Class 3: Refeeding Syndrome. Liz Hudson MPH, RD
|
|
|
- Clinton Ferguson
- 6 years ago
- Views:
Transcription
1 Class 3: Refeeding Syndrome Liz Hudson MPH, RD
2 Case Study #1 NUTRITION ASSESSMENT: Consult PATIENT MEDICAL/HEALTH HISTORY: 49 y/o male with significant history of HTN, DM, and stage V CKD currently on ihd, admitted with gastroparesis refractory to Reglan and for consideration of J- tube placement. DIET HISTORY: Pt endorses poor appetite and inability to tolerate food. He reports nausea, emesis, abdominal pain, bloating and discomfort after eating. Intake described as bites of meals, estimates eating ¼ of baseline/usual intake. Pt states this has resulted in 100 lb wt loss over the past year. Pt denies trying any specific diet for helping to control his gastroparesis, but also does state that he is not able to tolerate most foods. NUTRITION FOCUSED PHYSICAL FINDINGS: Temporal hollowing and depression noted on physical exam. BODY COMPOSTION/WEIGHT HISTORY: HEIGHT: 182.9cm WEIGHT: 79.5kg (admit) IBW: 80.9kg UBW: 120.9kg (~ 1 year ago, per patient report) % WEIGHT CHANGE: BMI:
3 Case Study #2 NUTRITION ASSESSMENT: Consult PATIENT MEDICAL/HEALTH HISTORY: 56 y/o female with history of advanced stage III papillary serous carcinoma of the ovary s/p ex lap (exploratory laparotomy) with LOA (lysis of adhesions) and omentum biopsy (12/28/10), with carcinomatosis that is inoperable; status post 1 cycle of chemotherapy, started second cycle of carboplatin and taxol on 2/10/11. Admitted on 2/17/11 with diarrhea, hypokalemia and pancytopenia. GASTROINTESTINAL: N/V x 4 days. Stool loose and foul-smelling. DIET HISTORY: Pt endorses decreased intake since having surgery in December, and states she has been suffering from bouts of nausea and vomiting since starting chemotherapy. Pt estimates she is eating half of her usual intake. She does like Ensure, but has been only been consuming 1 daily. Pt reports eating ice cream with chocolate syrup and cottage cheese as meal replacements on the days she is feeling good. NUTRITION FOCUSED PHYSICAL FINDINGS: Cachectic; Overt muscle wasting noted on temporal and clavicular regions. Depression noted between ribs. BODY COMPOSTION/WEIGHT HISTORY: HEIGHT: 165.1cm WEIGHT: 44.9kg (admit) IBW: 56.8kg UBW: 50kg (12/27/10) % WEIGHT CHANGE: BMI:
4 Case Study #3 NUTRITION ASSESSMENT: Consult PATIENT MEDICAL/HEALTH HISTORY: 72 y/o female with no past medical history, who is admitted with new diagnosis of AML. Plan to initiate chemotherapy today. GASTROINTESTINAL: Pt reports taste changes, specifically things have been tasting off over the past 3-4 weeks. Denies any N/V/D/C. Thrush noted per H&P. DIET HISTORY: Pt states she has been eating a little less than usual over the past couple of weeks due to issues with food not tasting good. Pt noticed she is getting full on less food. Pt states she was still eating her meals, however only ¾ of them (no longer finishing her plate). Pt states she noticed her clothes are fitting looser than normal, but does not know if she has lost weight because she doesn t weigh herself. BODY COMPOSTION/WEIGHT HISTORY: HEIGHT: 149.9cm WEIGHT: 60.5kg IBW: 45.5kg UBW: 63.5kg (~4 weeks ago, per medical record) % WEIGHT CHANGE: BMI:
5 Case Study #4 NUTRITION ASSESMENT PATIENT MEDICAL/HEALTH HISTORY: Pt is a 60 y/o woman with a medical history significant for IBD here for acute exacerbation of her Ulcerative colitis. GASTROINTESTINAL: Pt experiencing worsening diarrhea and abdominal pain over the last 7 days. Bloody stools started 2 days which prompted patient to come to the ED. CRP markedly elevated upon arrival. DIET HISTORY: Patient reports decreased intake over the last week secondary to worsening abdominal pain and diarrhea. She has been trying to keep herself well hydrated. Prior to the onset of her symptoms, she says her ulcerative colitis was under good control, she was eating well. This past week she notes her intake to be ~75% of what she usually eats, some days may be less depending on severity of abdominal pain. FOOD INTAKE: NPO x 2 days. BODY COMPOSTION/WEIGHT HISTORY: HEIGHT: 164 cm ADMIT WEIGHT: 65.9kg (2/1) CURRENT WEIGHT: 64.6kg (2/11) % WEIGHT CHANGE: BMI:
6 Case Study #5 NUTRITION ASSESSMENT: LOS PATIENT MEDICAL/HEALTH HISTORY: 72 y/o male admitted for acute exacerbation of CHF with a medical history of moderate mitral regurgitation, acute on chronic systolic CHF, 3rd degree heart block, and iron deficiency anemia. Currently being diuresed. DIET HISTORY: Pt reports a variable appetite and intake, states he has good and bad days. He states he likes to graze throughout the day rather than eating large meals. He reports his weight fluctuates due to fluid status and it s not uncommon for his weight to go up and down 5 lbs from day to day. Pt noted to be eating a varied amount from meals (25-75% of meals) per nursing flowsheets. Pt states he has been missing meals due to tests/procedures while inpatient. BODY COMPOSTION/WEIGHT HISTORY: HEIGHT: 175.3cm ADMIT WEIGHT: 105.3kg CURRENT WEIGHT: 103kg UBW: lbs (per pt report) % WEIGHT CHANGE: BMI:
7 Syndrome A disease is a pathophysiological response to internal or external factors. A disorder is a disruption to regular bodily structure and function. A syndrome is a collection of signs and symptoms associated with a specific health-related cause.
8 Refeeding Syndrome Constellation of metabolic disturbances that occur as a result of reinstitution of nutrition to patients who are starved, severely malnourished or metabolically stressed due to severe illness.
9 Some definitions. EN Enteral Nutrition: provision of nutrition into the GI tract (either into stomach or small bowel) through a feeding tube PN Parenteral Nutrition: provision of nutrition to a person intravenously, bypassing the usual process of eating and digestion
10 Refeeding Syndrome What historical references do these articles discuss?
11 Brief Overview of fuel sources during starvation First 24hrs: Glucose is obtain through glycogen stored in the liver via glycogenolysis Once glycogen stores are depleted skeletal muscle is broken down to release amino acids for gluconeogenesis After ~72 hours, metabolic pathways shift to free fatty acid oxidation to preserve skeletal muscle
12 Depletion of vitamins and minerals Prolonged decreased nutrient intake can lead to depleted vitamin and mineral status, including phosphorus, potassium and magnesium Leads to loss of lean body mass, adipose tissue, and fluid With eventual reduction of visceral protein mass and function of vital organs Respiratory muscle wasting, reduced cardiac mass declined respiratory function, decreased cardiac output
13
14
15 Hypophosphatemia Results from cellular uptake of uptake of phosphorus, as well as increased need for phosphorylated intermediates for glycolysis (ATP, and 2,3-disphosphoglycerate) Can result in decreased oxygen delivery to cells, due to decreased levels of inorganic phosphates (2,3-DPG), which impairs oxygen release from hemoglobin Physiologic manifestations of hypophosphatemia can include neurologic, respiratory, cardiac, and immune function effects Normal range: mg/dl Severe hypophosphatemia: <1 1.5 mg/dl
16 Hypokalemia Results from cellular uptake of potassium, induced by insulin produced in response to the nutritional load Effects of moderate hypokalemia ( meq/l) include nausea, vomiting, constipation, and weakness Severe hypokalemia (<2.5 meq/l) may lead to respiratory failure, rhabdomyolysis and muscle necrosis, electrocardiogram (ECG) changes, cardiac arrhythmias, and paralysis
17 Hypomagnesemia Magnesium essential for a number of metabolic pathways including those involving ATP production If magnesium not addressed, may impact ability to correct serum phosphorus and potassium levels Reference range: mg/dl Hypomagnesemia: <1.5 mg/dl
18 First Step: Identify patients at risk Primary goal is to preventing refeeding syndrome, which means identifying those that may be at risk Patients at risk for refeeding may include those with: Anorexia nervosa Classic marasmus/kwashiokor Residents admitted from skilled nursing facilities Patients who have been unfed for 7-10 days with evidence of stress/depletion Chronic disease causing undernutrition (examples?) History of excessive alcohol intake Morbid obesity with massive weight loss
19 Patients at risk for refeeding syndrome In order to prevent refeeding syndrome, this identification should occur prior to the initiation of nutrition support What are some considerations when evaluating lab values of minerals prior to initiation of nutrition support? Do normal levels mean there is not depletion? Normal serum levels may not be reflective of actual stores, these patients are likely to have depletion
20 Preventing Refeeding Syndrome Once nutrition support is initiated, it is essential to avoid overfeeding Rule of thumb: start low and go slow Day initiation recommendations: Start at 25% of estimated goal energy needs Gradually increase to goal over 3-5 days, maybe longer Any electrolyte abnormalities should corrected prior to initiation
21 Other considerations. Total fluid volume needs to be considered when making your recommendations These patients may have diminished cardiac reserve and are susceptible to fluid overload, fluid and sodium may need to minimized initially Good rule of thumb: Keep fluid 1000ml or less in first few days Monitor weight as well, weight gain >1kg/week may indicate fluid retention
22 Prevention: Identify those at risk Conservative initiation of nutrition support along with aggressive monitoring and replacement of electrolytes via IV Can use kcal/kg or % of total calorie goal Must keep in mind delivery of carbohydrate, as well as total fluid
23 Prevention Nutrition support should begin at 25% of estimated energy needs and advanced gradually to goal over the next 3-5 days Serum potassium, phosphorus and magnesium should be monitored closely twice daily during the first few days while advancing to goal Electrolytes should be supplemented preferably via IV, or via oral supplementation when appropriate. Why? Thiamine supplementation should be started without need to check serum or whole blood thiamine levels (100mg/day for at least the first week) Also usually receive 1mg folic acid daily for 7 days as water soluble vitamin deficiencies can occur rapidly
24 Treatment Patient starts to exhibit signs or symptoms of refeeding, what next? What do we do with regard to their nutrition support? Aggressive electrolyte replacement When and how should we restart nutrition support?
25 Example in article MH is a 73-year-old nursing home resident. She has a history of cerebrovascular accident approximately four months prior to admission resulting in dysphagia; she has been on a pureed diet with thickened liquids. Since that time her medical history includes hypertension, atrial fibrillation and asthma. MH is admitted to the hospital with fever, aspiration pneumonia, and dehydration. She is made NPO; IV fluids are started (D5, 1 2NS). A modified barium swallow demonstrates aspiration with all consistencies. Nasogastric feedings are initiated according to standard protocol. A weight obtained the following day is 56 kg; her weight at the time of her stroke four months earlier was 65 kg. The following day, MH developed worsening respiratory distress and was transferred to the ICU for further care. The results of her blood chemistries were: phosphorous 1.1 magnesium 1.3 potassium 2.9
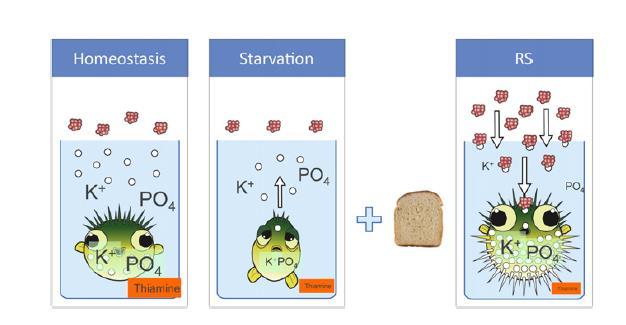
26 Summary of important points After prolonged malnutrition or starvation, the provision of parenteral or enteral nutrition support results in a sudden and dramatic shift back to glucose as a primary fuel. Insulin levels also increase to drive glucose into cells for use An increased demand for phosphorylated intermediates of glycolysis, such as adenosine triphosphate (ATP), results.
27 Summary of important points Increased insulin secretion results in rapid entrance of phosphorus, potassium, and magnesium into cells, exacerbating already low levels of these electrolytes. Furthermore, insulin exerts an antidiuretic effect, leading to sodium and water retention that result in the expansion of the extracellular water compartment.
28 Summary of Important Points Important to identify persons at risk for refeeding and take steps to prevent it Initiation of nutrition support at conservative goal with gradual progression over several days to goal Close monitoring of serum electrolyte levels Aggressive repletion of electrolytes as indicated and as well as supplementation of thiamin
29
Inflammatory Bowel Disease
 + Inflammatory Bowel Disease Christina Kalafsky, Dietetic Intern University of Maryland College Park Children s National Medical Center Case Study January 31, 2014 + Outline n Inflammatory Bowel Disease
+ Inflammatory Bowel Disease Christina Kalafsky, Dietetic Intern University of Maryland College Park Children s National Medical Center Case Study January 31, 2014 + Outline n Inflammatory Bowel Disease
Acute management of severe malnutrition. Dr Simon Gabe St Mark s Hospital, London
 Acute management of severe malnutrition Dr Simon Gabe St Mark s Hospital, London Malnutrition definition A state resulting from lack of uptake or intake of nutrition leading to altered body composition
Acute management of severe malnutrition Dr Simon Gabe St Mark s Hospital, London Malnutrition definition A state resulting from lack of uptake or intake of nutrition leading to altered body composition
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives
 Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
Nutrition. By Dr. Ali Saleh 2/27/2014 1
 Nutrition By Dr. Ali Saleh 2/27/2014 1 Nutrition Functions of nutrients: Providing energy for body processes and movement. Providing structural material for body tissues. Regulating body processes. 2/27/2014
Nutrition By Dr. Ali Saleh 2/27/2014 1 Nutrition Functions of nutrients: Providing energy for body processes and movement. Providing structural material for body tissues. Regulating body processes. 2/27/2014
Case Study BMIs in the range of are considered overweight. Therefore, F.V. s usual BMI indicates that she was overweight.
 Morgan McFarlane February 26 th, 2013 HHP 439 Professor White Case Study 7.10 1. What is your interpretation of F.V. s clinical data? F.V. s clinical data includes chronic abdominal pain, loose stools,
Morgan McFarlane February 26 th, 2013 HHP 439 Professor White Case Study 7.10 1. What is your interpretation of F.V. s clinical data? F.V. s clinical data includes chronic abdominal pain, loose stools,
CASE STUDY: ULCERATIVE COLITIS. Sammi Montag Dietetic Intern
 CASE STUDY: ULCERATIVE COLITIS Sammi Montag Dietetic Intern 2013-2014 PATIENT (CK) INTRODUCTION 26 year old female Chief complaint: bloody diarrhea and abdominal pain Admitting diagnosis: Ulcerative colitis
CASE STUDY: ULCERATIVE COLITIS Sammi Montag Dietetic Intern 2013-2014 PATIENT (CK) INTRODUCTION 26 year old female Chief complaint: bloody diarrhea and abdominal pain Admitting diagnosis: Ulcerative colitis
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ
 Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
Refeeding syndrome a practical approach
 Refeeding syndrome a practical approach PENG pre-bapen Conference Teaching Day Birmingham Monday 20 th November 2017 Rhys White Acting Clinical and Operational Lead Dietitian Guys and St Thomas NHS Foundation
Refeeding syndrome a practical approach PENG pre-bapen Conference Teaching Day Birmingham Monday 20 th November 2017 Rhys White Acting Clinical and Operational Lead Dietitian Guys and St Thomas NHS Foundation
Esophageal Cancer Treated with Surgery and Radiation Case Study (Evaluation and ADIME Note)
") Esophageal Cancer Treated with Surgery and Radiation Case Study (Evaluation and ADIME Note) Nutritional care plan: N.S. is a 58 yr old male. His serum albumin is below normal with a value of 3.1L (9/5)
Esophageal Cancer Treated with Surgery and Radiation Case Study (Evaluation and ADIME Note) Nutritional care plan: N.S. is a 58 yr old male. His serum albumin is below normal with a value of 3.1L (9/5)
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter
 Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Nutrition. Chapter 45. Reada Almashagba
 Nutrition Chapter 45 1 Nutrition: - Nutrient are organic substances found in food and are required for body function - No one food provide all essential nutrient Major function of nutrition: providing
Nutrition Chapter 45 1 Nutrition: - Nutrient are organic substances found in food and are required for body function - No one food provide all essential nutrient Major function of nutrition: providing
Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points. Ht: 5 11 Current wt: 156 # UBW: 167 # Serum albumin: 3.
 Name: Wan yi Wang Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He is currently suffering from
Name: Wan yi Wang Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He is currently suffering from
Major Case Study: Enteral and Parenteral Nutrition
 Major Case Study: Enteral and Parenteral Nutrition Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He is currently suffering from a severe concussion and lapses of consciousness,
Major Case Study: Enteral and Parenteral Nutrition Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He is currently suffering from a severe concussion and lapses of consciousness,
Shyana Sadiq DFM 484: MNT Case Study 33: Esophageal Cancer Treated with Surgery and Radiation 10/14/2013
 Shyana Sadiq DFM 484: MNT Case Study 33: Esophageal Cancer Treated with Surgery and Radiation 10/14/2013 I. Understanding the Disease and Pathophysiology 1. Mr. Seyer has been diagnosed with adenocarcinoma
Shyana Sadiq DFM 484: MNT Case Study 33: Esophageal Cancer Treated with Surgery and Radiation 10/14/2013 I. Understanding the Disease and Pathophysiology 1. Mr. Seyer has been diagnosed with adenocarcinoma
Introduction to Clinical Nutrition
 M-III Introduction to Clinical Nutrition Donald F. Kirby, MD Chief, Section of Nutrition Division of Gastroenterology 1 Things We Take for Granted Air to Breathe Death Taxes Another Admission Our Next
M-III Introduction to Clinical Nutrition Donald F. Kirby, MD Chief, Section of Nutrition Division of Gastroenterology 1 Things We Take for Granted Air to Breathe Death Taxes Another Admission Our Next
Nutrition Intervention After Gastric Bypass Revision
 Nutrition Intervention After Gastric Bypass Revision With an Anastomotic Leak Ali Fox- Montana Dietetic Intern Objectives 1. Describe the etiology of anastomotic leak post Roux-en-Y gastric bypass (G.B.)
Nutrition Intervention After Gastric Bypass Revision With an Anastomotic Leak Ali Fox- Montana Dietetic Intern Objectives 1. Describe the etiology of anastomotic leak post Roux-en-Y gastric bypass (G.B.)
Small Bowel Obstruction after operation in a severely malnourished man. By: Ms Bounmark Phoumesy
 Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Intensive Care Nutrition. Dr Alan Race BSc(Hons) PhD FRCA
 PhD FRCA") Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION
 ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines
 Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
Chapter 20. Assisting With Nutrition and Fluids
 Chapter 20 Assisting With Nutrition and Fluids Food and water: Are physical needs Basics of Nutrition Are necessary for life A poor diet and poor eating habits: Increase the risk for diseases and infection
Chapter 20 Assisting With Nutrition and Fluids Food and water: Are physical needs Basics of Nutrition Are necessary for life A poor diet and poor eating habits: Increase the risk for diseases and infection
Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points. Ht: 5 11 Current wt: 156 # UBW: 167 # Serum albumin: 3.
 NUT 116BL Winter 2015 Name: yimeng Ma Section: Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He
NUT 116BL Winter 2015 Name: yimeng Ma Section: Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He
Neoplastic Disease KNH 406
 Neoplastic Disease KNH 406 Cancer Carcinogenesis - Etiology Genes may be affected by antioxidants, soy, protein, fat, kcal, alcohol Nutritional genomics study of genetic variations that cause different
Neoplastic Disease KNH 406 Cancer Carcinogenesis - Etiology Genes may be affected by antioxidants, soy, protein, fat, kcal, alcohol Nutritional genomics study of genetic variations that cause different
Dutch consensus statement on Refeeding syndrome
 Dutch consensus statement on Refeeding syndrome Introduction Disease related malnutrition is a common problem in health care. The refeeding syndrome is defined as the severe and potentially fatal shifts
Dutch consensus statement on Refeeding syndrome Introduction Disease related malnutrition is a common problem in health care. The refeeding syndrome is defined as the severe and potentially fatal shifts
HOMES AND SENIORS SERVICES. APPROVAL DATE: February 2011 REVISION DATE: January 2015; July 2018
 POLICY: Page 1 of 6 A resident requiring enteral (tube) feeding as a sole source or adjunctive nutrition support have access to a comprehensive enteral feeding program and receive appropriate support from
POLICY: Page 1 of 6 A resident requiring enteral (tube) feeding as a sole source or adjunctive nutrition support have access to a comprehensive enteral feeding program and receive appropriate support from
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Guideline (2010) Chronic Kidney Disease CKD: Executive Summary of Recommendations (2010) Executive Summary of Recommendations Below are the major recommendations
Chronic Kidney Disease Chronic Kidney Disease (CKD) Guideline (2010) Chronic Kidney Disease CKD: Executive Summary of Recommendations (2010) Executive Summary of Recommendations Below are the major recommendations
NUTRITION. Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017
 NUTRITION Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017 Step One Competency 1.19 Factors contributing to nutritional impairment in critical illness. Nutritional
NUTRITION Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017 Step One Competency 1.19 Factors contributing to nutritional impairment in critical illness. Nutritional
MUST and Malnutrition
 MUST and Malnutrition Presenter Housekeeping Northern Devon Healthcare NHS Trust Confidentiality To respect confidentiality within the group unless it is necessary to address a current concern about the
MUST and Malnutrition Presenter Housekeeping Northern Devon Healthcare NHS Trust Confidentiality To respect confidentiality within the group unless it is necessary to address a current concern about the
WSVMA Annual Conference
 WSVMA Annual Conference Equine Nutrition Spokane Convention Center Spokane, Washington October 1-3, 2010 Steve Duren, PhD Performance Horse Nutrition, Weiser, ID Stephen Duren, MS, PhD, PAS Performance
WSVMA Annual Conference Equine Nutrition Spokane Convention Center Spokane, Washington October 1-3, 2010 Steve Duren, PhD Performance Horse Nutrition, Weiser, ID Stephen Duren, MS, PhD, PAS Performance
Dignity and Nutrition for Older People
 South Gloucestershire Community Health Services Dignity and Nutrition for Older People Lorraine Norris Nutrition and Dietetic Professional Lead South Gloucestershire Community Health November 9th 2011
South Gloucestershire Community Health Services Dignity and Nutrition for Older People Lorraine Norris Nutrition and Dietetic Professional Lead South Gloucestershire Community Health November 9th 2011
CHAPTER 10: Diet and nutrition & effect on physical activity and performance Practice questions - text book pages
 QUESTIONS AND ANSWERS CHAPTER 10: Diet and nutrition & effect on physical activity and performance Practice questions - text book pages 144-145 1) Complex carbohydrates do not include: a. lipids. b. triglycerides.
QUESTIONS AND ANSWERS CHAPTER 10: Diet and nutrition & effect on physical activity and performance Practice questions - text book pages 144-145 1) Complex carbohydrates do not include: a. lipids. b. triglycerides.
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS
 NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
Managing Nutrition and Unintended Weight Loss
 Managing Nutrition and Unintended Weight Loss Kathleen Niedert, PhD, RD, CSG, FADA, LNHA 2018 Spring Conference & Exhibitor Show May 2-3, 2018 OBJECTIVES Define the three main categories and three primary
Managing Nutrition and Unintended Weight Loss Kathleen Niedert, PhD, RD, CSG, FADA, LNHA 2018 Spring Conference & Exhibitor Show May 2-3, 2018 OBJECTIVES Define the three main categories and three primary
Pediatric Nutrition Care as a strategy to prevent hospital malnutrition. Div Pediatric Nutrition and Metabolic Diseases Dept of Child Health
 Pediatric Nutrition Care as a strategy to prevent hospital malnutrition Div Pediatric Nutrition and Metabolic Diseases Dept of Child Health Child is not a miniature adult Specific for child growth and
Pediatric Nutrition Care as a strategy to prevent hospital malnutrition Div Pediatric Nutrition and Metabolic Diseases Dept of Child Health Child is not a miniature adult Specific for child growth and
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Nutritional intervention in hospitalised paediatric patients. Dr Y.K.Amdekar
 Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Information about Feeding Tubes
 Information about Feeding Tubes By Theresa Imperato, RN and Lorraine Danowski, RD What is a feeding tube? It is a small, flexible tube, about ¼ in diameter that is an alternative route for nourishment
Information about Feeding Tubes By Theresa Imperato, RN and Lorraine Danowski, RD What is a feeding tube? It is a small, flexible tube, about ¼ in diameter that is an alternative route for nourishment
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor
 Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
Chapter 23. Nutrition Needs. Copyright 2019 by Elsevier, Inc. All rights reserved.
 Chapter 23 Nutrition Needs Copyright 2019 by Elsevier, Inc. All rights reserved. Lesson 23.1 Define the key terms and key abbreviations in this chapter. Explain the purpose and use of the MyPlate symbol.
Chapter 23 Nutrition Needs Copyright 2019 by Elsevier, Inc. All rights reserved. Lesson 23.1 Define the key terms and key abbreviations in this chapter. Explain the purpose and use of the MyPlate symbol.
Refeeding Low Weight Adolescents with AN
 RCPsych ED 2013 Refeeding Low Weight Adolescents with AN Graeme O Connor RD PhD Research Student -UCL Specialist paediatric Dietitian Great Ormond Street Hospital Foundation Trust Pathophysiology of starvation
RCPsych ED 2013 Refeeding Low Weight Adolescents with AN Graeme O Connor RD PhD Research Student -UCL Specialist paediatric Dietitian Great Ormond Street Hospital Foundation Trust Pathophysiology of starvation
EXSC- STANDARD 14. Nutrients
 SPORTS NUTRITION EXSC- STANDARD 14 Nutrients Standard 14 Gather relevant information from multiple authoritative print and digital sources related to the importance of a balanced diet in the achievement
SPORTS NUTRITION EXSC- STANDARD 14 Nutrients Standard 14 Gather relevant information from multiple authoritative print and digital sources related to the importance of a balanced diet in the achievement
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
Case Study: Celiac Disease
 Case Study: Celiac Disease 21 yo F currently attending UC Davis. She is a swimmer for the UC Davis swim team and trains extensively throughout the year. She is 5'5 and weighs 52 kg. Her UBW is 130lbs CC:
Case Study: Celiac Disease 21 yo F currently attending UC Davis. She is a swimmer for the UC Davis swim team and trains extensively throughout the year. She is 5'5 and weighs 52 kg. Her UBW is 130lbs CC:
Disclosures. Learning Objectives 4/21/2015. Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis. None
 Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis Robert DeChicco MS, RD, LD, CNSC Manager, Nutrition Support Team Center for Human Nutrition Cleveland Clinic Health System,
Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis Robert DeChicco MS, RD, LD, CNSC Manager, Nutrition Support Team Center for Human Nutrition Cleveland Clinic Health System,
FND 431 Clinical Experience Case Study! Introduction!
 FND 431 Clinical Experience Case Study Jennifer Millard Introduction Ms. B is a Type II diabetic with ESRD who has been receiving dialysis since April of 2013. Previously, she has shown excellent compliance
FND 431 Clinical Experience Case Study Jennifer Millard Introduction Ms. B is a Type II diabetic with ESRD who has been receiving dialysis since April of 2013. Previously, she has shown excellent compliance
CASE STUDY REPORT: NUTRITIONAL MANAGEMENT OF CROHN S DISEASE
 CASE STUDY REPORT: NUTRITIONAL MANAGEMENT OF CROHN S DISEASE Lindsey Warren, MS ARAMARK Dietetic Intern Providence Medical Center February 13 th, 2012 Crohn s Disease and Malnutrition Medication Malabsorption
CASE STUDY REPORT: NUTRITIONAL MANAGEMENT OF CROHN S DISEASE Lindsey Warren, MS ARAMARK Dietetic Intern Providence Medical Center February 13 th, 2012 Crohn s Disease and Malnutrition Medication Malabsorption
Nutrition Services at a glance
 Nutrition Services at a glance Ragini Raghuveer, MS, RD, LD/N Systems Clinical Nutrition Manager Linette De Armas, RD, LD/N Clinical Dietitian Melissa Lorenzo, RD, LD/N Clinical Dietitian 1 Learning Objectives
Nutrition Services at a glance Ragini Raghuveer, MS, RD, LD/N Systems Clinical Nutrition Manager Linette De Armas, RD, LD/N Clinical Dietitian Melissa Lorenzo, RD, LD/N Clinical Dietitian 1 Learning Objectives
Nutrition in Pancreatic Cancer. Edmond Sung Consultant Gastroenterologist Lead Clinician for Clinical Nutrition and Endoscopy
 Nutrition in Pancreatic Cancer Edmond Sung Consultant Gastroenterologist Lead Clinician for Clinical Nutrition and Endoscopy Overview The pancreas and nutrition Nutrition screening - can we do this well?
Nutrition in Pancreatic Cancer Edmond Sung Consultant Gastroenterologist Lead Clinician for Clinical Nutrition and Endoscopy Overview The pancreas and nutrition Nutrition screening - can we do this well?
Section K Swallowing/ Nutritional Status
 Instructor Guide Section K Swallowing/ Nutritional Status Objectives State the intent of Section K Swallowing and Nutritional Status. Describe how to conduct an assessment of a resident s nutritional status.
Instructor Guide Section K Swallowing/ Nutritional Status Objectives State the intent of Section K Swallowing and Nutritional Status. Describe how to conduct an assessment of a resident s nutritional status.
The Role of Parenteral Nutrition. in PEDIATRIC INTENSIVE CARE UNIT. Dzulfikar DLH. Pediatric Emergency and Intensive Care Unit
 The Role of Parenteral Nutrition in PEDIATRIC INTENSIVE CARE UNIT Dzulfikar DLH Pediatric Emergency and Intensive Care Unit Department of Child Health, Faculty of Medicine Universitas Padjajaran, Hasan
The Role of Parenteral Nutrition in PEDIATRIC INTENSIVE CARE UNIT Dzulfikar DLH Pediatric Emergency and Intensive Care Unit Department of Child Health, Faculty of Medicine Universitas Padjajaran, Hasan
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Parenteral Nutrition in Oncology
 Parenteral Nutrition in Oncology Presenter: Pam Wagner, RD, CNSC Learning Objectives List indications for initiating PN in oncology patients Describe considerations when determining an appropriate candidate
Parenteral Nutrition in Oncology Presenter: Pam Wagner, RD, CNSC Learning Objectives List indications for initiating PN in oncology patients Describe considerations when determining an appropriate candidate
Jennifer L. Gaudiani, MD, CEDS. Assistant Medical Director, ACUTE Associate Professor of Medicine, University of Colorado
 Jennifer L. Gaudiani, MD, CEDS Assistant Medical Director, ACUTE Associate Professor of Medicine, University of Colorado Who are ACUTE patients? 17 65 years old (average 26) 10% men Average BMI on admission
Jennifer L. Gaudiani, MD, CEDS Assistant Medical Director, ACUTE Associate Professor of Medicine, University of Colorado Who are ACUTE patients? 17 65 years old (average 26) 10% men Average BMI on admission
NUT 116BL Name: Jeana Lim Section: A01 Winter 2013
 NUT 116BL Name: Jeana Lim Section: A01 Winter 2013 Case Study #3: Renal Disease 50 points 1. Please be concise and use only the space provided. 2. Please cite sources as necessary. 3. You may use your
NUT 116BL Name: Jeana Lim Section: A01 Winter 2013 Case Study #3: Renal Disease 50 points 1. Please be concise and use only the space provided. 2. Please cite sources as necessary. 3. You may use your
Adaptation and re-feeding Hypokalemia Bone complications
 Adaptation and re-feeding Hypokalemia Bone complications René Klinkby Støving Odense University Hospital Denmark 10% 20% 30% 40% BMI 18.5 BMI 16.5 BMI 14.5 BMI 12.5 Willmore DW, The Metabolic Management
Adaptation and re-feeding Hypokalemia Bone complications René Klinkby Støving Odense University Hospital Denmark 10% 20% 30% 40% BMI 18.5 BMI 16.5 BMI 14.5 BMI 12.5 Willmore DW, The Metabolic Management
Chapter 27 & 28. Key Terms. Digestive System. Fig. 27-1, p. 443 Also known as the Gastrointestinal System (GI system)
") Chapter 27 & 28 Nutrition & Fluids Key Terms Aspiration Dehydration Edema Dysphagia Gastrostomy tube Intravenous therapy (IV) Digestive System Fig. 27-1, p. 443 Also known as the Gastrointestinal System
Chapter 27 & 28 Nutrition & Fluids Key Terms Aspiration Dehydration Edema Dysphagia Gastrostomy tube Intravenous therapy (IV) Digestive System Fig. 27-1, p. 443 Also known as the Gastrointestinal System
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS
 Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
NUTRITION & MALIGNANCY: An Overview
 NUTRITION & MALIGNANCY: An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ Temple 1 Malignancy and Weight loss (Cachexia)
NUTRITION & MALIGNANCY: An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ Temple 1 Malignancy and Weight loss (Cachexia)
Pediatric Dehydration and Oral Rehydration. May 16/17
 Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
4º ESO PRINCIPLES OF TRAINING FOOD BALANCE DIET PHYSICAL EDUCATION DIET AND ENERGY DIET AND SPORT
 4º ESO PRINCIPLES OF TRAINING FOOD BALANCE DIET DIET AND ENERGY PHYSICAL EDUCATION DIET AND SPORT FOUR BASIC PRINCIPLES OF TRAINING Specificity Overload Progression Reversibility Training needs to be done
4º ESO PRINCIPLES OF TRAINING FOOD BALANCE DIET DIET AND ENERGY PHYSICAL EDUCATION DIET AND SPORT FOUR BASIC PRINCIPLES OF TRAINING Specificity Overload Progression Reversibility Training needs to be done
Formulary and Prescribing Guidelines
 Formulary and Prescribing Guidelines SECTION 15: TREATMENT OF EATING DISORDERS 15.1 Introduction Please review the Trust document Guidelines for the assessment and treatment of eating disorders in the
Formulary and Prescribing Guidelines SECTION 15: TREATMENT OF EATING DISORDERS 15.1 Introduction Please review the Trust document Guidelines for the assessment and treatment of eating disorders in the
Nutritional Demands of Disease and Trauma
 al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
LONG-TERM NUTRITIONAL CONSIDERATIONS AFTER SPINAL CORD INJURY AND/OR TRAUMATIC BRAIN INJURY
 LONG-TERM NUTRITIONAL CONSIDERATIONS AFTER SPINAL CORD INJURY AND/OR TRAUMATIC BRAIN INJURY Angela Luciani, RD, LDN Magee Rehabilitation Hospital Philadelphia, PA SPEAKER DISCLOSURE STATEMENT Angela Luciani
LONG-TERM NUTRITIONAL CONSIDERATIONS AFTER SPINAL CORD INJURY AND/OR TRAUMATIC BRAIN INJURY Angela Luciani, RD, LDN Magee Rehabilitation Hospital Philadelphia, PA SPEAKER DISCLOSURE STATEMENT Angela Luciani
Nutrition for Cancer. Nutrition for Cancer. Patients. Geoffrey Axiak. Clinical Nutrition Nurse Mater Dei Hospital
 Nutrition for Cancer Nutrition for Cancer Patients Geoffrey Axiak Clinical Nutrition Nurse Mater Dei Hospital Change in Energy Expenditure in Change in Energy Expenditure in Disease (Northwestern University
Nutrition for Cancer Nutrition for Cancer Patients Geoffrey Axiak Clinical Nutrition Nurse Mater Dei Hospital Change in Energy Expenditure in Change in Energy Expenditure in Disease (Northwestern University
L.Mageswary Dietitian Hospital Selayang
 L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
Pressure Ulcers ecourse
 Pressure Ulcers ecourse Module 5.5: Nutrition Guidelines Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Module 5.5: Nutrition
Pressure Ulcers ecourse Module 5.5: Nutrition Guidelines Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Module 5.5: Nutrition
Nutrients are: water carbohydrates lipids proteins. minerals vitamins fiber
 Nutrients are: water carbohydrates lipids proteins minerals vitamins fiber WATER Essential nutrient 55-65% body weight Body loses water through evaporation, excretion, and respiration The only nutrient
Nutrients are: water carbohydrates lipids proteins minerals vitamins fiber WATER Essential nutrient 55-65% body weight Body loses water through evaporation, excretion, and respiration The only nutrient
Chapter 7- Metabolism: Transformations and Interactions Thomson - Wadsworth
 Chapter 7- Metabolism: Transformations and Interactions 2008 Thomson - Wadsworth Simple Overview of Energy Metabolism The sum of all chemical reactions that go on in living cells Introduction Energy Heat-
Chapter 7- Metabolism: Transformations and Interactions 2008 Thomson - Wadsworth Simple Overview of Energy Metabolism The sum of all chemical reactions that go on in living cells Introduction Energy Heat-
HISTORY OF THE KETOGENIC DIET
 Laura Roche RD Horizon Health Authority May 29, 2018 AGENDA History of the Ketogenic Diet Diet Pathophysiology Side Effects Pros and Cons How and Why the Diet works Ketogenic Diet for Type 2 Diabetes Ketogenic
Laura Roche RD Horizon Health Authority May 29, 2018 AGENDA History of the Ketogenic Diet Diet Pathophysiology Side Effects Pros and Cons How and Why the Diet works Ketogenic Diet for Type 2 Diabetes Ketogenic
Amanda Hernandez FND October 17, 2011 Enteral Feeding Case Study
 Amanda Hernandez FND 430-001 October 17, 2011 Enteral Feeding Case Study 1. Nutritional Assessment to determine energy and protein needs Percent Usual Body Weight [(current body weight/usual body weight)
Amanda Hernandez FND 430-001 October 17, 2011 Enteral Feeding Case Study 1. Nutritional Assessment to determine energy and protein needs Percent Usual Body Weight [(current body weight/usual body weight)
GUIDANCE NOTES. DIETETIC RISK ASSESSMENT FOR REFEEDING RECOMMENDED MEAL PLANS When commencing re-feeding: NICE (2006)
") When commencing re-feeding: NICE (2006) NICE (2006) Clinical Guideline 32 Nutrition support in adults: oral nutrition support, enteral tube feeding and parenteral nutrition (The following is based on www.nice.org.uk/cg032
When commencing re-feeding: NICE (2006) NICE (2006) Clinical Guideline 32 Nutrition support in adults: oral nutrition support, enteral tube feeding and parenteral nutrition (The following is based on www.nice.org.uk/cg032
Laparoscopic Gastric Bypass Information
 1441 Constitution Boulevard, Salinas, CA 93906 (831) 783-2556 www.natividad.com/weight-loss (Roux-en-Y Gastric Bypass) What is gastric bypass surgery? Gastric bypass surgery, a type of bariatric surgery
1441 Constitution Boulevard, Salinas, CA 93906 (831) 783-2556 www.natividad.com/weight-loss (Roux-en-Y Gastric Bypass) What is gastric bypass surgery? Gastric bypass surgery, a type of bariatric surgery
Energy Metabolism. Chapter Cengage Learning. All Rights Reserved.
 Energy Metabolism Chapter 7 Introduction Energy Heat, mechanical, electrical, and chemical Metabolism How the body uses foods to meet its needs Chemical Reactions in the Body Energy metabolism How body
Energy Metabolism Chapter 7 Introduction Energy Heat, mechanical, electrical, and chemical Metabolism How the body uses foods to meet its needs Chemical Reactions in the Body Energy metabolism How body
Nutritional Demands of Disease and Trauma
 Nutritional Demands of Disease and Trauma Lecture 89 2000 Northwestern University Medical School Nutritional Requirements Based on needs to support optimal physiological function Are changed by disease
Nutritional Demands of Disease and Trauma Lecture 89 2000 Northwestern University Medical School Nutritional Requirements Based on needs to support optimal physiological function Are changed by disease
KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing Pediatrics Case Studies: Child Dehydration
 Courtney Wiener 9/9/10 KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing 30020 - Pediatrics Case Studies: Child Dehydration Introduction: Dehydration can be life threatening to a child since a majority
Courtney Wiener 9/9/10 KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing 30020 - Pediatrics Case Studies: Child Dehydration Introduction: Dehydration can be life threatening to a child since a majority
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetate, in pediatric surgical patients, 525 526 Acute respiratory distress syndrome (ARDS), immune-modulating nutrition in, 584 585 Aerobic
Index Note: Page numbers of article titles are in boldface type. A Acetate, in pediatric surgical patients, 525 526 Acute respiratory distress syndrome (ARDS), immune-modulating nutrition in, 584 585 Aerobic
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
FLUIDS AND ELECTROLYTES
 FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
Parenteral Nutrition in IBD: Any indication?
 Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
CASE STUDY ON INPATIENT MALNUTRITION DISCUSSION
 CASE STUDY ON INPATIENT MALNUTRITION Elena Kret-Sudjian MD, PhD, UC Davis Medical Center A 59 year-old white man with a history of diabetes, severe PVD, CKD IV, chronic hepatitis C admitted for non-healing
CASE STUDY ON INPATIENT MALNUTRITION Elena Kret-Sudjian MD, PhD, UC Davis Medical Center A 59 year-old white man with a history of diabetes, severe PVD, CKD IV, chronic hepatitis C admitted for non-healing
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers
 WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
SERUM PHOSPHORUS TESTING
 MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS SERUM PHOSPHORUS TESTING Policy Number: CMP - 035 Effective Date: January 21, 2017 Table
MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS SERUM PHOSPHORUS TESTING Policy Number: CMP - 035 Effective Date: January 21, 2017 Table
Clinical Manifestations. Principles of Nutrition Assessment. Significance of nutritional assessment. Nutrition Deficiency States.
 Clinical Manifestations Principles of Nutrition Assessment Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Impaired cellular immunity Impaired wound healing End organ dysfunction
Clinical Manifestations Principles of Nutrition Assessment Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Impaired cellular immunity Impaired wound healing End organ dysfunction
Case Study: Renal Disease
 Name: Melissa Hayes Case Study: Renal Disease Part I: Initial Presentation Chief Complaint: progressive anorexia with N/V, 5 kg weight gain in the past 10 days, edema, fatigue, worsening SOB with 2 pillow
Name: Melissa Hayes Case Study: Renal Disease Part I: Initial Presentation Chief Complaint: progressive anorexia with N/V, 5 kg weight gain in the past 10 days, edema, fatigue, worsening SOB with 2 pillow
Chapter 20 8/23/2016. Fluids and Electrolytes. Fluid (Water) Fluid (Water) (Cont.) Functions
 Fluid (Water) (Cont.) Functions") Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Nutrition Care Process: Case Study B Examples of Charting in Various Formats
 Nutrition Care Process: Case Study B Examples of Charting in Various Formats Case: JG is a 68 year old woman with a history of type 2 diabetes, chronic renal failure which is treated with hemodialysis
Nutrition Care Process: Case Study B Examples of Charting in Various Formats Case: JG is a 68 year old woman with a history of type 2 diabetes, chronic renal failure which is treated with hemodialysis
Refeeding syndrome: An overlooked condition?
 Focused Review Refeeding syndrome: An overlooked condition? Yuttiwat Vorakunthada MD, Passisd Laoveeravat MD, Wasawat Vutthikraivit MD, Weerapong Lilitwat MD, FAAP, Ariwan Rakvit MD, FACG Abstract Refeeding
Focused Review Refeeding syndrome: An overlooked condition? Yuttiwat Vorakunthada MD, Passisd Laoveeravat MD, Wasawat Vutthikraivit MD, Weerapong Lilitwat MD, FAAP, Ariwan Rakvit MD, FACG Abstract Refeeding
SAMPLE. Failure to Thrive. Chapter 2. Nutrition Assessment. Mary Sheehan, RD, LD. Sample Client History Terms Related to Failure to Thrive
 Chapter 2 Failure to Thrive Mary Sheehan, RD, LD This chapter provides examples of International Nutrition and Dietetics Terminology (IDNT) terms appropriate for pediatric patients with a medical diagnosis
Chapter 2 Failure to Thrive Mary Sheehan, RD, LD This chapter provides examples of International Nutrition and Dietetics Terminology (IDNT) terms appropriate for pediatric patients with a medical diagnosis
Being Over-Fat D. Social, Economic and Psychological Effects. Goal Setting and Keeping Score
 C hapter 1 Basic Physiology Being Over-Fat D id you know that excess body-fat can lead to a multitude of health problems? For one thing, excess body-fat can precipitate hypertension thus increasing the
C hapter 1 Basic Physiology Being Over-Fat D id you know that excess body-fat can lead to a multitude of health problems? For one thing, excess body-fat can precipitate hypertension thus increasing the
Nutritional Considerations in Patients with Parkinson s Disease
 Nutritional Considerations in Patients with Parkinson s Disease Steven Rudner, BS Nutrition & Dietetics Dietetic Intern, Sodexo Allentown www.dieteticintern.com www.sodexo.com Overview of PD Chronic progressive
Nutritional Considerations in Patients with Parkinson s Disease Steven Rudner, BS Nutrition & Dietetics Dietetic Intern, Sodexo Allentown www.dieteticintern.com www.sodexo.com Overview of PD Chronic progressive
Frequently Asked Questions on Zinc and Suggested Responses
 Last edited: September 27, 2012 Zinc Treatment of Childhood Diarrhea Frequently Asked Questions Diarrhoea still remains a leading cause of morbidity and mortality in developing countries. Every year more
Last edited: September 27, 2012 Zinc Treatment of Childhood Diarrhea Frequently Asked Questions Diarrhoea still remains a leading cause of morbidity and mortality in developing countries. Every year more
ESPEN LLL Programme in Clinical Nutrition and Metabolism. List of Topics and Modules 2014
 ESPEN LLL Programme in Clinical Nutrition and Metabolism List of Topics and Modules 204 Code Title Credits for Live course Credits for on-line course Credits for Grading Quiz Topic 0 Introduction in Nutrition
ESPEN LLL Programme in Clinical Nutrition and Metabolism List of Topics and Modules 204 Code Title Credits for Live course Credits for on-line course Credits for Grading Quiz Topic 0 Introduction in Nutrition
has the following disclosures to make:
 Importance of Weight in Treating a person with TB Catalina B. Navarro RN, BSN September 23, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Catalina
Importance of Weight in Treating a person with TB Catalina B. Navarro RN, BSN September 23, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Catalina
Commission of Dietetic Registration Board Certified Specialist in Renal Nutrition Certification Examination Content Outline
 I. Nutrition Assessment and Re-assessment (36%) A. Food/Nutrition-Related History 1. Evaluate current nutrition intake, losses, and nutrient adequacy. 2. Assess nutritional needs related to ethnic and
I. Nutrition Assessment and Re-assessment (36%) A. Food/Nutrition-Related History 1. Evaluate current nutrition intake, losses, and nutrient adequacy. 2. Assess nutritional needs related to ethnic and
Documentation ASSOCIATION OF NUTRITION AND FOOD PROFESSIONALS. Amber Gordon RD LD Consultant Dietitian, Carolina Nutrition Consultants
 Documentation ASSOCIATION OF NUTRITION AND FOOD PROFESSIONALS Amber Gordon RD LD Consultant Dietitian, Carolina Nutrition Consultants Objective Review nutrition documentation with focus on individualization
Documentation ASSOCIATION OF NUTRITION AND FOOD PROFESSIONALS Amber Gordon RD LD Consultant Dietitian, Carolina Nutrition Consultants Objective Review nutrition documentation with focus on individualization