Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie
|
|
|
- Horace Newman
- 5 years ago
- Views:
Transcription


1 Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie Namens alle auteurs Michaël P. Casaer M.D. Department of Intensive Care Medicine University Hospital Gasthuisberg Catholic University of LEUVEN B-3000 BELGIUM
2 Casaer MP et al. N Engl J Med 2011; 365:

3 ICU patients : unable to feed normally

4 Malnourished patients in ICU patients : bad outcome

5 Early underfeeding and cumulative energy deficit Alberda: Increased mortaltity in BMI <25 or ICM Villet: More infections 2005 Clin. Nutr. Dvir D.: Complications 2006 Clin. Nutr.

6 Improved outcome trough enhanced feeding?

7 Or better feeding when less ill?
8 Does nutrition improve outcome? Adequate number of critically ill patients Randomization Nutrition No Nutrition
9 Does nutrition improve outcome? Power Adequate number of critically ill patients No selection bias Randomization Allocation concealed Nutrition No Nutrition
10 Does nutrition improve outcome? Power Adequate number of critically ill patients No selection bias Randomization Allocation concealed Nutrition No Nutrition Intention to treat Blinded assessors LOS QOL Mortality LOS QOL Mortality
11 Does nutrition improve outcome? Power Adequate number of critically ill patients No selection bias Randomization Allocation concealed Nutrition No Nutrition Intention to treat Blinded assessors LOS QOL Mortality LOS QOL Mortality
12 Nutrition strategies today EN only High risk of underfeeding Associated with Infections Morbidity Death
13 Nutrition strategies today EN only EN + PN High risk of underfeeding Risk of overfeeding and associated metabolic disturbances Associated with Infections Morbidity Death
14

15
16 Conflicting International Guidelines ESPEN Consider PN within 2 days if EN insufficient ASPEN No PN until > day 8, prefer hypocaloric nutrition
")
17 Causality? RCT! Casaer MP et al. N Engl J Med 2011; 365: EPaNIC multicenter randomized controlled trial (N=4640) clinical trials.gov [NCT ] : Different strategies
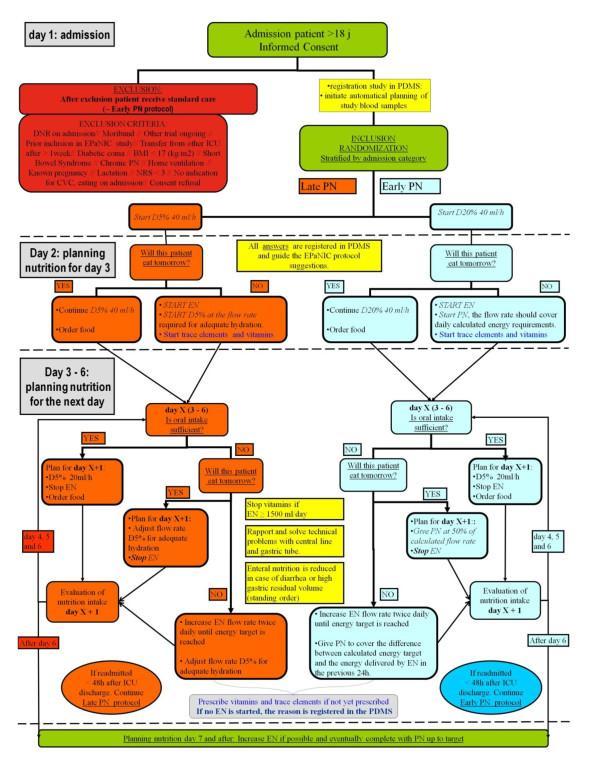
18 De EPaNIC intervention

19 EPaNIC intervention : PDMS supported
20 EPaNIC : study population Adult ICU patients, NRS 3, BMI 17 Late PN Early PN N = 2328 N = 2312 Age years 64 ± ± 14 BMI (kg/m²) Median (IQR) 25.6 ( ) 25.8 ( ) NRS score 4 n (%) 1278 (54.9) 1298 (56.1) Sepsis n (%) 505 (21.7) 510 (22.1) Emergency admission n (%) 970 (41.7) 956 (41.3) APACHE II score 23 ± ± 11 Casaer MP et al. N Engl J Med 2011; 365:
21 Nutrition administered Casaer MP et al. N Engl J Med 2011; 365:

22 Nutrition administered Casaer MP et al. N Engl J Med 2011; 365:
23 EPaNIC : In both groups Enteral nutrition initiated on the day after ICU admission Vitamins, trace elements, minerals administered early Overfeeding and hyperglycemia avoided Late PN Early PN Insulin dose 31 (19 48) IU 58 (40 85) IU P < Blood glucose levels 102 ± 14 mg/dl 107 ± 18 mg/dl P < Casaer MP et al. N Engl J Med 2011; 365:
24 EPaNIC : safety outcome Late PN Early PN ICU mortality 6.1 % 6.3 % P = 0.76 Hospital mortality 10.4 % 10.9 % P = day mortality 11.2 % 11.2 % P = 1.00 Casaer MP et al. N Engl J Med 2011; 365:

25 EPaNIC : safety outcome Kaplan-Meier survival Plot 1.0 Early PN Late PN Days after randomization
26 EPaNIC : safety outcome Late PN Early PN ICU mortality 6.1 % 6.3 % P = 0.76 Hospital mortality 10.4 % 10.9 % P = day mortality 11.2 % 11.2 % P = 1.00 Nutrition related complications 18.2 % 18.8% P = 0.62 Hypoglycemia 3.5 % 1.9 % P = Casaer MP et al. N Engl J Med 2011; 365:
27 EPaNIC : primary endpoints Late PN Early PN Discharged alive within 8 days 75.2 % 71.7 % P = ICU stay (days) median (IQR) mean 3 (2 7) 8 4 (2 9) 9 P = 0.02 Time to alive discharge from ICU ( ) P = 0.04 Hazard ratio (95%CI) Adjusted cox proportional hazard analysis Casaer MP et al. N Engl J Med 2011; 365:
28 EPaNIC : primary endpoints Casaer MP et al. N Engl J Med 2011; 365:
29 EPaNIC : infections & inflammation Late PN Early PN Patients with new ICU infection 22.8 % 26.2 % P = Airway or lung 16.4 % 19.3 % P = Bloodstream 6.1 % 7.5 % P = 0.05 Wound 2.7 % 4.2 % P = Highest CRP during ICU stay (mg/ liter) median (IQR) ( ) ( ) P < Casaer MP et al. N Engl J Med 2011; 365:
30 EPaNIC : MOF & recovery from MOF Late PN Early PN Mean duration of CMV 5 days 6 days Tracheostomy 5.8 % 7.0 % P = 0.08 Duration of CVVH IHD median (IQR) mean 7 (3 16) 15 days 10 (5 23) 18 days Proportion of patients During ICU week 1 P = Bilirubine > 3 mg/dl 12.2 % 10.5 % P = During entire ICU stay Gamma GT rise > 79.5 IU/L 32.6 % 38.4 % P = 0.05 Alk. Phosphatase > 405 IU/L 19.9 % 22.6 % P = Hepatic cytolysis (ALT rise > 123 IU/L or AST rise > 114 IU/L) similar in 2 groups Casaer MP et al. N Engl J Med 2011; 365:
31 EPaNIC : hospital stay Late PN Early PN Duration of hospital stay (days) median (IQR) mean 14 (9 27) (9 29) 26 P =0.004 Time to alive hospital discharge ( ) P = 0.04 Hazard ratio (95%CI) (Adjusted cox proportional hazard) Discharge from conventional ward was at discretion of attending physicians, who were blinded for treatment allocation Casaer MP et al. N Engl J Med 2011; 365:
32 EPaNIC : time to (alive) hospital discharge Casaer MP et al. N Engl J Med 2011; 365:

33 EPaNIC : functionality at hospital discharge Casaer MP et al. N Engl J Med 2011; 365:
34 EPaNIC : functionality at hospital discharge Late PN Early PN 6 Minutes Walking Distance (m) 277 ( ) 283 ( ) P = 0.69 N tested Patients independent for all ADL 73.5 % 75.5 % P = 0.31 N tested Casaer MP et al. N Engl J Med 2011; 365:
35 EPaNIC : subgroup analyses Similar effects of late PN in predefined subgroups: Cardiac surgery (N = 2818) BMI 25 OR 40 kg/m² (N = 1989) NRS 5, 6 and 7 (N = 863) Sepsis (N = 1015) Casaer MP et al. N Engl J Med 2011; 365:

36 Subgroup : surgical contra-indication for EN

37 Subgroup : surgical contra-indication for EN Posthoc subgroup, identifiable upon admission
38 Subgroup : surgical contra-indication for EN Late PN Early PN N = 261 N = 256 Enteral intake day 7 (kcal/day) median (IQR) 0 (0 263) 0 (0 142) P = 0.54 Patients with new ICU infection 29.9 % 40.2 % P = 0.01 Discharged alive from ICU 8 days Odds ratio (95%CI) Time to alive discharge from ICU Hazard ratio (95%CI) ( ) + 75% ( ) + 20% Casaer MP et al. N Engl J Med 2011; 365:
39 Subgroup : surgical contra-indication for EN What does this mean? More PN is more toxic? No feeding, irrespective of route, is better?
40 Health economy impact? Late PN Early PN Hospital stay cost mean (IQR) EUR Between patients difference Between groups difference ( ) 1110 EUR EUR ( ) P = 0.04 Cost of PN & hospital stay : flat compensation in Belgian healthcare system Difference explained by antibiotics and laboratory tests Casaer MP et al. N Engl J Med 2011; 365:
41 2 more questions? Is PN only beneficial in the most severely ill patients? Is PN only beneficial at moderate energy doses?
42 Patient specific? The wrong dose for the wrong patient? Perhaps less harmful when more severely ill EPaNIC subgroup analyses NRS 5 Contra indication EN Subgroups by severity of illness
43 Patient specific? The wrong dose for the wrong patient? Perhaps less harmful when more severely ill EPaNIC subgroup analyses NRS 5 Contra indication EN Subgroups by severity of illness

44 Patient specific? The wrong dose for the wrong patient? Perhaps less harmful when more severely ill EPaNIC subgroup analyses NRS 5 Contra indication EN Subgroups by severity of illness
45 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
46 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
47 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
48 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
49 EPaNIC, unpublished data M.P.C., K.U.Leuven
50 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
51 Type and severity of illness? No population doing better with early PN was identified. Benefit of Late PN most pronounced in the severely ill. No difference between cardiac surgery and others EPaNIC, unpublished data

52 Mismatch = more or less than the optimal dose
53 RCT s aiming at optimum nutrition intake Adapted from: Singer P ICM
54 Moore RCT s aiming at optimum nutrition intake Dissanaike Dudsk McClave 110% REE Adapted from: Singer P ICM N = 130
55 RCT s aiming at optimum nutrition intake Moore Dissanaike McClave 110% REE Dudsk Prolonged ICU stay Prolonged Mechanical ventilation Increased Infections? Reduced mortality? N = 130
56 Moore RCT s aiming at optimum nutrition intake Dissanaike Dudsk McClave 110% REE N = 4640
57 RCT s aiming at optimum nutrition intake N = 4640
58 RCT s aiming at optimum nutrition intake Cummulative Energy Deficit N = 4640
59 RCT s aiming at optimum nutrition intake Prolonged ICU stay Prolonged Mechanical ventilation Increased Infection N = 4640
60 RCT s aiming at optimum nutrition intake Interpretation of energy intake Based on the 2012 ESPEN presentation by Doig GS Displayed exclusively for the purpose of this discussion with kind permission of dr. Doig N = 1372
61 No effect on primary RCT s aiming at optimum nutrition intake endpoint Shorter mechanical ventilation? Improved subjective wellbeing N = 1372
62 RCT s aiming at optimum nutrition intake Patients expected to stay more than 5 days and live more than 7 days SPN started if EN < 60% of target on day 3 SPN group Control group PN Nutritional Target Day 4 EN ( IC) Day 4 EN Day 1 Day 7 Day 1 Day 7 Heidegger CP. 2012
63 RCT s aiming at optimum nutrition intake Patients expected to stay more than 5 days and live more than 7 days SPN started if EN < 60% of target on day 3 SPN group Control group PN Nutritional Target Day 4 EN ( IC) Day 4 EN Day 1 Day 7 Day 1 Day 7 Less infections Same ICU stay Heidegger CP N = 305
64 A new concept of overfeeding? observational data Hise <80% Preiser <50% Hise ME 2007 J Am Diet Assoc Preiser JC Glucontrol data Poster at ESPEN 2012
65 A new concept of overfeeding? Moore Dissanaike Dudsk Harm Hise <80% Preiser <50% No harm Hise ME 2007 J Am Diet Assoc Preiser JC Glucontrol data Poster at ESPEN 2012
66 Dose-response? Estimating the effect of increasing cumulative energy intake on likelihood of earlier discharge from the ICU AND detecting an eventual superior energy dose EPaNIC, unpublished data
67 Dose-response? Day 1 Day 3 Day 5 Day 7 Late PN patient Early PN patient EPaNIC, unpublished data
68 Dose-response? Day 1 Day 3 Day 5 Day 7 EPaNIC, unpublished data
69 Dose-response? Day 1 Day 3 Day 5 Day 7 EPaNIC, unpublished data
70 Dose-response? Day 1 Day 3 Day 5 Day 7 EPaNIC, unpublished data
71 Dose-response? Day 1 Day 3 Day 5 Day 7 EPaNIC, unpublished data
72 Dose-response? Day 1 Day 3 Day 5 Day 7 EPaNIC, unpublished data
73 Dose-response? Day 1 Day 3 Day 5 Day 7 EPaNIC, unpublished data
74 Dose-response? Likelihood for an earlier 1 discharge from ICU ~ nutrition dose EPaNIC, unpublished data
75 Dose-response? 10% of target /day increase in cumulative energy intake was associated with 2 8% decrease in likelihood for an earlier discharge from ICU ~ p < 0,0001 EPaNIC, unpublished data
76 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
77 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
78 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
79 Is less more when you are really ill? Casaer MP et al. N Engl J Med 2011; 365:

80 Is less more when you are really ill? Casaer MP et al. N Engl J Med 2011; 365: M.P.C.., K.U.Leuven
81 Likelihood of an earlier ICU discharge Relative effect of glucose versus protein intake 1,1 1,05 HR (CI) per 10% of target increase in glucose intake (± 28 g / day) 1 0,95 0,9 HR (CI) per 10% of target increase in protein intake (± 7 g / day) 0,85 day 1 day 3 day 5 day 7 EPaNIC, unpublished data M.P.C. & G.V.d.B., K.U.Leuven
82 Summary of clinical study findings Postponing PN to beyond day 8 (while providing micronutrients) in ICU pts at risk for malnutrition : is superior to preventing caloric deficit with early PN accelerates recovery from organ failure reduces number of infections shortens hospital stay, without compromising functionality at hospital discharge is less costly for patient, hospital and society Casaer MP et al. N Engl J Med 2011; 365:
83 Summary of clinical study findings The untoward effect of Early PN: is independent of type and severity of disease Is present at all nutrition doses except the lowest: less is more even for enteral nutrition The association between enhanced intake and delayed recovery is more pronounced for protein than glucose. Casaer MP et al. N Engl J Med 2011; 365:
84 Why? No indirect calorimetry? No Glutamine? Protein dosing?

85 Underlying mechanisms?
86 Withholding PN while providing parenteral micronutrients +Micronutrients Ziegler T 2011 N Engl J Med
87 Withholding PN while providing parenteral micronutrients =Micronutrients -Micronutrients +Micronutrients Ziegler T 2011 N Engl J Med
88 Withholding PN while providing parenteral micronutrients Ziegler T 2011 N Engl J Med +Micronutrients Less infections Enhanced Recovery
89 Withholding PN while providing parenteral micronutrients Macronutrient restriction + Early Micronutrients Ziegler T 2011 N Engl J Med
90 Withholding PN while providing parenteral micronutrients Macronutrient restriction + Early Micronutrients Derde S 2012 Endocrinology +++

91 Balance between damage induction & removal
92 Under investigation
93 Conclusions Postponing PN to beyond day 7 in ICU patients at risk of malnutrition is superior to preventing caloric deficit with early PN Underlying mechanisms could relate to cellular damage removal, which is suppressed by nutrients
94 Conclusion 3 RCT s, together > 6000 patients: EPaNIC, SPN, Early PN

95 All agree
96 Conclusion 3 RCT s, together > 6000 patients: EPaNIC, SPN, Early PN All Agree Parenteral nutrition before day 8, prevents caloric deficit but Does not improve survival Does not shorten ICU or hospital stay Long term functional outcome results will learn us more

97 A new concept of overfeeding: also true for EN 4000 kcal If less is equally benefical than more, I d prefer less No functional outcome Highly selected patients Rice T 2011 JAMA
98 FUNDING Methusalem (Flemish Government) FWO (Flemish Government) KULeuven GOA UZLeuven KOF Baxter (< 30%) Unconditional research grant and speaker fee


99 Thank You Laboratory and Department of Intensive Care Medicine

100 Thank you
101 Not enough protein in Early PN? Casaer MP et al. N Engl J Med 2011; 365:
102 Not enough protein in Early PN? Casaer MP et al. N Engl J Med 2011; 365:
103 Not enough protein in Early PN? Casaer MP et al. N Engl J Med 2011; 365:


104 Not enough protein in Early PN? Casaer MP et al. N Engl J Med 2011; 365:
105 Balance between damage induction & removal High Energy Hyperglycemia Mortality: 8% GVdB 1 & 2 High Energy TGC mg/dl Mortality: 6%
106 Balance between damage induction & removal High Energy Hyperglycemia Mortality: 8% GVdB 1 & 2 High Energy TGC mg/dl Mortality: 6% LOS ICU 4 [2-9] EPaNIC Low Energy TGC mg/dl Mortality: 6% LOS ICU 3 [2-7]
107 Balance between damage induction & removal High Energy Hyperglycemia Mortality: 8% GVdB 1 & 2 High Energy TGC mg/dl Mortality: 6% LOS ICU 4 [2-9] EPaNIC Low Energy Other Glycemic Target????????? Low Energy TGC mg/dl Mortality: 6% LOS ICU 3 [2-7]
108 How much energy, how much insulin? No Early PN in ICU Early EN? Recent trials showed no benefit Rice TW. CCM 2011 Ibrahim EH. JPEN 2002 Glycemic target based on accuracy of tools and adequacy of insulin provision.
109 ? PN REE?
110 PN REE REE
111 PN REE = PN REE
112 PN REE PN = U
113 Critical illness is a state of excessive availability of glucose and lipids. Wolfe R. Martini W. W. J Surg 2000 PN REE PN = U Inflammation Lipolysis Proteolysis
Timing of Parenteral Nutrition
 Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
When to start SPN in critically ill patients? Refereeravond IC
 When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
Kombinierte enterale und parenterale Ernährung für welche PatientInnen?
 2014 Kombinierte enterale und parenterale Ernährung für welche PatientInnen? Dr. CP. Heidegger Intensive Care/Geneva claudia-paula.heidegger@hcuge.ch Bern Freitag, 4. April 2014 Nutrition News Worldwide
2014 Kombinierte enterale und parenterale Ernährung für welche PatientInnen? Dr. CP. Heidegger Intensive Care/Geneva claudia-paula.heidegger@hcuge.ch Bern Freitag, 4. April 2014 Nutrition News Worldwide
Nutrition. ICU Fellowship Training Radboudumc
 Nutrition ICU Fellowship Training Radboudumc Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation.
Nutrition ICU Fellowship Training Radboudumc Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation.
Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal?
 Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal? PD Dr. med. Claudia Heidegger Service des Soins Intensifs Genf/Schweiz Dresden 11. Juni 2016 Nutrition News Nutrition controversy in
Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal? PD Dr. med. Claudia Heidegger Service des Soins Intensifs Genf/Schweiz Dresden 11. Juni 2016 Nutrition News Nutrition controversy in
Feeding the septic patient How and when? Masterclass ICU nurses
 Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
Nutrition Support in Critically Ill Cardiothoracic Patients
 Nutrition Support in Critically Ill Cardiothoracic Patients อ.นพ.พรพจน เปรมโยธ น สาชาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Outline Malnutrition in cardiothoracic patients Nutritional
Nutrition Support in Critically Ill Cardiothoracic Patients อ.นพ.พรพจน เปรมโยธ น สาชาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Outline Malnutrition in cardiothoracic patients Nutritional
IS THERE A PLACE IN THE ICU FOR PERMISSIVE UNDERFEEDING AND WHERE? ENGELA FRANCIS RD(SA)
") IS THERE A PLACE IN THE ICU FOR PERMISSIVE UNDERFEEDING AND WHERE? ENGELA FRANCIS RD(SA) DEFINITION: PERMISSIVE UNDERFEEDING No clear definition in literature Permissive underfeeding definition prior to
IS THERE A PLACE IN THE ICU FOR PERMISSIVE UNDERFEEDING AND WHERE? ENGELA FRANCIS RD(SA) DEFINITION: PERMISSIVE UNDERFEEDING No clear definition in literature Permissive underfeeding definition prior to
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
Metabolic Control in Critical Care: Nutrition Therapy
 LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
[No conflicts of interest]
![[No conflicts of interest]](/thumbs/86/94144068.jpg "[No conflicts of interest]") [No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
[No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
Oklahoma Dietetic Association. Ainsley Malone, MS, RD, LD, CNSD April, 16, 2008 Permissive Underfeeding: What, Where and Why? Mt.
 The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
Parenteral nutrition and calorie delivery in the ICU: controversy, clarity, or call to action?
 EDITORIAL C URRENT OPINION Parenteral nutrition and calorie delivery in the ICU: controversy, clarity, or call to action? Paul Wischmeyer Purpose of review This review will highlight recent data evaluating
EDITORIAL C URRENT OPINION Parenteral nutrition and calorie delivery in the ICU: controversy, clarity, or call to action? Paul Wischmeyer Purpose of review This review will highlight recent data evaluating
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Casaer MP, Mesotten D, Hermans G, et al. Early versus late
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Casaer MP, Mesotten D, Hermans G, et al. Early versus late
NO DISCLOSURES 5/9/2015
 Annette Stralovich-Romani, RD, CNSC Adult Critical Care Nutritionist UCSF Medical Center NO DISCLOSURES Incidence & consequences of malnutrition Underfeeding in the ICU Causes/ consequences Nutrition intervention
Annette Stralovich-Romani, RD, CNSC Adult Critical Care Nutritionist UCSF Medical Center NO DISCLOSURES Incidence & consequences of malnutrition Underfeeding in the ICU Causes/ consequences Nutrition intervention
The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND
 The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND 2013 Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 Use
The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND 2013 Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 Use
Advanced Enteral Nutrition Program For Dietitians. Week 5 Underfeeding in the ICU: Good or Bad? Presented on December 9, 2015
 Advanced Enteral Nutrition Program For Dietitians Week 5 Underfeeding in the ICU: Good or Bad? Presented on December 9, 2015 Sponsor Disclosure: Financial support for this presentation was provided by
Advanced Enteral Nutrition Program For Dietitians Week 5 Underfeeding in the ICU: Good or Bad? Presented on December 9, 2015 Sponsor Disclosure: Financial support for this presentation was provided by
Harm by hyperglycemia, early (parenteral) nutrition or both? from bed to bench and back
 nutrition or both? from bed to bench and back") Harm by hyperglycemia, early (parenteral) nutrition or both? from bed to bench and back G. Van den Berghe MD, PhD Department of Intensive Care Medicine University of Leuven (KU Leuven) Leuven, Belgium
Harm by hyperglycemia, early (parenteral) nutrition or both? from bed to bench and back G. Van den Berghe MD, PhD Department of Intensive Care Medicine University of Leuven (KU Leuven) Leuven, Belgium
ESPEN Congress Lisbon Water and electrolytes. Hyperglycemia management. G Van Den Berghe
 ESPEN Congress Lisbon 2004 Water and electrolytes Hyperglycemia management G Van Den Berghe Intensive Insulin Therapy in ICU G. Van den Berghe M.D., Ph.D. Department of Intensive Care Medicine University
ESPEN Congress Lisbon 2004 Water and electrolytes Hyperglycemia management G Van Den Berghe Intensive Insulin Therapy in ICU G. Van den Berghe M.D., Ph.D. Department of Intensive Care Medicine University
What s New in Parenteral Nutrition?
 1 What s New in Parenteral Nutrition? พ นโทหญ ง ส รกานต เตชะวณ ช MD, MSc, ABPNS ห วหน าหน วยโภชนศาสตร คล น ก กองอาย รกรรม โรงพยาบาลพระมงก ฎเกล า 7 กรกฎาคม พ.ศ. 2559 What s New in Parenteral Nutrition?
1 What s New in Parenteral Nutrition? พ นโทหญ ง ส รกานต เตชะวณ ช MD, MSc, ABPNS ห วหน าหน วยโภชนศาสตร คล น ก กองอาย รกรรม โรงพยาบาลพระมงก ฎเกล า 7 กรกฎาคม พ.ศ. 2559 What s New in Parenteral Nutrition?
This article was published on October 22, 2018, at NEJM.org.
 1 20 8 b E 8 b E C T aa 4 JG R d This article was published on October 22, 2018, at NEJM.org. 2003 2009 (ESPEN) (ASPEN/SCCM) CCPG 20-25kcal/kg/day 25-30kcal/kg/day EN PN( ) Enteral Nutrition EN 24 ICU
1 20 8 b E 8 b E C T aa 4 JG R d This article was published on October 22, 2018, at NEJM.org. 2003 2009 (ESPEN) (ASPEN/SCCM) CCPG 20-25kcal/kg/day 25-30kcal/kg/day EN PN( ) Enteral Nutrition EN 24 ICU
A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I
 FEEDING THE OBESE CRITICALLY ILL PATIENT A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I HOSPITAL, EDE,
FEEDING THE OBESE CRITICALLY ILL PATIENT A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I HOSPITAL, EDE,
Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017
 Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Providing Optimal Nutritional Support on the ICU common problems and practical solutions. Pete Turner Specialist Nutritional Support Dietitian
 Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
ESPEN Congress Madrid 2018
 ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Mechanisms And Consequences Of Dysglycaemia In Patients Receiving Nutritional Therapy M. León- Sanz (ES) Mechanisms and
ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Mechanisms And Consequences Of Dysglycaemia In Patients Receiving Nutritional Therapy M. León- Sanz (ES) Mechanisms and
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
ESPEN Congress Madrid 2018
 ESPEN Congress Madrid 2018 New ESPEN Guidelines Nutrition In The ICU P. Singer (IL) ESPEN Guidelines: Nutrition in the ICU Pierre Singer Annika Reintam Blaser Mette M Berger Waleed Alhazzani Philip C Calder
ESPEN Congress Madrid 2018 New ESPEN Guidelines Nutrition In The ICU P. Singer (IL) ESPEN Guidelines: Nutrition in the ICU Pierre Singer Annika Reintam Blaser Mette M Berger Waleed Alhazzani Philip C Calder
Nutrition in Acute Kidney Injury Enrico Fiaccadori
 Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Nutrition Supplementation in the ICU
 Nutrition Supplementation in the ICU ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 1 Use of Enteral vs
Nutrition Supplementation in the ICU ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 1 Use of Enteral vs
L.Mageswary Dietitian Hospital Selayang
 L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
2.0 Early vs. Delayed Nutrient Intake May 2015
 2.0 Early vs. Delayed Nutrient Intake May 2015 There were no new randomized controlled trials since the 2013 update and hence there are no changes to the following summary of evidence. 2013 Recommendation:
2.0 Early vs. Delayed Nutrient Intake May 2015 There were no new randomized controlled trials since the 2013 update and hence there are no changes to the following summary of evidence. 2013 Recommendation:
3.2 Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 2013
 . Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 01 There were no new randomized controlled trials since the 009 update and hence there are no changes to
. Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 01 There were no new randomized controlled trials since the 009 update and hence there are no changes to
Feeding the Critically Ill Obese Patient
 Feeding the Critically Ill Obese Patient Carla Vartanian 1 Critically Ill Obese Patients WHO: Obesity is abnormal or excessive fat accumulation that may impair health, or as a BMI 30. The American Medical
Feeding the Critically Ill Obese Patient Carla Vartanian 1 Critically Ill Obese Patients WHO: Obesity is abnormal or excessive fat accumulation that may impair health, or as a BMI 30. The American Medical
10/3/2012. Pediatric Parenteral Nutrition A Comprehensive Review
 Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial
 Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial Author: Version 1.0, Role, Name and Position Signature Date Chief investigator: Prof Kathryn Rowan (Director of Scientific & Strategic
Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial Author: Version 1.0, Role, Name and Position Signature Date Chief investigator: Prof Kathryn Rowan (Director of Scientific & Strategic
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital
 MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital") By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
A J shaped relationship between caloric intake and survival in critically ill patients
 Crosara et al. Ann. Intensive Care () :37 DOI.1186/s13613--79-3 RESEARCH Open Access A J shaped relationship between caloric intake and survival in critically ill patients Isabel Carolina Reis Crosara
Crosara et al. Ann. Intensive Care () :37 DOI.1186/s13613--79-3 RESEARCH Open Access A J shaped relationship between caloric intake and survival in critically ill patients Isabel Carolina Reis Crosara
8.0 Parenteral Nutrition vs. Standard care May 2015
 8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
ESPEN Congress Copenhagen 2016
 ESPEN Congress Copenhagen 2016 THE DIVERSITY OF OBESITY MALNUTRITION IN THE OBESE R. Barazzoni (IT) Malnutrition in the obese patient Rocco Barazzoni Dept of Medical, Surgical and Health Sciences University
ESPEN Congress Copenhagen 2016 THE DIVERSITY OF OBESITY MALNUTRITION IN THE OBESE R. Barazzoni (IT) Malnutrition in the obese patient Rocco Barazzoni Dept of Medical, Surgical and Health Sciences University
INTENSIVE INSULIN THERAPY: A Long History of Conflicting Data.
 INTENSIVE INSULIN THERAPY: A Long History of Conflicting Data. Candice Preslaski, PharmD BCPS Clinical Pharmacist Specialist SICU Denver Health Medical Center December 2014 OBJECTIVES Review the risk factors
INTENSIVE INSULIN THERAPY: A Long History of Conflicting Data. Candice Preslaski, PharmD BCPS Clinical Pharmacist Specialist SICU Denver Health Medical Center December 2014 OBJECTIVES Review the risk factors
Influence of Calorie Protein Delivery on Outcomes and Body Composition. Changes in the Intensive Care Unit. Sarah Peterson
 Influence of Calorie Protein Delivery on Outcomes and Body Composition Changes in the Intensive Care Unit BY Sarah Peterson B.A., Nutrition and Dietetics, The College of St. Scholastica, Duluth, MN 1999
Influence of Calorie Protein Delivery on Outcomes and Body Composition Changes in the Intensive Care Unit BY Sarah Peterson B.A., Nutrition and Dietetics, The College of St. Scholastica, Duluth, MN 1999
3.2 Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 2015
 . Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 015 015 Recommendation: Based on 1 level 1 study, level studies and cluster randomized controlled trials, when starting
. Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 015 015 Recommendation: Based on 1 level 1 study, level studies and cluster randomized controlled trials, when starting
Pharmaconutrition in PICU. Gan Chin Seng Paediatric Intensivist UMMC
 Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Indirect calorimetry: Is it necessary for everyone? Or do you prefer to guess?
 Indirect calorimetry: Is it necessary for everyone? Or do you prefer to guess? Is indirect calorimetry necessary? Pierre Singer, MD Institute for Nutrition Research Critical Care Department Rabin Medical
Indirect calorimetry: Is it necessary for everyone? Or do you prefer to guess? Is indirect calorimetry necessary? Pierre Singer, MD Institute for Nutrition Research Critical Care Department Rabin Medical
10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015
 10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015 There are no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes
10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015 There are no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes
11.1 Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 2013
 . Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 23 23 Recommendation: Based on 7 level and 7 level 2 studies, the use of supplemental combined vitamins and trace elements
. Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 23 23 Recommendation: Based on 7 level and 7 level 2 studies, the use of supplemental combined vitamins and trace elements
N U TRITION A N D C R I TICALLY I L L PATIENTS W I TH S E P S I S
 N U TRITION A N D M E TABOLISM: C R I TICALLY I L L PATIENTS W I TH S E P S I S A R T H U R R. H. V A N Z A N T E N, M D P H D I N T E R N IST - IN TENSIV IST H O S P I T AL M E D I C A L D I R E C T OR
N U TRITION A N D M E TABOLISM: C R I TICALLY I L L PATIENTS W I TH S E P S I S A R T H U R R. H. V A N Z A N T E N, M D P H D I N T E R N IST - IN TENSIV IST H O S P I T AL M E D I C A L D I R E C T OR
E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol
 E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol Arthur RH van Zanten, MD PhD Gelderse Vallei Hospital, Ede, The Netherlands Learning objectives Develop an evidence based
E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol Arthur RH van Zanten, MD PhD Gelderse Vallei Hospital, Ede, The Netherlands Learning objectives Develop an evidence based
Clinical Guidelines for the Hospitalized Adult Patient with Obesity
 Clinical Guidelines for the Hospitalized Adult Patient with Obesity 1 Definition of obesity: Obesity is characterized by an excess storage of adipose tissue that is related to an imbalance between energy
Clinical Guidelines for the Hospitalized Adult Patient with Obesity 1 Definition of obesity: Obesity is characterized by an excess storage of adipose tissue that is related to an imbalance between energy
Protein in Critically Ill Patients. Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital
 MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital") Protein in Critically Ill Patients Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital Proteins Proteins Protein is needed to Build, Maintain, and Repair body tissue
Protein in Critically Ill Patients Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital Proteins Proteins Protein is needed to Build, Maintain, and Repair body tissue
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION
 ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
Nutrition Procedures Nutrition Prescription Protein Target Lower Protein Dose Higher Protein Dose 1.2 g/kg/day Calorie Target
 Nutrition Procedures Nutrition Prescription Protein and energy targets will be achieved through any combination of EN, protein supplements, and PN or amino acids. The only difference between the nutrition
Nutrition Procedures Nutrition Prescription Protein and energy targets will be achieved through any combination of EN, protein supplements, and PN or amino acids. The only difference between the nutrition
5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013
 5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following
5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following
Indirect Calorimetry: Clinical Implications in Critically Ill Patients
 Indirect Calorimetry: Clinical Implications in Critically Ill Patients Sharla Tajchman, PharmD, BCPS, BCNSP Critical Care / Nutrition Support Clinical Pharmacy Specialist University of Texas MD Anderson
Indirect Calorimetry: Clinical Implications in Critically Ill Patients Sharla Tajchman, PharmD, BCPS, BCNSP Critical Care / Nutrition Support Clinical Pharmacy Specialist University of Texas MD Anderson
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Control of Blood Glucose in the ICU: Reconciling the Conflicting Data
 Control of Blood Glucose in the ICU: Reconciling the Conflicting Data Steven E. Nissen MD Disclosure Consulting: Many pharmaceutical companies Clinical Trials: AbbVie, Amgen, Astra Zeneca, Esperion, Eli
Control of Blood Glucose in the ICU: Reconciling the Conflicting Data Steven E. Nissen MD Disclosure Consulting: Many pharmaceutical companies Clinical Trials: AbbVie, Amgen, Astra Zeneca, Esperion, Eli
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Relationship of Delayed Parenteral Nutrition Protocol with the Clinical Outcomes in a Medical Intensive Care Unit
 Original Article Clin Nutr Res 2014;3:33-38 pissn 2287-3732 eissn 2287-3740 Relationship of Delayed Parenteral Nutrition Protocol with the Clinical Outcomes in a Medical Intensive Care Unit Hosun Lee 1,
Original Article Clin Nutr Res 2014;3:33-38 pissn 2287-3732 eissn 2287-3740 Relationship of Delayed Parenteral Nutrition Protocol with the Clinical Outcomes in a Medical Intensive Care Unit Hosun Lee 1,
What s New in ICU Nutrition Research? Danielle Bear Principal Critical Care Dietitian St Thomas Hospital, London
 What s New in ICU Nutrition Research? Danielle Bear Principal Critical Care Dietitian St Thomas Hospital, London Outline Individualised nutrition support Defining energy targets Feeding route Current research
What s New in ICU Nutrition Research? Danielle Bear Principal Critical Care Dietitian St Thomas Hospital, London Outline Individualised nutrition support Defining energy targets Feeding route Current research
Relevance of non-nutritional calories in mechanically ventilated critically ill patients
 OPEN European Journal of Clinical Nutrition (2016) 70, 1443 1450 www.nature.com/ejcn ORIGINAL ARTICLE Relevance of non-nutritional calories in mechanically ventilated critically ill patients E Bousie 1,
OPEN European Journal of Clinical Nutrition (2016) 70, 1443 1450 www.nature.com/ejcn ORIGINAL ARTICLE Relevance of non-nutritional calories in mechanically ventilated critically ill patients E Bousie 1,
AUTHORS: Luisito O. Llido, MD (1), Mariana S. Sioson, MD (1,2), Jesus Fernando Inciong, MD (1), Grace Manuales, MD (1)
, Mariana S. Sioson, MD (1,2), Jesus Fernando Inciong, MD (1), Grace Manuales, MD (1)") 9 Submitted: September 5, 2011 Posted: January 7, 2012 TITLE: Nutrition team supervision on nutrient intake in critical care patients: report of a ten- year experience in the Philippines (years 2000 to
9 Submitted: September 5, 2011 Posted: January 7, 2012 TITLE: Nutrition team supervision on nutrient intake in critical care patients: report of a ten- year experience in the Philippines (years 2000 to
What other beneficial effects might GLN exert in critical illness??
 What other beneficial effects might GLN exert in critical illness?? Prevention of Enhanced Gut Permeability Who believes bacteria translocate from the gut to blood and cause infection? Yes No Bacteria
What other beneficial effects might GLN exert in critical illness?? Prevention of Enhanced Gut Permeability Who believes bacteria translocate from the gut to blood and cause infection? Yes No Bacteria
Protein dosing in the ICU: How much, when and why?
 Protein dosing in the ICU: How much, when and why? Dr. Gordon S. Doig, Associate Professor in Intensive Care Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney, Australia
Protein dosing in the ICU: How much, when and why? Dr. Gordon S. Doig, Associate Professor in Intensive Care Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney, Australia
Long term monitoring. Dr Alison Culkin Research Dietitian St Mark s Hospital
 Long term monitoring Dr Alison Culkin Research Dietitian St Mark s Hospital Patient 23 year old lady 1/4/14 Colectomy for UC 3-7/4/14 Ischaemic bowel 4 laparotomies Jejunostomy at 35 cm 23/5/14 Weight
Long term monitoring Dr Alison Culkin Research Dietitian St Mark s Hospital Patient 23 year old lady 1/4/14 Colectomy for UC 3-7/4/14 Ischaemic bowel 4 laparotomies Jejunostomy at 35 cm 23/5/14 Weight
6.4 Enteral Nutrition (Other): Gastrostomy vs. Nasogastric feeding January 31 st, 2009
: Gastrostomy vs. Nasogastric feeding January 31 st, 2009") 6.4 Enteral Nutrition (Other): Gastrostomy vs. Nasogastric feeding January 31 st, 2009 Recommendation: There are insufficient data to make a recommendation on gastrostomy feeding vs. nasogastric feeding
6.4 Enteral Nutrition (Other): Gastrostomy vs. Nasogastric feeding January 31 st, 2009 Recommendation: There are insufficient data to make a recommendation on gastrostomy feeding vs. nasogastric feeding
Calorie delivery and clinical outcomes in the critically ill: a systematic review and meta-analysis
 Calorie delivery and clinical outcomes in the critically ill: a systematic review and meta-analysis Harshel G Parikh, Asaf Miller, Marianne Chapman, John L Moran, Sandra L Peake The generally accepted
Calorie delivery and clinical outcomes in the critically ill: a systematic review and meta-analysis Harshel G Parikh, Asaf Miller, Marianne Chapman, John L Moran, Sandra L Peake The generally accepted
Nutrition in ECMO. Elize Craucamp RD(SA)
") Nutrition in ECMO Elize Craucamp RD(SA) ECMO What now!? KEEP CALM AND FEED THE ECMO PATIENT Despite the fact that little is known about nutritional strategies for adult ECMO patients! Neither overcomplicate
Nutrition in ECMO Elize Craucamp RD(SA) ECMO What now!? KEEP CALM AND FEED THE ECMO PATIENT Despite the fact that little is known about nutritional strategies for adult ECMO patients! Neither overcomplicate
Stellenwert der prä- und postoperativen Sicht des Chirurgen
 Interdisziplinäre Chirurgie Stellenwert der prä- und postoperativen Ernährung Sicht des Chirurgen Kantonsspital Luzern 24.11.2005 Prof. L. Krähenbühl Chirurgische Klinik Hôpital Cantonal Fribourg Problems
Interdisziplinäre Chirurgie Stellenwert der prä- und postoperativen Ernährung Sicht des Chirurgen Kantonsspital Luzern 24.11.2005 Prof. L. Krähenbühl Chirurgische Klinik Hôpital Cantonal Fribourg Problems
4.2a Composition of Enteral Nutrition: (Carbohydrate/fat): High fat/low CHO March 2013
: High fat/low CHO March 2013") 4.2a Composition of Enteral Nutrition: (Carbohydrate/fat): March 203 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following Summary of Evidence.
4.2a Composition of Enteral Nutrition: (Carbohydrate/fat): March 203 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following Summary of Evidence.
Heather Evans, MD University of Washington Seattle, WA
 Heather Evans, MD University of Washington Seattle, WA 1 American College of Surgeons Division of Education Heather L. Evans, MD, MS, FACS Nothing to disclose 2 Determine nutritional goals Determine when
Heather Evans, MD University of Washington Seattle, WA 1 American College of Surgeons Division of Education Heather L. Evans, MD, MS, FACS Nothing to disclose 2 Determine nutritional goals Determine when
Disclosures. None. Enteral Nutrition and Vasoactive Therapy! But actually.. Stocks Advisory boards Grants Speakers Bureau. Paul Marik, MD,FCCM,FCCP
 Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Intensive Care Nutrition. Dr Alan Race BSc(Hons) PhD FRCA
 PhD FRCA") Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Nutrition care plan for surgical patients. Objectives
 Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
4.2(a) Composition of Enteral Nutrition: (Carbohydrate/fat): High fat/low CHO January 31 st, 2009
 Composition of Enteral Nutrition: (Carbohydrate/fat): High fat/low CHO January 31 st, 2009") 4.(a) Composition of Enteral Nutrition: (Carbohydrate/fat): January 31 st, 009 Recommendation: There are insufficient data to recommend high fat/low CHO diets for critically ill patients. Discussion: The
4.(a) Composition of Enteral Nutrition: (Carbohydrate/fat): January 31 st, 009 Recommendation: There are insufficient data to recommend high fat/low CHO diets for critically ill patients. Discussion: The
SECTION 4: RECRUIT PARTICIPANTS
 SECTION 4: RECRUIT PARTICIPANTS Contents Participant Eligibility & Enrollment... 2 Screening... 2 Study ID Numbers... 2 Inclusion Criteria... 2 Exclusion Criteria... 4 Co-Enrollment... 5 Informed Consent
SECTION 4: RECRUIT PARTICIPANTS Contents Participant Eligibility & Enrollment... 2 Screening... 2 Study ID Numbers... 2 Inclusion Criteria... 2 Exclusion Criteria... 4 Co-Enrollment... 5 Informed Consent
Nutritional physiology of the critically ill patient
 Section 1 General Concepts Nutritional physiology of the critically ill patient David C. Frankenfield 1 Introduction Nutritional physiology refers to the role of food and nutrition in the function of the
Section 1 General Concepts Nutritional physiology of the critically ill patient David C. Frankenfield 1 Introduction Nutritional physiology refers to the role of food and nutrition in the function of the
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014
 5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014 2013 Recommendation: Based on 15 level 2 studies, small bowel feeding compared to gastric feeding
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014 2013 Recommendation: Based on 15 level 2 studies, small bowel feeding compared to gastric feeding
Protein Supplementation in the Pediatric Intensive Care Unit. Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017
 Protein Supplementation in the Pediatric Intensive Care Unit Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017 1 Objectives Basis for protein supplementation Challenges in monitoring
Protein Supplementation in the Pediatric Intensive Care Unit Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017 1 Objectives Basis for protein supplementation Challenges in monitoring
ESPEN Congress Vienna Nutritional implications of renal replacement therapy in ICU Nutritional consequences of RRT. E. Fiaccadori (Italy)
") ESPEN Congress Vienna 2009 Nutritional implications of renal replacement therapy in ICU Nutritional consequences of RRT E. Fiaccadori (Italy) Nutritional consequences of RRT Enrico Fiaccadori Internal
ESPEN Congress Vienna 2009 Nutritional implications of renal replacement therapy in ICU Nutritional consequences of RRT E. Fiaccadori (Italy) Nutritional consequences of RRT Enrico Fiaccadori Internal
Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines
 Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines 1 Presented on January 24, 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics Section of Critical Care Baylor College
Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines 1 Presented on January 24, 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics Section of Critical Care Baylor College
Cholestatic liver dysfunction during critical illness
 Cholestatic liver dysfunction during critical illness Yoo-Mee Vanwijngaerden Lies Langouche Dieter Mesotten Greet Van den Berghe Department of Cellular and Molecular Medicine Laboratory of Intensive Care
Cholestatic liver dysfunction during critical illness Yoo-Mee Vanwijngaerden Lies Langouche Dieter Mesotten Greet Van den Berghe Department of Cellular and Molecular Medicine Laboratory of Intensive Care
Early versus Late Parenteral Nutrition in Critically Ill Adults
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Early versus Late Parenteral Nutrition in Critically Ill Adults Michael P. Casaer, M.D., Dieter Mesotten, M.D., Ph.D., Greet Hermans,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Early versus Late Parenteral Nutrition in Critically Ill Adults Michael P. Casaer, M.D., Dieter Mesotten, M.D., Ph.D., Greet Hermans,
THE AUTHOR OF THIS WHAT S NEW IN NUTRITION? OBJECTIVES & OUTLINE EVIDENCE-BASED MEDICINE: PARENTERAL NUTRITION (PN)
") WHAT S NEW IN NUTRITION? Alisha Mutch, Pharm.D., BCPS THE AUTHOR OF THIS PRESENTATION HAS NOTHING TO DISCLOSE. OBJECTIVES & OUTLINE MALNUTRITION OBJECTIVES Indicate when parenteral nutrition (PN) is warranted
WHAT S NEW IN NUTRITION? Alisha Mutch, Pharm.D., BCPS THE AUTHOR OF THIS PRESENTATION HAS NOTHING TO DISCLOSE. OBJECTIVES & OUTLINE MALNUTRITION OBJECTIVES Indicate when parenteral nutrition (PN) is warranted
Citation Casaer MP, Mesotten D, (2011), Enteral nutrition: better navigation, yet unknown destination? Crit Care. 2011;15(6):1015.
, Enteral nutrition: better navigation, yet unknown destination? Crit Care. 2011;15(6):1015.") Citation Casaer MP, Mesotten D, (2011), Enteral nutrition: better navigation, yet unknown destination? Crit Care. 2011;15(6):1015. Archived version Author manuscript: the content is identical to the content
Citation Casaer MP, Mesotten D, (2011), Enteral nutrition: better navigation, yet unknown destination? Crit Care. 2011;15(6):1015. Archived version Author manuscript: the content is identical to the content
Energy-Dense versus Routine Enteral Nutrition in the Critically Ill
 Original Article Energy-Dense versus Routine Enteral Nutrition in the Critically Ill The TARGET Investigators, for the ANZICS Clinical Trials Group* ABSTRACT BACKGROUND The effect of delivering nutrition
Original Article Energy-Dense versus Routine Enteral Nutrition in the Critically Ill The TARGET Investigators, for the ANZICS Clinical Trials Group* ABSTRACT BACKGROUND The effect of delivering nutrition
ICU Acquired Weakness: Role of Specific Nutrients
 ICU Acquired Weakness: Role of Specific Nutrients Dr Jonathan TAN Senior Consultant Dept of Anaesthesiology, Intensive Care & Pain Medicine Tan Tock Seng Hospital, Singapore Purpose? Healthcare professionals?
ICU Acquired Weakness: Role of Specific Nutrients Dr Jonathan TAN Senior Consultant Dept of Anaesthesiology, Intensive Care & Pain Medicine Tan Tock Seng Hospital, Singapore Purpose? Healthcare professionals?
Metabolic monitoring in the ICU
 Metabolic monitoring in the ICU Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hô pital Cochin & Institut Cochin, Paris-F Conflicts of interest - Disclosure GE Healthcare Received
Metabolic monitoring in the ICU Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hô pital Cochin & Institut Cochin, Paris-F Conflicts of interest - Disclosure GE Healthcare Received
SASPEN: Meet the Expert. Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland
 SASPEN: Meet the Expert Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland 40 Ensuring my patients are properly fed. Nutrition therapy must be planned as any other ICU therapy
SASPEN: Meet the Expert Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland 40 Ensuring my patients are properly fed. Nutrition therapy must be planned as any other ICU therapy
Protein targets in critical illness
 Protein targets in critical illness Danielle Bear HEE / NIHR Clinical Doctoral Fellow & Critical Care Dietitian Guy s and St Thomas NHS Foundation Trust, London, UK @danni_dietitian CONFLICTS Conference
Protein targets in critical illness Danielle Bear HEE / NIHR Clinical Doctoral Fellow & Critical Care Dietitian Guy s and St Thomas NHS Foundation Trust, London, UK @danni_dietitian CONFLICTS Conference
ESPEN Congress Madrid 2018
 ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Diabetes-Specific Feeds M. Karipidou (GR) Dysglycaemia in acute patients with nutritional therapy Diabetes specific feeds
ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Diabetes-Specific Feeds M. Karipidou (GR) Dysglycaemia in acute patients with nutritional therapy Diabetes specific feeds
Nutrients, insulin and muscle wasting during critical illness
 32 nd annual meeting of the Belgian Society of Intensive Care Medicine June 15, 212 Nutrients, insulin and muscle wasting during critical illness Sarah Derde Introduction Critical illness: feeding-resistant
32 nd annual meeting of the Belgian Society of Intensive Care Medicine June 15, 212 Nutrients, insulin and muscle wasting during critical illness Sarah Derde Introduction Critical illness: feeding-resistant
5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015
 5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015 There were no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes to the
5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015 There were no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes to the
CASE STUDY ON INPATIENT MALNUTRITION DISCUSSION
 CASE STUDY ON INPATIENT MALNUTRITION Elena Kret-Sudjian MD, PhD, UC Davis Medical Center A 59 year-old white man with a history of diabetes, severe PVD, CKD IV, chronic hepatitis C admitted for non-healing
CASE STUDY ON INPATIENT MALNUTRITION Elena Kret-Sudjian MD, PhD, UC Davis Medical Center A 59 year-old white man with a history of diabetes, severe PVD, CKD IV, chronic hepatitis C admitted for non-healing
Malnutrition: Where are we headed?
 Malnutrition: Where are we headed? Kris M. Mogensen, MS, RD-AP, LDN, CNSC Team Leader Dietitian Brigham and Women s Hospital Instructor Boston University College of Health and Rehabilitation Sciences:
Malnutrition: Where are we headed? Kris M. Mogensen, MS, RD-AP, LDN, CNSC Team Leader Dietitian Brigham and Women s Hospital Instructor Boston University College of Health and Rehabilitation Sciences:
Prolonged Mechanical Ventilation
 Prolonged Mechanical Ventilation Shannon S. Carson, MD Associate Professor and Chief Pulmonary and Critical Care Medicine University of North Carolina AJRCCM 2010 Projected Growth of Prolonged Acute MV
Prolonged Mechanical Ventilation Shannon S. Carson, MD Associate Professor and Chief Pulmonary and Critical Care Medicine University of North Carolina AJRCCM 2010 Projected Growth of Prolonged Acute MV
A number of observational studies of adult
 Carol Rees Parrish, M.S., R.D., Series Editor Full Force Enteral Nutrition: A New Hope, or the Dark Side? A Critical Look at Enhanced Enteral Feeding Protocols Joe Krenitsky Enteral nutrition (EN) is the
Carol Rees Parrish, M.S., R.D., Series Editor Full Force Enteral Nutrition: A New Hope, or the Dark Side? A Critical Look at Enhanced Enteral Feeding Protocols Joe Krenitsky Enteral nutrition (EN) is the
Dr Ahmad Shaltut Othman Anaesthesiologist & Intensivist Hosp Sultanah Bahiyah Alor Setar
 FEEDING WITH FISH OIL Dr Ahmad Shaltut Othman Anaesthesiologist & Intensivist Hosp Sultanah Bahiyah Alor Setar New horizons in clinical nutrition from Support to Therapy Landmarks in Parenteral Nutrition
FEEDING WITH FISH OIL Dr Ahmad Shaltut Othman Anaesthesiologist & Intensivist Hosp Sultanah Bahiyah Alor Setar New horizons in clinical nutrition from Support to Therapy Landmarks in Parenteral Nutrition
Nutritional Management of Emergency Gastrointestinal (GI) Surgeries
 Surgeries") Nutritional Management of Emergency Gastrointestinal (GI) Surgeries Alexander, MD, FACS Introduction Emergency gastrointestinal (GI) surgery is different than elective GI surgery in many ways. Emergencies
Nutritional Management of Emergency Gastrointestinal (GI) Surgeries Alexander, MD, FACS Introduction Emergency gastrointestinal (GI) surgery is different than elective GI surgery in many ways. Emergencies