2012, Görlinger Klaus
|
|
|
- Jane Nicholson
- 6 years ago
- Views:
Transcription


1 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net

2 CSL Behring GmbH Octapharma AG Tem International GmbH Conflicts of interest Verum Diagnostica GmbH Instrumentation Laboratory

3 Transfusion strategies Formula driven: 1:1:1-concept Lab-driven Individualized POC-driven
4 Results:... Patients arrived in the ICU 6.8 ± 0.3 hours after admission. Coagulopathy, present at hospital admission (pre-icu INR, 1.8 ± 0.2) persisted at ICU admission (initial ICU INR, 1.6 ± 0.1).... In the ICU during resuscitation mean INR decreased to 1.4 ± 0.03 within 8 hours, indicating moderate coagulopathy.... The ratio of FFP:PRBC was 1:1.... Statistical analysis found severity of coagulopathy (INR) at ICU admission associated with survival outcome (p = 0.02). 1: hours to achieve an INR < 1.5!
5 Conclusion:... More aggressive pre-icu intervention to correct coagulopathy may be effective in decreasing RPBC requirement during ICU resuscitation, and, because of the association with increased mortality, could improve outcome.... We think that treatment of coagulopathy can be improved with the development of standardized protocols, both empiric and data driven.!!
6
7 Exposure to ABO-compatible plasma results in an increase in overall complications (53.5% vs 40.5%, P =.002), in particular ARDS (19.4% vs 9.2%, P =.0011) and sepsis (38.0% vs 28.9%, P =.02). There is a stepwise increase in the complication rate as exposure increases (reaching 70.0% for patients receiving more than 6 U; these patients also had a 4-fold increase in ARDS).
8 86082 Swedish patients receiving their first plasma transfusion (follow up of 14 days) Transfusion of 5 or more units of AB0-compatible but non-identical plasma was associated with an increased mortality by 15% compared to recipients of only AB0-identical plasma
9
10


11
12 Results: A high ratio of FFP:RBC in the 15 TASH group was independently associated with survival, with an odds-ratio of 2.5 ( ), while the <15TASHgroupwas associated with increased multi-organ failure, 47% vs. 38%, (P < 0.005).

13 DO YOU HAVE THE BLEEDING UNDER CONTROL??? Will this patient bleed?
14 ROTEM analysis enables rapid detection of most coagulation disorders; this study demonstrates the additional benefit of MT risk stratification using results available within 10 minutes after CT.
15
16
17
18
19
20


21 Why does the patient bleed?
22
23 Pyramid of therapy in coagulopathy rfviia FVIII / FXIII Platelets PCC (or FFP) Fibrinogen (or Cryo) Hyperfibrinolysis? Aspirin? Oral anticoagulants? Heparin? Basic conditions (T C > 34ºC; ph > 7,2; Ca i > 1 mmol/l; Hb > 8 g/l) Surgical stanching (Compression bandage; MAST; pelvic compression; packing)
: 942-50.")

24 Trauma Algorithm Waydhas C, Görlinger K. Unfallchirurg. 2009; 112(11): Bleeding patient! Preconditions Tranexamic acid Fibrinogen or Cryo Platelets PCC or FFP Protamine Platelet function? FXIII or rfviia
25 Coagulation factors, anticoagulants, FDPs ROTEM parameters Platelets, fibrinogen, colloids Fibrinolytic enzymes, fibrinolysis inhibitors, F XIII A10 = Amplitude 10 min after CT
26 Regression-analysis and Bland-Altman analysis for ExTEM measurements from 866 patients undergoing non-cardiac surgery
27 Regression-analysis and Bland-Altman analysis for FibTEM measurements from 866 patients undergoing non-cardiac surgery
.")
28 Standard coagulation test results were available after a median of 53 min [inter-quartile range (IQR): min], whereas 10 min values of ROTEM results were available online after 23 min (IQR: min).



29 Postpartum haemorrhage with hyperfibrinolysis Intraoperative Substitution: 58 min 2 g tranexamic acid 4 g fibrinogen 3000 IU PCC 1 U pooled PC 4 g fibrinogen 6 U PRBC 28 min 41 min


30 ROTEM after haemodiltution by 50% with Ringer solution, Gelafundin 4% and HAES-steril 10% 50% B, 50% RINGER PT 51 % ATIII 19 % Fib 103 mg/dl PT 108 % ATIII 90 % Fib 218 mg/dl 50% B, 25% R, 25% GELA 50% B, 25% R, 25% HAES PT 54 % ATIII 23 % Fib 100 mg/dl PT 58 % ATIII 23 % Fib 110 mg/dl
31 Transfusion 2010
32
33 Diffuse bleeding after protamine (CABG surgery + AVR): calculated goal-directed therapy with Fibrinogen concentrate 5 min 34 min Targeted increase in MCF FIB = 8 mm 50 mg/kg x 80 kg = 4 g Fibrinogen Alternative: 16 U FFP?
34 mg/kg KG
 27% 44% 2000 IU PCC Alternative: 12 U FFP?")
35 Motorbike accident with open leg fracture and severe bleeding: goal-directed therapy with Prothrombin Complex Concentrate 2 min 19 min 175 cm, 110 kg INR Quick (PT in %) 27% 44% 2000 IU PCC Alternative: 12 U FFP?
36 Diffuse bleeding after protamine (CABG surgery + MVR): goal-directed therapy with Prothrombin Complex Concentrate 2 min 28 min 180 cm, 78 kg ACT 162 s INR 2.8 Quick 25% 25% x 80 kg = 2000 IU PCC Alternative: 12 U FFP? ACT 114 s INR 1.5 Quick 50%

37

38
39
40
41
42
43 115 patients with coagulopathy 44 patients (38.3%) received FFP transfusion INR was corrected in 16 of 44 patients (36%) Median dose of FFP in patients with corrected INR was 17 ml/kg Median dose of FFP in patients without corrected INR was 10 ml/kg New onset of acute lung injury (ALI) was more frequent in the transfused group (18% vs 4%; p = 0.021) Conclusion: The risk-benefit ratio of FFP transfusion in critically ill medical patients with coagulopathy may not be favorable!
44 Advantages of Fibrinogen concentrate and PCC against FFP Rapid, effective, and well predictable increase in coagulation factor activity Applicable in a small volume without the risk of transfusion-associated circulatory overload (TACO) No risk of TRALI and mistransfusion (both responsible for most fatal cases of transfusionrelated adverse events) Effective viral inactivation / elimination (no reported case of viral transmission within the last ten years)


45


46 ROTEM - and Multiplate -based algorithms for perioperative POC coagulation management -62% RBC -66% MT -95% FFP -66% Plt. +66% LTX % RBC -79% FFP -65% Plt. +16% Cases -8.4% RBC -58% MT -98% FFP +115% Plt. +32% Cases


47
48 Intraoperative transfusion requirements for LTX per case at University Hospital Essen, Germany (incidence; median [25 th / 75 th percent.] {90 th ; 95 th ; max}) LTX: 162 in 2010 RBC: 65%; 2 U/LTX [0 /4] {8; 10; 40} PC: 20%; 0 U/LTX [0 /0] {2; 2; 8} FFP: 17%; 0 U/LTX [0 / 0] {3; 5; 34} CRYO: 0%; 0 U/LTX [0 / 0] {0; 0; 0} rfviia: 0%; 0 mg/ltx [0 / 0] {0; 0; 0}
49 4.0% 96.0% Mean age: 53.7 ± 11.3 y 315 male and 180 female (36.4%)
50
51 % Safety and efficacy of prothrombin complex and fibrinogen concentrates in liver transplantation recipients (2-year period): 163 male, 103 female (38.7%); mean age y; mean MELD score p=0.73 4,5 3,6 p=0.4 0,6 0,6 p= % p=0.78 HAT PVT MI PE ST CAE 1,3 0,9 p= p=0.31 7,1 4,5 156 patients (59%) received CFC Study group Control group 110 patients (41%) did not receive any CFC
52 Cummulative cost saving compared to 1999 in visceral surgery and liver transplantation at University Hospital Essen, Germany 1999 = year before implementation of ROTEM diagnostic = 1,765, Euro Cost-saving per year compared to Cost-saving
53 Preise: 85/E 65/E 250/E 288/g 126/500IE 44/500IE 527/1250IE für POC-Diagnostik

54
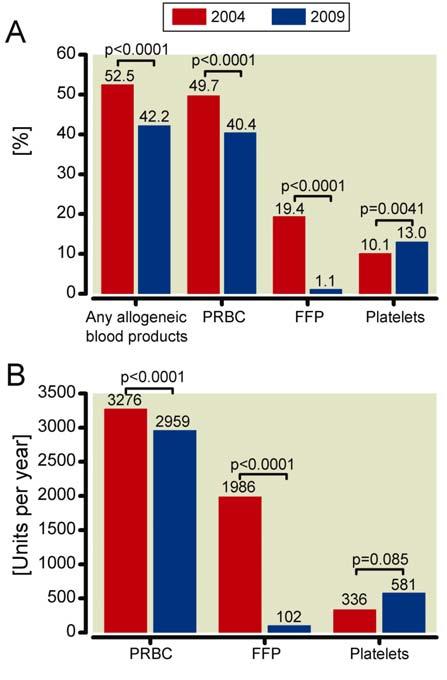
55 (1,718 patients in 2004 and 2,147 in 2009; = 25%)
: 174-7. Bleeding patient!")
56 Platelet function? Tranexamic acid Preconditions Cardiovascular Algorithm Görlinger K, et al. Appl Cardiopulmon Pathophysiol 2009; 13(2): Bleeding patient! Protamine Fibrinogen or Cryo 4F-PCC or FFP Platelets FXIII or rfviia

57 Antifibrinolytics Aprotinin Tranexamic acid

58


59



60 Recurrent thromboembolic events Sufficient (!?) oral anticoagulation and i.v. heparinisation: Quick 18%; INR 3.5; PTT 62,8 s; Fibrinogen 6.56 g/l
61 Tissue factor (TF) formation in the vascular space is a key molecular event leading to DIC.

62 Anesth Analg 2005; 100: ,4% 8,4% Confirmed thrombotic complications 0% 6,3% Myocardial infarction
63 = 23,23 x 2147 = ,81
64
65 1188 patients aged 18+ having cardiac surgery at the Heath Center of the Klinikum Augsburg in 2006; 6% with excessive hemorrhage. Excessive postoperative hemorrhage was defined as: Drainage loss 200 ml/h in any 1 hour (or part thereof) after a 30 min stabilization period within the first 6 h after surgery or Drainage loss 2 ml/kg/h for 2 consecutive hours in the first 6 hours after surgery
66 Variable Postop stroke (n, %) Total cohort (n=1.188) No Bleeding (n=1.112) Bleeding (n=76) p Bleeding vs. No Bleeding 58 (4.9) 46 (4.1) 12 (15.8) LOS ICU (d) 4.1 +/ / /-5.3 < Postop haemofiltration (n, %) In-hospitalmortality (n, %) 30-day-mortality (n, %) 188 (15.8) 165 (14.8) 23 (30.3) (6.1) 56 (5.0) 16 (21.1) < (6.6) 61 (5.5) 17 (22.4) <0.0001
67 Cost Components All Patients (n=1,188) (Cost in ) No Bleeding (n=1,112) (Cost in ) Bleeding (n=76) (Cost in ) P value Surgery-related* (mean SD) 2,304 ( 669) 2,274 ( 615) 4,018 ( 1,753) < Post OR Complications# (mean SD) 208 ( 848) 178 ( 785) 652 ( 1,429) < Re-exploration for bleeding (mean SD) 230 ( 842) 112 ( 600) 1,956 ( 1,635) < Cost of blood products (mean SD) 134 ( 346) 93 ( 257) 732 ( 730) < Cost of Total ICU stay (mean SD) 4,370 ( 6,779) 4,150 ( 6,699) 7,582 ( 7,172) < Total Cost (mean SD) 8,499 ( 7862) 8,027 ( 7,557) 15,404 ( 8,986) < 0.001
68 The treatment of bleeding is to stop the bleeding! Treatment... and to avoid of trauma-related thromboembolic hemorrhage events!... to reduce transfusion requirements and transfusion-related adverse events!... to safe patient s life and hospital costs!
69 Massive transfusion protocols are essential but massive transfusion avoiding algorithms are superior!
70 We can transfuse FFP early in order to stop bleeding or we can stop bleeding early in order to avoid FFP transfusion!
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
How can ROTEM testing help you in cardiac surgery?
 How can ROTEM testing help you in cardiac surgery? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential
How can ROTEM testing help you in cardiac surgery? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
How can ROTEM testing help you in trauma?
 How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
Platelet function in cardiovascular surgery. ROTEM User Meeting, UZ Leuven, 9 November Klaus Görlinger, MD Munich, Germany
 Platelet function in cardiovascular surgery ROTEM User Meeting, UZ Leuven, 9 November 2015 Klaus Görlinger, MD Munich, Germany Disclosures Senior Consultant for Anesthesiology, Emergency and Intensive
Platelet function in cardiovascular surgery ROTEM User Meeting, UZ Leuven, 9 November 2015 Klaus Görlinger, MD Munich, Germany Disclosures Senior Consultant for Anesthesiology, Emergency and Intensive
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference
 Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Hydroxyethyl starch and bleeding
 Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Pathophysiologie und Therapie bei Massenblutung
 Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
DIAGNOSTIC TESTING IN PATIENT BLOOD MANAGEMENT PROGRAMS
 DIAGNOSTIC TESTING IN PATIENT BLOOD MANAGEMENT PROGRAMS The Role of Diagnostic Point-of-Care Testing Diagnostic testing is an essential component of Patient Blood Management. The accurate assessment of
DIAGNOSTIC TESTING IN PATIENT BLOOD MANAGEMENT PROGRAMS The Role of Diagnostic Point-of-Care Testing Diagnostic testing is an essential component of Patient Blood Management. The accurate assessment of
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
1 Transfusion Medicine and Blood Bank Department, H. São João, Centro
 Original Article Interventional Algorithms for the Control of Coagulopathic Bleeding in Surgical, Trauma, and Postpartum Settings: Recommendations From the Share Network Group Clinical and Applied Thrombosis/Hemostasis
Original Article Interventional Algorithms for the Control of Coagulopathic Bleeding in Surgical, Trauma, and Postpartum Settings: Recommendations From the Share Network Group Clinical and Applied Thrombosis/Hemostasis
Recombinant Activated Factor VII: Useful. Department of Surgery Grand Rounds 11/8/10 David Mauchley MD
 Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
23/10/2011. Case One: Mrs. B. Mrs. B., 36 year old, 30 weeks pregnant, 2 nd baby Blood type A negative Belted driver of minivan, struck a parked car
 GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
Challenges in Perioperative. Coagulopathy in Elective and Urgent Cardiac Surgery
 Challenges in Perioperative Hemostasis: Managing Coagulopathy in Elective and Urgent Cardiac Surgery Ian J. Welsby, MD, MBBS, FRCA Assistant Professor Department of Anesthesiology and Critical Care Duke
Challenges in Perioperative Hemostasis: Managing Coagulopathy in Elective and Urgent Cardiac Surgery Ian J. Welsby, MD, MBBS, FRCA Assistant Professor Department of Anesthesiology and Critical Care Duke
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
PBM: The Future of Transfusion December 6 th 2012 East of England RTC. Sue Mallett Royal Free London NHS Foundation Trust
 PBM: The Future of Transfusion December 6 th 2012 East of England RTC Sue Mallett Royal Free London NHS Foundation Trust Patient Blood Management The 3 Pillars Pre-operative optimization of anaemia Minimizing
PBM: The Future of Transfusion December 6 th 2012 East of England RTC Sue Mallett Royal Free London NHS Foundation Trust Patient Blood Management The 3 Pillars Pre-operative optimization of anaemia Minimizing
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Clinical Overview of Coagulation Testing Issues
 Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Coagulation, Haemostasis and interpretation of Coagulation tests
 Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Hematology Review. CCRN exam. The Coagulation Cascade. The Coagulation Cascade. Components include: Intrinsic pathway Extrinsic pathway Common pathway
 CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
anesthesia & mass casualty events
 anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
Modern Transfusion Management in Cardiovascular Surgery
 Modern Transfusion Management in Cardiovascular Surgery Linda Shore-Lesserson, M.D. Professor of Anesthesiology Albert Einstein School of Medicine Montefiore Medical Center Bronx, New York Patient Blood
Modern Transfusion Management in Cardiovascular Surgery Linda Shore-Lesserson, M.D. Professor of Anesthesiology Albert Einstein School of Medicine Montefiore Medical Center Bronx, New York Patient Blood
Management of Massive Transfusion. Philippe Van der Linden MD, PhD CHU Brugmann-HUDERF, Free University of Brussels
 Management of Massive Transfusion Philippe Van der Linden MD, PhD CHU Brugmann-HUDERF, Free University of Brussels Massive Hemorrhage: definition? Replacement of one blood mass in less than 24 hours Dynamic
Management of Massive Transfusion Philippe Van der Linden MD, PhD CHU Brugmann-HUDERF, Free University of Brussels Massive Hemorrhage: definition? Replacement of one blood mass in less than 24 hours Dynamic
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
Managing Coagulopathy in Intensive Care Setting
 Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Damage control resuscitation using blood component therapy in standard doses has a limited effect on coagulopathy during trauma hemorrhage
 Intensive Care Med (2015) 41:239 247 DOI 10.1007/s00134-014-3584-1 ORIGINAL Sirat Khan Ross Davenport Imran Raza Simon Glasgow Henry D. De Ath Pär I. Johansson Nicola Curry Simon Stanworth Christine Gaarder
Intensive Care Med (2015) 41:239 247 DOI 10.1007/s00134-014-3584-1 ORIGINAL Sirat Khan Ross Davenport Imran Raza Simon Glasgow Henry D. De Ath Pär I. Johansson Nicola Curry Simon Stanworth Christine Gaarder
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
Blood and blood component therapy in the critically ill patient
 Blood and blood component therapy in the critically ill patient Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital Points that we shall ponder Transfusion triggers EGDT
Blood and blood component therapy in the critically ill patient Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital Points that we shall ponder Transfusion triggers EGDT
Disseminated Intravascular Coagulation. M.Bahmanpour MD Assistant professor IUMS
 به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
WELCOME. Evaluation Summary
 WELCOME Evaluation Summary 489 delegates from 40 countries Delegate s specialty 239 respondents Delegate s professional activity 208 respondents Overall Evaluation This symposium was helpful for your clinical
WELCOME Evaluation Summary 489 delegates from 40 countries Delegate s specialty 239 respondents Delegate s professional activity 208 respondents Overall Evaluation This symposium was helpful for your clinical
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
MANAGEMENT OF COMMON BLEEDING DISORDERS. Auro Viswabandya Department of Haematology, CMC, Vellore
 MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR
 MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
New Advances in Transfusion EM I LY CO BERLY, M D
 New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
CABG in the Post-Aprotinin Era: Are We Doing Better? Ziv Beckerman, David Kadosh, Zvi Peled, Keren Bitton-Worms, Oved Cohen and Gil Bolotin
 CABG in the Post-Aprotinin Era: Are We Doing Better? Ziv Beckerman, David Kadosh, Zvi Peled, Keren Bitton-Worms, Oved Cohen and Gil Bolotin DISCLOSURES None Objective(s): Our department routinely used
CABG in the Post-Aprotinin Era: Are We Doing Better? Ziv Beckerman, David Kadosh, Zvi Peled, Keren Bitton-Worms, Oved Cohen and Gil Bolotin DISCLOSURES None Objective(s): Our department routinely used
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Precilla V. Veigas 1, Jeannie Callum 2, Sandro Rizoli 3, Bartolomeu Nascimento 4 and Luis Teodoro da Luz 4*
 Veigas et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:114 DOI 10.1186/s13049-016-0308-2 REVIEW Open Access A systematic review on the rotational thrombelastometry
Veigas et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:114 DOI 10.1186/s13049-016-0308-2 REVIEW Open Access A systematic review on the rotational thrombelastometry
Code Blue Caesarean at midnight!
 Code Blue Caesarean at midnight! Disclaimer / Pre-amble These cases have been de-identified to protect the identity of the patient and the treating teams. These are all real cases and real ROTEMs. The
Code Blue Caesarean at midnight! Disclaimer / Pre-amble These cases have been de-identified to protect the identity of the patient and the treating teams. These are all real cases and real ROTEMs. The
Blood Components Transfusion Criteria
 Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Groupe d Intérêt en Hémostase Périopératoire
 How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Resuscitation Update
 Resuscitation Update? Dr. Edward Pyun Jr., M.D. FACS Trauma Medical Director/Surgical ICU Director OSF St. Anthony Medical Center Trauma Services Perryville Surgical Associates November 10, 2012 2009 Recommendations
Resuscitation Update? Dr. Edward Pyun Jr., M.D. FACS Trauma Medical Director/Surgical ICU Director OSF St. Anthony Medical Center Trauma Services Perryville Surgical Associates November 10, 2012 2009 Recommendations
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Massive Blood Transfusion Michael A. Belfort, MD, PhD Professor and Chairman Department of Obstetrics and Gynecology
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Massive Blood Transfusion Michael A. Belfort, MD, PhD Professor and Chairman Department of Obstetrics and Gynecology
A Retrospective, Single-center Cohort Study
 First-line Therapy with Factor Concentrates Combined with Point-of-Care Testing Is Associated with Decreased Allogeneic Blood Transfusion in Cardiovascular Surgery A Retrospective, Single-center Cohort
First-line Therapy with Factor Concentrates Combined with Point-of-Care Testing Is Associated with Decreased Allogeneic Blood Transfusion in Cardiovascular Surgery A Retrospective, Single-center Cohort
HEMOSTASIS AND LIVER DISEASE. P.M. Mannucci. Scientific Direction, IRCCS Ca Granda Foundation Maggiore Hospital, Milan, Italy
 HEMOSTASIS AND LIVER DISEASE P.M. Mannucci Scientific Direction, IRCCS Ca Granda Foundation Maggiore Hospital, Milan, Italy 1964 ACQUIRED HEMOSTASIS DISORDERS: LIVER DISEASE Severe liver disease not uncommonly
HEMOSTASIS AND LIVER DISEASE P.M. Mannucci Scientific Direction, IRCCS Ca Granda Foundation Maggiore Hospital, Milan, Italy 1964 ACQUIRED HEMOSTASIS DISORDERS: LIVER DISEASE Severe liver disease not uncommonly
Balanced Transfusion Resuscitation
 Transparency in Transfusion Medicine 2013 Balanced Transfusion Resuscitation HGD Hendriks MD, PhD University Medical Center Groningen Balancing 1 2 3 Preoperative Peroperative Postoperative Balanced Coagulation
Transparency in Transfusion Medicine 2013 Balanced Transfusion Resuscitation HGD Hendriks MD, PhD University Medical Center Groningen Balancing 1 2 3 Preoperative Peroperative Postoperative Balanced Coagulation
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES
 TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
Bleeding and Management of Coagulopathy
 Bleeding and Management of Coagulopathy Jerrold H. Levy, MD, FAHA Professor of Anesthesiology Deputy Chair for Research Emory University School of Medicine Director, Cardiothoracic Anesthesiology CT Anesthesiology
Bleeding and Management of Coagulopathy Jerrold H. Levy, MD, FAHA Professor of Anesthesiology Deputy Chair for Research Emory University School of Medicine Director, Cardiothoracic Anesthesiology CT Anesthesiology
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Use of Prothrombin Complex Concentrates (PCC) CONTENTS
 CONTENTS") CONTENTS Page 1: Exclusion Criteria and Approved Indications for Use Page 2: Dosing / Administration / Storage Page 4: Prescribing / Monitoring / Dispensing Page 5: Cautions / Warnings / Cost Analysis
CONTENTS Page 1: Exclusion Criteria and Approved Indications for Use Page 2: Dosing / Administration / Storage Page 4: Prescribing / Monitoring / Dispensing Page 5: Cautions / Warnings / Cost Analysis
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
EVIDENCE BASED RED CELL TRANSFUSION. Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System
 EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
Comparison of Tranexamic Acid and Aminocaproic Acid in Coronary Bypass Surgery
 Butler Journal of Undergraduate Research Volume 2 Article 24 2016 Comparison of Tranexamic Acid and Aminocaproic Acid in Coronary Bypass Surgery Lisa K. LeCleir Butler University, lisa.lecleir@gmail.com
Butler Journal of Undergraduate Research Volume 2 Article 24 2016 Comparison of Tranexamic Acid and Aminocaproic Acid in Coronary Bypass Surgery Lisa K. LeCleir Butler University, lisa.lecleir@gmail.com
Guideline for Prothrombin Complex Concentrate Utilization in Nova Scotia
 Nova Scotia Provincial Blood Coordinating Program Guideline for Prothrombin Complex Concentrate Utilization in Nova Scotia Version 3.0 April 2016 PROMOTING EXCELLENCE IN TRANSFUSION MEDICINE http://novascotia.ca/dhw/nspbcp
Nova Scotia Provincial Blood Coordinating Program Guideline for Prothrombin Complex Concentrate Utilization in Nova Scotia Version 3.0 April 2016 PROMOTING EXCELLENCE IN TRANSFUSION MEDICINE http://novascotia.ca/dhw/nspbcp
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol
 Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Dubbi e certezze nella gestione delle emorragie con metodiche point-of-care
 Sessione Educazionale 4 : Gestione del paziente emorragico Dubbi e certezze nella gestione delle emorragie con metodiche point-of-care P. Simioni Università di Padova hemostasis Vascular phase Platelet
Sessione Educazionale 4 : Gestione del paziente emorragico Dubbi e certezze nella gestione delle emorragie con metodiche point-of-care P. Simioni Università di Padova hemostasis Vascular phase Platelet
TRANSFUSIONS WHY DO WE EVEN CARE?????
 TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
HEMATOLOGY REVIEW FOR SURGICAL CRITICAL CARE
 HEMATOLOGY REVIEW FOR SURGICAL CRITICAL CARE Overview I. Blood and Blood Components II. Massive Transfusion and Resuscitation of Hemorrhagic shock III. Acute Coagulopathy of Trauma IV. Damage Control Resuscitation
HEMATOLOGY REVIEW FOR SURGICAL CRITICAL CARE Overview I. Blood and Blood Components II. Massive Transfusion and Resuscitation of Hemorrhagic shock III. Acute Coagulopathy of Trauma IV. Damage Control Resuscitation
Blood Product Utilization A Mythbusters! Style Review. Amanda Haynes, DO 4/28/18
 Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
The principle of 1:1:1 blood product use in the resuscitation of trauma victims. K. D. Boffard
 The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Transfusion Medicine Update KEMC Nov 5, 2014
 Transfusion Medicine Update KEMC Nov 5, 2014 Allison Collins MD FRCPC Ontario Regional Blood Coordinating Network Physician Clinical Project Coordinator Disclosure I have no conflict of interest with this
Transfusion Medicine Update KEMC Nov 5, 2014 Allison Collins MD FRCPC Ontario Regional Blood Coordinating Network Physician Clinical Project Coordinator Disclosure I have no conflict of interest with this
Laboratory Empowerment. Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance
 Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Kay Barrera MD. Surgery Grand Rounds June 19, 2014 SUNY Downstate
 Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
TEG-Directed Transfusion in Complex Cardiac Surgery: Impact on Blood Product Usage
 TEG-Directed Transfusion in Complex Cardiac Surgery: Impact on Blood Product Usage Kevin Fleming, CCP; Roberta E. Redfern, PhD; Rebekah L. March, MPH; Nathan Bobulski, CCP; Michael Kuehne, PhD, PA-C; John
TEG-Directed Transfusion in Complex Cardiac Surgery: Impact on Blood Product Usage Kevin Fleming, CCP; Roberta E. Redfern, PhD; Rebekah L. March, MPH; Nathan Bobulski, CCP; Michael Kuehne, PhD, PA-C; John
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department
 Dr. Klara Vezendi Szeged University Transfusiology Department") Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
American hospitals crawling towards Electronic Medical Records (EMR) and Computerized Physician Order Entry (CPOE)
 and Computerized Physician Order Entry (CPOE)") Welcome! American hospitals crawling towards Electronic Medical Records (EMR) and Computerized Physician Order Entry (CPOE) Still
Welcome! American hospitals crawling towards Electronic Medical Records (EMR) and Computerized Physician Order Entry (CPOE) Still
Figure 1 (A-J). Biochemistry and coagulation parameters in patients with liver insufficiency (n=40). The normal range is indicated by the shaded
. Biochemistry and coagulation parameters in patients with liver insufficiency (n=40). The normal range is indicated by the shaded") Figure 1 (A-J). Biochemistry and coagulation parameters in patients with liver insufficiency (n=40). The normal range is indicated by the shaded area. A vertical line separates the patients into Child-Pugh
Figure 1 (A-J). Biochemistry and coagulation parameters in patients with liver insufficiency (n=40). The normal range is indicated by the shaded area. A vertical line separates the patients into Child-Pugh
Blood Management of the Cardiac Patient in the Postoperative Period
 Blood Management of the Cardiac Patient in the Postoperative Period Al Stammers, MSA, CCP, Eric Tesdahl, PhD Andy Stasko MS, CCP, RRT, Linda Mongero, BS, CCP, Sam Weinstein, MD, MBA Goal To examine the
Blood Management of the Cardiac Patient in the Postoperative Period Al Stammers, MSA, CCP, Eric Tesdahl, PhD Andy Stasko MS, CCP, RRT, Linda Mongero, BS, CCP, Sam Weinstein, MD, MBA Goal To examine the
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
POSTOPERATIVE HEMORRHAGE in cardiac surgery is a
 Increased Chest Tube Drainage Is Independently Associated With Adverse Outcome After Cardiac Surgery Michael C. Christensen, MSc, MPA, DrPH,* Frank Dziewior, MD, Angela Kempel, MSc, and Christian von Heymann,
Increased Chest Tube Drainage Is Independently Associated With Adverse Outcome After Cardiac Surgery Michael C. Christensen, MSc, MPA, DrPH,* Frank Dziewior, MD, Angela Kempel, MSc, and Christian von Heymann,
Major Haemorrhage Transfusion Pathway
 Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Active date July Ratification date: Review date January 2014 Applies to: Staff managing patients on warfarin. Exclusions:
 Guideline Title: Guidelines for the management of warfarin reversal [key words : Beriplex, Octaplex, PCC, vitamin K, anticoagulant, anticoagulation] Authors: Dr Sarah Allford, Consultant Haematologist
Guideline Title: Guidelines for the management of warfarin reversal [key words : Beriplex, Octaplex, PCC, vitamin K, anticoagulant, anticoagulation] Authors: Dr Sarah Allford, Consultant Haematologist
Blood Component Therapy
 Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating