Neuropathy, Radiculopathy & Myelopathy. Jean D. Francois, MD Neurology & Neurophysiology
|
|
|
- Lauren Harvey
- 5 years ago
- Views:
Transcription
1 Neuropathy, Radiculopathy & Myelopathy Jean D. Francois, MD Neurology & Neurophysiology
2 Purpose and Objectives PURPOSE Avoid Confusing Certain Key Neurologic Concepts OBJECTIVES Objective 1: Define & Identify certain types of Neuropathies Objective 2: Define & Identify Radiculopathy & its causes Objective 3: Define & Identify Myelopathy FINANCIAL DISCLOSURE NONE
3 Basics
4 What is Neuropathy? The term 'neuropathy' is used to describe a problem with the nerves, usually the 'peripheral nerves' as opposed to the 'central nervous system' (the brain and spinal cord). It refers to Peripheral neuropathy It covers a wide area and many nerves, but the problem it causes depends on the type of nerves that are affected: Sensory nerves (the nerves that control sensation>skin) causing cause tingling, pain, numbness, or weakness in the feet and hands Motor nerves (the nerves that allow power and movement>muscles) causing weakness in the feet and hands Autonomic nerves (the nerves that control the systems of the body eg gut, bladder>internal organs) causing changes in the heart rate and blood pressure or sweating It May produce Numbness, tingling,(loss of sensation) along with weakness. It can also cause pain. It can affect a single nerve (mononeuropathy) or multiple nerves (polyneuropathy)
5 Neuropathy Symptoms usually start in the longest nerves in the body: Feet & later on the hands ( Stocking-glove pattern) Symptoms usually spread slowly and evenly up the legs and arms. Other body parts may also be affected. Peripheral Neuropathy can affect people of any age. But mostly people over age 55 CAUSES: Neuropathy has a variety of forms and causes. (an injury systemic illness, an infection, an inherited disorder) some of the causes are still unknown. Most common cause: Diabetes. Other causes: alcohol abuse, poor nutrition, autoimmune processes (where the body s own immune system attacks parts of the nerves) and genes. Exposure to certain drugs or toxins can lead to neuropathy. Direct pressure or compression of a single nerve, like in CTS, may cause it to malfunction
6 Diabetic Peripheral Neuropathy Sensory - Numbness as if wearing gloves or socks - Loss of balance, especially with the eyes closed - Painless injuries due to loss of sensation + Burning, prickling pain, tingling, electric shock like feelings, aching, or hypersensitivity to touch Motor UE: fine hand coordination (difficulty with opening jars or turning keys) LE: Foot slapping, toe scuffing, frequent tripping may be early symptoms of foot weakness. Proximal limb weakness: difficulty climbing up and down stairs, difficulty getting up from a seated or supine position, falls due to the knees giving way, and difficulty raising the arms above the shoulders Autonomic GI: Gastroparesis, Dysphagia, Abdominal pain, Diarrhea, Constipation : Persistent sinus tachycardia, Orthostatic hypotension Bladder: Poor urinary stream, incomplete emptying, Straining Sudomotor: sweating of head, neck, and trunk with anhidrosis of lower trunk and extremities

7
8 Neuropathic Pain Diagnosis: Clinical presentations / characteristic symptoms Investigative steps: medical conditions, medications taken, neurologic examination, Blood count, ESR, Blood sugar, Liver and renal function tests, Serum vitamin B 12, Paraprotein levels, Thyroid function tests, Vasculitis profile, electromyography and nerve conduction studies final cause may not be identified Treatment Options: For most types of neuropathy> no treatment is available to cure or modify condition. Treatments are therefore aimed at addressing certain symptoms. Physical therapy, TENS unit (a portable device that sends an electrical current to electrodes attached to the skin), assistive devices, addressing the root cause of condition, identified treatable associated medical cause exercise, Diet Living with PN: Lifestyle change, review habits(smoking, sleeping hours, smoking, alcohol intake, healthy diet, review meds taken including the so-called natural / OTC meds (excess B6 ), Support group
 have reached the level of the knees, paresthesias are noted in the secondlongest nerves (upper limbs) at the tips of")
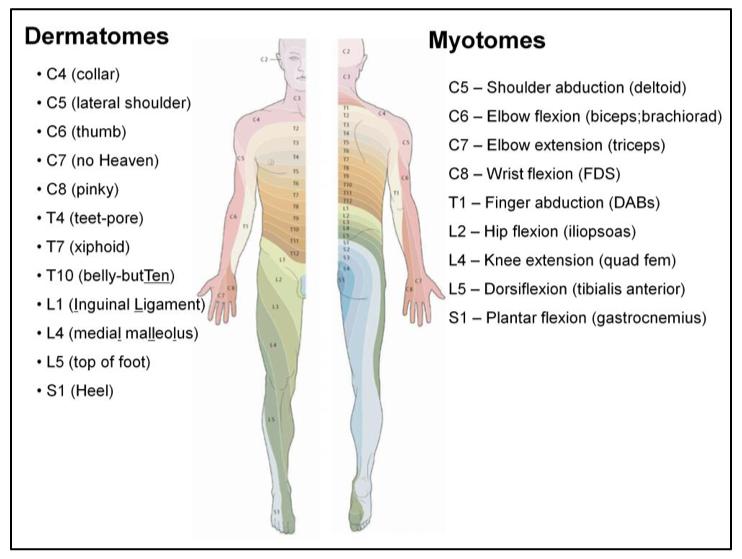
9 In polyneuropathy, the sensory deficits generally follow a length-dependent stocking-glove pattern. By the time sensory disturbances of the longest nerves in the body (lower limbs) have reached the level of the knees, paresthesias are noted in the secondlongest nerves (upper limbs) at the tips of the fingers. When sensory impairment reaches the mid-thigh, involvement of the thirdlongest nerves, the anterior intercostal and lumbar segmental nerves, leads to a tent-shaped area of hypoesthesia on the anterior chest and abdomen. At this point, the recurrent laryngeal nerves may be affected, resulting in hoarseness. Motor weakness is greater in extensor foot muscles than in corresponding flexors. For example, heel walking is affected earlier than toe walking. ILLUSTRATION
10 Charcot Marie Tooth Disease CMT1 Starts at y/o Distal legs: slow progressive weakness, muscle wasting, sensory Foot deformities, difficulties in running or walking resulting from symmetrical weakness and wasting in the intrinsic foot, peroneal, and anterior tibial muscles ankle reflexes are universal frequently knee and upper limb reflexes In 2/3 pts, upper limbs involved later in life CMT2 Begins later 20+, middle age+ Foot and spinal deformities less prominent peripheral nerves are not enlarged, and upper limb involvement, tremor, and general areflexia occur less frequently
11 Causes of Radiculopathies Radiculopathy is caused by compression or irritation of the nerves as they exit the spine. This can be due to mechanical compression of the nerve by a disc herniation, a bone spur (osteophytes) from osteoarthritis, or from thickening of surrounding ligaments. Other less common causes of mechanical compression of the nerves are from a tumor or infection. Either of these can reduce the amount of space in the spinal canal and compress the exiting nerve. Scoliosis can cause the nerves on one side of the spine to become compressed by the abnormal curve of the spine. Inflammation from trauma or degeneration can lead to radiculopathy from direct irritation of the nerves Radiculopathy is one of (if not )the most common cause of disability in people under M people in US seek treatment annually for back pain. 6-8 M with permanent disability
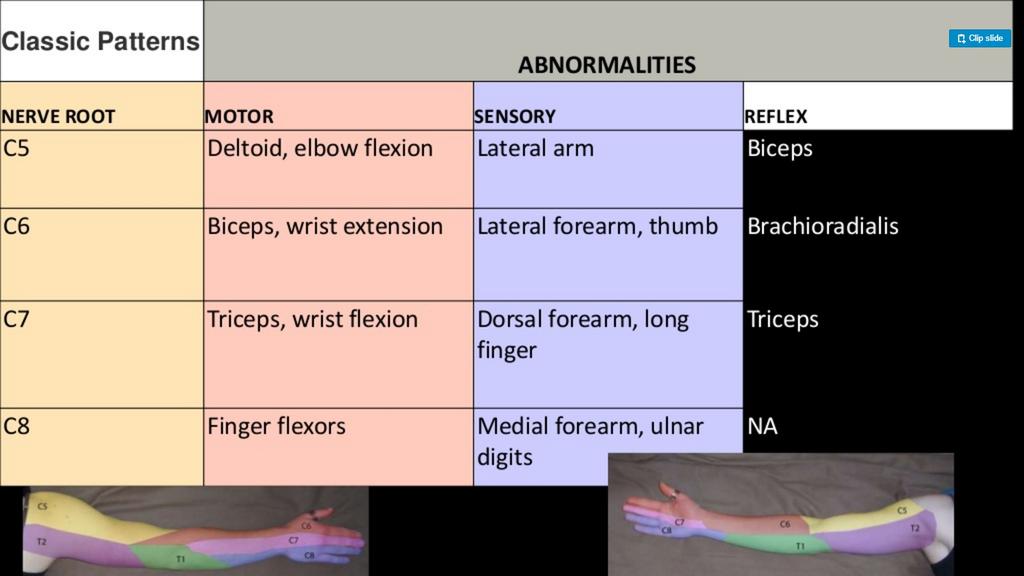
12 Radiculopathies Radix = root, Pathos = suffering or disease > Nerve root disorder Radiculopathy is a condition due to a compressed nerve in the spine that can cause pain, numbness, tingling, or weakness along the course of the nerve. Radiculopathy can occur in any part of the spine, but it is most common in the lower back (lumbar radiculopathy) and in the neck (cervical radiculopathy). It is less commonly found in the middle portion of the spine (thoracic radiculopathy). Lesions of a single nerve root are easier to recognize. Radicular pain and paresthesias (tingling, pins & needles) Sensory loss in the dermatome (skin innervated by a nerve root) Weakness in the myotome (muscles innervated by a spinal cord segment and its nerve root) Diminished deep tendon reflex activity at a segmental level However, with multiple roots involved (polyradiculopathy) clinically may resemble: Disorder of the peripheral nerves polyneuropathy? Disorder of the anterior horn cells - progressive muscular atrophy form of ALS? Supporting evidence for radiculopathy: CSF ( protein, WBCs), paraspinal muscle needle EMG (positive sharp waves and fibrillation potentials), spinal cord MRI (compromise or contrast enhancement of the nerve roots)
13 Causes of Radiculopathies continued Symptoms of RADICULOPATHY: The symptoms of radiculopathy depend on which nerves are affected. The nerves exiting from the neck (cervical spine) control the muscles of the neck and arms and supply sensation there (most common radiculopathies in arms: C5-C6). The nerves from the middle portion of the back (thoracic spine) control the muscles of the chest and abdomen and supply sensation there. The nerves from the lower back (lumbar spine) control the muscles of the buttocks and legs and supply sensation there(most common radiculopathies in legs affect L5 & S1 roots). The most common symptoms of radiculopathy are pain, numbness, and tingling in the arms or legs. It is common for patients to also have localized neck or back pain as well. Lumbar radiculopathy that causes pain that radiates down a lower extremity is commonly referred to as sciatica. Thoracic radiculopathy causes pain from the middle back that travels around to the chest. It is often mistaken for shingles. Some patients develop a hypersensitivity to light touch that feels painful in the area involved. Less commonly, patients can develop weakness in the muscles controlled by the affected nerves. This can indicate nerve damage.
14 Risk factors for Radiculopathy Radiculopathy Risk factors include: activities that place an excessive or repetitive load on the spine. Patients involved in heavy labor or contact sports are more prone to develop radiculopathy than those with a more sedentary lifestyle. A family history of radiculopathy or other spine disorders also increases the risk of developing radiculopathy. DIAGNOSIS: The diagnosis of radiculopathy requires a medical history and physical examination by the physician. (patient will describe the type and location of symptoms, how long they have been present, what makes them better and worse, and what other medical problems present. By knowing the exact location of the patient's symptoms, one can help localize the nerve that is responsible. The physical examination will focus on the extremity involved. It is important to check the patient's muscle strength, sensation, and reflexes to see if there are any abnormalities. Then, obtain imaging studies to look for a source of the radiculopathy. Plain X-rays are often obtained first. These can often identify the presence of trauma or osteoarthritis and early signs of tumor or infection. An MRI scan may then be obtained. This study provides the best look at the soft tissues around the spine including the nerves, the disc and the ligaments. If the patient is unable to obtain an MRI, they may obtain a CT scan instead to explore possible compression of the nerves. Based on condition and clinical indication, the neurologist may do a nerve conduction study (NCS) or electromyogram (EMG). These studies look at the electrical activity along the nerve and can show if there is damage to the nerve
15 Treatment for Radiculopathy Generally, most people can obtain good relief of their symptoms of radiculopathy with conservative treatment such as: anti-inflammatory medications, physical therapy or chiropractic treatment, Acupuncture, and avoiding activity that strains the neck or back. The majority of radiculopathy patients respond well to this conservative treatment, and symptoms often improve within 6 weeks to 3 months. (bear in mind that pain and discomfort has a subjective part) If patients do not improve with the treatments listed above they may benefit from an epidural steroid injection. With the help of an X-ray machine, a physician injects steroid medication between the bones of the spine adjacent to the involved nerves. This can help to rapidly reduce the inflammation and irritation of the nerve and help reduce the symptoms of radiculopathy. In some cases the symptoms continue despite all of the above treatment options. If this occurs and the symptoms are severe, surgery may be an option. The goal of the surgery is to remove the compression from the affected nerve. Depending on the cause of the radiculopathy, this can be done by a laminectomy or a discectomy. A laminectomy removes a small portion of the bone covering the nerve to allow it to have additional space. A discectomy removes the portion of the disc that has herniated out and is compressing a nerve. Overall, The outlook for radiculopathy is good. The majority of patients respond well to conservative treatment options. Those patients that need surgical procedures typically obtain good results as well with no long-term restrictions. Radiculopathy is caused by compression or irritation of a nerve as it exits the spinal column. Most patients with radiculopathy respond well to conservative treatment including medications, physical therapy, or chiropractic treatment. Radiculopathy may resolve within 6 weeks to 3 months. Condition must be individualized

16



17

18


19



20
21
 = root avulsion Status of the (posterior) root may remain uncertain if paraspinal fibrillation potentials are not")
22 Needle EMG into cervical paraspinal muscles (at rest) the posterior primary ramus (first branch of the spinal nerve) arises just beyond the DRG and proximal to the brachial plexus EMG shows cervical paraspinal fibrillation potentials (abnormal) = root avulsion Status of the (posterior) root may remain uncertain if paraspinal fibrillation potentials are not found
23 Diagnosis: Plain radiography, CT myelography, MRI; Needle EMG Sensory conduction studies are useful because SNAPs are typically normal because the lesion is proximal to the DRG in the intervertebral foramina (In contrast to plexopathy and peripheral nerve trunk lesions, where SNAPs are reduced or absent) L5 radiculopathy: if severe enough, compression of the L5 DRG may lead to loss of the superficial peroneal nerve SNAP Appropriate physical therapy > bed rest Epidural corticosteroid injection may help relieve pain, but does not improve neurological function or reduce the need for surgery
 Traumatic brown sequard syndrome Inflammation (myelitis) Transverse myelitis Vascular (vascular myelopathy)")
24 Myelopathy Defined as a neurological deficit in relation to the spinal cord. Myelopathy Traumatic (Acute spinal Cord injury) Traumatic brown sequard syndrome Inflammation (myelitis) Transverse myelitis Vascular (vascular myelopathy) Degenerative joint disease (spinal stenosis) Lumbar stenosis and cervical stenosis
25 Myelopathy Myelopathy is a broad term that refers to spinal cord involvement of multiple etiologies. Spinal cord diseases often have devastating consequences, ranging from quadriplegia and paraplegia to severe sensory deficits due to its confinement in a very small area. Many of these diseases are potentially reversible if they are recognized on time, hence the importance of recognizing the significance of magnetic resonance imaging when approaching a multifactorial disease considered as one of the most critical neurological emergencies, where prognosis depends on an early and accurate diagnosis. However, although MR scanning has become the key investigation in establishing the diagnosis for most patients presenting with a spinal cord syndrome, myelopathy with normal spinal imaging remains a common clinical conundrum: MR normal myelopathy. This is to underscore the challenges presented by such condition that may require urgent intervention. The term Myelopathy describes pathologic conditions that cause spinal cord, meningeal or perimeningeal space damage or dysfunction. It is a common neurologic finding and presentations may vary widely.
26 Myelopathy continued Traumatic injuries, vascular diseases, infections and inflammatory or autoimmune processes may affect the spinal cord. Myelopathy s clinical signs entail a broad spectrum of different etiologies and pathogeneses that may be responsible for such a condition. Whether it is structural, genetic, metabolic, or nutritional in nature, it is critical for the clinician to maintain and investigate a broad differential diagnosis to arrive at the correct diagnosis and provide appropriate treatment and intervention. Correct diagnosis leads to appropriate treatment that may be medical, surgical, or supportive.
27 Myelopathy Cervical = having to do with the spine in the neck Lumbar = lower back Spondylotic = having to do with spinal degeneration Myelopathy = damage to the spinal cord Spinal stenosis, a narrowing of the spinal canal, can damage the spinal cord and cause myelopathy. Degenerative disc disorders or other conditions that affect the spinal column, such as osteoporosis, can result in myelopathy. A tumor associated with the spinal column can cause myelopathy. Myelopathy may occur as the result of another disease, such as multiple sclerosis. Symptoms of Myelopathy: Numbness, clumsiness of the hands arm and/or hand weakness leg stiffness ( walking like a robot ),loss of balance, urinary urgency, neck & low back pain may be present but does not have to be a significant complaint People with myelopathy may have trouble with activities that require some degree of coordination, such as tying shoes or walking downstairs. It is not uncommon to have problems with balance, walking, or muscle weakness. These symptoms may be mild at first and go unnoticed or at least not be a cause of concern. They may notice: Changes in coordination, Sudden muscle weakness, Inability to control Their body, particularly hand-eye coordination, in ways they used to be able to do.,,,this Indicates urgent necessity to see a physician or even a visit in the emergency room.
28

29 MYELOPATHY Work Up: Plain films, Computed tomography, Magnetic resonance imaging Electrodiagnostic studies TREATMENT Since these patients seem to have a typical natural history, there are some particular indications for the surgical management. Thus, patients with gradual neurological deficits and those older than 60 years obtain significant benefits from the surgical treatment. These advantages are clearer in disabled patients, although patients with mild neurological deficits have greater tendency to have their deficits deteriorated when non-operative management is chosen. Non-surgical patients (CSM mild forms) may be treated with cervical immobilization, analgesics, anti-inflammatory and Physiotherapy. In cases associated with cervical radiculopathies, drugs such as Tricyclic antidepressants, anticonvulsants or even antagonists of drugs N-methyl -D-aspartate receptors as riluzole may be used. Myelopathy and spinal cord injuries are serious and complex medical problems. In some cases, compression or pressure on the spinal cord will put pressure on nerves. This may cause pain, weakness, or a lack of control. If patients develop muscle weakness and pain, They may be asked to consider surgery in order to relieve the pressure on the nerves. Over time, pressure on a nerve can permanently damage it. While many cells in the body have the ability to repair themselves, nerve cells can, in some instances, be irreversibly damaged. Typical cervical spine magnetic resonance imaging in cervical spondylotic myelopathy showing severe spinal cord compression in different levels.

30 Brown Sequard Syndrome Hemisection of the spinal cord usually due to traumatic injury. Symptoms Ipsilateral distal UMN dysfunction symptoms Ipsilateral LMN dysfunction AT level of lesion*** Ipsilateral proprioception, light touch and vibration sense lost below lesion Contralateral sensory loss of pain and temperature two levels below lesion due to input at various levels of spinal cord. Diagnosis Physical exam and MRI of spine Treatment Stabilize patient from any trauma that has occurred Expectant management neurological sequelae

31 Radiculopathy vs Myelopathy Any pathological condition involving spinal nerve root Spinal nerve root contains a segment of LMN that comes out of the spinal cord segment. Any pathological condition involving spinal cord Spinal Cord contains many UMN segments and a motor cell body at that level resulting in a few LMN symptoms (help in localization of lesion)
32 Myelopathy, Radiculopathy, Myopathy What You Should Remember about Myelopathy Myelopathy affects the entire spinal cord. It is not like other types of back problems where pain is localized to a specific area of the back, neck, or legs. Myelopathy can be challenging to diagnose. Myelopathy is a serious condition that requires prompt and expert medical attention. Myelopathy Versus Radiculopathy Myelopathy may sometimes be accompanied by radiculopathy. Radiculopathy is the term used to describe pinching of the nerve roots as they exit the spinal cord or cross the intervertebral disc, rather than the compression of the cord itself (myelopathy). Myelopathy Versus Myopathy Myopathy is a muscular disorder and should not be confused with myelopathy, which has to do with nerve damage inside the spinal cord.
33 Myopathy Neuromuscular disorder in which the primary symptom is muscle weakness due to dysfunction of muscle fiber. Etiologies: Congenital or inherited, Idiopathic, infectious, Metabolic, Inflammatory, Endocrine, Drug induced, Toxic Causes: Inflammatory Myopathies, Muscular dystrophies, Congenital Myopathies, Metabolic myopathies, Myotonic Syndromes, Endocrine myopathies, Drug Induced/toxic Types: Congenital, Metabolic, Inflammatory, Atrophic, Myotonic Differential Diagnoses : Motor neuron disease, Neuromuscular junction disorders, Tick-Borne Diseases, Myelopathy/ spinal stenosis, Parkinson s, Guillain-Barre Syndrome Treatment: Based on etiologies...
34 Overall Pearls from Above Presentation Most common disease affecting the peripheral nerve: Diabetes, Alcohol, Nutritional, Guillain-Barré syndrome, Trauma, Hereditary, environmental toxins and drugs, Rheumatic (collagen vascular), Amyloid, Paraneoplastic, Infections, Systemic disease and tumors. Most neuropathies begin distally. They are often asymmetric& accompanied by atrophy & fasciculations. They have Sensory Changes. However, a few may begin proximally: a) Sensory neuropathies: porphyria & rare cases of CMT and Tangier disease b) Motor neuropathies: GBS, Chronic inflammatory demyelinating neuropathy (CIDP), diabetes and idiopathic acute brachial plexus neuropathy. Neuropathies that are predominantly motor: Guillain-Barré syndrome, Diphteric neuropathy, dapsone-induced neuropathy and porphyria. If clinical findings and electrodiagnostic test results are inconclusive, do a biopsy (nerve biopsy for suspected large-fiber neuropathy or skin punch biopsy for suspected small-fiber neuropathy). If all limbs are affected, consider MRI to rule out cervical spinal cord compression. Peripheral neuropathy exam: distal, often asymmetric weakness, atrophy, fasciculations & sensory loss, Muscle tone is decreaced or normal. Reflexes are usually diminished, There may be changes in skin texture,some swelling, temperature dysregulation and loss of hair or nails. 34
35 Overall Pearls from Above Presentation continued RADICULOPATHIES: Hallmark is pain, that is usually described as sharp, stabbing, hot and electric. It typically shoots or radiates down the limb. Otherwise may resemble Peripheral neuropathy (asymmetric weakness, atrophy, fasciculations & sensory loss). Weakness may be proximal or distal depending upon which roots are involved. EXAMINATION: also may find asymmetric muscle weakness with atrophy, & fasciculations. Sensory loss occurs in a dermatomal distribution. Muscle tone is normal or decreased. Reflexes in the involved muscles are diminished or absent. Any maneuvers that tend to stretch the root often such as straight leg raising, or neck rotation- aggravate the pain. MYELOPATHY: patient with Spinal cord disease usually reveals a triad of symptoms: sensory level, Distal symmetric, spastic weakness, Bowel and bladder problems (exam: no significant atrophy or fasciculations, positive Babinski signs, increased reflexes / clonus, increased tone, greater distal weakness than proximal, greater weakness of extensors / antigravity muscles than flexors 35

36 Summary Neuropathy Symptoms most commonly appear distal to lesion. Lesion is in the periphery. Usually gives rise to sensory, motor, or automonic symptoms that do not exactly correlate with dermatomes and reflex locations Results in LMN motor symptoms Radiculopathy Symptoms most commonly involve a dermatomal pattern. Lesion is at the level of the nerve roots Often gives rise to sensory and motor abnormalities Results in LMN motor symptoms Can occur with myelopathy Myelopathy Symptoms most commonly are indicative of UMN lesion LMN symptoms present at level of pathology. (lost reflexes help with localization) Can occur with radiculopathy as well.
37 Contact Information Jean D. Francois, MD Neurologist & Neurophysiologist The Brookdale University Hospital and Medical Center Kingsbrook Jewish Medical Center VARIOUS SOURCES: WebMD newsletter Up-to-date Medicine net Merck Manuals American Academy of Neurology Archives PubMed ETC
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists
 & electromyography (EMG) for non-neurologists") Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Herniated Disk in the Lower Back
 Herniated Disk in the Lower Back This article is also available in Spanish: Hernia de disco en la columna lumbar (topic.cfm?topic=a00730). Sometimes called a slipped or ruptured disk, a herniated disk
Herniated Disk in the Lower Back This article is also available in Spanish: Hernia de disco en la columna lumbar (topic.cfm?topic=a00730). Sometimes called a slipped or ruptured disk, a herniated disk
The Internist s Approach to Neuropathy
 The Internist s Approach to Neuropathy VOLKAN GRANIT, MD, MSC ASSISTANT PROFESSOR OF NEUROLOGY NEUROMUSCU LAR DIVISION UNIVERSITY OF MIAMI, MILLER SCHOOL OF MEDICINE RELEVANT DECLARATIONS Financial disclosures:
The Internist s Approach to Neuropathy VOLKAN GRANIT, MD, MSC ASSISTANT PROFESSOR OF NEUROLOGY NEUROMUSCU LAR DIVISION UNIVERSITY OF MIAMI, MILLER SCHOOL OF MEDICINE RELEVANT DECLARATIONS Financial disclosures:
Lumbar Disc Prolapse. Dr. Ahmed Salah Eldin Hassan. Professor of Neurosurgery & Consultant spinal surgeon
 Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
 The spine is made of a column of bones. Each bone, or vertebra, is formed by a round block of bone, called a vertebral body. A bony ring attaches to the back of the vertebral body. When the vertebra bones
The spine is made of a column of bones. Each bone, or vertebra, is formed by a round block of bone, called a vertebral body. A bony ring attaches to the back of the vertebral body. When the vertebra bones
Daniel J. Blizzard, MD, MS
 Daniel J. Blizzard, MD, MS None Common degenerative (usually) condition caused by compression on the spinal cord that is characterized by clumsiness and difficulty with fine motor tasks in the hands and
Daniel J. Blizzard, MD, MS None Common degenerative (usually) condition caused by compression on the spinal cord that is characterized by clumsiness and difficulty with fine motor tasks in the hands and
American Board of Physical Medicine & Rehabilitation. Part I Curriculum & Weights
 American Board of Physical Medicine & Rehabilitation Part I Curriculum & Weights Neurologic Disorders 30% Stroke Spinal Cord Injury Traumatic Brain Injury Neuropathies a) Mononeuropathies b) Polyneuropathies
American Board of Physical Medicine & Rehabilitation Part I Curriculum & Weights Neurologic Disorders 30% Stroke Spinal Cord Injury Traumatic Brain Injury Neuropathies a) Mononeuropathies b) Polyneuropathies
Making sense of Nerve conduction & EMG
 Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Misdiagnosis in cervical spondylosis myelopathy.
 Journal of the International Society of Head and Neck Trauma (ISHANT) Case report Misdiagnosis in cervical spondylosis myelopathy. Dr. Reinel A. Junco Martin. Neurosurgeon. Assistant professor Miguel Enriquez
Journal of the International Society of Head and Neck Trauma (ISHANT) Case report Misdiagnosis in cervical spondylosis myelopathy. Dr. Reinel A. Junco Martin. Neurosurgeon. Assistant professor Miguel Enriquez
Neck Pain Guide. Understanding Causes, Treatment and Prevention
 Neck Pain Guide Understanding Causes, Treatment and Prevention Neck pain may be more than a nuisance; it could be a symptom of an underlying condition. Use this guide to help you understand common causes
Neck Pain Guide Understanding Causes, Treatment and Prevention Neck pain may be more than a nuisance; it could be a symptom of an underlying condition. Use this guide to help you understand common causes
X-Plain Muscles Reference Summary
 X-Plain Reference Summary Introduction are very important elements of the human body. They account for about half of a person s weight. Understanding how muscles work and how they can be injured is necessary
X-Plain Reference Summary Introduction are very important elements of the human body. They account for about half of a person s weight. Understanding how muscles work and how they can be injured is necessary
The main causes of cervical radiculopathy include degeneration, disc herniation, and spinal instability.
 SpineFAQs Cervical Radiculopathy Neck pain has many causes. Mechanical neck pain comes from injury or inflammation in the soft tissues of the neck. This is much different and less concerning than symptoms
SpineFAQs Cervical Radiculopathy Neck pain has many causes. Mechanical neck pain comes from injury or inflammation in the soft tissues of the neck. This is much different and less concerning than symptoms
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
Case Studies, Impairment of the Spine in Washington State
 Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Cervical Plating BACK PAIN
 BACK PAIN Back Pain Back pain is frequent complaint. It is the commonest cause of work-related absence in the world. Although back pain may be painful and uncomfortable, it is not usually serious. Even
BACK PAIN Back Pain Back pain is frequent complaint. It is the commonest cause of work-related absence in the world. Although back pain may be painful and uncomfortable, it is not usually serious. Even
Spine Conditions and Treatments. Your Guide to Common
 Your Guide to Common Spine Conditions and Treatments The spine is made up of your neck and backbone. It allows your body to bend and move freely. As you get older, it is normal to have aches and pains.
Your Guide to Common Spine Conditions and Treatments The spine is made up of your neck and backbone. It allows your body to bend and move freely. As you get older, it is normal to have aches and pains.
Electrodiagnostics for Back & Neck Pain. Steven Andersen, MD Providence Physiatry Clinic
 Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
SpineFAQs. Lumbar Spondylolisthesis
 SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
Cervical Spine in Baseball
 Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis by David Borenstein, MD In a previous article on low back pain, I reviewed the anatomy of the spine and discussed three causes of low back pain: muscle strain, herniated intervertebral
Lumbar Spinal Stenosis by David Borenstein, MD In a previous article on low back pain, I reviewed the anatomy of the spine and discussed three causes of low back pain: muscle strain, herniated intervertebral
Differential Diagnosis of Neuropathies and Compression. Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre
 Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Lumbosacral plexus lesion Lumbosacral plexus disorders G54.1 Neuralgic amyotrophy Neuralgic amyotrophy G
 ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES Focal Neuropathy ICD-9-CM ICD-10-CM Mononeuropathy G56.00 Carpal tunnel syndrome 354.00 Other median nerve lesion 354.10 Lesion of ulnar nerve 354.20
ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES Focal Neuropathy ICD-9-CM ICD-10-CM Mononeuropathy G56.00 Carpal tunnel syndrome 354.00 Other median nerve lesion 354.10 Lesion of ulnar nerve 354.20
A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017
 A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017 Disclosures Research support from Cytokinetics, Inc Catalyst, Inc Editorial fees from UptoDate. Objectives Describe
A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017 Disclosures Research support from Cytokinetics, Inc Catalyst, Inc Editorial fees from UptoDate. Objectives Describe
CERVICAL SPONDYLOSIS AND CERVICAL SPONDYLOTIC MYELOPATHY
 CERVICAL SPONDYLOSIS AND CERVICAL SPONDYLOTIC MYELOPATHY A NEUROSURGEON S VIEW A Preventable Journey to a wheelchair bound-life Dr H. BOODHOO F.C.S (Neurosurgery) Cervical Spondylosis Spinal Osteoarthritis
CERVICAL SPONDYLOSIS AND CERVICAL SPONDYLOTIC MYELOPATHY A NEUROSURGEON S VIEW A Preventable Journey to a wheelchair bound-life Dr H. BOODHOO F.C.S (Neurosurgery) Cervical Spondylosis Spinal Osteoarthritis
Degenerative Disease of the Spine
 Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Clinical Aspects of Peripheral Nerve and Muscle Disease. Roy Weller Clinical Neurosciences University of Southampton School of Medicine
 Clinical Aspects of Peripheral Nerve and Muscle Disease Roy Weller Clinical Neurosciences University of Southampton School of Medicine Normal Nerves 1. Anterior Horn Cell 2. Dorsal root ganglion cell 3.
Clinical Aspects of Peripheral Nerve and Muscle Disease Roy Weller Clinical Neurosciences University of Southampton School of Medicine Normal Nerves 1. Anterior Horn Cell 2. Dorsal root ganglion cell 3.
SpineFAQs. Neck Pain Diagnosis and Treatment
 SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
BACK PAIN. Disclaimer. Integrated web marketing. Multimedia Health Education
 BACK PAIN Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or a licensed healthcare
BACK PAIN Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or a licensed healthcare
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for
 Chapter 13 Outline Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for what you need to know from Exhibits 13.1 13.4 I. INTRODUCTION A. The spinal cord and spinal nerves
Chapter 13 Outline Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for what you need to know from Exhibits 13.1 13.4 I. INTRODUCTION A. The spinal cord and spinal nerves
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
NECK AND BACK PAIN AN INTRODUCTION TO
 AN INTRODUCTION TO NECK AND BACK PAIN This booklet provides general information on neck and back pain. It is not meant to replace any personal conversations that you might wish to have with your physician
AN INTRODUCTION TO NECK AND BACK PAIN This booklet provides general information on neck and back pain. It is not meant to replace any personal conversations that you might wish to have with your physician
Your back in focus. Degenerative disc disease Spinal stenosis. Information for patients 1 Ottobock Your back in focus
 Your back in focus Degenerative disc disease Spinal stenosis Information for patients 1 Ottobock Your back in focus What is degenerative disc disease? Degenerative disc disease occurs as a result of wear
Your back in focus Degenerative disc disease Spinal stenosis Information for patients 1 Ottobock Your back in focus What is degenerative disc disease? Degenerative disc disease occurs as a result of wear
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Electrodiagnostic Testing Electromyogram and Nerve Conduction Study
 Electrodiagnostic Testing Electromyogram and Nerve Conduction Study North American Spine Society Public Education Series What Is Electrodiagnostic Testing? The term electrodiagnostic testing covers a
Electrodiagnostic Testing Electromyogram and Nerve Conduction Study North American Spine Society Public Education Series What Is Electrodiagnostic Testing? The term electrodiagnostic testing covers a
Nerve Conduction Studies and EMG
 Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS
 CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
Spinal Stenosis Surgical
 Spinal Stenosis Surgical Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or
Spinal Stenosis Surgical Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Evaluation of Peripheral Neuropathy. Evaluation of Peripheral Neuropathy - Introduction
 Evaluation of Peripheral Neuropathy Chris Edwards, MD Ochsner Neurology, Main Campus Evaluation of Peripheral Neuropathy - Introduction A very common complaint in the clinic Presentation is variable Multiple
Evaluation of Peripheral Neuropathy Chris Edwards, MD Ochsner Neurology, Main Campus Evaluation of Peripheral Neuropathy - Introduction A very common complaint in the clinic Presentation is variable Multiple
Hailee Gibson, CCPA Neurosurgery Physician Assistant. Windsor Neurosurgery & Spine Associates. Windsor Regional Hospital Ouellette Campus
 Hailee Gibson, CCPA Neurosurgery Physician Assistant Windsor Neurosurgery & Spine Associates Windsor Regional Hospital Ouellette Campus Disclosures I have no disclosures Learning Objectives Provide information
Hailee Gibson, CCPA Neurosurgery Physician Assistant Windsor Neurosurgery & Spine Associates Windsor Regional Hospital Ouellette Campus Disclosures I have no disclosures Learning Objectives Provide information
Common Conditions. Visit our homepage for more info >> TABLE OF CONTENTS. Bulging/Herniated Disc... PAGE 2. Cervical (Neck) Pain...
 Pain...") Common Conditions TABLE OF CONTENTS Bulging/Herniated Disc... PAGE 2 Cervical (Neck) Pain... PAGE 3 Degenerative Disc Disease... PAGE 4 Sciatica...PAGE 5 Spinal Stenosis... PAGE 6 Spondylolisthesis...
Common Conditions TABLE OF CONTENTS Bulging/Herniated Disc... PAGE 2 Cervical (Neck) Pain... PAGE 3 Degenerative Disc Disease... PAGE 4 Sciatica...PAGE 5 Spinal Stenosis... PAGE 6 Spondylolisthesis...
Cervical intervertebral disc disease Degenerative diseases F 04
 Cervical intervertebral disc disease Degenerative diseases F 04 How is a herniated cervical intervertebral disc treated? Conservative treatment is generally sufficient for mild symptoms not complicated
Cervical intervertebral disc disease Degenerative diseases F 04 How is a herniated cervical intervertebral disc treated? Conservative treatment is generally sufficient for mild symptoms not complicated
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc. Copyright 2014, 2011, 2006 by Saunders, an imprint of Elsevier, Inc.
 Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
RADICULOPATHY AN INTRODUCTION TO
 AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
Corporate Medical Policy
 Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
A Patient s Guide to Cervical Radiculopathy
 A Patient s Guide to Cervical Radiculopathy 950 Breckinridge Lane Suite 220 Louisville, KY 40223 Phone: 502.708.2940 DISCLAIMER: The information in this booklet is compiled from a variety of sources. It
A Patient s Guide to Cervical Radiculopathy 950 Breckinridge Lane Suite 220 Louisville, KY 40223 Phone: 502.708.2940 DISCLAIMER: The information in this booklet is compiled from a variety of sources. It
Evaluation of Tingling and Numbness in the Upper Extremities
 Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Lumbar spinal canal stenosis Degenerative diseases F 08
 What is lumbar spinal canal stenosis? This condition involves the narrowing of the spinal canal, and of the lateral recesses (recesssus laterales) and exit openings (foramina intervertebralia) for the
What is lumbar spinal canal stenosis? This condition involves the narrowing of the spinal canal, and of the lateral recesses (recesssus laterales) and exit openings (foramina intervertebralia) for the
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology
 Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Ergonomics / Back Safety
 120 White Bridge Rd. Nashville, TN 37209 Ergonomics / Back Safety We often think of back safety as only being important for people in heavy physical jobs. The fact is that back safety is important for
120 White Bridge Rd. Nashville, TN 37209 Ergonomics / Back Safety We often think of back safety as only being important for people in heavy physical jobs. The fact is that back safety is important for
ACUTE AND CHRONIC NEUROPATHIES
 ACUTE AND CHRONIC NEUROPATHIES American College of Osteopathic Internists Internal Medicine Board Review Course 2018 April 25-29, 2018 Marriott Chicago Downtown Chicago, Illinois Scott Spradlin D.O.,FACP,FACOI
ACUTE AND CHRONIC NEUROPATHIES American College of Osteopathic Internists Internal Medicine Board Review Course 2018 April 25-29, 2018 Marriott Chicago Downtown Chicago, Illinois Scott Spradlin D.O.,FACP,FACOI
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
HERNIATED DISCS AN INTRODUCTION TO
 AN INTRODUCTION TO HERNIATED S This booklet provides general information on herniated discs. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO HERNIATED S This booklet provides general information on herniated discs. It is not meant to replace any personal conversations that you might wish to have with your physician or other
Discal herniation and spondylosis
 III.8.4.6 Degenerative disorders of the spine Introduction the frequency of locomotor disorders increases with age Low back pain is a very common disorder. According to medical literature, it is the second
III.8.4.6 Degenerative disorders of the spine Introduction the frequency of locomotor disorders increases with age Low back pain is a very common disorder. According to medical literature, it is the second
Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY?
 Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY? D iabetic neuropathy is actually a group of nerve diseases. All of these disorders affect the peripheral nerves, that is, the nerves that are outside the
Diabetic Neuropathy WHAT IS DIABETIC NEUROPATHY? D iabetic neuropathy is actually a group of nerve diseases. All of these disorders affect the peripheral nerves, that is, the nerves that are outside the
Index. Note: Page numbers of article titles are in boldface type.
 Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
CHAPTER 13 LECTURE OUTLINE
 CHAPTER 13 LECTURE OUTLINE I. INTRODUCTION A. The spinal cord and spinal nerves mediate reactions to environmental changes. B. The spinal cord has several functions. 1. It processes reflexes. 2. It is
CHAPTER 13 LECTURE OUTLINE I. INTRODUCTION A. The spinal cord and spinal nerves mediate reactions to environmental changes. B. The spinal cord has several functions. 1. It processes reflexes. 2. It is
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome
 A Patient s Guide to Pain Management: Complex Regional Pain Syndrome Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 DISCLAIMER:
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 DISCLAIMER:
Seema Sikka, MD January 18, 2014 TRANSVERSE MYELITIS: A CLINICAL OVERVIEW
 Seema Sikka, MD January 18, 2014 TRANSVERSE MYELITIS: A CLINICAL OVERVIEW DISCLOSURES I have no industry relationships to disclose. I will not discuss off-label use. OBJECTIVES: TRANSVERSE MYELITIS Review
Seema Sikka, MD January 18, 2014 TRANSVERSE MYELITIS: A CLINICAL OVERVIEW DISCLOSURES I have no industry relationships to disclose. I will not discuss off-label use. OBJECTIVES: TRANSVERSE MYELITIS Review
Medicare Regulations for Chiropractors. Presented by Clinic Pro Software Inc. Marilyn K. Gard. CEO, MBA
 Medicare Regulations for Chiropractors Presented by Clinic Pro Software Inc. Marilyn K. Gard. CEO, MBA Use AT modifier which means active treatment. Claims submitted for Chiropractic manipulative treatment
Medicare Regulations for Chiropractors Presented by Clinic Pro Software Inc. Marilyn K. Gard. CEO, MBA Use AT modifier which means active treatment. Claims submitted for Chiropractic manipulative treatment
Facet Joint Syndrome / Arthritis
 Facet Joint Syndrome / Arthritis Overview Facet joint syndrome is an arthritis-like condition of the spine that can be a significant source of back and neck pain. It is caused by degenerative changes to
Facet Joint Syndrome / Arthritis Overview Facet joint syndrome is an arthritis-like condition of the spine that can be a significant source of back and neck pain. It is caused by degenerative changes to
Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto
 Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome
 A Patient s Guide to Pain Management: Complex Regional Pain Syndrome 950 Breckinridge Lane Suite 220 Louisville, KY 40223 Phone: 502.708.2940 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Pain Management: Complex Regional Pain Syndrome 950 Breckinridge Lane Suite 220 Louisville, KY 40223 Phone: 502.708.2940 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Cervical Radiculopathy
 A Patient s Guide to Cervical Radiculopathy 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Cervical Radiculopathy 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety
The signs and symptoms of diabetic neuropathy vary, depending on the type of neuropathy and which nerves are affected.
 DIABETIC NEUROPATHY Overview Diabetic neuropathy is a type of nerve damage that can occur if you have diabetes. High blood sugar (glucose) can injure nerve fibers throughout your body, but diabetic neuropathy
DIABETIC NEUROPATHY Overview Diabetic neuropathy is a type of nerve damage that can occur if you have diabetes. High blood sugar (glucose) can injure nerve fibers throughout your body, but diabetic neuropathy
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis This article is also available in Spanish: Estenosis de la columna lumbar (topic.cfm?topic=a00701). A common cause of low back and leg pain is lumbar spinal stenosis. As we age,
Lumbar Spinal Stenosis This article is also available in Spanish: Estenosis de la columna lumbar (topic.cfm?topic=a00701). A common cause of low back and leg pain is lumbar spinal stenosis. As we age,
Regional Pain Syndromes: Neck and Low Back
 Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL
 SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018
 EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
A/Professor Arun Aggarwal Balmain Hospital
 A/Professor Arun Aggarwal Balmain Hospital Nerve Conduction Studies Test to evaluate the function of motor / sensory nerves Evaluate Paraesthesia (numbness, tingling, burning) Weakness of arms and legs
A/Professor Arun Aggarwal Balmain Hospital Nerve Conduction Studies Test to evaluate the function of motor / sensory nerves Evaluate Paraesthesia (numbness, tingling, burning) Weakness of arms and legs
Cox Technic Case Report #169 published at (sent 5/9/17) 1
 1") Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
Chapter 13. The Spinal Cord & Spinal Nerves. Spinal Cord. Spinal Cord Protection. Meninges. Together with brain forms the CNS Functions
 Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
NEUROCARE 1000/4P NEUROMUSCULAR ELECTRIC STIMULATOR FOR DIABETIC NEUROPATHY TREATMENT
 NEUROCARE 1000/4P NEUROMUSCULAR ELECTRIC STIMULATOR FOR DIABETIC NEUROPATHY TREATMENT Diabetic neuropathies are common in almost 50 percent of all sufferers. Although current studies still don t pinpoint
NEUROCARE 1000/4P NEUROMUSCULAR ELECTRIC STIMULATOR FOR DIABETIC NEUROPATHY TREATMENT Diabetic neuropathies are common in almost 50 percent of all sufferers. Although current studies still don t pinpoint
Brisbin Family Chiropractic
 Information reviewed with patient: Dr. Initials Today s Date Brisbin Family Chiropractic Name: Sex: Male Female Address: City: Postal Code: Home Ph# Work# Ext# Cell# Preferred number (circle one) Home
Information reviewed with patient: Dr. Initials Today s Date Brisbin Family Chiropractic Name: Sex: Male Female Address: City: Postal Code: Home Ph# Work# Ext# Cell# Preferred number (circle one) Home
PARADIGM SPINE. Patient Information. Treatment of a Narrow Lumbar Spinal Canal
 PARADIGM SPINE Patient Information Treatment of a Narrow Lumbar Spinal Canal Dear Patient, This brochure is intended to inform you of a possible treatment option for narrowing of the spinal canal, often
PARADIGM SPINE Patient Information Treatment of a Narrow Lumbar Spinal Canal Dear Patient, This brochure is intended to inform you of a possible treatment option for narrowing of the spinal canal, often
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
PNS and ANS Flashcards
 1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
Regional Review of Musculoskeletal System: Head, Neck, and Cervical Spine Presented by Michael L. Fink, PT, DSc, SCS, OCS Pre- Chapter Case Study
 Regional Review of Musculoskeletal System: Presented by Michael L. Fink, PT, DSc, SCS, OCS (20 minutes CEU Time) Subjective A 43-year-old male, reported a sudden onset of left-sided neck and upper extremity
Regional Review of Musculoskeletal System: Presented by Michael L. Fink, PT, DSc, SCS, OCS (20 minutes CEU Time) Subjective A 43-year-old male, reported a sudden onset of left-sided neck and upper extremity
Back and Neck Injuries: Surgical Advances and Treatment
 Back and Neck Injuries: Surgical Advances and Treatment Ara Deukmedjian, MD Board Certified Neurosurgeon June 8, 2017 1 2 Spinal Joints: Anatomy Two types of Spinal Joints: Spinal (intervertebral) disc
Back and Neck Injuries: Surgical Advances and Treatment Ara Deukmedjian, MD Board Certified Neurosurgeon June 8, 2017 1 2 Spinal Joints: Anatomy Two types of Spinal Joints: Spinal (intervertebral) disc
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management.
 River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
Scoliosis. This leaflet gives you information on scoliosis and what you can do to help manage the symptoms you are experiencing.
 Scoliosis This leaflet gives you information on scoliosis and what you can do to help manage the symptoms you are experiencing. What is Scoliosis? The term scoliosis refers to the abnormal twisting and
Scoliosis This leaflet gives you information on scoliosis and what you can do to help manage the symptoms you are experiencing. What is Scoliosis? The term scoliosis refers to the abnormal twisting and
P1: OTA/XYZ P2: ABC c01 BLBK231-Ginsberg December 23, :43 Printer Name: Yet to Come. Part 1. The Neurological Approach COPYRIGHTED MATERIAL
 Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Slide 1. Slide 2. Slide 3. Intro to Physical Therapy for Neuromuscular Conditions. PT Evaluation. PT Evaluation
 Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
North American Spine Society Public Education Series
 Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Numb bum means cauda equina Per rectal examination is indicated to assess anal tone
 SPINE Age and occupation Pain: Where: Low back or leg Which is worse? Where about in the leg? Describe the radiation How long? More than 6 wks need warrant evaluation How the pain is now compared to the
SPINE Age and occupation Pain: Where: Low back or leg Which is worse? Where about in the leg? Describe the radiation How long? More than 6 wks need warrant evaluation How the pain is now compared to the
Back Pain. John W. Engstrom, MD December 16, Disclosures. A Clinical Approach to the Evaluation of Back Pain and Lumbar Radiculopathy
 Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Acute Low Back Pain. North American Spine Society Public Education Series
 Acute Low Back Pain North American Spine Society Public Education Series What Is Acute Low Back Pain? Acute low back pain (LBP) is defined as low back pain present for up to six weeks. It may be experienced
Acute Low Back Pain North American Spine Society Public Education Series What Is Acute Low Back Pain? Acute low back pain (LBP) is defined as low back pain present for up to six weeks. It may be experienced
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
A Patient s Guide to Dropped Head Syndrome
 A Patient s Guide to Dropped Head Syndrome 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources. It
A Patient s Guide to Dropped Head Syndrome 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources. It
Chapter 13: The Spinal Cord and Spinal Nerves
 Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Peggers Super Summaries: The Aging Spine
 Aging Spine: AGING PROCESS Osteopenia 10% of 50 year old males and 25% of 50 year females Disc dehydration Facet degeneration Soft tissue hypertrophy 2 0 deformity Leg pain worse than back pain from nerve
Aging Spine: AGING PROCESS Osteopenia 10% of 50 year old males and 25% of 50 year females Disc dehydration Facet degeneration Soft tissue hypertrophy 2 0 deformity Leg pain worse than back pain from nerve
The Spine.
 The Spine www.fisiokinesiterapia.biz Characteristics of Vertebrae Cervical Spine 1 and 2 Sacrum and Coccyx Curves Lordotic in the Spine Kyphotic Lordotic Ligamentous Support Muscles of the Spine Spinal
The Spine www.fisiokinesiterapia.biz Characteristics of Vertebrae Cervical Spine 1 and 2 Sacrum and Coccyx Curves Lordotic in the Spine Kyphotic Lordotic Ligamentous Support Muscles of the Spine Spinal
MOTOR NEURONE DISEASE
 MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
Sir William Asher ANATOMY
 SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his