6/11/2015. MRI Arthroscopy Correlations: Rotator Cuff. Disclosures. Biomet, Inc Consulting and Speaking. Case #1
|
|
|
- Stuart Butler
- 6 years ago
- Views:
Transcription

1 6/11/2015 MRI Arthroscopy Correlations: Rotator Cuff Disclosures Biomet, Inc Consulting and Speaking Case #1 1


2 6/11/2015 Case #1 45 y/o RHD male s/p fall from ladder 3mos ago Pain at night and with overhead motions in R shoulder Failed PT PE: Full ROM 4/5 SS, 5/5 ER, Neg Belly Case #1 Case #1 2


3 6/11/2015 Case #1 Case #1 Case #2 3


4 6/11/2015 Case #2 48 y/o RHD female s/p motorcycle accident 4 weeks ago Dislocated R shoulder, reduced in ER Pain and dysfunction PE: FF 110, large shrug 3/5 SS, 4/5 ER, Neg Belly Case #2 Case #2 4




5 6/11/2015 Case #2 Mobilize Tendon Bursal -> Scapular Spine Articular -> Capsule- Labral Junction Carefule to avoid suprascapular nerve. Case #2 Anchors placed at articular margin through percutaneous incision lateral to acromion Case #2 Work away from where you are retrieving sutures 5

 Alternate colors of sutures")
6 6/11/2015 Case #2 Case #2 Pearls History and fatty infiltration dictate repairability Adequate mobilization Percutaneous portal for anchor Use penetrator for far posterior Use suturing device for superior Work away from retrieving portal (ie, if retrieving through anterior portal, then pass anterior to posterior) Alternate colors of sutures Case #2 6

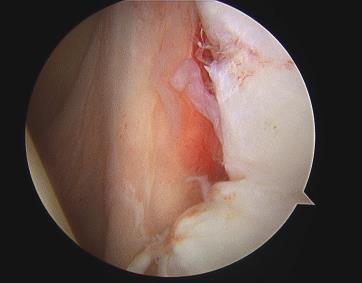
7 6/11/2015 Case #3 Case #3 58 RHD male s/p fall down stairs 2 months ago. Pain and dysfunction in R shoulder PE: FF 150, with shrug 4/5 SS, 5/5 ER, Pos Belly Case #3 7




8 6/11/2015 Case #3 Case #3 Case #3 External Rotation, Forward Flexion allows familiar view 8





9 6/11/2015 Case #3 270 degree release of subscapularis Superior base of coracoid Posterior MGHL/capsule Anterior Conjoint to axillary nerve Keep lateral interval tissue intact Case #3 Anterosuperior Tears 9
10 6/11/2015 Case #3 Pearls Arm Position External rotation to pass Internal rotation to tie Forward flexion to see Penetrator for far anterior Maintain Integrity of the Cuff Case #3 Case #4 10




11 6/11/2015 Case #4 72 RHD male with R shoulder pain, no trauma. Good but temporary relief from cortisone 3 months of PT Function OK PE: ROM 170/45/T12 4/5 SS, 4/5 ER, Pos Belly Case #4 Case #4 11


12 6/11/2015 Case #4 Summary Fatty infiltration biggest indicator of ability to repair. Head may be elevated on MRI with acute massive tears -> doesn t mean you can t repair it. Have a methodical system for repair, maintain cuff. If unable to repair, and function is adequate pre-op, then partial, margin convergence repair can be effective at pain relief. Thank You 12


13 6/8/2015 IMAGING OF THE ROTATOR CUFF AND BICEPS LABRUM COMPLEX Gabrielle P. Konin, MD Department of Imaging Hospital for Special Surgery Assistant Professor of Radiology Weill Medical College of Cornell University Financial Disclosures I have nothing to disclose. TENDINOPATHY Tendons are intact Increased signal on short TE Intermediate signal on long TE (not fluid signal) Alteration in tendon size or morphology 1





14 6/8/2015 HADD 60 year-old man with anterior pain for 1 month. No trauma. Intraosseous HADD can have an intense marrow edema pattern and may be confused for tumor or greater tuberosity fracture. IMPINGEMENT SYNDROME Assessment of Secondary Signs Acromial morphology: anterior +/- lateral subacromial spur / slope of acromion CA ligament thickening Tendinopathy Partial Tear Lateral downsloping of the acromion. Tendinosis with bursal fraying and intrasubstance fissuring at critical zone. Synovitis of the subacromial space. 2











15 6/8/2015 IMPINGEMENT SYNDROME Assessment of Secondary Signs AC joint arthrosis Os acromiale Partial Thickness Footprint Tear Partial thickness tendon discontinuity Increased signal intensity on moderate to long TE sequences Bursal vs. articular vs. intrasubstance Intrasubstance / concealed tears - invisible to scope Sept 2014 Nov year old pitcher with intrasubstance footprint tear 3











16 6/8/2015 Sentinel ganglion cyst Sentinel cyst without evidence of tear indicates prior delaminating intrasubstance tear. Interstitial fluid extension between layers of rotator cuff. Typical location is posterior supraspinatus. Partial tear of the subscapularis tendon FULL THICKNESS TEAR Acute tear Failure with continuity 4
")




17 6/8/2015 FULL THICKNESS RE-TEAR CHRONIC ROTATOR CUFF TEAR Superior migration AH interval (<7mm) Remodeling of acromion Assess tendon quality & degree of retraction for repair *Assess quality of muscle: predictor of outcome Assess articular cartilage CUFF TEAR ARTHROPATHY Chronic rotator cuff tear Anterosuperior migration of humerus Acromial acetabularization Coracoacromial ligament stabilizes progressive superior migration Osteoarthrosis: apron osteophyte, loose bodies Assess glenoid Deltoid dehiscence 5








18 6/8/2015 Classification of SLAP lesions (Snyder et al 1990) I : Labral and biceps fraying, intact anchor II : Labral fraying with stripping of both the labrum and biceps III : Bucket handle tear with displacement and intact biceps anchor IV: Same as III, but with detached biceps anchor Stripping of the labrum and biceps SLAP II 22 year-old NBA player with shoulder pain Chronic stripping of the labrum and biceps anchor 6














19 6/8/ year-old man with pain for 1-2 months Stripping of the anterosuperior labrum with intact anchor and displacement of the labrum into the joint 47 year-old tennis player. Stripping of labrum & biceps anchor w tear extension into biceps 7



20 6/8/ year-old 4 days post diving accident. Near complete detachment of the biceps anchor Thank you 8




21 6/15/2015 MRI : Biceps Chondromalacia? Disclosure Neither I, Stephen J. O Brien, MD, MBA, nor any family member(s), author(s), have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated with or without recognition within the presentation. The Role of MRI in Diagnosing Biceps Chondromalacia Mary E Shorey BA Samuel A Taylor MD Joshua A Dines MD Hollis Potter MD Joe Nguyen MPH Stephen J O'Brien MD MBA 1







22 6/15/2015 Nothing New Under The Sun... Sisterman - "Biceps Footprint" Castagna - "Chondral Imprints" Kuhn et al - "Humeral Head Abrasions" Appeared that BCM Lesions COULD BE Seen on MRI, Especially COR PD. Normal "Blush" Two Types of BCM 2
 Pain had Multiple Sites Of Pain and Pathology")

BLC Lesions WithVisible BCM (34pts) 2)BLC Lesions Without Visible BCM (21pts) 3)Control Group Instability Surgery")
 Digital OR Pictures Only Single Experienced Sports MRI radiologist (HP)- blinded of any")
23 6/15/2015 Which is the Pain Generator? O'Brien et al- 280 Pts 70% of Pts with Biceps Labral Complex (BLC) Pain had Multiple Sites Of Pain and Pathology Which is the Pain Generator? O'Brien et al- 3 "Pack" 145 Pts prospective "Groove" "Junction" "Deep Inside" Materials and Methods Retrospective Review- 3 Groups - All MRI's at HSS- Pts with OA EXCLUDED. 1)BLC Lesions WithVisible BCM (34pts) 2)BLC Lesions Without Visible BCM (21pts) 3)Control Group Instability Surgery w/o BLC SXS (29pts) Groups 1&2 Age Matched (Mean Age 42). Group 3 (Mean age 29) Digital OR Pictures Only Single Experienced Sports MRI radiologist (HP)- blinded of any clinical data or OR Photos MRI CRITERIA Major 1) Loss of ARTICULAR Cartilage where LHBT traverses 2) Subchondral Signal Change 3) Abnormal Signal in Proximal LHBT Minor 4) Labral Tear 5) Scarring in Rotator Interval 6) Evidence of more global Adhesive Capsulitis Statistical Analysis by Biostatistician 3



24 6/15/2015 Group 1 Cartilage Loss- 85% Subchondral Signal Changes - 64% Pathological Changes Proximal LHBT- 85% Results Group 2 Cartilage Loss- 86% Subchondral Signal Changes - 52% Pathological Changes Proximal LHBT- 81% Group 3 Cartilage Loss- 51% Subchondral Signal Changes - 34% Pathological Changes Proximal LHBT- 44% Results Within the Boundaries of this Analysis (younger) Cohort, Age was not a factor in the presence or absence of a BCM Lesion or the ability of the MRI to Diagnose It. Diagnostic Statistics 4





25 6/15/2015 Biceps Chondromalacia "Medial" 5




26 6/15/2015 Thank you 6



27 MRI / Arthroscopy Correlation: SHOULDER INSTABILITY Stephen F. Brockmeier, MD Sports Medicine & Shoulder Surgery Associate Professor, Orthopaedic Surgery University of Virginia Team Physician, UVA Athletics Cree M. Gaskin, MD Vice-Chair, Radiology Associate Professor, Radiology and Orthopaedic Surgery University of Virginia Charlottesville, VA SFB: Disclosure Consultant: Biomet, MicroAire Medical Education: Biomet, Arthrex Royalties, Springer Publishing Research Grant: Arthrex, Tornier, Biomet Fellowship Support Grant: Arthrex, Depuy Mitek, DJO CMG: Consultant, Depuy Mitek Royalties, Oxford University Press Royalties, Thieme Medical Publishing 1


28 CASE #1 Case #1 19 yo collegiate football player Injured making a tackle Pain / Recurrent subluxation Unable to continue to play Exam: Pain / apprehension in ABER Positive Jobe relocation Rotator cuff exam WNL Positive active compression 2
29 MRI Diagnosis? 3



30 Labral Tear (Bankart) & Chondral Injury NORMAL Sag T2 Fat Sat 4


31 Axial Sag T2 Fat Sat Anterior-Inferior Labrum Generally occurs due to anterior instability SEMANTICS: Bankart - generic term Perthes ALPSA GLAD Artwork of Salvador Beltran. From: Stoller DW. MRI, Arthroscopy, and Surgical Anatomy of the Joints. Lippincott Publishers. 5


32 Perthes Lesion Axial T2 Fat Sat Perthes Lesion Axial T2 Fat Sat 6





33 ALPSA lesion Anterior labroligamentous periosteal sleeve avulsion Periosteum stripped, but not disrupted Displaced when scars down to glenoid Axial T1 ALPSA lesion Axial T1 7

34 ALPSA lesion Axial T1 ALPSA lesion Axial T1 8


35 ALPSA lesion Axial T1 ALPSA lesion Coronal T1 FS 9


36 Coronal T2 FS ALPSA lesion Sag T2 Fat Sat 10




37 ALPSA lesion Sag T2 Fat Sat ALPSA lesion 11




38 GLAD Glenolabral Articular Disruption Ant-inf chondral defect + superficial labral tear Often applied to other glenoid sites Modified artwork of Salvador Beltran. From: Stoller DW. MRI, Arthroscopy, and Surgical Anatomy of the Joints. Lippincott Publishers. GLAD 12




39 Case #1: Arthroscopic Photos Arthroscopic Anterior Stabilization Beach chair vs. lateral 13


40 Arthroscopic Anterior Stabilization Beach chair vs. lateral Low anterior portal Mobilization Stimulate healing response Arthroscopic Anterior Stabilization Beach chair vs. lateral Low anterior portal Mobilization Stimulate healing response Translate tissue medial and superiorly 14


41 Arthroscopic Anterior Stabilization Beach chair vs. lateral Low anterior portal Mobilization Stimulate healing response Translate tissue medial and superiorly 3 anchors, minimum Arthroscopic Anterior Stabilization Beach chair vs. lateral Low anterior portal Mobilization Stimulate healing response Translate tissue medial and superiorly 3 anchors, minimum Bumper?? 15


42 CASE #2 Case #2 29 yo Ortho Resident Former Kickboxer / MMA Many years of recurrent shoulder dislocations (>10) Now comes out with minimal trauma No prior surgeries On exam: Apprehension at 90 & 45 degrees 16


43 Plain Films MRI 17
 Humeral: 93 100% (recurrent instability) Combined:")
44 Diagnosis? Evolving Algorithm Epidemiology Clinically relevant bone loss clearly underappreciated Glenoid: 49 86% (recurrent instability) Humeral: % (recurrent instability) Combined: Almost always some combined deficiency Presentation Mechanism (axial load) Acute vs. Chronic Easy to come out; Easy to reduce Instability mid-range Failed prior sx 18

45 19
46 20
47 21
48 22

49 23
50 24
51 25


52 26


53 27
54 28


55 Diagnostic Scope 29





56 Technique Beach chair position Articulated arm positioner Axillary incision No paralysis Postop regional block EUA Diagnostic Scope Technique Subscap split (2/3 rd s down the tendinous portion) Arm in IR for the majority of the case 3/32 nd pin for superior retraction Careful retraction medially No retraction inferiorly 30




57 Technique Intra-op Fluoro 31





58 Technique Postop Films 32

59 CASE #3 Case #3 27 yo male, outdoor enthusiast Posterior shoulder pain 8 months duration Injury bench pressing Exam: Pain with jerk test 33
60 T1 T2 Fat Sat Diagnosis? 34




61 Diagnosis = Posterior Labral Tear w/ Paralabral Cyst Axial T2 FS Sag T2 FS Sag T2 FS Axial T1 FS Companion case: Post. labral tear 35




62 Companion case Axial T2 Fat Sat Suprascapular nerve 36



63 Posterior Labral Tear w/ Paralabral Cyst Cyst Decompression & Labral Repair 37





64 Companion Case: 30 yo laborer, 3 months severe posterior shoulder pain Axial T2 Fat Sat Axial T1 Sagittal T2 fat sat Sagittal T1 Sagittal T2 fat sat 38




65 Cyst Decompression, Post. Labral Repair Additional Companion Case: 19yo D1 Offensive Lineman, Prior Failed AS Posterior Stabilization 39



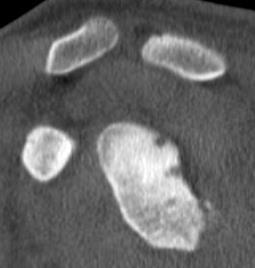
66 MRI CT SCAN 40


67 CT SCAN CT SCAN 41





68 Arthroscopic Findings OPEN OC ALLOGRAFT 42


69 FRESH DISTAL TIBIA OC ALLOGRAFT OPEN OC ALLOGRAFT 43



70 OPEN OC ALLOGRAFT POSTERIOR DTA 44




71 Post-op Xrays (6 weeks) THANK YOU 45
72 MRI Arthroscopy Correlations in the Throwing Shoulder Seth Gamradt, MD Director of Orthopaedic Athletic Medicine Associate Professor Orthopaedic Surgery and Sports Medicine Keck School of Medicine of USC University of Southern California SUMMARY APPROACH TO SHOULDER PHASES OF THROWING PATHOPHYSIOLOGY MRI CORRELATIONS SLAP PARTIAL THICKNESS RC TEARS GIRD INSTABILITY GENERAL APPROACH TO SHOULDER PATIENT < 30 = INSTABILITY AND LABRAL TEARS IMPINGEMENT AND TENDONITIS 60+ ROTATOR CUFF AND ARTHRITIS THROWER 1

73 Phases of Throwing Stage I Windup Stage II Early cocking Stage III Late cocking Shoulder ER increases from (92N-m of Torque) Stage IV Accleration Internal rotation (80 degrees) and adduction of the humerus with rapid elbow extension Terminates with ball release Stage V - Follow-through Dissipation of excess kinetic energy Eccentric cuff contraction and posterior capsule absorbs 100 percent or more body weight. Wind-up Wind-up 2 2
74 Cocking Late Cocking Late Cocking Early Acceleration 3
75 Ball Release Follow Through Follow Through 2 4
76 WHY DOES THE SHOULDER GET INJURED RAPID KINETIC CHAIN CORE----SHOULDER ELBOW----HAND 7000 DEG/SEC OF ROTATIONAL VELOCITY OF THE SHOULER EX ROT OF UP TO 170 DEG NORMAL ADAPTATIONS ER IR Arc is the same but shifted into ER INCREASE IN HUMERAL RETROVERSION ANTERIOR LAXITY MAKE SURE YOUR TREATMENT DOES NOT RUIN WHAT MAKES THIS SHOULDER GOOD FOR PITCHING! THROWING THEORIES--OLDER BENNETT TRACTION ON POSTERIOR GLENOID NEER SUBACROMIAL IMPINGEMENT JOBE ANTERIOR INSTABILITY 5



77 THROWING THEORIES GIRD GLENOHUMERAL INTERNAL ROTATION DEFICIT INTERNAL IMPINGMENT CUFF/LABBRUM CONTACT IN ABER SCAPULAR DYSKINESIS KINETIC CHAIN WEAKNESS IN LEG/TRUNK REQ 15%-40% INCR IN SHOULDER ROTATIONAL VELOCITY MRI-ARTHROSCOPY CORRELATIONS REHAB SHOULD ALWAYS BE THE FIRST OPTION EXCEPTION IS ACUTE TRAUMA MRI-ARTHROSCOPY CORRELATIONS THROWERS HAVE MRI ABNORMALITIES WITH OR WITHOUT SYMPTOMS LESNIAK ET AL AJSM 2013 CONNOR ET AL AJSM 2003 MINIACI AJSM 2002 MULTIPLE STUDIES SHOW LABRUM AND CUFF ABNORMALITIES IN ASYMPTOMATIC PITCHERS OPERATE ON THE PATIENT NOT THE MRI. 6



78 CASE 1: SLAP 20M CASE 1: SLAP 20M CASE 2: GIRD SLAP--PTRCT 25M 7



79 CASE 2: GIRD SLAP--PTRCT 25M CASE 2: GIRD SLAP--PTRCT 25M CASE 3: PTRCT--REPAIR 20M 8







80 CASE 3: PTRCT--REPAIR 20M CASE 4: INSTABILITY 22M CASE 4: INSTABILITY 22M 9
81 SUMMARY LATE COCKING EARLY ACCELERATION STRESSES SHOULDER AND ELBOW MULTIPLE PATHOPHYSIOLOGIC THEORIES GIRD/INTERNAL IMPINGEMENT PTRCT/SLAP SCAPULA/KINETIC CHAIN MRI ABNORMALITIES COMMON REHAB FIRST IF SURGERY DON T TIGHTEN 10
MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging
 MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging MRI of the Shoulder Benefits of Ultrasound: * Dynamic * Interactive real time
MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging MRI of the Shoulder Benefits of Ultrasound: * Dynamic * Interactive real time
MRI SHOULDER WHAT TO SEE
 MRI SHOULDER WHAT TO SEE DR SHEKHAR SRIVASTAV Sr. Consultant- Knee & Shoulder Arthroscopy Sant Parmanand Hospital Normal Anatomy Normal Shoulder MRI Coronal Oblique Sagital Oblique Axial Cuts Normal Coronal
MRI SHOULDER WHAT TO SEE DR SHEKHAR SRIVASTAV Sr. Consultant- Knee & Shoulder Arthroscopy Sant Parmanand Hospital Normal Anatomy Normal Shoulder MRI Coronal Oblique Sagital Oblique Axial Cuts Normal Coronal
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases
 Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases Mary Lloyd Ireland, M.D. University of Kentucky Dept. of Orthopaedic Surgery & Sports Medicine Lexington, KY Broken screw s/p Bristow procedure
Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases Mary Lloyd Ireland, M.D. University of Kentucky Dept. of Orthopaedic Surgery & Sports Medicine Lexington, KY Broken screw s/p Bristow procedure
R. Frank Henn III, MD. Associate Professor Chief of Sports Medicine Residency Program Director
 R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director Disclosures No financial relationships to disclose 1. Labral anatomy 2. Adaptations of the throwing shoulder
R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director Disclosures No financial relationships to disclose 1. Labral anatomy 2. Adaptations of the throwing shoulder
ROTATOR CUFF DISORDERS/IMPINGEMENT
 ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
I (and/or my co-authors) have something to disclose.
 have something to disclose.") Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
SLAP Repairs Versus Biceps Tenodesis in Athletes 15 min
 SLAP Repairs Versus Biceps Tenodesis in Athletes 15 min Power Points Not all SLAP tears need surgery Preservation of Native Anatomy GOAL Not all labral repairs are equal Kinetic chain MUST be addressed
SLAP Repairs Versus Biceps Tenodesis in Athletes 15 min Power Points Not all SLAP tears need surgery Preservation of Native Anatomy GOAL Not all labral repairs are equal Kinetic chain MUST be addressed
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
Sports Medicine: Shoulder Arthrography. Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System
 Sports Medicine: Shoulder Arthrography Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Disclosure Off-label use for gadolinium Pediatric Sports Injuries
Sports Medicine: Shoulder Arthrography Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Disclosure Off-label use for gadolinium Pediatric Sports Injuries
Lawrence Gulotta Gillian Lieberman, MD October Gillian Lieberman, MD. Shoulder Imaging. Lawrence V. Gulotta, HMS IV 10/16/02
 October 2002 Shoulder Imaging Lawrence V. Gulotta, HMS IV 10/16/02 Goals Review Anatomy of the Shoulder -Dynamic Stabilizers -> Rotator Cuff -Static Stabilizers -> Labrum and Capsule Systematic Approach
October 2002 Shoulder Imaging Lawrence V. Gulotta, HMS IV 10/16/02 Goals Review Anatomy of the Shoulder -Dynamic Stabilizers -> Rotator Cuff -Static Stabilizers -> Labrum and Capsule Systematic Approach
Upper Extremity Injuries in Youth Baseball: Causes and Prevention
 Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
The Shoulder. Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014
 The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
Management of Anterior Shoulder Instability
 Management of Anterior Shoulder Instability Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Management of Anterior Shoulder Instability Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Glenohumeral Capsule Tears in Baseball Pitchers
 Glenohumeral Capsule Tears in Baseball Pitchers Christopher S. Ahmad, MD Professor Orthopedic Surgery Chief Sports Medicine Head Team Physician New York Yankees New York City Football Club Disclosure 1.
Glenohumeral Capsule Tears in Baseball Pitchers Christopher S. Ahmad, MD Professor Orthopedic Surgery Chief Sports Medicine Head Team Physician New York Yankees New York City Football Club Disclosure 1.
SLAP Lesions Assessment & Treatment
 SLAP Lesions Assessment & Treatment Kevin E. Wilk,, PT, DPT Glenoid Labral Lesions Introduction Common injury - difficult to diagnose May occur in isolation or in combination SLAP lesions: Snyder: Arthroscopy
SLAP Lesions Assessment & Treatment Kevin E. Wilk,, PT, DPT Glenoid Labral Lesions Introduction Common injury - difficult to diagnose May occur in isolation or in combination SLAP lesions: Snyder: Arthroscopy
Shoulder Arthroscopy. Dr. J.J.A.M. van Raaij. NOV Jaarvergadering Den Bosch 25 jan 2018
 Shoulder Arthroscopy Dr. J.J.A.M. van Raaij NOV Jaarvergadering Den Bosch 25 jan 2018 No disclosures Disclosure Shoulder Instability Traumatic anterior Traumatic posterior Acquired atraumatic Multidirectional
Shoulder Arthroscopy Dr. J.J.A.M. van Raaij NOV Jaarvergadering Den Bosch 25 jan 2018 No disclosures Disclosure Shoulder Instability Traumatic anterior Traumatic posterior Acquired atraumatic Multidirectional
P.O. Box Sierra Park Road Mammoth Lakes, CA Orthopedic Surgery & Sports Medicine
 P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
Superior Labral Pathology in Throwers
 Superior Labral Pathology in Throwers Disclosures Available via AAOS website None relevant to this presentation L. Pearce McCarty, III M.D. Team Physician, Minnesota Twins Chairman, Orthopedic Surgery,
Superior Labral Pathology in Throwers Disclosures Available via AAOS website None relevant to this presentation L. Pearce McCarty, III M.D. Team Physician, Minnesota Twins Chairman, Orthopedic Surgery,
Disclosure 11/14/2016. Partial Thickness Rotator Cuff Tears in the Throwing Athlete. Partial Thickness Rotator Cuff Tears. Neal S. ElAttrache, M.D.
 Partial Thickness Rotator Cuff Tears in the Throwing Athlete Neal S. ElAttrache, M.D. Disclosure I, Neal ElAttrache, or a family member(s), have relevant financial relationships to be discussed, directly
Partial Thickness Rotator Cuff Tears in the Throwing Athlete Neal S. ElAttrache, M.D. Disclosure I, Neal ElAttrache, or a family member(s), have relevant financial relationships to be discussed, directly
Glenohumeral Joint Instability. Static Stabilizers of the GHJ. Static Stabilizers of the GHJ. Static Stabilizers of the GHJ
 1 Glenohumeral Joint Instability GHJ Joint Stability: Or Lack Thereof! Christine B. Chung, M.D. Assistant Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Static Stabilizers
1 Glenohumeral Joint Instability GHJ Joint Stability: Or Lack Thereof! Christine B. Chung, M.D. Assistant Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Static Stabilizers
Arthroscopy / MRI Correlation Conference. Department of Radiology, Section of MSK Imaging Department of Orthopedic Surgery 7/19/16
 Arthroscopy / MRI Correlation Conference Department of Radiology, Section of MSK Imaging Department of Orthopedic Surgery 7/19/16 Case 1: 29 YOM with recurrent shoulder dislocations Glenoid Axial T1FS
Arthroscopy / MRI Correlation Conference Department of Radiology, Section of MSK Imaging Department of Orthopedic Surgery 7/19/16 Case 1: 29 YOM with recurrent shoulder dislocations Glenoid Axial T1FS
Patient ID. Case Conference. Physical Examination. Image examination. Treatment 2011/6/16
 Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Ultrasound of the Shoulder
 Ultrasound of the Shoulder Patrick Battaglia, DC, DACBR Logan University, Department of Radiology Outline Review ultrasound appearance of NMSK tissues Present indications for ultrasound of the shoulder.
Ultrasound of the Shoulder Patrick Battaglia, DC, DACBR Logan University, Department of Radiology Outline Review ultrasound appearance of NMSK tissues Present indications for ultrasound of the shoulder.
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT
 SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
Rotator Cuff Repair TRENDS OF REPAIRS. Evolution of Arthroscopic Repair. Shoulder Girdle. Rotator Cuff Repair 8/29/2013
 Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
Partial Thickness Rotator Cuff Tears: All-Inside Repair of PASTA Lesions in Athletes
 Partial Thickness Rotator Cuff Tears: All-Inside Repair of PASTA Lesions in Athletes Thomas M. DeBerardino, MD Associate Professor, UConn Health Center Team Physician, Orthopaedic Consultant UConn Huskie
Partial Thickness Rotator Cuff Tears: All-Inside Repair of PASTA Lesions in Athletes Thomas M. DeBerardino, MD Associate Professor, UConn Health Center Team Physician, Orthopaedic Consultant UConn Huskie
Anterior shoulder instability: Evaluation using MR arthrography.
 Anterior shoulder instability: Evaluation using MR arthrography. Poster No.: C-2407 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Lord, I. Katsimilis, N. Purohit, V. T. Skiadas; Southampton/UK
Anterior shoulder instability: Evaluation using MR arthrography. Poster No.: C-2407 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Lord, I. Katsimilis, N. Purohit, V. T. Skiadas; Southampton/UK
Anatomy GH Joint. Glenohumeral Instability. Components of Stability. Components of Stability 7/7/2017. AllinaHealthSystem
 Glenohumeral Instability Dr. John Steubs Allina Sports Medicine Conference July 7, 2017 Anatomy GH Joint Teardrop or oval shape Inherently unstable Golf ball and tee analogy Stabilizers Static Dynamic
Glenohumeral Instability Dr. John Steubs Allina Sports Medicine Conference July 7, 2017 Anatomy GH Joint Teardrop or oval shape Inherently unstable Golf ball and tee analogy Stabilizers Static Dynamic
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint injuries in football players, 318, 319 ALPSA. See Anterior labroligamentous periosteal sleeve avulsion. Anterior
Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint injuries in football players, 318, 319 ALPSA. See Anterior labroligamentous periosteal sleeve avulsion. Anterior
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Shoulder Arthroscopy Lab Manual
 Shoulder Arthroscopy Lab Manual Dalhousie University Orthopaedic Program May 5, 2017 Skills Centre OBJECTIVES 1. Demonstrate a competent understanding of the arthroscopic anatomy and biomechanics of the
Shoulder Arthroscopy Lab Manual Dalhousie University Orthopaedic Program May 5, 2017 Skills Centre OBJECTIVES 1. Demonstrate a competent understanding of the arthroscopic anatomy and biomechanics of the
Shoulder Pain: Diagnosis and Management
 Shoulder Pain: Diagnosis and Management Thomas J. Gill, M.D. Director, Boston Sports Medicine and Research Institute Associate Professor of Orthopedic Surgery Tufts Medical School www.bostonsportsmedicine.com
Shoulder Pain: Diagnosis and Management Thomas J. Gill, M.D. Director, Boston Sports Medicine and Research Institute Associate Professor of Orthopedic Surgery Tufts Medical School www.bostonsportsmedicine.com
Clinical pearls for the shoulder/arm exam and the treatment. What is seeing youare you seeing it
 Clinical pearls for the shoulder/arm exam and the treatment What is seeing youare you seeing it W. Ben Kibler, MD Medical director Case 1 18 y/o R hand dominant high school pitcher, with 6 week hx gradual
Clinical pearls for the shoulder/arm exam and the treatment What is seeing youare you seeing it W. Ben Kibler, MD Medical director Case 1 18 y/o R hand dominant high school pitcher, with 6 week hx gradual
Introduction & Question 1
 Page 1 of 7 www.medscape.com To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/424981 Case Q & A Shoulder Pain, Part
Page 1 of 7 www.medscape.com To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/424981 Case Q & A Shoulder Pain, Part
Common Surgical Shoulder Injury Repairs
 Common Surgical Shoulder Injury Repairs Mr Ilia Elkinson BHB, MBChB, FRACS (Ortho), FNZOA Orthopaedic and Upper Limb Surgeon Bowen Hospital Wellington Hospital Objectives Review pertinent anatomy of the
Common Surgical Shoulder Injury Repairs Mr Ilia Elkinson BHB, MBChB, FRACS (Ortho), FNZOA Orthopaedic and Upper Limb Surgeon Bowen Hospital Wellington Hospital Objectives Review pertinent anatomy of the
Subacromial Impingement (diagnostic methods )
") Subacromial Impingement (diagnostic methods ) M.N. Naderi Fellowship in shoulder and arthroscopic surgery Neer : Definition Impingement on the tendinous portion of the rotator cuff by the coracoacromial
Subacromial Impingement (diagnostic methods ) M.N. Naderi Fellowship in shoulder and arthroscopic surgery Neer : Definition Impingement on the tendinous portion of the rotator cuff by the coracoacromial
Management of Massive/Revision Rotator Cuff Tears
 Management of Massive/Revision Rotator Cuff Tears Nikhil N. Verma MD, Director Sports Medicine, Rush University Medical Center, Midwest Orthopedics at Rush, Chicago, IL nverma@rushortho.com I. Anatomy
Management of Massive/Revision Rotator Cuff Tears Nikhil N. Verma MD, Director Sports Medicine, Rush University Medical Center, Midwest Orthopedics at Rush, Chicago, IL nverma@rushortho.com I. Anatomy
The suction cup mechanism is enhanced by the slightly negative intra articular pressure within the joint.
 SHOULDER INSTABILITY Stability A. The stability of the shoulder is improved by depth of the glenoid. This is determined by: 1. Osseous glenoid, 2. Articular cartilage of the glenoid, which is thicker at
SHOULDER INSTABILITY Stability A. The stability of the shoulder is improved by depth of the glenoid. This is determined by: 1. Osseous glenoid, 2. Articular cartilage of the glenoid, which is thicker at
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Your shoulder is the most flexible joint in your body, allowing you to throw fastballs, lift a heavy suitcase, scratch your back, and reach in almost any direction. Your shoulder joint
SHOULDER INSTABILITY Your shoulder is the most flexible joint in your body, allowing you to throw fastballs, lift a heavy suitcase, scratch your back, and reach in almost any direction. Your shoulder joint
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
Index. Note: Page numbers of article titles are in boldface type.
 Magn Reson Imaging Clin N Am 12 (2004) 185 189 Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint, MR imaging findings concerning, 161 Acromion, types of, 77 79
Magn Reson Imaging Clin N Am 12 (2004) 185 189 Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint, MR imaging findings concerning, 161 Acromion, types of, 77 79
Throwing Injuries and Prevention: The Physical Therapy Perspective
 Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
ANATOMY / BIOMECHANICS LONG HEAD OF BICEPS ATTACHES AT THE SUPERIOR GLENOIDAL TUBERCLE WITH THE LABRUM FIBROCARTILAGINOUS TISSUE IF THERE IS A TORN SU
 SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Christopher A Brown, MD Sports Medicine Orthopedist. Duke Orthopedic Residency Sports Medicine Fellowship Stanford
 Christopher A Brown, MD Sports Medicine Orthopedist Duke Orthopedic Residency Sports Medicine Fellowship Stanford Office Geneva Newark Opening Canandaigua and Penfield Topics Of Discussion Shoulder dislocation
Christopher A Brown, MD Sports Medicine Orthopedist Duke Orthopedic Residency Sports Medicine Fellowship Stanford Office Geneva Newark Opening Canandaigua and Penfield Topics Of Discussion Shoulder dislocation
Labral Tears. Fig 1: Intact labrum and biceps tendon
 Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Recurrent Shoulder Dislocation.
 Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012
 Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012 Multiaxial ball and socket Little Inherent Instability Glenohumeral
Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012 Multiaxial ball and socket Little Inherent Instability Glenohumeral
DIFFERENTIAL DIAGNOSIS: Looking for the causes of impingement
 DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
DK7215-Levine-ch12_R2_211106
 12 Arthroscopic Rotator Interval Closure Andreas H. Gomoll Department of Orthopedic Surgery, Brigham and Women s Hospital, Harvard Medical School, Boston, Massachusetts, U.S.A. Brian J. Cole Departments
12 Arthroscopic Rotator Interval Closure Andreas H. Gomoll Department of Orthopedic Surgery, Brigham and Women s Hospital, Harvard Medical School, Boston, Massachusetts, U.S.A. Brian J. Cole Departments
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
What can Imaging tell us?
 What can Imaging tell us? David Connell FRANZCR, FFSEM (UK) Assoc Professor Dept of Medicine, Nursing & Healthcare Monash University, Melbourne, Australia Assoc Professor Sport & Exercise Medicine Research
What can Imaging tell us? David Connell FRANZCR, FFSEM (UK) Assoc Professor Dept of Medicine, Nursing & Healthcare Monash University, Melbourne, Australia Assoc Professor Sport & Exercise Medicine Research
Football and netball season A review of the apophysis and the acute shoulder: assessment. Simon Locke Sport and Exercise Physician
 Football and netball season A review of the apophysis and the acute shoulder: assessment Simon Locke Sport and Exercise Physician Apophyseal injuries; How to diagnose and manage? Goals for tonight Recognise
Football and netball season A review of the apophysis and the acute shoulder: assessment Simon Locke Sport and Exercise Physician Apophyseal injuries; How to diagnose and manage? Goals for tonight Recognise
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai
 POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai Posterior instability is less common among cases of shoulder instability, accounting for 2% to 10% of all cases of instability. More common in sporting groups:
POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai Posterior instability is less common among cases of shoulder instability, accounting for 2% to 10% of all cases of instability. More common in sporting groups:
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abduction pillow, ultrasling, 880, 881, 882, 883 Adolescents, shoulder instability in. See Shoulder, instability of, pediatric and adolescent.
Index Note: Page numbers of article titles are in boldface type. A Abduction pillow, ultrasling, 880, 881, 882, 883 Adolescents, shoulder instability in. See Shoulder, instability of, pediatric and adolescent.
Diagnosis and Treatment of Common Shoulder Disorders
 Diagnosis and Treatment of Common Shoulder Disorders NAOEM Oct 14 th, 2017 Michael Codsi, M.D. www.drcodsi.com Learning Objectives SLAP tears diagnosis, imaging and treatment How to diagnose rotator cuff
Diagnosis and Treatment of Common Shoulder Disorders NAOEM Oct 14 th, 2017 Michael Codsi, M.D. www.drcodsi.com Learning Objectives SLAP tears diagnosis, imaging and treatment How to diagnose rotator cuff
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D.
 Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX Tel#
 Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX 78240 www.saspine.com Tel# 210-487-7463 PATIENT GUIDE TO SHOULDER INSTABILITY LABRAL (BANKART) REPAIR / CAPSULAR SHIFT WHAT IS
Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX 78240 www.saspine.com Tel# 210-487-7463 PATIENT GUIDE TO SHOULDER INSTABILITY LABRAL (BANKART) REPAIR / CAPSULAR SHIFT WHAT IS
SLAP Lesions of the Shoulder
 Arthroscopy: The Journal of Arthroscopic and Related Surgery 6(4):21&279 Published by Raven Press, Ltd. Q 1990 Arthroscopy Association of North America SLAP Lesions of the Shoulder Stephen J. Snyder, M.D.,
Arthroscopy: The Journal of Arthroscopic and Related Surgery 6(4):21&279 Published by Raven Press, Ltd. Q 1990 Arthroscopy Association of North America SLAP Lesions of the Shoulder Stephen J. Snyder, M.D.,
MRI of Shoulder Instabilities
 MRI of Shoulder Instabilities Anna Hirschmann, MD Musculoskeletal Division Clinic of Radiology and Nuclear Medicine University of Basel Hospital Glenohumeral Articulation Centering of the humeral head
MRI of Shoulder Instabilities Anna Hirschmann, MD Musculoskeletal Division Clinic of Radiology and Nuclear Medicine University of Basel Hospital Glenohumeral Articulation Centering of the humeral head
Shoulder Instability
 J F de Beer, K van Rooyen, D Bhatia Shoulder Instability INSTABILITY means that the shoulder dislocates completely (dislocation) or partially (subluxation). Anatomy The shoulder consists of a ball (humeral
J F de Beer, K van Rooyen, D Bhatia Shoulder Instability INSTABILITY means that the shoulder dislocates completely (dislocation) or partially (subluxation). Anatomy The shoulder consists of a ball (humeral
US finding of the shoulder (with live demonstration) 인제의대상계백병원 안재기
 인제의대상계백병원 안재기") US finding of the shoulder (with live demonstration) 인제의대상계백병원 안재기 Shoulder US Biceps tendon & Rotator Cuff Long Head of Biceps Tendon Subscapularis tendon Supraspinatus tendon Infraspinatus tendon Teres
US finding of the shoulder (with live demonstration) 인제의대상계백병원 안재기 Shoulder US Biceps tendon & Rotator Cuff Long Head of Biceps Tendon Subscapularis tendon Supraspinatus tendon Infraspinatus tendon Teres
Case 1: Primary Dislocation. How I Manage Failed Instability Surgery. Case Presentations: Shoulder Instability
 Case Presentations: Shoulder Instability Chicago Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Team Physician, Chicago White Sox and Bulls Chief Medical Editor, Orthopaedics
Case Presentations: Shoulder Instability Chicago Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Team Physician, Chicago White Sox and Bulls Chief Medical Editor, Orthopaedics
Posterior Shoulder Instability
 Posterior Shoulder Instability Robert A. Arciero, MD Professor of Orthopaedics University of Connecticut USA Classification of Posterior Instability Dislocation -acute -chronic- fixed or locked Subluxation
Posterior Shoulder Instability Robert A. Arciero, MD Professor of Orthopaedics University of Connecticut USA Classification of Posterior Instability Dislocation -acute -chronic- fixed or locked Subluxation
Case 1. Exam. Cases. Shoulder Service
 Cases Friday Afternoon Session Case 1 49 yr male Injury with loss of active elevation and now an internal rotation drop at side Lifting 20 lb bag at time Mild previous infrequent shoulder pain Exam AFE:
Cases Friday Afternoon Session Case 1 49 yr male Injury with loss of active elevation and now an internal rotation drop at side Lifting 20 lb bag at time Mild previous infrequent shoulder pain Exam AFE:
Shoulder Labral Tear and Shoulder Dislocation
 Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
Shoulder Injuries. Glenoid labrum injuries. SLAP Lesions
 Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
SHOULDER ANATOMY AND FUNCTION. Disclosure. Case. Learning Objectives MRI. Plan? 3/23/2017 5
 Disclosure Doc, My Shoulder Keeps me Up at Night! Evaluation and Treatment of Atraumatic Shoulder Pain Matthew F. Dilisio, MD Shoulder and Elbow Surgery, CHI Health Orthopedics Assistant Professor, Creighton
Disclosure Doc, My Shoulder Keeps me Up at Night! Evaluation and Treatment of Atraumatic Shoulder Pain Matthew F. Dilisio, MD Shoulder and Elbow Surgery, CHI Health Orthopedics Assistant Professor, Creighton
Shoulder Case Studies
 Shoulder Case Studies Eden Raleigh Orthopaedic Surgeon Shoulder & Knee Surgery Ph: 9421 1900 0402697115 dredenraleigh@gmail.com My Background Specialising in Shoulder and Knee Surgery Main focus on Arthroscopic/Sports
Shoulder Case Studies Eden Raleigh Orthopaedic Surgeon Shoulder & Knee Surgery Ph: 9421 1900 0402697115 dredenraleigh@gmail.com My Background Specialising in Shoulder and Knee Surgery Main focus on Arthroscopic/Sports
IMPINGEMENT-TESTSTESTS
 «thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
«thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Shoulder Arthroscopy Portals
 Shoulder Arthroscopy Portals Alper Deveci and Metin Dogan 7 7.1 Bony Landmarks Before starting shoulder arthroscopy, the patient must be positioned and draping applied. Then the bony landmarks are identified
Shoulder Arthroscopy Portals Alper Deveci and Metin Dogan 7 7.1 Bony Landmarks Before starting shoulder arthroscopy, the patient must be positioned and draping applied. Then the bony landmarks are identified
The Upper Limb. Elbow Rotation 4/25/18. Dr Peter Friis
 The Upper Limb Dr Peter Friis Elbow Rotation Depending upon the sport, the elbow moves through an arc of approximately 75⁰ to 100⁰ in about 20 to 35 msec. The resultant angular velocity is between 1185
The Upper Limb Dr Peter Friis Elbow Rotation Depending upon the sport, the elbow moves through an arc of approximately 75⁰ to 100⁰ in about 20 to 35 msec. The resultant angular velocity is between 1185
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA
 Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Technique For SLAP Repair in 2016
 Technique For SLAP Repair in 2016 Eric J. Strauss MD Division of Sports Medicine NYU Hospital for Joint Diseases Hospital for Joint Diseases Department of Orthopaedic Surgery Disclosures Joint Restoration
Technique For SLAP Repair in 2016 Eric J. Strauss MD Division of Sports Medicine NYU Hospital for Joint Diseases Hospital for Joint Diseases Department of Orthopaedic Surgery Disclosures Joint Restoration
Gregory P. Nicholson, M.D. Disclosures. Indications for Open RCR. Open RC Repairs 2015 and Role of Tendon Transfers. Associate Professor
 Open RC Repairs 2015 and Role of Tendon Transfers Gregory P. Nicholson, M.D. Associate Professor Rush University Medical Center Chicago, Illinois Disclosures Research and Educational Support: Tornier,
Open RC Repairs 2015 and Role of Tendon Transfers Gregory P. Nicholson, M.D. Associate Professor Rush University Medical Center Chicago, Illinois Disclosures Research and Educational Support: Tornier,
Rotator cuff. MR Imaging of the Shoulder: Rotator Cuff. Trauma. Trauma. Trauma. Tendon calcification. Acute. Degenerative. Trauma Calcific tendinitis
 Rotator cuff MR Imaging of the Shoulder: Rotator Cuff Dr. Mini N. Pathria M.D., FRCP(C) Department of Radiology University of California School of Medicine San Diego, California Acute Trauma Calcific tendinitis
Rotator cuff MR Imaging of the Shoulder: Rotator Cuff Dr. Mini N. Pathria M.D., FRCP(C) Department of Radiology University of California School of Medicine San Diego, California Acute Trauma Calcific tendinitis
MR Arthrography of the Shoulder - A Beginner's Guide
 MR Arthrography of the Shoulder - A Beginner's Guide Poster No.: C-1034 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Jain, S. Connolly; Prescot/UK Keywords: Pathology, Arthrography, MR, Musculoskeletal
MR Arthrography of the Shoulder - A Beginner's Guide Poster No.: C-1034 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Jain, S. Connolly; Prescot/UK Keywords: Pathology, Arthrography, MR, Musculoskeletal
OBJECTIVES. Therapists Management of Shoulder Instability SHOULDER STABILITY SHOULDER STABILITY WHAT IS SHOULDER INSTABILITY? SHOULDER INSTABILITY
 Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Common Shoulder Problems and Treatment Options. Benjamin W. Szerlip D.O. Austin Shoulder Institute
 Common Shoulder Problems and Treatment Options Benjamin W. Szerlip D.O. Austin Shoulder Institute Speaker Disclosure Dr. Szerlip has disclosed that he has no actual or potential conflict of interest in
Common Shoulder Problems and Treatment Options Benjamin W. Szerlip D.O. Austin Shoulder Institute Speaker Disclosure Dr. Szerlip has disclosed that he has no actual or potential conflict of interest in
Strategies for Failed Instability Repair
 Strategies for Failed Instability Repair Robert E Hunter MD Director, Orthopedic Sports Medicine Center HRRMC Salida, Colorado CU Sports Medicine Course Sept 28, 2012 Conflict of Interest Paid Consultant:
Strategies for Failed Instability Repair Robert E Hunter MD Director, Orthopedic Sports Medicine Center HRRMC Salida, Colorado CU Sports Medicine Course Sept 28, 2012 Conflict of Interest Paid Consultant:
The Shoulder. By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson
 The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
11/13/2017. Disclosures: The Irreparable Rotator Cuff. I am a consultant for Arhtrex, Inc and Endo Pharmaceuticals.
 Massive Rotator Cuff Tears without Arthritis THE CASE FOR SUPERIOR CAPSULAR RECONSTRUCTION MICHAEL GARCIA, MD NOVEMBER 4, 2017 FLORIDA ORTHOPAEDIC INSTITUTE Disclosures: I am a consultant for Arhtrex,
Massive Rotator Cuff Tears without Arthritis THE CASE FOR SUPERIOR CAPSULAR RECONSTRUCTION MICHAEL GARCIA, MD NOVEMBER 4, 2017 FLORIDA ORTHOPAEDIC INSTITUTE Disclosures: I am a consultant for Arhtrex,
My shoulder popped out what now?
 My shoulder popped out what now? Richard Dallalana Epworth Shoulder Symposium June 2017 Shoulder Dislocation First event Best approach? Manual Reduction Should it be put back on field? - YES Prone lying
My shoulder popped out what now? Richard Dallalana Epworth Shoulder Symposium June 2017 Shoulder Dislocation First event Best approach? Manual Reduction Should it be put back on field? - YES Prone lying
Massive Rotator Cuff Tears. Rafael M. Williams, MD
 Massive Rotator Cuff Tears Rafael M. Williams, MD Rotator Cuff MRI MRI Small / Partial Thickness Medium Tear Arthroscopic View Massive Tear Fatty Atrophy Arthroscopic View MassiveTears Tear is > 5cm
Massive Rotator Cuff Tears Rafael M. Williams, MD Rotator Cuff MRI MRI Small / Partial Thickness Medium Tear Arthroscopic View Massive Tear Fatty Atrophy Arthroscopic View MassiveTears Tear is > 5cm
Shoulder Arthroscopy Curriculum
 ARTHRO Mentor 1 Description All those with an interest in the shoulder should develop a basic level of proficiency and should be able to perform a thorough diagnostic exam, looking from both the anterior
ARTHRO Mentor 1 Description All those with an interest in the shoulder should develop a basic level of proficiency and should be able to perform a thorough diagnostic exam, looking from both the anterior
Double bucket handle tears of the superior labrum
 Case Report http://dx.doi.org/10.14517/aosm13013 pissn 2289-005X eissn 2289-0068 Double bucket handle tears of the superior labrum Dong-Soo Kim, Kyoung-Jin Park, Yong-Min Kim, Eui-Sung Choi, Hyun-Chul
Case Report http://dx.doi.org/10.14517/aosm13013 pissn 2289-005X eissn 2289-0068 Double bucket handle tears of the superior labrum Dong-Soo Kim, Kyoung-Jin Park, Yong-Min Kim, Eui-Sung Choi, Hyun-Chul
Suprascapular Nerve: How to identify when it is a problem and what to do? Speaker Disclosure
 Suprascapular Nerve: How to identify when it is a problem and what to do? Eric C. McCarty, MD Associate Professor Chief of Sports Medicine and Shoulder Surgery University of Colorado School of Medicine
Suprascapular Nerve: How to identify when it is a problem and what to do? Eric C. McCarty, MD Associate Professor Chief of Sports Medicine and Shoulder Surgery University of Colorado School of Medicine
Management of Humeral Bone Loss in Anterior Shoulder Instability. Scott D. Mair, MD University of Kentucky Sports Medicine
 Management of Humeral Bone Loss in Anterior Shoulder Instability Scott D. Mair, MD University of Kentucky Sports Medicine Disclosure Smith and Nephew Endoscopy fellowship support Importance Bone loss (glenoid
Management of Humeral Bone Loss in Anterior Shoulder Instability Scott D. Mair, MD University of Kentucky Sports Medicine Disclosure Smith and Nephew Endoscopy fellowship support Importance Bone loss (glenoid
Glenohumeral Joint Instability: An Athlete s Perspective
 Anatomic Considerations Glenohumeral Joint Instability: An Athlete s Perspective Michael D. Loeb, MD Texas Orthopedics, Sports Medicine, and Rehabilitation Associates Austin, Texas Static Stabilizers Osseous
Anatomic Considerations Glenohumeral Joint Instability: An Athlete s Perspective Michael D. Loeb, MD Texas Orthopedics, Sports Medicine, and Rehabilitation Associates Austin, Texas Static Stabilizers Osseous
Current Controversies in Shoulder Surgery:
 Current Controversies in Shoulder Surgery: Shoulder Instability Rotator Cuff Injury and Repair Reverse Shoulder Arthroplasty Brian Feeley, MD UC San Francisco Sports Medicine and Shoulder Surgery Disclosures
Current Controversies in Shoulder Surgery: Shoulder Instability Rotator Cuff Injury and Repair Reverse Shoulder Arthroplasty Brian Feeley, MD UC San Francisco Sports Medicine and Shoulder Surgery Disclosures