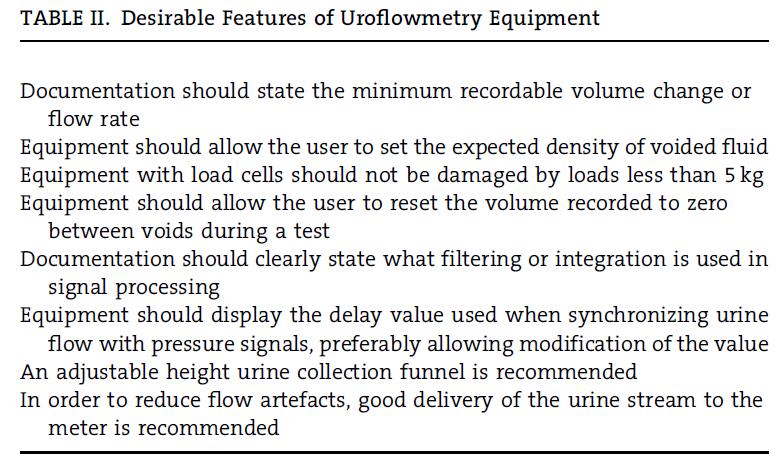
52 UROFLOWMETRY Adequate privacy should be provided and patients should be asked to void when they feel a normal desire to void Patients should be asked if their voiding was representative of their usual voiding and their view should be documented. Automated data analysis must be verified by inspection of the flow curve, artifacts must be excluded, and verification must be documented
53 UROFLOWMETRY The results from uroflowmetry should be compared with the data from the patient s own recording on a frequency/volume chart. Sonographic estimation of post-void residual volume completes the non-invasive assessment of voiding function.
54 Detrusor contractility This is not contractility As the voiding function reflects the interaction between the relaxed outlet and the contracting detrusor, variation of both will affect the flow. For steady outflow conditions, all variations in flowrate are related to changes in detrusor activity alone. The detrusor contraction strength varies neurogenically and myogenically, and can cause significant variability in urine flow rate measurements.
55 Bladder Outflow Resistance & volume If detrusor, contractile function is constant, then changes in outflow resistance will lead to changes in flow rate, for example, in patients with detrusor-sphincter dyssynergia As the bladder volume increases and the detrusor muscle fibres become more stretched, there is an increase in the potential bladder power and work associated with a contraction. Q max is physiologically dependent on the bladder volume
56 Recommendations for Uroflowmetry graphical scaling should be standardized as follows: one millimetre should equal 1 s on the x-axis and 1ml/s & 10 ml voided volume on the y-axis. routine clinical measurements should read flowrate values only to the nearest full ml/s and volumes to the nearest 10 ml. a sliding average over 2 s should be used to remove positive and negative spike artifacts. It is recommended that: only flow rate values, which have been smoothed, either electronically or manually, should be reported.
57 If a maximum flow value is determined electronically by simple signal peak detection without the recommended electronic smoothing, it should be labelled differently, Qmax.raw. The interpretation of any dynamic variation (signal patterns) in free flow will rely on personal experience, can be only descriptive, and in general will remain speculative. Maximum (smoothed) urine flow rate should be rounded to the nearest whole number Voided volume and post void residual volume should be rounded to the nearest 10 ml The maximum flow rate should always be documented together with voided volume and post void residual volume using a standard format VOID: Maximum Flow Rate/ VolumeVoided/PostVoid Residual Volume.
58 International Continence Society Guidelines on Urodynamic Equipment Performance Andrew Gammie, Becky Clarkson, Chris Constantinou, Margot Damaser, Michael Drinnan, Geert Geleijnse, Derek Griffiths, Peter Rosier, Werner Schafer, Ron Van Mastrigt (The International Continence Society Urodynamic Equipment Working Group)
59
60 INVASIVE URODYNAMICS: FILLING CYSTOMETRY, PRESSURE-FLOW STUDY OF VOIDING A good urodynamic investigation should be performed interactively with the patient. It should be established by discussion with the patient that the patient s symptoms have been reproduced during the test There should be continuous and careful observation of the signals as they are collected, and the continuous assessment of the qualitative and quantitative plausibility of all signals
61 Artifacts should be avoided, and any artifacts that occur should be corrected immediately. the same quality criteria apply for ambulatory urodynamic monitoring before invasive urodynamics, a frequency volume chart should be completed and multiple free flows should be evaluated.
62 a significant delay is to be expected for the typical urodynamic flow rate recorded extracorporally ( s). This delay will vary with anatomy, pathology, flow rate, and the set-up for measurement. the time delay between urethral closure and the end of any flow recording may be much longer in, prostatic obstruction terminal dribbling than between the opening of the urethra and the start of a flow rate signal descriptive terminology for synchronizing pressure and flow values, p det.q beg for the pressure at which flow begins instead of p det.open p det.q end when flow ends instead of p det.close
63 Multi-channel cystometry Measurement of intravesical and abdominal pressure ICS standardization of zero pressure and reference height. Zero pressure and reference height are concepts which are often confused in urodynamics. Zero pressure is the surrounding atmospheric pressure, recorded when a transducer is open to the environment when disconnected from any tubes or catheters, or when the open end of a connected, fluid-filled tube is at the same vertical level as the transducer. The reference height is defined as the upper edge of the symphysis pubis.
64 Microtip pressure transducers It is impossible to define the precise position of an intravesical and a rectal catheter It is impossible to position them at the standard level of the upper border of the symphysis pubis. Setting the catheter mounted pressure transducers to zero pressure when inside the body at the start of pressure recording means that both the standard zero pressure as well the reference level are ignored such recorded pressures cannot be compared between patients or centres. initial intravesical and abdominal resting pressures are different between patients, and depend significantly on patient s position. by ignoring the correct atmospheric zero pressure, an error of up to 50 cmh 2 O, can occur. In addition, when a study starts with zero abdominal pressure then the commonly observed abdominal pressure decrease at pelvic floor relaxation during voiding will result in negative abdominal pressure values, and p det will be higher than p ves.

65 For intravesical and abdominal pressure recording external transducers connected to fluid filled tubing and catheters be used. If microtip or air-filled catheters are used, any deviation from standard zero and reference level should be minimized and taken into account at the time of data analysis.
66 Urodynamic catheters For the measurement of intravesical pressure and for bladder filling, the standard catheter for routine urodynamics is a transurethral double-lumen catheter. A double lumen catheter facilitates a second fill/void study to establish reproducibility. Reintroduction of the separate filling tube for a repeated study is more invasive and complicated.
67 The use of a rectal balloon catheter is recommended for the measurement of abdominal pressure, p abd. a flaccid, air-free balloon in the rectal ampulla gives a suitable signal for p abd to determine a meaningful p det when p ves is measured synchronously. In females, vaginal recording may be more acceptable and provides comparable results.
68 Requirements for Filling Cystometry and Pressure-Flow Studies of Voiding three measurement channels, two for pressure and one for flow, a display and secure storage of three pressures (p abd, p ves, p det ) and flow (Q) as tracings against time infused volume and voided volume may be shown graphically or numerically on-line display of pressures and flow, with adequate scale and resolution; scales must be clearly given on all axes; no information should be lost electronically when tracings go off-scale on display; possibilities to record standard information about sensation and additional comments (event recording).
69
70 Minimum accuracy should be ± 1 cmh 2 O for pressure and ± 5% full scale for flow and volume; Ranges of cmh 2 O, 0-25(50) ml/s, and 1,000 ml for pressure, flow, and volume The software must ensure that no information for pressures up to 250 cmh 2 O and for flow rates up to 50 ml/s is lost internally even when not displayed and that off-scale values are clearly identified; An analog/digital (A/D) frequency of 10 Hz per channel as the lower limit for pressure and flow; A higher frequency (minimum 20 khz) is necessary for recording EMG; Calibration of all measurements should be possible.
71 The following criteria form the minimum recommendations for ensuring quality control of pressure recordings: Resting values for abdominal, intravesical, and detrusor pressure are in a typical range The abdominal and intravesical pressure signals are live with minor variations caused by breathing or talking being similar for both signals; these variations should not appear in p det Coughs are used (every I min. or, for example, 50 ml filled volume) to ensure that the abdominal and intravesical pressure signals respond equally. Coughs immediately before voiding and immediately after voiding should be included. When standards are followed, a typical range for initial resting pressures values fo rpves and pabd supine 5-20 cmh2o. sitting cmh2o. standing cmh2o.
72 All negative pressure values, except when caused by rectal activity, should be corrected immediately. P det cannot be negative. The urodynamic findings and the interpretation of the results should be documented immediately after the study is finished
73 Pressure artefacts Catheter-tip transducers and air-filled transducers will have an error due to their unknown and changing height within the bladder, which is difficult to correct. Air bubbles Dislodged catheter. Incomplete pressure transmission Incomplete cough cancellation. Artefacts with separate lines. Single Lumen artefact. Dual-lumen artefact (pump)
74 User interface
75 Conclusions Standardised terminology assists communication and analysis GUP assures quality investigations Standardised equipment performance allows data sharing and grouped analysis
76 I forgot my business cards Dr. Bing Chung Tong will make the slides available
Report from the Standardisation Sub-committee of the International Continence Society
 THE STANDARDISATION OF TERMINOLOGY IN LOWER URINARY TRACT FUNCTION Report from the Standardisation Sub-committee of the International Continence Society Committee: Paul Abrams, Linda Cardozo, Magnus Fall,
THE STANDARDISATION OF TERMINOLOGY IN LOWER URINARY TRACT FUNCTION Report from the Standardisation Sub-committee of the International Continence Society Committee: Paul Abrams, Linda Cardozo, Magnus Fall,
This report presents definitions of the symptoms,
 UPDATE THE STANDARDISATION OF TERMINOLOGY IN LOWER URINARY TRACT FUNCTION: REPORT FROM THE STANDARDISATION SUB-COMMITTEE OF THE INTERNATIONAL CONTINENCE SOCIETY PAUL ABRAMS, LINDA CARDOZO, MAGNUS FALL,
UPDATE THE STANDARDISATION OF TERMINOLOGY IN LOWER URINARY TRACT FUNCTION: REPORT FROM THE STANDARDISATION SUB-COMMITTEE OF THE INTERNATIONAL CONTINENCE SOCIETY PAUL ABRAMS, LINDA CARDOZO, MAGNUS FALL,
Bristol Urological Institute, Bristol, UK. The Warrell Unit, St Mary s Hospital, Manchester. UK.
 Disclosures Basic Principles of Urodynamics Andrew Gammie Bristol Urological Institute, Bristol, UK Albyn, Andromeda, Laborie, Mediwatch, MMS Project sponsorship T-Doc LLC Trial sponsorship with grateful
Disclosures Basic Principles of Urodynamics Andrew Gammie Bristol Urological Institute, Bristol, UK Albyn, Andromeda, Laborie, Mediwatch, MMS Project sponsorship T-Doc LLC Trial sponsorship with grateful
Peter K. Sand, M.D. Roger Dmochowski, M.D.
 ANALYSIS OF THE STANDARDISATION OF TERMINOLOGY OF LOWER URINARY TRACT DYSFUNCTION: REPORT FROM THE STANDARDISATION SUB-COMMITTEE OF THE INTERNATIONAL CONTINENCE SOCIETY Neurourol Urodynam 21: 167-78, 2002
ANALYSIS OF THE STANDARDISATION OF TERMINOLOGY OF LOWER URINARY TRACT DYSFUNCTION: REPORT FROM THE STANDARDISATION SUB-COMMITTEE OF THE INTERNATIONAL CONTINENCE SOCIETY Neurourol Urodynam 21: 167-78, 2002
Neurogenic bladder. Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder.
 Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
The Management of Female Urinary Incontinence. Part 1: Aetiology and Investigations
 The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
Dr. Aso Urinary Symptoms
 Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Standardization of Terminology of Urodynamics And Good Urodynamic Practices
 Standardization of Terminology of Urodynamics And Good Urodynamic Practices Peter F.W.M. Rosier MD PhD Department of urology, University Medical Centre Utrecht,The Netherlands Standardization of Terminology
Standardization of Terminology of Urodynamics And Good Urodynamic Practices Peter F.W.M. Rosier MD PhD Department of urology, University Medical Centre Utrecht,The Netherlands Standardization of Terminology
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist
 Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Urodynamics in Neurological Lower Urinary Tract Dysfunction. Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne
 Urodynamics in Neurological Lower Urinary Tract Dysfunction Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne Learning Objectives Review functional neurology relevant to lower
Urodynamics in Neurological Lower Urinary Tract Dysfunction Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne Learning Objectives Review functional neurology relevant to lower
Guidelines on Neurogenic Lower Urinary Tract Dysfunction
 Guidelines on Neurogenic Lower Urinary Tract Dysfunction (Text update March 2009) M. Stöhrer (chairman), B. Blok, D. Castro-Diaz, E. Chartier- Kastler, P. Denys, G. Kramer, J. Pannek, G. del Popolo, P.
Guidelines on Neurogenic Lower Urinary Tract Dysfunction (Text update March 2009) M. Stöhrer (chairman), B. Blok, D. Castro-Diaz, E. Chartier- Kastler, P. Denys, G. Kramer, J. Pannek, G. del Popolo, P.
W11: Basic Urodynamics - An Interactive Workshop Workshop Chair: Hashim Hashim, United Kingdom 06 October :00-17:00
 W11: Basic Urodynamics - An Interactive Workshop Workshop Chair: Hashim Hashim, United Kingdom 06 October 2015 14:00-17:00 Start End Topic Speakers 14:00 14:15 Introduction Hashim Hashim 14:15 14:30 Physics
W11: Basic Urodynamics - An Interactive Workshop Workshop Chair: Hashim Hashim, United Kingdom 06 October 2015 14:00-17:00 Start End Topic Speakers 14:00 14:15 Introduction Hashim Hashim 14:15 14:30 Physics
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Mr. GIT KAH ANN. Pakar Klinikal Urologi Hospital Kuala Lumpur.
 Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Various Types. Ralph Boling, DO, FACOG
 Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Voiding Diary. Begin recording upon rising in the morning and continue for a full 24 hours.
 Urodvnamics Your physician has scheduled you for a test called URODYNAMICS. This test is a series of different measurements of bladder function and can be used to determine the cause of a variety of bladder
Urodvnamics Your physician has scheduled you for a test called URODYNAMICS. This test is a series of different measurements of bladder function and can be used to determine the cause of a variety of bladder
Practical urodynamics What PA s need to know. Gary E. Lemack, MD Professor of Urology and Neurology
 Practical urodynamics What PA s need to know Gary E. Lemack, MD Professor of Urology and Neurology Urodynamics essential elements Urethral catheter Fill rate Catheter size Intravesical pressure measurements
Practical urodynamics What PA s need to know Gary E. Lemack, MD Professor of Urology and Neurology Urodynamics essential elements Urethral catheter Fill rate Catheter size Intravesical pressure measurements
Urogynecology ICD-9 to ICD-10 Crosswalks
 1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
ATLAS OF URODYNAMICS. Bladder. Pure. Pves. Pabd. Pdet EMG. Bladder. volume. Cough Strain IDC. Filling. Pure. Pves. Pabd. Pdet EMG
 2 Normal Micturition The micturition cycle (urine storage and voiding) is a nearly subconscious process that is under complete voluntary control. Bladder filling is accomplished without sensation and without
2 Normal Micturition The micturition cycle (urine storage and voiding) is a nearly subconscious process that is under complete voluntary control. Bladder filling is accomplished without sensation and without
Overactive Bladder: Diagnosis and Approaches to Treatment
 Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
INCONTINENCE. Continence and Pelvic Floor Rehabilitation TYPES OF INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE 11/08/2015
 INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
The new International Continence Society
 ROLE OF CYSTOMETRY IN EVALUATING PATIENTS WITH OVERACTIVE BLADDER ADAM J. FLISSER AND JERRY G. BLAIVAS ABSTRACT Overactive bladder (OAB) can be caused by a variety of conditions. We believe that cystometrography
ROLE OF CYSTOMETRY IN EVALUATING PATIENTS WITH OVERACTIVE BLADDER ADAM J. FLISSER AND JERRY G. BLAIVAS ABSTRACT Overactive bladder (OAB) can be caused by a variety of conditions. We believe that cystometrography
The Neurogenic Bladder
 The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
Urodynamic findings in women with insensible incontinence
 bs_bs_banner International Journal of Urology (2013) 20, 429 433 doi: 10.1111/j.1442-2042.2012.03146.x Original Article: Clinical Investigation Urodynamic findings in women with insensible Benjamin M Brucker,
bs_bs_banner International Journal of Urology (2013) 20, 429 433 doi: 10.1111/j.1442-2042.2012.03146.x Original Article: Clinical Investigation Urodynamic findings in women with insensible Benjamin M Brucker,
Urogynaecology. Colm McAlinden
 Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
THE ACONTRACTILE BLADDER - FACT OR FICTION?
 THE ACONTRACTILE BLADDER - FACT OR FICTION? Jacob Golomb Department of Urology Chaim Sheba Medical Center Tel Hashomer NEUROGENIC UNDERACTIVE DETRUSOR Central (complete/incomplete): Spinal cord injury-
THE ACONTRACTILE BLADDER - FACT OR FICTION? Jacob Golomb Department of Urology Chaim Sheba Medical Center Tel Hashomer NEUROGENIC UNDERACTIVE DETRUSOR Central (complete/incomplete): Spinal cord injury-
Key words: consensus; diagnosis; female pelvic floor dysfunction; symptomatology; terminology; urodynamics
 Neurourology and Urodynamics 29:4 20 (2010) REVIEW ARTICLE An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic
Neurourology and Urodynamics 29:4 20 (2010) REVIEW ARTICLE An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic
International Continence Society Good Urodynamic Practices and Terms 2016: Urodynamics, uroflowmetry, cystometry, and pressure-flow study
 Received: 12 May 2016 Accepted: 13 May 2016 DOI 10.1002/nau.23124 REVIEW ARTICLE International Continence Society Good Urodynamic Practices and Terms 2016: Urodynamics, uroflowmetry, cystometry, and pressure-flow
Received: 12 May 2016 Accepted: 13 May 2016 DOI 10.1002/nau.23124 REVIEW ARTICLE International Continence Society Good Urodynamic Practices and Terms 2016: Urodynamics, uroflowmetry, cystometry, and pressure-flow
Glossary of terms Urinary Incontinence
 Patient Information English Glossary of terms Urinary Incontinence Anaesthesia (general, spinal, or local) Before a procedure you will get medication to make sure that you don t feel pain. Under general
Patient Information English Glossary of terms Urinary Incontinence Anaesthesia (general, spinal, or local) Before a procedure you will get medication to make sure that you don t feel pain. Under general
Tools for Evaluation. Urodynamics Case Studies. Case 1. Evaluation. Case 1. Bladder Diary SUI 19/01/2018
 Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN
 Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline
/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline") Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline TARGET POPULATION Eligibility Decidable (Y or N) Inclusion
Adult Urodynamics: American Urological Association (AUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) Guideline TARGET POPULATION Eligibility Decidable (Y or N) Inclusion
Clean Intermittent Self-Catheterisation (CISC)
") Saint Mary s Hospital & Trafford General Hospital Uro-gynaecology Service Information for Patients Clean Intermittent Self-Catheterisation (CISC) What is catheterisation? Catheterisation involves passing
Saint Mary s Hospital & Trafford General Hospital Uro-gynaecology Service Information for Patients Clean Intermittent Self-Catheterisation (CISC) What is catheterisation? Catheterisation involves passing
Paediatric Urotherapy Training
 Paediatric Urotherapy Training Frances Shit NS, MSc (Hons), ET, Dept. of Surgery, PWH, CUHK HKSAR Urinary Incontinence in Children Urine leakage in a child from 5 years of age Leakage occurs on a regular
Paediatric Urotherapy Training Frances Shit NS, MSc (Hons), ET, Dept. of Surgery, PWH, CUHK HKSAR Urinary Incontinence in Children Urine leakage in a child from 5 years of age Leakage occurs on a regular
Urogynecology Associates of Philadelphia URODYNAMIC TESTING
 URODYNAMIC TESTING Urogynecology Associates of Philadelphia Most women with urinary incontinence will need to complete a few simple tests, performed in the office, to help your doctor assess your symptoms
URODYNAMIC TESTING Urogynecology Associates of Philadelphia Most women with urinary incontinence will need to complete a few simple tests, performed in the office, to help your doctor assess your symptoms
Urodynamics in women. Aims of Urodynamics in women. Why do Urodynamics?
 Urodynamics in women Chendrimada Madhu MD, MA, MRCOG Subspecialty Trainee in Urogynaecology Southmead Hospital 2013 Aims of Urodynamics in women n Confirmation of incontinence and its cause n Definition
Urodynamics in women Chendrimada Madhu MD, MA, MRCOG Subspecialty Trainee in Urogynaecology Southmead Hospital 2013 Aims of Urodynamics in women n Confirmation of incontinence and its cause n Definition
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Male LUTS. Dr. Brian Ho. Division of Urology Department of Surgery Queen Mary Hospital
 Male LUTS Dr. Brian Ho Division of Urology Department of Surgery Queen Mary Hospital Mr. Siu M/78 Known to have HT & DM since 2008 on follow up with General ut-patient Clinic (GPC) Noticed to have worsening
Male LUTS Dr. Brian Ho Division of Urology Department of Surgery Queen Mary Hospital Mr. Siu M/78 Known to have HT & DM since 2008 on follow up with General ut-patient Clinic (GPC) Noticed to have worsening
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS
 Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
GUIDELINES ON NEURO-UROLOGY
 GUIDELINES ON NEURO-UROLOGY (Text update pril 2014) J. Pannek (co-chair), B. Blok (co-chair), D. Castro-Diaz, G. del Popolo, J. Groen, G. Karsenty, T.M. Kessler, G. Kramer, M. Stöhrer Eur Urol 2009 Jul;56(1):81-8
GUIDELINES ON NEURO-UROLOGY (Text update pril 2014) J. Pannek (co-chair), B. Blok (co-chair), D. Castro-Diaz, G. del Popolo, J. Groen, G. Karsenty, T.M. Kessler, G. Kramer, M. Stöhrer Eur Urol 2009 Jul;56(1):81-8
Urogynecology in EDS. Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018
 Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH
 MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
Prolapse and Urogynae Incontinence. Lucy Tiffin and Hannah Wheldon-Holmes
 Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
What should we consider before surgery? BPH with bladder dysfunction. Inje University Sanggye Paik Hospital Sung Luck Hee
 What should we consider before surgery? BPH with bladder dysfunction Inje University Sanggye Paik Hospital Sung Luck Hee Diagnostic tests in three categories Recommendation: there is evidence to support
What should we consider before surgery? BPH with bladder dysfunction Inje University Sanggye Paik Hospital Sung Luck Hee Diagnostic tests in three categories Recommendation: there is evidence to support
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital
 and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital") Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
April Clinical Focus Topic URINARY FREQUENCY
 April Clinical Focus Topic URINARY FREQUENCY This month I am focusing on a topic that may seem a little boring. But I would like to look at it from a less common perspective.urinary Frequency and its relationship
April Clinical Focus Topic URINARY FREQUENCY This month I am focusing on a topic that may seem a little boring. But I would like to look at it from a less common perspective.urinary Frequency and its relationship
Physiology & Neurophysiology of lower U.T.
 Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Prostate surgery. What is the prostate? What is a TURP? Why is a TURP operation necessary? Deciding to have a TURP operation.
 What is the prostate? The prostate is a gland about the size of a walnut that is only present in men. It is located just below the bladder and surrounds the urethra, the tube through which urine flows
What is the prostate? The prostate is a gland about the size of a walnut that is only present in men. It is located just below the bladder and surrounds the urethra, the tube through which urine flows
Urodynamic Patterns of the Idiopathic Overactive Bladder
 Science Journal of Clinical Medicine 2017; 6(5): 74-79 http://www.sciencepublishinggroup.com/j/sjcm doi: 10.11648/j.sjcm.20170605.12 ISSN: 2327-2724 (Print); ISSN: 2327-2732 (Online) Urodynamic Patterns
Science Journal of Clinical Medicine 2017; 6(5): 74-79 http://www.sciencepublishinggroup.com/j/sjcm doi: 10.11648/j.sjcm.20170605.12 ISSN: 2327-2724 (Print); ISSN: 2327-2732 (Online) Urodynamic Patterns
Using Physiotherapy to Manage Urinary Incontinence in Women
 Using Physiotherapy to Manage Urinary Incontinence in Women Bladder control problems are common, and affect people of all ages, genders and backgrounds. These problems are referred to as urinary incontinence
Using Physiotherapy to Manage Urinary Incontinence in Women Bladder control problems are common, and affect people of all ages, genders and backgrounds. These problems are referred to as urinary incontinence
Dysfunctional voiding
 Dysfunctional voiding The importance of assessment, diagnosis and treatment of dysfunctional voiding and its role in recurrent UTI Dr Dean Wallace Consultant Paediatric Nephrologist RMCH Objectives Development
Dysfunctional voiding The importance of assessment, diagnosis and treatment of dysfunctional voiding and its role in recurrent UTI Dr Dean Wallace Consultant Paediatric Nephrologist RMCH Objectives Development
GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION
 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E. Chartier-Kastler, G. Kramer, A. Mattiasson, J-J. Wyndaele Introduction NLUTD (neurogenic lower urinary
GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E. Chartier-Kastler, G. Kramer, A. Mattiasson, J-J. Wyndaele Introduction NLUTD (neurogenic lower urinary
CHAPTER 6. M.D. Eckhardt, G.E.P.M. van Venrooij, T.A. Boon. hoofdstuk :49 Pagina 89
 hoofdstuk 06 19-12-2001 09:49 Pagina 89 Urethral Resistance Factor (URA) Versus Schäfer s Obstruction Grade and Abrams-Griffiths (AG) Number in the Diagnosis of Obstructive Benign Prostatic Hyperplasia
hoofdstuk 06 19-12-2001 09:49 Pagina 89 Urethral Resistance Factor (URA) Versus Schäfer s Obstruction Grade and Abrams-Griffiths (AG) Number in the Diagnosis of Obstructive Benign Prostatic Hyperplasia
Neuropathic Bladder. Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014
 Neuropathic Bladder Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014 Plan Physiology- bladder and sphincter behaviour in neurological disease Clinical consequences of Symptoms
Neuropathic Bladder Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014 Plan Physiology- bladder and sphincter behaviour in neurological disease Clinical consequences of Symptoms
AN INTERNATIONAL UROGYNECOLOGICAL ASSOCIATION (IUGA) / INTERNATIONAL CONTINENCE SOCIETY (ICS) JOINT REPORT ON THE TERMINOLOGY
 / INTERNATIONAL CONTINENCE SOCIETY (ICS) JOINT REPORT ON THE TERMINOLOGY") AN INTERNATIONAL UROGYNECOLOGICAL ASSOCIATION (IUGA) / INTERNATIONAL CONTINENCE SOCIETY (ICS) JOINT REPORT ON THE TERMINOLOGY FOR FEMALE PELVIC FLOOR DYSFUNCTION Bernard T. Haylen *^, Dirk de Ridder #^,
AN INTERNATIONAL UROGYNECOLOGICAL ASSOCIATION (IUGA) / INTERNATIONAL CONTINENCE SOCIETY (ICS) JOINT REPORT ON THE TERMINOLOGY FOR FEMALE PELVIC FLOOR DYSFUNCTION Bernard T. Haylen *^, Dirk de Ridder #^,
Diagnostic approach to LUTS in men. Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center
 Diagnostic approach to LUTS in men Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center Classification of LUTS Storage symptoms Voiding symptoms Post micturition
Diagnostic approach to LUTS in men Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center Classification of LUTS Storage symptoms Voiding symptoms Post micturition
2 Voiding Dysfunction
 2 Voiding Dysfunction Diagnostic Evaluation Victor W. Nitti, MD and Michael Ficazzola, MD Contents Introduction Classification of Voiding Dysfunction History Physical Examination Laboratory Testing Simple
2 Voiding Dysfunction Diagnostic Evaluation Victor W. Nitti, MD and Michael Ficazzola, MD Contents Introduction Classification of Voiding Dysfunction History Physical Examination Laboratory Testing Simple
GUIDELINES ON NEURO-UROLOGY
 GUIDELINES ON NEURO-UROLOGY (Limited text update March 2015) B. Blok (Co-chair), J. Pannek (Co-chair), D. Castro Diaz, G. del Popolo, J. Groen, T. Gross (Guidelines ssociate), R. Hamid, G. Karsenty, T.M.
GUIDELINES ON NEURO-UROLOGY (Limited text update March 2015) B. Blok (Co-chair), J. Pannek (Co-chair), D. Castro Diaz, G. del Popolo, J. Groen, T. Gross (Guidelines ssociate), R. Hamid, G. Karsenty, T.M.
PRE-OPERATIVE URODYNAMIC
 PRE-OPERATIVE URODYNAMIC STUDIES: IS THERE VALUE IN PREDICTING POST-OPERATIVE STRESS URINARY INCONTINENCE IN WOMEN UNDERGOING PROLAPSE SURGERY? Dr K Janse van Rensburg Dr JA van Rensburg INTRODUCTION POP
PRE-OPERATIVE URODYNAMIC STUDIES: IS THERE VALUE IN PREDICTING POST-OPERATIVE STRESS URINARY INCONTINENCE IN WOMEN UNDERGOING PROLAPSE SURGERY? Dr K Janse van Rensburg Dr JA van Rensburg INTRODUCTION POP
Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M.
 UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
Recommandations de prise en charge des vessies neurogènes EAU 2006
 Annexe 4-1 Recommandations de prise en charge des vessies neurogènes EAU 2006 (Version courte) 685 686 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E.
Annexe 4-1 Recommandations de prise en charge des vessies neurogènes EAU 2006 (Version courte) 685 686 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E.
National Kidney and Urologic Diseases Information Clearinghouse
 Urodynamic Testing National Kidney and Urologic Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is the urinary tract? The urinary tract
Urodynamic Testing National Kidney and Urologic Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is the urinary tract? The urinary tract
Bill Landry BScPT, BScH, MCPA, CAFCI Family Physiotherapy Centre of London
 Bill Landry BScPT, BScH, MCPA, CAFCI blandry@fpclondon.com Family Physiotherapy Centre of London Objectives To describe the scope of post-prostatectomy incontinence To describe what s been done To provide
Bill Landry BScPT, BScH, MCPA, CAFCI blandry@fpclondon.com Family Physiotherapy Centre of London Objectives To describe the scope of post-prostatectomy incontinence To describe what s been done To provide
Video-urodynamics. P J R Shah Institute of Urology and UCH
 Video-urodynamics P J R Shah Institute of Urology and UCH Bladder Function Storage Capacity and Pressure Emptying Pressure/flow/emptying URODYNAMIC INVESTIGATIONS Free urine flow rate Urethral pressure
Video-urodynamics P J R Shah Institute of Urology and UCH Bladder Function Storage Capacity and Pressure Emptying Pressure/flow/emptying URODYNAMIC INVESTIGATIONS Free urine flow rate Urethral pressure
4. Know how to examine and name relevant test performed on patients
 Chapter 18 Female Urinary lncontinence Dr Zeelha Abdool Ed ucational Objectives : After completion of this chapter you should be able to: 1. Understand the pathophysiology of incontinence 2. Define and
Chapter 18 Female Urinary lncontinence Dr Zeelha Abdool Ed ucational Objectives : After completion of this chapter you should be able to: 1. Understand the pathophysiology of incontinence 2. Define and
15. Prevention of UTI and lifestyle modifications
 15. Prevention of UTI and lifestyle modifications Key questions: Does improving poor voiding habits help prevent UTI recurrence? Does improving constipation help prevent UTI recurrence? Does increasing
15. Prevention of UTI and lifestyle modifications Key questions: Does improving poor voiding habits help prevent UTI recurrence? Does improving constipation help prevent UTI recurrence? Does increasing
Bladder dysfunction in ALD and AMN
 Bladder dysfunction in ALD and AMN Sara Simeoni, MD Department of Uro-Neurology National Hospital for Neurology and Neurosurgery Queen Square, London 10:15 Dr Sara Simeoni- Bladder issues for AMN patients
Bladder dysfunction in ALD and AMN Sara Simeoni, MD Department of Uro-Neurology National Hospital for Neurology and Neurosurgery Queen Square, London 10:15 Dr Sara Simeoni- Bladder issues for AMN patients
TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Prolapse and Urogynae. By Sarah Rangan & Daniel Warrell
 Prolapse and Urogynae By Sarah Rangan & Daniel Warrell Anatomy and physiology of the pelvic supports The pelvic floor supports the pelvic viscera and vaginal, urethral and rectal openings Endopelvic fascial
Prolapse and Urogynae By Sarah Rangan & Daniel Warrell Anatomy and physiology of the pelvic supports The pelvic floor supports the pelvic viscera and vaginal, urethral and rectal openings Endopelvic fascial
Incontinence. When I was given this topic in urology to discuss with you today I
 Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT
 UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT Yunizaf, MD Division of Urogynecology Department of Obstetrics and Gynecology School of Medicine, University of Indonesia/ Dr. Cipto Mangunkusumo Hospital
UP DATE MANAGEMENT OF URINARY INCONTINENCE IN ADULT Yunizaf, MD Division of Urogynecology Department of Obstetrics and Gynecology School of Medicine, University of Indonesia/ Dr. Cipto Mangunkusumo Hospital
Objectives. Prevalence of Urinary Incontinence URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS
 URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
Overactive bladder can result from one or more of the following causes:
 Overactive bladder can affect people of any age; however, it is more common in older people. Effective treatments are available and seeing your doctor for symptoms of overactive bladder often results in
Overactive bladder can affect people of any age; however, it is more common in older people. Effective treatments are available and seeing your doctor for symptoms of overactive bladder often results in
An International Continence Society (ICS) report on the terminology for adult neurogenic lower urinary tract dysfunction (ANLUTD)
 report on the terminology for adult neurogenic lower urinary tract dysfunction (ANLUTD)") Received: 20 July 2017 Accepted: 3 August 2017 DOI: 10.1002/nau.23397 SOUNDING BOARD An International Continence Society (ICS) report on the terminology for adult neurogenic lower urinary tract dysfunction
Received: 20 July 2017 Accepted: 3 August 2017 DOI: 10.1002/nau.23397 SOUNDING BOARD An International Continence Society (ICS) report on the terminology for adult neurogenic lower urinary tract dysfunction
Urodynamic Testing National Kidney and Urologic Diseases Information Clearinghouse
 Urodynamic Testing National Kidney and Urologic Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Urodynamic Testing National Kidney and Urologic Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
5/29/2015. Objectives. Functions of the PFM. Various phases of PFM. Evaluation of the PFM
 The Physical Therapist s Approach to the Female Pelvic Floor Musculature Examination and Treatment. Presented By: Evelyne Burtis, DPT Objectives Core and pelvic floor muscles (PFM) Functions of the PFM
The Physical Therapist s Approach to the Female Pelvic Floor Musculature Examination and Treatment. Presented By: Evelyne Burtis, DPT Objectives Core and pelvic floor muscles (PFM) Functions of the PFM
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives
 Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives 1 Aims of this self assessment competency To equip Midwives with the knowledge and skills to teach pelvic floor
Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives 1 Aims of this self assessment competency To equip Midwives with the knowledge and skills to teach pelvic floor
Urinary incontinence. Urology Department. Patient Information Leaflet
 Urinary incontinence Urology Department Patient Information Leaflet Introduction This leaflet is for people who have been diagnosed with urinary incontinence. It contains information about the bladder,
Urinary incontinence Urology Department Patient Information Leaflet Introduction This leaflet is for people who have been diagnosed with urinary incontinence. It contains information about the bladder,
Continence Promotion in
 Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Spinal Cord Injury. R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH
 Spinal Cord Injury R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH SCI 800 1000 new cases per year in UK Car accidents 35%
Spinal Cord Injury R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH SCI 800 1000 new cases per year in UK Car accidents 35%
I am certain readers will find Voiding Dysfunction: Diagnosis and Treatment informative, practical, and clinically relevant. Rodney A.
 PREFACE The purpose of Voiding Dysfunction: Diagnosis and Treatment is to bring the reader up-to-date on all clinical apsects of voiding dysfunction, not just urodynamic and other evaluative techniques,
PREFACE The purpose of Voiding Dysfunction: Diagnosis and Treatment is to bring the reader up-to-date on all clinical apsects of voiding dysfunction, not just urodynamic and other evaluative techniques,
Loss of Bladder Control
 BLADDER HEALTH: Surgery for Urinary Incontinence Loss of Bladder Control Surgery for Urinary Incontinence Don t Let Urinary Incontinence Keep You from Enjoying Life. What is Urinary Incontinence? What
BLADDER HEALTH: Surgery for Urinary Incontinence Loss of Bladder Control Surgery for Urinary Incontinence Don t Let Urinary Incontinence Keep You from Enjoying Life. What is Urinary Incontinence? What
Content. Terminology Anatomy Aetiology Presentation Classification Management
 Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
The Standardisation of Terminology of Lower Urinary Tract Function: Pressure-Flow Studies of Voiding, Urethral Resistance and Urethral Obstruction
 The Standardisation of Terminology of Lower Urinary Tract Function: Pressure-Flow Studies of Voiding, Urethral Resistance and Urethral Obstruction 1. Introduction 2. Evaluation of Micturition 2.1. Pressure
The Standardisation of Terminology of Lower Urinary Tract Function: Pressure-Flow Studies of Voiding, Urethral Resistance and Urethral Obstruction 1. Introduction 2. Evaluation of Micturition 2.1. Pressure
Original Article. Annals of Rehabilitation Medicine INTRODUCTION
 Original Article Ann Rehabil Med 2014;38(3):342-346 pissn: 2234-0645 eissn: 2234-0653 http://dx.doi.org/10.5535/arm.2014.38.3.342 Annals of Rehabilitation Medicine Phasic Changes in Bladder Compliance
Original Article Ann Rehabil Med 2014;38(3):342-346 pissn: 2234-0645 eissn: 2234-0653 http://dx.doi.org/10.5535/arm.2014.38.3.342 Annals of Rehabilitation Medicine Phasic Changes in Bladder Compliance
Disease Management. Incontinence Care. Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09
 Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
Incontinence: Risks, Causes and Care
 Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
ICD-10 Common Codes for Pelvic Rehab Providers
 ICD-10 Common Codes for Pelvic Rehab Providers With ICD-10 changes taking place in 2015, we thought it would be helpful to put together a bit of a cheat sheet for our pelvic health providers. Keep in mind
ICD-10 Common Codes for Pelvic Rehab Providers With ICD-10 changes taking place in 2015, we thought it would be helpful to put together a bit of a cheat sheet for our pelvic health providers. Keep in mind
Northwest Rehabilitation Associates, Inc.
 Pelvic Health Patient Intake Form Name: Date: Please answer the following questions as honestly and thoroughly as you can. Your responses will help us better understand your condition and provide the best
Pelvic Health Patient Intake Form Name: Date: Please answer the following questions as honestly and thoroughly as you can. Your responses will help us better understand your condition and provide the best
This Special Report supplement
 ...INTRODUCTION... Overactive Bladder: Defining the Disease Alan J. Wein, MD This Special Report supplement to The American Journal of Managed Care features proceedings from the workshop, Overactive Bladder:
...INTRODUCTION... Overactive Bladder: Defining the Disease Alan J. Wein, MD This Special Report supplement to The American Journal of Managed Care features proceedings from the workshop, Overactive Bladder:
4) Urinary Incontinence - Dr. Abeer
 Urinary Incontinence - Dr. Abeer") 4) Urinary Incontinence - Dr. Abeer INTRODUCTION Involuntary loss of urine Social and hygienic problem It affects individuals physical, psychological and social which is associated with a significant reduction
4) Urinary Incontinence - Dr. Abeer INTRODUCTION Involuntary loss of urine Social and hygienic problem It affects individuals physical, psychological and social which is associated with a significant reduction
Summary. Neuro-urodynamics. The bladder cycle. and voiding. 14/12/2015. Neural control of the LUT Initial assessment Urodynamics
 Neuro-urodynamics Summary Neural control of the LUT Initial assessment Urodynamics Marcus Drake, Bristol Urological Institute SAFETY FIRST; renal failure, dysreflexia, latex allergy SYMPTOMS SECOND; storage,
Neuro-urodynamics Summary Neural control of the LUT Initial assessment Urodynamics Marcus Drake, Bristol Urological Institute SAFETY FIRST; renal failure, dysreflexia, latex allergy SYMPTOMS SECOND; storage,
Postpartum Complications
 ACOG Postpartum Toolkit Postpartum Complications Introduction The effects of pregnancy on many organ systems begin to resolve spontaneously after birth of the infant and delivery of the placenta. The timeline
ACOG Postpartum Toolkit Postpartum Complications Introduction The effects of pregnancy on many organ systems begin to resolve spontaneously after birth of the infant and delivery of the placenta. The timeline
Urodynamics Assessment & Urotherapy in Children
 Urodynamics Assessment & Urotherapy in Children APN Ng Wai Hing Department of Surgery QEH Nursing Management in Children with Nocturnal Enuresis Assessment Investigations Urotherapy Program Support Urodynamic
Urodynamics Assessment & Urotherapy in Children APN Ng Wai Hing Department of Surgery QEH Nursing Management in Children with Nocturnal Enuresis Assessment Investigations Urotherapy Program Support Urodynamic
Overactive Bladder Syndrome
 Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Managing Female Urinary Incontinence Within Primary Care
 Managing Female Urinary Incontinence Within Primary Care Angela Patterson Lead Clinical Nurse Specialist in Bladder and Bowel Dysfunction. South Eastern HSCT Background More than 14 million in the UK affected
Managing Female Urinary Incontinence Within Primary Care Angela Patterson Lead Clinical Nurse Specialist in Bladder and Bowel Dysfunction. South Eastern HSCT Background More than 14 million in the UK affected
Module 5 Management Of Urinary Incontinence
 Management Of Urinary Incontinence V3: Last Reviewed September 2017 Learning Outcomes Outline conservative management options Discover the options available to manage the different types of incontinence
Management Of Urinary Incontinence V3: Last Reviewed September 2017 Learning Outcomes Outline conservative management options Discover the options available to manage the different types of incontinence
Involuntary Detrusor Contractions: Correlation of Urodynamic Data to Clinical Categories
 Neurourology and Urodynamics 20:249±257 (2001) Involuntary Detrusor Contractions: Correlation of Urodynamic Data to Clinical Categories Lauri J. Romanzi, Asnat Groutz, Dianne M. Heritz, and Jerry G. Blaivas*
Neurourology and Urodynamics 20:249±257 (2001) Involuntary Detrusor Contractions: Correlation of Urodynamic Data to Clinical Categories Lauri J. Romanzi, Asnat Groutz, Dianne M. Heritz, and Jerry G. Blaivas*