Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ
|
|
|
- Sheila Quinn
- 5 years ago
- Views:
Transcription
1 Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ
2 Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage and prevent?
3 Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at high risk? How to manage and prevent?
4 Refeeding Syndrome
5 Metabolic and hormonal changes caused by over-rapid or unbalanced nutrition support in malnourished patients Whether enterally or parenterally Result in Micronutrient deficiencies Fluid and electrolyte imbalance Disturbances of organ function Death NICE 2006 Clinical guideline CG32 HM Mehanna BMJ 2008;336:1495-8
6 Incidence -?? Lack of a universally accepted definition Often not recognized HM Mehanna BMJ 2008;336:1495-8
7 Pathophysiology
8 Pathogenesis of Refeeding Syndrome Z Stanga EJCN ,
9 Starvation Pathogenesis of Refeeding Syndrome Z Stanga EJCN ,

10 Starvation Basal metabolic rate decreases 20-25% Body switches from using carbohydrate to protein in fasting state and fat in starvation state as the main source of energy Brain s switching from a glucose-based to a ketone-based fuel supply Intracellular minerals become depleted, while serum concentrations may remain normal HM Mehanna BMJ 2008;336: Modern Nutrition in Health and Disease 11 th edition
 Z Stanga EJCN 2008 62, 687")
11 Pathogenesis of Refeeding Syndrome Refeeding (switch to anabolism) Z Stanga EJCN ,
12 Refeeding (Major Energy => Carbohydrate) Increased Insulin 1. Stimulate glycogen, fat, and protein synthesis Requires minerals (phosphate and magnesium) and cofactors (thiamine) for phosphorylation and ATP synthesis Phosphate and magnesium are taken up into the cells 2. Stimulate potassium and glucose absorption into the cells through the sodium-potassium ATPase symporter Cause a decrease in serum phosphate, magnesium, and potassium Clinical features occur as a result of the functional deficits of these electrolytes and the rapid change in basal metabolic rate HM Mehanna BMJ 2008;336:1495-8
13 Clinical Features
14 Clinical Manifestations of Electrolyte Abnormalities Associated with Refeeding Syndrome Hypophosphatemia (PO 4 3- < 0.8 mmol/l) Cardiovascular - Cardiomyopathy - Heart failure - Arrhythmia Respiratory - Respiratory failure - Pulmonary edema Skeleton - Rhabdomyolysis - Weakness - Myalgia Hematology - Hemolysis - Leukocyte and platelet dysfunction Neurological - Delirium - Seizure L. U. R. Khan Gastroenterology research and practice 2011 Article ID , 6 pages
15 Clinical Manifestations of Electrolyte Abnormalities Associated with Refeeding Syndrome Hypokalemia (K + < 3.5 mmol/l) Cardiovascular - Ventricular arrhythmia - Brady/tachycardia - Cardiac arrest Respiratory - Hypoventilation - Respiratory failure Skeleton - Weakness/Fatigue - Muscle twitching Gastrointestinal - Ileus - Constipation Metabolic - Metabolic Alkalosis L. U. R. Khan Gastroenterology research and practice 2011 Article ID , 6 pages
16 Clinical Manifestations of Electrolyte Abnormalities Associated with Refeeding Syndrome Hypomagnesemia (Mg 2+ < 0.7 mmol/l) Cardiovascular - Arrhythmias - Heart failure Respiratory - Hypoventilation - Respiratory failure Skeleton - Muscle cramps - Weakness/Fatigue Neurological - Seizure - Paresthesia Gastrointestinal - Ileus - Constipation Metabolic - Hypocalcemia L. U. R. Khan Gastroenterology research and practice 2011 Article ID , 6 pages
17 1. Classical Re-Feeding Syndrome Acute circulatory fluid overload or depletion Pulmonary edema Cardiac failure / Arrhythmias Hyperglycemia Lactic acidosis 2. Wernicke-Korsakoff Syndrome Disorientation Opthalmoplegia / nystagmus Ataxia Short-term memory impairment Confabulation NICE 2006 Clinical guideline CG32
18 1. Classical Re-Feeding Syndrome Acute circulatory fluid overload or depletion Pulmonary edema Cardiac failure / Arrhythmias Hyperglycemia Lactic acidosis 2. Wernicke-Korsakoff Syndrome Disorientation Opthalmoplegia / nystagmus Ataxia Short-term memory impairment Confabulation Electrolyte Abnormalities Thiamine Deficiency NICE 2006 Clinical guideline CG32
19 What Electrolytes and Minerals are Involved in Pathogenesis of Refeeding Syndrome? Phosphorus - - Hallmark Magnesium Potassium Sodium
20 Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at high risk? How to manage and prevent?
21 Malnourished Patients at Particular Risk of Developing Refeeding Syndrome Z Stanga EJCN ,
22 Malnourished Patients at Particular Risk of Developing Refeeding Syndrome Z Stanga EJCN ,
23 Malnourished Patients at Particular Risk of Developing Refeeding Syndrome Z Stanga EJCN ,
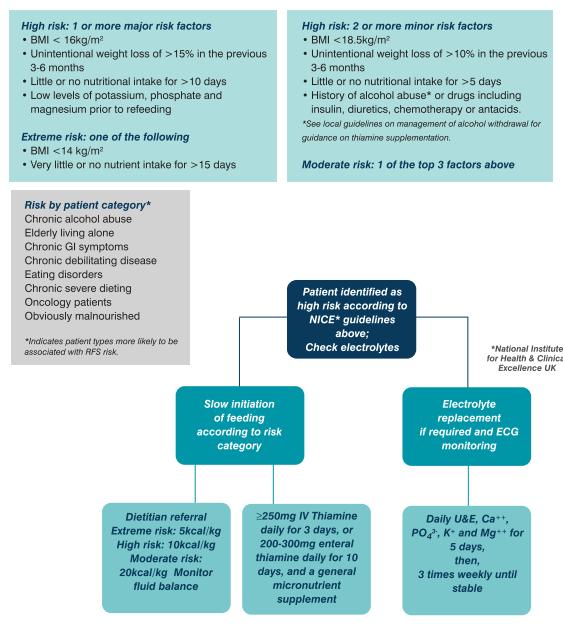
24 National Institute for Health and Care Excellence (NICE 2006) Criteria for Identifying Patient at High Risk of Refeeding Problems 1 criteria 2 criteria BMI (kg/m 2 ) < 16 < 18.5 Unintentional weight loss in previous 3-6 months (%) > 15 > 10 Little or no nutritional intake (days) > 10 > 5 Low level of serum electrolyte before feeding - Phosphate - Potassium - Magnesium Alcohol or drug uses - Insulin - Chemotherapy - Antacids - Diuretics
25 Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at high risk? How to manage and prevent?
26 Management There are no internationally validated guidelines for the treatment of the refeeding syndrome
")
27 National Institute for Clinical Excellence (NICE) 2006
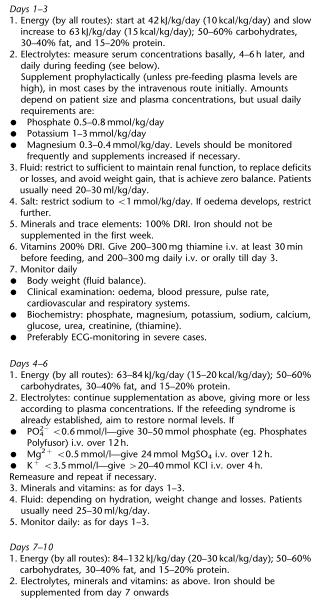
28 NICE 2006 Recommendation for Clinical Practice Patients at High Risk of Refeeding Syndrome Macronutrients - Calories Intake (All Routes) Start - 10 kcal/kg/d - 5 kcal/kg/d (if BMI < 14 kg/m 2 or no food intake > 15 d) Slowly Increase over 4-7 days to meet the full target Micronutrients Vitamins and Trace Elements Providing immediately before and during the first 10 days of oral thiamine mg daily Vitamin B co strong 1-2 tab, three times a day (or full dose daily intravenous vitamin B preparation) Multivitamin/trace element supplement once daily
29 NICE 2006 Recommendation for Clinical Practice Patients at High Risk of Refeeding Syndrome Electolytes Oral or intravenous supplementation of potassium, phosphate and magnesium unless pre-feeding plasma levels are high - Phosphate mmol/kg/d - Magnesium 0.2 mmol/kg/d (IV), 0.4 mmol/kg/d (oral) - Potassium 2-4 mmol/kg/d Pre-feeding correction of low plasma levels is unnecessary Fluid Carefully restoring circulatory volume Monitoring fluid balance and overall clinical status closely
30 Mehanna H Head & Neck Oncology 2009, 1:4 HM Mehanna BMJ 2008;336:1495-8
31
32 L. U. R. Khan Gastroenterology research and practice 2011 Article ID , 6 pages
33
34 ( mg/dl) (1-1.8 mg/dl) (< 1 mg/dl) HM Mehanna BMJ 2008;336:1495-8
35 Phosphorus Supplements (Parenteral) Inorganic Phosphate Dipotassium phosphate (K 2 HPO 4 ) PO mmol/ml K + 1 mmol/ml Organic Phosphate Fructose 1,6 phosphate (Esafosfina) PO mmol/ml Sodium Glycerophosphate (Glycophos) PO mmol/ml Na + 2 mmol/ml
 HM Mehanna BMJ")
36 (< 1.2 mg/dl) ( mg/dl) HM Mehanna BMJ 2008;336:1495-8
37 Serum Potassium (mmol/l) Critical deficit < 2.0 or < ECG changes Severe deficit no ECG changes Moderate deficit Mild deficit Recommendation for Replacement - Central IV KCL 10 meq/100ml NSS replace in intensive setting (max rate 20 meq/hr) - Peripheral IV 40 mmol/1l - Check serum K at 8 hr (if repeat 40 mmol/1l) - Peripheral IV 40 mmol/1l - Check serum K at 8 hr (if repeat 20 mmol/500ml) - Oral replacement - Peripheral IV 20 mmol IV/500 ml (if intolerance to oral) Cardiac monitoring if rate > 10 meq/hr Maximal rate : peripheral = 10 meq/hr, central = 20 meq/hr Maximal IV dose = 200 meq/24 hr Maximal concentration for peripheral vein = meq/l
38 Electrolyte/ Mineral Daily Parenteral Electrolyte and Mineral Requirements Preterm/ Neonates Infants/ Children Adults Sodium meq/kg/d 1-2 meq/kg/d Potassium meq/kg/d 1-2 meq/kg/d Calcium meq/kg/d meq/d Magnesium meq/kg/d 8-24 meq/d Phosphorus mmol/kg/d mmol/d Acetate Chloride As needed to maintain acid-base balance Note : Based on normal age-related organ function and normal losses Mirtallo J JPEN 2004;28(6):S39-S70 Manpreet S JPEN 2017;41:
39 Take Home Messages Aware of at risk individuals Appropriate feeding regimen Calories : slowly increase over a week Vitamins and trace elements : esp. thiamine Supplementation of the electrolytes : PO 4 3-, Mg 2+, K + Carefully restoring circulatory volume Monitoring during refeeding
Dutch consensus statement on Refeeding syndrome
 Dutch consensus statement on Refeeding syndrome Introduction Disease related malnutrition is a common problem in health care. The refeeding syndrome is defined as the severe and potentially fatal shifts
Dutch consensus statement on Refeeding syndrome Introduction Disease related malnutrition is a common problem in health care. The refeeding syndrome is defined as the severe and potentially fatal shifts
Refeeding syndrome a practical approach
 Refeeding syndrome a practical approach PENG pre-bapen Conference Teaching Day Birmingham Monday 20 th November 2017 Rhys White Acting Clinical and Operational Lead Dietitian Guys and St Thomas NHS Foundation
Refeeding syndrome a practical approach PENG pre-bapen Conference Teaching Day Birmingham Monday 20 th November 2017 Rhys White Acting Clinical and Operational Lead Dietitian Guys and St Thomas NHS Foundation
GUIDANCE NOTES. DIETETIC RISK ASSESSMENT FOR REFEEDING RECOMMENDED MEAL PLANS When commencing re-feeding: NICE (2006)
") When commencing re-feeding: NICE (2006) NICE (2006) Clinical Guideline 32 Nutrition support in adults: oral nutrition support, enteral tube feeding and parenteral nutrition (The following is based on www.nice.org.uk/cg032
When commencing re-feeding: NICE (2006) NICE (2006) Clinical Guideline 32 Nutrition support in adults: oral nutrition support, enteral tube feeding and parenteral nutrition (The following is based on www.nice.org.uk/cg032
MANAGEMENT AND PREVENTION OF REFEEDING SYNDROME IN INPATIENTS: A PRACTICAL APPROACH
 MANAGEMENT AND PREVENTION OF REFEEDING SYNDROME IN INPATIENTS: A PRACTICAL APPROACH Prof. Zeno Stanga, MD Nutritional Medicine Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism
MANAGEMENT AND PREVENTION OF REFEEDING SYNDROME IN INPATIENTS: A PRACTICAL APPROACH Prof. Zeno Stanga, MD Nutritional Medicine Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism
Refeeding syndrome: An overlooked condition?
 Focused Review Refeeding syndrome: An overlooked condition? Yuttiwat Vorakunthada MD, Passisd Laoveeravat MD, Wasawat Vutthikraivit MD, Weerapong Lilitwat MD, FAAP, Ariwan Rakvit MD, FACG Abstract Refeeding
Focused Review Refeeding syndrome: An overlooked condition? Yuttiwat Vorakunthada MD, Passisd Laoveeravat MD, Wasawat Vutthikraivit MD, Weerapong Lilitwat MD, FAAP, Ariwan Rakvit MD, FACG Abstract Refeeding
Acute management of severe malnutrition. Dr Simon Gabe St Mark s Hospital, London
 Acute management of severe malnutrition Dr Simon Gabe St Mark s Hospital, London Malnutrition definition A state resulting from lack of uptake or intake of nutrition leading to altered body composition
Acute management of severe malnutrition Dr Simon Gabe St Mark s Hospital, London Malnutrition definition A state resulting from lack of uptake or intake of nutrition leading to altered body composition
Formulary and Prescribing Guidelines
 Formulary and Prescribing Guidelines SECTION 15: TREATMENT OF EATING DISORDERS 15.1 Introduction Please review the Trust document Guidelines for the assessment and treatment of eating disorders in the
Formulary and Prescribing Guidelines SECTION 15: TREATMENT OF EATING DISORDERS 15.1 Introduction Please review the Trust document Guidelines for the assessment and treatment of eating disorders in the
Refeeding Syndrome Guideline
 Refeeding Syndrome Guideline Author: Responsible Lead Executive Director: Endorsing Body: Governance or Assurance Committee Pamela Miller Biochemistry Implementation Date: January 2017 Version Number:
Refeeding Syndrome Guideline Author: Responsible Lead Executive Director: Endorsing Body: Governance or Assurance Committee Pamela Miller Biochemistry Implementation Date: January 2017 Version Number:
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Case Study: Nutritional management of a patient at high risk of developing refeeding syndrome
 Case Study: Nutritional management of a patient at high risk of developing refeeding syndrome Dolman RC, PhD, Senior Lecturer; Conradie C, MSc, Lecturer Lombard MJ, PhD, Senior Lecturer; Nienaber A, MSc,
Case Study: Nutritional management of a patient at high risk of developing refeeding syndrome Dolman RC, PhD, Senior Lecturer; Conradie C, MSc, Lecturer Lombard MJ, PhD, Senior Lecturer; Nienaber A, MSc,
ISPUB.COM. Electrolyte Replacement: A Review. B Phillips INTRODUCTION ELECTROLYTES I. CALCIUM
 ISPUB.COM The Internet Journal of Internal Medicine Volume 5 Number 1 Electrolyte Replacement: A Review B Phillips Citation B Phillips. Electrolyte Replacement: A Review. The Internet Journal of Internal
ISPUB.COM The Internet Journal of Internal Medicine Volume 5 Number 1 Electrolyte Replacement: A Review B Phillips Citation B Phillips. Electrolyte Replacement: A Review. The Internet Journal of Internal
Does the patient need an enteral feed out of hours?
 Out of hours Enteral tube feeding (Nasogastric) Starter Regimen for an Adult Inpatient With Renal Failure (Including management of re-feeding syndrome) Guidance for Practice 1. Introduction 1.1 This clinical
Out of hours Enteral tube feeding (Nasogastric) Starter Regimen for an Adult Inpatient With Renal Failure (Including management of re-feeding syndrome) Guidance for Practice 1. Introduction 1.1 This clinical
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter
 Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
SERUM PHOSPHORUS TESTING
 MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS SERUM PHOSPHORUS TESTING Policy Number: CMP - 035 Effective Date: January 21, 2017 Table
MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS SERUM PHOSPHORUS TESTING Policy Number: CMP - 035 Effective Date: January 21, 2017 Table
Adaptation and re-feeding Hypokalemia Bone complications
 Adaptation and re-feeding Hypokalemia Bone complications René Klinkby Støving Odense University Hospital Denmark 10% 20% 30% 40% BMI 18.5 BMI 16.5 BMI 14.5 BMI 12.5 Willmore DW, The Metabolic Management
Adaptation and re-feeding Hypokalemia Bone complications René Klinkby Støving Odense University Hospital Denmark 10% 20% 30% 40% BMI 18.5 BMI 16.5 BMI 14.5 BMI 12.5 Willmore DW, The Metabolic Management
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Financial Interest Disclosure (over the past 24 months)
") : Across the Spectrum of Primary care Jan Greenwood, R.D. Nutrition Support Consultant The Basic Five Programs The opinions expressed in this presentation are that of the presenter and do not necessarily
: Across the Spectrum of Primary care Jan Greenwood, R.D. Nutrition Support Consultant The Basic Five Programs The opinions expressed in this presentation are that of the presenter and do not necessarily
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Alterations in Fluids and Electrolytes During Refeeding Syndrome. Objectives. Refeeding Syndrome (RS) 4/26/2013. Barbara Magnuson, PharmD, BCNSP
 4/26/2013. Barbara Magnuson, PharmD, BCNSP") Alterations in Fluids and Electrolytes During Refeeding Syndrome Barbara Magnuson, PharmD, BCNSP Objectives Define refeeding syndrome including its signs and symptoms Identify fluid and electrolyte disturbances
Alterations in Fluids and Electrolytes During Refeeding Syndrome Barbara Magnuson, PharmD, BCNSP Objectives Define refeeding syndrome including its signs and symptoms Identify fluid and electrolyte disturbances
THE PATHOPHYSIOLOGY OF THE REFEEDING SYNDROME
 THE PATHOPHYSIOLOGY OF THE REFEEDING SYNDROME Zeno Stanga, MD Division of Endocrinology, Diabetes and Clinical Nutrition Division of General Internal Medicine Minnesota Experiment Aim To guide the Allied
THE PATHOPHYSIOLOGY OF THE REFEEDING SYNDROME Zeno Stanga, MD Division of Endocrinology, Diabetes and Clinical Nutrition Division of General Internal Medicine Minnesota Experiment Aim To guide the Allied
, 吳文傑. Refeeding syndrome (RFS) is a well described but often forgotten condition,
 is a well described but often forgotten condition,") 中文題目 : 再餵食症候群 - 病例報告 英文題目 : Refeeding syndrome in a patient with suspected MEN-I syndrome: a case report 作者 : 楊光祖 1, 沈曉津 2, 廖麗瑛 3 3*, 吳文傑 1 服務單位 : 臺北市立聯合醫院仁愛院區內科部臺北市立聯合醫院仁愛院區教學 2 研究部臺北市立聯合醫院仁愛院區消化內科 Introduction
中文題目 : 再餵食症候群 - 病例報告 英文題目 : Refeeding syndrome in a patient with suspected MEN-I syndrome: a case report 作者 : 楊光祖 1, 沈曉津 2, 廖麗瑛 3 3*, 吳文傑 1 服務單位 : 臺北市立聯合醫院仁愛院區內科部臺北市立聯合醫院仁愛院區教學 2 研究部臺北市立聯合醫院仁愛院區消化內科 Introduction
Acid-Base Balance 11/18/2011. Regulation of Potassium Balance. Regulation of Potassium Balance. Regulatory Site: Cortical Collecting Ducts.
 Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
9/11/2012. Chapter 11. Learning Objectives. Learning Objectives. Endocrine Emergencies. Differentiate type 1 and type 2 diabetes
 Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
PARENTERAL NUTRITION
 PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
Refeeding Low Weight Adolescents with AN
 RCPsych ED 2013 Refeeding Low Weight Adolescents with AN Graeme O Connor RD PhD Research Student -UCL Specialist paediatric Dietitian Great Ormond Street Hospital Foundation Trust Pathophysiology of starvation
RCPsych ED 2013 Refeeding Low Weight Adolescents with AN Graeme O Connor RD PhD Research Student -UCL Specialist paediatric Dietitian Great Ormond Street Hospital Foundation Trust Pathophysiology of starvation
NHS Grampian Staff Guideline For The Management Of Acute Hypophosphataemia In Adults
 NHS Grampian Staff Guideline For The Management Of Acute Hypophosphataemia In Adults Co-ordinators: Medicine Information Pharmacist Consultation Group: See Page 5 Approver: Medicine Guidelines and Policies
NHS Grampian Staff Guideline For The Management Of Acute Hypophosphataemia In Adults Co-ordinators: Medicine Information Pharmacist Consultation Group: See Page 5 Approver: Medicine Guidelines and Policies
Class 3: Refeeding Syndrome. Liz Hudson MPH, RD
 Class 3: Refeeding Syndrome Liz Hudson MPH, RD Case Study #1 NUTRITION ASSESSMENT: Consult PATIENT MEDICAL/HEALTH HISTORY: 49 y/o male with significant history of HTN, DM, and stage V CKD currently on
Class 3: Refeeding Syndrome Liz Hudson MPH, RD Case Study #1 NUTRITION ASSESSMENT: Consult PATIENT MEDICAL/HEALTH HISTORY: 49 y/o male with significant history of HTN, DM, and stage V CKD currently on
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Nutritional intervention in hospitalised paediatric patients. Dr Y.K.Amdekar
 Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Hypophosphatemia is an uncommon condition
 HYPOPHOSPHATEMIA AND REFEEDING SYNDROME Nathan Lippo, DVM Resident, Emergency and Critical Care Medicine Christopher G. Byers, DVM, DACVECC Director, Intensive Care Internal Medicine Critical Care Department
HYPOPHOSPHATEMIA AND REFEEDING SYNDROME Nathan Lippo, DVM Resident, Emergency and Critical Care Medicine Christopher G. Byers, DVM, DACVECC Director, Intensive Care Internal Medicine Critical Care Department
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology
 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
Salicylate (Aspirin) Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes
 Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes") Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
Electrolytes Solution
 Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetate, in pediatric surgical patients, 525 526 Acute respiratory distress syndrome (ARDS), immune-modulating nutrition in, 584 585 Aerobic
Index Note: Page numbers of article titles are in boldface type. A Acetate, in pediatric surgical patients, 525 526 Acute respiratory distress syndrome (ARDS), immune-modulating nutrition in, 584 585 Aerobic
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Intensive Care Nutrition. Dr Alan Race BSc(Hons) PhD FRCA
 PhD FRCA") Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Parenteral Nutrition in Oncology
 Parenteral Nutrition in Oncology Presenter: Pam Wagner, RD, CNSC Learning Objectives List indications for initiating PN in oncology patients Describe considerations when determining an appropriate candidate
Parenteral Nutrition in Oncology Presenter: Pam Wagner, RD, CNSC Learning Objectives List indications for initiating PN in oncology patients Describe considerations when determining an appropriate candidate
NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults
 NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults Co-ordinators: Medicines Information Pharmacist Consultation Group: See relevant page in guidance Approver: Medicine Guidelines
NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults Co-ordinators: Medicines Information Pharmacist Consultation Group: See relevant page in guidance Approver: Medicine Guidelines
TOTAL PARENTERAL NUTRITION
 TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion , version 1.1
 Nutriflex Omega peri emulsion for infusion , version 1.1") EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion 13.7.2015, version 1.1 III.1. Elements for a Public Summary III.1.1. Overview of disease epidemiology Patients may need parenteral
EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion 13.7.2015, version 1.1 III.1. Elements for a Public Summary III.1.1. Overview of disease epidemiology Patients may need parenteral
Phosphoremia (mmol/l) Calcemia (mmol/l) Postnatal age (days) Postnatal age (days) Urinary Calcium (mg/kg/d) Phosphoremia (mmol/l)
 Calcemia (mmol/l) Postnatal age (days) Postnatal age (days) Urinary Calcium (mg/kg/d) Phosphoremia (mmol/l)") 3,0 3,2 Calcemia (mmol/l) 2,8 2,6 2,4 2,2 2,0 1,8 Phosphoremia (mmol/l) 3,0 2,8 2,6 2,4 2,2 2,0 1,8 1,6 1,4 1,2 1,6 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Postnatal age (days) 1,0 0 1 2 3 4 5 6 7 8 9 10 11
3,0 3,2 Calcemia (mmol/l) 2,8 2,6 2,4 2,2 2,0 1,8 Phosphoremia (mmol/l) 3,0 2,8 2,6 2,4 2,2 2,0 1,8 1,6 1,4 1,2 1,6 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Postnatal age (days) 1,0 0 1 2 3 4 5 6 7 8 9 10 11
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Accepted Article. Celiac crisis in adults: a case report and review of the literature focusing in the prevention of refeeding syndrome
 Accepted Article Celiac crisis in adults: a case report and review of the literature focusing in the prevention of refeeding syndrome Marcela de Almeida Menezes, Vírginia Cabral, Sônia Letícia Silva Lorena
Accepted Article Celiac crisis in adults: a case report and review of the literature focusing in the prevention of refeeding syndrome Marcela de Almeida Menezes, Vírginia Cabral, Sônia Letícia Silva Lorena
Start. What is the serum phosphate concentration? Moderate Hypophosphataemia mmol/l. Replace using oral. phosphate. (See section 3.
 CLINICAL GUIDELINE FOR THE MANAGEMENT OF HYPOPHOSPHATAEMIA IN ADULTS Summary. Key: General Notes GP/SWASFT ED/MAU/SRU/Acute GP/Amb-Care In-patient wards Start What is the serum concentration? Mild Hypophosphataemia
CLINICAL GUIDELINE FOR THE MANAGEMENT OF HYPOPHOSPHATAEMIA IN ADULTS Summary. Key: General Notes GP/SWASFT ED/MAU/SRU/Acute GP/Amb-Care In-patient wards Start What is the serum concentration? Mild Hypophosphataemia
PRODUCT INFORMATION RESONIUM A. Na m
 PRODUCT INFORMATION RESONIUM A NAME OF THE MEDICINE Non-proprietary Name Sodium polystyrene sulfonate Chemical Structure CH - 2 CH SO 3 Na + n CAS Number 28210-41-5 [9003-59-2] CH 2 CH SO - 3 m DESCRIPTION
PRODUCT INFORMATION RESONIUM A NAME OF THE MEDICINE Non-proprietary Name Sodium polystyrene sulfonate Chemical Structure CH - 2 CH SO 3 Na + n CAS Number 28210-41-5 [9003-59-2] CH 2 CH SO - 3 m DESCRIPTION
ESPEN Congress Vienna Neglected deficiencies in severe malnutrition: Commentary - Thiamine. E. Doberer (Austria)
") ESPEN Congress Vienna 2009 Neglected deficiencies in severe malnutrition: Commentary - Thiamine E. Doberer (Austria) Neglected deficiencies in severe malnutrition: Commentary - Thiamine Edith Doberer Department
ESPEN Congress Vienna 2009 Neglected deficiencies in severe malnutrition: Commentary - Thiamine E. Doberer (Austria) Neglected deficiencies in severe malnutrition: Commentary - Thiamine Edith Doberer Department
6-7 JULY 2015, BIRMINGHAM CONGRESS
 6-7 JULY 2015, BIRMINGHAM CONGRESS Keywords: /Malnutrition/ Enteral feeding/critical illness This article has been double-blind peer reviewed Patients who are critically ill are at greater risk of malnutrition
6-7 JULY 2015, BIRMINGHAM CONGRESS Keywords: /Malnutrition/ Enteral feeding/critical illness This article has been double-blind peer reviewed Patients who are critically ill are at greater risk of malnutrition
FLUIDS AND ELECTROLYTES
 FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN *
 For the use of a registered medical practitioner or a Hospital or a Laboratory only Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN * DESCRIPTION: NIRMIN * is a clear, colourless injection
For the use of a registered medical practitioner or a Hospital or a Laboratory only Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN * DESCRIPTION: NIRMIN * is a clear, colourless injection
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
ACUTE & CHRONIC ETHANOL EFFECTS An Overview
 ACUTE & CHRONIC ETHANOL EFFECTS An Overview University of Papua New Guinea School of Medicine & Health Sciences, Division of Basic Medical Sciences Clinical Biochemistry: PBL Seminar MBBS Yr 4 VJ Temple
ACUTE & CHRONIC ETHANOL EFFECTS An Overview University of Papua New Guinea School of Medicine & Health Sciences, Division of Basic Medical Sciences Clinical Biochemistry: PBL Seminar MBBS Yr 4 VJ Temple
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION
 ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
Potassium Chloride in 5% Dextrose Injection, USP In VIAFLEX Plastic Container
 PRESCRIBING INFORMATION Potassium Chloride in 5% Dextrose Injection, USP In VIAFLEX Plastic Container IV Fluid and Nutrient Replenisher Baxter Corporation Mississauga, Ontario L5N 0C2 Canada Date of Revision:
PRESCRIBING INFORMATION Potassium Chloride in 5% Dextrose Injection, USP In VIAFLEX Plastic Container IV Fluid and Nutrient Replenisher Baxter Corporation Mississauga, Ontario L5N 0C2 Canada Date of Revision:
Ensuring Safe Management of Parenteral Nutrition During Drug Shortages: Strategies and Protocols for Enabling Clinician Success
 Ensuring Safe Management of Parenteral Nutrition During Drug Shortages: Strategies and Protocols for Enabling Clinician Success Mandy Corrigan, MPH, RD, CNSC Nutrition Support Clinician mandycorrigan1@gmail.com
Ensuring Safe Management of Parenteral Nutrition During Drug Shortages: Strategies and Protocols for Enabling Clinician Success Mandy Corrigan, MPH, RD, CNSC Nutrition Support Clinician mandycorrigan1@gmail.com
Refeeding Syndrome: An Important Complication Following Obesity Surgery
 Received: July 27, 2015 Accepted: October 28, 2015 Published online: January 9, 2016 2016 The Author(s) Published by S. Karger GmbH, Freiburg 1662 4033/15/0091 0012$39.50/0 This article is licensed under
Received: July 27, 2015 Accepted: October 28, 2015 Published online: January 9, 2016 2016 The Author(s) Published by S. Karger GmbH, Freiburg 1662 4033/15/0091 0012$39.50/0 This article is licensed under
Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + )
") Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration in body fluids Precise regulation of ph at
Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration in body fluids Precise regulation of ph at
Introduction to Clinical Nutrition
 M-III Introduction to Clinical Nutrition Donald F. Kirby, MD Chief, Section of Nutrition Division of Gastroenterology 1 Things We Take for Granted Air to Breathe Death Taxes Another Admission Our Next
M-III Introduction to Clinical Nutrition Donald F. Kirby, MD Chief, Section of Nutrition Division of Gastroenterology 1 Things We Take for Granted Air to Breathe Death Taxes Another Admission Our Next
Refeeding Syndrom: Ein Update. Prof. Philipp Schuetz, Leitender Arzt Medizinische Uniklinik, Kantonsspital Aarau GESKES Kurs Aarau, April 14 th 2016
 Refeeding Syndrom: Ein Update Prof. Philipp Schuetz, Leitender Arzt Medizinische Uniklinik, Kantonsspital Aarau GESKES Kurs Aarau, April 14 th 2016 Email: Schuetzph@gmail.com Historical perspective First
Refeeding Syndrom: Ein Update Prof. Philipp Schuetz, Leitender Arzt Medizinische Uniklinik, Kantonsspital Aarau GESKES Kurs Aarau, April 14 th 2016 Email: Schuetzph@gmail.com Historical perspective First
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Drug Shortages with Parenteral Nutrition
 Drug Shortages with Parenteral Nutrition Carol J Rollins, MS, RD, PharmD, BCNSP Coordinator, Nutrition Support Team The University of Arizona Medical Center www.nutritioncare.org Conflict of Interest None
Drug Shortages with Parenteral Nutrition Carol J Rollins, MS, RD, PharmD, BCNSP Coordinator, Nutrition Support Team The University of Arizona Medical Center www.nutritioncare.org Conflict of Interest None
Chapter 20 8/23/2016. Fluids and Electrolytes. Fluid (Water) Fluid (Water) (Cont.) Functions
 Fluid (Water) (Cont.) Functions") Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
H 2 O, Electrolytes and Acid-Base Balance
 H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
Guideline scope Neonatal parenteral nutrition
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Neonatal parenteral nutrition The Department of Health in England has asked NICE to develop a new guideline on parenteral nutrition in
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Neonatal parenteral nutrition The Department of Health in England has asked NICE to develop a new guideline on parenteral nutrition in
Volume and Electrolytes. Fluid and Electrolyte Management. Why 125ml? Question. Normal fluid requirement. Normal losses
 Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Acid Base Balance. Professor Dr. Raid M. H. Al-Salih. Clinical Chemistry Professor Dr. Raid M. H. Al-Salih
 Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Acid-Base Balance Dr. Gary Mumaugh
 Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
The Role of Parenteral Nutrition. in PEDIATRIC INTENSIVE CARE UNIT. Dzulfikar DLH. Pediatric Emergency and Intensive Care Unit
 The Role of Parenteral Nutrition in PEDIATRIC INTENSIVE CARE UNIT Dzulfikar DLH Pediatric Emergency and Intensive Care Unit Department of Child Health, Faculty of Medicine Universitas Padjajaran, Hasan
The Role of Parenteral Nutrition in PEDIATRIC INTENSIVE CARE UNIT Dzulfikar DLH Pediatric Emergency and Intensive Care Unit Department of Child Health, Faculty of Medicine Universitas Padjajaran, Hasan
PAEDIATRIC PARENTERAL NUTRITION. Ezatul Mazuin Ayla binti Mamdooh Waffa Hospital Sultanah Aminah
 PAEDIATRIC PARENTERAL NUTRITION Ezatul Mazuin Ayla binti Mamdooh Waffa Hospital Sultanah Aminah Johor Bahru Malnutrition INTRODUCTION pathologic state of varying severity with clinical features caused
PAEDIATRIC PARENTERAL NUTRITION Ezatul Mazuin Ayla binti Mamdooh Waffa Hospital Sultanah Aminah Johor Bahru Malnutrition INTRODUCTION pathologic state of varying severity with clinical features caused
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 27 Fluid, Electrolyte, and Acid Base Fluid Compartments and Fluid In adults, body fluids make up between 55% and 65% of total body mass. Body
Principles of Anatomy and Physiology 14 th Edition CHAPTER 27 Fluid, Electrolyte, and Acid Base Fluid Compartments and Fluid In adults, body fluids make up between 55% and 65% of total body mass. Body
Nutrition. Chapter 45. Reada Almashagba
 Nutrition Chapter 45 1 Nutrition: - Nutrient are organic substances found in food and are required for body function - No one food provide all essential nutrient Major function of nutrition: providing
Nutrition Chapter 45 1 Nutrition: - Nutrient are organic substances found in food and are required for body function - No one food provide all essential nutrient Major function of nutrition: providing
ADMIT DIABETIC KETOACIDOSIS (DKA) PLAN - Phase: Begin Immediately/Emergency Center
 PLAN - Phase: Begin Immediately/Emergency Center") - Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
- Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
HOMES AND SENIORS SERVICES. APPROVAL DATE: February 2011 REVISION DATE: January 2015; July 2018
 POLICY: Page 1 of 6 A resident requiring enteral (tube) feeding as a sole source or adjunctive nutrition support have access to a comprehensive enteral feeding program and receive appropriate support from
POLICY: Page 1 of 6 A resident requiring enteral (tube) feeding as a sole source or adjunctive nutrition support have access to a comprehensive enteral feeding program and receive appropriate support from
NHS Grampian Staff Guidance For The Management Of Hypomagnesaemia In Adults. Consultation Group: See Page 4. Review Date: June 2021
 NHS...... Grampian NHS Grampian Staff Guidance For The Management Of Hypomagnesaemia In Adults Co-ordinators: Consultation Group: Approver:. Senior Medicines Information Pharmacist See Page 4 Medicine
NHS...... Grampian NHS Grampian Staff Guidance For The Management Of Hypomagnesaemia In Adults Co-ordinators: Consultation Group: Approver:. Senior Medicines Information Pharmacist See Page 4 Medicine
Who Needs Parenteral Nutrition? Is Parenteral Nutrition An Appropriate Intervention?
 Who Needs Parenteral Nutrition? 1 Is Parenteral Nutrition An Appropriate Intervention? Key questions to ask with initial consultation Can the gastrointestinal (GI) tract be utilized? Can the GI tract be
Who Needs Parenteral Nutrition? 1 Is Parenteral Nutrition An Appropriate Intervention? Key questions to ask with initial consultation Can the gastrointestinal (GI) tract be utilized? Can the GI tract be
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Module 8: Practice Problems
 Module 8: Practice Problems 1. Convert a blood plasma level range of 5 to 20 µg/ml of tobramycin (Z = 467.52) to µmol/l. 5 µg/ml = 10.7 µmol/l 20 µg/ml = 42.8 µmol/l 2. A preparation contains in each milliliter,
Module 8: Practice Problems 1. Convert a blood plasma level range of 5 to 20 µg/ml of tobramycin (Z = 467.52) to µmol/l. 5 µg/ml = 10.7 µmol/l 20 µg/ml = 42.8 µmol/l 2. A preparation contains in each milliliter,
Entry Level Clinical Nutrition. Dr. Jeff Moss. Dr. Jeff Moss
 Entry Level Clinical Nutrition Part XII Micronutrient imbalances: Water soluble vitamins Jeffrey Moss, DDS, CNS, DACBN jeffmoss@mossnutrition.com 413-530-08580858 (cell) 1 Quality of life issues are the
Entry Level Clinical Nutrition Part XII Micronutrient imbalances: Water soluble vitamins Jeffrey Moss, DDS, CNS, DACBN jeffmoss@mossnutrition.com 413-530-08580858 (cell) 1 Quality of life issues are the
TOTUM SPORT: THE SCIENCE BEHIND THE PERFORMANCE
 TOTUM SPORT: THE SCIENCE BEHIND THE PERFORMANCE Hydration is one of the most important aspects for maximising performance, supporting all other factors of speed, strength, stamina, concentration, immunity
TOTUM SPORT: THE SCIENCE BEHIND THE PERFORMANCE Hydration is one of the most important aspects for maximising performance, supporting all other factors of speed, strength, stamina, concentration, immunity
ESPEN LLL Programme in Clinical Nutrition and Metabolism. List of Topics and Modules 2014
 ESPEN LLL Programme in Clinical Nutrition and Metabolism List of Topics and Modules 204 Code Title Credits for Live course Credits for on-line course Credits for Grading Quiz Topic 0 Introduction in Nutrition
ESPEN LLL Programme in Clinical Nutrition and Metabolism List of Topics and Modules 204 Code Title Credits for Live course Credits for on-line course Credits for Grading Quiz Topic 0 Introduction in Nutrition
TKIs ( Tyrosine Kinase Inhibitors ) Mechanism of action and toxicity in CML Patients. Moustafa Sameer Hematology Medical Advsior,Novartis oncology
 Mechanism of action and toxicity in CML Patients. Moustafa Sameer Hematology Medical Advsior,Novartis oncology") TKIs ( Tyrosine Kinase Inhibitors ) Mechanism of action and toxicity in CML Patients Moustafa Sameer Hematology Medical Advsior,Novartis oncology Introduction In people with chronic myeloid leukemia, A
TKIs ( Tyrosine Kinase Inhibitors ) Mechanism of action and toxicity in CML Patients Moustafa Sameer Hematology Medical Advsior,Novartis oncology Introduction In people with chronic myeloid leukemia, A
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09. Terminal Learning Objective. References. Hours: 2.0 Last updated: November 2015
 SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
Acid Base Balance by: Susan Mberenga RN, BSN, MSN
 Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
A Guide to Prescribing Adult Oral Nutritional Supplements in West Kent CCG
 A Guide to Prescribing Adult Oral Nutritional Supplements in West Kent CCG Aim This guideline has been designed to support primary care prescribers initiating nutrition support for adults in West Kent.
A Guide to Prescribing Adult Oral Nutritional Supplements in West Kent CCG Aim This guideline has been designed to support primary care prescribers initiating nutrition support for adults in West Kent.
DONATION AFTER CARDIAC DEATH PLAN
 DONATION AFTER CARDIAC DEATH PLAN Diagnosis Weight Allergies Patient Care Core Body Temperature Monitoring Maintain body temp 96-99 degrees Farenheit. Utilize Hyper/Hypothermia blanket prn Insert Gastric
DONATION AFTER CARDIAC DEATH PLAN Diagnosis Weight Allergies Patient Care Core Body Temperature Monitoring Maintain body temp 96-99 degrees Farenheit. Utilize Hyper/Hypothermia blanket prn Insert Gastric
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Nutritional Interventions in Primary Mitochondrial Disorders
 Nutritional Interventions in Primary Mitochondrial Disorders Carolyn J Ellaway MBBS PhD FRACP CGHGSA Genetic Metabolic Disorders Service Sydney Children s Hospital Network Disciplines of Child and Adolescent
Nutritional Interventions in Primary Mitochondrial Disorders Carolyn J Ellaway MBBS PhD FRACP CGHGSA Genetic Metabolic Disorders Service Sydney Children s Hospital Network Disciplines of Child and Adolescent
Normosol -R and 5% Dextrose Injection MULTIPLE ELECTROLYTES AND 5% DEXTROSE INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid
 Normosol -R and 5% Dextrose Injection MULTIPLE ELECTROLYTES AND 5% DEXTROSE INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid R x only Flexible Plastic Container DESCRIPTION Normosol-R
Normosol -R and 5% Dextrose Injection MULTIPLE ELECTROLYTES AND 5% DEXTROSE INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid R x only Flexible Plastic Container DESCRIPTION Normosol-R
Parenteral and Enteral Nutrition
 Parenteral and Enteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Parenteral Nutrition Definition process of supplying nutrients via the intravenous route
Parenteral and Enteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Parenteral Nutrition Definition process of supplying nutrients via the intravenous route
CLINICAL GUIDELINES ID TAG
 CLINICAL GUIDELINES ID TAG Title: Treatment of Hypomagnesaemia in adults Author: Speciality / Division: Directorate: Dr Peter Sharpe, Dr Neal Morgan, Jillian Redpath Chemical Pathology/Nephrology/Pharmacy
CLINICAL GUIDELINES ID TAG Title: Treatment of Hypomagnesaemia in adults Author: Speciality / Division: Directorate: Dr Peter Sharpe, Dr Neal Morgan, Jillian Redpath Chemical Pathology/Nephrology/Pharmacy
ELECTROLYTE DISTURBANCES AND ABNORMAL URINE ANALYSIS IN CHILDREN WITH DENGUE INFECTION
 ELECTROLYTE DISTURBANCES AND ABNORMAL URINE ANALYSIS IN CHILDREN WITH DENGUE INFECTION Adisorn Lumpaopong 1, Pinyada Kaewplang 1, Veerachai Watanaveeradej 2, Prapaipim Thirakhupt 1, Sangkae Chamnanvanakij
ELECTROLYTE DISTURBANCES AND ABNORMAL URINE ANALYSIS IN CHILDREN WITH DENGUE INFECTION Adisorn Lumpaopong 1, Pinyada Kaewplang 1, Veerachai Watanaveeradej 2, Prapaipim Thirakhupt 1, Sangkae Chamnanvanakij