Dr. M.Etminani-Esfahani AJUMS
|
|
|
- Harry Warren
- 5 years ago
- Views:
Transcription

1 Dr. M.Etminani-Esfahani AJUMS
2 Introduction Problems related to the menstrual cycle are exceedingly common in women of reproductive age. Amenorrhea Menorrhagia Anovulatory bleeding Dysmenorrhea Premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD)
3 The need for effective treatments because of impact on: Reduced quality of life Negative effects on reproductive health Long-term detrimental health effects, such as osteoporosis with amenorrhea and cardiovascular disease with polycystic ovary syndrome (PCOS).

4 فیزیولوژی سیستم تولید مثلی زنانه: سیکل ماهیانه Cycle( :)Menstrual مکبویسم بی خ د تىظیمی بی ل صیک اوذام بی سیز را شبمل می ش وذ: یپ تبالم س غذ یپ فیش قذامی تخمذان ب الی اوذيمتز رحم. ایه ب بب کمک یکذیگز سیکل 28 ريس را ب يج د می آيروذ. یپ تبالم س GnRH را سىتش کزد ي ب ص رت پبلسی تزشح می کىذ. GnRH ببعث تحزیک سىتش ي تزشح رم ن بی LH, FSH می ش د. LH, FSH ببعث تحزیک تزشح رم ن بی استزيصن ي پزيصستزين اس تخمذان بمی ش وذ. استزيصن ي پزيصستزين بب مکبویسم فیذبک مىفی ببعث م بر تزشح LH,FSH اس یپ فیش می ش د. سیکل مب یبو ب 3 فبس تقسیم می ش د: فبس ف لیک لی تخمک گذاری فبس ل تئبل

5 Menstrual Flow Proliferative Phase Secretory Phase
6
7 Amenorrhea Primary absence of menses by age 16 years in normal secondary sexual development OR absence of menses by age 14 in the absence of normal secondary sexual development Secondary absence of menses for three cycles OR for 6 months in a previously menstruating woman There is a significant amount of overlap between the two.
8 Etiology Consider the organs involved in the menstrual cycle, which include the uterus, ovaries, anterior pituitary, and hypothalamus.
9 Unrecognized pregnancy: the most common cause A urine pregnancy test After excluding pregnancy, the most common causes of secondary amenorrhea are: o hypothalamic suppression o chronic anovulation o Hyperprolactinemia o ovarian failure o uterine disorders
10 Uterus/Outflow Tract Several anatomic abnormalities may cause amenorrhea. If primary amenorrhea, a congenital anomaly such as imperforate hymen or uterine agenesis may be present and often discovered by physical examination. An acquired condition of the genital tract, such as Asherman syndrome or cervical stenosis, is more likely in secondary amenorrhea.
 and luteinizing hormone (LH) by secreting estrogen and")
11 Ovaries Normal ovarian function is critical for menstruation to occur. The ovaries must respond appropriately to folliclestimulating hormone (FSH) and luteinizing hormone (LH) by secreting estrogen and progesterone in proper sequence to influence endometrial growth and shedding.
12 Pituitary Gland The anterior pituitary gland secretes FSH and LH in sequential fashion in response to hypothalamic stimulation and a complex ovarian feedback mechanism. Normal secretion of FSH and LH is altered by several endocrinologic and iatrogenic conditions, including thyroid disease, hyperprolactinemia, and dopaminergic drug administration.
13 Hypothalamus The hypothalamus secretes cyclic gonadotropinreleasing hormone (GnRH), which causes the pituitary to produce FSH and LH. Disrupting this cyclic excretion will interrupt the hormonal cascade that results in normal menstruation. Anorexia nervosa, bulimia, intense exercise, and stress may cause hypothalamic amenorrhea.
14 Clinical Presentation of Amenorrhea Symptoms Complain of cessation of menses Complain of infertility, vaginal dryness, or decreased libido

15 Signs Cessation of menses Recent significant weight loss or weight gain Presence of acne, hirsutism, hair loss, or acanthosis nigrans may suggest androgen excess
16 Laboratory Tests Pregnancy test Thyroid-stimulating hormone Prolactin If PCOS is suspected, free or total testosterone, 17- hydroxyprogesterone, fasting glucose, fasting lipid panel If suspect premature ovarian failure, FSH, LH
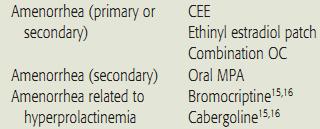
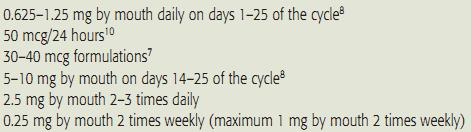
17 Treatment The treatment options for amenorrhea are as varied as its causes. For hypoestrogenic conditions estrogen (with a progestin) is provided. It can be administered as an oral contraceptive (OC), conjugated equine estrogen, or estradiol patch. Estrogen therapy reduces osteoporosis risk and improves quality of life.
18 When hyperprolactinemia is the cause of amenorrhea, dopamine agonists, including bromocriptine and cabergoline reducing prolactin Bromocriptine requires multiple doses per day Cabergoline is dosed twice weekly Bromocriptine is less effective in normalizing prolactin and has a higher incidence of adverse events

19 Amenorrhea related to PCOS-induced anovulation may respond to agents that reduce insulin resistance. Metformin and the thiazolidinediones for this purpose are discussed in the anovulatory bleeding section.
20 Progestins induce withdrawal bleeding in women with secondary amenorrhea. Several factors predict progesterone's efficacy for this purpose: Estrogen concentrations greater than or equal to 35 pg/ml (128 pmol/l) Endometrial thickness (greater initial thickness resulting in more withdrawal bleeding).
21 Progesterone in oil administered intramuscularly results in withdrawal bleeding in 70% of treated patients Oral medroxyprogesterone acetate (MPA) induces withdrawal bleeding in 95% of treated patients.
22

23
24 Menstrual blood loss greater than 80 ml/cycle This definition has been questioned because of several factors, including difficulty quantifying menstrual loss in clinical practice.

25 Menorrhagia rates in healthy women range from 9% to 14%.
26 Symptoms Patients may complain of heavy/prolonged menstrual flow. Signs of fatigue and lightheadedness in cases of severe blood loss. These symptoms may or may not occur with dysmenorrhea.

27 Signs Orthostasis Tachycardia Pallor may


28 Initial treatment choice for menorrhagia is influenced by whether or not the woman desires to become pregnant
29 Nonsteroidal antiinflammatory drugs (NSAIDs) have the advantage of administration only during menses. NSAID use is associated with a 20% to 50% reduction in blood loss in 75% of treated women. This choice is convenient (only taken during menses) and comparatively inexpensive

30 For women desiring to avoid pregnancy, OC use is beneficial for menorrhagia. A 43% to 53% reduction in menstrual blood loss has been observed in 68% of menorrhagia patients treated with OCs containing greater than or equal to 35 mcg of estradiol. The reduction in menorrhagia-related blood loss with use of NSAIDs and OCs is directly proportional to the amount of pretreatment blood loss.

31 Levonorgestrel-releasing intrauterine device (IUD) very effective treatment that consistently reduces menstrual flow by at least 90%. Progesterone therapy either during the luteal phase of the menstrual cycle or for 21 days, starting on day 5 after onset of menses, results in a 32% to 50% reduction in menstrual blood loss. Tranexamic acid Its use is associated with a significant 40% to 50% reduction in menstrual blood loss.
32

33
34 Bleeding from the uterine endometrium as a result of a dysfunctioning menstrual system, specifically excluding an anatomic lesion of the uterus. Anovulatory bleeding is also referred to as dysfunctional or irregular uterine bleeding.

35
36 PCOS can present as a variety of menstruation disorders, including amenorrhea, menorrhagia, and/or anovulatory bleeding. It is a disorder of androgen excess that often includes polycystic ovarian morphology and ovulatory dysfunction.
37 It is a significant risk factor for the metabolic syndrome, type 2 diabetes, dyslipidemia, hypertension, and possibly cardiovascular disease. PCOS is a common cause of ovulation dysfunction in adult women. Other common causes: Hyperprolactinemia Hypothalamic amenorrhea Hypogonadotropic hypogonadism Premature ovarian failure Thyroid dysfunction


38
39 Normal menstrual cycles occur through a complex interaction of the hypothalamus, pituitary gland, ovaries, and endometrium. In an ovulatory cycle, the ovary produces a mature, estrogen-secreting follicle in response to FSH release from the pituitary. The endometrium proliferates under the influence of this estrogen production.

40 At a critical level of estrogen concentration, the pituitary responds by producing an "LH surge," which creates a cascade of ovarian events, culminating in ovulation. Upon oocyte release, the follicle becomes a progesterone-producing corpus luteum. The endometrium "organizes" into secretory endometrium in the presence of adequate progesterone.
41 If conception and implantation do not occur, corpus luteum involution causes a decline in estrogen and progesterone leading to predictable, organized menstrual flow as the endometrium sloughs.

42 If ovulation does not occur, progesterone is not produced, and the endometrium will continue to proliferate in an "unorganized" fashion under the influence of continued estrogen production. Eventually the endometrium will become so thick that it can no longer be supported by continued estrogen production. This results in unorganized, sporadic sloughing of the endometrium, characteristic of the unpredictable and heavy bleeding of anovulation.
43 Anovulation has several etiologies. In adolescence, hypothalamic pituitary axis immaturity contributes to the absence of the LH surge required for ovulation. In the anorexic patient, the hypothalamus loses much of its pulsatile GnRH release, leading to low levels of FSH and LH, enough for estrogen production but not enough to induce ovulation.
 Signs Acne, hirsutism,")
44 Symptoms Irregular, heavy, or prolonged vaginal bleeding, perimenopausal symptoms (hot flashes, night sweats, vaginal dryness) Signs Acne, hirsutism, obesity
.")
45 Optimizing anovulatory bleeding therapy depends on accurate identification of the disorder's cause(s). The treatment options for anovulatory bleeding are wide and varied.

46 Estrogen : Recommended treatment for managing acute severe bleeding episodes because it promotes endometrial stabilization. Following, therapy continuation may be necessary to prevent future occurrences. OC use fulfills this role and contributes to predictable menstrual cycles.

47 OCs : Prevent recurrent anovulatory bleeding by providing a progestin and suppressing ovarian hormones and adrenal androgen production. They also, indirectly, increase SHBG. SHBG binds androgens and reduces their circulating free concentrations.
48 For women with high androgen levels and its related signs such as hirsutism (PCOS), OCs containing less than or equal to 35 mcg of ethinyl estradiol and a progesterone that exhibits minimal androgenic side effects (norgestimate and desogestrel) or with antiandrogenic effects (drospirenone) may be desirable.


49 Managing the acne and hirsutism Suppress ovarian androgen production and increase sex hormone binding globulin Reducing testosterone free concentrations Controversy : potential adverse effects on insulin resistance, glucose tolerance, vascular reactivity, and coagulability. Additional, longer-term clinical trials will identify whether the benefits of these agents outweigh the risks.

50 In women with contraindication(s) to estrogen or in whom the side effects are unacceptable, progesterone-only products are an option. Metformin and the thiazolidinediones, including pioglitazone and rosiglitazone, improve insulin sensitivity. In patients with PCOS, this contributes to reduced circulating androgen concentrations, increased ovulation rates, and improved glucose tolerance. Metformin is pregnancy category B, and pioglitazone and rosiglitazone are category C.
51 If the treatment goal is improved fertility via ovulation induction, clomiphene citrate is an option. Treatment with 50 mg/day for 5 days can be initiated between menstrual cycle days 3 and 5. This often occurs after inducing withdrawal bleeding with a progesterone such as MPA 10 mg daily orally for 10 days. If ovulation does not occur with this dose of clomiphene, a dose of 100 mg/day is warranted. In rare instances, it may be increased by 50 mg increments up to 250 mg/day.
52
53 Dysmenorrhea is one of the most commonly encountered gynecologic complaints. It is defined as crampy pelvic pain occurring with or just prior to menses. 1. Primary dysmenorrhea implies pain in the setting of normal pelvic anatomy and physiology. 2. Secondary dysmenorrhea is associated with underlying pelvic pathology.



54 Dysmenorrhea prevalence rates range from 16% to 90%. Its presence may be associated with significant interference in work and school attendance. Risk factors include young age, heavy menses, nulliparity, early menarche, and cigarette smoking

55 For most patients, dysmenorrhea is associated with normal ovulatory cycles and normal pelvic anatomy. This is referred to as primary, or functional, dysmenorrhea. However, in approximately 10% of the adolescents and young adults presenting with painful menses, an underlying anatomic or physiologic cause exists.


56 Release of prostaglandins and leukotrienes into the menstrual fluid, initiating an inflammatory response and possibly vasopressin-mediated vasoconstriction. Causes of secondary dysmenorrhea include cervical stenosis, endometriosis, pelvic infections, pelvic congestion syndrome, uterine or cervical polyps, uterine fibroids, genital outflow tract obstructions, and pelvic adhesions.
57 Topical heat therapy Exercise Low-fat vegetarian diet have been shown to reduce dysmenorrhea intensity. Topical heat application via an abdominal patch worn for 12 consecutive hours/day is as effective as 400 mg of ibuprofen dosed 3 times daily.
58 NSAIDs are the initial treatment of choice. These agents do not differ in efficacy. The most commonly used agents are naproxen and ibuprofen. Choice of one agent over another may be based on cost, convenience, and patient preference. All NSAIDs have a propensity for causing gastrointestinal distress and ulceration; their administration with food or milk minimizes these effects.
59 In women who have a history of NSAID-induced gastric effects, the use of celecoxib, a cyclooxygenase 2 (COX-2) inhibitor, is an alternative. Some research suggests that NSAID therapy should begin at the onset of menses or perhaps even the day before and continued around the clock instead of waiting until symptom onset. If an NSAID or celecoxib use is contraindicated or not desired, hormonal agents should be considered. Acetaminophen is inferior to NSAID in treatment of this disorder.
60 OCs improve dysmenorrhea by inhibiting endometrial tissue proliferation which reduces endometrial-derived prostaglandins that cause the pelvic pain. Significant improvements in mild, moderate, and severe dysmenorrhea have been noted with OCs.
61 Depot MPA can be considered for dysmenorrhea treatment. Because the pelvic pain of dysmenorrhea is related to the prostaglandins released during menses, in the setting of amenorrhea the underlying cause of dysmenorrhea is removed. Levonorgestrel-releasing IUD

62
63 PMS is a constellation of symptoms including mild mood disturbances and physical symptoms occurring prior to menses and resolving with menses initiation.
64 Up to 75% of menstruating women experience PMS symptoms. However, a spectrum of premenstrual mood disturbances exists, and PMDD is the most severe. Approximately 3% to 8% of women have PMDD.
65 PMDD is a complex psychiatric disorder with multiple biological, psychological, and sociocultural determinants. Some evidence suggests that PMS and PMDD symptoms are related to low levels of the centrally active progesterone metabolite in the luteal phase and/or lower cortical - aminobutyric acid levels in the follicular phase. A number of studies suggest a link between PMS and PMDD and low serotonin levels.
66 A summary of the American Psychiatric Association's criteria for PMDD is as follows: 1. Symptoms are temporally associated with the last week of the luteal phase and remit with onset of menses. 2. At least five of the following symptoms are present: markedly depressed mood, marked anxiety, marked affective lability, marked anger or irritability, decreased interest in activities, fatigue, difficulty concentrating, changes in appetite, sleep disturbance, feelings of being overwhelmed, and physical symptoms, such as breast tenderness or bloating.
67 3. One of the symptoms must be markedly depressed mood, anxiety, irritability, or affective lability. 4. Symptoms interfere significantly with work and/or social relationships. 5. Symptoms are not an exacerbation of another underlying psychiatric disorder. 6. The criteria are confirmed prospectively by daily ratings over two menstrual cycles.
68 Miss significantly more work and school than do controls. Report significant impairment of their ability to participate in social activities and hobbies and in their relationships with others. Given this, the need for effective treatment modalities is clear.
69 Some lifestyle changes for women with mild-tomoderate premenstrual symptoms include minimizing intake of caffeine, refined sugar, and sodium and increasing exercise. Vitamin and mineral supplements, such as vitamin B6 ( mg daily) and calcium carbonate (1,200 mg daily), may help reduce the physical symptoms associated with PMS.
70 A clinical trial review concludes that the following options lack efficacy and safety data and should not be recommended: herbal medicines, homeopathic remedies, dietary supplements, relaxation, massage therapy, reflexology, chiropractic treatments, and biofeedback.

71 If symptoms persist after 2 months of symptom charting and lifestyle modifications, pharmacologic therapy for PMDD management is warranted. Over the past decade, SSRIs have been studied significantly for this disorder. Studies have revealed very positive results relative to most symptoms associated with PMDD.
72 Clomipramine Venlafaxine GnRH agonist, such as leuprolide Leuprolide OC containing 20 mcg of ethinyl estradiol and 3 mg of drospirenone, a progesterone with antiandrogenic effects, improves premenstrual symptoms in women with PMDD.

73
CASE 41. What is the pathophysiologic cause of her amenorrhea? Which cells in the ovary secrete estrogen?
 CASE 41 A 19-year-old woman presents to her gynecologist with complaints of not having had a period for 6 months. She reports having normal periods since menarche at age 12. She denies sexual activity,
CASE 41 A 19-year-old woman presents to her gynecologist with complaints of not having had a period for 6 months. She reports having normal periods since menarche at age 12. She denies sexual activity,
Abnormal Uterine Bleeding Case Studies
 Case Study 1 Abnormal Uterine Bleeding Case Studies Abigail, a 24 year old female, presents to your office complaining that her menstrual cycles have become a problem. They are now lasting 6 7 days instead
Case Study 1 Abnormal Uterine Bleeding Case Studies Abigail, a 24 year old female, presents to your office complaining that her menstrual cycles have become a problem. They are now lasting 6 7 days instead
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018
 Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Hormonal Control of Human Reproduction
 Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Polycystic Ovarian Syndrome (PCOS) LOGO
 LOGO") Polycystic Ovarian Syndrome (PCOS) Ma qianhong Ob/Gyn Department LOGO Contents Epidemiology and Definition Pathophysiology, Endocrinological Features Diagnostic Criteria Treatment Prognosis Introduction
Polycystic Ovarian Syndrome (PCOS) Ma qianhong Ob/Gyn Department LOGO Contents Epidemiology and Definition Pathophysiology, Endocrinological Features Diagnostic Criteria Treatment Prognosis Introduction
Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital
 Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital Touchdown to CME Eighth District Academy of Osteopathic Medicine & Surgery October 8. 2017 Goals
Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital Touchdown to CME Eighth District Academy of Osteopathic Medicine & Surgery October 8. 2017 Goals
12/13/2017. Important references for PCOS. Polycystic Ovarian Syndrome (PCOS) for the Family Physician. 35 year old obese woman
 for the Family Physician. 35 year old obese woman") Polycystic Ovarian Syndrome (PCOS) for the Family Physician Barbara S. Apgar MD, MS Professor or Family Medicine University of Michigan Ann Arbor, Michigan Important references for PCOS Endocrine Society
Polycystic Ovarian Syndrome (PCOS) for the Family Physician Barbara S. Apgar MD, MS Professor or Family Medicine University of Michigan Ann Arbor, Michigan Important references for PCOS Endocrine Society
Overview of Reproductive Endocrinology
 Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
1. During the follicular phase of the ovarian cycle, the hypothalamus releases GnRH.
 1. During the follicular phase of the ovarian cycle, the hypothalamus releases GnRH. 2. This causes the anterior pituitary to secrete small quantities of FSH and LH. 3. At this time, the follicles in the
1. During the follicular phase of the ovarian cycle, the hypothalamus releases GnRH. 2. This causes the anterior pituitary to secrete small quantities of FSH and LH. 3. At this time, the follicles in the
Polycystic Ovary Syndrome
 Polycystic Ovary Syndrome Definition: the diagnostic criteria Evidence of hyperandrogenism, biochemical &/or clinical (hirsutism, acne & male pattern baldness). Ovulatory dysfunction; amenorrhoea; oligomenorrhoea
Polycystic Ovary Syndrome Definition: the diagnostic criteria Evidence of hyperandrogenism, biochemical &/or clinical (hirsutism, acne & male pattern baldness). Ovulatory dysfunction; amenorrhoea; oligomenorrhoea
Infertility DR. RAHUL BEVARA
 Infertility DR. RAHUL BEVARA Definitions Infertility is defined as the inability to conceive after one year of unprotected coitus. Affects 10-15% of couples Primary Infertility, that is inability to conceive
Infertility DR. RAHUL BEVARA Definitions Infertility is defined as the inability to conceive after one year of unprotected coitus. Affects 10-15% of couples Primary Infertility, that is inability to conceive
SAMPLE REPORT. Order Number: PATIENT. Age: 40 Sex: F MRN:
 Patient: Age: 40 Sex: F MRN: SAMPLE PATIENT Order Number: Completed: Received: Collected: SAMPLE REPORT Progesterone ng/ml 0.34 0.95 21.00 DHEA-S mcg/dl Testosterone ng/ml 48 35 0.10 0.54 0.80 430 Sex
Patient: Age: 40 Sex: F MRN: SAMPLE PATIENT Order Number: Completed: Received: Collected: SAMPLE REPORT Progesterone ng/ml 0.34 0.95 21.00 DHEA-S mcg/dl Testosterone ng/ml 48 35 0.10 0.54 0.80 430 Sex
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal myomectomy in leiomyoma management, 77 Abnormal uterine bleeding (AUB) described, 103 105 normal menstrual bleeding vs., 104
Index Note: Page numbers of article titles are in boldface type. A Abdominal myomectomy in leiomyoma management, 77 Abnormal uterine bleeding (AUB) described, 103 105 normal menstrual bleeding vs., 104
POTION OR POISON? MEDICAL TREATMENT ALTERNATIVES TO THE PILL. Lester Ruppersberger, D.O., FACOOG,CNFPI NFP only Gynecologist
 POTION OR POISON? MEDICAL TREATMENT ALTERNATIVES TO THE PILL Lester Ruppersberger, D.O., FACOOG,CNFPI NFP only Gynecologist THE PILL Released to US market in 1960 10-15 x dose of hormones in HRT Over 10-14
POTION OR POISON? MEDICAL TREATMENT ALTERNATIVES TO THE PILL Lester Ruppersberger, D.O., FACOOG,CNFPI NFP only Gynecologist THE PILL Released to US market in 1960 10-15 x dose of hormones in HRT Over 10-14
Female Reproductive System. Lesson 10
 Female Reproductive System Lesson 10 Learning Goals 1. What are the five hormones involved in the female reproductive system? 2. Understand the four phases of the menstrual cycle. Human Reproductive System
Female Reproductive System Lesson 10 Learning Goals 1. What are the five hormones involved in the female reproductive system? 2. Understand the four phases of the menstrual cycle. Human Reproductive System
Frequency of menses. Duration of menses 3 days to 7 days. Flow/amount of menses Average blood loss with menstruation is 60-80cc.
 Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
PCOS and Obesity DUB is better treated by OCPs
 PCOS and Obesity DUB is better treated by OCPs Dr. Ritu Joshi Senior consultant Fortis escorts Hospital, Jaipur Chairperson Family welfare com. FOGSI (20092012) Vice President FOGSI 2014 Introduction One
PCOS and Obesity DUB is better treated by OCPs Dr. Ritu Joshi Senior consultant Fortis escorts Hospital, Jaipur Chairperson Family welfare com. FOGSI (20092012) Vice President FOGSI 2014 Introduction One
PERIMENOPAUSE. Objectives. Disclosure. The Perimenopause Perimenopause Menopause. Definitions of Menopausal Transition: STRAW.
 PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
Estrogens and progestogens
 Estrogens and progestogens Estradiol and Progesterone hormones produced by the gonads are necessary for: conception embryonic maturation development of primary and secondary sexual characteristics at puberty.
Estrogens and progestogens Estradiol and Progesterone hormones produced by the gonads are necessary for: conception embryonic maturation development of primary and secondary sexual characteristics at puberty.
Infertility: failure to conceive within one year of unprotected regular sexual intercourse. Primary secondary
 Subfertility Infertility: failure to conceive within one year of unprotected regular sexual intercourse. Primary secondary Infertility affects about 15 % of couples. age of the female. Other factors that
Subfertility Infertility: failure to conceive within one year of unprotected regular sexual intercourse. Primary secondary Infertility affects about 15 % of couples. age of the female. Other factors that
CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology
 CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology A 49-year-old woman complains of irregular menses over the past 6 months, feelings of inadequacy, vaginal dryness, difficulty sleeping, and episodes
CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology A 49-year-old woman complains of irregular menses over the past 6 months, feelings of inadequacy, vaginal dryness, difficulty sleeping, and episodes
Investigation: The Human Menstrual Cycle Research Question: How do hormones control the menstrual cycle?
 Investigation: The Human Menstrual Cycle Research Question: How do hormones control the menstrual cycle? Introduction: The menstrual cycle (changes within the uterus) is an approximately 28-day cycle that
Investigation: The Human Menstrual Cycle Research Question: How do hormones control the menstrual cycle? Introduction: The menstrual cycle (changes within the uterus) is an approximately 28-day cycle that
lactotrophs 120 min- FSH 60 min- LH Hypothalamus GnRH pituitary Estradiol +/- Progesterone _ FSH L H Ovary Uterus Ovulation Antral follicle >2mm
 lactotrophs Hypothalamus GnRH 120 min- 60 min- LH Progesterone _ pituitary L H + Ovary + Estradiol +/- Uterus Antral follicle >2mm Ovulation Preovulatory follicles atresia Follicular phase Luteal phase
lactotrophs Hypothalamus GnRH 120 min- 60 min- LH Progesterone _ pituitary L H + Ovary + Estradiol +/- Uterus Antral follicle >2mm Ovulation Preovulatory follicles atresia Follicular phase Luteal phase
Sexual dysfunction of chronic kidney disease. Razieh salehian.md psychiatrist
 Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Topics. Periods Menopause & HRT Contraception Vulva problems
 Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Reproductive System. Testes. Accessory reproductive organs. gametogenesis hormones. Reproductive tract & Glands
 Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
9.4 Regulating the Reproductive System
 9.4 Regulating the Reproductive System The Reproductive System to unite a single reproductive cell from a female with a single reproductive cell from a male Both male and female reproductive systems include
9.4 Regulating the Reproductive System The Reproductive System to unite a single reproductive cell from a female with a single reproductive cell from a male Both male and female reproductive systems include
Dr Mary Birdsall. Fertility Associates Auckland
 Dr Mary Birdsall Fertility Associates Auckland Period Problems Mary Birdsall Medical Director Fertility Associates Auckland Period Problems Basic Physiology No Periods Irregular Periods Heavy Periods
Dr Mary Birdsall Fertility Associates Auckland Period Problems Mary Birdsall Medical Director Fertility Associates Auckland Period Problems Basic Physiology No Periods Irregular Periods Heavy Periods
INFERTILITY CAUSES. Basic evaluation of the female
 INFERTILITY Infertility is the inability to conceive after 12 months of unprotected intercourse. There are multiple causes of infertility and a systematic way to evaluate the condition. Let s look at some
INFERTILITY Infertility is the inability to conceive after 12 months of unprotected intercourse. There are multiple causes of infertility and a systematic way to evaluate the condition. Let s look at some
Achieving Pregnancy: Obesity and Infertility. Jordan Vaughan, MSN, APN, WHNP-BC Women s Health Nurse Practitioner Nashville Fertility Center
 Achieving Pregnancy: Obesity and Infertility Jordan Vaughan, MSN, APN, WHNP-BC Women s Health Nurse Practitioner Nashville Fertility Center Disclosures Speakers Bureau EMD Serono Board of Directors Nurse
Achieving Pregnancy: Obesity and Infertility Jordan Vaughan, MSN, APN, WHNP-BC Women s Health Nurse Practitioner Nashville Fertility Center Disclosures Speakers Bureau EMD Serono Board of Directors Nurse
Dysfunctional Uterine Bleeding (DUB) OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Tel:
 OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Tel:") Dysfunctional Uterine Bleeding (DUB) OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Email: wfeng7347@aliyun.com Tel: 13918551061 2014-8-20 Contents DUB: definition, mechanism of normal menses,
Dysfunctional Uterine Bleeding (DUB) OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Email: wfeng7347@aliyun.com Tel: 13918551061 2014-8-20 Contents DUB: definition, mechanism of normal menses,
I. Endocrine System & Hormones Figure 1: Human Endocrine System
 I. Endocrine System & Hormones Figure 1: Human Endocrine System Endocrine System: a) Endocrine glands are ductless since they lack specific vessels for the transport of hormones throughout the body. Instead,
I. Endocrine System & Hormones Figure 1: Human Endocrine System Endocrine System: a) Endocrine glands are ductless since they lack specific vessels for the transport of hormones throughout the body. Instead,
Case Questions. Polycystic Ovarian Syndrome: Treatment Goals and Options. Differential Diagnosis of Hyperandrogenic Anovulation
 Polycystic Ovarian Syndrome: Treatment Goals and Options Marc Cornier, MD Division of Endocrinology, Metabolism and Diabetes Colorado Center for Health and Wellness University of Colorado School of Medicine
Polycystic Ovarian Syndrome: Treatment Goals and Options Marc Cornier, MD Division of Endocrinology, Metabolism and Diabetes Colorado Center for Health and Wellness University of Colorado School of Medicine
Polycystic Ovary Syndrome
 What is the polycystic ovary syndrome? Polycystic Ovary Syndrome The polycystic ovary syndrome (PCOS) is a clinical diagnosis characterized by the presence of two or more of the following features: irregular
What is the polycystic ovary syndrome? Polycystic Ovary Syndrome The polycystic ovary syndrome (PCOS) is a clinical diagnosis characterized by the presence of two or more of the following features: irregular
2006 CE Series Lesson Two An Overview of The Premenstrual Syndrome ACPE Universal Program No H01 Expiration Date: 1/31/09
 2006 CE Series Lesson Two An Overview of The Premenstrual Syndrome ACPE Universal Program No. 406-000-06-002-H01 Expiration Date: 1/31/09 by H. David Bergman, Ph.D. Dean, Southwestern Oklahoma State University,
2006 CE Series Lesson Two An Overview of The Premenstrual Syndrome ACPE Universal Program No. 406-000-06-002-H01 Expiration Date: 1/31/09 by H. David Bergman, Ph.D. Dean, Southwestern Oklahoma State University,
FERTILITY & TCM. On line course provided by. Taught by Clara Cohen
 FERTILITY & TCM On line course provided by Taught by Clara Cohen FERTILITY & TCM FERTILITY AND TCM THE PRACTITIONER S ROLE CAUSES OF INFERTILITY RISK FACTORS OBJECTIVES UNDERSTANDING TESTS Conception in
FERTILITY & TCM On line course provided by Taught by Clara Cohen FERTILITY & TCM FERTILITY AND TCM THE PRACTITIONER S ROLE CAUSES OF INFERTILITY RISK FACTORS OBJECTIVES UNDERSTANDING TESTS Conception in
Reproductive Hormones
 Reproductive Hormones Male gonads: testes produce male sex cells! sperm Female gonads: ovaries produce female sex cells! ovum The union of male and female sex cells during fertilization produces a zygote
Reproductive Hormones Male gonads: testes produce male sex cells! sperm Female gonads: ovaries produce female sex cells! ovum The union of male and female sex cells during fertilization produces a zygote
ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU)
") ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU) In 1935, Stein and Leventhal described 7 women with bilateral enlarged PCO, amenorrhea or irregular menses, infertility and masculinizing
ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU) In 1935, Stein and Leventhal described 7 women with bilateral enlarged PCO, amenorrhea or irregular menses, infertility and masculinizing
Dysmenorrhoea Gynaecology د.شيماءعبداالميرالجميلي. Aetiology of secondary dysmenorrhea
 30-11-2014 Gynaecology Dysmenorrhoea د.شيماءعبداالميرالجميلي Dysmenorrhoea is defined as painful menstruation. It is experienced by 45 95 per cent of women of reproductive age.primary Spasmodic Dysmenorrhea
30-11-2014 Gynaecology Dysmenorrhoea د.شيماءعبداالميرالجميلي Dysmenorrhoea is defined as painful menstruation. It is experienced by 45 95 per cent of women of reproductive age.primary Spasmodic Dysmenorrhea
Infertility for the Primary Care Provider
 Infertility for the Primary Care Provider David A. Forstein, DO FACOOG Clinical Associate Professor Obstetrics and Gynecology University of South Carolina School of Medicine Greenville Disclosure I have
Infertility for the Primary Care Provider David A. Forstein, DO FACOOG Clinical Associate Professor Obstetrics and Gynecology University of South Carolina School of Medicine Greenville Disclosure I have
Chapter 100 Gynecologic Disorders
 Chapter 100 Gynecologic Disorders Episode Overview: 1. Describe the presentation and RF for Adnexal torsion 2. List the imaging findings of adnexal torsion (US vs CT) 3. What is the management of adnexal
Chapter 100 Gynecologic Disorders Episode Overview: 1. Describe the presentation and RF for Adnexal torsion 2. List the imaging findings of adnexal torsion (US vs CT) 3. What is the management of adnexal
Chapter 14 Reproduction Review Assignment
 Date: Mark: _/45 Chapter 14 Reproduction Review Assignment Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Use the diagram above to answer the next question.
Date: Mark: _/45 Chapter 14 Reproduction Review Assignment Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Use the diagram above to answer the next question.
What is PCOS? PCOS THE CONQUER PCOS E-BOOK. You'll be amazed when you read this...
 PCOS What is PCOS? You'll be amazed when you read this... What is PCOS?. Who is at risk? How to get tested? What are the complications. Is there a cure? What are the right ways to eat? What lifestyle changes
PCOS What is PCOS? You'll be amazed when you read this... What is PCOS?. Who is at risk? How to get tested? What are the complications. Is there a cure? What are the right ways to eat? What lifestyle changes
Polycystic Ovary Syndrome
 Polycystic Ovary Syndrome Kathleen Colleran, MD Professor of Medicine University of New Mexico HSC Presented for COMM-TC May 4, 2012 Objectives Understand the pathophysiology of PCOS Understand how to
Polycystic Ovary Syndrome Kathleen Colleran, MD Professor of Medicine University of New Mexico HSC Presented for COMM-TC May 4, 2012 Objectives Understand the pathophysiology of PCOS Understand how to
Ohio Northern University HealthWise. Authors: Alexis Dolin, Andrew Duska, Hannah Lamb, Eric Miller, Pharm D Candidates 2018 May 2018
 Women s Health Authors: Alexis Dolin, Andrew Duska, Hannah Lamb, Eric Miller, Pharm D Candidates 2018 May 2018 Let Your Body Empower You! National Women s Health Week Polycystic Ovary Syndrome Page 2 Breast
Women s Health Authors: Alexis Dolin, Andrew Duska, Hannah Lamb, Eric Miller, Pharm D Candidates 2018 May 2018 Let Your Body Empower You! National Women s Health Week Polycystic Ovary Syndrome Page 2 Breast
Female Reproductive Endocrinology
 Female Reproductive Endocrinology Dr. Channa Jayasena PhD MRCP FRCPath Clinical Senior Lecturer & Consultant Endocrinologist Department of Gynaecology, Hammersmith Hospital Anovulation is a common cause
Female Reproductive Endocrinology Dr. Channa Jayasena PhD MRCP FRCPath Clinical Senior Lecturer & Consultant Endocrinologist Department of Gynaecology, Hammersmith Hospital Anovulation is a common cause
Month-Long Hormone Assessment: What goes up must come down. Disclaimer. Aims and Objectives. George Gillson MD PhD
 Month-Long Hormone Assessment: What goes up must come down George Gillson MD PhD 1 Disclaimer The information presented in this Webinar is the opinion of Dr. Gillson based on his research and experience.
Month-Long Hormone Assessment: What goes up must come down George Gillson MD PhD 1 Disclaimer The information presented in this Webinar is the opinion of Dr. Gillson based on his research and experience.
Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital. Objectives
 Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital Objectives Definition of normal menstrual cycle and abnormal uterine bleeding (AUB) Evaluation of AUB Medical options for AUB Surgical
Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital Objectives Definition of normal menstrual cycle and abnormal uterine bleeding (AUB) Evaluation of AUB Medical options for AUB Surgical
5/5/2010. Infertility FINANCIAL DISCLOSURE. Infertility Definition. Objectives. Normal Human Fertility. Normal Menstrual Cycle
 Infertility FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology I AM RECEIVING COMPENSATION
Infertility FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology I AM RECEIVING COMPENSATION
Managing Menstrual Disorders
 Managing Menstrual Disorders David G. Weismiller, MD, ScM, FAAFP Professor Department of Family Medicine The Brody School of Medicine at East Carolina University Greenville, North Carolina Learning Objectives
Managing Menstrual Disorders David G. Weismiller, MD, ScM, FAAFP Professor Department of Family Medicine The Brody School of Medicine at East Carolina University Greenville, North Carolina Learning Objectives
Stage 4 - Ovarian Cancer Symptoms
 WELCOME Stage 4 - Ovarian Cancer Symptoms University of Baghdad College of Nursing Department of Basic Medical Sciences Overview of Anatomy and Physioloy II Second Year Students Asaad Ismail Ahmad,
WELCOME Stage 4 - Ovarian Cancer Symptoms University of Baghdad College of Nursing Department of Basic Medical Sciences Overview of Anatomy and Physioloy II Second Year Students Asaad Ismail Ahmad,
Physiology of Male Reproductive System
 Physiology of Male Reproductive System the anterior pituitary gland serves as the primary control of reproductive function at puberty Ant Pituitary secretes FSH & large amounts of LH (ICSH) FSH & LH cause
Physiology of Male Reproductive System the anterior pituitary gland serves as the primary control of reproductive function at puberty Ant Pituitary secretes FSH & large amounts of LH (ICSH) FSH & LH cause
The reproductive lifespan
 The reproductive lifespan Reproductive potential Ovarian cycles Pregnancy Lactation Male Female Puberty Menopause Age Menstruation is an external indicator of ovarian events controlled by the hypothalamicpituitary
The reproductive lifespan Reproductive potential Ovarian cycles Pregnancy Lactation Male Female Puberty Menopause Age Menstruation is an external indicator of ovarian events controlled by the hypothalamicpituitary
OVERVIEW. FEMM (Fertility Education & Medical Management) is headquartered in New York City, NY. 1
 is headquartered in New York City, NY. 1") OVERVIEW FEMM (Fertility Education & Medical Management) is headquartered in New York City, NY. 1 FEMM is a three-tiered women s healthcare project. Grounded in revolutionary, peer-reviewed research in
OVERVIEW FEMM (Fertility Education & Medical Management) is headquartered in New York City, NY. 1 FEMM is a three-tiered women s healthcare project. Grounded in revolutionary, peer-reviewed research in
10.7 The Reproductive Hormones
 10.7 The Reproductive Hormones December 10, 2013. Website survey?? QUESTION: Who is more complicated: men or women? The Female Reproductive System ovaries: produce gametes (eggs) produce estrogen (steroid
10.7 The Reproductive Hormones December 10, 2013. Website survey?? QUESTION: Who is more complicated: men or women? The Female Reproductive System ovaries: produce gametes (eggs) produce estrogen (steroid
Chapter 27 The Reproductive System. MDufilho
 Chapter 27 The Reproductive System 1 Figure 27.19 Events of oogenesis. Before birth Meiotic events 2n Oogonium (stem cell) Mitosis Follicle development in ovary Follicle cells Oocyte 2n Primary oocyte
Chapter 27 The Reproductive System 1 Figure 27.19 Events of oogenesis. Before birth Meiotic events 2n Oogonium (stem cell) Mitosis Follicle development in ovary Follicle cells Oocyte 2n Primary oocyte
MULTIPLE CHOICE: match the term(s) or description with the appropriate letter of the structure.
 or description with the appropriate letter of the structure.") Chapter 27 Exam Due NLT Thursday, July 31, 2015 Name MULTIPLE CHOICE: match the term(s) or description with the appropriate letter of the structure. Figure 27.1 Using Figure 27.1, match the following:
Chapter 27 Exam Due NLT Thursday, July 31, 2015 Name MULTIPLE CHOICE: match the term(s) or description with the appropriate letter of the structure. Figure 27.1 Using Figure 27.1, match the following:
AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE
 AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Formerly The American Fertility Society OVULATION DETECTION A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive
AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Formerly The American Fertility Society OVULATION DETECTION A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive
Womens Early Years. Nayan Patel PharmD
 Womens Early Years. Nayan Patel PharmD Dr. Katharina Dalton (OBGYN) Treating PMS since 1953 with Dr. Greene (Endocrinologist) This is the 6 th edition published in 1999 Definition * PMS - is a group of
Womens Early Years. Nayan Patel PharmD Dr. Katharina Dalton (OBGYN) Treating PMS since 1953 with Dr. Greene (Endocrinologist) This is the 6 th edition published in 1999 Definition * PMS - is a group of
Dr Stella Milsom. Endocrinologist Fertility Associates Auckland. 12:30-12:40 When Puberty is PCO
 Dr Stella Milsom Endocrinologist Fertility Associates Auckland 12:30-12:40 When Puberty is PCO Puberty or Polycystic Ovary Syndrome? Stella Milsom Endocrinologist Auckland DHB, University of Auckland,
Dr Stella Milsom Endocrinologist Fertility Associates Auckland 12:30-12:40 When Puberty is PCO Puberty or Polycystic Ovary Syndrome? Stella Milsom Endocrinologist Auckland DHB, University of Auckland,
Web Activity: Simulation Structures of the Female Reproductive System
 differentiate. The epididymis is a coiled tube found along the outer edge of the testis where the sperm mature. 3. Testosterone is a male sex hormone produced in the interstitial cells of the testes. It
differentiate. The epididymis is a coiled tube found along the outer edge of the testis where the sperm mature. 3. Testosterone is a male sex hormone produced in the interstitial cells of the testes. It
What s New in Adolescent Contraception?
 What s New in Adolescent Contraception? Abby Furukawa, MD Legacy Medical Group Portland Obstetrics and Gynecology April 29, 2017 Objectives Provide an update on contraception options for the adolescent
What s New in Adolescent Contraception? Abby Furukawa, MD Legacy Medical Group Portland Obstetrics and Gynecology April 29, 2017 Objectives Provide an update on contraception options for the adolescent
Endocrine Glands. Endocrine glands
 ENDOCRINOLOGY Endocrine Glands Endocrine glands Produce substances called hormones. Ductless glands, i.e., they release hormones directly into the bloodstream Hormones only act at their target tissue where
ENDOCRINOLOGY Endocrine Glands Endocrine glands Produce substances called hormones. Ductless glands, i.e., they release hormones directly into the bloodstream Hormones only act at their target tissue where
Polycystic ovarian disease and Endometriosis
 Polycystic ovarian disease and Endometriosis Objectives: At the end of this lecture, the student should be able to: Know the clinicopathologic features of endometriosis with special emphasis on: definition,
Polycystic ovarian disease and Endometriosis Objectives: At the end of this lecture, the student should be able to: Know the clinicopathologic features of endometriosis with special emphasis on: definition,
Reproductive Testing: Less is More G. Wright Bates, Jr., M.D. Professor and Director Reproductive Endocrinology and Infertility Objectives
 Reproductive Testing: Less is More G. Wright Bates, Jr., M.D. Professor and Director Reproductive Endocrinology and Infertility Objectives 1. Review definition of infertility and impact of age 2. Stress
Reproductive Testing: Less is More G. Wright Bates, Jr., M.D. Professor and Director Reproductive Endocrinology and Infertility Objectives 1. Review definition of infertility and impact of age 2. Stress
Infertility. Review and Update Clifford C. Hayslip MD Intrauterine Inseminations
 Infertility Review and Update Clifford C. Hayslip MD Intrauterine Inseminations Beneficial effects of IUI not consistently documented in studies No deleterious effects on fertility 3-4 cycles of IUI should
Infertility Review and Update Clifford C. Hayslip MD Intrauterine Inseminations Beneficial effects of IUI not consistently documented in studies No deleterious effects on fertility 3-4 cycles of IUI should
Causes of Infertility and Treatment Options
 Causes of Infertility and Treatment Options Dr Mrs.Kiran D. Sekhar Former vice President-FOGSI Former Chairperson- Genetics and Foetal medicine-fogsi Founder and Medical Director-Kiran Infertility centre
Causes of Infertility and Treatment Options Dr Mrs.Kiran D. Sekhar Former vice President-FOGSI Former Chairperson- Genetics and Foetal medicine-fogsi Founder and Medical Director-Kiran Infertility centre
Dysfunctional Uterine Bleeding
 Long term effects of PCOS Dysfunctional Uterine Bleeding Dr. Arulmozhi Ramarajan Church of South India Hospital, Bangalore Abnormal uterine bleeding Affects health-related QOL Causes social embarrasment
Long term effects of PCOS Dysfunctional Uterine Bleeding Dr. Arulmozhi Ramarajan Church of South India Hospital, Bangalore Abnormal uterine bleeding Affects health-related QOL Causes social embarrasment
Functions of male Reproductive System: produce gametes deliver gametes protect and support gametes
 Functions of male Reproductive System: produce gametes deliver gametes protect and support gametes Spermatogenesis occurs in the testes after puberty. From the testes they are deposited into the epididymas
Functions of male Reproductive System: produce gametes deliver gametes protect and support gametes Spermatogenesis occurs in the testes after puberty. From the testes they are deposited into the epididymas
Hormone Balance - Female Report SAMPLE. result graph based on Luteal Phase. result graph based on Luteal Phase
 Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Polycystic ovary syndrome
 Polycystic ovary syndrome Overview Polycystic ovary syndrome (PCOS) is a condition most often characterized by irregular menstrual periods, excess hair growth and obesity, but it can affect women in a
Polycystic ovary syndrome Overview Polycystic ovary syndrome (PCOS) is a condition most often characterized by irregular menstrual periods, excess hair growth and obesity, but it can affect women in a
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre
 Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
TRHC.UEMEE Ph P y h si s o i logy l of fmen M str st u r at a i t on i
 . TRHCUEMEE Physiology of Menstruation Learning objectives: By the end of this lecture the students should be able to: Define menstruation. List the Characters of normal menstruation Enumerate Components
. TRHCUEMEE Physiology of Menstruation Learning objectives: By the end of this lecture the students should be able to: Define menstruation. List the Characters of normal menstruation Enumerate Components
Abnormal Uterine Bleeding: Evaluation of Premenopausal Women. Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF
 Abnormal Uterine Bleeding: Evaluation of Premenopausal Women Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF Objectives Define normal and abnormal uterine bleeding Review
Abnormal Uterine Bleeding: Evaluation of Premenopausal Women Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF Objectives Define normal and abnormal uterine bleeding Review
Reproductive physiology. About this Chapter. Case introduction. The brain directs reproduction 2010/6/29. The Male Reproductive System
 Section Ⅻ Reproductive physiology Ming-jie Wang E-Mail: mjwang@shmu.edu.cn About this Chapter The reproductive organs and how they work the major endocrine functions of sexual glands actions of sex hormones
Section Ⅻ Reproductive physiology Ming-jie Wang E-Mail: mjwang@shmu.edu.cn About this Chapter The reproductive organs and how they work the major endocrine functions of sexual glands actions of sex hormones
Polycystic Ovarian Syndrome. Heidi Hallonquist, MD Concord Hospital Concord Obstetrics and Gynecology
 Polycystic Ovarian Syndrome Heidi Hallonquist, MD Concord Hospital Concord Obstetrics and Gynecology Outline Definition Symptoms Causal factors Diagnosis Complications Treatment Why are we talking about
Polycystic Ovarian Syndrome Heidi Hallonquist, MD Concord Hospital Concord Obstetrics and Gynecology Outline Definition Symptoms Causal factors Diagnosis Complications Treatment Why are we talking about
Conflicts 10/5/2016. Abnormal Uterine Bleeding. Objectives Review diagnosis and updated nomenclature. Management options for acute and chronic AUB.
 Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
The 6 th Scientific Meeting of the Asia Pacific Menopause Federation
 Abnormal uterine bleeding in the perimenopause Perimenopausal menstrual problems are among the most common causes for family practitioner and specialist referral. Often it is due to the hormone changes
Abnormal uterine bleeding in the perimenopause Perimenopausal menstrual problems are among the most common causes for family practitioner and specialist referral. Often it is due to the hormone changes
Sample Provincial exam Q s: Reproduction
 Sample Provincial exam Q s: Reproduction 11. Functions Testosterone Makes the male sex organs function normally, and also inhibits hypothalamus s release of GnRH and thus LH & FSH and thus testosterone
Sample Provincial exam Q s: Reproduction 11. Functions Testosterone Makes the male sex organs function normally, and also inhibits hypothalamus s release of GnRH and thus LH & FSH and thus testosterone
Estrogens & Antiestrogens
 Estrogens & Antiestrogens Menstrual cycle... Changes and hormonal events Natural estrogens: Estadiol >> Estrone > Estriol Ineffective orally Synthesis: From cholesterol ; role of aromatase enzyme in converting
Estrogens & Antiestrogens Menstrual cycle... Changes and hormonal events Natural estrogens: Estadiol >> Estrone > Estriol Ineffective orally Synthesis: From cholesterol ; role of aromatase enzyme in converting
N orethindrone-mestranol as a Therapeutic Agent
 N orethindrone-mestranol as a Therapeutic Agent WILLIAM J. CAMERON, M.D., and JAMES C. WARREN, M.D., Ph.D. OVER THE LAST SEVERAL YEARS, intensive research has resulted in the availability of potent synthetic
N orethindrone-mestranol as a Therapeutic Agent WILLIAM J. CAMERON, M.D., and JAMES C. WARREN, M.D., Ph.D. OVER THE LAST SEVERAL YEARS, intensive research has resulted in the availability of potent synthetic
GONADAL FUNCTION: An Overview
 GONADAL FUNCTION: An Overview University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences Clinical Biochemistry BMLS III & BDS IV VJ Temple 1 What are the Steroid hormones?
GONADAL FUNCTION: An Overview University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences Clinical Biochemistry BMLS III & BDS IV VJ Temple 1 What are the Steroid hormones?
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc)
") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Guideline for the Investigation and Management of Polycystic Ovary Syndrome Author: Contact Name and Job Title
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Guideline for the Investigation and Management of Polycystic Ovary Syndrome Author: Contact Name and Job Title
By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University
 By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University Cessation of menstruation as a result of the aging process of or surgical removal of the ovaries; change
By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University Cessation of menstruation as a result of the aging process of or surgical removal of the ovaries; change
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
ORILISSA (elagolix) oral tablet
 oral tablet") ORILISSA (elagolix) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ORILISSA (elagolix) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Reproduction and Development. Female Reproductive System
 Reproduction and Development Female Reproductive System Outcomes 5. Identify the structures in the human female reproductive system and describe their functions. Ovaries, Fallopian tubes, Uterus, Endometrium,
Reproduction and Development Female Reproductive System Outcomes 5. Identify the structures in the human female reproductive system and describe their functions. Ovaries, Fallopian tubes, Uterus, Endometrium,
Test Briefing on Hormonal Disorders and Infertility
 Test Briefing on Hormonal Disorders and Infertility Test Briefing on Hormonal Disorders Common Tests FSH LH Progesterone Estradiol Prolactin Testosterone AFP AMH PCOS Panel FSH (Follicle Stimulating Hormone)
Test Briefing on Hormonal Disorders and Infertility Test Briefing on Hormonal Disorders Common Tests FSH LH Progesterone Estradiol Prolactin Testosterone AFP AMH PCOS Panel FSH (Follicle Stimulating Hormone)
Breast Cancer Risk in Patients Using Hormonal Contraception
 Breast Cancer Risk in Patients Using Hormonal Contraception Bradley L. Smith, Pharm.D. Smith.bradley1@mayo.edu Pharmacy Ground Rounds Mayo Clinic Rochester April 3 rd, 2018 2017 MFMER slide-1 Presentation
Breast Cancer Risk in Patients Using Hormonal Contraception Bradley L. Smith, Pharm.D. Smith.bradley1@mayo.edu Pharmacy Ground Rounds Mayo Clinic Rochester April 3 rd, 2018 2017 MFMER slide-1 Presentation
Exam Key. NROSCI/BIOSC 1070 and MSNBIO 2070 Final Exam December 19, 2015 Total POINTS: % of grade in class
 NROSCI/BIOSC 1070 and MSNBIO 2070 Final Exam December 19, 2015 Total POINTS: 100 20% of grade in class 1) Zollinger-Ellison syndrome results from a gastrin-secreting tumor, producing increased numbers
NROSCI/BIOSC 1070 and MSNBIO 2070 Final Exam December 19, 2015 Total POINTS: 100 20% of grade in class 1) Zollinger-Ellison syndrome results from a gastrin-secreting tumor, producing increased numbers
Progesterone, A Central Role in Hormone Balance and Cycle Control Today s Ignorance of Hormonal Importance:
 G eorgia H orm ones, P.C. R obert P. G oldm an, M D 3400-A O ld M ilton P kw k y, Suite 360, A lpharetta G A 30005 770-475 475-0077 w w w.g eorgiah orm ones.com 2009-05-18 Progesterone, A Central Role
G eorgia H orm ones, P.C. R obert P. G oldm an, M D 3400-A O ld M ilton P kw k y, Suite 360, A lpharetta G A 30005 770-475 475-0077 w w w.g eorgiah orm ones.com 2009-05-18 Progesterone, A Central Role
Clinical evaluation of infertility
 Clinical evaluation of infertility DR. FARIBA KHANIPOUYANI OBSTETRICIAN & GYNECOLOGIST PRENATOLOGIST Definition: inability to achieve conception despite one year of frequent unprotected intercourse. Male
Clinical evaluation of infertility DR. FARIBA KHANIPOUYANI OBSTETRICIAN & GYNECOLOGIST PRENATOLOGIST Definition: inability to achieve conception despite one year of frequent unprotected intercourse. Male
Test Results SB Samples Arrived: 01/15/2014 Samples Collected: Saliva: 01/11/14 07:14 Date Closed: 01/18/2014
 Test Results 8605 SW Creekside Place Beaverton, OR 97008 Phone: 503-466-2445 Fax: 503-466-1636 info@zrtlab.com www.zrtlab.com 2014 01 15 001 SB Samples Arrived: 01/15/2014 Samples Collected: Saliva: 01/11/14
Test Results 8605 SW Creekside Place Beaverton, OR 97008 Phone: 503-466-2445 Fax: 503-466-1636 info@zrtlab.com www.zrtlab.com 2014 01 15 001 SB Samples Arrived: 01/15/2014 Samples Collected: Saliva: 01/11/14
Hormone. Free Androgen Index. 2-Hydroxyestrone. Reference Range. Hormone. Estrone Ratio. Free Androgen Index
 Hormonal Health PATIENT: Sample Report TEST REF: TST-12345 Hormonal Health 0.61 0.30-1.13 ng/ml DHEA-S 91 35-430 mcg/dl tient: SAMPLE TIENT e: x: N: Sex Binding Globulin 80 18-114 nmol/l Testosterone 0.34
Hormonal Health PATIENT: Sample Report TEST REF: TST-12345 Hormonal Health 0.61 0.30-1.13 ng/ml DHEA-S 91 35-430 mcg/dl tient: SAMPLE TIENT e: x: N: Sex Binding Globulin 80 18-114 nmol/l Testosterone 0.34
8605 SW Creekside Place Beaverton, OR Phone: Fax: Samples Collected. Samples Received 06/21/2017
 TEST RESULTS Ordering Provider: Getuwell Clinic Patient Name: Patient Phone Number: 555 555 5555 Gender Female DOB 6/9/1978 (39 yrs) Menses Status Pre-Menopausal 8605 SW Creekside Place Beaverton, OR 97008
TEST RESULTS Ordering Provider: Getuwell Clinic Patient Name: Patient Phone Number: 555 555 5555 Gender Female DOB 6/9/1978 (39 yrs) Menses Status Pre-Menopausal 8605 SW Creekside Place Beaverton, OR 97008
Reproductive physiology
 Reproductive physiology Sex hormones: Androgens Estrogens Gestagens Learning objectives 86 (also 90) Sex Genetic sex Gonadal sex Phenotypic sex XY - XX chromosomes testes - ovaries external features Tha
Reproductive physiology Sex hormones: Androgens Estrogens Gestagens Learning objectives 86 (also 90) Sex Genetic sex Gonadal sex Phenotypic sex XY - XX chromosomes testes - ovaries external features Tha
12/27/2013. Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND
 Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND 7% of all women 18-45 Obesity 1/3 of all US women Incidence of PCOS is increasing with increase obesity Obesity Irregular
Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND 7% of all women 18-45 Obesity 1/3 of all US women Incidence of PCOS is increasing with increase obesity Obesity Irregular
Phases of the Ovarian Cycle
 OVARIAN CYCLE An ovary contains many follicles, and each one contains an immature egg called an oocyte. A female is born with as many as 2 million follicles, but the number is reduced to 300,000 to 400,000
OVARIAN CYCLE An ovary contains many follicles, and each one contains an immature egg called an oocyte. A female is born with as many as 2 million follicles, but the number is reduced to 300,000 to 400,000
Polycystic Ovary Syndrome
 Polycystic Ovary Syndrome Polycystic ovary syndrome (PCOS) is common. It can cause period problems, reduced fertility, excess hair growth, and acne. Many women with PCOS are also overweight. Treatment
Polycystic Ovary Syndrome Polycystic ovary syndrome (PCOS) is common. It can cause period problems, reduced fertility, excess hair growth, and acne. Many women with PCOS are also overweight. Treatment