A discussion about Adhesive capsulitis 한상민
|
|
|
- Christopher Kelly
- 5 years ago
- Views:
Transcription
1 A discussion about Adhesive capsulitis 한상민
2 Adhesive capsulitis Frozen shoulder Periarthritis Irritative capsulitis Scapulohumeral periarthritis

3 Shoulder anatomy SC joint AC joint GH joint team ST joint
")

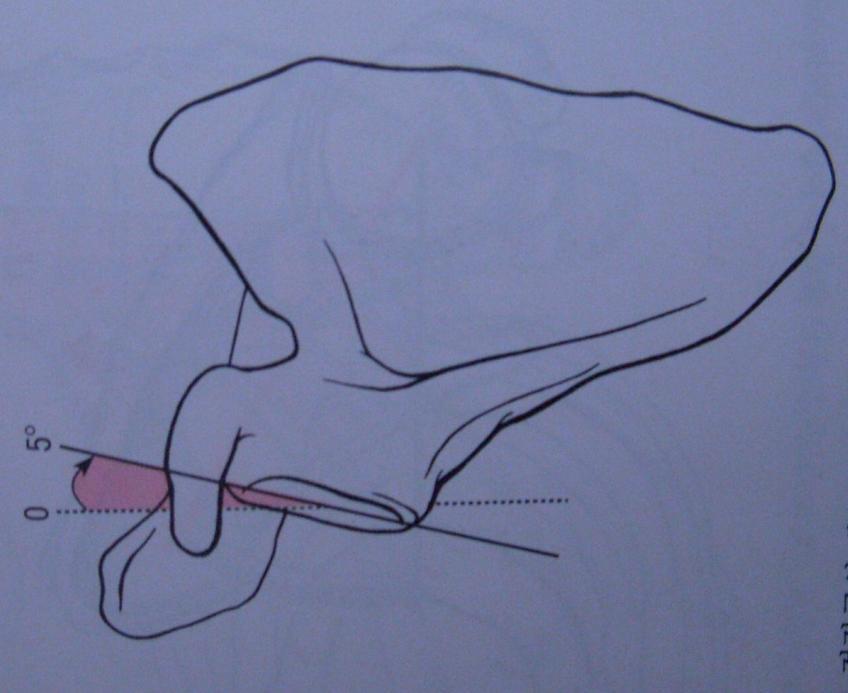
4 Shoulder anantomy(clavicle) Medial- convex, Lateral- concave 수평면에서약간위쪽과후방으로기움 (20도) Medial- Costal facet Lateral- Acromial facet Humuerus 30 retroversion Scapula frontal plan 35

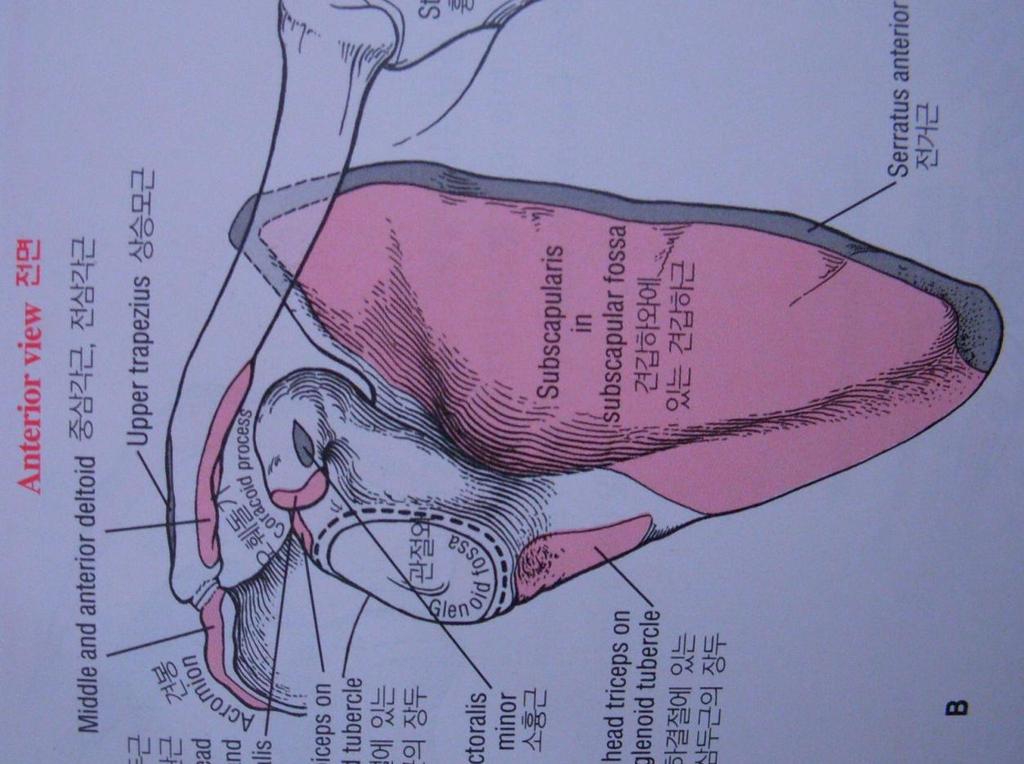
5 Shoulder anatomy(scapula)



6 Shoulder anatomy(humerus) Humeral head Anatomical neck Greater tubercle Intertubercular groove Deltoid tuberosity Superior medial 135 도 30 도 retroversion


7 Shoulder anatomy(gh joint) GHJ- 섬유성관절낭에둘러싸여있다. Synovial sheath- 이두건장두를감싸고내려온다. Axillary pouch- sling Rotator cuff m GH capsular ligament Coracohumeral ligament fix Biceps tendon

8 Shoulder anatomy(gh joint) SGHL adduction, humeral head inferior & posterior translation -> tightness MGHL humeral head anterior translation, ER -> tightness IGHL abduction Axillary pouch 90 abduction -> tightness

9 GHJ Static stability primary stability: glenoid fossa position - static locking mechanism Secondary stability: supurasupinatus Biceps, triceps, detoid EMG 연구결과 - 정적안정성에크게관여하지 X Scapula position & suprasupinatus -> static stability

10 Shoulder anatomy Coracoacromial arch= CAL + acromial process Nomal 1cm Subacromial space - suprarspinatus tendon - subacromial bursa - biceps long head - superior capsular ligament Subacromial bursa - supurasupinatus protect Deltoid bursa - Suprasupinatus & deltoid & humural head protect
 STJ 60 도 = SCJ elevation (30) + ACJ up ro")
11 Shoulder anatomy Scapulo-humeral rhythm 2:1 ratio (GHJ:STJ) STJ 60 도 = SCJ elevation (30) + ACJ up ro (30)

12 Shoulder anatomy SCJ & ACJ cooperation - early 90도 GHJ 60도 abduction + STJ 30도 up ro - terminal 90도 ~180도 GHJ 60도 abduction + STJ 30도 up ro SCJ 20~25 도 elevation v ACJ 5~10 도 up ro SCJ 5 도 elevation ACJ 20~25 도 up ro v



13 Shoulder anatomy SCJ & ACJ cooperation (clavical posterior ro) 40 도 posterior ro CCL stretch Posterior ro
 Global limitation of glenohumeral")

14 Sub-types of Adhesive Capsulitis Idiopathic (Primary) Global limitation of glenohumeral motion secondary to contracture and loss of compliance of the glenohumeral joint capsule.
15 Sub-types of Adhesive Capsulitis Secondary or Acquired Limitation of motion secondary to injury, low-level repetitive trauma, or part of another condition resulting in contracture of structures which contribute to shoulder motion. May be post-traumatic, post-surgical, CVD or from a known systemic illness.
16 Epidemiology of Adhesive Capsulitis Affects about 2% of general population and possibly as high as 3-5% Idiopathic is seen in age group of years. (hormone) Mean age was 50 for both men and women, and IDDM and NIDDM patients Male to Female Ratio of 58:42. Diabetics: affects 10-20%. The incidence in IDDM rises to 36%. Also see bilateral involvement more frequently in DM.
17 Epidemiology of Adhesive Capsulitis Injuries: can develop from a minor incident, rotator cuff strain, impingement syndrome Surgical Trauma: shoulder, axillary node dissection, neck dissection Immobility: the majority of pts referred
18 Epidemiology of Adhesive Capsulitis Cervical Disease: Most common at C5-6 and C6-7. with DDD are more likely to develop stiffness. Thyroid: can have bilateral invovlement and will often resolve with thyroidectomy and stable thyroid levels Cardiac Disease: may be triggered by catheterization of brachial artery or post sternotomy pain Pulmonary: incidence increases with COPD and use of isoniazid Neurologic: CVA(stroke), Parkinsons
19 Schematic painful shoulder musculoskeletal vascular Neurologic Visceral referred vasospasm pain Muscle spasm hypoxia 2 nd vasospasm Diminished Venous return immobilization congestion Fibrous reaction disuse Functional disability


20 Common injury What happened? Repeated microtrauma Loss of the Elastic connective tissue Inflammatory reaction Critical zone Fibroblast damage Traction or compressive force Adhesion result ischemia blood supply degenerative


21 Capsule capacity Normal capsule Adhesive capsulitis
22 Stages of Adhesive Capsulitis Painful Phase: Freezing - high irritability (3~6 month) Progressive Stiffness Phase: Frozen - morderate irritability (3~6 month) Resolution Phase: Thawing - low irritability (6~12 month) - aggressive rehab
23 Painful Phase: Freezing Lasts 3-6 months. Begins with pt having the onset of achy pain. Pain often begins at night and persists through the day. Pain is enough to substantially disturb sleep and will often request meds at night.
24 Painful Phase: Freezing As symptoms progress, fewer arm positions are comfortable and usually is most comfortable with arm at side and internally rotated (sling position). -> Add, IR rest Usually first treatment is to immobilize the arm which only worsens stiffening process. Progresses to constant pain and worse with repetitive movement, stress, exposure to cold or vibration, change in weather. Moderate Tx pain free (mobilization, distraction, self ROM ex, PRICE)
25 Progressive Stiffness: Frozen Lasts 6~12 month but may be much longer. Stiffness progresses so that ROM is lost in all planes. Pain usually less than in freezing stage have inability to sleep comfortably on the affected side. ADLs severely limited: particularly with overhead and behind back motions. Pain continues to decrease, but only within a very limited ROM.
26 Resolution Phase: Thawing Final stage is characterized by slow gains in motion and comfort. May have persistence of symptoms for as long as 6-10 years from onset. May have persistent motion and function restrictions.(disable 20~30%) Resolution TX -> aggressive rehabilitation
27 Night pain?? Abnormal blood circulation Traction effect (daytime) Scapula attach muscle compression Dopamine hormone secretion (daytime) sunbeam Humeral head At translation (supine position) Rest position, Ice ~~~
28 Physical Examination Body condition (drug ) Grade classification - verbally PROM and AROM with solid endpoint feel to endrange motion Posture (stooped, round shoulder, shrug sign) - posture classification (neck) in the future (adjustment) - ACJ & SCJ length discrepancy - humeral head torsion (olecrenon process) - scapula (rest, motion)
29 Physical Examination Six directions for ROM: - Forward elevation/flexion - ER at side and in abduction, - IR in adduction and against the spine. - Cross body Adduction AROM: Flexion measured against thorax to avoid trunk tilt or increased ST contributions. PROM Assessed with pt supine to restrict ST contribution.




30 Physical Examination ASIS ~ greater tuberosity Greater tuberosity ~ lateral epicondyle ACJ ~ medial styloid process Olecrenon process ~ lateral styloid process




31 Physical Examination Olecrenon process ~ lateral styloid process Thumb check Length or angle(??) Involve side, uninvolve side check spread on the records
32 Rehabilitation Painful Phase: Freezing -> pain control period - Rotator cuff m, deltoid m release - GHJ distraction (oscillation) - Joint mobilization (4 shoulder joint) - pain free range -> PNF pattern (passive) - scapula setting ex, multidirection motion (pain free) - correct muscle stretch (neck area), IR, ER isometric ex (??)
33 Rehabilitation Progressive Stiffness Phase: Frozen -> ROM maintain - sling active motion warm up -> multidirection - PNF pattern (passive ~ active motion) end range of motion - MET (PIR) end range - Joint mobilization (4 shoulder joint) - scapula stability ex - rotator cuff passive stretch education IR,ER strengthning (eccentric focus), scaption
34 Rehabilitation Resolution Phase: Thawing - aggressive rehab - GHJ multiful joint mobilization (inferior, Ant, post, IR, ER) - Isotonic eccentric MET - PNF pattern (eccentric) - end range stretch (low intensity, long time) - self PA, AA stretch (T bar, pully) over end range * connective tissue -> permanent stretch
35
36 Discussion Joint capsule release technique -> application?? - PNF, MET, JM, ART, PRT Capsular pattern Tx?? - flex, abd, ER, IR (normal) - ER, abd, flex, add, IR (parker) - abd, flex, ER, IR (Hill, Bogumill) - scapula plane (flex, ER, abd), IR Strangth (isometric, isotonic- con,ecc) -> application??
Returning the Shoulder Back to Optimal Function. Scapula. Clavicle. Humerus. Bones of the Shoulder (Osteology) Joints of the Shoulder (Arthrology)
 Joints of the Shoulder (Arthrology)") Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
Shoulder: Clinical Anatomy, Kinematics & Biomechanics
 Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
Structure and Function of the Bones and Joints of the Shoulder Girdle
 Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson
 Dr. Carson") REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Rotator Cuff Conditioning Exercises with th i R ck Kaselj, MS ck K Rick Kaselj Exercises
 Rotator Cuff Conditioning Exercises with Rick Kaselj, MS Before I Start Recording - Webinar will be recorded - I will send you details on how to access the video tomorrow - Tour of Things / Questions:
Rotator Cuff Conditioning Exercises with Rick Kaselj, MS Before I Start Recording - Webinar will be recorded - I will send you details on how to access the video tomorrow - Tour of Things / Questions:
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer
 Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION)
(+/- SUBACROMIAL DECOMPRESSION)") REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
Tendinosis & Subacromial Impingement Syndrome. Gene Desepoli, LMT, D.C.
 Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR
 REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
OrthoCarolina. Arthroscopic SLAP Lesion (Type II) Repair Protocol
 Repair Protocol") OrthoCarolina Arthroscopic SLAP Lesion (Type II) Repair Protocol Surgical Overview: SLAP, which stands for superior labrum anterior to posterior, lesions are labral detachments that originate posterior
OrthoCarolina Arthroscopic SLAP Lesion (Type II) Repair Protocol Surgical Overview: SLAP, which stands for superior labrum anterior to posterior, lesions are labral detachments that originate posterior
Latissimus Dorsi Transfer
 Latissimus Dorsi Transfer 1. Defined a. Transfer of the latissimus dorsi from it insertion anteriorly on the proximal humeral shaft to a superior and posterior insertion on the humeral head in the subacromial
Latissimus Dorsi Transfer 1. Defined a. Transfer of the latissimus dorsi from it insertion anteriorly on the proximal humeral shaft to a superior and posterior insertion on the humeral head in the subacromial
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines
 Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
- I know people are busy and will do all I can to wrap up on time - CEC I will submit it for CEC -Send me your feedback - Helps improve the webinars
 Rotator t Cuff Conditioning i Exercises with Rick Kaselj, MS Before I Start Recording - Webinar will be recorded - I will send you details on how to access the video tomorrow - Tour of Things / Questions:
Rotator t Cuff Conditioning i Exercises with Rick Kaselj, MS Before I Start Recording - Webinar will be recorded - I will send you details on how to access the video tomorrow - Tour of Things / Questions:
PHASE I (Begin PT 3-5 days post-op) DOS:
 DOS:") REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT
 REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
MASSIVE ROTATOR CUFF REPAIR. REHABITATION PROTOCOL >3 cm
 MASSIVE ROTATOR CUFF REPAIR REHABITATION PROTOCOL >3 cm Phase I: (Protective Phase) Weeks 0 to 8 Goals: Minimize pain and inflammatory response Achieve ROM goals Establish stable scapula 1. Elbow, wrist
MASSIVE ROTATOR CUFF REPAIR REHABITATION PROTOCOL >3 cm Phase I: (Protective Phase) Weeks 0 to 8 Goals: Minimize pain and inflammatory response Achieve ROM goals Establish stable scapula 1. Elbow, wrist
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers
 Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Shoulder Injury Evaluation.
 Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
Core deconditioning Smoking Outpatient Phase 1 ROM Other
 whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair
 Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair
 THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair **It is important for the clinician to determine the capsular response to the heat probe. Patients that have excessive ROM early in the rehab
THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair **It is important for the clinician to determine the capsular response to the heat probe. Patients that have excessive ROM early in the rehab
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Arthroscopic Anterior Stabilization Rehab
 Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
SHOULDER JOINT ANATOMY AND KINESIOLOGY
 SHOULDER JOINT ANATOMY AND KINESIOLOGY SHOULDER JOINT ANATOMY AND KINESIOLOGY The shoulder joint, also called the glenohumeral joint, consists of the scapula and humerus. The motions of the shoulder joint
SHOULDER JOINT ANATOMY AND KINESIOLOGY SHOULDER JOINT ANATOMY AND KINESIOLOGY The shoulder joint, also called the glenohumeral joint, consists of the scapula and humerus. The motions of the shoulder joint
Rehabilitation Guidelines for Shoulder Arthroscopy
 Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
UNDERSTANDING YOUR SHOULDERS
 It is a widely known fact that the shoulder is one of the body s most mobile joints. Unfortunately this mobility comes at a cost. With its high degree of mobility, stability is often compromised. This
It is a widely known fact that the shoulder is one of the body s most mobile joints. Unfortunately this mobility comes at a cost. With its high degree of mobility, stability is often compromised. This
Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries)
") Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries) All information contained in this protocol is to be used as general
Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries) All information contained in this protocol is to be used as general
Chronic Shoulder Disorders
 Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
MUSCLES OF SHOULDER REGION
 Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
SLAP Lesion Type II Repair Rehabilitation Program
 SLAP Lesion Type II Repair Rehabilitation Program The GLSM SLAP Type II Repair Rehabilitation Program is an evidence-based and soft tissue healing dependent program allowing patients to progress to vocational
SLAP Lesion Type II Repair Rehabilitation Program The GLSM SLAP Type II Repair Rehabilitation Program is an evidence-based and soft tissue healing dependent program allowing patients to progress to vocational
Large/Massive Rotator Cuff Repair
 Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T
 J O I N T") THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
Rehab protocol. Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits. Goals:
 Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
UPPER EXTREMITY INJURIES. Recognizing common injuries to the upper extremity
 UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
Latarjet Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Small Rotator Cuff Repair
 Small Rotator Cuff Repair 1. Defined a. Surgical repair of the rotator cuff (most commonly supraspinatus muscle) utilizing sutures b. May be done arthroscopically or open. c. May be done in conjunction
Small Rotator Cuff Repair 1. Defined a. Surgical repair of the rotator cuff (most commonly supraspinatus muscle) utilizing sutures b. May be done arthroscopically or open. c. May be done in conjunction
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft
 Day of Surgery Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft A. Relax. Diet as tolerated. B. Icing is important for the first 5-7 days post-op. While the post-op
Day of Surgery Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft A. Relax. Diet as tolerated. B. Icing is important for the first 5-7 days post-op. While the post-op
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Reverse Total Shoulder Arthroplasty Protocol
 General Information: Reverse Total Shoulder Arthroplasty Protocol Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH) arthritis when it
General Information: Reverse Total Shoulder Arthroplasty Protocol Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH) arthritis when it
7/31/2012 THE SHOULDER JOINT CLARIFICATION OF TERMS OSTEOLOGY OF THE GH JOINT(BONES)
") THE SHOULDER JOINT T H E G L E N O H U M E R AL ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumerual joint) = scapula and Lippert, p115 OSTEOLOGY
THE SHOULDER JOINT T H E G L E N O H U M E R AL ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumerual joint) = scapula and Lippert, p115 OSTEOLOGY
Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity
 Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity Sheldon C. Yao, D.O. Acting Department Chair March 1, 2013 Clinical significance Upper extremity
Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity Sheldon C. Yao, D.O. Acting Department Chair March 1, 2013 Clinical significance Upper extremity
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE I TEARS (+/- SUBACROMINAL DECOMPRESSION)
") REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE I TEARS (+/- SUBACROMINAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames are
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE I TEARS (+/- SUBACROMINAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames are
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Rehabilitation of Overhead Shoulder Injuries
 Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD
 General Information: Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH)
General Information: Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH)
OBJECTIVES. Therapists Management of Shoulder Instability SHOULDER STABILITY SHOULDER STABILITY WHAT IS SHOULDER INSTABILITY? SHOULDER INSTABILITY
 Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Shoulder Arthroscopy with Posterior Labral Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Scapular and Deltoid Regions
 M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
Joint Range of Motion Assessment Techniques. Presentation Created by Ken Baldwin, M.Ed Copyright
 Joint Range of Motion Assessment Techniques Presentation Created by Ken Baldwin, M.Ed Copyright 2001-2006 Objectives Understand how joint range of motion & goniometric assessment is an important component
Joint Range of Motion Assessment Techniques Presentation Created by Ken Baldwin, M.Ed Copyright 2001-2006 Objectives Understand how joint range of motion & goniometric assessment is an important component
ORTHOPEDIC AND SPORTS MEDICINE CENTER
 ORTHOPEDIC AND SPORTS MEDICINE CENTER SPORTS MEDICINE DIVISION COMBINED REHAB PROTOCOLS AAMC ORTHOPEDIC AND SPORTS MEDICINE SPECIALISTS Office: (410) 268-8862 Fax: (410) 268-0380 Rotator Cuff Repair Rehab
ORTHOPEDIC AND SPORTS MEDICINE CENTER SPORTS MEDICINE DIVISION COMBINED REHAB PROTOCOLS AAMC ORTHOPEDIC AND SPORTS MEDICINE SPECIALISTS Office: (410) 268-8862 Fax: (410) 268-0380 Rotator Cuff Repair Rehab
Recurrent Shoulder Dislocation.
 Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Acromioplasty. Surgical Indications and Considerations
 1 Acromioplasty Surgical Indications and Considerations Anatomical Considerations: Any abnormality that disrupts the intricate relationship within the subacromial space may lead to impingement. Both intrinsic
1 Acromioplasty Surgical Indications and Considerations Anatomical Considerations: Any abnormality that disrupts the intricate relationship within the subacromial space may lead to impingement. Both intrinsic
REMINDER. Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns
 Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair
 Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair General Information Frozen shoulder is a condition where the shoulder joint (glenohumeral joint) gradually becomes stiff, resulting in
Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair General Information Frozen shoulder is a condition where the shoulder joint (glenohumeral joint) gradually becomes stiff, resulting in
Type II SLAP lesions are created when the biceps anchor has pulled away from the glenoid attachment.
 Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Reverse Total Shoulder Protocol
 Marion Herring, M.D. OrthoVirginia PH: (804) 270-1305 FX: (804) 273-9294 www.orthovirginia.com Reverse Total Shoulder Protocol General Information: Reverse Total Shoulder Arthroplasty (rtsa) is designed
Marion Herring, M.D. OrthoVirginia PH: (804) 270-1305 FX: (804) 273-9294 www.orthovirginia.com Reverse Total Shoulder Protocol General Information: Reverse Total Shoulder Arthroplasty (rtsa) is designed
Anatomy of the Shoulder Girdle. Prof Oluwadiya Kehinde FMCS (Orthop)
") Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Hemiplegic Shoulder Power Point for staff education sessions
 Appendix B Hemiplegic Shoulder Power Point for staff education sessions Jennifer Curry Physiotherapist, London Health Sciences Centre www.swostroke.ca Acknowledgements Maria Lung BSc (PT), MSc Train the
Appendix B Hemiplegic Shoulder Power Point for staff education sessions Jennifer Curry Physiotherapist, London Health Sciences Centre www.swostroke.ca Acknowledgements Maria Lung BSc (PT), MSc Train the
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA
 Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Alternative Therapies for Adhesive Capsulitis: A Case Study LANIE ALPHIN
 Alternative Therapies for Adhesive Capsulitis: A Case Study LANIE ALPHIN Case Background 53 year old female Chief Complaint: Right shoulder pain for 6 months Diagnosis: Adhesive Capsulitis Imagining indicated
Alternative Therapies for Adhesive Capsulitis: A Case Study LANIE ALPHIN Case Background 53 year old female Chief Complaint: Right shoulder pain for 6 months Diagnosis: Adhesive Capsulitis Imagining indicated
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Evaluation of the Knee and Shoulder
 Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Rotator Cuff Repair Protocol
 Rotator Cuff Repair Protocol Applicability: Physician Practices Date Effective: 11/2016 Department: Rehabilitation Services Supersedes: Rotator Cuff Repair (Beattie) Date Last Reviewed / or Date Last Revision:
Rotator Cuff Repair Protocol Applicability: Physician Practices Date Effective: 11/2016 Department: Rehabilitation Services Supersedes: Rotator Cuff Repair (Beattie) Date Last Reviewed / or Date Last Revision:
(PROTOCOL #18) REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL
 REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL") The following is a set of general guidelines. It is important to remember that each patient is different. The progression of the patient depends on many factors including age and medical health of the
The following is a set of general guidelines. It is important to remember that each patient is different. The progression of the patient depends on many factors including age and medical health of the
SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations
 SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations Meagan Pehnke, MS, OTR/L, CHT, CLT March 1 st, 2019 Philadelphia Surgery & Rehabilitation of the Hand: Pediatric Pre-course OUTLINE Discuss
SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations Meagan Pehnke, MS, OTR/L, CHT, CLT March 1 st, 2019 Philadelphia Surgery & Rehabilitation of the Hand: Pediatric Pre-course OUTLINE Discuss
Breakout Session #7: Manual therapy for shoulder pain and limited mobility
 Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck.
 and lower lateral neck.") Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck. includes Pectoral Scapular Deltoid regions of the upper limb
Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck. includes Pectoral Scapular Deltoid regions of the upper limb
IP: Sling for 6 weeks Week 0-6: Immobilisation + Pendulum exercise Week 6-4 Months: Active ROM 4 Months-on: Strengthening exercises
 Supplemental material 5 Table 1. Summary of rehabilitation programs postoperative. Author (year) Early Rehabilitation Conservative Rehabilitation Arndt et al., 2012 [35] First day postoperative-week 6:
Supplemental material 5 Table 1. Summary of rehabilitation programs postoperative. Author (year) Early Rehabilitation Conservative Rehabilitation Arndt et al., 2012 [35] First day postoperative-week 6:
Aquatic Exercise. Rehabilitation after the SLAP lesion repair. I. Anatomy & Function SLAP 의가장흔한손상기전. Anatomy of the Shoulder (I)
") Aquatic Exercise Rehabilitation after the SLAP lesion repair Sports Medicine Clinic Sky 임승길 ATC 2 SLAP 의가장흔한손상기전 SLAP Superior Labrum Anterior to Posterior 1. Compression force Attempting to catch a heavy
Aquatic Exercise Rehabilitation after the SLAP lesion repair Sports Medicine Clinic Sky 임승길 ATC 2 SLAP 의가장흔한손상기전 SLAP Superior Labrum Anterior to Posterior 1. Compression force Attempting to catch a heavy
No Financial Disclosures
 Rehabilitation Following Total and Reverse Shoulder Arthroplasty, PT, DPT, SCS, CSCS No Financial Disclosures Total Shoulder Arthroplasty Arthritic shoulder increasing in prevalence More active as we age
Rehabilitation Following Total and Reverse Shoulder Arthroplasty, PT, DPT, SCS, CSCS No Financial Disclosures Total Shoulder Arthroplasty Arthritic shoulder increasing in prevalence More active as we age
The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery. Phase 1: Immediate postoperative period (weeks 0-6) Goals
 Goals") The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery Phase 1: Immediate postoperative period (weeks 0-6) Maintain/protect integrity of repair Gradually increase PROM Diminish
The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery Phase 1: Immediate postoperative period (weeks 0-6) Maintain/protect integrity of repair Gradually increase PROM Diminish
C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center
 Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center A 65-year-old
Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center A 65-year-old
Shoulder Biomechanics
 Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Rehabilitation Guidelines for Arthroscopic Capsular Shift
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Arthroscopic Capsular Shift The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee.
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Arthroscopic Capsular Shift The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee.
Patient ID. Case Conference. Physical Examination. Image examination. Treatment 2011/6/16
 Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Work-related shoulder pain
 Work-related shoulder pain Stadler Kirsten M.B., Ch.B. (1987) (Pret), M. Med. (Orthop) (1998) (Stell.), Orthopaedic Surgeon, Room 333, Louis Leipoldt Medical Centre, Broadway Street, Bellville Cape Town
Work-related shoulder pain Stadler Kirsten M.B., Ch.B. (1987) (Pret), M. Med. (Orthop) (1998) (Stell.), Orthopaedic Surgeon, Room 333, Louis Leipoldt Medical Centre, Broadway Street, Bellville Cape Town
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood
 Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
I (and/or my co-authors) have something to disclose.
 have something to disclose.") Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Gross Anatomy Questions That Should be Answerable After October 27, 2017
 Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
ANTERIOR OPEN CAPSULAR SHIFT REHABILITATION PROTOCOL (Accelerated - Overhead Athlete)
") ANTERIOR OPEN CAPSULAR SHIFT REHABILITATION PROTOCOL (Accelerated - Overhead Athlete) This rehabilitation program's goal is to return the patient/athlete to their activity/sport as quickly and safely as
ANTERIOR OPEN CAPSULAR SHIFT REHABILITATION PROTOCOL (Accelerated - Overhead Athlete) This rehabilitation program's goal is to return the patient/athlete to their activity/sport as quickly and safely as
4/12/2016. Goals. Anatomy. Basic Anatomy. Biomechanics. Function. Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management
 Goals Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management Thomas F. LaPorta, MD To understand the anatomy of the biceps at the shoulder To present the mechanism, signs and symptoms,
Goals Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management Thomas F. LaPorta, MD To understand the anatomy of the biceps at the shoulder To present the mechanism, signs and symptoms,
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction. Rarely does a single muscle act in isolation at the shoulder complex.
 Shoulder complex 1 Introduction Our study of the upper limb begins with the shoulder complex, a set of four articulations involving the sternum, clavicle, ribs, scapula, and humerus. Rarely does a single
Shoulder complex 1 Introduction Our study of the upper limb begins with the shoulder complex, a set of four articulations involving the sternum, clavicle, ribs, scapula, and humerus. Rarely does a single